Embed Size (px)
Citation preview

Stiell, Ian G Research Proposal
Research Module, Page 12a
A Study to Develop Clinical Decision Rules for the Hospital Admission of Patients with Acute Dyspnea
1. INTRODUCTION
Shortness of breath or dyspnea is a common presenting complaint in the emergency department (ED) and is associated with clinical conditions that have high rates of death and morbidity, particularly in older patients. Patients with dyspnea require the use of substantial diagnostic and therapeutic resources in the ED prior to a decision being made on whether hospital admission is warranted. There is, however, little evidence to guide decisions on appropriate patient disposition.
The most common conditions causing respiratory difficulty in older patients are congestive heart failure, chronic obstructive pulmonary disease, and community acquired pneumonia. Congestive heart failure (CHF) is a condition in which the heart cannot pump enough blood to the other organs. This can lead to swelling in the lower extremities and to fluid collecting in the lungs which interferes with breathing. Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking, which is characterized by progressive, partially reversible airflow obstruction, systemic manifestations, and exacerbations of dyspnea that increase in frequency and severity over time. Community acquired pneumonia (CAP) is an infection of the lungs caused by one of many different types of bacteria or viruses in patients who have not recently been hospitalized.
Older patients with CHF, COPD, and CAP are often admitted to hospital for their treatment. A small but important number of these patients die, require intensive care therapy, or suffer morbidity such as myocardial infarction. Many other patients are discharged after a brief period of therapy in the ED and do well at home. Some patients initially discharged from the ED, however, suffer relapse and must return to receive additional ED treatment or be admitted to the hospital. The issue of hospital admission decisions is an important question in modern health care. There is a significant shortage of hospital beds, EDs are overcrowded, and the decision to admit or discharge a patient from the ED is of considerable importance to the patient and to the health care system. There are, however, no widely accepted or validated guidelines to aid with the decision to admit or discharge these patients.
Our research group has developed an expertise for developing clinical decision rules such as the Ottawa Ankle Rules and the Canadian C-Spine Rule. Clinical decision rules are clinical tools developed from original data for the purpose of assisting with bedside diagnostic and therapeutic decisions. We believe there is a need to develop new decision rules to assist with the admission decisions for ED patients with CHF, COPD, and CAP. We have also piloted a standardized assessment tool for respiratory distress patients being considered for discharge from the ED, the “3-Minute Walk Test” and we believe this may become a key component of decision rules for admission. This walk test assessment has patients walk at their own pace for 3 minutes with ongoing measurements of respiratory rate, heart rate, and oxygen saturation. Our preliminary data suggest that this tool may be able to identify patients at increased risk of adverse events and who, therefore, are not safe for discharge. Our research group also has considerable experience in conducting clinical studies on patients with CHF, COPD, and CAP and in conducting patient safety studies.
The overall goal of this study will be to develop three separate decision rules to guide the admission decisions of physicians for older ED patients with acute dyspnea secondary to CHF, COPD, or CAP. In particular, these rules will be highly sensitive for predicting the potential for development of adverse events amongst such patients. This will improve and standardize admission practices for these patients, diminishing both unnecessary admissions as well as unsafe discharge decisions.
2. BACKGROUND 2.1 Statement of the Problem
2.1.1 Emergency Department Crowding and Admission Decisions Overcrowding in hospital EDs is one of the most challenging issues currently facing the
Canadian health care system. It is defined as a situation in which the demand for emergency services has exceeded the ability to provide care within a reasonable time.1 It is a complex issue which has been emerging as a health care crisis in the past decade in most large, urban and academic North American

Stiell, Ian G Research Proposal
Research Module, Page 12b
EDs.2 In Canada, there is recognition that the cause of ED overcrowding is multifactorial and the problem is system wide, with no simple solutions.3;4 An ED Overcrowding model has been used to conceptualize ED processes and to identify strategies for reducing overcrowding.5 This model is based on engineering principles, queuing theory and compartmental models of patient flow. The role of admissions in the current overcrowding crisis cannot be ignored. For example, the leading cause of ED overcrowding cited in a recent Canadian Agency for Drugs and Technologies in Health report was ED in-patients or access block, whereby patients admitted to the hospital must stay in the ED due to a lack of ward beds.6 The inability of EDs to decant the admitted patients reflects system wide issues related to active care bed shortages, lack of chronic care alternatives, inefficiencies within the in-patient setting, and inconsistencies in ED decision making among physicians. The issue of admissions has become so important in the UK that they have recently established a commission to reduce admissions on 20 sentinel diagnoses. Importantly, CHF, COPD, and CAP are all on that list.7 2.1.2 Patient Safety Patient safety is a major problem in healthcare.8 Studies from Canada, the US, and many other countries demonstrate that large numbers of patients experience avoidable harm during the course of their treatments.9-15 In Canada, an estimated 28,000 patients die from health care error annually.9 Several types of healthcare errors can lead to ‘avoidable harm’. For example, diagnostic errors can lead to harm as patients will have delayed or incorrect treatments. Other common errors include treatment errors and procedural errors. Another class of errors is termed ‘system errors’. These occur when defects in the health care system are the direct cause of harm. For example, system errors include cases in which equipment malfunctions lead to harm, or situations where a patient receives inappropriate attention because of overcrowding. In the ED, one common error includes unsafe disposition decisions. In these cases, patients with serious conditions such as CHF, COPD, or CAP are sent home inappropriately and consequently experience worse outcomes than expected. Our preliminary research suggests that 4-6% of ED patients experience harm related to such errors.16;17 2.1.3 Dyspnea in the ED Setting The appropriate evaluation of dyspnea is key to the practice of emergency medicine. This symptom is associated with high risk clinical syndromes including myocardial infarction, pulmonary embolism, asthma, CHF, COPD and CAP. This proposal will focus on the latter three common ED presentations of dyspnea for which accurate medical decisions on disposition are critical and for which evidence-based guidelines are lacking. 2.1.4 Congestive Heart Failure CHF is a common and serious condition that affects 200,000 to 300,000 people in Canada.18 In one study, CHF was the second most common reason for hospitalization in Canada with the average length of stay being 12.9 days and accounting for 1.4 million hospital days.19 Moreover, CHF often co-exists with other chronic diseases (such as diabetes mellitus, COPD, and coronary artery disease) which further contribute to hospitalization and prolonged lengths of stay. Importantly, patients who are admitted to hospital for CHF have readmission rates as high as 30% to 60% within 3 to 6 months after initial discharge.20-22 Randomized controlled trial evidence for the efficacy of well accepted therapies in the ED setting is lacking.23-26 Until recently, there were no clinical guidelines for the management of acute CHF. The recent European Society of Cardiology acute CHF guidelines focused primarily on treatment of the acute heart failure symptoms.27
The decision to admit patients to the hospital from the ED for CHF is largely not evidence-based. Although there are numerous studies that have examined the outcome of patients hospitalized for heart failure there are surprisingly few published studies on the outcome of patients discharged from the ED with a primary diagnosis of acute CHF. Relapse after discharge is a particularly problematic issue.28-32 For example, in a recent study in Edmonton, Alberta, 46% of patients with CHF were discharged from the ED after their assessment and treatment, 14% relapsed (50% were admitted) within 30 days, and 7.4% of patients died within 180 days after initial presentation to the ED.33 Patients with CHF exacerbations re-presented with acute myocardial infarction, acute coronary syndrome, and recurrent CHF. In 2003, Brewer reported that 43% of patients discharged from the ED with heart failure returned for an unscheduled visit within 30 days and overall 20% of patients required hospital admission within this period.34 A study by Rame showed that 60% of patients returned to the ED with another acute episode of CHF within 3 months of the initial visit; more than half of these

Stiell, Ian G Research Proposal
Research Module, Page 12c
patients required hospitalization.35 Clearly, the ED presentation of CHF is a critical event for patients with CHF, and better decision making in the ED could reduce resource utilization, improve outcomes and improve the patient’s quality of life. 2.1.5 Chronic Obstructive Pulmonary Disease Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking, which is characterized by progressive, incompletely reversible airflow obstruction, systemic manifestations, and increasing frequency and severity of exacerbations.36 COPD is a major cause of morbidity and mortality in North America. Estimates of Canadian health-professional-diagnosed COPD prevalence rates, derived from the 1994-95 National Health Survey, indicate a COPD prevalence rate of 4.7% in persons aged 55-64, 5.4% in those 65-74 and 8.3% in persons aged greater than 75.37 Recent trends suggest that disease prevalence and hospital discharge rate in Canada is stable in men, but increasing among women, reflecting a 40 year societal trend towards increased smoking among females.38 As outlined below, these estimates likely underestimate the true prevalence of COPD in Canada. In Canada, deaths from COPD increased from 4,438 in 1980 to 9,398 in 1998, establishing COPD as the fourth leading cause of death in men and the seventh in Canadian women.39 Studies suggest that patients who experience frequent exacerbations of COPD (more than two per year) are at higher risk for death, and that these patients experience greater declines in health-related quality of life compared to those who have fewer exacerbations.40 Canadian data show that hospitalizations for COPD peak in mid-winter and are linked to hospitalizations for respiratory tract infections among men and women over age 50.39 Economic analyses suggest that hospitalization alone consumes up to 70% of all medical expenses for patients with COPD.38
Data from the US National Hospital Ambulatory Medical Care Survey showed that there were an estimated 1,549,000 annual ED visits for COPD in the US in 2000.41 This rate has been increasing over time.36 Roughly one half of COPD patients who present to the ED are hospitalized and 2000 data from the US National Hospital Discharge Survey showed that 726,000 hospitalizations from COPD.42 A clinical trial done by our group showed that relapse, defined as an unscheduled visit to a physician’s office or return to the ED within 30 days because of worsening respiratory symptoms, occurred in 35% of COPD patients who were discharged from 10 Canadian academic EDs.43 2.1.6 Community Acquired Pneumonia CAP is commonly defined as an acute infection of the pulmonary parenchyma that is associated with at least some symptoms of acute infection, accompanied by the presence of an acute infiltrate on a chest radiograph consistent with pneumonia in a patient not
hospitalized or residing in a long-term-care facility for >14 days before onset of symptoms. Symptoms of acute lower respiratory infection may include several (in most studies, at least 2) of the following:
fever or hypothermia, rigors, sweats, new cough with or without sputum production or change in color
of respiratory secretions in a patient with chronic cough, chest discomfort, or the onset of dyspnea.44 CAP is a common ED presentation and assessments are an important component of
management. In the United States, the incidence of pneumonia has been estimated at 12 per 1000, and annual admissions to hospital are in the range of 1 million per year.44;45 Further, it is estimated that 75% of the decisions to admit patients are made in the ED. There have been many guidelines developed to guide treatment, admission varies based on factors such as age, gender, co-morbidities, severity of illness, and outcomes can range to the extreme of respiratory failure and death.
Admission to hospital is a complex issue fraught with medical misjudgment. For example, in the past many patients with excellent outcomes were admitted, consuming valuable in-patient resources. Conversely, those who needed to be admitted often were not, and suffered adverse consequences such as relapse, prolonged morbidity, and even death. Admission rules were first developed and validated by the Patient Outcomes Research Team (PORT), and suggested that patients could be categorized into 5 classes from low risk (Class I; mortality < 1%) to high risk (Class V; mortality ~ 30%).46-48 The PORT Pneumonia Severity Index (PSI) is composed of demographic, clinical, laboratory and radiographic findings at presentation (Appendix 1-2a). Emergency physicians find these guidelines to be cumbersome and difficult to use, to be lacking other issues (e.g., intravenous drug abuse, homelessness, support systems), and to be lacking any functional

Stiell, Ian G Research Proposal
Research Module, Page 12d
assessment.49 In summary, despite some advancement in the past decade, the decision to admit CAP patients remains complex and often not evidence-based.50;51
Relapse after ED discharge for CAP patients does occur but less frequently than for COPD and CHF patients.52 In a recent study in North American EDs, approximately 12% of patients with CAP who were discharged from the ED after their assessment and treatment returned with a relapse.53 Patients with CAP relapses can also present with co-morbidities such as CHF, exacerbations of COPD and other chronic conditions, as well as complications of treatment. Clearly, the ED presentation of CAP is a critical event for patients, especially the elderly. Improved decision making in the ED could reduce resource utilization, improve outcomes and improve the patient’s quality of life.
2.2 Methodological Standards 2.2.1 Clinical Decision Rules Clinical decision (or prediction) rules attempt to reduce the uncertainty of medical decision making by standardizing the collection and interpretation of clinical data.21;54-57 A decision rule is derived from original research and may be defined as a decision making tool that incorporates three or more variables from the history, physical examination, or simple tests. These decision rules help clinicians with diagnostic or therapeutic decisions at the bedside. There has been considerable interest in the methodological standards for their development and validation and these may be summarized as follows.58-60 a) The outcome or diagnosis to be predicted must be clearly defined and assessment should be made in a blinded fashion. b) The clinical findings to be used as predictors must be clearly defined and standardized and their assessment must be done without knowledge of the outcome. c) The reliability or reproducibility of the predictor findings must be demonstrated. d) The subjects in the study should be selected without bias and should represent a wide spectrum of characteristics to increase generalizability. e) The mathematical techniques for deriving the rules must be identified. f) Decision rules should be clinically sensible: have a clear purpose, be relevant, demonstrate content validity, be concise, and be easy to use in the intended clinical application. g) The accuracy of the decision rule in classifying patients with (sensitivity) and without (specificity) the targeted outcome should be demonstrated. h) Prospective validation on a new set of patients is an essential test of a new decision rule. This validation process is very important because many statistically derived rules or guidelines fail to perform well when tested in a new population.61-63 The reason for this poor performance may be statistical, i.e., overfitting or instability of the original derived model,64 or may be due to differences in prevalence of disease or differences in how the decision rule is applied.65;66 The methodological standards for a validation study are similar to those described above. i) Implementation to demonstrate the true effect on patient care is the ultimate test of a decision rule; transportability can be tested at this stage.67 2.2.2 Patient Safety Studies evaluating patient safety commonly use ‘adverse events’ and ‘preventable adverse events’ as outcomes. 9-15 In this literature, an adverse event is a poor health outcome that is caused by medical care as opposed to the patient’s underlying disease. For example, an allergic reaction to penicillin would be considered an adverse event. Adverse events are preventable if they were avoidable. For example, if a patient was prescribed penicillin despite having a previous reaction to it, then the adverse event should not have occurred (i.e. it was preventable). On the other hand, if the patient had never been exposed to penicillin, the event would not be avoidable.
Rating cases as adverse events is not based on explicit criteria because there are large numbers of treatments in healthcare and even larger number of possible adverse events. It would be almost impossible to achieve consensus on explicit criteria for all such complications. Therefore, in order to determine whether an outcome was due to medical care and whether it was preventable, physicians review the case and perform judgments based on their own implicit criteria. To classify cases as adverse events, patient safety investigators require that ratings from two physicians must agree.9-15
2.3 Previous Studies to Develop Admission Criteria for Respiratory Distress 2.3.1 Congestive Heart Failure In the past, virtually all patients with acute CHF were hospitalized.68 Today, many of these patients are seen in the ED and subsequently discharged to the community for follow up with their personal physicians. Although numerous studies have examined the outcome of patients hospitalized for heart failure, there are surprisingly little published data on the

Stiell, Ian G Research Proposal
Research Module, Page 12e
outcome of patients discharged from the ED with a primary diagnosis of acute CHF.28-32 This suggests that the decision to hospitalize or discharge a patient with acute CHF from the ED is largely based on a lack of high-quality evidence and/or administrative factors. The few studies to develop admission guidelines for CHF have important limitations. In particular, these studies use large administrative databases rather that prospective and specific ED data collection. Hence, they were unable to evaluate the status of patients after a period of ED management and they did not incorporate any form of walk test. None of these guidelines have been prospectively validated nor been implemented into practice. Auble developed a rule based upon a retrospective review of two proprietary Pennsylvania databases and used only patients who were admitted.28 This rule has not been prospectively validated. Fonarow developed a decision guideline from a large U.S. in-hospital registry of heart failure patients and stratified risk based upon 3 variables: systolic blood pressure, blood urea nitrogen, and serum creatinine.69 This model also does not incorporate variables later in the ED course and has not been prospectively validated to evaluate safety and effectiveness. Lee developed a complex scoring model to predict mortality for CHF patients already admitted to Canadian hospitals.70 Again, this study is limited by not including patients discharged from the ED, by not including ED status after treatment, and not being prospectively validated. Recently there has been much discussion of the role of the serum marker, B-type Natriuretic Peptide (BNP), for the diagnosis and prognosis of patients with CHF.71-74 BNP is a cardiac neurohormone released by the ventricles during systolic dysfunction or ventricular wall stress. There is a correlation between elevated BNP levels and the presence and severity of CHF. Higher BNP levels are associated with increased mortality and morbidity for outpatients with CHF, an effect that is independent of other cardiac markers, including troponin. Despite enthusiasm for BNP in the literature and in U.S. EDs, its value for improving care in the ED is unclear and its use is not common in Canada.75;76 We believe that our study offers a unique opportunity to evaluate the usefulness of BNP levels in predicting adverse events for CHF patients being considered for discharge. 2.3.2 Chronic Obstructive Pulmonary Disease A recently published prospective cohort study of 140 COPD patients discharged from 29 North American EDs revealed that by day 14, 21% had relapsed and re-presented for urgent clinic or ED visits.77 This study developed a multivariate model for relapse but is limited by very small sample size, not including response to therapy or a walk test. No prospective validation has been reported. An ED study of 83 COPD patients showed that a spirometry FEV1 value of less than 40% of predicted, identified patients who required hospital admission or who suffered a relapse after being discharged from hospital with a sensitivity of 0.96, specificity of 0.58, and overall accuracy of 0.78.78 Combining clinical assessment with spirometry led to an improvement in specificity to 0.73. The authors concluded that patients with an FEV1 of > 40% of predicted or no clinical evidence of respiratory distress after treatment may be safely discharged from the ED. This very small study has not been validated but does provide useful information. Other ED studies have shown that physician estimation of FEV1 in the ED is poor, that peak expiratory flow rates in the ED do not acceptably agree with the actual FEV1 measurement, and that there is not good correlation between the arterial pO2 and the FEV1 in the ED.79-81 2.3.3 Community Acquired Pneumonia Early work in the development of decision rules for CAP has focused on the decision to hospitalize53.82;83 Subsequently, models focused on mortality, based on the argument that the identification of patients at low risk for mortality or complication would result in these patients being safely treated as outpatients. Researchers have developed and validated prognostic rules for the elderly;84 for patients admitted to the general ward,85-88 and to the intensive care unit .89-92
The most frequently quoted rule is the Patient Outcomes Research Team (PORT) Pneumonia Severity Index (PSI) developed for pneumonia.46 In this rule, a variety of historical, physiological, physical examination and laboratory factors are combined to determine a cumulative PORT PSI score. Scores that are low represent groups of patients (Class I and II) with low mortality risk (< 1%) and these patients are generally safe for discharge if they have appropriate antibiotic treatment and follow-up. Patients with higher scores (Classes IV, V) have higher mortality (~10 and 30%, respectively) and should be admitted to hospital. Class III patients may need short hospitalizations or observation

Stiell, Ian G Research Proposal
Research Module, Page 12f
following assessment. The PORT PSI score has been validated and its use has been widely encouraged in North American guidelines.46-48;51 Unfortunately, the rule is cumbersome, difficult to remember, and many emergency physicians feel that it does not reflect some of the important issues relevant to their setting (e.g., social situation, homelessness, compliance, poverty, drug abuse, etc). In addition, the rule does not incorporate response to ED therapy nor any form of walk test. The 2006 edition of "Rosen's Emergency Medicine" says this about the PORT PSI: "Although this method of assessing the likelihood of successful outpatient management is helpful, it can be cumbersome to use, has not been modeled to predict acute life threatening events, does not take into account dynamic evaluations over time, and has many important exceptions (e.g. an otherwise low-risk patient with hypoxia would be discharged by strict interpretation of this rule)…Additional discharge criteria could include improving vital signs over a several-hour observation period, ability to take oral medications, an ambulatory pulse oximetry greater than 90%, home support, and ability to follow up.”49 2.3.4 Functional Walk Tests Patients with chronic cardiac and respiratory disease often have walk tests administered as a means of evaluating functional status, treatment effectiveness, and establishing prognosis.93 These are done in the office or clinic setting under controlled conditions. A variety of walk tests exist, including time-based tests (e.g. 2-min walk test, 6-min walk test, 2 and 12-min walk test); fixed-distance tests (e.g. 100 m, half-mile, and 2-km walk tests; velocity-determined walk tests (e.g. self-paced walk test); and controlled-pacing incremental tests (e.g. incremental shuttle walk test).94-100 These functional walk tests are exercise tests that measure functional status or capacity, mainly the ability to undertake activities of daily living. Walk tests require no technical expertise, making them inexpensive and easy to administer and therefore ideal for the ED setting. More importantly, they employ an activity that individuals perform on a daily basis (i.e. walking).
A recent review documented the use of these walk tests in the outpatient setting but we are aware of no previous work validating this approach for acutely ill patients in the ED setting.93 Nevertheless, many emergency physicians use some variation of a walk test as part of their assessment of the suitability to discharge older patients, particularly those with shortness of breath.49 We believe there is a great need to standardize the walk test for ED use and to validate its usefulness in predicting short-term outcomes for these patients.
2.4 Preparatory Work by Applicants 3-Minute Walk Test Pilot Study The applicants recently conducted a pilot study to evaluate the feasibility and predictive value of a “3-Minute Walk Test” specifically designed for older ED patients with shortness of breath.101 Details are provided in the draft manuscript (Appendix 1-3a). We enrolled Ottawa Hospital ED patients aged 50 years or older with CHF, COPD, or stable chest pain and who were being considered for discharge by the attending emergency physician. Patients were supervised by a respiratory therapist and medical student research assistant and were asked to ambulate within the ED at their own pace either on room air or baseline home oxygen level. At each minute for 3 minutes, one minute post-walk, and at baseline, the values four measurements were recorded: dyspnea on the modified Borg scale, oxygen saturation, heart rate, and respiratory rate. The outcome measures included admission to hospital, need for BiPAP, need for intubation, relapse within 14 days, and death.
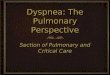
Overall, 40 patients were enrolled into the study (16 CHF, 9 COPD, 15 stable chest pain) and 12 patients (30%) had adverse outcomes (Table 1). Completion of the walk test was the best predictor of outcome, with 96% of those with good outcomes completing the test compared to only 58% of those with adverse outcomes (p<0.01) (Table 2). A repeated measures general linear model compared minute-by-minute measurements and showed good discrimination between the good and adverse outcome groups, with p-values <0.10 for dyspnea, respiratory rate, heart rate, and oxygen saturation measurements (Figure). We believe that the additional effort of measuring respiratory rate manually is not a useful component. We concluded that this standardized 3-Minute Walk Test was simple to perform in the ED and provided valuable prognostic information and should be further evaluated. Review of Cases at Study Sites To prepare for the current application, we conducted a health records review of all patients seen in the ED with CHF and COPD at one Ottawa Hospital campus over a 3-month period in 2005.102 After excluding patients who were obviously too ill to be discharged

Stiell, Ian G Research Proposal
Research Module, Page 12g
(HR > 110, Oxygen saturation < 90%, chest pain), we reviewed clinical and outcome characteristics (Table 3). Among 77 CHF patients, 38% were admitted from the ED, 29% suffered an adverse event, and 19% of all patients relapsed within 14 days. Among 40 COPD patients, 30% were admitted from the ED, 20% suffered an adverse event, and 15% relapsed within 14 days. We also found that 12 specific clinical and laboratory findings were significantly associated with adverse outcome. For CAP patients, we reviewed data from a cohort seen in the University of Alberta Hospital.52 Among 364 CAP patients seen in the ED and aged 50 years or more, 75% were admitted to hospital, 7.5% died, and 8% relapsed back to the ED within 7 days. Clinical Decision Rule Research Over the past 15 years our group has conducted a unique series of studies to develop clinical decision rules for diagnostic imaging in the ED. We hold a CIHR Group Grant for Decision Support Tools for Clinicians and Patients and have also published several methodology papers.59;60;103;104 a) Ottawa Ankle Rules Project. From 1991-95, we conducted a series of studies involving 17,000 patients to derive, validate, and implement decision rules for radiography in acute ankle injuries.105-108 A cost-effectiveness study showed that widespread use could lead to large health care savings.109 Two large surveys showed that the Rules are used by virtually all Canadian emergency physicians and by most in the U.S., U.K., France, and Spain.110;111 b) Ottawa Knee Rule Project. We also completed studies to develop a decision rule for radiography in knee injuries.112-114 We demonstrated the potential cost-effectiveness of this rule as well as the fact that it is being widely adopted by physicians.115 c) Canadian C-Spine Rule Project. We have conducted a series of CIHR funded studies to derive, validate and implement the Canadian C-Spine Rule in multicentre studies with more than 27,000 patients.116-118 d) Canadian CT Head Rule Project. We have also conducted another series of CIHR funded studies to derive, validate and implement the Canadian CT Head Rule in multicentre studies with more than 10,000 patients.119;120 Patient Safety Research Our group has performed patient safety studies in a number of settings demonstrating that errors occur across the continuum of healthcare, including hospitals, family doctors offices, nursing homes, and EDs. In the ED, one common error includes unsafe disposition decisions. In these cases, patients with serious conditions such as CHF, COPD, or CAP are sent home inappropriately and consequently experience worse outcomes than expected. Our preliminary research suggests that 4-6% of ED patients experience harm related to such errors.16;17
2.5 Rationale for the Study Patients older than 50 years of age frequently present to the ED with shortness of breath due to
CHF, COPD, and CAP. These patients are often admitted to hospital and not uncommonly suffer adverse events. At the same time, Canadian hospitals suffer from a shortage of in-patient beds and severe overcrowding in the ED. There are no widely accepted guidelines to assist physicians with their decision to admit or discharge these patients with shortness of breath. Our research group has considerable experience with the management of CHF, COPD, and CAP, with the development of clinical decision rules, and with patient safety research. We have also conducted pilot research into the standardization of the 3-Minute Walk Test which we believe will have an important role in ED admission guidelines. We believe that there is a strong need to develop validated decision rules to allow rational and safe admission decisions for patients with these conditions. This will ultimately improve and standardize admission practices for these patients, diminishing both unnecessary admissions as well as unsafe discharge decisions.
3. SPECIFIC OBJECTIVES The overall goal of this study will be to develop three separate clinical decision rules to guide
the admission decisions of physicians for older ED patients with acute dyspnea secondary to CHF, COPD, or CAP. In particular, these rules will be highly sensitive for predicting the potential for development of adverse events amongst patients aged 50 or more with these three conditions. Clinical decision rules will improve and standardize admission practices for these patients, diminishing both unnecessary admissions as well as unsafe discharge decisions.
Specific objectives with regards to older COPD, CHF, and CAP ED patients are to: 1. Prospectively evaluate patients for standardized clinical and laboratory assessments;

Stiell, Ian G Research Proposal
Research Module, Page 12h
2. Evaluate patients for the 3-Minute Walk Test; 3. Evaluate patients for the development of adverse events within 14 days; 4. Determine the association between the clinical findings, laboratory findings, and the 3-Minute Walk Test with adverse events; 5. Use multivariate techniques to derive 3 highly sensitive clinical decision rules; 6. Assess the classification performance and potential impact of the derived decision rules; and 7. Determine if the adverse events should be considered “preventable”.
4. METHODS 4.1 Study Design
We will conduct a prospective observational cohort study in four Canadian EDs and will evaluate older patients with dyspnea for predictor variables prior to assessment of adverse events.
4.2 Setting The study setting will be four Canadian teaching hospitals with a combined annual ED volume of approximately 240,000 patient visits (Ottawa Hospital Civic and General Campuses, Kingston General Hospital, University of Alberta Hospital, Edmonton). These sites have had considerable success in recruiting many ED patients for clinical studies conducted by the applicants. We are confident that these sites will enrol large numbers of patients with a wide spectrum of disease severity. 4.3 Study Population 4.3.1 Inclusion Criteria Included will be all stable adults > 50 years, who present with shortness of breath or dyspnea due to CHF, COPD, or CAP and are well enough to be considered for discharge by the attending ED physician. Some patients will have more than one diagnosis from amongst CHF, COPD, and CAP.
a) CHF refers to patients with acute shortness of breath secondary to an exacerbation of chronic CHF or new onset CHF. There is no gold standard for the diagnosis of heart failure and there has been much variation in the diagnostic criteria used in previous studies. We will use the criteria recommended by the working group on heart failure of the European Society of Cardiology.29;121;122 Patients must have appropriate symptoms (shortness of breath or fatigue) with clinical signs of fluid retention (pulmonary or peripheral) in the presence of an underlying abnormality of cardiac structure or function. If an element of doubt remains, a beneficial response to treatment for heart failure (for example, a brisk diuresis accompanied by substantial improvement in breathlessness) will also be considered. Where the diagnosis is unclear from the case records, a panel of three investigators, blinded to the outcome and treating physician’s diagnosis, will review the cases. We will not base diagnosis on BNP as this test is not considered to be specific for CHF.
b) COPD refers to patients with exacerbation of COPD, defined as the presence of an increase in at least two of the following three clinical criteria: breathlessness, sputum volume, or sputum purulence.43 Patients either have previously received a diagnosis of COPD or have a one-year history of chronic dyspnea or cough with sputum production. Additional inclusion criteria necessary are a history of 15 pack-years or more of cigarette smoking, and evidence of at least moderate airflow obstruction (as defined by GOLD guidelines) in the emergency department.123 Moderate airflow obstruction is defined as a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity of 0.70 or less, and a post-bronchodilator FEV1 less than 80 percent of the predicted value.
c) CAP refers to patients who present with a new episode of CAP defined as: 1) presence of a new radiographic pulmonary infiltrate, and 2) the acute onset of at least one confirmatory clinical finding suggestive of pneumonia, including cough, dyspnea, pleuritic chest pain, sputum production, fever, and altered mental status.83 Patients must not have been hospitalized or residing in a long-term-care facility for 14 or more days before onset of symptoms.44 4.3.2 Exclusion Criteria We will exclude patients with any of the following critieria (i.e. patients who appear to be too ill to be considered for discharge after several (4-8) hours of ED management or who do not fit with the accepted definitions of CHF, COPD, or CAP): 1. Resting oxygen saturation < 90% on room air or on baseline oxygen levels (after 4-8 hours in ED); 2. Heart rate greater than or equal to 110 bpm (after 4-8 hours in ED);

Stiell, Ian G Research Proposal
Research Module, Page 12i
3. Systolic blood pressure < 90 mm Hg (after 4-8 hours in ED); 4. Confusion or disorientation; 5. Inability to walk; 6. Ischemic chest pain requiring treatment; 7. Acute ischemic ST-T ECG changes; 8. Terminal status – death expected within weeks from chronic illness; 9. Immunocompromised, neutropenia, HIV infection, transplant patients, immunosuppressive drugs (CAP patients); 10. Unusual pneumonias such as those due to an obstructing tumour or tuberculosis (CAP patients); 11. Hospital admission within 14 days; pneumonia within 6 weeks (CAP patients); 12. From nursing home or chronic care facility. 4.3.3 Patient Selection Consecutive eligible patients will be entered into the study if they meet the inclusion and exclusion criteria and if study personnel are available to perform the 3-Minute Walk Test. This will occur 24 hours per day, seven days per week. The initial decision to select patients will be made by the attending emergency physicians based upon their diagnosis of CHF, COPD, or CAP. Final determination of eligibility will be made by a panel of investigators, who will be blinded to the outcomes of the patients. Basic demographic and clinical data will also be collected for eligible patients who are not enrolled into the study. 4.3.4 Ethical Considerations The research ethics boards of the participating hospitals have determined that written informed consent need not be obtained for this observational study. As in previous similar studies conducted by our group, normal patient management will not be altered. Patients are not being subjected to new therapy, invasive procedures, undue risk or discomfort, or investigations beyond that which would normally be required in the course of patient care. The 3-Minute Walk Test is merely a standardized form of the clinical assessment which is part of routine care for these patients. We do not expect to approach patients after discharge from the ED. Patient confidentiality will be maintained throughout the study and patient identifiers will be removed.
4.4 Management Protocols We will encourage each of the four sites to standardize the ED management of patients with the three sentinel study conditions, CHF, COPD, and CAP. Towards that end, we have reviewed local care plans and guidelines for these conditions from Kingston and Edmonton (Appendix 1-2b). We will encourage all sites to adopt variations on these care plans for their ED staff.
4.4 Standardized Patient Assessment 4.4.1 Patient Assessment Patient assessments will be made by Registered Respiratory Therapists or Registered Nurses. These research assistants will be trained by means of lectures and practical demonstrations to assess the 3-Minute Walk Test, the Modified Borg Scale, and other variables in a uniform manner. A standardized description of each assessment will be appended to the data collection sheets. The research assistants will record their findings on data collection sheets (Appendix 1-2c). There will be ongoing evaluation of the quality of the patient assessments judged by completeness of data collection sheets and compliance in enrolling eligible patients. Staff will be provided regular feedback of a general nature as well as specific review of any individual problems which may arise. 4.4.2 Selection of Variables The variables selected for assessment in the study were chosen by the investigators based on their clinical experience and reports in the literature for CHF,28;69;70;124;125 COPD,43;77;126;127 CAP,46;48;51;128;129 and 3-Minute Walk Test.93-101 These variables are felt to be useful in predicting whether or not patients are likely to suffer adverse events in the 14 days following the ED visit. The inclusion of too many variables in the protocol would increase the burden for patients and the assessors and lead to decreased compliance with the study. Several variables discussed in the literature were felt to be not useful or not reliable and will not be included (e.g. cyanosis, gallop, rales, wheezes,). The following sections list the variables to be collected and the proposed data Case Record Form is shown in Appendix 1-2d. 4.4.3 Variables from History a) Demographic (age, gender); b) Past Medical History (congestive heart failure, NYHA classification, angina, myocardial infarction, percutaneous coronary intervention,

Stiell, Ian G Research Proposal
Research Module, Page 12j
CABG, diabetes mellitus, chronic obstructive pulmonary disease, chronic renal disease, peripheral vascular disease, cancer, chronic liver disease/cirrhosis, cerebrovascular disease, dementia, pacemaker, current smoker, smoker pack-years, hypertension, atrial fibrillation, previous admission for respiratory distress, previous intubation for respiratory distress); c) Medications (current oral antibiotic use, home oxygen, current prednisone, chronic medications); d) Current Symptoms (dyspnea, duration of dyspnea, pleuritic chest pain); and, e) Social factors (lives alone with no caregiver). 4.4.4 Variables from General Examination Some variables will be assessed on arrival and then again at reassessment, 4 to 8 hours after the initial assessment. The exact time of reassessment will be determined by the attending physician’s judgment that there has been sufficient time for response to therapy and that the patient is well enough to undergo the 3-Minute Walk Test. a) Vital Signs on arrival and after 4 - 8 hours (systolic blood pressure, heart rate, respiratory rate, temperature); b) Oxygen Saturation on arrival and after 4-8 hours, by pulse oximetry on room air or home O2 level; c) Altered Mental Status, defined as disorientation to place, person, or time; d) Quantity of Diuresis after 4-8 hours (CHF patients); e) Ability to Intake Fluids Orally; and, f) Modified Borg Scale on arrival and after 4 – 8 hours (Appendix 1-2c).130 4.4.5 The 3-Minute Walk Test The 3-Minute Walk Test assessment will be performed by trained Registered Respiratory Therapists (RRT) or Registered Nurses (RN) at time of reassessment, i.e. 4-8 hours after initial assessment. Patients will be asked to walk at their own pace in the ED for a fixed period of 3 minutes, regardless of the distance covered. Patients may use their normal walking aids (e.g. cane or walker) but may not be physically supported by another person. Patients will use no supplementary oxygen or will use their normal home oxygen flow level. The attending RRT or RN will attach the study pulse oximeter to the patient’s finger and the oximeter will continually measure heart rate and oxygen saturation levels, giving ongoing readouts and also keeping permanent recordings. We will request purchase of specific recording oximeters in our study budget. For safety reasons, the 3-Minute Walk Test will be discontinued immediately if: a) Patient requests to stop for any reason or is unable to continue walking; b) Oxygen saturation decreases to less than 86%; c) Heart rate exceeds 110 bpm; or d) Patient complains of chest pain. The RRT or RN will record the following data on the 3-Minute Walk Test form (Appendix 2-1c): a) Initial heart rate and oxygen saturation level, at rest; b) Highest heart rate and lowest oxygen saturation level, during the 3 minutes of the walk test; c) Heart rate and oxygen saturation level, one minute following the walk test; d) Inability to complete the walk test and the reason for not completing (fatigue, dyspnea, chest pain, oxygen saturation level, heart rate). 4.4.6 Variables from Laboratory Tests We will collect results of routinely performed laboratory tests but will not require non-routine tests other than BNP for CHF patients. a) Routine Chemistry (blood urea nitrogen, creatinine, sodium, potassium, glucose, CO2); b) B-type Natriuretic Peptide (BNP) for CHF patients only (not routinely collected in Canadian hospitals – will reimburse hospitals); c) Hematology (hemoglobin, white blood cell count); d) Arterial blood gases - pCO2, pO2, pH (optional at discretion of treating physician; not routine management for all patients); e) ECG Abnormalities – acute or potentially serious findings (infarction, ischemia, atrial fibrillation/flutter, ventricular tachycardia, a-v conduction disturbance, intraventricular conduction disturbance); f) Chest X-ray Findings – relevant acute or serious findings by final radiology report (pulmonary congestion, pleural effusion, cardiomegaly, pneumonia, pneumonia number of lobes); g) Spirometry (FEV1, FVC, peak flow on arrival and at 4 – 8 hours – COPD only). 4.4.7 Interobserver Reliability Interobserver reliability of the predictor variables will NOT be evaluated as most variables are discrete and clear-cut with little need for subjective interpretation. The only exception is the 3-Minute Walk Test and we believe that it is not appropriate to ask some patients to repeat this assessment for a second observer. 4.4.8 Data Collection The patient assessment data, as described above, will comprise the predictor variables for the data analyses and will be collected from the following sources: a) ED Health Record, including physician, nursing, and RRT notes; b) Ambulance Call Report (if applicable);

Stiell, Ian G Research Proposal
Research Module, Page 12k
c) Hospital Health Record; d) 3-Minute Walk Test Form, to be completed by study RRT or RN (Appendix 1-2c). e) Case Record Form, to be completed by site research assistant (Appendix 1-2d).
4.5 Outcome Measures 4.5.1 Primary Outcome The primary outcome measure will be “adverse event” defined as any of the following within 14 days of the ED visit, regardless of whether or not the patient is admitted to hospital: a) Death from any cause; b) Admission to a Monitored Unit (including intensive care units, coronary care units, acute monitoring units, or stepdown units); c) Endotracheal Intubation; d) Need for Non-Invasive Ventilation (e.g. BiPAP) after hospital admission, unless on BiPAP at home; e) Myocardial infarction as defined by international consensus standards.131;132 Either one of the following criteria satisfies the diagnosis for an acute, evolving or recent MI: 1) Typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis with at least one of the following: a) ischemic symptoms; b) development of pathologic Q waves on the ECG; c) ECG changes indicative of ischemia (ST segment elevation or depression); or d) coronary artery intervention (e.g., coronary angioplasty). 2) Pathologic findings of an acute MI; f) Relapse for patients who are discharged on the initial ED visit. Relapse is defined as a return to the ED for any related medical problem within 14 days, i.e. worsening dyspnea, fever, sepsis, chest pain, inability to ambulate.43 For every suspected relapse we will review the ED health record to determine that the return visit was for a related medical problem.
Hence, adverse events may occur both in patients who are initially admitted to hospital or who are initially discharged from the ED. The simple act of hospital admission does not constitute an adverse event as admission practices may vary from hospital to hospital and may also be influenced by social factors and bed availability. 4.5.2 Outcome Assessment Assessment of the primary outcome measure, adverse event, will be made by research staff, blinded to the patient status for the predictor variables. The following source documents will be used: a) ED health records; b) Hospital health records; c) Computerized hospital patient tracking and record system, available at all participating sites; d) Review of death records from the provincial coroner’s offices. The availability of these data has been assured by representatives of the Coroner’s Offices in Ontario and Medical Examiner’s Office in Alberta (Appendix 1-1). Final determination of adverse event status will be made by a panel of investigators, who will be blinded to the predictor variables of the patients. These physician investigators are specialists in emergency medicine, internal medicine, and respirology. 4.5.3 Secondary Outcome: Preventability The secondary outcome will be determination of whether adverse events were preventable, i.e. could have been avoided. If a patient suffers an adverse event, a research assistant will review the source documents described above (Section 4.5.2) and will extract additional information regarding the event: circumstances surrounding, treatment received by patient, whether the patient responded to the treatment, and the treating physician’s opinion pertaining to the cause of the outcome (if recorded). A blinded case summary will be prepared for the index ED visit. Two physicians will independently review the case summary and make three ratings. First they will rate whether the outcome was related to the same disease process that led to the patient’s index ED visit. Second, they will rate whether the outcome was due to treatment. Third, for cases rated adverse events, they will rate whether it was avoidable. For the purposes of this study, the two physicians must agree. If they disagree, then a third physician will perform the ratings and make a final judgment. 4.6 Data Analysis 4.6.1 Analysis Plan Each major patient cohort, i.e. CHF, COPD, and CAP, will be analyzed separately. Hence, we will develop three separate predictive models for CHF, COPD, and CAP but will use an identical approach for each. For patients with overlapping diagnoses, the panel of investigators will review the cases and attempt to determine the most responsible diagnosis for that

Stiell, Ian G Research Proposal
Research Module, Page 12l
visit. Each predictor variable, including the 3-Minute Walk Test (components and ability to complete) will be evaluated for its univariate association with the primary outcome. Those variables found to be strongly associated with the outcome measure (P < 0.05) will be combined using recursive partitioning. 4.6.2 Univariate Analysis Univariate analyses will be used to determine the strength of association between each variable and the primary outcome. This will aid selection of the best variables for the multivariate analyses. The appropriate univariate technique will be chosen according to the type of data: for nominal data, the chi-square test with continuity correction; for ordinal variables, the Mann-Whitney U test; and, for continuous variables, the unpaired 2-tailed t-test, using pooled or separate variance estimates as appropriate. 4.6.3 Multivariate Analysis Recursive partitioning analyses will derive models to predict the primary outcome, adverse event, as defined in Section 4.5.1, separately for each of the three study cohorts. The objective will be to find the best combinations of predictor variables that are highly sensitive for detecting the outcome measure while achieving the maximum possible specificity. To be clinically acceptable, the model must be nearly 100% sensitive. The derived models must be easy to use by clinicians and should contain as few variables as possible. A model will only be acceptable, therefore, if it fulfils these criteria: a) 99% or greater sensitivity for adverse event, b) highest possible specificity (which ideally leads to reduction in hospital admission), and c) has no more than six component variables. Assuming more than one model meets the minimum acceptable criteria, the best model will be the one which has the highest specificity and the fewest number of component variables. Recursive partitioning will be performed using KnowledgeSEEKER V5 Software (Angoss Software, Toronto).133-136 We have had extensive experience in using recursive partitioning to develop four validated ED clinical decision rules (ankle, knee, cervical spine, and minor head injuries). Our experience suggests that recursive partitioning is much more suitable than logistic regression when the objective is to correctly classify one outcome group at the expense of the other, i.e. where high sensitivity is more important than overall accuracy. Identification of all or most adverse events is the priority of the model building and misclassification of some cases without adverse events will be quite acceptable. We can deliberately drive the analysis to correctly classify the adverse event outcome group at the expense of the group with good outcomes. We can also deliberately avoid complex models with significant interactions that would be difficult for clinicians to interpret or apply. The variables chosen by the best models for each condition will constitute the decision rules for selecting which patients with CHF, COPD, and CAP should be admitted. The decision rules will be presented in clear narrative form that does not require computation or use of statistical aids. A hypothetical example of a decision rule is as follows: "Stable patients with exacerbation of CHF in the ED should be admitted to hospital if they demonstrate any one of these findings: (i) age 80 or greater; (ii) resting heart rate of 100 or greater after ED treatment; (iii) diuresis of less than 250 ml, 4 hours after treatment; or (iv) inability to successfully complete the “3-Minute Walk Test." 4.6.4 Classification Performance The derived rules will be cross-validated by comparing the classification of each patient to their actual status for the primary outcome, adverse event. This will allow an estimate, with 95% confidence intervals, of the sensitivity and specificity of the rules. More robust prospective validations will be carried out on new cohorts of patients in a future phase II study. 4.7 Sample Size 4.7.1 Feasibility Based on pilot studies in Ottawa and Edmonton, we can estimate for each of the CHF, COPD, and CAP patient groups, the number of eligible patients available, current admission rates, and the incidence of adverse events. a) CHF: Table 3 indicates that in a 3-month period at one Ottawa ED site, 77 eligible patients were seen with an admission rate of 38% and an adverse event rate of 29%. Hence, with a projected 50% recruitment rate and extrapolating to 4 sites over 24 months, we can expect to enroll 1,200 patients with 456 adverse events over a 2-year period. b) COPD: Table 3 indicates that in a 3-month period at one Ottawa ED site, 40 eligible patients were seen with an admission rate of 30% and an adverse event rate of 20%. Hence, with a

Stiell, Ian G Research Proposal
Research Module, Page 12m
projected 50% recruitment rate and extrapolating to 4 sites over 24 months, we can expect to enroll 640 patients with 128 adverse events over a 2-year period. c) CAP: From the 1-year patient review at the University of Alberta Hospital site, 364 eligible patients were seen with an admission rate of 75% and an estimated adverse event rate of 16%. Hence, with a projected 50% recruitment rate and extrapolating to 4 sites over 24 months, we can expect to enroll 1,200 patients with 192 adverse events over a 2-year period. 4.7.2 Patients Required We plan to enrol a total of 3,040 patients over the 2-year enrolment period. Since no hypothesis is being tested, sample size is based on estimation of the precision of the sensitivity of the derived rules and on the stability of the multivariate models. The sample size has to accommodate the large number of potential clinical variables and the large number of evaluating physicians. Our primary goal is to enrol sufficient numbers of adverse event cases to be able to develop decision rules with nearly 100% sensitivity and upper and lower limits of the 95% confidence intervals at 100% and 97.0% respectively. The condition with the lowest number of adverse events available is COPD and hence can be considered to drive the recruitment period for this study. A 24-month recruitment period will yield an estimated 128 adverse events for COPD. CHF and COPD will have more adverse event cases and can be expected to have rules with even more precision of sensitivity.
4.8 Methodological Issues 4.8.1 Should We Have Included Both Admitted and Discharged Patients? We have carefully considered the issue of including both admitted and discharged patients in this study. We recognize that that admission status may confound the likelihood of an adverse event occurring. Some admitted patients will not suffer adverse events because they receive more intensive therapy in hospital. In contrast, the same patients might have suffered adverse events if they had been discharged from the ED. Nevertheless, we believe that the best approach is to include admitted patients so that we can adequately address the specificity of the new rules as well as their sensitivity. In other words, our objectives are to develop decision rules that ensure appropriate admission of patients at high risk (i.e. sensitivity) as well as ensuring the admission of a minimal number of patients at low risk (i.e. specificity). In addition, admission practices likely vary considerably among different hospitals and the inclusion criteria for the study would not likely be consistently applied from site to site. 4.8.2 Can We Improve Upon the PORT PSI Criteria for CAP? While the PORT PSI guidelines have been validated, we believe they have significant weaknesses as described in Section 2.3.3. These guidelines were only developed to predict mortality and not important morbidity. Unfortunately, the guidelines are cumbersome, difficult to remember, and do not include variables considered important to emergency physicians. In particular, the PORT PSI does not assess oxygen saturation by pulse oximetry, either at rest or during ambulation. We are confident that we can develop better guidelines. 4.8.3 Should We Have Used “Admission to a Monitored Unit” as an Adverse Event? We recognize that there is a risk that “Admission to a Monitored Unit” as one of the criteria for “Adverse Event” may be somewhat subjective and variable from site to site. Nevertheless, we believe that this is an important criterion that almost always reflects the severity of illness of admitted patients. It is likely that such patients would suffer significant morbidity or death if they had been discharged.
4. Study Organization and Timeline (see budget module) 5. RELEVANCE
In Canada, both patient safety and hospital overcrowding are important healthcare issues. Management of older patients presenting to the ED with acute dyspnea due to CHF, COPD, and CAP is a common problem. This study will develop clinical decision rules for the hospital admission of these patients. We expect these guidelines, once validated, will be widely used and will improve the efficiency of hospital admission practices and will also improve the safety of ED patient disposition decisions. Future research will validate and implement these clinical decision rules. This will ultimately improve and standardize admission practices for these patients, diminishing both unnecessary admissions as well as unsafe discharge decisions.

Stiell, Ian G Research Proposal
Research Module, Page 12n
6. TABLES AND FIGURES Table 1. Characteristics of the 40 ‘3-Minute Walk Test’ Patients with Congestive Heart Failure, Chronic Obstructive Pulmonary Disease, or Stable Chest Pain CHF
(N=16)COPD (N=9)
Chest Pain (N=15)
Overall (N=40)
Mean Age (years) 75 69 63 69 Range 56 – 91 53 – 83 53 – 83 53 – 91Male gender (%) 63 44 67 60 Vitals signs on arrival Temperature (ºC) 36.2 36.7 35.9 36.2 Heart rate (beats/min) 91 89 75 85 Respiratory rate (breaths/min) 20 25 18 20 Systolic blood pressure (mmHg) 147 147 143 146 SaO2 on room air (% sat) 96 96 98 97 Past medical history (%) Coronary artery disease and/or angina 69 22 87 58 CABG and/or PCI 56 22 47 45 Congestive heart failure 100 11 7 45 Hypertension 56 44 53 53 Prior myocardial infarction 44 44 47 45 Chronic obstructive pulmonary disease 0 100 7 25 Lung and/or other cancers 13 11 0 8 Chest X-ray findings (%) Nil acute or normal 13 22 60 32 Congestive heart failure 75 0 0 30 Chronic obstructive pulmonary disease 0 44 0 10 Infiltrate/pneumonia 6 33 0 10 Electrocardiogram findings (%) Nil acute or normal 69 56 87 73 Acute ischemia 6 0 0 3 Atrial fibrillation or flutter 19 0 7 10 Walk test (%) Completed walk test 69 89 100 85 Duration of walk test [mean] (min) 2.8 2.9 3 2.9 Experienced chest pain during test 0 0 0 0 Given nitroglycerin during test 0 0 0 0 Outcome measures (%) Admitted to hospital 25 22 0 15 BiPAP required 0 0 0 0 Intubation required 0 0 0 0 Myocardial infarction 0 11 0 3 Relapse 25 22 0 15 Deceased 0 11 0 3

Stiell, Ian G Research Proposal
Research Module, Page 12o
Table 2. Association of 3-Minute Walk Test Patient Characteristics and Findings with Outcomes
Good Outcome
(N=28)
Adverse Outcome
(N=12) P value
Diagnosis (%) <0.01 Congestive heart failure 29 67 Chronic obstructive pulmonary disease 18 33 Stable chest pain 54 0 Gender – Male (%) 57 67 0.73 Age [mean (range)] (yrs) 69 (53 – 91) 70 (56 – 82) 0.66 Vitals on arrival (mean values) Heart rate (beats/min) 81 94 0.13 Respiratory rate (breaths/min) 20 21 0.43 Systolic blood pressure (mmHg) 149 138 0.30 Diastolic blood pressure (mmHg) 78 76 0.73 SaO2 – room air (N=27:11) 97 95 0.19 Past Medical History (%) Coronary artery disease 46 53 0.73 Coronary artery bypass graft 14 58 <0.01 Angioplasty 29 17 0.69 Chronic obstructive pulmonary disease 21 33 0.45 Congestive heart failure 36 67 0.09 Prior myocardial infarction 36 67 0.09 Lung cancer 4 8 0.52 Support (%) Caregiver at home 54 67 0.50 Cardiologist 36 67 0.09 CXR findings (%) 0.03 Congestive heart failure 21 50 Chronic obstructive pulmonary disease 4 25 Nil acute or normal 39 25 ECG – abnormal findings (%) 18 25 0.49 Walk test results (%) Completed 96 58 <0.01 SaO2 < 90% at 3 minutes 0 25 <0.01

Stiell, Ian G Research Proposal
Research Module, Page 12p
Table 3. Summary of Patient Characteristics and Findings for CHF and COPD Patients seen over 3 Months at Ottawa Hospital Civic Campus ED CHF (N=77) COPD (N=40)Age, mean Range (years)
74.550.4 – 101.6
72.950.6 – 88.2
Gender – Male (%) 64 35Vitals on arrival Temperature (°C) [N=69:39] 36.2 36.6Heart rate (beats/min) [N=73:40] 77 92Respiratory rate (breaths/min) [N=66:34] 23 23Systolic blood pressure (mmHg) [N=75:40] 139 142SaO2 on room air (%) [N=62:30] 96 95History Duration of shortness of breath (days) [N=64:38] 10.3 5.5Emergency Department Medications (%) ACE inhibitor 1 0Angiontensin II receptor blocker 0 0Beta blocker 3 0Calcium channel blocker 1 0Anti-arrhythmic 3 0ASA 4 0Heparin 3 0Coumadin 1 0Diuretic 71 5Vasodilator 8 0Inhaled beta agonist 6 90Inhaled anticholinergic 3 88Inhaled steroid 0 0Oral steroid 0 33Antibiotic 10 23Past medical history Coronary artery disease 49 15COPD 13 100Congestive heart failure 96 25Lung cancer 4 3Other active cancer 3 5Diabetes (type 1) 25 3CXR findings Nil acute 12 35CHF 78 3Infiltrate/pneumonia 5 30COPD 0 15Pleural effusion 3 3ECG findings Nil acute 65 48Abnormal 32 18Outcome Measures (%) Admission on 1st visit 38 30Adverse Event 29 20 BiPAP after admission 3 0 Intubation 1 3 Myocardial infarction 5 0 Relapse 19 15 Deceased 8 5Admitted after relapse (N = 15: 6) 60 33

Stiell, Ian G Research Proposal
Research Module, Page 12q
Figure. Comparison of The 3-Minute Walk Test Results of Patients With and Without
Adverse Outcomes for a) Dyspnea, b) Respiratory Rate, c) Heart Rate, and d) Oxygen Saturation Measurements
0
1
2
3
4
Baseline 1 minute 2 minutes 3 minutes 4 minutes
Time
Mod
ified
Bor
g Sc
ale
No adverse outcome
Adverse outcome(s)
13
14
15
16
17
18
19
20
21
22
Baseline 1 minute 2 minutes 3 minutes 4 minutes
Time
Resp
irato
ry R
ate
(bre
aths
/min
)
Figure a Figure b
70
75
80
85
90
95
Baseline 1 minute 2 minutes 3 minutes 4 minutes
Time
Hear
t Rat
e (b
eats
/min
)
92
93
94
95
96
97
Baseline 1 minute 2 minutes 3 minutes 4 minutes
Time
Oxy
gen
Satu
ratio
n (%
)
Figure c Figure d

Stiell, Ian G Research Proposal
Research Module, Page 12r
7. REFERENCES (1) Canadian Association of Emergency Physicians, National Emergency Nurses Affiliation. Joint position
statement on emergency department overcrowding. Can J Emerg Med 2001; 3(2):82-84.
(2) Forster AJ. An agenda for reducing emergency department crowding (Comment). Ann Emerg Med 2005; 45(5):479-481.
(3) Derlet RW, Richards JR. Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med 2000; 35(1):63-68.
(4) Forster AJ, Stiell IG, Wells GA, Lee AJ, van Walraven C. The effect of hospital occupancy on emergency department length of stay and patient disposition. Acad Emerg Med 2003; 10(2):127-133.
(5) Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA. A conceptual model of emergency department crowding. Ann Emerg Med 2003; 42(2):173-180.
(6) Rowe BH, Bond K, Ospina MB, Blitz S, Friesen C, Schull M et al. Emergency department overcrowding in Canada - what are the issues and what can be done? 2006. Ottawa, Canadian Agency for Drugs and Technologies in Health.
(7) Anonymous. Keeping people out of hospital: the challenge of reducing emergency admissions. Dr Foster
Intelligence 2006.
(8) The Institute of Medicine. To err is human: building a safer health system. 2000. Washington, DC, National Academy Press.
(9) Baker GR, Norton PG, Flintoft V, Blais R, Brown A, Cox J et al. The Canadian Adverse Events Study: the
incidence of adverse events among hospital patients in Canada. Can Med Assoc J 2004; 170(11):1678-1686.
(10) Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ 2001; 322(7285):517-519.
(11) Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The Quality in Australian Health Care Study. Med J Aust 1995; 163(9):458-471.
(12) Thomas EJ, Studdert DM, Burstin HR, Orav EJ, Zeena T, Williams EJ et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care 2000; 38(3):261-271.
(13) Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, Lawthers AG et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. New England Journal of Medicine 1991; 324(6):370-376.
(14) Davis P, Lay-Yee R, Briant R, Ali W, Scott A, Schug S. Adverse events in New Zealand public hospitals I: occurrence and impact. New Zealand Med J 2002; 115(1167):U271.
(15) Forster AJ, Asmis TR, Clark HD, Al Saied G, Code CC, Caughey SC et al. Ottawa Hospital Patient Safety Study: incidence and timing of adverse events in patients admitted to a Canadian teaching hospital. Can Med Assoc J 2004; 170(8):1235-1240.
(16) Forster AJ, Rose NGW, van Walraven C, Stiell IG. Adverse Events Following an Emergency Department Visit. J Quality Patient Safety 2006.
(17) Calder LA, Stiell IG, Forster AJ. Adverse events related to emergency department care (Abstract). Can J Emerg Med 2006; 8(3):180.
(18) Statistics Canada. Statistics Canada 2004.
(19) Tsuyuki RT, Shibata MC, Nilsson C, Hervas-Malo M. Contemporary burden of illness of congestive heart failure in Canada. Can J Cardiol 2003; 19(4):436-438.

Stiell, Ian G Research Proposal
Research Module, Page 12s
(20) Krumholz HM, Parent EM, Tu N, Vaccarino V, Wang Y, Radford MJ et al. Readmission after hospitalization for congestive heart failure among medicare beneficiaries. Arch Intern Med 1997; 157(99):104.
(21) Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE, Carney RM. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. New England Journal of Medicine 1995; 333:1190-1195.
(22) McAlister FA, Lawson FME, Teo KK, Armstrong PW. A systematic review of randomized trials of disease management programs in heart failure. Am J Med 2001; 110:378-384.
(23) Epstein M, Lepp BA, Hoffman DS, Levinson R. Potentiation of furosemide by metolazone in refractory edema. Curr Therapeutic Res 1977; 21(5):656-667.
(24) Ellison DH. The physiologic basis of diuretic synergism: its role in treating diuretic resistance. Ann Intern Med 1991; 114(10):886-894.
(25) Cotter G, Weissgarten J, Metzkor E, Moshkovitz Y, Litinski I, Tavori U et al. Increased toxicity of high-dose furosemide versus low-dose dopamine in the treatment of refractory congestive heart failure. Clin Pharmacol Ther 1997; 62:187-193.
(26) Franciosa JA, Silverstein SR. Hemodynamic effects of nitroprusside and furosemide in left ventricular failure. Clin Pharmacol Ther 1982; 32(1):62-69.
(27) Nieminen MS, Bohm M, Cowie MR, Drexler H, Filippatos GS, Jondeau G et al. Executive summary of the guidelines on the diagnosis and treatment of acute heart failure. Eur Heart J 2005; 26:384-416.
(28) Auble TE, Hsieh M, Gardner W, Cooper GF, Stone RA, McCausland JB. A prediction rule to identify low-risk patients with heart failure. Acad Emerg Med 2005; 12:514-521.
(29) Cowie MR, Wood DA, Coats AJS, Thompson SG, Suresh V, Poole-Wilson PA et al. Survival of patients with a new diagnosis of heart failure: a population based study. Heart 2000; 83:505-510.
(30) Lee DS, Johansen H, Gong Y, Hall RE, Tu JV, Cox JL et al. Regional outcomes of heart failure in Canada. Can J Cardiol 2004; 20(6):599-607.
(31) Sheppard R, Behlouli H, Hugues R, Pilote L. Effect of gender on treatment, resource utilization, and outcomes in congestive heart failure in Quebec, Canada. Am J Cardiol 2005; 95:955-959.
(32) Galofre N, San Vicente L, Gonzalez JA, Planas F, Vila J, Grau J. Predictive factors for readmission in heart failure patients. Med Clin (Barc) 2005; 124(8):285-290.
(33) Tsuyuki RT, Richter CA, Rowe BH. Practice patterns and outcomes in patients presenting to the emergency department with acute heart failure. Can J Cardiol 2005; 21(C):93C.
(34) Brewer AV, Burton JH, Strout TD. Emergency department patients with acutely decompensated congestive heart failure: is discharge a safe disposition? Acad Emerg Med 2003; 10(5):544.
(35) Rame JE, Sheffield MA, Dries DL, Gardner EB, Toto KH, Yancy CW et al. Outcomes after emergency department discharge with a primary diagnosis of heart failure. Am Heart J 2001; 142:714-719.
(36) Lacasse Y, Brooks D, Goldstein RS, for the COPD and Rehabilitation Committee of the Canadian Thoracic Society. Trends in the epidemiology of COPD in Canada, 1980 to 1995. Chest 1999; 116(2):306-313.
(37) Feinleib M, Rosenberg HM, Collins JG, Delozier JE, Pokras R, Chevarley FM. Trends in COPD Morbidity and Mortality in the United States. Am Rev Respir Dis 1989; 140:S9-S18.
(38) American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1995; 152:S77-S120.
(39) Canadian Institute for Health Information, Canadian Lung Association, Health Canada, Statistics Canada. Respiratory Disease in Canada. Respiratory Disease in Canada, editor. 2001. Ottawa, Health Canada.

Stiell, Ian G Research Proposal
Research Module, Page 12t
(40) Seemungal TAR, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1998; 157:1418-1422.
(41) McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2000 Emergency Department Summary. Advance Data from Vital and Health Statistics 2004; 340.
(42) CDC. Chronic Obstructive Pulmonary Disease Surveillance United States 1971-2000. 2000. Atlanta, GA, CDC. (43) Aaron SD, Vandemheen K, Hebert P, Dales R, Stiell IG, Ahuja J et al. Outpatient oral prednisone after
emergency treatment of chronic obstructive pulmonary disease. New England Journal of Medicine 2003; 348:2618-2625.
(44) Mandell LA, Bartlett JG, Dowell SF, File TMJ, Musher DM. Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clinical Infectious Diseases 2003; 37:1405-1453.
(45) Garibaldi RA. Epidemiology of community-acquired respiratory tract infections in adults. Amer J Medicine 1985; 78(S6B):32-37.
(46) Fine MJ, Auble TE, Yealy DM, Hanusa BH, Singer DE, Coley CM et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med 1997; 336(4):243-250.
(47) Marrie TJ, Lau CY, Wheeler SL, Wong CJ, Vandervoort MK, Feagan BG. A controlled trial of a critical pathway for treatment of community-acquired pneumonia. JAMA 2000; 283:749-755.
(48) Carratala J, Fernandez-Sabe N, Ortega L, Castellsague X, Roson B, Dorca J et al. Outpatient care compared with hospitalization for community-acquired pneumonia. Ann Intern Med 2005; 142:165-172.
(49) Marx JA, Hockberger RS, Walls RW. Rosen's Emergency Medicine: concepts and clinical practice. 6th ed. St. Louis: Mosby, 2006.
(50) Marrie TJ, Huang JQ. Low-risk patients admitted with community-acquired pneumonia. Am J Med 2005; 118:1357-1363.
(51) Mandell LA. Decisions about treatment community-acquired pneumonia (Editorial). Ann Intern Med 2005; 142(3):215-216.
(52) Marrie TJ, Huang JQ. Epidemiology of community-acquired pneumonia in Edmonton, Alberta: an emergency department-based study. Can Respir J 2005; 12(3):139-142.
(53) Rowe BH, Blitz S, Campbell S, Clark S, Camargo CAJ. Prospective multicenter study of relapses following emergency department discharge for low-risk pneumonia (Abstract). Acad Emerg Med 2006; 13:S58.
(54) Pozen MW, D'agostino RB, Mitchell JB, Rosenfeld M, Guglielmino JT, Schwartz ML et al. The usefulness of a predictive instrument to reduce inappropriate admissions to the coronary care unit. Ann Intern Med 1980; 92:238-242.
(55) Goldman L, Cook EF, Brand DA. A computer protocol to predict myocardial infarction in emergency department patients with chest pain. N Engl J Med 1988; 318:797-803.
(56) Heckerling PS, Tape TG, Wigston RS. Clinical prediction rule for pulmonary infiltrates. Ann Intern Med 1990; 113:664-670.
(57) Bates DW, Cook EF, Goldman L, Lee TH. Predicting bacteremia in hospitalized patients: a prospectively validated model. Ann Intern Med 1990; 113:495-500.
(58) Wasson JH, Sox HC, Neff RK, Goldman L. Clinical prediction rules: application and methodological standards. N Engl J Med 1985; 313:793-799.

Stiell, Ian G Research Proposal
Research Module, Page 12u
(59) Laupacis A, Sekar N, Stiell IG. Clinical prediction rules: a review and suggested modifications of methodological standards. JAMA 1997; 277:488-494.
(60) Stiell IG, Wells GA. Methodologic standards for the development of clinical decision rules in emergency medicine. Ann Emerg Med 1999; 33:437-447.
(61) Fischl MA, Pitchenik A, Gardner LB. An index predicting relapse and need for hospitalization in patients with acute bronchial asthma. N Engl J Med 1981; 305:783-799.
(62) Rose CC, Murphy JG, Schwartz JS. Performance of an index predicting the response of patients with acute bronchial asthma to intensive emergency department treatment. N Engl J Med 1984; 310:573-577.
(63) Centor RM, Yarbrough B, Wood JP. Inability to predict relapse in acute asthma. N Engl J Med 1984; 310:577-580.
(64) Charlson ME, Ales KL, Simon R, MacKenzie CR. Why predictive indexes perform less well in validation studies. Arch Intern Med 1987; 147:2155-2161.
(65) Poses RM, Cebul RD, Collins M, Fager SS. The importance of disease prevalence in transporting clinical prediction rules: the case of streptococcal pharyngitis. Ann Intern Med 1986; 105:586-591.
(66) Wigton RS, Connor JL, Centor RM. Transportability of a decision rule for the diagnosis of streptococcal pharyngitis. Arch Intern Med 1986; 146:81-83.
(67) Lee TH. Evaluating decision aids: the next painful step. J Gen Intern Med 1990; 5:528-529.
(68) Brophy JM, Deslauriers G, Boucher B, Rouleau JL. The hospital course and short term prognosis of patients presenting to the emergency department with decompensated congestive heart failure. Can J Cardiol 1993; 9(3):219-224.
(69) Fonarow GC, Adams KFJ, Abraham WT, Yancy CW, Boscardin WJ, for the ADHERE Scientific Advisory Committee SGaI. Risk stratification for in-hospital mortality in acutely decompensated heart failure. JAMA 2005; 293(5):572-580.
(70) Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure. JAMA 2003; 290(19):2581-2587.
(71) Januzzi JLJr, Camargo CA, Anwaruddin S, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol 2005; 95:948-954.
(72) Mueller C, Scholer A, Laule-Kilian K, et al. Use of B-type natriuretic peptide in the evaluation and management of acute dyspnea. N Engl J Med 2004; 350:647-654.
(73) Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002; 347:161-167.
(74) Harrison A, Morrison LK, Krishnaswamy P, et al. B-type natriuretic peptide predicts future cardiac events in patients presenting to the emergency department with dyspnea. Ann Emerg Med 2002; 39:131-138.
(75) Murray H, Cload B, Collier CP, Sivilotti MLA. Potential impact of N-terminal pro-BNP testing on the emergency department evaluation of acute dyspnea. Can J Emerg Med 2006; 8(4):251-258.
(76) Hohl CM. Should natriuretic peptide testing be incorporated into emergency medicine practice? (Commentary). Can J Emerg Med 2006; 8(4):259-261.
(77) Kim S, Emerman CL, Cydulka RK, Rowe BH, Clark S, Camargo CAJ et al. Prospective multicenter study of relapse following emergency department treatment of COPD exacerbation. Chest 2004; 125:473-481.
(78) Emerman CL, Effron D, Lukens TW. Spirometric criteria for hospital admission of patients with acute exacerbation of COPD. Chest 1991; 99:595-599.

Stiell, Ian G Research Proposal
Research Module, Page 12v
(79) Emerman CL, Connors AF, Lukens T, Effron D, May ME. Relationship between arterial blood gases and spirometry in acute exacerbations of chronic obstructive pulmonary disease. Ann Emerg Med 1989; 18:523-527.
(80) Emerman CL, Lukens TW, Effron D. Physician estimation of FEV1 in acute exacerbation of COPD. Chest 1994; 105(6):1709-1712.
(81) Emerman CL, Cydulka RK. Use of peak expiratory flow rate in emergency department evaluation of acute exacerbation of chronic obstructive pulmonary disease. Ann Emerg Med 1996; 27(2):159-163.
(82) Black ER, Mushlin AI, Griner PF, Suchman AL, James RL, Jr., Schoch DR. Predicting the need for hospitalization of ambulatory patients with pneumonia. J Gen Intern Med 1991; 6:394-400.
(83) Fine MJ, Smith DN, Singer DE. Hospitalization decision in patients with community-acquired pneumonia: a prospective cohort study. Am J Med 1990; 89:713-721.
(84) Riquelme R, Torres A, El-Ebiary M. Community acquired pneumonia in the elderly. A multivariate analysis of risk and prognostic factors. Am J Respir Crit Care Med 1996; 154:1450-1455.
(85) Ortqvist A, Hedlund J, Grillner L, Jalonen E, Kallings I, Leinonen M et al. Aetiology, outcome and prognostic factors in community-acquired pneumonia requiring hospitalization. Eur Respir J 1990; 3:1105-1113.
(86) Farr BM, Sloman AJ, Fisch MJ. Predicting death in patients hospitalized for community-acquired pneumonia. Ann Intern Med 1991; 115:428-436.
(87) Ewig S, Bauer T, Hasper E, Pizzulli L, Kubini R, Luderitz B. Prognostic analysis and predictive rule for outcome of hospital-treated community-acquired pneumonia. Eur Respir J 1995; 8:392-397.
(88) Neill AM, Martin IR, Anderson R, Chereshsky A, Epton MJ, Jackson R et al. Community acquired pneumonia: aetiology and usefulness of severity criteria on admission. Thorax 1996; 51:1010-1016.
(89) Torres A, Serra-Batlles J, Ferrer A, Jimenez P, Celis R, Cobo E et al. Severe community-acquired pneumonia. Am Rev Respir Dis 1991; 144:312-318.
(90) Moine P, Vercken J-P, Chevret S, Chastang C, Gajdos P, and the French Study Group for Community-Acquired Pneumonia in the Intensive Care Unit. Severe community-acquired pneumonia - etiology, epidemiology, and prognosis factors. Chest 1994; 105(5):1487-1495.
(91) Almirall J, Mesalles E, Klamburg J, Parra O, Agudo A. Prognostic factors of pneumonia requiring admission to the intensive care unit. Chest 1995; 107(2):511-516.
(92) Leroy O, Devos P, Guery B, Georges H, Vandenbussche C, Coffinier C et al. Simplified prediction rule for prognosis of patients with severe community-acquired pneumonia in ICUs. Chest 1999; 116(1):157-165.
(93) Solway S, Brooks D, Lacasse Y, Thomas S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001; 119:256-270.
(94) Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med 1998; 158:1384-1387.
(95) Curtis JP, Rathore SS, Wang Y, Krumholz HM. The association of 6-minute walk performance and outcomes in stable outpatients with heart failure. J Cardiac Failure 2004; 10(1):9-14.
(96) Lama VN, Flaherty KR, Toews GB, Colby TV, Travis WD, Long Q et al. Prognostic value of desaturation during a 6-minute walk test in idiopathic interstitial pneumonia. Am J Respir Crit Care Med 2003; 168:1084-1090.
(97) Sciurba F, Criner GJ, Lee SM, Mohsenifar Z, Shade D, Slivka W et al. Six-minute walk distance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003; 167:1522-1527.
(98) Enright PL. The six-minute walk test. Respir Care 2003; 48(8):783-785.

Stiell, Ian G Research Proposal
Research Module, Page 12w
(99) Enright PL, McBurnie MA, Bittner V, Tracy RP, McNamara R, Arnold A et al. The 6-min walk test - a quick measure of functional status in elderly adults. Chest 2003; 123:387-398.
(100) Brooks D, Parson J, Tran D, Jeng B, Gorczyca B, Newton J et al. The two-minute walk test as a measure of functional capacity in cardiac surgery patients. Arch Phys Med Rehab 2004; 86:1525-1530.
(101) Pan A, Stiell IG, Clement C, Acheson J, Aaron SD. The 3-minute walk test: an investigation into its use as a novel clinical decision tool for patients with congestive heart failure, chronic obstructive pulmonary disease, or stable chest pain. Acad Emerg Med 2006; 13(5):S78.
(102) Pan A, Stiell IG, Clement C. The feasibility of developing novel clinical decision rules for patients with congestive heart failure or chronic obstructive pulmonary disease (Abstract). Can J Emerg Med 2006; 8(3):209.
(103) McGinn TG, Guyatt GH, Wyer PC, Naylor CD, Stiell IG, Richardson WS. Users' guides to the medical literature: XXII: How to use articles about clinical decision rules. JAMA 2000; 284(1):79-84.
(104) McGinn T, Guyatt GH, Wyer PC, Naylor CD, Stiell IG. Users' Guide to the Medical Literature: A Manual for Evidence-Based Clinical Practice. American Medical Association, 2002.
(105) Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Ann Emerg Med 1992; 21:384-390.
(106) Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Reardon M et al. Decision rules for the use of radiography in acute ankle injuries: refinement and prospective validation. JAMA 1993; 269:1127-1132.
(107) Stiell IG, McKnight RD, Greenberg GH, McDowell I, Nair RC, Wells GA et al. Implementation of the Ottawa Ankle Rules. JAMA 1994; 271:827-832.
(108) Stiell IG, Wells G, Laupacis A, Brison R, Verbeek R, Vandemheen K et al. A multicentre trial to introduce clinical decision rules for the use of radiography in acute ankle injuries. Br Med J 1995; 311:594-597.
(109) Anis AH, Stiell IG, Stewart DG, Laupacis A. Cost-effectiveness analysis of the Ottawa Ankle Rules. Ann Emerg Med 1995; 26:422-428.
(110) Graham ID, Stiell IG, Laupacis A, O'Connor AM, Wells GA. Emergency physicians' attitudes toward the use of clinical decision rules for radiography. Acad Emerg Med 1998; 5:134-140.
(111) Graham ID, Stiell IG, Laupacis A, McAuley L, Howell M, Clancy M et al. Awareness and use of the Ottawa ankle and knee rules in 5 countries: Can publication alone be enough to change practice? Ann Emerg Med 2001; 37(3):259-266.
(112) Stiell IG, Greenberg GH, Wells GA, McKnight RD, Cwinn AA, Cacciotti T et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Ann Emerg Med 1995; 26:405-413.
(113) Stiell IG, Greenberg GH, Wells GA, McDowell I, Cwinn AA, Smith NA et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA 1996; 275:611-615.
(114) Stiell IG, Wells GA, Hoag RA, Sivilotti MLA, Cacciotti TF, Verbeek RP et al. Implementation of the Ottawa Knee Rule for the use of radiography in acute knee injuries. JAMA 1997; 278:2075-2078.
(115) Nichol G, Stiell IG, Wells GA, Juergensen LS, Laupacis A. An economic analysis of the Ottawa Knee Rule. Ann Emerg Med 1999; 34:438-447.
(116) Stiell IG, Wells GA, Vandemheen K, Clement C, Lesiuk H, De Maio VJ et al. The Canadian Cervical Spine Radiography Rule for alert and stable trauma patients. JAMA 2001; 286(15):1841-1848.
(117) Stiell IG, Clement C, McKnight RD, Brison R, Schull MJ, Rowe BH et al. The Canadian C-spine Rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med 2003; 349:2510-2518.

Stiell, Ian G Research Proposal
Research Module, Page 12x
(118) Stiell IG, Brehaut JC, Clement C, Grimshaw J, Graham ID, Brison R et al. Implementation of the Canadian C-Spine Rule: prospective 12-center cluster randomized trial with 11,104 patients (Abstract). Acad Emerg Med 2006; 13(5):S78.
(119) Stiell IG, Wells GA, Vandemheen K, Clement C, Lesiuk H, Laupacis A et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001; 357:1391-1396.
(120) Stiell IG, Clement C, Rowe BH, Schull MJ, Brison R, Cass D et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in Patients with Minor Head Injury. JAMA 2005; 294:1151-1518.
(121) The Task Force on Heart Failure of the European Society of Cardiology. Guidelines for the diagnosis of heart failure. Eur Heart J 1995; 16:741-751.
(122) Fraticelli A, Gesuita R, Vespa A, Paciaroni E. Congestive heart failure in the elderly requiring hospital admission. Arch Gerontol Geriatr 1996; 23(3):225-238.
(123) Global Strategy for the Diagnostic Management and Prevention of Chronic Obstructive Pulmonary Disease NWW. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease - Executive Summary. Global Initiative for Chronic Obstructive Lung Disease 2005;1-32.
(124) Aronson D, Mittleman MA, Burger AJ. Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. Am J Med 2004; 116:466-473.
(125) Hsieh M, Auble TE, Yealy DM. Predicting the future: can this patient with acute congestive heart failure be safely discharged from the emergency department? Ann Emerg Med 2002; 39(2):181-189.
(126) Soler JJ, Sanchez L, Roman P, Martinez MA, Perpina M. Risk factors of emergency care and admissions in COPD patients with high consumption of health resources. Respiratory Medicine 2004; 98:318-329.
(127) Roberts CM, Ryland I, Lowe D, Kelly Y, Bucknall CE, Pearson MG et al. Audit of acute admissions of COPD: standards of care and management in the hospital setting. Eur Respir J 2001; 17:343-349.
(128) Ewig S, de Roux A, Bauer T, Garcia E, Mensa J, Niederman M et al. Validation of predictive rules and indices of severity for community acquired pneumonia. Thorax 2004; 59:421-427.
(129) Espana PP, Capelastegui A, Quintana JM, Soto A, Gorordo I, Garcia-Urbaneja M et al. A prediction rule to identify allocation of inpatient care in community-acquired pneumonia. Eur Respir J 2003; 21:695-701.
(130) Kendrick KR, Baxi SC, Smith RM. Usefulness of the modified 0-10 Borg Scale in assessing the degree of dyspnea in patients with COPD and asthma. J Emergency Nursing 2000; 26(30):216-222.
(131) Gillum RF, Fortmann SP, Prineas RJ, Kottke TE. International diagnostic criteria for acute myocardial infarction and acute stroke. Am Heart J 1984; 108:150-158.
(132) Alpert JS, Thygesen K, Antman E, Bassan JP. Myocardial infarction redefined - a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Card 2000; 36:959-969.
(133) Friedman JH. A recursive partitioning decision rule for nonparametric classification. IEEE Trans Comput 1977; 16:404-408.
(134) Ciampi A, Thiffault J, Nakache J-P, Asselain B. Stratification by stepwise regression, correspondence analysis and recursive partition: a comparison of three methods of analysis for survival data with covariates. Comput Stat Data Anal 1986; 4:185-204.
(135) Ciampi A, Chang CH, Hogg S, McKinney S. Recursive partition: a versatile method for exploratory data analysis in biostatistics. In: MacNeill IB, Umphrey GJ, editors. Time series and econometric modelling / Biostatistics Vol. V. Boston: D. Reidel Publishing Company, 1987: 23-50.

Stiell, Ian G Research Proposal
Research Module, Page 12y
(136) Ciampi A, Hogg SA, McKinney S, Thiffault J. RECPAM: a computer program for recursive partition and amalgamation for censored survival data and other situations frequently occurring in biostatistics. I. Methods and program features. Comput Meth Prog Biomed 1988; 26:239-256.