Embed Size (px)
Citation preview

494 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
ABSTRACT• Objectives: To conduct a systematic review of the
literatureexamininginterventionsdeliveredbyhealthcarepractitionerstoimprovemedicationadherenceinpatientswithdiabetesmellitus(DM).
• Methods: Databases were searched up to 2 July2013toidentifyeligiblestudiesthatincludedinterven-tions that were conducted in a clinic-based settinganddeliveredbyahealthcarepractitioner(eg,nurse,physician,diabeteseducator) to improveadherencetodiabetesmedications(includingoralhypoglycemicagentsandinsulin).Articleswerelimitedtopublishedclinical trials conducted inadults≥ 18yearsofageandpublishedinEnglish-languagejournals.
• Results:18paperswerereviewed:15trialstargetedpatientswithDM,3targetedhealthcarepractitioners.7 patient-focused and 1 practitioner-focused trialdemonstrated a beneficial effect of the interventioncomparedwithacontrol group.Thepatient-focusedtrialswerecomplex interventions involvingacombi-nation of adherence-enhancing strategies such asindividualizedpatientcounseling,tailoredpatientedu-cation, medication reminders, behavioral feedbackand reinforcement, and caremanagement byancil-lary staff, nurses, text message or telephone-linkedsystem. The practitioner-focused trial employed anelectronicfeedbacksystemforindividualizedcareandquality improvement.Limitationsincludedthediversityin the measures employed to assess adherence; dif-feringdefinitionsofadherence;theinclusionofpatientsregardlessofbaselineadherencestatus;andtheshortdurationofthetrials.
• Conclusions:Additionalresearchisneededtounder-standtheconditionsunderwhichinterventionstarget-ing thepatient-practitioner interaction canbe imple-mentedinclinicsettingstoimprovemedicationadher-enceinpatientswithDM.
The prevalence of diabetes mellitus (DM) has grown to epidemic proportions. DM affects nearly 26 million Americans, ranking as the 7th leading
cause of death in the United States, and is a major risk factor for stroke, heart disease, kidney disease, blindness and lower-limb amputations [1]. Despite the availability of numerous efficacious treatments (eg, oral hypoglyce-mic agents and insulin) to manage DM, and their proven efficacy in reducing cardiovascular morbidity and mor-tality, adherence to treatment remains suboptimal [2]. Recent systematic reviews have documented medication adherence rates for oral hypoglycemic agents (as assessed by self-report and objective measures) ranging from 36% to 93% among patients with DM [3,4]. Rates of insulin adherence range from 62% to 64% depending on the population studied [3]. Poor adherence to DM treatments is a major contributor to inadequate glycemic control and is estimated to incur up to $289 billion annually in direct healthcare costs [5–7]. Given these consequences, patient nonadherence has been described as one of the greatest challenges for successful treatment of chronic diseases such as DM [8].
The definition of medication adherence has taken nu-merous forms over time. Once regarded as the patient’s responsibility (eg, compliance), the success of the pre-scribed medication in reaching the intended therapeutic target rested solely on the patient’s ability to understand and execute the health care practitioner’s directions [9]. More recently, adherence has been recognized as a com-plex behavior that requires patients and practitioners to form a partnership based on a shared understanding of one another’s perspectives within a supportive healthcare
A Systematic Review of Interventions to Improve Adherence to Diabetes Medications within the Patient–Practitioner Interaction Antoinette Schoenthaler, EdD, and Yendelela L. Cuffee, PhD, MPH
From the Center for Healthful Behavior Change, Department of Population Health, New York University School of Medi-cine, New York, NY.

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 495
delivery system [8,10]. When patients and practitioners engage in a collaborative relationship that includes shared decision-making [11,12], patient-centeredness [13–15], and information exchange[16,17], patients are more likely to report better adherence to their medications.
While much work has been done to identify patient factors, and to a lesser extent practitioner factors, associ-ated with better medication adherence in patients with DM in observational studies, effective intervention ap-proaches that practitioners can incorporate into clinical practice has not been evaluated. In this systematic review, we appraise the existing literature examining interven-tions delivered by health care practitioners on medication adherence in patients with DM.
METHODSSearch StrategyThe search strategy were similar to the ones used by Cra-mer et al [3] (in their systematic review of adherence to diabetes medications) and McDonald et al [18] (in their systematic review of interventions to improve adherence to medications). To identify manuscripts that met inclu-sion criteria for this review, we used standard Cochrane Collaboration systematic review techniques [19]. The PubMed and EMBASE databases were searched from in-ception to 2 July 2013 for our concepts. In addition, key articles from each search were run in PubMed using the “related articles” feature to identify further articles. Ad-ditional strategies included searching the bibliographies of eligible articles and searching other systematic reviews and meta-analyses for relevant articles. The concepts for medication adherence, intervention type, and diabetes were included in the search with several keyword syn-onyms and the subject headings for practitioner-patient relations. Articles were limited to reports of clinical trials published in English-language peer-reviewed journals and conducted in adults (age ≥ 18 years). The full search strategy in PubMed is available online.
Eligibility CriteriaStudies were eligible for the review if they met the fol-lowing criteria: (1) patients had a diagnosis of diabetes; (2) included an intervention to improve adherence to dia-betes medications (including oral hypoglycemic agents and insulin); (3) there was assessment of medication adherence as an outcome either through electronic moni-toring devices, self-report, pill counts or pharmacy refills; (4) the intervention took place in a clinic-based setting
and delivered by a health care practitioner, defined as either a nurse, physician, diabetes educator, or care man-ager; and (5) the study was a clinical trial (case-control study or randomized controlled trial [RCT]). We ex-cluded studies that included pharmacist-led interventions given that this topic has been addressed in other recent systematic reviews [20–24]. We also excluded studies that did not report adherence rates for diabetes medications or the methods used to determine medication adherence. The outcome of interest was the between-group differ-ence in medication adherence between intervention and control arms.
Data ExtractionAll titles and abstracts from the search were reviewed independently by the authors. Citations were categorized as potentially relevant, not clearly relevant, or gave insuf-ficient information to make a judgment. Any disagree-ments about inclusion in the review were discussed by the authors, with all differences resolved by consensus. Percent agreement between the 2 authors was high (86%) across all reviewed citations. Printed copies of all poten-tially relevant citations were obtained. The authors inde-pendently abstracted all data from the eligible citations. Data were abstracted from tables, figures, and text using a structured data collection form. Data including partici-pant and site characteristics, study methods, outcomes, and risk of bias were collected on the form. In addition, 2 authors of potentially relevant citations were contacted about unpublished data. Risk of bias for each study was assessed using the guidelines outlined in The Cochrane Collaboration Handbook for Systematic Review of Interventions [19]. Percent agreement between the au-thors was high (96%) across all abstracted data.
RESULTS
A total of 1011 articles were identified, 24 of which were extracted for full review. Six of these studies were ex-cluded for one of the following reasons: incomplete data on adherence outcome [25, 26], the intervention was not clinic-based [27–29], or the adherence assessment was not specific to diabetes medications [30]. Thus, 18 trials were included in this systematic review [31–48]. (See page 528 for a Figure summarizing the literature search results.)
Trial Characteristics The characteristics of the included trials are shown in Table 1. Seventeen of the included studies were RCTs
CliniCal Review

496 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
[31–37, 39–48] and 1 was a single-group pre-post study [38]. Among the RCTs, the comparison group was usual care (UC) in 11 trials [32–34, 36, 39–42, 44–46]. An attention control (ie, sessions that are peripheral to the intervention topics to control for additional time and attention) or a minimal intervention was used in 6 tri-als [31, 35,37,43,47,48]. Approximately one-third of the trials (n = 7) were conducted in the United States [32,33,37,41,42,44,45]. The number of participating clin-ics per trial ranged from 1 to 86 (mean, 15). The majority of the trials (n = 11) were conducted in primary care clinics [32–37,41,42,44–46]. Seven trials were conducted in spe-cialty clinics (eg, endocrinology clinic) or tertiary hospital settings [31,38–40,43,47,48].
Fifteen of the trials targeted patients [31–35,37–41,43–45,47,48] and 3 targeted practitioners [36,42,46]. The sample size of the trials ranged from 45 to 2458 patients (median, 197) and 40 to 160 practitioners (me-
dian, 140). Fifty-four percent of the patients were male with a mean age of 58.3 (SD, 5.2) years. Nine trials targeted patients with poor glycemic control (HbA1c > 7.0%) at baseline [33,34,37,39–42,47,48]; one trial targeted patients newly diagnosed with DM [46]. Three of the trials targeted high-risk patients with comorbid conditions including hypertension [33] and depression [32,41]. The practitioner-focused trials targeted primary care physicians, physician assistants, and nurse practitio-ners [36,42,46]. Only one of the practitioner-focused trials reported demographic characteristics [36].
Eleven of the trials (60%) were complex interventions that used a combination of strategies to target multiple self-management behaviors (eg, self-monitoring blood glucose [SMBG], foot care) [26,33,37–40,43–45,47,48] Eleven of the trials were delivered by practitioners that were existing members of the clinic staff [31,33,34,36,37,40–43,46,48]; 7 trials employed ancillary staff for the purposes of the
Table 1.CharacteristicsofIncludedTrials
Study
Study Design
Study Duration
No. of Patients
No. of Providers
% Patients Completing Follow-up
Adherence Measure
HbA1c Measured?
Between- Group
Adherence Improvement?
Intervention Control
Ahmadiouretal,2010 RCT 3mo 87 * * * Pillcount Yes Yes
Bogneretal,2012 RCT 3mo 182 * 98 100 Electronicmonitoringdevice Yes Yes
Edelmanetal,2010 RCT 13mo 239 * 91.7 83.9 Self-report Yes No
Farmeretal,2009 RCT 12mo 453 * 90.6 88 Self-report Yes No
Farmeretal,2012 RCT 3mo 211 * 90.5 95.3 Electronicmonitoringdevice;self-report
Yes Yes
Guldbergetal,2011 RCT 15mo 2458 160 90.6 90.3 Pharmacydata Yes Yes
Heisleretal,2010 RCT 6mo 244 * 92.8 96 Self-report Yes No
Kimetal,2003 RCT 3mo 50 * 80 64 Self-report Yes No
Kimetal,2006 Pre-Post 3mo 45 * 73.3 — Self-report Yes Yes
Koetal,2004 RCT 12mo 180 * 100 97.8 Pillcount Yes No
Linetal,2006 RCT 12mo 329 * 80.5 79.4 Pharmacydata Yes No
Mullanetal,2009 RCT 6mo 85 40 93.8 94.6 Pharmacydata;self-report Yes No
Negarandehetal,2013
RCT 6wk 127 * 96.7 88.9 Self-report No Yes
Pietteetal,2000 RCT 12mo 280 * 89.5 84.7 Self-report Yes Yes
Pietteetal,2001 RCT 12mo 292 * 90.4 95.9 Self-report Yes No
Rubaketal,2011 RCT 12mo 628 140 78 75 Pharmacydata Yes No
Tanetal,2011 RCT 3mo 164 * 95.1 89 Self-report Yes Yes
Wongetal,2005 RCT 6mo 101 * * * Self-report Yes No
*Valuenotreported.

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 497
study [32,35,38,39,44,45,47]. The median duration of the trials was 6 months (range, 1.5–15 months). Follow-up was adequate in majority of the trials (range, 64–100%). Most studies used a single measure of adherence: electronic monitoring devices (EMD) were used in 2 trials [32,34], pill count was used in 2 trials [31,40], pharmacy refills was used in 4 trials [36,41,42,46], and self-report data was collected in 10 trials [33,35,37–39,43–45,47,48]. The Morisky medication adherence scale was the most commonly used self-report measure. Two studies used a combination of objective (eg, EMD or pharmacy) and self-report measures to assess adherence [34,42]. A major-ity (n = 17) of the studies also assessed the impact of the intervention on change in glycemic control. Four trials also assessed the impact of the intervention on changes in patient trust in the practitioner and patient involvement in decision making [42] or perceived satisfaction with the practitioner’s communication skills [34,44,48].
Risk of BiasFifteen of the 17 reviewed RCTs specified the random-ization procedures or included clear description of the allocation concealment procedures [32–38,40–44,46–48]. Eleven of the RCTs included information on blind-ing of the data collection procedures and/or whether the interventionist was blinded to the study objectives [32–35,37,41–45,47]. One trial used the same clinic staff member to deliver the intervention and control arms [43]. The majority of studies adequately reported how incomplete outcome data was handled with most (n = 10) using an intent-to-treat analysis [32–35,37,41,42,44–46] Finally, all of the studies adequately reported data for the primary outcome. A table showing the ratings of risk of bias for each article is available online.
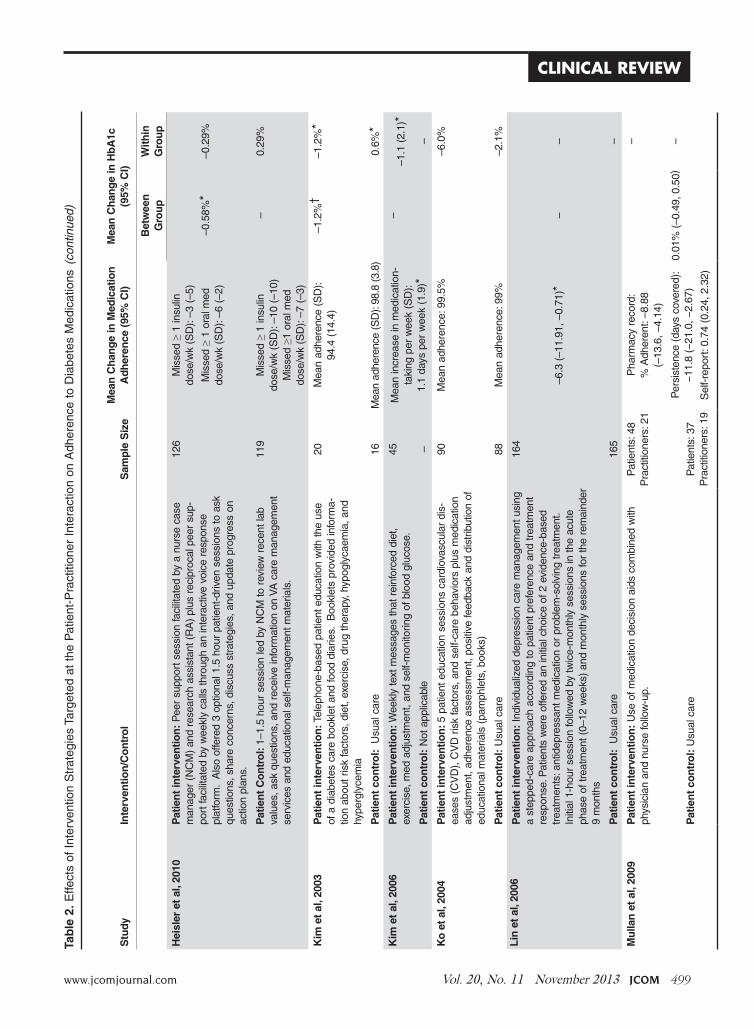
Effects of Included Interventions on Medication AdherenceThe effects of the interventions are summarized below and in Table 2. A meta-analytic approach could not be used to calculate study effect sizes due to the high het-erogeneity of the interventions and measures employed. As such, we only reported whether statistically significant differences were noted in adherence outcomes between the intervention and control groups. Of the 18 included trials, 8 reported statistically significant improvements in medication adherence attributed to the intervention [31,32,34,36,38,43,45,47]. Seven of these trials targeted patients [31,32,34,38,43,45,47] and 1 targeted practi-
tioners [36]. Among the nonsignificant trials, 8 targeted patients [35,37,39–41,44,48] while 2 were practitioner-focused [42,46]. Comparison of participant characteris-tics across trials that reported such data showed that the positive trials tended to consist of a higher percentage of minority patients (32.7% vs. 17.5%) and patients with a high school education or less (60.2% vs. 43.8%) than patients in nonsignificant trials. Patients also had a longer mean duration of time with diabetes in the positive trials (9.18 vs. 7.87 years); however, they were less like to be prescribed insulin (24.3% vs. 33.0%) as compared with patients in nonsignificant trials. Finally, trials reporting positive findings were more likely to be conducted in primary care clinics [32,34,36,45]. Alternatively, tri-als reporting negative findings were more likely to be comprised of older male patients (60.8% male, mean 61.4 years of age vs. 46.3% male, mean 55.8 years of age in positive trials). All 3 studies performed in Veterans Affairs Medical Centers also reported negative findings [33,37,44], which could not be explained by differences in baseline HbA1c or participant health status when compared with negative trials in other clinic settings. Below we describe the characteristics of the positive interventions as compared with nonsignificant trials in terms of the intervention content, methods of interven-tion delivery and dose, assessment of medication adher-ence, and impact on HbA1c. Descriptions are further cat-egorized by intervention target: patients or practitioners.
Patient-Focused InterventionsIntervention content. In the 7 patient-focused trials re-porting positive effects, 3 primarily focused on improving medication adherence [31,32,34]. The interventions were comprised of multiple strategies including medication reminders, care management, individualized counsel-ing to address patient-specific barriers to nonadherence (eg, beliefs about medications, medication cost), patient education, and self-management support [31,32,34]. For example, Bogner et al [32] randomized 180 patients with comorbid DM and depression to either an integrated care intervention or usual care; adherence was assessed with an EMD for a period of 12 weeks. The integrated care inter-vention consisted of individualized sessions that addressed patients’ psychosocial and logistical barriers to adherence while also providing patient education about the course and treatment of DM and depression, and assistance with referrals. Care managers also collaborated with patients’ primary care physician to facilitate adherence to guideline-
CliniCal Review

498 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes MedicationsTa
ble
2.E
ffect
sof
Int
erve
ntio
nS
trat
egie
sTa
rget
eda
tth
eP
atie
nt-P
ract
ition
erI
nter
actio
non
Adh
eren
cet
oD
iabe
tes
Med
icat
ions
Stu
dy
Inte
rven
tion
/Co
ntr
ol
S
amp
le S
ize
M
ean
Ch
ang
e in
Med
icat
ion
A
dh
eren
ce (
95%
CI)
M
ean
Ch
ang
e in
Hb
A1c
(9
5% C
I)
Bet
wee
n
Gro
up
With
in
Gro
up
Ah
mad
iou
r et
al,
2010
Pat
ien
t In
terv
entio
n: 1
2w
eek
educ
atio
nals
essi
ono
nad
here
nce
and
impo
rtan
ceo
fgly
cem
icc
ontr
ol.p
lus
med
icat
ion
diar
y30
Mea
nad
here
nce
(SD
):
97.4
(4.
14)†
Non
-sig
nific
ant;
D
ata
not
repo
rted
–
Pat
ien
t C
on
tro
l:12
wee
ked
ucat
iona
lses
sion
on
adhe
renc
ean
d
impo
rtan
ceo
fgly
cem
icc
ontr
ol.
57M
ean
adhe
renc
e(S
D):
86
.5(
15.7
)–
Bo
gn
er e
t al
, 201
2P
atie
nt
Inte
rven
tion
: 5in
divi
dual
ized
ses
sion
sto
add
ress
pa
tient
-leve
lbar
riers
tod
iabe
tes
and
depr
essi
on.C
olla
bora
ting
with
pa
tient
s’p
rimar
yca
rep
hysi
cian
for
med
icat
ion
man
agem
ent.
88%
≥8
0%a
dher
ent:
65%
†
–1.2
0%
(–1.
56,0
.84)
†
–
Pat
ien
t C
on
tro
l:U
sual
car
e92
%≥
80%
adh
eren
t:30
%–
Ed
elm
an e
t al
, 201
0P
atie
nt
Inte
rven
tion
:G
roup
med
ical
clin
ic(
GM
C)
care
team
ses
sion
sw
hich
com
bine
din
tera
ctiv
eed
ucat
ion
and
med
icat
ion
man
agem
ent.
133
0.8
(0.5
,1.4
)–0
.33%
(–
0.13
,0.8
0)
–
Pat
ien
t C
on
tro
l:U
sual
car
e10
6–
Farm
er e
t al
, 200
9P
atie
nt
inte
rven
tion
: Pat
ient
edu
catio
non
goa
lset
ting,
bel
iefs
abo
ut
diab
etes
as
wel
las
role
ofd
iet,
phys
ical
act
ivity
and
med
icat
ion
adhe
r-en
cein
dia
bete
sca
rep
lus
rand
omiz
edto
1o
f2g
roup
s:
Less
inte
nsiv
em
onito
ring:
Tra
ined
inu
seo
fag
luco
sem
eter
and
dia
ries
for
reco
rdin
ggo
als
and
activ
ities
plu
sed
ucat
ion
on
goal
set
ting,
bel
iefs
ab
outd
iabe
tes
asw
ella
sro
leo
fdie
t,ph
ysic
ala
ctiv
itya
ndm
edic
atio
nad
here
nce
ind
iabe
tes
care
150
Mea
nim
prov
emen
tin
ad
here
nce
(SD
):0.
1(0
.2)
Mea
n(S
D):
–0
.14
(0.8
2)–
Mor
ein
tens
ive
self-
mon
itorin
g:T
rain
edin
use
ofm
eter
plu
sin
stru
ctio
nin
se
lf-in
terp
reta
tion
ofg
luco
sele
vels
.
Inb
oth
grou
ps,p
atie
nts'
phy
sici
anw
asg
iven
blo
odg
luco
ser
esul
tsfo
rm
edic
atio
nm
anag
emen
t.
151
Mea
nim
prov
emen
tin
ad
here
nce
(SD
):0.
1(0
.1)
0.17
(0.
73)
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
plus
edu
catio
n15
2M
ean
impr
ovem
enti
n
adhe
renc
e(S
D):
–0.1
(0.
4)–0
.00
(1.0
2)–
Farm
er e
t al
, 201
2P
atie
nt
inte
rven
tion
: 1–3
0m
inut
em
otiv
atio
nalc
ouns
elin
gse
ssio
nto
ad
dres
spa
tient
bel
iefs
abo
utm
edic
atio
ns
126
EM
D:8
.4(
0.2,
16.7
) *
Sel
f-re
port
:–0.
4(–
1.0,
0.2
)0.
06%
(–
0.19
,0.3
2)
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
85–
Gu
ldb
erg
et
al, 2
010
Pra
ctiti
on
er in
terv
entio
n:
CD
RO
M-b
ased
ele
ctro
nic
feed
back
sy
stem
that
pre
sent
edd
ata
onp
ract
ition
er’s
pat
ient
pan
elw
ith
diab
etes
with
an
optio
nto
use
dat
adu
ring
indi
vidu
alc
onsu
ltatio
ns
ora
san
ove
rvie
wo
fthe
qua
lity
ofth
eir
diab
etes
car
eco
mpa
red
toth
eir
colle
ague
s’p
ract
ices
Pat
ient
s:1
317
Pra
ctiti
oner
:89
Initi
atio
nof
ora
lmed
icat
ion
(no
insu
lin):
20.9
(7.
9,34
.8)*
Sus
tain
men
tofo
ral
med
icat
ion:
–2.
3(–
5.3,
0.3
)
Initi
atio
nof
insu
linw
hen
HbA
1c
>8%
:21.
4(9
.9,3
2.8)
†
Sus
tain
men
tofi
nsul
in:
–0.3
(–3
.2,2
.5)
–0.0
5%
(–4.
2,1
4.2)
–
Pra
ctiti
on
er c
on
tro
l:U
sual
car
eP
atie
nts:
114
1P
ract
ition
er:7
1–
www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 499
CliniCal ReviewTa
ble
2.E
ffect
sof
Int
erve
ntio
nS
trat
egie
sTa
rget
eda
tth
eP
atie
nt-P
ract
ition
erI
nter
actio
non
Adh
eren
cet
oD
iabe
tes
Med
icat
ions
(con
tinue
d)
Stu
dy
Inte
rven
tion
/Co
ntr
ol
S
amp
le S
ize
M
ean
Ch
ang
e in
Med
icat
ion
A
dh
eren
ce (
95%
CI)
M
ean
Ch
ang
e in
Hb
A1c
(9
5% C
I)
Bet
wee
n
Gro
up
With
in
Gro
up
Hei
sler
et
al, 2
010
Pat
ien
t in
terv
entio
n:
Pee
rsu
ppor
tses
sion
faci
litat
edb
ya
nurs
eca
se
man
ager
(N
CM
)an
dre
sear
cha
ssis
tant
(R
A)
plus
rec
ipro
calp
eer
sup-
port
faci
litat
edb
yw
eekl
yca
llsth
roug
han
inte
ract
ive
voic
ere
spon
se
plat
form
.A
lso
offe
red
3op
tiona
l1.5
hou
rpa
tient
-driv
ens
essi
ons
toa
sk
ques
tions
,sha
rec
once
rns,
dis
cuss
stra
tegi
es,a
ndu
pdat
epr
ogre
sso
nac
tion
plan
s.
126
Mis
sed
≥1
insu
lin
dose
/wk
(SD
):–3
(–5
)
Mis
sed
≥1
oral
med
do
se/w
k(S
D):
–6(
–2)
–0.5
8%*
–0.2
9%
Pat
ien
t C
on
tro
l: 1–
1.5
hour
ses
sion
led
byN
CM
tor
evie
wr
ecen
tlab
va
lues
,ask
que
stio
ns,a
ndr
ecei
vein
form
atio
non
VA
car
em
anag
emen
tse
rvic
esa
nde
duca
tiona
lsel
f-m
anag
emen
tmat
eria
ls.
119
Mis
sed
≥ 1
insu
lin
dose
/wk
(SD
):–1
0(–
10)
Mis
sed
≥1o
ralm
ed
dose
/wk
(SD
):–7
(–3
)
–0.
29%
Kim
et
al, 2
003
Pat
ien
t in
terv
entio
n: T
elep
hone
-bas
edp
atie
nte
duca
tion
with
the
use
ofa
dia
bete
sca
reb
ookl
eta
ndfo
odd
iarie
s.
Boo
klet
spr
ovid
edin
form
a-tio
nab
outr
isk
fact
ors,
die
t,ex
erci
se,d
rug
ther
apy,
hyp
ogly
caem
ia,a
nd
hype
rgly
cem
ia
20M
ean
adhe
renc
e(S
D):
94
.4(
14.4
)–1
.2%
†–1
.2%
*
Pat
ien
t co
ntr
ol:
Usu
alc
are
16M
ean
adhe
renc
e(S
D):
98.8
(3.
8)0.
6%*
Kim
et
al, 2
006
Pat
ien
t in
terv
entio
n:W
eekl
yte
xtm
essa
ges
that
rei
nfor
ced
diet
,ex
erci
se,m
eda
djus
tmen
t,an
dse
lf-m
onito
ring
ofb
lood
glu
cose
.45
Mea
nin
crea
sein
med
icat
ion-
taki
ngp
erw
eek
(SD
):
1.1
days
per
wee
k(1
.9) *
––1
.1(
2.1)
*
Pat
ien
t co
ntr
ol:
Not
app
licab
le–
–
Ko
et
al, 2
004
Pat
ien
t in
terv
entio
n: 5
pat
ient
edu
catio
nse
ssio
nsc
ardi
ovas
cula
rdi
s-ea
ses
(CV
D),
CV
Dr
isk
fact
ors,
and
sel
f-ca
reb
ehav
iors
plu
sm
edic
atio
nad
just
men
t,ad
here
nce
asse
ssm
ent,
posi
tive
feed
back
and
dis
trib
utio
nof
ed
ucat
iona
lmat
eria
ls(
pam
phle
ts,b
ooks
)
90M
ean
adhe
renc
e:9
9.5%
–6.0
%
Pat
ien
t co
ntr
ol:
Usu
alc
are
88M
ean
adhe
renc
e:9
9%–2
.1%
Lin
et
al, 2
006
Pat
ien
t in
terv
entio
n:
Indi
vidu
aliz
edd
epre
ssio
nca
rem
anag
emen
tusi
ng
ast
eppe
d-ca
rea
ppro
ach
acco
rdin
gto
pat
ient
pre
fere
nce
and
trea
tmen
tre
spon
se.P
atie
nts
wer
eof
fere
dan
initi
alc
hoic
eof
2e
vide
nce-
base
dtr
eatm
ents
:ant
idep
ress
antm
edic
atio
nor
pro
blem
-sol
ving
trea
tmen
t.
Initi
al1
-hou
rse
ssio
nfo
llow
edb
ytw
ice-
mon
thly
ses
sion
sin
the
acut
eph
ase
oftr
eatm
ent(
0–12
wee
ks)
and
mon
thly
ses
sion
sfo
rth
ere
mai
nder
9
mon
ths
164
–6.3
(–1
1.91
,–0.
71) *
––
Pat
ien
t co
ntr
ol:
Usu
alc
are
165
–
Mu
llan
et
al, 2
009
Pat
ien
t in
terv
entio
n:
Use
ofm
edic
atio
nde
cisi
ona
ids
com
bine
dw
ith
phys
icia
nan
dnu
rse
follo
w-u
p.P
atie
nts:
48
Pra
ctiti
oner
s:2
1P
harm
acy
reco
rd:
%
Adh
eren
t:–8
.88
(–
13.6
,–4.
14)
0.01
%(
–0.4
9,0
.50)
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
Pat
ient
s:3
7P
ract
ition
ers:
19
Per
sist
ence
(da
ysc
over
ed):
−11.
8(−
21.0
,−2.
67)
Sel
f-re
port
:0.7
4(0
.24,
2.3
2)
–

500 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes MedicationsTa
ble
2.E
ffect
sof
Int
erve
ntio
nS
trat
egie
sTa
rget
eda
tth
eP
atie
nt-P
ract
ition
erI
nter
actio
non
Adh
eren
cet
oD
iabe
tes
Med
icat
ions
(con
tinue
d)
Stu
dy
Inte
rven
tion
/Co
ntr
ol
S
amp
le S
ize
M
ean
Ch
ang
e in
Med
icat
ion
A
dh
eren
ce (
95%
CI)
M
ean
Ch
ang
e in
Hb
A1c
(9
5% C
I)
Bet
wee
n
Gro
up
With
in
Gro
up
Neg
aran
deh
et
al, 2
013
Pat
ien
t In
terv
entio
n:
Pat
ient
sw
ere
rand
omiz
edto
1o
f2g
roup
s:
Gro
up1
-P
rovi
ded
patie
nte
duca
tion
ond
iabe
tes
usin
gte
ach
back
to
con
firm
pat
ient
s’c
ompr
ehen
sion
Gro
up2
-P
rovi
ded
patie
nte
duca
tion
ond
iabe
tes
usin
gpi
ctor
ial
imag
es
43
44
Gro
up1
vs.
UC
:–2.
71
(–3.
43,–
1.99
)†
Gro
up2
vs.
UC
:–2.
40
(–3.
12,–
1.69
)†
– –
– –
Pat
ien
t co
ntr
ol:
Usu
alc
are
40G
roup
1v
s.G
roup
2:
–0.3
0(–
1.01
,0.4
0)–
–
Pie
tte
et a
l, 20
00P
atie
nt
inte
rven
tion
:B
iwee
kly
calls
with
an
auto
mat
edte
leph
one
di
seas
em
anag
emen
t(AT
DM
)sy
stem
des
igne
dto
ass
ess
patie
nt's
he
alth
sta
tus,
pro
vide
hea
lthti
psa
nd/o
rpa
rtic
ipat
ein
opt
iona
lsel
f-
care
mod
ules
plu
ste
leph
one
NC
Mfo
llow
-up
124
–21
(–34
,–7)
*
All
patie
nts:
–0.3
%(
–0.7
,0.1
)
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
124
Atta
inH
bA1c
<
6.4%
:9(
7,3
0)*
–
Pie
tte
et a
l, 20
01P
atie
nt
inte
rven
tion
:B
iwee
kly
calls
with
AT
DM
plu
ste
leph
one
N
CM
follo
w-u
p14
6%
with
med
icat
ion
pr
oble
ms:
45%
For
allp
atie
nts:
–0
.1%
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
146
%w
ithm
edic
atio
npr
oble
ms:
39%
HbA
1cb
asel
ine
≥
8%o
nly:
–0.
5%*
HbA
1cb
asel
ine
≥
9%o
nly:
–1.
1%*
–
Ru
bak
et
al, 2
011
Pat
ien
t in
terv
entio
n:T
rain
ing
inm
otiv
atio
nali
nter
view
ing
tofa
cilit
ate
disc
ussi
ons
abou
tdia
bete
str
eatm
entd
ecis
ions
41%
red
eem
edp
resc
riptio
n:9
6%N
ots
igni
fican
t;da
tan
ot
repo
rted
–0.7
%*
Pat
ien
t co
ntr
ol:
Usu
alc
are
37%
red
eem
edp
resc
riptio
n:10
0%–0
.7%
*Ta
n e
t al
, 201
1P
atie
nt
inte
rven
tion
:3
stru
ctur
edp
atie
nte
duca
tion
sess
ions
on
di
abet
ess
elf-
care
beh
avio
rsp
lus
mot
ivat
iona
lsup
port
,pro
blem
so
lvin
gan
dac
tion
plan
ning
82>
90%
adh
eren
tadj
ustin
gfo
rhy
pogl
ycem
ia:9
1.42
(8
9.12
,3.7
2)*
–0.9
2%†
–
Pat
ien
t co
ntr
ol:
Usu
alc
are
82>
90%
adh
eren
tadj
ustin
gfo
rhy
pogl
ycem
ia:8
4.48
(8
1.76
,87.
20)
–
Wo
ng
et
al, 2
005
Pat
ien
t in
terv
entio
n:
Ear
lyh
ospi
tald
isch
arge
pro
gram
with
pat
ient
ed
ucat
ion
ons
elf-
care
beh
avio
rsp
lus
tight
glu
cose
mon
itorin
gby
an
urse
52
Mea
nad
here
nce
(SD
):5.
9(0
.4)
–0.5
%–3
.6%
*
Pat
ien
t co
ntr
ol:
Rem
aine
din
hos
pita
lunt
ilgl
ycem
icle
velw
ass
tabi
lized
49M
ean
adhe
renc
e(S
D):
5.7
(1.1
)–2
.5%
*
CI=
con
fiden
cein
terv
al.
*p<
0.0
5.
† p<
0.0
01.

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 501
based treatment recommendations. At baseline, the medi-cation adherence rates for oral medications (measured as proportion of patients with ≥ 80% adherence) were the same for both conditions over the past 2 weeks. At the 12-week follow-up, the proportion of patients with adher-ence rates ≥ 80% was significantly higher for the interven-tion group than for the control group (65.2% vs. 30.7%, P < 0.001). The intervention group was also significantly more likely to achieve glucose control (HbA1c < 7%) and experience fewer depressive symptoms at 12 weeks [32].
The remaining positive patient-focused trials targeted several diabetes self-care behaviors in addition to medication adherence and employed intervention strategies that in-cluded tailored patient education, development of problem solving skills, action planning, and behavioral feedback and reinforcement delivered either by trained nurses, text mes-sage, or a telephone-linked system [38,45,47]. The teach-back method and using pictorial images to explain concepts were also identified as effective strategies for delivering in-formation to patients with low health literacy [43]. Neither of the positive trials that assessed patients’ satisfaction with the practitioners’ communication skills reported significant differences between the intervention and control group at the final follow-up [34,48]. In contrast with the positive interventions, the nonsignificant trials were more likely to use patient education as the primary strategy [33,39,40,48] and target multiple diabetes self-care behaviors (eg, weight management, SMBG) with none focusing solely on medi-cation adherence. However, in 1 trial, patients’ perceived satisfaction with the interpersonal aspects of care was higher among the intervention group than the control group [44].
Intervention delivery and dose. The method of inter-vention delivery varied across trials. Research nurses or college-level students delivered the intervention in 4 of the positive trials [32,38,45,47] while existing clinic staff were utilized in 3 trials [31,34,43]. Two trials utilized technology as a means to provide tailored interventions that maximized nurses’ time by focusing on patients with the greatest care needs [38,45]. For example, in the trial by Piette et al [45], an automated telephone disease man-agement (ATDM) system designed to assess health risks, provide health tips, and allow patients to engage in inter-active self-care modules was used to augment nurse case management (NCM). At the 12 month follow-up, medi-cation non-adherence decreased by 21% among patients randomized to the ATDM+NCM group as compared with the UC group [45].
Interventions delivered by clinic staff tended to include fewer intervention contacts (mean, 2 sessions) for shorter duration (average length of intervention, 45 minutes over 2.5 months). In contrast, interventions delivered by trained research staff ranged from 3 to 12 sessions (mean, 6.67) and were of longer duration (average length of intervention, 111 minutes over the course of 5.25 months). Technology-assisted interventions also had higher interven-tion contacts with up to 72 contacts in a trial utilizing text messaging [38]. Exposure to the intervention was assessed in 3 of the positive trials [34,43,45]; an average of 90% of patients received the intervention as intended.
Patient-level trials reporting nonsignificant findings were more likely to utilize existing clinic staff (n = 5) [33,37,40,41,48] than research staff (n = 3) [35,39,44]. Two of the trials utilized group-based intervention strate-gies [33,37], of which 1 used trained peer supporters [37]. One trial used an ATDM system [45]. In contrast to the positive trials, clinic staff–led interventions in the nonsig-nificant trials had a higher number of intervention contacts (mean,9 sessions) and were of longer duration (mean, 10 months). Interventions led by research staff ranged from 4 to 16 sessions (mean, 10 sessions) for an average of 9 months. Intervention contact time was not consistently reported in these trials. Primary care physicians were in-volved in 6 of the trials for medication management and to address acute health concerns [33,35,39,41,44,48]. Six trials reported intervention attendance rates with an average of 78% of patients receiving at least some of the intervention as intended [33,35,37,39,41,44].
Assessment of medication adherence. Three of the posi-tive trials (43%) utilized an objective measure [31,32,34] to assess medication adherence while 4 trials utilized validated patient self-report questionnaires [38,43,45,47]. All of the trials assessed patients’ baseline adherence level, of which 3 (43%) included patients with high adherence (≥ 80% adherence at baseline visit) [31,34,47]. In 1 trial adherence was assessed via an EMD and self-report ques-tionnaire [34]. At the final follow-up, a higher proportion of patients reported being adherent to their oral medica-tions than what was “objectively” reported by the EMD. Finally, 2 of the trials assessed medication adherence to oral medications only [32,34], 3 trials assessed both oral medications and insulin usage [38,45,47], and 2 did not specify [31,43]. Two of the trials assessing both types of medicines accounted for occurrences of hypogylcemia in the calculation of medication adherence [45,47]. However,
CliniCal Review

502 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
neither study reported differential effects of the interven-tion on adherence to oral medications as compared to insulin.
In contrast to the positive trials, 75% (n = 6) of the nonsignificant trials utilized self-report measures [33,35,37,39,44,48]. Baseline adherence was assessed in 7 of the trials, of which 4 (57%) included patients with high adherence [28,35,41,48]. Three of the trials assessed medication adherence to oral medications only [35,39,40], 4 trials assessed both oral medication and insulin usage [37,41,44,48], and 1 did not specify [33]. Only the trial by Heisler et al [37] reported the differential effects of the intervention by medication type. While nonsignificant, pa-tients randomized to the NCM attention control group ex-hibited greater improvements in adherence to insulin at the 6 month follow-up compared with the reciprocal peer sup-port intervention group (–10% vs. –3% reduction in missed doses over the past week). The remaining 3 trials that col-lected data on both medication types did not account for insulin usage in the calculation of medication adherence.
Impact on HbA1c. Six of the positive trials examined the impact of the intervention on HbA1c (mean baseline level, 8.47%) [31,32,34,38,45,47]. Four (67%) of the tri-als demonstrating a positive effect on medication adher-ence also reported significant improvements in HbA1c (average reduction, –0.88%) [32,38,45,47]. All of the nonsignificant trials also assessed the impact of the inter-vention on HbA1c (mean baseline level, 8.58%). Half of the trials reported significant between-group differences in HbA1c despite having no effect on medication adher-ence (average reduction, –0.83%) [37,39,44,48].
Practitioner-Focused TrialsIntervention content. Health care practitioners were the primary focus in 3 of the trials [36,42,46]. One of the trials demonstrated a significant benefit from the inter-vention. In this RCT, Guldberg et al [36] randomized 86 general practices to receive either a CD ROM–based electronic feedback system or usual care. The electronic feedback system presented practitioners with data on their DM patient population which could be used for individual consultations or quality assurance. Medication adherence was assessed as the initiation and sustainment of treatment as documented in pharmacy records. At the 15-month follow-up, patients followed in interven-tion practices were significantly more likely to redeem prescriptions for their initial oral medication (mean
change, 20.9%; 95% confidence interval [95CI], 7.9–34.8 [P = 0.002]) and insulin treatment (mean change, 21.4%; 95CI, 9.9–32.8 [P < 0.001]) than patients in the control practices [36]. In the 2 nonsignificant trials, practitioners were trained to counsel patients on making shared treat-ment decisions for their DM by using either motivational interviewing techniques [46] or a decision aid tool [42].
Intervention delivery and dose. Participating practitio-ners delivered the intervention in all the trials, however, training in the intervention content, frequency of con-tacts, and adherence to the study protocol varied greatly. In the positive trial, the CD ROM–based feedback system was distributed at 3 time points over the course of the 15-month study [36]. Qualitative data from par-ticipating practitioners showed that the system was most often used to assess overall quality of their diabetes care rather than for individual consultations [49]. In the motivational interviewing trial, practitioners attended a 1.5-day training session with 2 half-day follow-up ses-sions over the course of 1 year [46]. More than 90% of participating practitioners attended all of the trainings. This is in contrast to the trial employing a decision aid whereby practitioners received one training session for less than 3 minutes before meeting with the first enrolled patient [42]. In regards to intervention dose, practitio-ners in the motivational interviewing trial were expected to deliver 3 sessions of 45 minutes each per patient [46]. No data was provided on the percentage of sessions de-livered or adherence to the counseling protocol. In the decision aid trial, practitioners were randomized to either use the tool with all of their eligible patients (interven-tion group) or discuss treatment as usual. Fidelity to the study protocol was assessed by coding videotaped clinical encounters with the OPTION decision-making instru-ment [42]. While this study did not report a beneficial effect of the decision aid tool on medication adherence, intervention patients were rated as having significantly higher levels of involvement in the clinical encounter than the control group [42].
Assessment of medication adherence. All 3 trials utilized pharmacy records to assess medication adherence. One trial also used patient self-report to assess adherence to all diabetes medications [42]. Comparisons of the mea-sures showed that patients in both study groups tended to overreport nonadherence by self-report as compared with pharmacy record data (24% and 19% nonadherent

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 503
by self-report in the intervention and usual care groups vs. 2.5% and 0% by pharmacy record). Baseline adherence levels were only assessed in the motivational interviewing trial; 96% of intervention patients and 100% of control patients were considered adherent by pharmacy records [46]. Two trials collected data on both oral medications and insulin [36,42] and 1 trial assessed adherence solely to oral medications [46]. Only the positive trial assessed the differential impact of the intervention on adherence by medication type [36]. The intervention was equally beneficial for the initiation of oral and insulin prescrip-tions in intervention practices.
Impact on HbA1c. Most patients had baseline HbA1c lev-els lower than 8% in the practitioner-focused trials (mean, 7.27%), of which none demonstrated significant between-group differences in HbA1c. A significant within-group reduction in HbA1c was demonstrated in both the in-tervention and control groups among patients participat-ing in the motivational interviewing trial (mean change, –0.7%, P < 0.01) [46].
DISCUSSION
A systematic review of the literature yielded 18 studies that tested the effects of intervention strategies delivered by health care practitioners on adherence to diabetes medica-tions. Patient-focused trials comprised 83% of the reviewed interventions, and 17% were practitioner-focused. Eight of the 18 reviewed trials (44%) reported a statistically significant improvement in medication adherence attributed to the in-tervention [31,32,34,36,38,43,45,47]. The effective patient-focused interventions (n = 7) were complex, including a combination of patient education, individualized counseling targeting the psychosocial (eg, depression, self-efficacy) and logistical (eg, medication cost, referrals) barriers to adherence, medication reminders, action planning, and reinforcement of positive behavior. The effective practitioner-focused interven-tion utilized an electronic feedback system to increase the quality of care provided to patients with diabetes [36].
When comparing the intervention content across trials, we found that effective interventions were more likely to directly target medication nonadherence and be delivered in one-on-one sessions by trained ancillary staff through the use of care managers and/or technology than those reporting nonsignificant findings. Despite improvements in adherence, patients in the control group were equally likely to report high satisfaction with practitioners’ com-munication skills as the intervention group [34,48]. How-
ever, lack of baseline assessment of perceived satisfaction with practitioners’ communication skills make it difficult to determine if nonsignificant findings reflect ceiling ef-fects or other extraneous confounding variables. When comparing the intervention dose, we found that clinic staff in the nonsignificant trials led 4½ times as many in-tervention sessions (average, 9 sessions vs. 2 sessions) over a longer duration of time (10 months vs. 2.5 months) than in the positive trials. This finding may be explained by the intervention content in the nonsignificant trials, with most primarily focusing on delivering patient education, which is a necessary but insufficient condition for lasting behavior change [50]. For example, previous studies have shown that neither patient’s knowledge of their HbA1c level or high diabetes-related knowledge scores were associated with better medication adherence or reduc-tions in Hb1Ac levels [51,52]. Rather, as demonstrated by the positive trials, patients are more likely to initiate and maintain self-management behaviors when they work collaboratively with health care practitioners to become an active, informed partner in their care [53]. Specifically, patient-centered intervention strategies that provide tai-lored education and assist patients in developing problem solving and decision making skills through behavioral feedback and reinforcement equip patients with the knowl-edge, skills, and confidence to manage their health [54].
Few studies targeted practitioners making it difficult to draw conclusions about effective approaches to improve diabetes medication adherence. Findings from the positive trial suggests that provision of feedback on performance measures related to guideline-concordant care may be more effective (in the short term) for improving medica-tion adherence than intervention approaches that try to modify practitioners’ communication skills. Finally, objec-tive measures of medication adherence were more likely to be utilized in positive trials. However, trials employing objective measures were no more likely to report improve-ments in HbA1c than those utilizing patient self-report in both the positive and nonsignificant trials.
Four limitations in the methodology of the reviewed trials warrant consideration when examining the effects of interventions on medication adherence. First, the adherence measure varied with only 2 trials [32,34] report-ing adherence with the objective electronic assessments. When both an objective and subjective measure of adher-ence was used, results between the 2 types of measures conflicted (eg, the objective measure rated the patient as less adherent but patients reported perfect adherence).
CliniCal Review

504 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
This highlights one of the greatest challenges to the adher-ence field—no single measure can be considered the “gold standard” for all types of research or clinic settings.
Second, there was great variability in how medication adherence was defined across trials. Definitions of adher-ence were partly dependent on the measure used and ranged from the percent of prescribed doses taken cor-rectly for objective measures to a summary score derived from self-report measures that use different recall periods. Frequency of the dosing regimen (once-daily vs. twice-daily dosing) and medication type (oral medication vs. injection) also affect the interpretation of one’s findings. For example, Tan et al [47] showed that failure to account for occur-rences of hypoglycemia during the course of the study can underestimate the proportion of adherent patients.
Third, a limitation of the trials is the inclusion of pa-tients irrespective of their baseline adherence status. That is, adherent and nonadherent patients form a single group and as a result are exposed to the same intervention ap-proach. As a result, initially adherent patients maintain their high adherence levels and nonadherent patients do not get the dose or specificity of intervention strategies they may need to improve their behaviors. Trials that in-cluded initially adherent patients in this review were also less likely to detect changes in Hba1c, suggesting that other self-care behaviors are important intervention targets for these patients [31,34,35,41,48]. Lack of a baseline assessment of medication adherence in the negative prac-titioner-focused trials also makes it difficult to distinguish whether nonsignificant findings reflected an inability to alter practitioners’ skills, ceiling effects, or extraneous con-founding variables.
Finally, most (75%) of the positive trials were 3 or fewer months in duration as compared with the non-significant trials, where 60% of trials lasted at least 12 months. Thus, the question remains whether positive findings were due to a Hawthorne effect in some of the trials. Replication of the findings in trials with longer follow-up periods and more robust assessments of medi-cation adherence are needed to answer this question.
There are limitations of this review. We only included trials with published data in English-language journals and may have missed some trials that met the predefined criteria. We also limited our review to interventions to improve adherence to diabetes medications that are delivered by health care professionals thus, we may have excluded relevant work using different intervention strat-egies. However, we did include trials reporting nonsig-
nificant findings thereby minimizing the negative pub-lishing bias. Finally, heterogeneity of the interventions and measures used in the studies precluded quantitative meta-analysis of the findings.
ImplicationsDiabetes is a complex chronic condition that requires patients to develop the knowledge, skills, and confidence to execute daily self-management behaviors. A collab-orative patient-practitioner interaction is at the forefront of effective patient self-management and can lay the foun-dation for patient’s acceptance and implementation of a medication regimen [15]. However, increasing demands on practitioners to address patients’ complex medical needs within time-constrained visits greatly diminishes opportu-nities to engage in discussions about medication adherence. Furthermore, the current health care system is structured to support visit-based, acute care, making it difficult for practitioners to change their communication style or imple-ment multi-component intervention strategies, even when provided with ample training opportunities.
Findings from this review suggest that medication adherence among patients with DM can be improved when practitioners are supported by trained ancillary staff who have the dedicated time to provide individualized patient-centered adherence counseling. Technology also provides an efficient and cost-effective means to enhance medication adherence by offering patients continuous monitoring, feedback, and reinforcement [55]. Practi-tioners similarly benefit from technology-based systems that utilize continuous quality improvement principles to provide feedback on performance measures [56].
Application of these findings to real world clinic settings will require the adoption of new models of care such as the patient-centered medical home and panel management that facilitate the provision of high quality, patient-centered care for patients with chronic disease [57]. Core elements of these models include team-based approaches that support physician decision-making by utilizing nonphysician sup-port staff (eg, health coaches), health information technolo-gy, and structured work processes to deliver proactive, coor-dinated care [58]. The Geisinger Health System and Group Health Cooperative serve as examples of innovative delivery systems that are implementing multidimensional adherence strategies that are producing clinical and cost-saving benefits [59]. The lessons learned from these organizations will be invaluable as health care reform moves from law to reality for patients and health care practitioners alike.

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM 505
Corresponding author: Dr. Antoinette Schoenthaler, Center for Healthful Behavior Change, Dept. of Population Health, NYU School of Medicine, 227 E. 30th St., 634, New York, NY 10016, [email protected].
Funding/support: This work was supported by K23 HL 098564-01 from the National Heart, Lung, and Blood Institute.
Financial disclosures: None.
REfERENCES1. Center for Disease Control and Prevention. National Diabetes
Fact Sheet: National estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA; 2011.
2. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med 2006;166:1836–41.
3. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care 2004;27:1218–24.
4. Odegard PS, Capoccia K. Medication taking and diabe-tes: A systematic review of the literature. Diabetes Educ 2007;33:1014–29.
5. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353:487–97.
6. Peterson AM, Takiya L, Finley R. Meta-analysis of trials of interventions to improve medication adherence. Am J Health Syst Pharm 2003;60:657–65.
7. DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes: A meta-analysis. Med Care 2002;40:794–811.
8. World Health Organization: Adherence to long-term therapies: evidence for action. Geneva: World Health Organization; 2003.
9 . Haynes R, Taylor D, Sackert D, editors. Compliance in health care. Baltimore: Johns Hopkins University Press; 1979.
10. Miller NH, Hill M, Kottke T, Ockene IS. The multilevel compliance challenge: recommendations for a call to ac-tion. A statement for healthcare professionals. Circulation 1997;95:1085–90.
11. Heisler M, Bouknight RR, Hayward RA, et al. The rela-tive importance of physician communication, participatory decision making, and patient understanding in diabetes self-management. J Gen Intern Med 2002;17:243–52.
12. Parchman ML, Zeber JE, Palmer RF. Participatory decision making, patient activation, medication adherence, and in-termediate clinical outcomes in type 2 diabetes: A STARNet study. Ann Family Med 2010;8:410–7.
13. Fuertes JN, Mislowack A, Bennett J, et al. The physician-patient working alliance. Patient Educ Couns 2007;66:29–36.
14. van Dam HA, van der Horst F, van den Borne B, et al. Provider-patient interaction in diabetes care: Effects on patient self-care and outcomes. A systematic review. Patient Educ Couns 2003;51:17–28.
15. Ratanawongsa N, Karter AJ, Parker MM, et al. Communica-tion and medication refill adherence: The Diabetes Study of Northern California. JAMA 2013;173:210–8.
16. Piette JD, Schillinger D, Potter MB, Heisler M. Dimen-
sions of patient-provider communication and diabetes self-care in an ethnically diverse population. J Gen Intern Med 2003;18:624–33.
17. Schneider J, Kaplan SH, Greenfield S, et al. Better physician-patient relationships are associated with higher reported adherence to antiretroviral therapy in patients with HIV infec-tion. J Gen Intern Med 2004;19:1096–103.
18. McDonald HP, Garg AX, Haynes RB. Interventions to en-hance patient adherence to medication prescriptions: Scientific review. JAMA 2002;288:2868–79.
19. Higgins J, Green S, editors. Cochrane Handbook for system-atic reviews of interventions. 5.1.0 ed [updated March 2011]. The Cochrane Collaboration; 2011.
20. Chisholm-Burns MA, Graff Zivin JS, Lee JK, et al. Eco-nomic effects of pharmacists on health outcomes in the United States: A systematic review. Am J Health Syst Pharm 2010;67:1624–34.
21. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US phar-macists’ effect as team members on patient care: systematic review and meta-analyses. Med Care 2010;48:923–33.
22. Hatah E, Braund R, Tordoff J, Duffull SB. A systematic review and meta-analysis of pharmacist-led fee-for-services medication review. Br J Clin Pharmacol;2013.
23. Hatah E, Tordoff J, Duffull SB, Braund R. Pharmacists’ per-formance of clinical interventions during adherence support medication reviews. Res Soc Admin Pharm 2013.
24. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part I: System-atic review and meta-analysis in diabetes management. Ann Pharmacother 2007;41:1569–82.
25. McKee MD, Fletcher J, Sigal I, et al. A collaborative approach to control hypertension in diabetes: Outcomes of a pilot in-tervention. J Primary Care Comm Health 2011;2:148–52.
26. Pearce KA, Love MM, Shelton BJ, et al. Cardiovascular risk education and social support (CaRESS): report of a random-ized controlled trial from the Kentucky Ambulatory Network (KAN). J Am Board Family Med 2008;21:269–81.
27. Zolfaghari M, Mousavifar SA, Pedram S, Haghani H. The impact of nurse short message services and telephone follow-ups on diabetic adherence: which one is more effective? J Clin Nursing 2012;21:1922–31.
28. Hendricks LE, Hendricks RT. The effect of diabetes self-management education with frequent follow-up on the health outcomes of African American men. Diabetes Educ 2000;26:995–1002.
29. Wolever RQ, Dreusicke M, Fikkan J, et al. Integrative health coaching for patients with type 2 diabetes: a randomized clini-cal trial. Diabetes Educ 2010;36:629–39.
30. Crowley MJ, Powers BJ, Olsen MK et al. The Cholesterol, Hypertension, And Glucose Education (CHANGE) study: Results from a randomized controlled trial in African Ameri-cans with diabetes. Am Heart J 2013;166:179–86.
31. Ahmadipour H, Farajzadegan Z, Kachoei A, Pirdehghan A. Secondary prevention by enhancing adherence in diabetic patients. Int J Prevent Med 2010;1:50–5.
32. Bogner HR, Morales KH, de Vries HF, Cappola AR. Inte-grated management of type 2 diabetes mellitus and depression
CliniCal Review

506 JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
treatment to improve medication adherence: A randomized controlled trial. Ann Family Med 2012;10:15–22.
33. Edelman D, Fredrickson SK, Melnyk SD, et al Medical clinics versus usual care for patients with both diabetes and hyperten-sion: a randomized trial. Ann Intern Med 2010;152:689–96.
34. Farmer A, Hardeman W, Hughes D, et al. An explanatory randomised controlled trial of a nurse-led, consultation-based intervention to support patients with adherence to taking glucose lowering medication for type 2 diabetes. BMC Fam Pract 2012;13:30.
35. Farmer AJ, Wade AN, French DP, et al. Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial. Health Technol Assess 2009;13:1–50.
36. Guldberg TL, Vedsted P, Kristensen JK, Lauritzen T. Im-proved quality of type 2 diabetes care following electronic feedback of treatment status to general practitioners: A cluster randomized controlled trial. Diabetic Med 2011;28:325–32.
37. Heisler M, Vijan S, Makki F, Piette JD. Diabetes control with reciprocal peer support versus nurse care management: A ran-domized trial. Ann Intern Med 2010;153:507–15.
38. Kim HS, Kim NC, Ahn SH. Impact of a nurse short message service intervention for patients with diabetes. J Nurs Care Qual 2006;21:266–71.
39. Kim HS, Oh JA. Adherence to diabetes control recommendations: impact of nurse telephone calls. J Adv Nurs 2003;44:256–61.
40. Ko GT, Li JK, Kan EC, Lo MK. Effects of a structured health education programme by a diabetic education nurse on cardiovascular risk factors in Chinese Type 2 diabetic pa-tients: A 1-year prospective randomized study. Diabetic Med 2004;21:1274–9.
41. Lin EH, Katon W, Rutter C, et al Effects of enhanced de-pression treatment on diabetes self-care. Ann Family Med 2006;4:46–53.
42. Mullan RJ, Montori VM, Shah ND, et al. The diabetes mel-litus medication choice decision aid: a randomized trial. Arch Intern Med 2009;169:1560–8.
43. Negarandeh R, Mahmoodi H, Noktehdan H, et al. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Prim Care Diabe-tes 2013;7:111–8.
44. Piette JD, Weinberger M, Kraemer FB, McPhee SJ. Impact of automated calls with nurse follow-up on diabetes treat-ment outcomes in a Department of Veterans Affairs Health Care System: A randomized controlled trial. Diabetes Care 2001;24:202–8.
45. Piette JD, Weinberger M, McPhee SJ, et al. Do automated calls with nurse follow-up improve self-care and glycemic control among vulnerable patients with diabetes? Am J Med
2000;108:20–7.46. Rubak S, Sandbaek A, Lauritzen T, et al. Effect of “moti-
vational interviewing” on quality of care measures in screen detected type 2 diabetes patients: A one-year follow-up of an RCT, ADDITION Denmark. Scand J Primary Health Care 2011;29:92–8.
47. Tan MY, Magarey JM, Chee SS, et al. A brief structured edu-cation programme enhances self-care practices and improves glycaemic control in Malaysians with poorly controlled diabe-tes. Health Educ Res 2011;26:896–907.
48. Wong FK, Mok MP, Chan T, Tsang MW. Nurse follow-up of patients with diabetes: Randomized controlled trial. J Adv Nurs 2005;50:391–402.
49. Guldberg TL, Vedsted P, Lauritzen T, Zoffmann V. Sub-optimal quality of type 2 diabetes care discovered through electronic feedback led to increased nurse-GP cooperation. A qualitative study. Prim Care Diabetes 2010;4:33–9.
50. Beukelman D. Information alone does not change behavior. In: Michigan Consortium on Assistive Device Delivery Sys-tems: Resource Directory. 2nd ed. 1990:79-82.
51. Heisler M, Piette JD, Spencer M, et al. The relationship between knowledge of recent HbA1c values and diabetes care understanding and self-management. Diabetes Care 2005;28:816–22.
52. Schoenthaler AM, Schwartz BS, Wood C, Stewart WF. Patient and physician factors associated with adherence to diabetes medications. Diabetes Educ 2012;38:397–408.
53. Hibbard JH, Mahoney ER, Stock R, Tusler M. Do increases in patient activation result in improved self-management be-haviors? Health Serv Res 2007;42:1443–63.
54. Funnell MM, Anderson RM, Arnold MS, et al. Empower-ment: an idea whose time has come in diabetes education. Diabetes Educ 1991;17:37–41.
55. Piette JD. Interactive behavior change technology to support diabetes self-management: Where do we stand? Diabetes Care 2007;30:2425–32.
56. Bu D, Pan E, Walker J, et al. Benefits of information technol-ogy-enabled diabetes management. Diabetes Care 2007;30: 1137–42.
57. Meyers D, Peikes D, Genevro J, et al. The roles of patient-centered medical homes and accountable care organizations in coordinating patient care. Rockville, MD: Agency for Health-care Research and Quality; 2010.
58. Margolius D, Bodenheimer T. Transforming primary care: From past practice to the practice of the future. Health Aff 2010;29:779–84.
59. Cutler DM, Everett W. Thinking outside the pillbox--medica-tion adherence as a priority for health care reform. N Engl J Med 2010;362:1553–5.

www.jcomjournal.com Vol. 20, No. 11 November 2013 JCOM A
CliniCal Review
Figure.Reviewflowchart.This figure appeared on page 528 of the printed November issue.
Reportsidentifiedfromliteraturesearch/handsearchofreviews(n=1011)
Excluded (n = 940)Notleadbyphysiciansornurse(n=34)NotavailableinEnglish(n=5)Notanintervention(n=35)Didnotmeasuremedicationadherence(n=756)Notclinic-based(n=22)Dietary/physicalactivity/weightloss(n=21)Systematicreview/meta-analysis(n=31)Protocol(n=19)Qualitative(n=13)Targetchildren(n=4)
Studiesobtainedforfullpaperreview(n =70) Excluded (n = 55)Nomedicationadherence(n=35)Cross-sectionalstudy(n=11)Pharmacist-ledintervention(n=3)Notpractice-based(n=3)NotEnglish(n=3)
Studiesidentifiedfromhandsearchofreviewsandmeta-analyses(n=1)
Addedbyhandsearch(n=9)
Studiesprovisionallyincluded(n=24) Excluded (n = 6)Notclinic-based(n =3)Incompleteadherencedata(n =2)Didnotassessdiabetesmedication
adherence(n =1)Studiesincludedinfinalanalysis(n=18)

B JCOM November 2013 Vol. 20, No. 11 www.jcomjournal.com
adherence to diabetes Medications
Table.RiskofBias
Study
Sequence Generation
Allocation Concealment
Blinding
Incomplete Outcome data
Selective Outcome Reporting
Ahmadiouretal.,2010 Unclear Unclear Unclear Unclear Adequate
Bogneretal.,2012 Adequate Unclear Adequate Adequate Unclear
Edelmanetal.,2010 Adequate Adequate Adequate Adequate Adequate
Farmeretal.,2009 Adequate Adequate Adequate Adequate Adequate
Farmeretal.,2012 Adequate Adequate Adequate Adequate Adequate
Guldbergetal.,2010 Adequate Unclear Unclear Adequate Adequate
Heisleretal.,2010 Adequate Adequate Adequate Adequate Adequate
Kimetal.,2006* – – – Unclear Adequate
Kimetal.,2003 Adequate Unclear Unclear Unclear Adequate
Koetal,2004 Adequate Unclear Unclear Unclear Unclear
Linetal.,2006 Adequate Adequate Adequate Adequate Adequate
Mullanetal.,2009 Adequate Adequate Adequate Adequate Adequate
Negarandehetat,2013 Adequate Adequate Adequate Unclear Adequate
Pietteetal.,2000 Unclear Unclear Adequate Adequate Inadequate
Pietteetal.,2001 Adequate Adequate Adequate Adequate Adequate
Rubaketal.,2011 Adequate Adequate Unclear Adequate Unclear
Tanetal,2011 Adequate Adequate Adequate Unclear Unclear
Wongetal.,2005 Adequate Unclear Unclear Unclear Unclear
*Notarandomizedcontrolledtrial.
Supplemental material (not included in printed November issue):
PubMed Search Strategy
((((type2diabetesOR(diabetesmellitusAND("type2"OR"typeII"))))AND(patientcomplianceOR"patientadher-ence"OR "medical regimencompliance"ORmedicationadherenceOR "medicationnon-adherence"OR "patientnon-adherence"ORselfcareORtreatmentrefusalOR"treatmentadherence"))AND(physician-patientrelationORphysician-patientrelationsORphysician-patientrelationshipORpatient-physicianrelationORpatient-physicianrela-tionsORpatient-physicianrelationshipORpatient-physiciancommunicationORpatient-physiciancommunicationsORphysician-patientcommunicationORphysician-patientcommunicationsORdoctor-patient relationORdoctor-patient relations OR doctor-patient relationship OR doctor-patient communication OR doctor-patient communica-tionsORpatient-doctorrelationORpatient-doctorrelationsORpatientdoctorrelationshipORpatient-doctorcom-municationORpatient-doctorcommunicationsORprofessional-patientrelationORprofessional-patientrelationsORprofessional-patientrelationshipORprofessional-patientcommunicationORprofessionalpatientcommunicationORpatientprofessionalrelationsORpatient-professionalrelationsORpatient-professionalrelationshipORpatient-pro-fessionalcommunicationORpatientprofessionalcommunicationORproviderpatientrelationsORprovider-patientrelationsORprovider-patientrelationshipORprovider-patientcommunicationORprovider-patientcommunicationsORpatient-providerrelationORpatient-providerrelationsORpatient-providerrelationshipORpatient-providercom-municationORpatient-providercommunicationsORcommunicationORpatient-centeredORpatient-centeredcareORpatientparticipationORpatienteducation))AND(((“Case-ControlStudies”[Mesh]OR“ControlGroups”[Mesh]OR(case[TIAB]ANDcontrol[TIAB])OR(cases[TIAB]ANDcontrols[TIAB])OR(cases[TIAB]ANDcontrolled[TIAB])OR (case[TIAB] AND comparison*[TIAB]) OR (cases[TIAB] AND comparison*[TIAB]) OR “control group”[TIAB]OR “control groups”[TIAB]) OR (“clinical trial”[Publication Type] OR “Clinical Trials as Topic”[mesh] OR “Double-BlindMethod”[Mesh]OR (randomized[TIAB]AND (trial[TIAB]OR trials[tiab]))OR ((single[TIAB]ORdouble[TIAB]OR doubled[TIAB] OR triple[TIAB] OR tripled[TIAB] OR treble[TIAB] OR treble[TIAB]) AND (blind*[TIAB] ORmask*[TIAB]))))))
Copyright 2013 by Turner White Communications Inc., Wayne, PA. All rights reserved.

![ReviewArticle - Hindawi Publishing Corporation · 2020. 9. 19. · Cochrane Handbook for Systematic Reviews of Interven-tions [19]. e risks of allocation concealment (selection bias)andblindingofoutcomeassessment(detection](https://img.dokumen.tips/doc/110x75/611894beea522a525f0d7fcc/reviewarticle-hindawi-publishing-corporation-2020-9-19-cochrane-handbook.jpg)



























