Embed Size (px)
Citation preview

a study on the ICDS
and Child Survival issues in Madhya Pradesh
a study on the ICDS
and Child Survival issues in Madhya Pradesh
Sanket - Centre for Budget Studies, Vikas Samvad&
Right to Food Campaign Madhya Pradesh Support Group
Moribund ICDS(a study on the ICDS and Child Survival issues in Madhya Pradesh)
Vikas Samvad
Sanket - Center for Budget Studies
Printed by -
Design and layout -
Moribund ICDS(a study on the ICDS and Child Survival issues in Madhya Pradesh)
Analysis & Report Writing
Vikas SamvadE-7/226, Ist Floor, Opp Dhanvantri Complex, Arera Colony, Shahpura, Bhopal, MPPhone 0755 4252789, email - [email protected], web - www.mediaforrights.org
Sanket - Center for Budget Studies E-2/141, Arera Colony, Bhopal, MP. Phone 0755 2468050
Published by - Right to Food Campaign Madhya Pradesh Support Group, Vikas Samvad and Sanket-Centre for Budget Studies, Bhopal
Data collection and field support Spandan (Khandwa), Saheriya Mukti Morcha (Sheopur), Adiwasi Adhikar Manch (Satna), Manav Adhikar Forum (Shivpuri), Sanket (Bhopal), Lok Jagruti Manch (Jhabua), Bundelkhand Janutthan Samiti (Tikamgarh), Patthar Khadan Majdur Sangh (Panna), Community Development Center (Balaghat), Dalit Sangh (Hoshangabad), Adiwasi Susashan Sangh (Seoni), Abhar Mahila Samiti (Chhatarpur) and NIWCYD-Bachpan (Bhopal).
Year of Publication - 2009
Printed Copies - 1000
Declaration - This study is resulted out of joint efforts by different NGOs, alliances and CSOs working intensively for recognizing children's right to food, survival and nutrition across the State.
We are deeply indebted to Child Rights and You (CRY), Action Aid, UNICEF and MDG Campaign of UNDP for supporting us in building hypothesis, data collection, editing, designing and giving a final shape to the study.
The views and analysis presented in the study is the responsibility are of publishers. Publishers do not claim any copyright to this report and any part of it may be used or quoted with the due credit.
Printed by - MSP Offset, Bhopal
Design and layout - Amit Saxena
Suggested Contribution - Rs. 100.00
Malnutrition and food insecurity amongst the children has turned out death-defying owing to the
threatening fact that we have denied them their most basic right to sustain in the life. We the adult
people with strong mind and energy understand what our rights are even know very well to
demonstrate as and when needed. The children's right to health and nutrition has been out of the
democratic political framework of development for uncounted years. This reality has not given the
due respect at par with the human rights. May be for few intellectuals it is a technical issue but
considering its social implications it is one of the thought provoking and burning issue. But in the long
run it has severe repercussions related to overall growth and development of child to be a healthy
citizen; hence important from social context. It is this 44 percent proportion of population who
sacrifices basic human rights in the name of development and growth and occasionally faces
gender, caste and religion based discrimination.
The fourth goal of the Millennium Development Goals declared by United Nations is to reduce
mortality rate of children below 5 years age by two third till 2015 from the position of 1990. It is just not
possible to achieve the said goal unless and until the issue of child mortality is brought forward and
debated on the greater social and political platforms. EVEN THEN WE DO NOT HAVE EITHER A
CHILD HEALTH POLICY OR A LEGAL FRAMEWORK DEFINING THE CHILDREN'S RIGHT TO
HEALTH AND NUTRITION!!
Pace of growth based economic development process is so fast, that the common person is left
behind as if not in the existence. On one hand when the economy of the state is glimmering with rising
GDP on the other hand one out of every two children in the Madhya Pradesh succumbs to
malnutrition. It is not just a coincidence that Madhya Pradesh scores the top position for highest
Infant Mortality Rate (IMR), lowest life expectancy of 57.7 years in comparison to Indian average of
63.2 years and also staying top in list of Indian states with more than 60 percent malnutrition among
children under the age of 5 years. Alarmingly, the situation is critical among the tribal children where th140 out of every thousand live births dies before celebrating their 5 birthday. The world is renowned
medical research journal “The Lancet” establishes that the death chances due to diseases like
diarrhea, measles and malaria for a malnourished child increases 9 to 18 folds as compared to a
normal child. WHO and UNICEF also unanimously agree that malnutrition is the major killer of
children less than five years in age. Thus it is crystal clear fact that malnutrition is biggest challenge
before the state government and ignoring it will lead the state into a dark and hopeless tunnel with no
scope to revert back.
Nearly 12 million (16%) of the population in Madhya Pradesh is below six years age, needs health,
nutrition and development care. However, budgetary allocation for this section is just Rs 156 crore in
the health and Rs 325 crore in ICDS which comes out to Rs. 400 per child per year only. The past 35
years of experiences of Integrated Child Development Scheme (ICDS) are indicating many shortfalls
on the account of convergence and coordination among implementing government departments.
The issues of starvation and children deaths are directly related with the community but no efforts
had been yet done to promote and ensure the community's participation in tackling these menaces.
Instead, administration engages itself in hiding the truth of increasing malnutrition among children
deaths thereby by manipulating facts and figures.
P R E F A C E

Perhaps, Tamilnadu is the only state in India that has linked malnutrition not only with poor health
services but also with the poor conditions of poverty, hunger and social exclusion spread in the
society. It has taken the challenge to eradicate malnutrition and adopted Integrated Life Cycle
Nutrition Security Programme by earning community participation to overcome the problem.
Also, one can not ignore the truth that 6.6 million households in the state are surviving below poverty
line. These households are unable to live their life without the state support. Moreover still more than
half the districts of Madhya Pradesh are lacking the basic health services and infrastructure facilities.
Painfully, still majority population in the state is not prepared enough to face pro-market and pro-
capitalist economy. Thus, emphasizing greater need for responsible role of the state government in
addressing the issue.
In fact, ground reality of ICDS implementation is too dismal. Considering the severity of the problem
of persisting malnutrition in the state, it is lacking more than 40, 000 anganwadi centres at present.
Many of the centers lack regular supply of supplementary nutrition food, growth registers, weighing
machines, playing kits, medicine kits, and drinking water facility. Besides, anganwadi workers are not
getting their remuneration timely but showing the long time lag from 7 to 14 months.
It is evident from the above facts that it's high time to neglect the crucial issue like malnutrition among
the children of our state considering its social repercussions in the long run. It is therefore we are
urging all the civil society organizations to take note of the things and try to join hands to step firm
steps for the welfare of our children before it's too late. It is with this conviction we should make the
state government realized that we can survive without four lane roadways, multinational companies
and big commercial malls but our children cannot survive without nutritious food and proper health
services. It is for this the network and service delivery mechanism of ICDS should be made most
effective and efficient in the state.
This study has been prepared by Right to Food Campaign Madhya Pradesh Support Group and
Sanket Center for Budget Studies and Initiative of Sanket Development Group. But it would not have
completed without the kind help and co-operation and throughout involvement of our small group.
We are very grateful to all NGOs, alliances and CSOs across Madhya Pradesh for their support in
data collection and information from the field. The list of all the organization that has helped us our
endeavor is as follows :
Spandan (Khandwa), Saheriya Mukti Morcha (Sheopur), Adiwasi Adhikar Manch (Satna), Manav
Adhikar Forum (Shivpuri), Sanket Development Group (Bhopal), Lok Jagruti Manch (Jhabua),
Bundelkhand Janutthan Samiti (Tikamgarh), Patthar Khadan Majdur Sangh (Panna), Community
Development Center (Balaghat), Spandan Samaj Sevi Sanstha (Khandwa), Dalit Sangh
(Hoshangabad), Adiwasi Sushasan Sangh (Seoni), Abhar Mahila Samiti (Chhatarpur) NIWCYD-
Bachpan (Bhopal), and Madhya Pradesh Lok Sangarsh Saajha Manch.
We thank our contributors namely, Smriti, Seema Prakash, Prashant Dubey, Sachin Kumar Jain,
Rolly Shivhare, Sanjay Shrivastava and Pallavi K. Mali for putting immense hard work in analyzing
both primary and secondary data and then undertaking the report writing work. We also appreciate
Ms Pallavi for her efforts in undertaking the editing of this document.
MPRTFCSG & Sanket
A Executive Summary 1
B Hunger in Indian states is alarming 5
1. Basic Human Development Indicators 6
2. Key facts about Madhya Pradesh 7
1. Child Malnutrition-A Catastrophe in Madhya Pradesh 10
1.1 A Close Encounter 10
1.2 Malnutrition in Madhya Pradesh- Stories directly from the field 13
1.3 Health Status in Madhya Pradesh 20
1.4 Health Infrastructures 20
1.5 Far behind from GOALS 22
1.6 Status of Health Facilities 23
1.7 Accessibility to Health System 24
2. Integrated Child Development Services 26
2.1 Implementation process of ICDS 26
2.2 Services provided under ICDS 26
2.3 Population covered under an AWC 28
2.4 The Truth of Universalisation of ICDS 29
2.5 Status of ICDS in Madhya Pradesh 30
2.6 Allocation for Travel and Fuel 30
2.7 No more Medicine Kits ICDS 31
2.8 What is a Medicine Kit in ICDS? 31
2.9 Provision of Budget 32
2.10 Growth charts vs. Monitoring of growth 32
2.11 Field realities 33
2.12 Nutrition component testing 34
2.13 Targeted population Vs Actual coverage 34
2.14 Human Resources: Vacant posts, a bitter truth 34
2.15 Nutritional Rehabilitation Centers 36
2.16 Few more observations based on the Rapid Assessment Study of NRC 37
2.17 Bal Sanjeevni Abhiyan 38
2.18 Targeted Public Distribution System in MP 39
2.19 Midday Meal Scheme 39
D XIN E
3. Ground Realities of ICDS - A Field Study 413.1 Infrastructure of Anganwadi Centers 41
3.2 Exclusion of deprived sections 41
3.3 Functioning days of Anganwadi Centers 42
3.4 Toilet Facility 42
3.5 Drinking Water Facility 43
3.6 Availability of Supplementary Nutritious Food 43
3.7 Quality of Supplementary Food 44
3.8 Availability of Hot Cooked Meal 44
3.9 Relishing (Ruchikar) of Supplementary Food 45
3.10 Availability of Utensils 45
3.11 Availability of Playing Kits (Pre-School Education Kit) 45
3.12 Availability of Medicinal Kit 46
3.13 Growth Monitoring 47
3.14 Pre-School Education 48
3.15 Hot Cooked Meal Vs. Packaged Food 49
3.16 Conclusions of Field Study 50
4. Denial by State: Biggest Challenge for Child Survival 53
4.1 Children in Denial and Negligence Vs World's best child 55
survival in records in MP
5. Nutrition Policies Questioned 57
5.1 Importance of Cooked Meal over Packaged Foods 58
6. Judicial Interventions in ICDS 60
6.1 Supreme Court Orders in ICDS 60
6.2 Steps of High Court of Madhya Pradesh in ICDS 61
6.3 Orders of Supreme Court - Violation Continues 61
7. Budget Analysis of Supplementary Nutrition Programme : 65A Deteriorating Condition
7.1 Growth of Children in MP 65
7.2 The Coverage under Nutrition Programme 66
7.3 Universalization of ICDS : A Legal Obligation 66
7.4 Resource Gap Analysis in the context of Universalization of ICDS 67
7.5 Response of the State Government through Budget Allocations 69
7.6 Budget Estimate and Actual Expenditure for SNP 70
7.7 Budget Utilization 70
7.8 ICDS in Budget Books 71

7.9 Latest Addition 72
7.10 Criticism by Comptroller and Auditor General (CAG) 72
8. Exceptions are always there… 73
8.1 Balaghat - A district paving its own way 73
8.2 Mai's local initiative for Child Protection in Khandwa 76
9. Strategies for Children under Six 79
A. Comprehensive Strategies 79
B. Strategies for the treatment of SAM 83
Boxes
01 Malnutrition in south Asia 5
02 Hunger in Indian States 6
03 Dance of Deaths 8
04 Joint Statement by UNICEF, WHO and UNSSCN 10
05 Distant Goals 12
06 Dilution of Supreme Court's Orders 16
07 A Complex Life 17
08 End begins from beginning 19
09 Losing Faith in System 21
10 An Eye Opener 22
11 Key facts about Maternal Health from NHFS-3 Statistics 29
12 Budget of NRC 36
13 Reality Bites 38
14 Ground Zero: Sidhi, a place on the brink of negligence 50
15 Denial mode on starvation deaths 54
16 Supreme Court Orders on ICDS 62
Tables
01 Health budget of Madhya Pradesh government
02 Total number of Health Institutions in MP
03 Available and required number of Health Institutions in MP
04 Available and Required number of Health workers in MP
05 Criteria for Anganwadi Centers
06 Nutritional Entitlements
07 Budget for Medicine Kit
08 Status of Growth charts in Madhya Pradesh
09 Available and Required numbers of CDPO/ACDPO/Supervisors in AWC
10 Infrastructure at Anganwadi centers
11 Functioning days of Anganwadi Centers
12 Toilet facility in AWC
13 Drinking Water Facility in AWC
14 Availability of Supp. Nutrition in AWC
15 Quality of Nutritious Food
16 Availability of Hot cooked meal in AWC
17 Relishness of SNF in AWC
18 Utensils availability in AWC
19 Availability of Playing Kit
20 Availability of Medical Kit
21 Availability of Salter machine
22 Availability of Adult weighing machines
23 Availability of Growth Monitoring Register
24 Pre-school education facility
25 Willingness to packaged food
26 Non-reporting of Infant deaths
27 Infant Mortality in MP-Far from comparison
28 Status of Malnutrition in MP
29 Growth indicators expressed as a percentage
30 Gap between the required number of anganwadi centres andthe sanctioned one
31 Resource Gap
32 Budget Allocations for Special Nutrition Programme
33 Allocations for Supplementary Nutrition
34 Budgets of ICDS
Annexure I 86
Annexure II 88
Annexure III 91
Annexure IV 100

Today malnutrition in the State of Madhya
Pradesh is not only recognized as a biggest
blight for the small children but the political
parties are also coming out with special
promises in there manifestoes to save the
future generation from malnutrition. Deaths
of innocent children across the state and
continuous negligence of administration
towards these deaths has spurt out the
urgent need for bringing positive changes
and generating demands for the benefit
poor and marginalized section. It would be
possible through bringing attitudinal
change on part of the health of children and
winning faith of the community, specifically
the rural and tribal folks, as well as making
the state administration more accountable
on this serious issue.
Both NFHS and IFPRI reports have
indicated the poor status of nutrition and
health services specifically of women and
children in the state of Madhya Pradesh.
However, state government through its
statistics presenting the incorrect picture of
malnutrition status in the state. The study
findings clearly shows that ICDS which is
the only scheme for addressing needs and
rights of children under six is not efficiently
implementing in the state. Besides the
orders of Supreme Court, to universalize
the ICDS; scheme it is not effective in terms
of low proportion of coverage of preg-
nant/lactating women and almost nil
coverage of adolescent girls of age group
11-18 as the beneficiaries.
Health Services
The health services available in the state
are also depicting threatening fact that
most of needed persons are left without any
benefits of the facilities. State records for
highest infant mortality rate (72), second
highest in maternal mortality rate (379) and
about 60 percent children below six years
of age are under weight. The reach of
health and nutrition can be understood by
the fact that only 22 percent of the children
have received all vaccinations before 12
months and only 25 percent of children in
the age group 6-35 months received at
least one dose of Vitamin 'A'. Health
budgets has shown sharp decline as a
proportion to total expenditure from 5.1
percent in 2000-01 to 3.9 percent in 2008-
09. The public health infrastructure in the
state is far from satisfactory. The state is
lacking 1614 SHCs, 1625 PHCs and 128
CHCs. Shortfall of manpower is also a big
problem. Furthermore, the accessibility to
the health institutions is also in a dwindling
condition due to poor quality of care (62.9
percent), no nearby facility (50.8 percent),
long waiting hours (26.4 percent),
inconvenient timings (10.0 percent), health
personnel often absent (7.7 percent) and
other reason (1.6 percent) according to
NFHS III.
ICDS Services - Field study results
An action study was attempted to check out
the status of ICDS in 65 Anganwadi centres
from 12 blocks in 10 districts of the State.
Following issues in emerged about the
status of ICDS from the field :-
l Though the orders of Supreme Court
stated that the universalization of the
ICDS and providing all the 7 services
to all its beneficiaries is mandatory but
Executive Summary
"A"
Moribund ICDS01
the latest report from DWCD shows
that still 60 percent children and more
than 73 percent eligible women
beneficiaries are out of the focus.
l Exclusion of children and women from
ICDS services on the basis of caste
and community is also prevalent in the
state due to which a vast section of
tribal and dalit communities are kept
deprived of the facilities. The matter of
exclusion observed in Chhatarpur
district was worst compared to other 9
districts included in the study.
l Most of the anganwadi centres across
the state are lacking their own
buildings, the most vital requirement
to provide a safe, secure and
spacious environment for children. It
was observed that out of 65 centers
studied only 37 percent anganwadis
are having their own building.
l Supreme Court has strictly ordered
that each and every anganwadi centre
must open and provide the basic
services to its beneficiaries for 300
days annually. But in practice most of
the anganwadi centres were not found
functional as per the order, thus
violating the orders of Supreme Court.
The study revealed that out of the
studied centers only 43 percent
anganwadi centres were providing
services for 26 days a month which is
in accordance to the orders of
Supreme Court. While rest of the
centres were providing services either
for 21 days (40 percent), 15 days (15
percent). Two percent centers are
providing services only for 7 days in a
month.
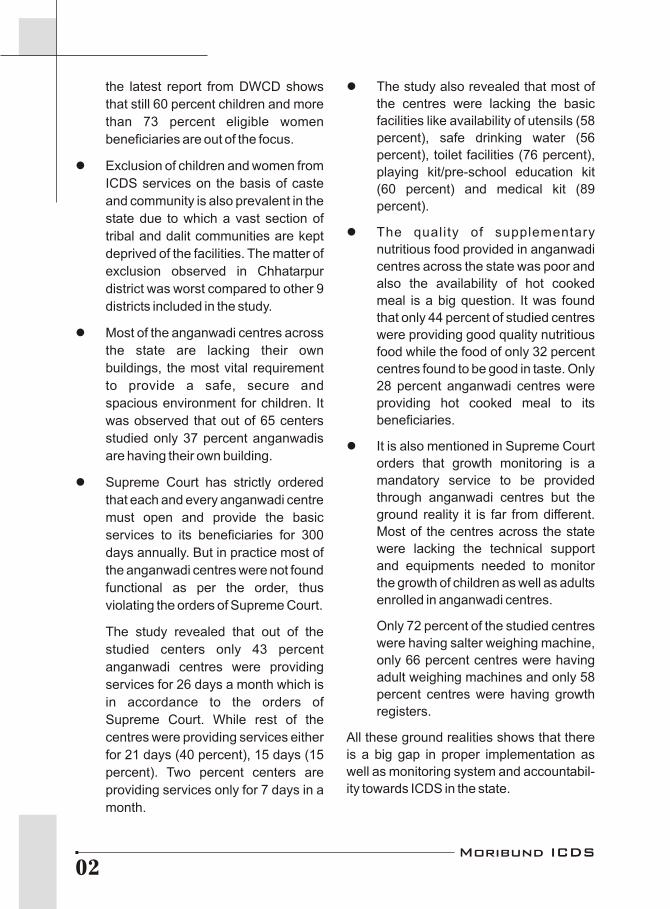
l The study also revealed that most of
the centres were lacking the basic
facilities like availability of utensils (58
percent), safe drinking water (56
percent), toilet facilities (76 percent),
playing kit/pre-school education kit
(60 percent) and medical kit (89
percent).
l The quality of supplementary
nutritious food provided in anganwadi
centres across the state was poor and
also the availability of hot cooked
meal is a big question. It was found
that only 44 percent of studied centres
were providing good quality nutritious
food while the food of only 32 percent
centres found to be good in taste. Only
28 percent anganwadi centres were
providing hot cooked meal to its
beneficiaries.
l It is also mentioned in Supreme Court
orders that growth monitoring is a
mandatory service to be provided
through anganwadi centres but the
ground reality it is far from different.
Most of the centres across the state
were lacking the technical support
and equipments needed to monitor
the growth of children as well as adults
enrolled in anganwadi centres.
Only 72 percent of the studied centres
were having salter weighing machine,
only 66 percent centres were having
adult weighing machines and only 58
percent centres were having growth
registers.
All these ground realities shows that there
is a big gap in proper implementation as
well as monitoring system and accountabil-
ity towards ICDS in the state.
Moribund ICDS02

Shortage of field staff
At present, there are 367 Child
Development Projects are sanctioned by
Government of India (GoI) in Madhya
Pradesh. Under these projects 69238
anaganwadi centres have been sanctioned.
Through 67770 functional anagan-wadi
centres 'Supplementary Nutr i t ion
Programme' is being currently imple-
mented in the state. The programme is
serving around 5340498 beneficiaries. To
look after such a vast number of ICDS
projects covering a noticeable number of
beneficiaries only 290 CDPOs, 46
ACDPOs and 2538 Supervisors have been
appointed till date. While 76 posts of CDPO,
69 posts of ACDPOs and 200 posts of
Supervisors are still vacant. Going with the
given situation one CDPO is responsible for
managing about 189 anganwadi centres.
Thus one can imagine about the quality of
ICDS services being provided in such a
scarce and lacking situation.
NRCs and Bal Sanjeevni Abhiyaan
These two are the programs that are run by
the state government to tackle the
occurrence of malnutrition among young
children but the government has failed to
assure the authenticity of these vital
programs. There are only 135 NRCs in the
State to take care of 13 lakh severely
malnourished children. Moreover out of
these NRCs only 95 centres are fully
functional while 40 are partially functional.
The budget allocated for these NRCs is
also not sufficient to provide proper care
and treatment to the malnourished children.
Similarly, the State is claiming that level of
malnutrition has decreased as per the data
of Bal Sanjeevni Abhiyan but the reality is
that the level of malnutrition is continuously
increasing in the state, if one goes by NFHS
statistics.
Packaged food and hot cooked meal
The field study shows that due to socio-
cultural and sustainability reasons
community is not in the favor of packaged
food. Around 90 percent of the respondents
oppose the use of packaged food in
anganwadi centers and feel that locally
made, prepared and supplied food should
be made available.
There has always been a debate over hot
cooked meal being replaced by commer-
cial/packaged food. The administration is in
strong support of allocating packaged food
claiming that packaged food (supple-
mented with micronutrients) is more
nutritious and safe than hot cooked meal
and more effective in reducing the malnutri-
tion level in state. While many nutritionists
and activists are of the view that hot cooked
meal can not be replaced with any kind of
micronutrient supplemented packaged
meals. It has been proved through various
studies that hot cooked meal is more
nutritious than packaged food and the
chances of contamination are also less in
case of hot cooked meal than packaged
food. Hot cooked meal is the traditional
food and the children enjoy the traditional
food much as compared to any packaged,
non-traditional food. Also, the quality,
sustainability and regular availability of
packaged food are quite in question
whereas hot cooked meals are sustainable
and its regular availability can also be
assured. All this simply put forth the
importance of hot cooked meal.
Though RUTF is a therapeutic food to
tackle the severe acute malnutrition; its
impact has not been tested in the context of
Moribund ICDS03

Indian population. Further it would promote
the commercialization as well privatization
of food allocating practices which is again
the violation of the orders of Apex Court,
which states decentralized process must
be adopted to distribute supplementary
food in anganwadi centres.
Budget of ICDS
The claims of spending of Rs. 2 per
beneficiary is the key statement in all the
responses released from the State
Government. But when the implementation
and coverage analysis in terms of budget
provision was done, it is found that only Rs.
0.84 per beneficiary have been allocated in
Madhya Pradesh. Even if we believe that
Government has spent Rs. 2 per
beneficiary per day in this budget, then it
means all the covered (not actual
populat ion) beneficiar ies wi l l get
Supplementary Nutrition for 126 days in a
year, whereas it should have been for at
least 300 days in a year, as per the
Supreme Court order. Even after the four
years of Supreme Courts orders the budget
allocation are not proportionate to the
needs of beneficiaries.
Moribund ICDS04

On the count of Global Hunger Index (GHI), hunger is a major threat in 33 countries says a report developed by US-based, International Food Policy Research Institute (IFPRI) in 2008. Situation in these countries is either alarming or extremely alarming and world's progress in hunger reduction since 1990 has been slow. The index shows that South Asia and Sub-Saharan Africa continue to suffer from high levels of hunger. On one hand where South Asia has made rapid progress in combating hunger, Sub-Saharan Africa has made only marginal progress. GHI uses a multidimensional approach that gives a very comprehensive picture of hunger in developing and transitional countries. GHI measures hunger on the basis of three indicators namely child malnutrition, rates of child mortality and the number of people who are calorie deficient. The problem of hunger is measured in five categories like low, moderate, serious, alarming or extremely alarming.
India's GHI 2008 score is 23.7 with thranking at 66 position out of 88 countries.
It is slightly better over previous year thscore of 25.03 and 94 rank out of 118
countries in 2007. These scores indicate towards little efforts made in curbing h u n g e r a n d p o v e r t y i n I n d i a . Neighbouring countries like Pakistan, Sri Lanka and Nepal have faired better than India in the GHI list. With more than 200 million food-insecure people (FAO 2008), India is home to the largest number of hungry people in the world. India is long known to have some of the highest rates of child malnutrition and mortality in under-fives in the world. This situation is a consequence of very long neglect of agriculture; one of the heavily dependent sector for livelihood for people in the country in the opinion of Mr. Yoginder K. Alagh, author of India's poverty line and former planning minister.
'Scored Worse'
Twelve Indian states have "alarming" levels of hunger while the situation is "extremely alarming" in the state of Madhya Pradesh, says the above report.
The India State Hunger Index (ISHI) 2008 was constructed in a similar fashion as the GHI 2008 to allow for comparisons of states within India and for comparisons of Indian states to GHI 2008 scores and ranks for other countries. The ISHI 2008 score was estimated for 17
1Hunger in Indian states is 'alarming'
"B"
Malnutrition inSouth Asia
In South Asia, the major problem is a high prevalence of child malnutrition, which stems from the lower nutritional and educational status of women, as well as poorly designed and poorly implemented nutrition and health programs and inadequate water and sanitation services. In contrast, the high GHI in Sub-Saharan Africa is due to high child mortality and a high proportion of people who cannot meet their ca lor ie requ i rements . Low government effectiveness, conflict, and political instability, and high rates of HIV/AIDS, have driven these two indicators.
Box - 1
1Story from BBC NEWS:http://news.bbc.co.uk/go/pr/fr/-/2/hi/south_asia/7669152.stm,
Published: 2008/10/14 12:24:13 GMT
Moribund ICDS05
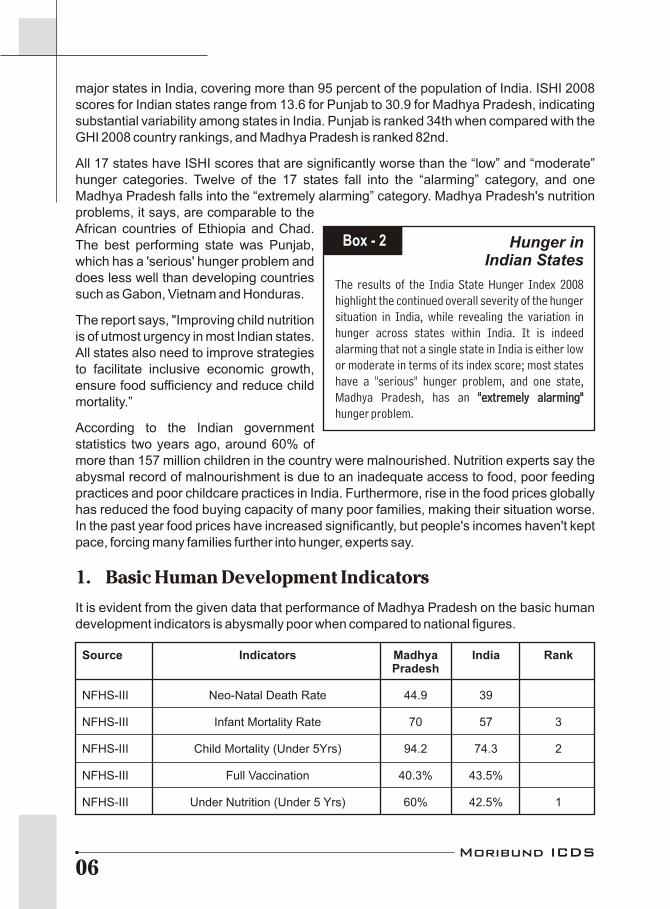
major states in India, covering more than 95 percent of the population of India. ISHI 2008 scores for Indian states range from 13.6 for Punjab to 30.9 for Madhya Pradesh, indicating substantial variability among states in India. Punjab is ranked 34th when compared with the GHI 2008 country rankings, and Madhya Pradesh is ranked 82nd.
All 17 states have ISHI scores that are significantly worse than the “low” and “moderate” hunger categories. Twelve of the 17 states fall into the “alarming” category, and one Madhya Pradesh falls into the “extremely alarming” category. Madhya Pradesh's nutrition problems, it says, are comparable to the African countries of Ethiopia and Chad. The best performing state was Punjab, which has a 'serious' hunger problem and does less well than developing countries such as Gabon, Vietnam and Honduras.
The report says, "Improving child nutrition is of utmost urgency in most Indian states. All states also need to improve strategies to facilitate inclusive economic growth, ensure food sufficiency and reduce child mortality.”
According to the Indian government statistics two years ago, around 60% of more than 157 million children in the country were malnourished. Nutrition experts say the abysmal record of malnourishment is due to an inadequate access to food, poor feeding practices and poor childcare practices in India. Furthermore, rise in the food prices globally has reduced the food buying capacity of many poor families, making their situation worse. In the past year food prices have increased significantly, but people's incomes haven't kept pace, forcing many families further into hunger, experts say.
1. Basic Human Development Indicators
It is evident from the given data that performance of Madhya Pradesh on the basic human development indicators is abysmally poor when compared to national figures.
"extremely alarming"
Hunger inIndian States
The results of the India State Hunger Index 2008 highlight the continued overall severity of the hunger situation in India, while revealing the variation in hunger across states within India. It is indeed alarming that not a single state in India is either low or moderate in terms of its index score; most states have a "serious" hunger problem, and one state, Madhya Pradesh, has an "extremely alarming" hunger problem.
Box - 2
Source Indicators Madhya India RankPradesh
NFHS-III Neo-Natal Death Rate 44.9 39
NFHS-III Infant Mortality Rate 70 57 3
NFHS-III Child Mortality (Under 5Yrs) 94.2 74.3 2
NFHS-III Full Vaccination 40.3% 43.5%
NFHS-III Under Nutrition (Under 5 Yrs) 60% 42.5% 1
Moribund ICDS06

2Source - http://www.health.mp.gov.in/bulletin (as accessed on 30th April 09)
Source Indicators Madhya India RankPradesh
NFHS-III Severe Malnutrition (-3SD) 27.3% 15.80%
NFHS-III Breast feeding within one hour of Birth 15.9% 25%
NFHS-III Anemia among children 74.1% 69.5% 2(under the age of 5 years)
Economic Below Poverty Line (BPL) Families 38.3% 27.5% 5Survey(2007-08)
Economic MPCE (Monthly per Capita Expenditure) Rs. 439.06 Rs. 559 4 (low Survey (Rural) (Rural) expenditure)(2007-08) Rs. 903.68 Rs.1052
(Urban) (Urban)
Economic Life Expectancy (Average age) 57.7 Years 63.2 Years Lowest inSurvey the country(2007-08)
Government Maternal Mortality Rate 379/ 100000 301 3of India live births
rdEconomic Literacy (Census 2001) 63.74% 64.64% 23 rank inSurvey India(2007-08)
2. Key facts about Madhya Pradesh
Threatening truth of malnutrition
l Infant Mortality Rate (IMR) is highest in Madhya Pradesh at 72 deaths per 1000 live births as per Sample Registration Survey (SRS) 2007 released in October 2008.
l In Madhya Pradesh nearly One lakh eighteen thousand children of one year age have 2lost their lives during the period from April 2005 to March 2009 .
l According to National Family Health Survey (NFHS) III, Madhya Pradesh tops the list of undernourished state with 60 percent children suffering from malnutrition indicating less opportunity for the children in terms of overall health and development in their life span.
l Only 40.3 percent children in the state are fully immunized, merely 14.7 percent children are breast fed within half an hour of birth and only 15.9 percent children are breast fed within one hour of birth in the state according to NFHS-III findings.
Moribund ICDS07
l Severe malnutrition among children (below 3SD level) is highest in Madhya Pradesh. Around 12.6 percent children in the state are on the verge of death by being thin, low weight, weak and sick compared to 6.4 percent in India. It means nearly 13 lakh 35 thousand children in the state have 30 percent more chances of death.
Reality of Integrated Child Development Services (ICDS) in the state
l ICDS is the one and only scheme catering the needs for the population below six years that constitute for nearly 16 percent of the total population.
l Till date only 69,238 Anganwadi centres are in existence under ICDS against the huge need of 1.46 lakhs. Government is reaching only three fourth or 76.51 percent of the malnourished children in the state going by its own statistics and leaving around one fourth malnourished children out of the coverage of ICDS.
l As far as universalization of ICDS is concerned the coverage turns out to only 36.58 percent for the children in the age group 0-6.
l State government's coverage of total expectant and lactating mothers under ICDS is merely 9.5 lakhs that is just 30 percent of the eligible beneficiaries.
l According to the government statistics no adolescent girls in the age group 11-17 were covered under nutrition programme although they are one of the eligible beneficiaries under universalization of ICDS.
l There observed a shortfall of 47 percent anganwadi centres, if one follows the Supreme Court's Directions for the norm of one functional anganwadi centre in each hamlet.
l The '7th Report of the Supreme Court Commissioners on Right to Food' states that 12985 tribal habitations have been covered by ICDS centres and about 4168 tribal habitations are yet to cover under the scheme.
l Furthermore, the existing Angan-wadi centres are facing a huge crisis of trained staff members. 76 posts of Child Development Project Officer (CDPO), 69 posts of (ACDPO) and 200 posts of Supervisors are still vacant throughout the State of Madhya Pradesh.
l Medicine Kit is an essential component of the ICDS services, for which Anganwadi worker has been trained to provide initial medicinal support for the symptoms like itching, injury, de-worming etc. But no such Medicine kit has ever reached the Anganwadi centres.
Box - 3 Dance ofDeaths
Nearly 230 malnutrition deaths have been reported by the Civil Society Organizations (CSOs) after due investigation in 4 districts of Madhya Pradesh in just four Months between May to August 2008. The numbers of deaths reported in four districts were Satna -72, Khandwa-62, Sheopur-64 and Shivpuri-32 respectively. The issue of children deaths is very much important because all the dead children belong to tribal/indigenous communities like Kol, Mawasi, Saheriya and Korku.
Moribund ICDS08
l Moreover, the State Government is allocating just Rs. 1.44 per beneficiary for addressing small health problems at each anganwadi centre under ICDS.
ICDS and Budget
l Madhya Pradesh budget expenditure on Child specific sectors specially Child Health, as a proportion of State Domestic Product is merely 0.1 percent.
l In order to cover all the beneficiaries under universalization of ICDS, the required budget allocation should be six times greater than the present one.
l The total budgetary requirement for 2007-08 was Rs 1320 crore including Children of 0-6 age group, Pregnant and Lactating women and Adolescent girls @ Rs 2 per beneficiary. However, the present budgetary allocations by the government for nutrition were Rs 320 crore in 2007-08, in which nutrition or food component comprised of around 80 percent that comes to Rs 255.54 crore.
l These allocations would be able to fulfill only 19.35 percent or one fifth of the requirement of the beneficiaries, which a very miniscule proportion considering the severity of the problem.
l State government has been actually ended up spending just Rs 212.89 crore against the total allocation of Rs 320 crore on 53.40 lakh beneficiaries in the state. It means per beneficiary expenditure comes to only Rs 1.33 per day in 2007-08 as against the Supreme Court's order of spending at least Rs 2 per beneficiary per day.
l Low allocation of funds and under spending of the funds further aggravated the ineffective results of ICDS.
l If taken into account the total budgetary requirement inclusive of administrative cost and other expenditure the figure turn out to be Rs 1650 crore for the year 2007-08 as against the miniscule budget allocation of Rs 535 crore taking together the allocations made under Supplementary Nutrition Programme (SNP) and ICDS.
Veracity of NRCs
l Madhya Pradesh Government has established Nutritional Rehabilitation Centers (NRC) at the block level to tackle the severe malnutrition. Total 135 NRCs has been established; out of which only 95 are fully functional.
l These centers have only 1678 beds to take care of nearly 13 lakh malnourished children in the state. Normally one child gets services for minimum 14 days, indicating no end to sever malnutrition!
l Alarmingly 49 NRCs do not have adequate trained staff.
Moribund ICDS09
Child Malnutrition-A Catastrophe inMadhya Pradesh
1
1.1 A Close Encounter
“Malnourished Children Flood Hospitals in Madhya Pradesh”
“Number of malnourished children hospitalized for treatment of malnutrition and resultant life threatening complications swollen to 150 in Khandwa district”.
“About 200 children admitted to government-run-NRCs in 13 other districts of MP”
“Situation is alarming in the tribal pockets of Khandwa, Satna,Jhabua and Shivpuri Districts”.
“Chhatarpur district hospital cites lack of beds at NRCs, malnourished kids left on floor”.
These were the few headlines of the daily newspapers of the past few months that have uncovered the shocking but the eye opening stories related to nutritional status of children in Madhya Pradesh. Malnutrition death figures are roaring by each passing day. Yesterday it was Satna, Shivpuri, Khandwa and Khargone, today it is Dhar, Jhabua, Sheopur, Rewa and Satna. Latest by now the children in the state capital Bhopal, are also engulfed by the deadliest malnutrition. You just name it and the list of malnutrition-affected dist r ic ts, b l o c k s a n d t h e pockets within the districts it goes count-less. But Madhya Pradesh government seems deaf to all the screaming for scourge of hunger news across the state. It has been a constantly denying the pragmatic fact saying that malnutrition is not really the reasons for children death.
Malnutrition is directly or indirectly responsi-
Joint Statement by UNICEF,WHO and UNSSCN
Severe acute malnutrition remains a major killer of children under five years of age. Until recently, treatment has been restricted to facility-based approaches, greatly limiting its coverage and impact. New evidence suggests, however, that large numbers of children with severe acute malnutrition can be treated in their communities without being admitted to a health facility or a therapeutic feeding centre.
The mortality rates (among children with severely acute malnutrition) reflect a 5-20 times higher risk of death compared to well-nourished children. Severe acute malnutrition can be a direct cause of child death, or it can act as an indirect cause by dramatically increasing the fatality rate in children suffering from such common childhood illness as diarrhea and pneumonia.
- Community based management of severe acute Malnutrition, A Joint Statement by the World Health Organization, The World Food Programme, and the United Nations
System Standing Committee on Nutrition and the United NationsChildren's Fund
Box - 4
Moribund ICDS10
ble for two-third deaths of children under the age of five; out of which two- third of these deaths takes place in the first year of child's life. In India, these deaths are preventable if the quality and nutritional outreach is taken better care of.
Malnutrition turn out to be the biggest curse for children in Madhya Pradesh. It is not a new phenomenon but put the state on backburner in terms of various social development indicators. The horrifying stories from the field would stun every sensitive citizen in the state. On the contrary state government statistics shows decrease in levels of malnutrition. However the ground reality differs to great extent. NFHS III reported that infact the level of malnourished children in Madhya Pradesh has become worst and rose from 54 percent in 1998-99 to 60 percent in 2005-06.
Further the recent report of IFPRI corroborates the fact of children death in MP is owing to hunger. IFPRI reports that 59.8 percents of the child population in the state are caught in the vicious cycle of malnutrition and hunger death. The graveness of the malnutrition situation in Madhya Pradesh can be assessed using following statistics. Out of the 63 lakhs malnourished children in the state more than 13 lakhs or one fifth children falls in the
3severely malnourished category . The serious impact of malnutrition on the life of children is 4resulting in 72 deaths before completing one year and 94 children in every 1000 births die
thbefore celebrating their 5 birthday.
The issue of malnutrition deaths of children came into limelight when the death cases of 7 children from Satna district was raised by the Right to Food Campaign Support Group and M.P. Lok Sangharsh Sajha Manch in the second week of May 2008. There after the death cases were also reported from Khandwa, Sheopur and Shivpuri districts. The civil society organizations and media continuously came up with the related facts on the issue of malnutrition; the important factor behind the early demise of children in M.P.
In spite of all these revealing facts along with the field reporting of dire increase in malnutrition levels; the State Government is in complete denial of malnutrition deaths in the State. Instead the state government manipulated the truth by establishing the fact that children are dying due to diseases or heat strokes but not due to malnutrition. The two departments namely Health and Women and Child Development (WCD) departments are cross firing each other on the whole issue. The former is stating that malnutrition was the underlying cause leading to multiple infections and some infections are too severe to be medically treated. However, WCD is putting the blame on Health department saying that the deaths were due to outbreak of diseases and the Health department could not able to control it.
However, World Health Organization (WHO) categorically stated that malnutrition can be the direct killer of the children. It raises the risk of mortality from 5-20 times. The Indian Association of Pediatrics has held the same opinion. In the light of all these innocent children were continuously losing their life to malnutrition as evident from the following data. 68 children died in Satna district, 163 children died in Sheopur, 62 in Khandwa district and
3Source NFHS III Report
4SRS 2007
Moribund ICDS11

32 children died in Shivpuri district of Madhya Pradesh over a span of 4 months from May to August 2008. But most importantly these children belong to tribal communities of like Kol, Mawasi, Korku and Saheriya tribes, which are one of the most deprived communities in the State with no land holding and no permanent source of income. Status of these families revealed a sorry state of chronic hunger and acute poverty. The government policy too has contributed to this food crisis among the poor.
It was observed in the field that although various government schemes have been launched yet the problem of food insecurity persists continuously due to lack of proper implementation. NREGS is the biggest anti-hunger programme and has a potential to transform the face and fate of rural India. The scheme was launched with a huge promise of providing 100 days employment but it is not gearing up as it was expected. A study by Centre for Environment and Food Security (CEFS), New Delhi stated that actually not more than 16 days of average employment was given to the needy households during 2007-08 against the State government's claim of 63 days of average annual employment. The data gap arises out of the fact that in the information provided by the state government, only 25 percent of the job figures are based on actual data while the remaining three-fourth job figures are based on fake job cards and fake entries
5in the muster rolls . The information collected by local organizations working at Satna, Khandwa, Sheopur and Shivpuri are also in agreement with the findings of CEFS. Villagers of Hardua, Nakjhir and Kirhai- Pukhri villages of Satna district have actually received 2 to 8 days of work while government records shows 14 to 94 days of employment. Similarly, in Khandwa district the cases of undue delay in payments and false entries of employment days in job cards were encountered.
Most of the deaths occurred in the families possessing BPL or Antyodaya Ration Cards; indicating the fact that malnutrition has hit the most vulnerable families with greater food insecurity. The grain allocation for BPL families under Public Distribution System (PDS) has been gradually decreasing from stipulated 35 kg to barely 20 kilograms a month. Moreover, Satna, Sheopur, Shivpuri and Khandwa districts are also facing consecutive drought for past 4-5 years aggravating the problem.
5Source : http://www.cefsindia.org/reports/ (Report of CEFS)
Distant Goals
Even after completing seven and a half years; the time limit set for achieving Millennium Development Goals (MDG), around 44.77 lakh or 38 percent families in Madhya Pradesh are living below the poverty line (BPL). The starkest truth is that out of total BPL families nearly 15.81 lakh families fall in the
.category of extreme poverty Thus at present there are near about 60 lakh families are deprived of enough food and the possibility of leading respectable lives. The National Sample Survey
stOrganizations (NSSO) report of 62 Round highlighted that Orissa, Chhattisgarh, Madhya Pradesh, Bihar, Jharkhand and UP remains the poorest states in the country in terms of Monthly Per Capita Expenditure (MPCE) of the rural population. In Madhya Pradesh, 47 percent of the rural population is living on Rs 12 a day followed by Bihar and Jharkhand 46 percent, Uttar Pradesh 33 percent, Karnataka 32 percent and Maharashtra 30 percent.
Box - 5
Moribund ICDS12

1.2 Malnutrition in Madhya Pradesh- Stories directly from the field
Madhya Pradesh is a centrally located state of India and it is divided into 50 districts with the population between 1 to 2 million in each district. There are 55393 villages in the state covered by 22 thousand elected Panchayats - Local governance body. The state has yet to achieve real developmental goals to come out of the group of BIMARU state. Economic Survey of Union Government states that 38 percent of the state's population (6.44 million families) is leaving below poverty line and deprived of basic amenities like food, shelter and cloth, struggling every day for survival.
1.2.1 Satna…a silent deprivation
Right to Food Campaign and Lok Sangarsh Saajha Manch raised a case of death of 7 children in Satna district in the second week of May 2008. In next 20 days the death toll moved up to the level of 27. Action began, but only on papers and State Government continued to deny the malnutrition deaths, instead cited diseases or heat stroke as the reasons behind the deaths. Malnutrition deaths are considered closest to hunger deaths. One can identify malnutrition but can not investigate or prove any malnutrition deaths. It is because in forensic science and in pediatrics there is no clear definition to identify the symptoms of deaths due to malnutrition. The local organizations argued on the basis of circumstantial evidences that the families belonging to communities of Kol and Mawasi tribes were living with acute poverty, chronic hunger and uncertainty of life. The victim families got merely 2-3 days of work under National Rural Employment Guarantee Scheme (NREGS) and received only 15 to 20 Kgs of subsidized food grains from PDS.
In the villages where Aadiwasi Adhikar Manch and Right to Food Campaign visited it was not a normal encounter with situation, where 2-6 children died in a short span of 20 days. However, it is worth mentioning that particularly August and September months were identified as most food insecure and disease prone months especially for the tribal, migrants and labour communities. In spite of various promising programs to ensure the better growth and survival of children, the death toll continue to increase in Satna district and reached to 68 by August 2008. It was observed that during the whole period role of the state government was not proactive. It's true that simply organizing health camps or providing supplementary nutrients to Anganwadi centers after the children's death is by no means going to sort out the serious problem like malnutrition.
This area is suffering from drought trouble for past four years but no concrete steps have been taken to help the villagers. Records of state government say that 28745 children under the age of one year died in the state during 2008-09 and Satna tops the list with 1856 deaths. In 2007-08 there were 29383 children below one year age died in the state and again Satna topped with 1668 infant deaths.
Adiwasi Adhikar Manch an ally of M.P. Lok sangharsh Sajha Manch and Right to Food Campaign Group together presented a report to the Advisor to Supreme Court
thCommissioners about Right to Food on 11 June 2008 mentioning the poor implementation of the Government schemes in the district along with the cases of continued deaths of children. The then Collector of the Satna district was asked to submit a detail report about
Moribund ICDS13
hunger and starvation deaths and failure of government programmes related to food security and employment schemes till 15th July 2008. But unfortunately Collector, the most responsible officer of the District, was busy in election campaign.
Probably the issue of deaths of children was not of so importance as Collector did not take any action on the grim situation until 14th of July 2008, except stating that the deaths were due to seasonal diseases and not due to malnutrition. When the number of died children reached 27 and the issue got the momentum in media, it was only then, on 15th of July Collector visited the field that to just one village Hardua and announced number of relief measures on the spot in order to console the families who lost their kids. Some of those relief measures were as follows:
l 65 kg ration to families of children died due to malnourishment.
l Suspension of salesman of Puraina village to correct the PDS supply
l Sanction of fund for anganwadi and EGS Centres.
l Allotment of Social Security Pension, NREGS Job cards and Ration cards to eligible beneficiaries.
l Work order for plantation and cement concrete (CC) road construction were sanctioned.
l Free treatment of weak & malnourished children and landless patients at Nagaud or District health centre.
l Regular medical camps in the villages were announced every week.
Here the question comes to mind that such short span announcements are sufficient enough to tackle the devastating problem like persistent malnutrition? Moreover, all the promises made were seem to be faked one for the obvious reasons. It is because within the 7 days of the announcement of the relief measures, the work under NREGS was halted, construction of anganwadi centre was limited to base work of the building only and the regularity of health camps were maintained just for two weeks. Another sorry state that with the denial of malnutrition deaths by the government; the issue of just compensation to the families of victims was ruled out quite cleverly.
District Collector submitted his report to the Advisor to Supreme Court Commissioners on 15th of September 2008 a month later after the due date. The report clearly mentioned that all the deaths of children were due to some seasonal diseases like heat stroke, measles, diarrhea, etc. rather than malnutrition. Meanwhile, two enquiry commissions visited Satna district to enquire about the deaths, but the result presented by these commissions once again established no evidences of malnutrition deaths, as it was expected previously!
Status of ICDS in Satna
In Satna district children; the prime beneficiaries like are deprived of the benefits to the fullest. According to the Supreme Court orders, one anganwadi centre should cater to 40-80 children but in case of Uchhehra block of Satna, there are 21380 children enrolled in 152
Moribund ICDS14

anganwadi centers. It means on an average 140 children are enrolled per anganwadi center. This shows there is a need of 267 more anganwadi centers in the block to provide services to all the children. Besides, anganwadi centers lack basic amenities like proper arrangement for drinking water, separate toilets and even separate space for cooking nutritious food. Almost all the centers deprived of growth charts, playing kit and educational materials and weighing machines called salter machine. Furthermore, almost all the anganwadi workers are untrained and illiterate and inexperienced to handle the job responsibility. Quality of supplementary nutritional food being supplied in anganwadi centers is really dubious one. It was observed that the Panjiri supplied by the contractor was actually the animal feed. When the district Administration was informed but no steps were taken against. Thus to check the malnutrition with such minimal existing facilities is the real challenge.
Reality of NRCs
In Satna district proportion of under six population is 15% i.e 2.8 lakh and number of malnourished children is around 33,820. To cater these children there are merely 2 NRCs and with only 30 beds. Thus it is a blunt fact that the malnourished children have no other option but to wait for their turn with such a sparse medicinal facilities. According to the NRC norms, each child should be given a treatment of at least 14 days to cope up the malnutrition, but in Satna the children are admitted in the district NRC for only 7 days due to shortage of facilities. It was only after the cases of malnutrition and deformities were highlighted against the Health and Women and Child Development departments, the treatment days were increased to 14 days. It is a further shabby work that once the children are relieved from the NRC, there is no proper follow up about health of children and also there observed the communication gap between NRC and Anganwadis in the field.
1.2.2 Khandwa….children living on verge of death
When such mess was continuing in Satna, at the same time news regarding critical incidences of malnutrition deaths started flowing from Khandwa district. Khalwa Block of Khandwa District is a Korku tribal dominated block. By virtue of backwardness it has been earmarked as Fifth Scheduled Area. Traditionally it is a chronic malnutrition prone area and it was not the first incidence when the malnutrition among the children under fives or deaths thereby has been reported from the region. For past many years the children have continued to die and tribal families have been appeasing the traditional deities for saving their children.
Back in 2003-04, Spandan Samaj Seva Samiti, an NGO working in the region brought to light the issue of severe malnutrition and deaths of children. About dozen of deaths were recorded and the fact was highlighted that acute food security at the household level was one of the contributing reasons. This initial efforts exerted substantial pressure and government took steps like starting of Nutrition Rehabilitation Centers (NRCs/Bal Shakti Kendras) and running Bal Sanjeevani Abhiyans (campaign to weigh and grade malnutrition). The Bal Sanjeevani reports have now become the official statistics for measuring malnutrition. Over the years these figures showed drastic reduction in malnutrition and it was claimed that the malnutrition situation in the state is under control.
Moribund ICDS15

But the grass roots reality is far from such claims when the recent malnutrition deaths were reported in the district.
Till date the deaths of 39 children across 18 villages of Khalwa block shows that the average deaths were more than two per village. This reveals the severity of the situation in the district. Out of the recently reported 27 deaths, more than 50 percent deaths were mainly from the three villages namely Mohalkhari, Salidhana and Ambada. These villages are located within the radius of three kilometer from the Government Hospital at Roshni. Among the dead 12 children could not have celebrated even their first birthday and the severity of problem among girl child seems to be worst with 10 out of 11 succumbed to malnutrition deaths. In one of the striking case both mother and the child died in a span of just two days owing to hunger and malnutrition.
Malnutrition seems to be widespread in Khalwa block and the extreme poverty is triggered by acute household food insecurity citing as a major cause of deaths. The families who lost their children were found to be forced to borrow grains or money for purchasing grains at soaring interest rate, sometimes double the rate. Most of the deaths occurred in the families that are either BPL or Antyodaya Ration Cards holders, justifying the fact that malnutrition has hit in the most vulnerable and food insecure families.
Although the acute household level food insecurity seems to be the major underlying cause of the tragedy, but the bottlenecks and irresponsibility of programme implementing individuals and agencies cannot be sidelined. The intriguing facts is that despite the mishap the government field staff like Anganwadi workers, Auxiliary Nurse Midwife (ANMs) and Panchayat secretaries are not monitoring the ground situation properly. If proper data had maintained at the district level; it would have prompted the early administrative response to averting many deaths. Prima facie investigations revealed that the records of Anganwadi worker about name of the deceased children, their weight or date of death had aura of doubt over the authenticity. For example, the name of a deceased child named Amarsingh (as parents informed us and as media reported) was later altered to Ramsingh. Anganwadi worker reported another deceased child named Aarti Totaram's weight as 9 kilograms but
A Complex Life
Sivram, a landless wage earner from village Medhapani lost his 18 months old daughter, Shivani. He do not posses a ration card and hence was forced to borrow 1000 rupees recently to buy grains but was failed to save his child.
Amarsingh Vishram from village Jamnapur lost 3 years old Ravishanker is also a landless wage earner. He neither has a ration card nor a job card to ensure food security.
Suraj from the village Mohalkhari lost two children Chhotu (4years) and Sagar (6 months) recently. He possess two acres of un-irrigated which is not yielding sufficient for feeding the family. The family is so pressed with sickness of the children that they could not even weed their field this year. They borrowed 2000 rupees for treatment of the children and will have to return one and a half time the amount borrowed. Recently they have borrowed one quintal of grains for which they will have to return double the quantity. Family with disabled mother earlier had a Antyodaya Ration Card but that has now been replaced with BPL card as a result often they are unable to buy ration as they have to pay more now. Family claimed that elder daughter alone worked for two weeks in NREGA but the job card does not show the dates of work.
Box - 6
Moribund ICDS16
the child actually weighs 4.5 kg only. The severity of malnutrition can be inferred from the fact that at least three children died at the NRC itself and one of them could not be saved even after visiting Chacha Nehru Hospital at Indore.
1.2.3 Sheopur……usual incidents
In Sheopur, Saheriya Mukti Morcha has reported that 162 children belonging to Saheriya Primitive Tribal Group have lost their lives. This community is known for highly vulnerable in terms of food insecurity and malnourishment in the country. Many reports are coming from the field briefing about continuous deaths in the district and denial from government side. Prior to the present situations, Patalgarh village of Sheopur district has been the center of discussion since February 2005 where 13 child-deaths were reported, due to malnutrition. The issue was highlighted almost at every platform. Taking note of gravity of situation, the Hon'ble Supreme Court nominated a Commissioner for reviewing the remedial measures, and in turn issued directions for curbing malnutrition.
In this village, merely 5 days work has been allotted to villagers during last three years under various employment schemes. There is absolutely no trace of the provisions like mid-day meals and anganwadi centres, for the simple reason that the village population is very sparse and in numbers it is less than 700. As far as other facilities are concerned, rural hospital is about 63 kilometers away from this village. It is due to scarcity, poverty and non-availability of proper and nutritious food, one out of every 10 expectant mothers succumb to death during delivery.
Subsequently, between March to May 2006, 10 more untimely child-deaths were reported from the same area. The then Adviser to the Commissioner, Supreme Court of India in the 'Right to Food Case' once again wrote to the District Collector urging him to take more decisive actions in the matter. Following this a Joint Commission of Enquiry (JCE) was constituted to examine the cases reported and to look into the status of implementation of food-related schemes in the district. The committee consisted of Shri P.S. Vijay Shankar (representative of Dr. Mihir Shah), Dr. SK Singh, Dr. Vijay Gupta, Shri R.N. Raghuvanshi, Joint Director, WCD, GoMP and Dr. Mohan Singh, Divisional Joint Director, was constituted in November 2006.
During their visit, JCE quoted that the infant mortality rate for the district at 110 infant deaths per 1000 live births is comparable to some of the poorest regions in the world like Sub-Saharan Africa. The most critical issues mentioned in the report of JCE are as follows:
End begins frombeginning!
Guddi wife of Gamandi is a severely malnourished woman. She lost her five children in past few years. In her own words "Woh to sookh ke mar gaye". Upon enquiring the mother Guddi, when she would start breast-feeding her infants, replied very painfully, "How I can feed my infant when I myself did not had anything for last seven days". Tulsi, another severely malnourished woman in the village, lost her two children, a girl and a boy last year. The above cases throw light on the fact that the real problem starts with unsafe motherhood and resulted into never-ending vicious circle of malnutrition.
Box - 8Box - 7
Moribund ICDS17
l Poor functioning of various Government Schemes like ICDS, Mid Day Meal (MDM), Targeted Public Distribution System (TPDS), and National Old Age Pension Scheme (NOAPS) were observed in the villages visited.
l Poor implementation of NREGA where minimum wages are not being paid for work done.
l High Incidence of starvation deaths, particularly among the children and poor status of delivery of health services to women and children.
l The JCE also noted several cases of neglect of child health in the villages where to some extent the ANM is little active.
l The JCE recommended that there are structural reasons (like inaccessibility to and fro in the villages, lack of development thrust in the region, poor implementation of various government programs, etc) for persistent of poverty and malnutrition which need to be immediately tackle on a war footing basis, if the starvation deaths in the area have to be checked.
l The committee suggested that the kind of "nutritional emergency" prevailing in a small district like Sheopur is completely preventable if the administration undertakes the steps as outlined above and work in close partnership with civil society organizations to achieve these common goals.
Visits of JCE and the submitted report clearly depicted the pictures of ground realities that the grim situation of malnutrition and hunger in the districts are nothing but the reflection of poor implementation status of the government programmes and schemes. It was observed that with the overall lack of development thrust, no concrete steps have ever been taken to resurrect the failure of the system in the region. Reporting of child death is still continuous in the district and in 2008 the toll of children succumbed to malnutrition has reached to 160 merely in past 5 months from May to September 2008.
Since February 2008, except for allocation of panjiri on 21st August 2008, there was no supply of supplementary nutrition to any of the anganwadi centers of the district. Also, the basic amenities like pre-school education, weighing machines, utensils, and medicine kits were missing from the anganwadi centers. Even there is no anganwadi bhawan in most of the villages of the district. The job cards of most of the villagers are in the hands of Panchayat secretary. Villagers have got only 10-15 days of employment under NREGS while the entries in job cards shows that 50-150 days of employment has been provided.
1.2.4 Shivpuri……deaths continue
Shivpuri is another Sahariya tribe dominated district. This community never bother about their future, because they are confident that forests, which they respect and protect, would never leave them hungry. However, continuous exploitation of forest by other social groups in the district has resulted in irretrievably damaging the very source of food security to the families of ̀ Sahariyas' tribe. Left with no alternative, the Sahariyas had to look out for labour work in the local stone mines to earn their livelihood. But again the mystery does not stop
Moribund ICDS18

here as the elders working in the stone mines succumb to deaths at the early age of 40 years due to silicosis.
Shivpuri district has been badly hit by drought for the past 5-6 years. During the drought periods most critical problem, people used to face is about securing the means of livelihood. Caught in the web of constant shrinking of forests and strict provisions of various forestry laws, the Sahariya tribes were left to face an unending state of hunger. In this district cases of children dying of malnutrition have been reported during 2003. Manav Adhikar Forum surveyed the district and reported about 47 children have succumbed to death in the District in just 2 months (June and July) in 2008.
The issue of death of 8 children came into limelight from the village Bamhouri of the district but there was no response from Government until media raised the issue. Though there is a PHC in the village and ANM also has posted in the village but she hardly visits the village, usually once in a month. The allocation of supplementary nutrition in the anganwadi center of the village is irregular thus the beneficiaries of AWC are deprived of the nutritional feed. Not a single family is getting the
6benefit of Deendayal Antyoday Upchar Yojana in the village. Although the Government claims to undertake relief work, but the fact is in spite of resorting to hard labour work with empty stomach, they have not been paid their wages for about two years now. According to Shyam Adiwasi of Bamhouri village false entries of 100-150 work days have been made in the NREGS job cards of villagers against the actual work of 2-4 days, they really do not know as to who is responsible for scuttling their rights. The situation is further aggravated due to prevailing political and social system that tribals do not have the strength and courage to stand for and demand their just rights. The only aid provided by the Government was through organizing the health camps in the regions that were in the media glare by providing mosquito nets and plastic sheets to the families living in huts.
7As per a study of Right to Food Campaign , although 26 percent people of Sahariyas tribe possess 5-8 Bighas of land, but nearly 70 percent of this land is unirrigated and stony and
Losing faithin the system
Prakash Adiwasi, resident of village Bamhouri of Shivpuri district, lost his 3 kids in just 15 days. There were 9 members in his family with 2 son, 4 daughters, his wife and he himself. Prakash is the only earning member in the family and every day he has to struggle for livelihood. As there is no availability of work in the village, he has to go out of the village for earning. His daughter Neetu (3 years) caught in fever and finally succumbs to death in the absence of any medical help owing to poor financial condition. The family has yet to recover from the shock of the death of Neetu and suddenly the siblings Raju (6 months) and Chhoti (6 months) also died in the same conditions. Meanwhile, Prakash tried his level best to save his children; he ran from pillar to post but failed to arrange money for medical treatment to his ailing children. The family now being left with only 6 members who have lost the hope of surviving anymore in the village and finally decided to migrate and left for Gwalior forever.
6The scheme provides free medical treatment and investigation in all government health facilities up to a
limit of Rs. 20000/- to all BPL families.7Jain, Sachin. (2006) 'Poverty, migration & national rural employment guarantee scheme a case study on
Sahariya primitive tribal group in Madhya Pradesh', http://www.righttofoodindia.org/links/field_reports.html
Box - 8
Moribund ICDS19
situated at mountainous slopes. Unless these lands are developed properly cannot be put to suitable for cultivation or any other useful purposes. In the last one year more than 60 hunger deaths of Sahariya tribes were reported from Shivpuri district. Although some temporary measures were taken by the Government at that time, but not a single long term solution was initiated. Besides, these tribals are often gets exploited at the hands of government staff. To give an example of such exploitation, the bicycles belonging to scheduled tribe people of 30 villages of Kolaras block, including Bairasia, Sanwara and Gugwara, were confiscated by the Forest Department staff and demanded a penalty of Rs.200/- each, on the pretext that they were carrying the dry and dead woods from the forest area for selling, ignoring the fact that the tribals living in the forest area are duly authorized to do so. The plight of their financial condition was such that they could not secure the release of their bicycles for about six months and it was only upon intervention of some local organizations, district administration has instructed the Forest Department to return the bicycles. Facing the social ignorance, anger, deprivation and inhuman treatment inherent in the system, the people of `Sahariyas' tribe is once again in the miserable condition. In the absence of sources of livelihood, this tribal group is again forced to resort to migration.
1.3 Health Status in Madhya Pradesh
Malnutrition among children stirred the political environment and took a central stage in Madhya Pradesh after media and civil society organizations spearheaded the whole issue through people's campaign mode. Undoubtedly it is very difficult on the part of the State Government to accept the fact that children in the state are dying in huge numbers due to malnutrition. Meanwhile the death toll reached to 360 in the same 4 districts namely Satna, Khandwa, Sheopur and Shivpuri. Reports of severe malnutrition started flowing from the districts like Barwani, Jhabua, Dhar, Burhanpur and around, where 2450 severely malnourished children have reached to the Nutritional Rehabilitation Centers. In recent years, malnutrition as one of the indicators of the status of human development has been on the steady rise in Madhya Pradesh. NFHS III data states that 12.6% children in Madhya Pradesh are suffering from most severe malnutrition and are on the verge of death. It means around 13 lakh children in the state are at highest risk of survival, thus indicating the urgent need to address the issue with some serious interventions in the state in general and in the affected areas very particularly. If we take a look at the various governmental schemes, we will find huge discrepancies in proper implementation of these schemes and programmes at the village level. The following section presents some of the hard-core facts about the situation in the State.
1.4 Health Infrastructures
In Madhya Pradesh, of the total population nearly 20 percent population belongs to indigenous tribes; mostly resides on the fringes of forest and greatly dependent on forest for their livelihoods. It is important to mention this because these are the areas where health
8facilities are minimal and incidence of malnutrition is even greater . Malnutrition lowers the
8Alert note on Malnutrition in Madhya Pradesh by Right to Food Campaign Madhya Pradesh Group
Moribund ICDS20
resistance power making the people weak thus succumb to ordinary diseases that could be cured easily. The important step in curbing child or infant mortality would be a promising health facilities reaching to the remotest rural areas through wide spread functioning anganwadi centers with due recognition to their importance. Aanganwadi centers not only run the programmes of women and child development department but also the programmes of the health department like vaccination, nutrition, and school education and look after and monitor the malnourished children.
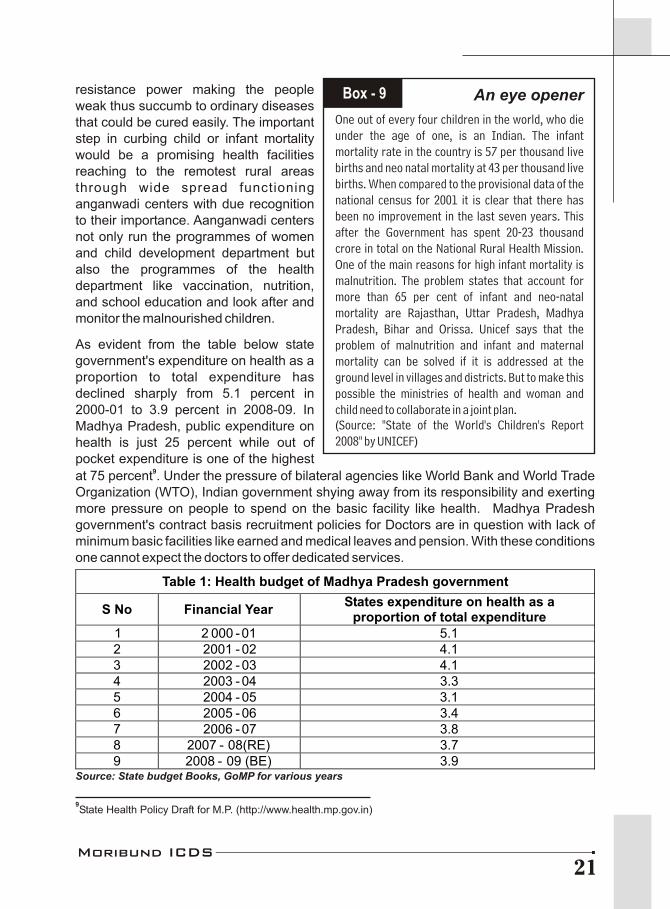
As evident from the table below state government's expenditure on health as a proportion to total expenditure has declined sharply from 5.1 percent in 2000-01 to 3.9 percent in 2008-09. In Madhya Pradesh, public expenditure on health is just 25 percent while out of pocket expenditure is one of the highest
9at 75 percent . Under the pressure of bilateral agencies like World Bank and World Trade Organization (WTO), Indian government shying away from its responsibility and exerting more pressure on people to spend on the basic facility like health. Madhya Pradesh government's contract basis recruitment policies for Doctors are in question with lack of minimum basic facilities like earned and medical leaves and pension. With these conditions one cannot expect the doctors to offer dedicated services.
An eye opener
One out of every four children in the world, who die under the age of one, is an Indian. The infant mortality rate in the country is 57 per thousand live births and neo natal mortality at 43 per thousand live births. When compared to the provisional data of the national census for 2001 it is clear that there has been no improvement in the last seven years. This after the Government has spent 20-23 thousand crore in total on the National Rural Health Mission. One of the main reasons for high infant mortality is malnutrition. The problem states that account for more than 65 per cent of infant and neo-natal mortality are Rajasthan, Uttar Pradesh, Madhya Pradesh, Bihar and Orissa. Unicef says that the problem of malnutrition and infant and maternal mortality can be solved if it is addressed at the ground level in villages and districts. But to make this possible the ministries of health and woman and child need to collaborate in a joint plan.(Source: "State of the World's Children's Report 2008" by UNICEF)
Box - 9
Table 1: Health budget of Madhya Pradesh government
S No Financial YearStates expenditure on health as a
proportion of total expenditure1 2 000 -01 2 2001 - 02 3 2002 - 03 4 2003 - 04 5 2004 - 05 6 2005 - 06 7 2006 - 07 8 2007 - 08(RE) 9 2008 - 09 (BE)
5.1 4.1 4.1 3.3 3.1 3.4 3.8 3.7 3.9
Source: State budget Books, GoMP for various years
9State Health Policy Draft for M.P. (http://www.health.mp.gov.in)
Moribund ICDS21

The basic issues like health and malnutrition in Madhya Pradesh are summarized as follows:
l The state has highest rate of infant mortality and malnutrition among children. Nearly 55 percent of all children below 3 years are under weight, 51 percent are stunted, 20 percent are wasted and 75 percent are anemic.
l Various reports of UNICEF state that out of every thousand live births 100 children die in the developing countries. Preventable diseases cause the deaths. Moreover, in M.P. a child dies every 5 minutes.
l Proportion of children receiving immunization against all prevent-able diseases in the age group 12-24 months is only 22.4 percent.
l Only 25 percent of children 6-35 months having received at least one dose of Vitamin 'A'.
l Maternal mortality rate in the State, which is second highest in the country i.e. 379 per lakh live births.
10l IMR is also highest at 72 per thousand live births .
l One has to understand the fact that the high level of Maternal Mortality also contributes to the high level of Infant Mortality. Medium term health sector strategy for Madhya Pradesh-2006 has recognized the MMR at the rate of 400 per lakh but no projections has been made to reduce it by three quarters till 2015 in order to achieve the MDGs.
1.5 Far behind from GOALS
It is important to note that the Reproductive Child Health (RCH)-II programme implementation plan sets itself a goal of reaching IMR of 60 by 2010, which in itself is a modest goal, after the MDG commitment. But what is more interesting to know is that based on the predictive modelling exercise published in the National Commission of Macroeconomics and Health Report predicts that the given current trends of IMR for the state would reach 69 by 2010 and to 60 by 2015 (with a range from 51 to 71 even the lower limit of the range being well above the commitment and comparatively the lowest amongst the states.). Clearly there is a need to work out strategies to accelerate the pace of
Key facts aboutMaternal Health from
NHFS-3 statistics
8 Mothers who had at least 3 antenatal care visits for their last birth- 40.2 percent
8 Births assisted by a doctor/nurse/Lady Health Worker (LHV)/ANM/other health personnel - 37.1 percent
8 Institutional birth-29.7 percent
8 Mothers who received postnatal care within two days of delivery-27.9 percent
8 Women whose body mass index is below normal-40.1 percent
8 Ever married women (age 15-49) who are anaemic-57.6 percent
8 Pregnant women (age 15-49) who are anaemic-57.9 percent
Box - 10
10SRS Data-October 2008
Moribund ICDS22
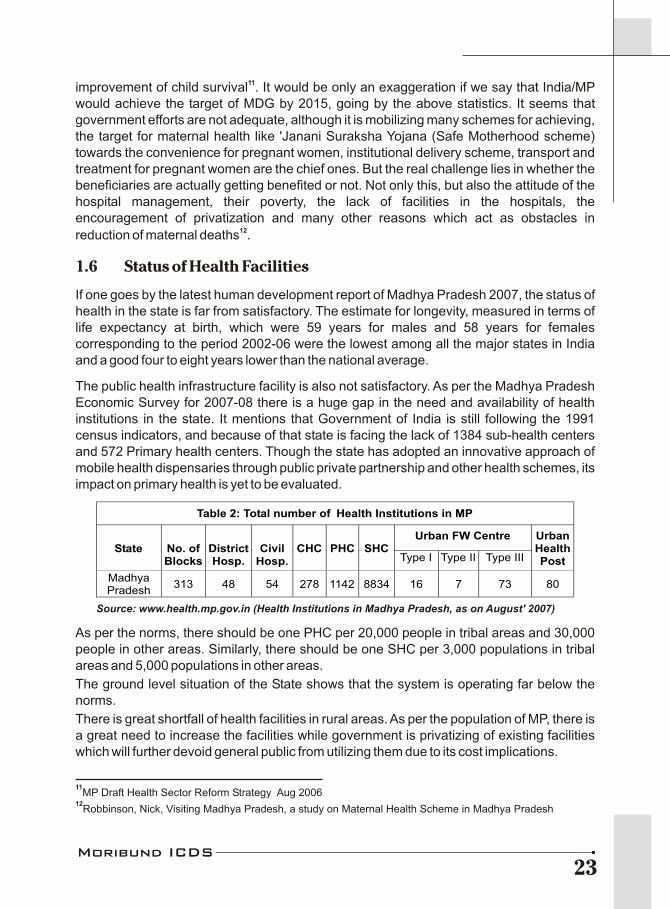
11improvement of child survival . It would be only an exaggeration if we say that India/MP would achieve the target of MDG by 2015, going by the above statistics. It seems that government efforts are not adequate, although it is mobilizing many schemes for achieving, the target for maternal health like 'Janani Suraksha Yojana (Safe Motherhood scheme) towards the convenience for pregnant women, institutional delivery scheme, transport and treatment for pregnant women are the chief ones. But the real challenge lies in whether the beneficiaries are actually getting benefited or not. Not only this, but also the attitude of the hospital management, their poverty, the lack of facilities in the hospitals, the encouragement of privatization and many other reasons which act as obstacles in
12reduction of maternal deaths .
1.6 Status of Health Facilities
If one goes by the latest human development report of Madhya Pradesh 2007, the status of health in the state is far from satisfactory. The estimate for longevity, measured in terms of life expectancy at birth, which were 59 years for males and 58 years for females corresponding to the period 2002-06 were the lowest among all the major states in India and a good four to eight years lower than the national average.
The public health infrastructure facility is also not satisfactory. As per the Madhya Pradesh Economic Survey for 2007-08 there is a huge gap in the need and availability of health institutions in the state. It mentions that Government of India is still following the 1991 census indicators, and because of that state is facing the lack of 1384 sub-health centers and 572 Primary health centers. Though the state has adopted an innovative approach of mobile health dispensaries through public private partnership and other health schemes, its impact on primary health is yet to be evaluated.
As per the norms, there should be one PHC per 20,000 people in tribal areas and 30,000 people in other areas. Similarly, there should be one SHC per 3,000 populations in tribal areas and 5,000 populations in other areas.
The ground level situation of the State shows that the system is operating far below the norms.
There is great shortfall of health facilities in rural areas. As per the population of MP, there is a great need to increase the facilities while government is privatizing of existing facilities which will further devoid general public from utilizing them due to its cost implications.
11MP Draft Health Sector Reform Strategy Aug 2006
12Robbinson, Nick, Visiting Madhya Pradesh, a study on Maternal Health Scheme in Madhya Pradesh
Table 2: Total number of Health Institutions in MP
Urban FW Centre State No. of
Blocks District Hosp.
Civil Hosp.
CHC PHC SHC Type I Type II Type III
Urban Health Post
Madhya Pradesh
313 48 54 278 1142 8834 16 7 73 80
Source: www.health.mp.gov.in (Health Institutions in Madhya Pradesh, as on August' 2007)
Moribund ICDS23
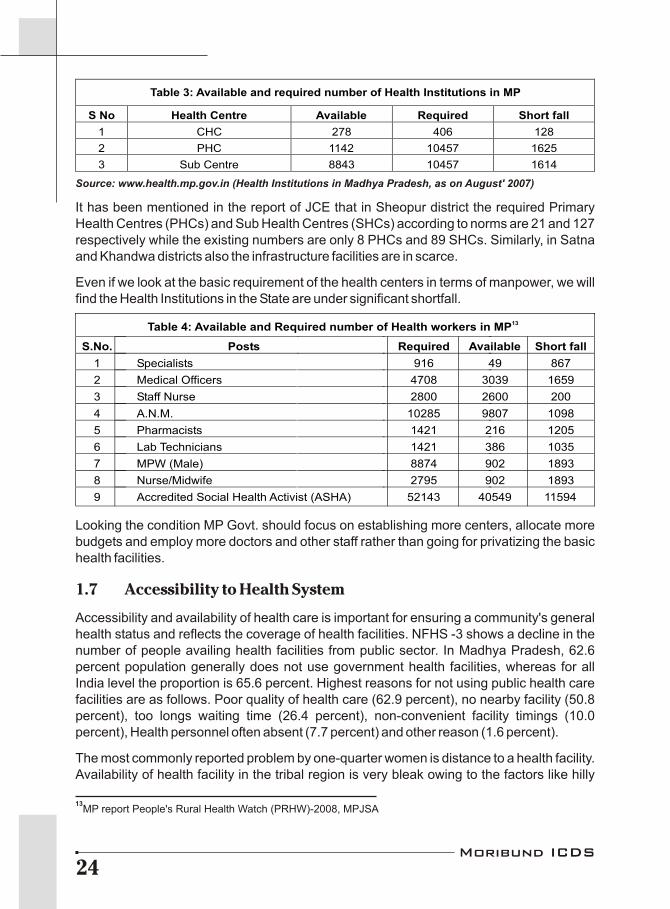
It has been mentioned in the report of JCE that in Sheopur district the required Primary Health Centres (PHCs) and Sub Health Centres (SHCs) according to norms are 21 and 127 respectively while the existing numbers are only 8 PHCs and 89 SHCs. Similarly, in Satna and Khandwa districts also the infrastructure facilities are in scarce.
Even if we look at the basic requirement of the health centers in terms of manpower, we will find the Health Institutions in the State are under significant shortfall.
Looking the condition MP Govt. should focus on establishing more centers, allocate more budgets and employ more doctors and other staff rather than going for privatizing the basic health facilities.
1.7 Accessibility to Health System
Accessibility and availability of health care is important for ensuring a community's general health status and reflects the coverage of health facilities. NFHS -3 shows a decline in the number of people availing health facilities from public sector. In Madhya Pradesh, 62.6 percent population generally does not use government health facilities, whereas for all India level the proportion is 65.6 percent. Highest reasons for not using public health care facilities are as follows. Poor quality of health care (62.9 percent), no nearby facility (50.8 percent), too longs waiting time (26.4 percent), non-convenient facility timings (10.0 percent), Health personnel often absent (7.7 percent) and other reason (1.6 percent).
The most commonly reported problem by one-quarter women is distance to a health facility. Availability of health facility in the tribal region is very bleak owing to the factors like hilly
13MP report People's Rural Health Watch (PRHW)-2008, MPJSA
Table 3: Available and required number of Health Institutions in MP
S No Health Centre Available Required Short fall
1 CHC 278 406 128
2 PHC 1142 10457 1625
3 Sub Centre 8843 10457 1614
Source: www.health.mp.gov.in (Health Institutions in Madhya Pradesh, as on August' 2007)
13Table 4: Available and Required number of Health workers in MP
S.No. Posts Required Available Short fall
1 Specialists 916 49 867
2 Medical Officers 4708 3039 1659
3 Staff Nurse 2800 2600 200
4 A.N.M. 10285 9807 1098
5 Pharmacists 1421 216 1205
6 Lab Technicians 1421 386 1035
7 MPW (Male) 8874 902 1893
8 Nurse/Midwife 2795 902 1893
9 Accredited Social Health Activist (ASHA) 52143 40549 11594
Moribund ICDS24
terrain, bad roads and lack of transport facilities. As a result the habitants are completely deprived of the government PHCs. Around 44 percent women from scheduled tribe reported distance to be a big problem. Only 17 percent of the deliveries of women belong to Scheduled Tribes were assisted by a doctor, compared to 47 percent births to women of other classes. Prevalence of anaemia is highest in the Scheduled tribes; both men and women.
The undernourished SystemThe undernourished System
214 children were registered in the AWC of Lakhrawan village falling under Rajnagar block of Chhatarpur
district; however capacity of the centre is just enough to support only 40 children. Also these children have not
received any hot cooked supplementary nutritious food for the past two months (i.e. since March 2009). It was
observed during the field visit that the amount of Rs. 3765/- per month was allotted for the supplementary
nutritious food to this anganwadi center in the Kota Panchayat. This meager amount is not at all sufficient to
support all the children of age 3-6 years enrolled in Anganwadi. Even this scanty fund is not reaching in the
hands of SHG (authorized for cooking food in the center) but the fund get siphoned off due to prevalent practices
of corruption. The irony of the situation is that the ICDS Supervisor of the center and the officials of W&CD
department are totally unaware of the fact that there is no supply of SNP in the Anganwdi of Lakhrawan since
March 2009. It clearly shows how strong the monitoring system of the ICDS network is! The things don't end
here; the anganwadi worker of Lakhrawan village has not received her remuneration for the past seven months
and the same situation is being faced by the anganwadi workers of Kota and Para village also.
This case study has been observed by Right to Food Campaign Madhya Pradesh Support Group. (June 2009)
Moribund ICDS25
Integrated Child Development Services
2
Integrated Child Development Services programme has main focus on catering the need of children under the age of six years through supplementary nutrition, health care and pre-school education. It also covers adolescent girls, pregnant women and nursing mothers. Government of India started it in 1975 with the following objectives;
l To improve nutritional and health status of children below six years age.
l To lay down the foundation for proper psychological, physical and social development of the child.
l To reduce the incident of mortality, morbidity, malnutrition and school dropouts.
l To achieve effective co-ordination of policy and implementation among various departments to promote child development.
l To enhance the capability of mother to look after the normal health, nutritional and developmental needs of the child through proper community education.
2.1 Implementation process of ICDS
Women and Child Development department is the nodal department for implementing ICDS scheme. Medical and Public Health department has been given the responsibility of immunization of children under health services.
Basic services provided under ICDS can be categorized under three heads namely, nutrition, health and pre-school education. In nutrition services there is supplementary feeding, growth monitoring and nutrition and health counseling. Health services include immunization, basic health care and referral services. These health services are delivered through public health infrastructure viz. PHC, CHC and SHC. Under Pre-school education various stimulation and learning activities are covered at the anganwadi.
2.2 Services provided under ICDS
Different services under ICDS are provided through 'Anaganwadis' a network of ICDS centres. Anganwadi Worker (AWW) is assigned with the responsibility of operating anganwadi. An Anganwadi Helper (AWH) supports them. The seven basic services provided through Anganwadi centers are as follows
1. Supplementary Nutrition - This includes the allocation of supplementary nutritious feed to all the children below the age of six, adolescent girls and pregnant and nursing mothers for at-least 300 days per annum or 26 days a month. By providing supplementary feeding, the anganwadi attempts to bridge the protein energy gap between the recommended dietary allowance and average dietary intake of children and women to control vitamin A deficiency and nutritional anaemia. According to this component children
Moribund ICDS26

are given supplementary food containing 300 calories energy and 8 to 10 grams of protein while women (pregnant & lactating) are given food with 500 calories energy and 20-25 grams of protein. Besides, severely malnourished children are given special supplementary feeding and referred to sub health centres and PHCs as and when required. Prioritizing the nutritional needs of children (0-6 years), new norms have been released by Ministry of WCD in Feb. 2009.
2. Growth Monitoring - Growth monitoring is another important activity that is supposedly to be operational at anganwadi centers is one of the many ICDS functions. The programme is expected to monitor the growth of children by weighing them every month and plotting their growth on a chart. It is important for assessing the impact of health and nutrition-related services and enabling communities to improve the same. As per ICDS guidelines, children below three years of age should be weighed once a month and children 3-6 years of age quarterly. Weight for age growth cards or growth registers is supposed to be maintained for all children below 6 years of age in the village. These help to detect growth faltering and to assess nutritional status. The entire monitoring of malnutrition is based on this system of growth monitoring data. To monitor the growth each anganwadi center is provided with three types of weighing machines one adult weighing machine to record weights of adolescent girls and pregnant/lactating women, second salter weighing machine to weigh the children of 3-6 age group and the third machine to weigh young children below three years of age. A growth chart register is provided to keep a record of weight and age of the children enrolled in anganwadi center.
3. Nutrition and Health Counseling - Anganwadi workers are trained to impart Nutrition and Health Counseling to the women enrolled in AWC. This forms part of BCC (Behaviour Change Communication) strategy. This has the long term goal of capacity-building of women especially in the age group of 15-45 years so that they can look after their own health, nutrition and development needs as well as that of their children and families.
4. Immunization - Immunization of pregnant women and infants protects children from six vaccine preventable diseases-poliomyelitis, diphtheria, pertussis, tetanus, tuberculosis and measles. These are major preventable causes of child mortality, disability, morbidity and related malnutrition. Immunization of pregnant women against tetanus also reduces maternal and neonatal mortality. The Ministry of Health and Family Welfare deliver this service under its Reproductive Child Health (RCH) programme. In addition, the Iron and Vitamin "A" supplementation to children and pregnant women is done under the RCH programme of the Ministry of Health and Family Welfare.
5. Basic Health Care - This includes health care of children less than six years of age, antenatal care of expectant mothers and postnatal care of nursing mothers. The ANM, Sub Health Centres and Primary Health Centres provide these services. The various health services include regular health check-ups, immunization, management of malnutrition, treatment of diarrhea, deworming and distribution of simple medicines etc.
6. Referral Services - During health check-ups and growth monitoring, sick or malnourished children, in need of prompt medical attention, are referred to Nutritional
Moribund ICDS27
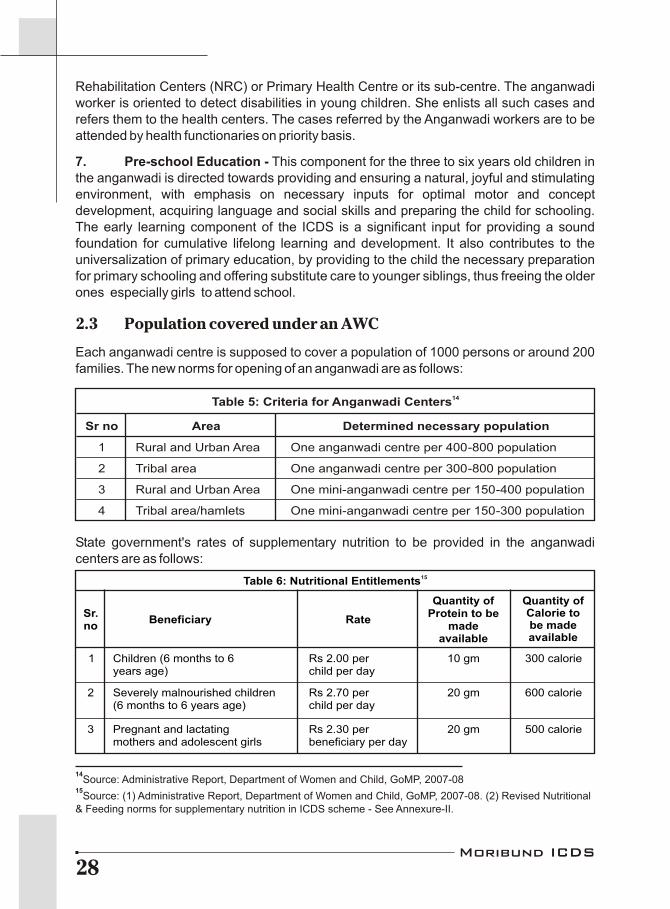
14Source: Administrative Report, Department of Women and Child, GoMP, 2007-08
15Source: (1) Administrative Report, Department of Women and Child, GoMP, 2007-08. (2) Revised Nutritional
& Feeding norms for supplementary nutrition in ICDS scheme - See Annexure-II.
Rehabilitation Centers (NRC) or Primary Health Centre or its sub-centre. The anganwadi worker is oriented to detect disabilities in young children. She enlists all such cases and refers them to the health centers. The cases referred by the Anganwadi workers are to be attended by health functionaries on priority basis.
7. Pre-school Education - This component for the three to six years old children in the anganwadi is directed towards providing and ensuring a natural, joyful and stimulating environment, with emphasis on necessary inputs for optimal motor and concept development, acquiring language and social skills and preparing the child for schooling. The early learning component of the ICDS is a significant input for providing a sound foundation for cumulative lifelong learning and development. It also contributes to the universalization of primary education, by providing to the child the necessary preparation for primary schooling and offering substitute care to younger siblings, thus freeing the older ones especially girls to attend school.
2.3 Population covered under an AWC
Each anganwadi centre is supposed to cover a population of 1000 persons or around 200 families. The new norms for opening of an anganwadi are as follows:
State government's rates of supplementary nutrition to be provided in the anganwadi centers are as follows:
14Table 5: Criteria for Anganwadi Centers
Sr no Area Determined necessary population
1 Rural and Urban Area One anganwadi centre per 400-800 population
2 Tribal area One anganwadi centre per 300-800 population
3 Rural and Urban Area One mini-anganwadi centre per 150-400 population
4 Tribal area/hamlets One mini-anganwadi centre per 150-300 population
Table 6: Nutritional Entitlements15
Sr. no
Beneficiary Rate
Quantity of Protein to be
made available
Quantity ofCalorie to be madeavailable
1 Children (6 months to 6 years age)
Rs 2.00 per child per day
10 gm 300 calorie
2 Severely malnourished children(6 months to 6 years age)
Rs 2.70 per child per day
20 gm 600 calorie
3 Pregnant and lactating mothers and adolescent girls
Rs 2.30 per beneficiary per day
20 gm 500 calorie
Moribund ICDS28

2.4 The Truth of Universalisation of ICDS thSupreme Court of India in its order dated 29 April 2004 mentions the definition of
Universalization of ICDS by saying that all the Children under the age of 6 years, all the Pregnant and Lactating Women and all the Adolescent Girls must be provided with all seven services from the ICDS center, but latest report from DWCD provides information that still 60% children and more then 73% eligible women are out of the focus.
ICDS in the field
ICDS is one of the biggest and the only scheme which addresses the nutritional needs of children in the age group 0-6 which comprises of 16 per cent of the total population in the State according to Census 2001. But the performance of ICDS in the field is not complying with its objectives of reaching the beneficiaries with adequacy. The Seventh Report of the Commissioners of the Supreme Court stated that as per Census 2001 as many as 6.6 million children should be enrolled in anganwadis that are running under ICDS in Madhya Pradesh. But only 3.89 million, (35.9 percent of total children population), gets the supplementary nutrition from the State through Anganwadis, indicating ICDS benefits are not reaching even to all the malnourished children of state considering the severity of the problem.
State government with the assistance from United Nation's Children Fund (UNICEF) and World Food Programme (WFP) launched special schemes like Bal Shakti Yojana, Shaktimaan and the Bal Sanjeevani Abhiyan to reach out severely malnourished children. All these schemes are being implemented under the umbrella of ICDS but have been failed to contribute in tackling the problem of malnutrition. If budgetary allocation of funds is any indication, then state government is spending 0.86 percent of its total budget for the children under six.
Another key component of the ICDS is the supplementary feeding that is being provided to the beneficiaries including children in the age group from 6 months to 6 years, pregnant and nursing mothers and adolescent girls. But in reality this basic service has come to a grind halt in most of the Anganwadi centers of the State mentioned the field reports. Major blockade in reaching the supplementary
"Contractors should not be engaged in for the supplying nutritional food in anganwadi's, but it shall be utilize the services of village communities, self help groups and mahila mandals in the villages"
Dilution of SupremeCourt's Orders
In the light of vested interests and rampant corruption in the present system, the Supreme Court of India has given strict directions four years back to all the State governments stating "Contractors should not be engaged in for the supplying nutritional food in anganwadi's, but it shall be utilize the services of village communities, self help groups and mahila mandals in the villages". The system of having the nutritional food supplied through these groups has many advantages. First and foremost among them is the fact that it would bring about a definite change in the economic condition of women through income and employment generation. And secondly the system would also pave the way for the community to have closer links with ICDS implementation. Further it will also strengthen the involvement of local institution i.e. Panchayati Raj through decentralized supply of SNP. But despite the orders from Supreme Court the State government is promoting the distribution and supply of the supplementary nutrition food to the Anganwadi Centers through contractors or private firms by sidelining the local community based initiatives.
Box - 11
Moribund ICDS29

feeding to the beneficiaries is the fact that this entire programme is into the hands of private contractors over the years; who are supplying ready to eat food powders. These readymade foods are not culturally acceptable, calorie wise inadequate and in many of the cases never reached the ICDS centers at all.
Another side of the story is that the state government is promoting the supply of Ready to Use Energy Food (RUEF) and Ready to Use Therapeutic Food (RUTF) under strategic guidance of non-governmental agencies and corporate alliances like Global Alliance for Improved Nutrition (GAIN). This will gradually destroy the traditional food habits of the indigenous people. Though it is true that such ready to eat food is a boon to tackle the problem of acute malnutrition but at the same time one has to be cautious because presently these foods are the imported one and its impact on indigenous population of India is yet to be tested. The most critical question arises here is how the government could promote the use of ready to eat foods without being tested in the first place and secondly would this imported food component be a sustainable solution to tackle the problem of malnutrition in our State? Can't the RUTF be replaced with some locally procured alternatives or can't we have locally produced RUTF?
2.5 Status of ICDS in Madhya Pradesh
l Total population (under the age of 6 Years) - 1.078 Crore
17l Total Children covered under SNP - 4390624
18l Proportion of children covered - 40.72%
19l Total pregnant and lactating women - 36 Lakh
l Actual benefited women in this category - 9 Lakh
l Proportion of women covered - 26.5%
l Number of adolescent girls age (11-17) - 64 Lakhs
l Proportion of adolescent girls covered - Nil
2.6 Allocation for Travel and Fuel
On one hand, in the past 3 years rates of petroleum products have been increased more than 25 percent and on the other hand 20000 new anganwadi centers have been opened in the same period. Thus it requires substantial increase in allocation for Fuel and Oil for the field visits under ICDS implementation. But actually it has gone down heavily by nearly half
16Source: Note has been prepared by Right to Food Campaign Support Group Madhya Pradesh.
Administrative report 2007-08, Department of Women and Child Development, Govt of MP, Page 17.18
Administrative report 2007-08, Department of Women and Child Development, Govt. of MP, Page 17.19
Calculated as per the population growth rate 3.2% per year in Madhya Pradesh. It includes 24 lakh pregnant women and 12 lakh lactating women.
Moribund ICDS30

20Budget Book Demand for Department of Women and Child Development for the Year 2008-09 page 24.
21Budget Book Demand for Department of Women and Child Development for the Year 2008-09 page 24.
22Budget Book Demand for Department of Women and Child Development for the Year 2008-09 page 24.
23Informations and Data provided in this section are based on the informations provided by the
Department of Women and Child Development under Right to Information on 15th December 2008.
the rate from 0.72 percent in 2006-07 to 0.35 percent in 2008-09 as a percentage of total departmental budget for this head.
20l Year 2006-07 - Rs. 2.18 Crore (0.72% of the total Expenditure)
21l Year 2007-08 - Rs. 2.985 Crore (0.55% of the total Expenditure)
22l Year 2008-09 - Rs. 2.179 Crore (0.35% of the total Expenditure)
District officials including District Women and Child Development Officer and District project Officers-DPO in the Department of Women and Child Development gets an amount of Rs. 50000 per year for Vehicle and Fuel. Unfortunately, the amount has remained unchanged in the past five years. It has a practical implication on the effectiveness of the scheme, because of it's directly link to the monitoring mechanism of the scheme.
But on the same line allocations for the transportation of professional/expert services has been increased from Rs13.92 lakh in 2006-07, to Rs 41.86 lakh in 2007-08 and to whopping high at Rs 1.02 crore in the year 2008-09. This increase in meant for the transportation of contractual staff, professional experts etc, but not for the field staff.
232.7 No more Medicine Kits in ICDS
It is an essential component of the ICDS services, where Anganwadi worker has been trained to provide initial medicinal support for symptoms like itching, injury, de-worming etc through medicine kit component. For this purpose there is a system to ensure the availability of essential medicines through Medicine Kit in all anganwadi centers. These medicine kits should contain prescribed drugs, so that motive of the program could be fulfilled and basic health problems are addressed at the very primary level. Unfortunately, there is no separate provision of budget allocation for the medicine kits under ICDS for the past two years but a minimum possible amount on the basis of tenders received is spent on buying medicine kits for Anganwadi Centers. Moreover, the medicines kept in these kits are not according to the need of a particular area but these are according to a fixed chart depicting which medicines should be kept. This shows how sensitive is our government towards the health of unborn and young children; the next generation of the State.
2.8 What is a Medicine Kit in ICDS?
As per the Government of India norms following drugs should be available in each medicine kit
1. Paracetamol Tablets IP 500 mg - 500 Tablets.
2. Paracetamol Syrup IP 125 mg - 1 Bottle
Moribund ICDS31

3. Mebendazole Tablets - 450 Tablets
4. Benzyl Benzoate Lotion - 500 ML Bottle
5. Chloramphenicol Eye Ointment - 10 Tubes
6. Sulphacetamide Sodium Eye drop - 6 Vials
There is no specific budget provision for purchasing medicines for Anganwadi Centers. Department of Women and Child Development procure the medicines from the budget they are allocated for overall ICDS project. These drugs are procured under a tender based purchasing system it means it is not a part of any ongoing Health program and Department of Women and Child Development has to make provisions in their budget, so that medicine kits could be provided to the Anganwadi centers regularly.
We started with analyzing the programmatic systems and budget provision issues related to availability of medicine kits, we started. The finding of policy level analysis gave a shocking sketch.
2.9 Provision of Budget
It is interesting to see the budget allocations for medicine kits. The informations provided by the Department of WCD for this study makes it clear that the allocations are too little when compared to actual need.
In the Year 2002-03, State Government made an allocation of Rs 268.47 Lakhs for 47433 Anganwadi Centres (AWCs). This comes out to be Rs 5.65 in 2002-03 and Rs 5.74 in 2005-06 for the proposed medi-cine kit comprising essential drugs. Considering the large quantities of medicines required the allocation is too little. Allocations for medi-cine kits continued until 2005-06 only and then no allocations were made for the medicine kits. It seems that, ICDS has been de-linked from the mandate of basic health care services envisaged in larger perspective.
2.10 Growth charts vs. Monitoring of growth
Growth charts or weight charts are to be kept with the anganwadi worker for the purpose of recording the weight of the child up to the age of 6 years. The growth of the child is required to be monitored through this chart where the anganwadi worker is expected to record the child's weight every month. It is also to be used as an educational tool to teach mother to
Moribund ICDS32
Table 7: Budget for Medicine Kit
Sr No.
Year Allocated Budget
Covered AWCs
Allocation per
Medicine Kit
1 2002 -03 268.47 Lakhs 47433 Rs. 5.65
2 2003 -04 275.18 Lakhs
49784 Rs. 5.52
3 2004 -05 290.18 Lakhs
49784 Rs. 5.84
4 2005 -06 340.67 Lakhs
59324 Rs. 5.74
5 2006 -07 No allocation 59324 Nil
6 2007 -08 No allocation 69238 Nil
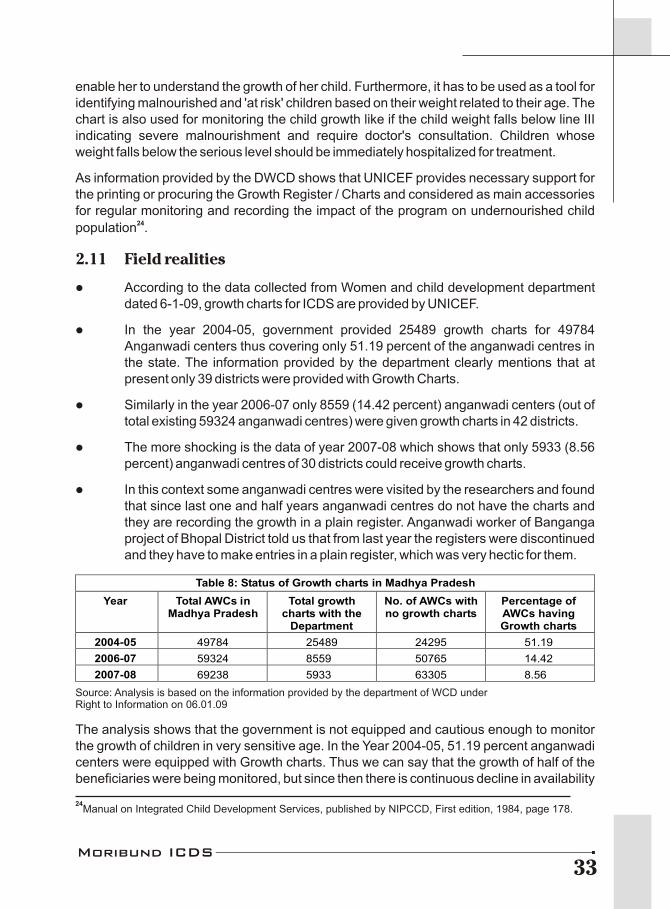
enable her to understand the growth of her child. Furthermore, it has to be used as a tool for identifying malnourished and 'at risk' children based on their weight related to their age. The chart is also used for monitoring the child growth like if the child weight falls below line III indicating severe malnourishment and require doctor's consultation. Children whose weight falls below the serious level should be immediately hospitalized for treatment.
As information provided by the DWCD shows that UNICEF provides necessary support for the printing or procuring the Growth Register / Charts and considered as main accessories for regular monitoring and recording the impact of the program on undernourished child
24population .
2.11 Field realities
l According to the data collected from Women and child development department dated 6-1-09, growth charts for ICDS are provided by UNICEF.
l In the year 2004-05, government provided 25489 growth charts for 49784 Anganwadi centers thus covering only 51.19 percent of the anganwadi centres in the state. The information provided by the department clearly mentions that at present only 39 districts were provided with Growth Charts.
l Similarly in the year 2006-07 only 8559 (14.42 percent) anganwadi centers (out of total existing 59324 anganwadi centres) were given growth charts in 42 districts.
l The more shocking is the data of year 2007-08 which shows that only 5933 (8.56 percent) anganwadi centres of 30 districts could receive growth charts.
l In this context some anganwadi centres were visited by the researchers and found that since last one and half years anganwadi centres do not have the charts and they are recording the growth in a plain register. Anganwadi worker of Banganga project of Bhopal District told us that from last year the registers were discontinued and they have to make entries in a plain register, which was very hectic for them.
The analysis shows that the government is not equipped and cautious enough to monitor the growth of children in very sensitive age. In the Year 2004-05, 51.19 percent anganwadi centers were equipped with Growth charts. Thus we can say that the growth of half of the beneficiaries were being monitored, but since then there is continuous decline in availability
Table 8: Status of Growth charts in Madhya Pradesh
Year Total AWCs in Madhya Pradesh
Total growthcharts with the
Department
No. of AWCs with no growth charts
Percentage of AWCs having Growth charts
2004-05
2006-07
2007-08
49784
59324
69238
25489
8559
5933
24295
50765
63305
51.19
14.42
8.56
Source: Analysis is based on the information provided by the department of WCD underRight to Information on 06.01.09
24Manual on Integrated Child Development Services, published by NIPCCD, First edition, 1984, page 178.
Moribund ICDS33

of this essential document. The availability declined from 51.19 percent to 8.56 percent. Growth chart is actually a register, representing the monthly weight gain and growth of a child in a simple way with line or bar diagrams. The graphical picture helps the illiterate mother to enable her to understand the growth of her child but the complicated entries in registers makes them difficult to learn the things. Further more the government has discontinued the supply of charts without intimating the AWW and without knowing the need after 2007-2008.
2.12 Nutrition component testing
At present there are 69238 anganwadi centres being run by the Madhya Pradesh Government and are providing supplementary nutrition to more then 53 lakh (5.3 million) beneficiaries for 300 days in a year as claimed by the DWCD. But for such a big effort there is no support for the testing of the quality of material being provided under supplementary nutrition by the state government.
There is norm in the scheme and from the Supreme Court Order on the nutritional component that each and every child should receive 300 calorie and 8-10 gram protein from the ICDS centers. Earlier for checking this component department used to send samples of nutrition to the Labs located in Mumbai or Delhi. The report of Comptroller and Auditor General has also pointed out that in Madhya Pradesh ICDS System is not fulfilling the criteria of 300 Calorie and 8-10 Gram protein being provided through anganwadi centers.
2.13 Targeted population Vs Actual Coverage
As per Monthly Progress Report (MPR) for the month of May' 2008 available on the website of Department of Women and Child Development shows that the total population of Children under 6 years is 86.96 lakhs, but as per the Census 2001, the population of this age group is 1.078 Crore. It means the existence of approximately 2.1 Million Children is still out of the focus. Government is reporting that it is providing supplementary nutrition to 45.28 lakh children under the 6 years age, thus it is covering only 42% of the total child population if one goes by the provisions under Universalization of ICDS.
When the implementation and coverage analysis in terms of budget provision was done, it was found that the state government is allocating only Rs. 0.84 per beneficiary, but is claiming the spending of Rs. 2 per beneficiary in all its key statement responses. On the other side, if we believe that Government has spent Rs. 2 per beneficiary per day in the allotted budget, then it means all the covered (not the actual population) beneficiaries will get Supplementary Nutrition for 126 days only in a year, whereas it should have been for at least 300 days in a year, as per the Supreme Court Order. Thus this shows a case of complete negligence and violation of norms of Special Nutrition Program.
2.14 Human Resources: Vacant posts, a bitter truth
In ICDS program, Child Development Project Officer (CDPO) is a key person to ensure the proper implementation of ICDS services. This person is a bridge between field
Moribund ICDS34
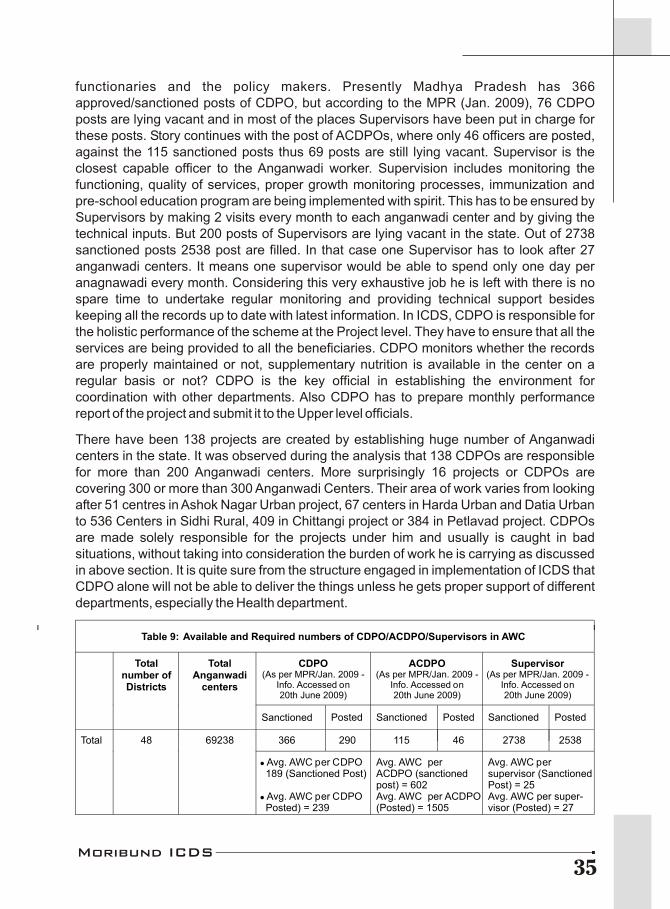
functionaries and the policy makers. Presently Madhya Pradesh has 366 approved/sanctioned posts of CDPO, but according to the MPR (Jan. 2009), 76 CDPO posts are lying vacant and in most of the places Supervisors have been put in charge for these posts. Story continues with the post of ACDPOs, where only 46 officers are posted, against the 115 sanctioned posts thus 69 posts are still lying vacant. Supervisor is the closest capable officer to the Anganwadi worker. Supervision includes monitoring the functioning, quality of services, proper growth monitoring processes, immunization and pre-school education program are being implemented with spirit. This has to be ensured by Supervisors by making 2 visits every month to each anganwadi center and by giving the technical inputs. But 200 posts of Supervisors are lying vacant in the state. Out of 2738 sanctioned posts 2538 post are filled. In that case one Supervisor has to look after 27 anganwadi centers. It means one supervisor would be able to spend only one day per anagnawadi every month. Considering this very exhaustive job he is left with there is no spare time to undertake regular monitoring and providing technical support besides keeping all the records up to date with latest information. In ICDS, CDPO is responsible for the holistic performance of the scheme at the Project level. They have to ensure that all the services are being provided to all the beneficiaries. CDPO monitors whether the records are properly maintained or not, supplementary nutrition is available in the center on a regular basis or not? CDPO is the key official in establishing the environment for coordination with other departments. Also CDPO has to prepare monthly performance report of the project and submit it to the Upper level officials.
There have been 138 projects are created by establishing huge number of Anganwadi centers in the state. It was observed during the analysis that 138 CDPOs are responsible for more than 200 Anganwadi centers. More surprisingly 16 projects or CDPOs are covering 300 or more than 300 Anganwadi Centers. Their area of work varies from looking after 51 centres in Ashok Nagar Urban project, 67 centers in Harda Urban and Datia Urban to 536 Centers in Sidhi Rural, 409 in Chittangi project or 384 in Petlavad project. CDPOs are made solely responsible for the projects under him and usually is caught in bad situations, without taking into consideration the burden of work he is carrying as discussed in above section. It is quite sure from the structure engaged in implementation of ICDS that CDPO alone will not be able to deliver the things unless he gets proper support of different departments, especially the Health department.
Table 9: Available and Required numbers of CDPO/ACDPO/Supervisors in AWC
CDPO(As per MPR/Jan. 2009 -
Info. Accessed on20th June 2009)
ACDPO(As per MPR/Jan. 2009 -
Info. Accessed on20th June 2009)
Supervisor(As per MPR/Jan. 2009 -
Info. Accessed on20th June 2009)
Sanctioned
Posted
Sanctioned
Posted
Sanctioned
Posted
366 290 115 46 2738 2538 Total 48 69238
l Avg. AWC per CDPO 189 (Sanctioned Post)
l Avg. AWC per CDPO Posted) = 239
Avg. AWC perACDPO (sanctionedpost) = 602Avg. AWC per ACDPO(Posted) = 1505
Avg. AWC persupervisor (SanctionedPost) = 25Avg. AWC per super-visor (Posted) = 27
Total Anganwadi
centers
Total number of Districts
Moribund ICDS35

2.15 Nutritional Rehabilitation Centers
As we all know that 60 percent of children in the State are suffering from malnutrition and moreover alarmingly 13 lakh children are on the verge of death being severely malnourished. In order to tackle the issue, state government is running a scheme called Balsanjeevni Abhiyan to check the problem of malnutrition. Outcomes of this scheme are magical in the sense that it claims that the number of malnourished children get noticeably decreased with every round of Bal Sanjivani with an interval of six months.
Like Balsanjeevni many more initiatives have been taken by the State Administration to tackle the malnutrition by involving Health Department. Starting NRC last year, is one more such scheme which includes an important component of referral services provided under ICDS through anganwadi Centers. Functioning of NRC is a joint responsibility of WCD as well as Health departments. Severely malnourished children that are falling in the category of grade 3 and grade 4) along with their parents preferably anganwadi worker refers the mother of a child to NRCs. Children can be kept in NRC at least for a period of 14 days. During this treatment period, every child is given special treatment in terms of nutrition, health and psychological as well as social development. NRC at the district level is having 20 beds and 10 beds at the block level. Categorically Department of Health has to play a very crucial role in malnutrition eradica-tion efforts through institutional channel like NRCs for addressing issues of severe malnourished children. NRCs are established in District Hospitals or Community Health Centers (CHCs) run by the Health Department.
Each NRC is suppose to be a well maintained center with a neat and clean environment, a kitchen and facility of safe drinking water, separate toilets for parents and children and a recreation room with plenty of educational toys for children. A Nutritionist and Child specialist along with sufficient trained staffs are posted in each NRC to take care of malnourished children. Once the children are cured of malnutrition and all subsequent infec-tions, they are relieved from NRC and it is expected to undertake a regular follow up at the intervals of 15 days, 1 month, 3 months and 6 months.
All these provisions for a standard NRC are posing a picture perfect situation with
Budget of NRC
Let us take a look at the budget component of NRC. An ideal NRC with 20 beds has been allotted an amount of Rs. 2160/- per child for 14 days. The amount includes cost of food @ Rs 25 per day for the child, wages compensation of 14 days and the food costing @ Rs 65 per day for the mother of child along with travel expenses (@ Rs 200/-) and the stipend (Rs. 100/- per child) given to Anganwadi worker for bringing the child to NRC. Along with fulfilling all these requirements, we can now imagine that how much money is being is being left for the medicines and supplementary nutrition of the child; its astonishing only Rs. 600/- for 14 days! Similarly, to establish NRC with kitchen, recreational room, treatment ward, separate toilets and other basic requirements, a sum of only 1. 35 lakhs is being sanctioned. Also the budgetary provision meant for the follow-up process is kept too little. It's a gigantic question in front of development practitioners that with such inadequate resources at hand, how the state government would be able to check the horrendous situation of malnutrition in the state?
Box - 12
Moribund ICDS36
good and effective place to cure the malnutrition among the children. But once again the reality bites are very extremely in which the concept of NRC is being implemented in the field. To take care of 13 lakh severely malnourished children in the State there are only 135 NRCs that have been established so far. Moreover, out of these only 95 centers are fully functional while 40 NRCs are partially functional. There is a facility of merely 1678 beds to take care suffering children and alarmingly 49 NRCs do not have trained staff. In such pity circumstances, even if every thing functions properly in the system, it will take long 33 years to reach and serve all the severely malnourished children in the state.
We would like to throw more light on the grim situation on the field on account of dichotomy in registering the malnutrition cases. Although the four districts namely, Satna, Khandwa, Sheopur and Shivpuri where deaths of 325 malnourished children have been reported between May to September 2008, the number of malnourished children admitted in the NRC centers is either nil or negligible. On this basis the state administration use to point out that there is no severe malnutrition in the districts. But when the local organizations and media continuously raised the issue of malnutrition deaths than suddenly the NRC centers of these districts get flooded with malnourished children. Nearly 100 children were admitted in Khandwa NRC while it had the capacity of only 20 children. 40 children were admitted in Satna district and similar was the conditions of NRCs of Sheopur and Shivpuri districts. Thus with this the question arises here that would it be possible that would there not be any cases of malnutrition in other district as well? Also if there are malnourished children in other districts, then why the NRCs are not reporting any?
One more lacuna observed in the operational system of NRC is lack of any co-ordination between the NRC center and field staff i.e. anganwadi worker under ICDS. For example, there is no means by which anganwadi worker would come to know whether there is a vacant place to admit a new (malnourished) child in the center or not. Another major drawback is that the child admitted in NRC is essentially relieved from the center in 14 days, no matter whether he/she is fully cured off malnutrition and infection or not! The follow-up system of children relieved from NRCs is also very weak due to which the children dies even after being treated in NRC in the absence of continued treatment. All these lacunae show that there is a great need of establishing a proper co-ordination among the implementing agencies.
2.16 Few more observations based on the Rapid Assessment Study of 25NRC
In order to collect the facts and actually analyze the ground veracities of the situations of NRCs in the State, 23 NRCs of 14 districts were studied by the Right to Food Campaign Madhya Pradesh Support Group. Following observations were revealed from the filed study:
l There were total of 16638 severely malnourished children found in the selected NRCs of 14 studied districts.
25Conducted by Organizations working on Right to Food issues in Madhya Pradesh in Dec. 2008 - Feb. 2009
Moribund ICDS37
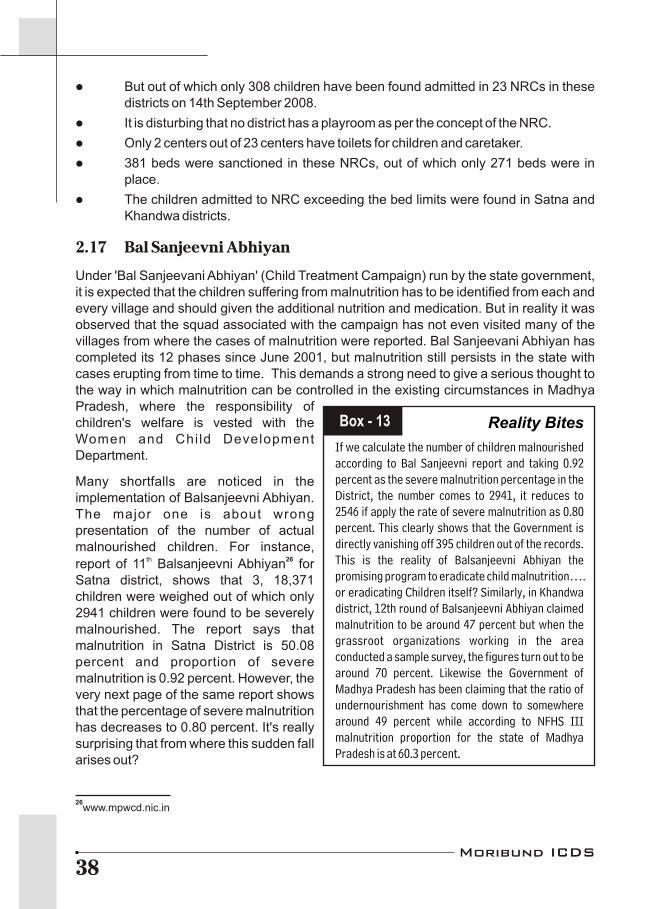
l But out of which only 308 children have been found admitted in 23 NRCs in these districts on 14th September 2008.
l It is disturbing that no district has a playroom as per the concept of the NRC.
l Only 2 centers out of 23 centers have toilets for children and caretaker.
l 381 beds were sanctioned in these NRCs, out of which only 271 beds were in place.
l The children admitted to NRC exceeding the bed limits were found in Satna and Khandwa districts.
2.17 Bal Sanjeevni Abhiyan
Under 'Bal Sanjeevani Abhiyan' (Child Treatment Campaign) run by the state government, it is expected that the children suffering from malnutrition has to be identified from each and every village and should given the additional nutrition and medication. But in reality it was observed that the squad associated with the campaign has not even visited many of the villages from where the cases of malnutrition were reported. Bal Sanjeevani Abhiyan has completed its 12 phases since June 2001, but malnutrition still persists in the state with cases erupting from time to time. This demands a strong need to give a serious thought to the way in which malnutrition can be controlled in the existing circumstances in Madhya Pradesh, where the responsibility of children's welfare is vested with the Women and Chi ld Development Department.
Many shortfalls are noticed in the implementation of Balsanjeevni Abhiyan. The major one is about wrong presentation of the number of actual malnourished children. For instance,
th 26report of 11 Balsanjeevni Abhiyan for Satna district, shows that 3, 18,371 children were weighed out of which only 2941 children were found to be severely malnourished. The report says that malnutrition in Satna District is 50.08 percent and proportion of severe malnutrition is 0.92 percent. However, the very next page of the same report shows that the percentage of severe malnutrition has decreases to 0.80 percent. It's really surprising that from where this sudden fall arises out?
Reality Bites
If we calculate the number of children malnourished according to Bal Sanjeevni report and taking 0.92 percent as the severe malnutrition percentage in the District, the number comes to 2941, it reduces to 2546 if apply the rate of severe malnutrition as 0.80 percent. This clearly shows that the Government is directly vanishing off 395 children out of the records. This is the reality of Balsanjeevni Abhiyan the promising program to eradicate child malnutrition…. or eradicating Children itself? Similarly, in Khandwa district, 12th round of Balsanjeevni Abhiyan claimed malnutrition to be around 47 percent but when the grassroot organizations working in the area conducted a sample survey, the figures turn out to be around 70 percent. Likewise the Government of Madhya Pradesh has been claiming that the ratio of undernourishment has come down to somewhere around 49 percent while according to NFHS III malnutrition proportion for the state of Madhya Pradesh is at 60.3 percent.
Box - 13
26www.mpwcd.nic.in
Moribund ICDS38
Persistence of malnutrition among tribal belt has many reasons like lack of anganwadi centers in the tribal areas, lack of timely and regular vaccination, non-distribution of regular nutrition etc. But the foremost reason is non-availability of adequate livelihood opportunities so that the people can get enough food for both meals, and do not reach the stage of malnutrition. But this is not happening and in fact the situation has deteriorated, which is why as compared to the 53.5 percent children below 3 years suffering from
27malnutrition in 1998-99 the number has risen to 60.3 percent in 2005-06 and the number 28of those children below 3 years breastfed within one hour of birth is 14 percent.
2.18 Targeted Public Distribution System in MPthThe Supreme Court in its order dated 8 May 2002 gave the clear directions that the PDS
shops should remain open throughout the month during fixed hours. Also details of what the ndshop would contain shall be displayed on the notice board. In its order dated 2 May 2003,
the Supreme Court further directed that the licenses of those who do not keep their shops open throughout the month during the stipulated period would be cancelled. In the same order, the Supreme Court directed to permit BPL families to purchase grain in installments.
But the ground realities of TPDS are not at all in consonance with the direction of Supreme Court. In Madhya Pradesh the TPDS shops are kept open only for 3-4 days instead of the
29whole month . Also, the norms for the amount of ration allocated through the shops is 35 kg for Antyoday Anna Yojna (AAY) card holder and 20 kg for BPL card holders while the actual amount of ration being allocated is different in different districts. For instance, in Karahal block of Sheopur district 32 kg ration is being provided to AAY card holders while in Satna
30 the ration allocated to AAY card holding families is only 20 kg . This deformity in ration supply is also one of the factors responsible for prevailing food crisis among the poor population of the State.
2.19 Midday Meal Scheme
A survey of Indian Council of Social Science Research (ICSSR) in year 2004 survey concluded, "The shift to a ruchikar (relishing) mid-day meal in Madhya Pradesh in 2004 marks a dramatic improvement over the earlier daliya-based meal. The ruchikar meal is being provided with fair regularity in most schools across the state. The meal is an immense contribution to overcoming classroom hunger for millions of children whose families may
31 have been unable to provide them food. However, in Madhya Pradesh, the sorry state of
27Fact sheet of National Family Health Survey-III
28Fact sheet of National Family Health Survey-III
29Real stories of Public Distribution System Document of case studies collected during the state level public
hearing conducted by Right to Food Campaign Madhya Pradesh Support Group in collaboration with Sampark& Sopan in Bhopal on 28th December'04.30
As revealed in the field survey done by Saheriya Mukti Morcha (Karahal) and Right to Food CampaignSupport Group of MP (Satna)31
Shah, M. & J. Jain (2005): Antyodaya Anna Yojana and Mid-day Meals in Madhya Pradesh:Findings of a Survey in Seven Districts, Economic and Political Weekly, 26th November
Moribund ICDS39
primary education renders the MDMS almost ineffective. In almost every school in the state, the actual number of teachers is less than the sanctioned number of posts. As a result, many of the government primary schools in the state are highly understaffed; on an average a primary teacher in rural parts of State handle about 100 pupils in most of the
32schools . As a result schools do not open every day and hence midday meals are served only on those days when the school opens. Satna, Khandwa, Sheopur and Shivpuri all are drought affected regions. According to orders of Supreme Court, MDM should be made available in the schools of drought affected areas even during the summer vacation. But the field reality is something very different. The local organizations working in these districts reported about the irregular allocation of MDM not only during the summer vacation but also during the complete past years.
32A survey conducted by National Institute of Education Planning and Administration, 2003.
Actions all acrossActions all across
As mentioned, 62 children died in Khandwa in the span of 4 months from June to September 2008. These deaths were exposed by the efforts of local organisation Spandan & Media. After that a fact-finding report was subsequently submitted to the Supreme Court Commissioner. In response the Supreme Court Commissioner send a 16 points recommendation to the district administration asking for instant actions and report within 15 days. They also urge to provide 35 Kgs of food grains every month to all the BPL and AAY card holder. The recommendations by the Supreme Court and the continuous pressure of community's agitation, actions of people's organizations and media forced the administrative authority to provide relief for the children in the villages. Hundreds of children were brought to the Nutrition Rehabilitation Centres (NRC; Bal Shakti Kendras) and the Shaktiman project was introduced in 299 Child Care Centre (Anganwadi centre; AWC) all over the district. The NRC is a child rights structure to treat malnourished children living in remote forest villages. The Shaktiman project was launched in 2007 to ensure nutrition for children with a focus on predominantly tribal areas in MP.
Few months back “The Asian Human Rights Commission (AHRC)” started intervening in the matter. The AHRC has also written a separate letter to the UN Special Rapporteur on the Right to Food calling for intervention. They commission regularly keep an eye on government action regarding the victims and their family. They also release an appeal and update in the month of April & May 2009 for the cause. In one of their appeal they mentioned that on 8 May 2009, the district government officially announced that they would issue the AAY ration cards within three days to all families who had lost children due to malnutrition in 2008. It means that the government has admitted the fact that the children died of malnutrition and intends to take responsibility for their deaths.
This case study has been observed by Spandan Samaj Sevi Sanstha, Khandwa . (June 2009)
Moribund ICDS40
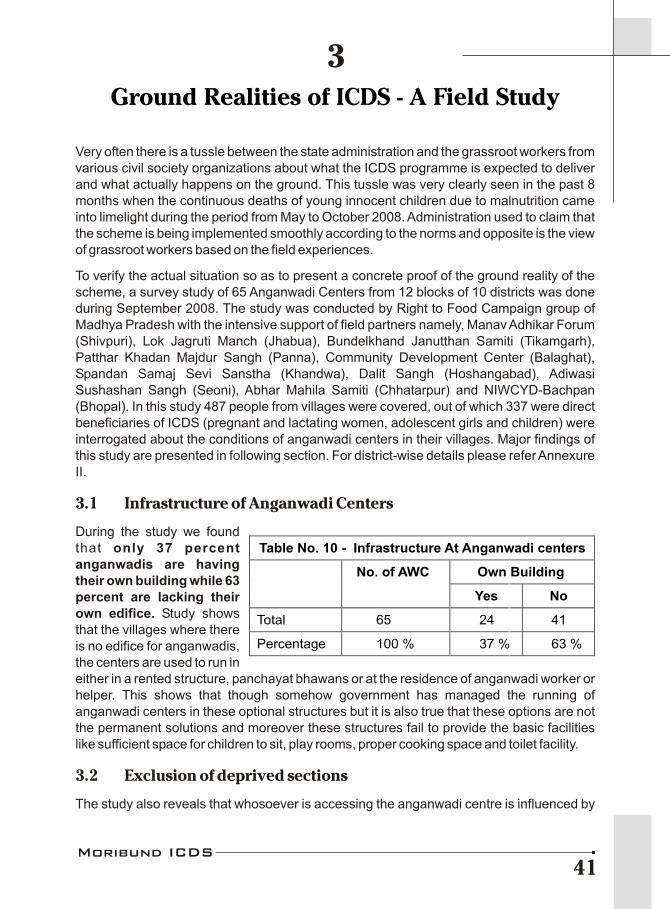
Ground Realities of ICDS - A Field Study
3
Very often there is a tussle between the state administration and the grassroot workers from various civil society organizations about what the ICDS programme is expected to deliver and what actually happens on the ground. This tussle was very clearly seen in the past 8 months when the continuous deaths of young innocent children due to malnutrition came into limelight during the period from May to October 2008. Administration used to claim that the scheme is being implemented smoothly according to the norms and opposite is the view of grassroot workers based on the field experiences.
To verify the actual situation so as to present a concrete proof of the ground reality of the scheme, a survey study of 65 Anganwadi Centers from 12 blocks of 10 districts was done during September 2008. The study was conducted by Right to Food Campaign group of Madhya Pradesh with the intensive support of field partners namely, Manav Adhikar Forum (Shivpuri), Lok Jagruti Manch (Jhabua), Bundelkhand Janutthan Samiti (Tikamgarh), Patthar Khadan Majdur Sangh (Panna), Community Development Center (Balaghat), Spandan Samaj Sevi Sanstha (Khandwa), Dalit Sangh (Hoshangabad), Adiwasi Sushashan Sangh (Seoni), Abhar Mahila Samiti (Chhatarpur) and NIWCYD-Bachpan (Bhopal). In this study 487 people from villages were covered, out of which 337 were direct beneficiaries of ICDS (pregnant and lactating women, adolescent girls and children) were interrogated about the conditions of anganwadi centers in their villages. Major findings of this study are presented in following section. For district-wise details please refer Annexure II.
3.1 Infrastructure of Anganwadi Centers
During the study we found that only 37 percent anganwadis are having their own building while 63 percent are lacking their own edifice. Study shows that the villages where there is no edifice for anganwadis, the centers are used to run in either in a rented structure, panchayat bhawans or at the residence of anganwadi worker or helper. This shows that though somehow government has managed the running of anganwadi centers in these optional structures but it is also true that these options are not the permanent solutions and moreover these structures fail to provide the basic facilities like sufficient space for children to sit, play rooms, proper cooking space and toilet facility.
3.2 Exclusion of deprived sections
The study also reveals that whosoever is accessing the anganwadi centre is influenced by
Table No. 10 - Infrastructure At Anganwadi centers
Own Building No. of AWC
Yes No
Total 65 24 41
Percentage 100 % 37 % 63 %
Moribund ICDS41
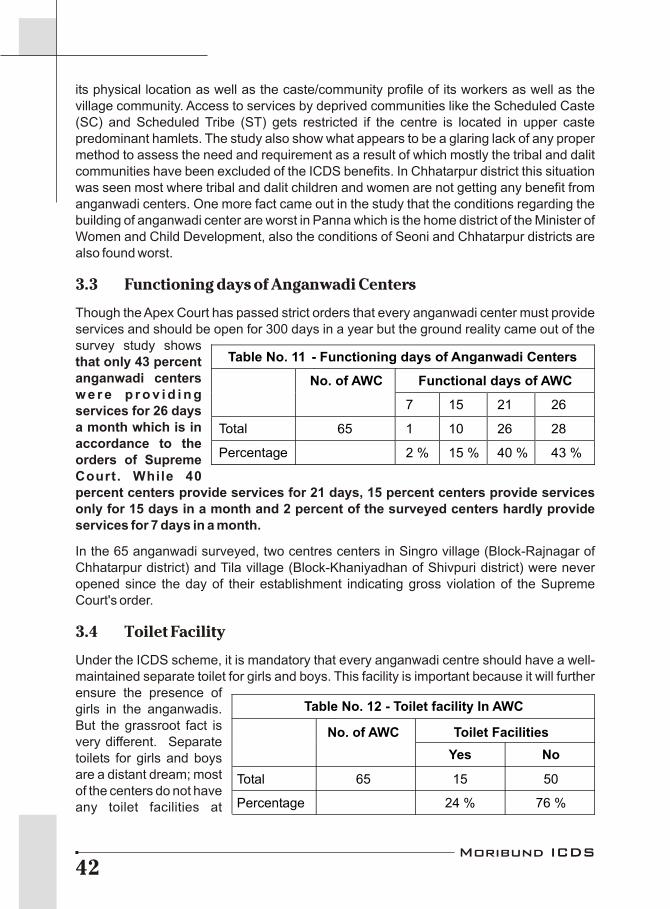
its physical location as well as the caste/community profile of its workers as well as the village community. Access to services by deprived communities like the Scheduled Caste (SC) and Scheduled Tribe (ST) gets restricted if the centre is located in upper caste predominant hamlets. The study also show what appears to be a glaring lack of any proper method to assess the need and requirement as a result of which mostly the tribal and dalit communities have been excluded of the ICDS benefits. In Chhatarpur district this situation was seen most where tribal and dalit children and women are not getting any benefit from anganwadi centers. One more fact came out in the study that the conditions regarding the building of anganwadi center are worst in Panna which is the home district of the Minister of Women and Child Development, also the conditions of Seoni and Chhatarpur districts are also found worst.
3.3 Functioning days of Anganwadi Centers
Though the Apex Court has passed strict orders that every anganwadi center must provide services and should be open for 300 days in a year but the ground reality came out of the survey study shows that only 43 percent anganwadi centers w e r e p r o v i d i n g services for 26 days a month which is in accordance to the orders of Supreme Court. While 40 percent centers provide services for 21 days, 15 percent centers provide services only for 15 days in a month and 2 percent of the surveyed centers hardly provide services for 7 days in a month.
In the 65 anganwadi surveyed, two centres centers in Singro village (Block-Rajnagar of Chhatarpur district) and Tila village (Block-Khaniyadhan of Shivpuri district) were never opened since the day of their establishment indicating gross violation of the Supreme Court's order.
3.4 Toilet Facility
Under the ICDS scheme, it is mandatory that every anganwadi centre should have a well-maintained separate toilet for girls and boys. This facility is important because it will further ensure the presence of girls in the anganwadis. But the grassroot fact is very different. Separate toilets for girls and boys are a distant dream; most of the centers do not have any toilet facilities at
Table No. 11 - Functioning days of Anganwadi Centers
Functional days of AWC No. of AWC
7 15 21 26
Total 65 1 10 26 28
Percentage 2 % 15 % 40 % 43 %
Table No. 12 - Toilet facility In AWC
No. of AWC Toilet Facilities
Yes No
Total 65 15 50
Percentage 24 % 76 %
Moribund ICDS42
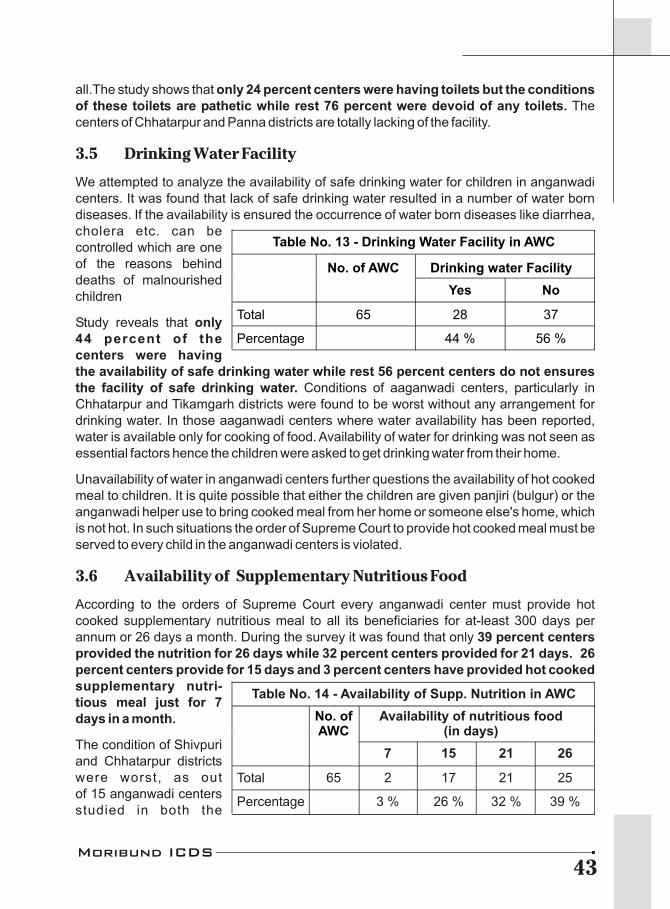
all.The study shows that only 24 percent centers were having toilets but the conditions of these toilets are pathetic while rest 76 percent were devoid of any toilets. The centers of Chhatarpur and Panna districts are totally lacking of the facility.
3.5 Drinking Water Facility
We attempted to analyze the availability of safe drinking water for children in anganwadi centers. It was found that lack of safe drinking water resulted in a number of water born diseases. If the availability is ensured the occurrence of water born diseases like diarrhea, cholera etc. can be controlled which are one of the reasons behind deaths of malnourished children
Study reveals that only 44 percent of the centers were having the availability of safe drinking water while rest 56 percent centers do not ensures the facility of safe drinking water. Conditions of aaganwadi centers, particularly in Chhatarpur and Tikamgarh districts were found to be worst without any arrangement for drinking water. In those aaganwadi centers where water availability has been reported, water is available only for cooking of food. Availability of water for drinking was not seen as essential factors hence the children were asked to get drinking water from their home.
Unavailability of water in anganwadi centers further questions the availability of hot cooked meal to children. It is quite possible that either the children are given panjiri (bulgur) or the anganwadi helper use to bring cooked meal from her home or someone else's home, which is not hot. In such situations the order of Supreme Court to provide hot cooked meal must be served to every child in the anganwadi centers is violated.
3.6 Availability of Supplementary Nutritious Food
According to the orders of Supreme Court every anganwadi center must provide hot cooked supplementary nutritious meal to all its beneficiaries for at-least 300 days per annum or 26 days a month. During the survey it was found that only 39 percent centers provided the nutrition for 26 days while 32 percent centers provided for 21 days. 26 percent centers provide for 15 days and 3 percent centers have provided hot cooked supplementary nutri-tious meal just for 7 days in a month.
The condition of Shivpuri and Chhatarpur districts were worst, as out of 15 anganwadi centers studied in both the
Table No. 13 - Drinking Water Facility in AWC
No. of AWC Drinking water Facility
Yes No
Total 65 28 37
Percentage 44 % 56 %
Table No. 14 - Availability of Supp. Nutrition in AWC
Availability of nutritious food(in days)
7 15 21 26
Total 65 2 17 21 25
Percentage 3 % 26 % 32 % 39 %
No. ofAWC
Moribund ICDS43
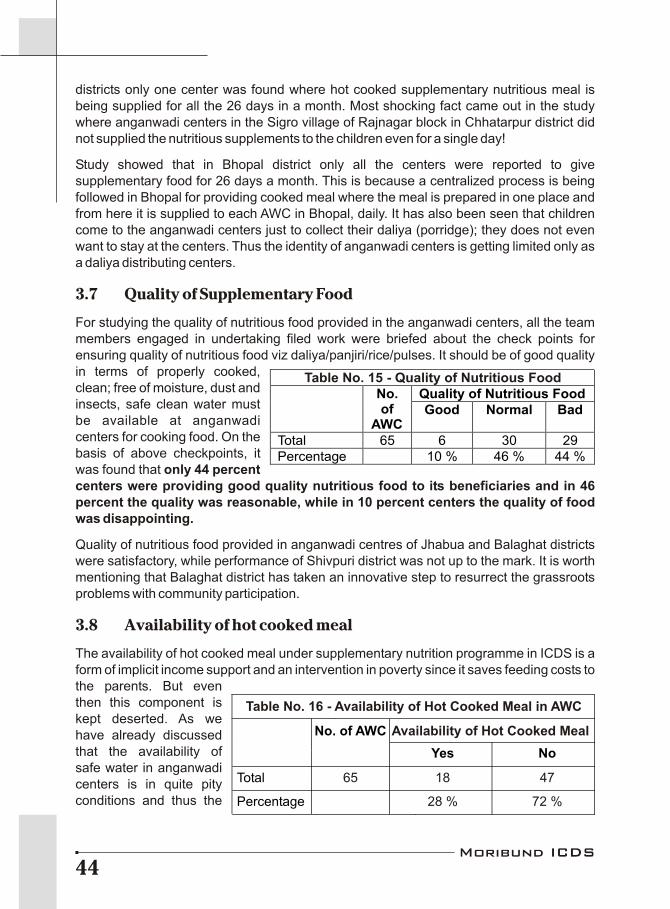
districts only one center was found where hot cooked supplementary nutritious meal is being supplied for all the 26 days in a month. Most shocking fact came out in the study where anganwadi centers in the Sigro village of Rajnagar block in Chhatarpur district did not supplied the nutritious supplements to the children even for a single day!
Study showed that in Bhopal district only all the centers were reported to give supplementary food for 26 days a month. This is because a centralized process is being followed in Bhopal for providing cooked meal where the meal is prepared in one place and from here it is supplied to each AWC in Bhopal, daily. It has also been seen that children come to the anganwadi centers just to collect their daliya (porridge); they does not even want to stay at the centers. Thus the identity of anganwadi centers is getting limited only as a daliya distributing centers.
3.7 Quality of Supplementary Food
For studying the quality of nutritious food provided in the anganwadi centers, all the team members engaged in undertaking filed work were briefed about the check points for ensuring quality of nutritious food viz daliya/panjiri/rice/pulses. It should be of good quality in terms of properly cooked, clean; free of moisture, dust and insects, safe clean water must be available at anganwadi centers for cooking food. On the basis of above checkpoints, it was found that only 44 percent centers were providing good quality nutritious food to its beneficiaries and in 46 percent the quality was reasonable, while in 10 percent centers the quality of food was disappointing.
Quality of nutritious food provided in anganwadi centres of Jhabua and Balaghat districts were satisfactory, while performance of Shivpuri district was not up to the mark. It is worth mentioning that Balaghat district has taken an innovative step to resurrect the grassroots problems with community participation.
3.8 Availability of hot cooked meal
The availability of hot cooked meal under supplementary nutrition programme in ICDS is a form of implicit income support and an intervention in poverty since it saves feeding costs to the parents. But even then this component is kept deserted. As we have already discussed that the availability of safe water in anganwadi centers is in quite pity conditions and thus the
Table No. 15 - Quality of Nutritious FoodQuality of Nutritious Food No.
of AWC
Good Normal Bad
Total 65 6 30 29 Percentage 10 % 46 % 44 %
Table No. 16 - Availability of Hot Cooked Meal in AWC
Availability of Hot Cooked Meal
65 18 47
28 % 72 %
No. of AWC
Yes No
Total
Percentage
Moribund ICDS44
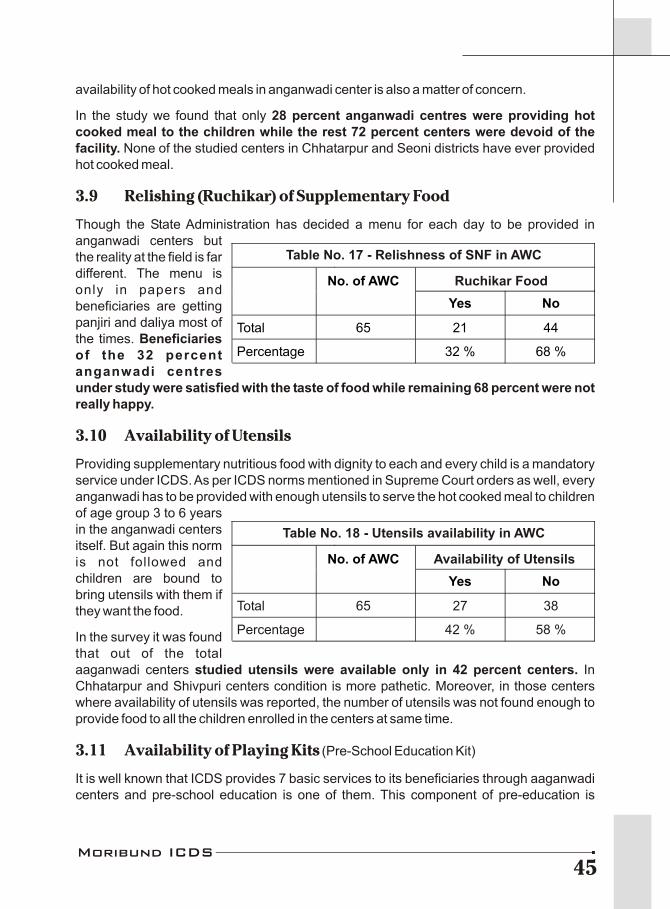
availability of hot cooked meals in anganwadi center is also a matter of concern.
In the study we found that only 28 percent anganwadi centres were providing hot cooked meal to the children while the rest 72 percent centers were devoid of the facility. None of the studied centers in Chhatarpur and Seoni districts have ever provided hot cooked meal.
3.9 Relishing (Ruchikar) of Supplementary Food
Though the State Administration has decided a menu for each day to be provided in anganwadi centers but the reality at the field is far different. The menu is only in papers and beneficiaries are getting panjiri and daliya most of the times. Beneficiaries of the 32 percent anganwadi centres under study were satisfied with the taste of food while remaining 68 percent were not really happy.
3.10 Availability of Utensils
Providing supplementary nutritious food with dignity to each and every child is a mandatory service under ICDS. As per ICDS norms mentioned in Supreme Court orders as well, every anganwadi has to be provided with enough utensils to serve the hot cooked meal to children of age group 3 to 6 years in the anganwadi centers itself. But again this norm is not followed and children are bound to bring utensils with them if they want the food.
In the survey it was found that out of the total aaganwadi centers studied utensils were available only in 42 percent centers. In Chhatarpur and Shivpuri centers condition is more pathetic. Moreover, in those centers where availability of utensils was reported, the number of utensils was not found enough to provide food to all the children enrolled in the centers at same time.
3.11 Availability of Playing Kits (Pre-School Education Kit)
It is well known that ICDS provides 7 basic services to its beneficiaries through aaganwadi centers and pre-school education is one of them. This component of pre-education is
Table No. 17 - Relishness of SNF in AWC
Ruchikar FoodNo. of AWC
Yes No
Total 65 21 44
Percentage 32 % 68 %
Table No. 18 - Utensils availability in AWC
Availability of Utensils
Total 65 27 38
Percentage 42 % 58 %
No. of AWC
Yes No
Moribund ICDS45

directed towards promoting holistic child development with emphasis on necessary inputs for optimal growth and development. It also contributes to the universalization of primary education and preparing the child for schooling. For this purpose learning by playing technique is being applied for which anganwadis are made available with (learning) toys or playing kits. These toys are also helpful in providing and ensuring a natural, joyful and stimulating environment for young children. Thus the availability of playing kit in anganwadi is beneficial to attract towards the center and keep engaged young children.
In our study we found that only 40 percent centers were having playing kits while rest 60 percent were not having the same. In the centres where playing kits were available were actually not reaching the children because either the kit is kept wrapped or are kept in the house of anganwadi workers. However, many of the anganwadi workers reported that they never received any playing kit. It is rather kept under the possession of supervisors or sometimes not supplied from higher authorities. Study shows that the condition of Hoshangabad and Chhatarpur districts is very poor where all the anganwadi centres studies were devoid of the facility of playing kits.
3.12 Availability of Medicinal Kit
Of the basic services provided through ICDS, primary health care is one of the important c o m p o n e n t a n d t o provide primary health care a medicine kit is made available in every anganwadi center. This kit also called first aid box is consists of bandage, tincture, medicines for normal fever and de-worming tablets.
The children of 6 to 36 months are very much susceptible to parasitic infections and thus these children must be given de-worming doses in every six months on priority basis. In such circumstances, availability of medicinal kit at aaganwadi centers is really beneficial but unfortunately these kits are not available at most of the centers. The survey study shows that only 11 percent centers were having the medicinal kit facility.
Moreover, if we see the budgetary component for this facility we will find that the service is kept quite in negligence. There has been no single rupee expenditure on the medicine kit
Table No. 19 - Availability of Playing Kits
No. of AWC Availability of Playing kit
Yes No
Total 65 26 39
Percentage 40 % 60 %
Table No. 20 Availability of Medical Kits
No. of AWC Availability of Medical kit
Yes No
Total 65 7 58
Percentage 11 % 89 %
Moribund ICDS46

component since past 2 years i.e. 2006-07 and 2007-08. In the year 2006-07 a budget of Rs. 21.65 lakh was allocated to the department of women and child development for medicinal kits while in year 2007-08 this amount was decreased to Rs.1 lakh, despite the fact that number of anganwadi centers is increasing day by day all across the State. Furthermore, even if the medicines are made available, they are not distributed on the basis of demand or need in the areas but variety of medicines are prescribed and allocated to each and every aganwadi centers. Also if we analyze the budget further, we will find that our Government is providing Rs. 1.44 per anganwadi center only that turn out to be miniscule figures of expenditure just 2 paisa per beneficiary.
3.13 Growth Monitoring
As mentioned above that the entire monitoring of malnutrition is based on the system of growth monitoring through growth charts and weight records. In the survey we tried to look at the availability of the machines and growth registers in the studied anganwadi centers. We came across the dire truth of growth monitoring component of the ICDS scheme that not a single center studied was having the machine to weigh the young children below three years of age.
a. Availability of Salter Machine
Out of the studied AWC, 72 percent centers were having the machine. This clearly indicates that in the centres where there is no sa l te r mach ine, no growth monitoring would have been done for the children aged 3-6 years. Anganwadi workers of these centers revealed that children are weighed only during the Balsanjeevni campaign by borrowing the machines from nearby centers. It means children are weighed once in six months. Out of the 10 districts studied the status of Jhabua was worst. Besides appalling fact is that in the centers with of weighing machines, children are not weighed regularly because most of these machines are not working properly.
One more thing to be noticed here is that UNICEF provides the technical support for ICDS services and the salter machine is also provided by UNICEF. About 10000 new anganwadi centers have been started in the State during past four years and according to UNICEF records no machines have been purchased or supplied to WCD department since past four years. It means that these centers are devoid of any weighing machines and thus no growth monitoring or growth records are being maintained in these centers. All these conditions clearly spelt out the seriousness of the government's towards health and well being of children in the state.
Table No. 21 - Availability of Salter machine
No. of AWC Availability of Salter Machine
Yes No
Total 65 47 18
Percentage 72 % 28 %
Moribund ICDS47

b. Availability of Adult Weighing Machine
The problem of malnutrition in children has not cropped up suddenly but it began to take shape much before the birth of a child. Most of the women especially the tribal women are found to be undernourished and anemic. The data of NFHS III shows that more than half the women (nearly 56 percent) in the State are anemic and figure closely correspond to the national figure of 55.3 percent. Madhya Pradesh stands in third position with 42 percent proportion of undernourished women. Ultimately a weak mother will give birth to an undernourished child. In order to control the existing malnutrition in the children; keeping a check on the health of women and adolescent girls is compulsory. With this vision regular health check-ups and weighing of pregnant/lactating women and adolescent girls is expected to undertake in anganwadi centers with the provision of adult weighing machine.
The study revealed that only 66 percent of the studied centers were having the machines to weigh adults. Also there were no scales in any of the centers to measure the height of girls and women. When there are no records of monitoring the health of pregnant women; it means there is no system in place to aware them about any complications in the delivery.
c. Growth Registers
To monitor the health and to keep proper monthly records of weight and age of children is an e s s e n t i a l s e r v i c e provided under ICDS scheme and growth registers are provided for the same. In our study we found only 58 percent aaganwadis were having growth registers. Moreover, if we compare the availability of weighing machines and growth registers we saw that there were 14 percent centers where weighing machines are available but there is no growth register to keep record of weights of children in thee centers.
3.14 Pre-School Education
Pre-school education is an important service provided by AWCs so that young children get comfortable with education and studies by learning with playing in AWCs. But in Madhya
Table No. 22 - Availability of Adult Weighing Machines
No. of AWC Availability ofAdult Weighing Machine
Yes No
Total 65 43 22
Percentage 66 % 34 %
Table No. 23 - Availability of Growth Monitoring Register
No. of AWC Availability ofGrowth Monitoring Register
Yes No
Total 65 38 27
Percentage 58 % 42 %
Moribund ICDS48
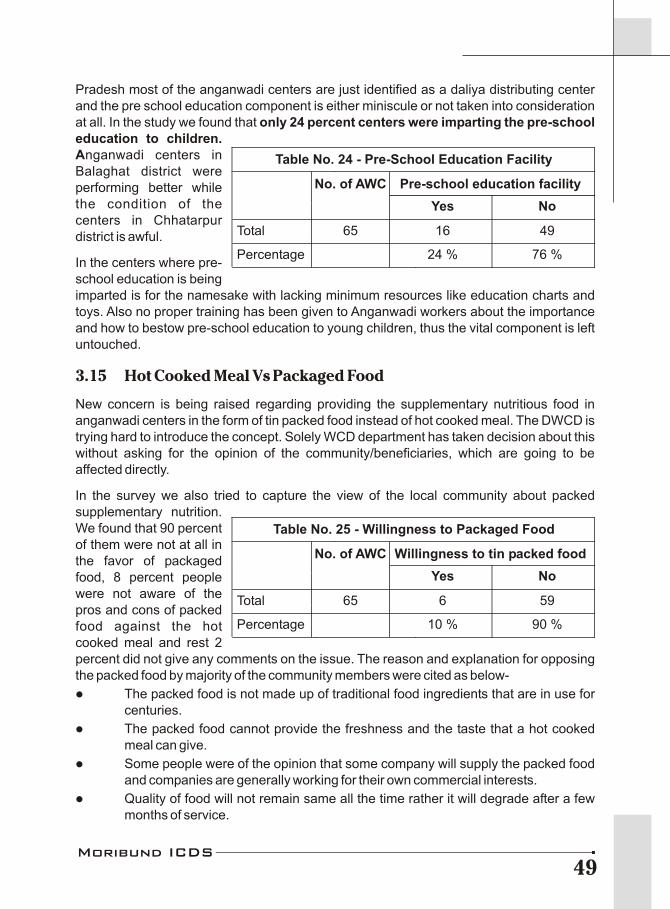
Pradesh most of the anganwadi centers are just identified as a daliya distributing center and the pre school education component is either miniscule or not taken into consideration at all. In the study we found that only 24 percent centers were imparting the pre-school education to children. Anganwadi centers in Balaghat district were performing better while the condition of the centers in Chhatarpur district is awful.
In the centers where pre-school education is being imparted is for the namesake with lacking minimum resources like education charts and toys. Also no proper training has been given to Anganwadi workers about the importance and how to bestow pre-school education to young children, thus the vital component is left untouched.
3.15 Hot Cooked Meal Vs Packaged Food
New concern is being raised regarding providing the supplementary nutritious food in anganwadi centers in the form of tin packed food instead of hot cooked meal. The DWCD is trying hard to introduce the concept. Solely WCD department has taken decision about this without asking for the opinion of the community/beneficiaries, which are going to be affected directly.
In the survey we also tried to capture the view of the local community about packed supplementary nutrition. We found that 90 percent of them were not at all in the favor of packaged food, 8 percent people were not aware of the pros and cons of packed food against the hot cooked meal and rest 2 percent did not give any comments on the issue. The reason and explanation for opposing the packed food by majority of the community members were cited as below-
l The packed food is not made up of traditional food ingredients that are in use for centuries.
l The packed food cannot provide the freshness and the taste that a hot cooked meal can give.
l Some people were of the opinion that some company will supply the packed food and companies are generally working for their own commercial interests.
l Quality of food will not remain same all the time rather it will degrade after a few months of service.
Table No. 24 - Pre-School Education Facility
No. of AWC Pre-school education facility
Yes No
Total 65 16 49
Percentage 24 % 76 %
Table No. 25 - Willingness to Packaged Food
No. of AWC Willingness to tin packed food
Yes No
Total 65 6 59
Percentage 10 % 90 %
Moribund ICDS49
Ground Zero:Sidhi, a place on the brink of negligence
The AWC in Amha village of Mata panchayat of Sidhi district is a case depicting the utter negligence towards the operation of AWC at ground level. There is no building for the center and no supply of supplementary nutritious food from July to September 2008, and with no food there is no question of quality. There is no weighing machine, no playing kit and no medicine kit in the center. Post of anganwadi worker (AWW) is lying vacant since last year. Absence of supporting staff has adversely affected the provision of basic services to needy beneficiaries. Not a single child or pregnant/lactating women have received any vaccination for the past 6 months.
Despite the fact and urgent need for health facilities and monitoring of the prevailing situation of ICDS, no administrative staff from both health and WCD department is willing to visit the village owing to its distant and remote location. In the village children are weighed only once in a year during the Balsanjeevni Abhiyan round.With the support of Mahila Adhikar Manch, 24 AWC were studied in the district. It was found that only one-fourth (6) centers were having the building. There was no salter-weighing machine in 12 centers whereas 15 centers were devoid of adult weighing machines. Neither of the centers were having medical kit facility, playing kit and the facilities for pre-school component were also missing from all the centres studied in the district. Most of the centres were either lacking utensils, if having they were inadequate to support all the children enrolled in the AWC. It was also observed that in many centers anganwadi worker is appointed but helper is not and vice-versa thus it affected the preparations of cooked meal.
thDuring the 12 round of Balsanjeevni abhiyan 52 children were identified in serious malnourished stage from these 24 villages but not a single child have been referred to NRCs till October end 2008. When explored further the reason behind it was found that in the NRC children are admitted according to the list of malnourished children prepared by the district officials. No preference has been given to the condition or stage of malnutrition. It means that children have to wait for there turn to get treated of malnutrition.
Under the ICDS scheme monitoring of anganwadi centers, capacity building of anganwadi workers and motivating anganwadi worker/helper as well as community for health and nutrition education are the important components. Separate supervisors are appointed at block level. It is expected from these supervisors to visit every anganwadi center at least twice a month. But in the studied 24 centers in Sidhi district no visits have been reported in the past three months. On further exploring we found an appalling fact that the ICDS project of Sidhi is the largest one in the State that include 536 ICDS centers, while there is only one supervisor has been appointed to manage this huge number of centers making it quietly impossible for the supervisor to visit all the centers even once in a month. Shortage of working staff is not only the problem of Sidhi district but the whole State is facing this problem.
Anganwadi workers also supports the views of communities and beneficiaries by saying that hot cooked meal is far better than the packaged food and children must get the traditional, hot cooked meal in anganwadi centers instead of some tin packed food.
3.16 Conclusions of Field study
What do all the observations from the field study lead to? What are the lessons that we can learn from the gaps between what the ICDS programme is expected to deliver and what
Box - 14
Moribund ICDS50
actually happens on the ground? Child development programmes of the state government need an extraordinary attention. Given the size of the problem, and the complexity of issues involved government has to take the lead and ensure that the persisting problem of hunger and malnutrition among children has to be addressed with great care and sensitivity. A rigorous monitoring of the implementation process has to be followed coupled with and a concerted effort to make the programme more participatory by involving the local people. New strategies are to be shaped that would go long way to help ICDS functioning effectively in reducing widespread malnutrition.
Ground realities pose a very serious question why is the flagship programme meant for child nutrition and development is in such a terrible state? May be the following points throwing some light on the probable reasons.
l It seems health and well being of children is not really a priority with political parties. The political leaders raise no debates on the conditions of children in State, whether the leader is of ruling party or the party in left. Also, there are no provisions of making better policies for children in the manifestos of any political party because the children are not the eligible vote banks.
l There is a big gap in proper implementation as well as monitoring system and accountability towards ICDS which is the only scheme for children under six year age group.
l The original intent of the ICDS programme was to address the various sub-stages (like from birth to 6 months age, less then 3 years and 3-6 years of age) of growth. Purpose of this was to ensure that the negative health and nutritional outcomes for a child any one stage would not be carried forward to the next. But it is apparent from the ground realities that the programme effectively concentrates only the children in the age group from 3 to 6 years only. Various empirical studies reveal the fact that reaching out the children below three is one of the major constraints in ICDS implementation.
l Exclusion on the basis of caste and class is also a big problem as it refuses the deprived sections of the society most needed access.
l Non-recognition of malnutrition deaths by the state government is one of the foremost challenges in front of development practitioners working closely on the issue. The problem gets aggravated in the light of fact as constant denial by the state government of the malnutrition deaths but the deaths are due to disease.
l Lack of co-ordination and continuous blame game between the women and child development department and health department also contributes to the ineffectiveness of the scheme.
l Owing to socio-cultural and sustainability reasons community is not in favor of regular supply of packaged food. 90 percent of the respondents' feel that locally made, prepared and supplied food will be welcomed.
The survey study clearly shows that despite the higher extent of undernourishment in the state, performance of ICDS is far from satisfactory levels. Many of the Anganwadi centers in the state are not even providing the basic services to children like supplying supplementary nutrition, growth monitoring and nutrition surveillance and imparting pre-school education.
Moribund ICDS51

Who else will take care!!Who else will take care!!
In Tamia block of Chhindwara district, there is a place called Patalkot which is recognized for its natural beauty
and unique location. No body tries to unveil the problems the tribal people living in Patalkot faced due to gradual
effects of climate change, hiking markets and various policies of government through which common people's
reach to natural resources are being limited. Patalkot is the valley mainly habited by the Baiga tribes (one of the
3 PTG of MP) and the health status of their children is becoming inferior day by day.
To take care of the health of children and to provide them the benefits of Integrated Child Development Scheme,
an Aganwadi Center was established in the Gaildubba village of Patalkot valley in 2007. Really it's an
appreciating effort of the district administration that it took an initiative to establish AWC in such an hard to reach
area. But see the irony! At present the AWC of Gaildubba is now converted into a Guest House for government
authorities. Actually, when the AWC was established then our Chief Minister in the year 2007 reached there to
inaugurate the centre and as there was no other option, the same AWC was used as the guest house for him.
Since then the local administration said that this building will be used as a guest house rather as an Anganwadi
Center. The villagers are yet fighting for converting the guest house turned AWC back into AWC for children.
This case study has been observed by Right to Food Campaign Madhya Pradesh Support Group in June 2009
Moribund ICDS52
Consequently children with severe malnutrition are not identified properly and these children remain far away from the prescribed special treatment or referral services. This not only shows faulty implementation but also indicate gross negligence in delivering ICDS programme. Field reality emerged from ground definitely demands an extra ordinary efforts to improve the efficiency of the programme and ameliorate malnutrition and ill health of children in the state. The time has come to turn the ICDS programme upside down doing away with the existing model and thinking afresh on how best we can reach out to the most vulnerable. State government has to play a more proactive role and should try its level best to accomplish universalisation of the ICDS programme. We need to plan separately for different sub-groups of children looking at the specific needs of home-based care and outreach services up to 3 years and a centre based approach for the 3+ groups of children. Concrete efforts are necessary in the sense that poor health, malnutrition and frequent bouts of illness at the young age of 6 months to 5 years have an irreversible impact on the overall health and well being of children.
Denial by State :Biggest Challenge for Child Survival
4
thAccording to the 12 Bal Sanjeevni Campaign data; around 48,220 (0.56%) children in Madhya Pradesh are suffering from severe malnutrition. So stark is the situation that one evaluation report of UNICEF said that even if the children were saved, they might go blind due to lack of vitamin A.
In last 3 years malnutrition; an indicator of human development has been on the rise in Madhya Pradesh. According to data collected by the state government's own Bal Sanjeevni Abhiyaan, eighty thousand children are suffering from most severe malnutrition and are on the verge of death.
Malnutrition in itself is a multi-dimensional problem because it is related with the process of socio-political transformation like social behavior, household livelihood, state services, equality and human rights with dignity. It has been observed that immediately after the birth of a child, mother feeds the child for around 6 months but after that the child does not get required nutritional food for his growth and development owing to household food insecurity. Its well-known fact that child requires more attention and supplementary nutrition during the first two years of birth, as in this period of age, 80 percent physical and mental growth takes place. But due to poverty child do not get required qualitative food and is been pushed towards hunger deaths.
In Madhya Pradesh the proportion of children who are severely malnourished is also 33notable: 24% children are severely stunted and 16% are severely underweight . Women
and Child Development Department has tried to provide daliya (porridge) and panjiri (bulgar) to children up to the age of 6 years. But this approach has had very limited success as a cup of boiled daliya cannot improve health condition of malnourished children?
Moreover every time when children die out of chronic hunger, Government officials usually say that children are dying due to TB, diarrhea and measles and not due to malnutrition forgetting the truth that malnutrition actually creates the ground for these diseases. These diseases occur due to the lack of immunization and in turn decrease life expectancy of children. In MP, only 40.3 percent of the children receive proper immunization according to the NFHS III data.
The state administration and the political groups do not have a strategic understanding to solve the problem of malnutrition. They see it as an untouchable issue to protect their self-interests. The government does not want to believe that malnutrition is result of its anti-human rights development policies. There is no magic that can solve the problem. Lack of accountability and coordination among various related Departments like Women and Child Development, Department of Health, Department of Panchayat and Social Welfare,
33NFHS III Data
Moribund ICDS53
Departments of Rural and Urban Development, and Department of Education has to be seen as a big draw back in the campaign against malnutrition. Also it's reprehensible that not only the system but also the society has not given much priority to the matter, which has already taken a huge toll on the poor. Government has failed to provide a life with rights and dignity to its people and even unable to save the lives of children which is the future of the State. Malnutrition can be linked with a number of other issues like the functioning of the PDS in the region, the break up of the traditional food security system of the people, the non functioning social security schemes and the ineffective ICDS implementation, lack of means to earn livelihood, and above all the irresponsible attitude of the government functionaries. The health status of a family is directly dependent on the earning capacity of the family. Most of the children dying due to malnutrition belong to tribal communities that used to depend mainly on the forest and its produces for livelihood. It is not that the condition is out of control. Still all these mishap can be handled simply by resurrecting the systems and by making some positive changes in policies. This can be achieved fairly quickly, given the right combinations of political commitment, strategic programming and resources. But no one is even ready to accept the truth that there are some problems in the policies and systems.
Denial mode on starvation deathsFor several months now the media has been flooded with reports on starvation deaths in Satna, Sheopur and Khandwa districts of the Madhya Pradesh. The State administration, however, is in a denial mode. We are in great pain to dismiss the state government's claim that the starvation deaths occurred due to reasons other than starvation. There is nothing new in this denial. I learnt it very early in my police career that at any given time any State Government is wary of admitting even single starvation death leave aside scores of them as in the present case. And, that too in the election year - Na baba na! It is a taboo.
I was posted as a trainee Station House Officer at Ramgarh Police Station, Bilaspur district in 1963. One afternoon, a kotwar brought the report of a starvation death. As the rest of the staff had gone out on various duties, I was the only one available at the police station. On interrogating kotwar, I was convinced that the deceased had in fact died of hunger; I was about to make a roznamcha (Day Book) entry that Head Constable Moharrir Abdul Karim entered the police station office. I told him about the starvation death and what I had intended to do. With a look of disbelief and he remonstrated me that by doing so I might loose my job in future. All such reports have to be treated as natural deaths and its better the Head Constable be handled the case.
Head Constable sat down to make a roznamcha (Day Book) entry of a marg (filing an incidence in police records, so that the investigation process of the incidence could be started) and then picked up his bag and left with the Kotwar for the village of occurrence. On return, he made a detailed entry in the roznamcha that the death had taken place due to natural reasons. He had a copy of the postmortem report too which endorsed with his panchnama duly attested by two witnesses. The medical officer had certified the cause of death due to old age. Putting the postmortem report in my hands he muttered 'dheere dheere sab samajh me aa jayega.'
How long shall we continue to do the fudging? The latest World Bank report says that one third of the world's poor live in India. Those of us who have seen the abysmal poverty in the countryside know that starvation deaths are not unusual. Denial may temporarily help a political party to return to power but it doesn't solve the basic problem of deprivation, poverty and hunger and State's indifference.
Box - 15
Moribund ICDS54
4.1 Children in Denial and Negligence Vs World's best child survival in records in MP
The Health Department of Madhya Pradesh Government claims that not a single infant death has been reported from Dhar and Chindwara districts (both the districts are tribal populace districts) of Madhya Pradesh. On the contrary the Department of Women and Child Development have registered 560 infant deaths in just a short period of 7 months from November 2007 to May 2008 in the same districts. No infant mortality was reported from Chindwara district in past 42 months (April 2005 to September 2008) and Dhar district shows no infant death in last 30 months (April 2006 to September 2008).
The analysis is based on the data provided by the Monthly Health Bulletin of Department of Public Health and Family Welfare. This report the Maternal and Infant deaths regularly and hence can be considered as the authentic information.
l For the past more than 3 and half years only 6 infant deaths have been registered in Chindwara district. In that sense ranking the district as best performing with lowest infant mortality. Interestingly all these 6 deaths have been registered in the month of October 2008.
l Dhar has registered 233 infant deaths in 2005-06 but since then, in the past two and half years there is not a single infant death.
l Jabalpur has registered 9 infant deaths in 2005-06, 10 deaths in 2006-07, 23 deaths in 2007-08 and 4 deaths in first 7months in 2008-09.
With the above information State government would like to pursue the feelings that the state is not reeling under storm of malnutrition by putting the few districts under the category of world's best places with lowest IMR, however the field reality and well as national level survey figures quoted in NFHS turn down all the claims. It's really shameful on the part of the health department that the state with highest Infant Mortality Rate in India, along with the Highest Malnutrition level in the country provides such fake and unbelievable information.
But on the other hand, MPRs of Integrated Child Development Services revealed a clear contrasting picture. The analysis of MPRs shows that in the 7-month period from November 2007 to May 2008, 469 infants in Dhar, 91 infants in Chhindwara and 213 infants under the age of one year have died in Jabalpur district. This definitely propel upon the Health department for not having proper accountable system that keep serious records of child deaths in the state. This provokes the larger debate of coordination between Women and Child Development department and Department of Public Health and Family Welfare on effective ICDS implementation on the field.
Few calculations were done based on the IMR data, actual registered births and the official IMR figures registered by the health department of the state government. According to latest Sample Registration Survey report 2007 released in October 2008, Infant Mortality Rate of Madhya Pradesh is 72 per one thousand live births. The inferences of the trend
Moribund ICDS55
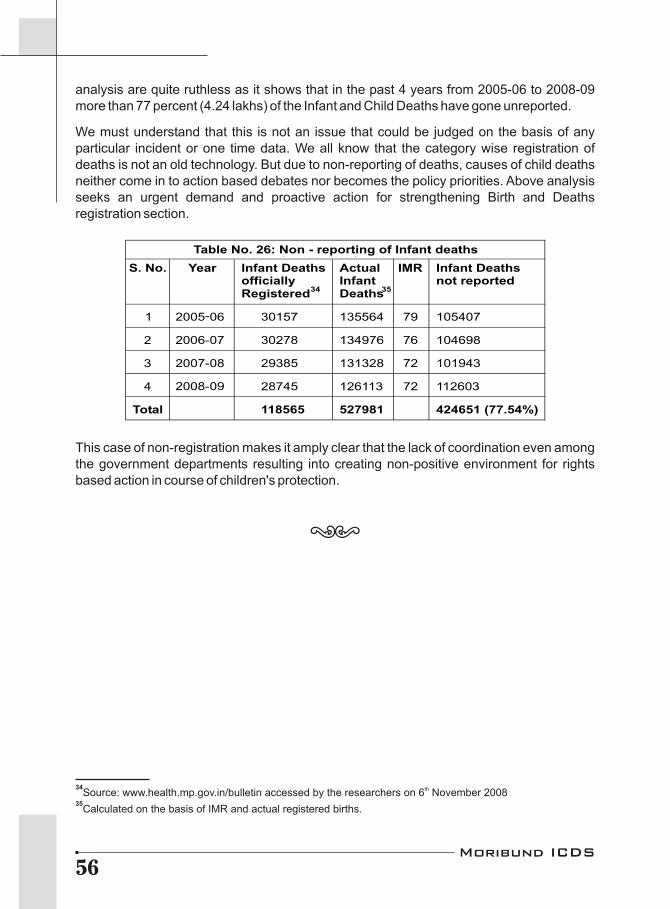
analysis are quite ruthless as it shows that in the past 4 years from 2005-06 to 2008-09 more than 77 percent (4.24 lakhs) of the Infant and Child Deaths have gone unreported.
We must understand that this is not an issue that could be judged on the basis of any particular incident or one time data. We all know that the category wise registration of deaths is not an old technology. But due to non-reporting of deaths, causes of child deaths neither come in to action based debates nor becomes the policy priorities. Above analysis seeks an urgent demand and proactive action for strengthening Birth and Deaths registration section.
This case of non-registration makes it amply clear that the lack of coordination even among the government departments resulting into creating non-positive environment for rights based action in course of children's protection.
Table No. 26: Non - reporting of Infant deaths
S. No. Year Infant Deaths officially Registered
34
Actual Infant Deaths
35
IMR Infant Deaths not reported
1 135564 79 105407
2 134976 76 104698
3 131328 72 101943
4
2005-06
2006-07
2007-08
2008-09 126113 72 112603
Total
30157
30278
29385
28745
118565 527981 424651 (77.54%)
34 thSource: www.health.mp.gov.in/bulletin accessed by the researchers on 6 November 200835
Calculated on the basis of IMR and actual registered births.
Moribund ICDS56
Nutrition Policies Questioned
5
An important component of ICDS scheme is that all the beneficiaries of ICDS must be provided supplementary nutritious food. The children above 3 years of age are entitled for getting hot cooked meal at Anganwadi center itself while children below 3 years, pregnant and lactating women are provided with take home foods which are ready to eat energy foods like daliya, panjiri etc. It is because small children (under 3 years) and pregnant and lactating women are not part of the hot cooked meal scheme as yet. The ready to eat energy food provided by ICDS should not be commercial but locally prepared foodstuff with locally grown grains with the shelf life dependent on how often is the food is distributed by AWC (daily/weekly/twice a week/twice a month). But the reality of this service in the State is something else.
Supplementary nutrition services have come to a grinding halt in large parts of Madhya Pradesh with the orders of Supreme Court to ban contractors in Supplementary nutrition supply to ICDS. State government then encouraged the Self Help Groups (SHGs) formations and also promoted/invited local women's self-help groups and Mahila Mandals for supply of supplementary nutritious food through ICDS but the very same government that set up the SHG's for the so-called empowerment of women has today started digging the grave for it. The Women and Child Development Department of the Government of Madhya Pradesh is inviting sealed bids from the eligible manufacturers or producers to supply of Ready to Eat Energy Food as a Supplementary Nutrition Food to ICDS Projects in various districts. If one go through the terms and conditions of the tender it is obvious that large manufacturers and producers only be able to bid for the work. The notification specifies that the bidder should possess ISO 9001 or 9002 series Quality System Certification and Hazard Analysis and Critical Control Point (HACCP) Certification for the manufacture of supplementary nutrition and the average annual turn over of the firm should not be less than Rs. 24 crores in the past three completed financial years. No wonder the SHGs in the state in at any cost would be able to qualify the criteria mentioned above to get the work order.
37 thMr. Harsh Mander mentioned in his letter dated 17 October 2008 to Shri R.C. Sahni, Chief Secretary, Government of Madhya Pradesh that “SHGs have been asked to tender for supplying ready to eat food under ICDS in the state. This seems an extraordinary formality to be completed on the part of SHGs. It is because the genuine SHGs and mothers' committees would be locally rooted and unlikely to be able to engage in formal tendering processes and also who would they be competing against?” He recommended that this process must be discontinued for the larger interest of the society. He also mentioned that the current practice of purchasing from the MP Agro-Industries Corporation is nothing but an indirect purchase from contractors, which is again a violation of the Court's orders. He further wrote in his letter that weaning foods for the children below 3 years could best be
37Special Commissioner of the Supreme Court [in the case:
PUCL v. UOI & Ors. Writ petition (civil) no. 196 of 2001]
Moribund ICDS57

locally produced. It should be prepared using culturally and nutritionally appropriate recipes from every region in the state. He very strongly recommended reverting back to the varied weekly menu of hot cooked meals that included food item like puri-sabji, kheer-puri, poha, halwa etc. that were being served until a few months ago.
Another evidence of negligence of local SHGs and mothers committee (Matru Sahyogini Samiti) by state government can be gauged from the example of Bhind district. Here on one hand government has stopped the allocation of budget for SNP flowing to the joint account of Anganwadi Worker and Mother's Committee for the reason of financial irregularities
38observed . On the other hand the government is slapping a fine of Rs. 10/- per day on the 39firms engaged in supplying SNP in Angawadis in case of gap in the supply . It means if local
organizations are unable to supply SNP regularly then they would be directly banned from further supplying, but for the same fault private firms./companies would be charged with fine of miniscule amount are not supplying SNP on regular basis they will only be charged (fined) Rs. 10/-. Such actions hint a conspiracy to keep off the local organizations out of loop.
Mr. Ajai Singh, Ex-Minister and a Congress Member of Legislative Assembly (MLA), wrote a letter to the Chief Minister Mr. Shivraj Singh Chauhan stating that pursuant to the Supreme Court Orders, the procurement and distribution of the food for the Anganwadi's had been handed over to the Self Help Groups. This would unable in providing employment to a large number of marginalized families especially the women at local levels. But now the concerned department has taken steps to privatize and centralize it, which can be clearly understood by the tender specifications and this move is not the one that is welcome. The then Chief Minister is also believed to have written to the District Collectors saying that the distribution should be continued through the SHG's.
5.1 Importance of Cooked Meal over Packaged Foods
Another point where Government is trying hard is the efforts to promote the ready to eat energy food. It seems that by doing so Government is trying to destroy the traditional food habits of the people. Also Government has not shown any concern to chalk out nutrition programs, which are practically applicable, and at the same time sustainable at village/local levels. The food supplied by the government-undertaking firms like Madhya Pradesh Agro-Industries Corporation (which procures supplementary nutrition from various private producers) is not the traditional food of the local communities across the State. For instance, MP Agro supplies panjiri to all the AWCs across the State while panjiri is not consumed readily in all the parts of the State. We are all aware of the fact that the food habits in the state are diverse and vary from groups/society and region to region. This is true especially in case of tribals who largely consume food collected from the forest that is very nutritious.
The food supplied by the local SHG's are in compliance with the food habits with regional flavor and taste of the local people as against food supplied by the private companies pays
38 stLetter of WCD department, Govt. of M.P. dated 31 May 2008.39
Agreement letter between Govt. of M.P. WCD department and Ms. Vaishno Food Products Pvt. Lim., Gwalior.
Moribund ICDS58

little heed to the traditional food habits of the people. By pursuing ready to eat food, State government is instrumental in promoting rumors like it is higher in nutritious value compared to the traditional food supplied by the SHG's, also establishing that the cooked meals have the possibility of food borne diseases. However, the studies of University
40 School Resource Network of Jawaharlal Nehru University (USRN) acknowledged that such situations have been very few and far between. Such incidences where cooked food has been found with the problems of food borne diseases in overall implementation are rare and this is an achievement for SHGs of the program. On the other hand, there are instances particularly in the context of contractor-supplied rations in ICDS where packaged food was of bad quality and was sometimes rotten.
A study conducted by the Department of Food Science and Technology, Jabalpur, on the nutritious value of traditional food products like Kodo, Kutki, Ragi etc shows that it is rich in calcium and fibre content and hence is used in the formulation of various weaning and supplementary foods. These could be consumed as ready to eat food for various categories of people like young children, pregnant women and old persons, as it is a cheap source of good quality proteins and minerals. The study recommended that it could be commercialized for ease of preparation at household or at commercial levels. This is what exactly the SHG's have been doing through preparing Ready to Eat Energy Food from traditional pulses and supplying them to the ICDS Centers. By bringing in privatization into the whole system the government is misleading the people by saying that their food habits are not upto the mark and devoid of nutritional component. With such circumstances government is once again all set to repeat the stupidity committed by it in the 1960's, when it had proclaimed that supplementary milk products like Lactogen and Nan were better than breast milk for new born babies. However, it's now the established fact that breast milk is the best for infants and now government is investing huge sums on campaigns to draw attention of the people on this.
Utility of dry snacks or ready to eat energy food has been questioned. It is seen that nutritious value of dry snacks is far lower compared to a cooked meal. A freshly cooked meal offers a better range of nutrients while packaged food is costlier in terms of per rupee nutrient yield. In both the cases of ICDS and MDM evidence suggests that children often take the dry foods home and may or may not eat it later; also in the context of poverty, the
41chances are that these gets shared with the family members often . Cooked meal provides general protection against hunger especially in drought-affected areas and districts with poor levels of socio-economic development. Besides, children also learn to sit and eat together often contributing to breaking barriers of caste and class.
40 & 41Mita Deshpande, Rajib Dasgupta, Rama Baru And Aparna Mohanty, The Case For
Cooked Meals: Concerns Regarding The Proposed Policy Shifts in The Mid-day Meal AndICDS Programs; Indian Pediatrics 2008 Volume 45:445 -449
Moribund ICDS59

Judicial Interventions in ICDS
6
6.1 Supreme Court Orders in ICDS
In April 2001, People's Union for Civil Liberties (PUCL, Rajasthan) submitted a writ petition to the Supreme Court of India seeking enforcement of the right to food. The basic argument is that the right to food is an aspect of the fundamental “right to life” enshrined in Article 21 of the Indian Constitution. Indeed, the Supreme Court has made it clear that the right to life should be interpreted as a right to “Live with Dignity”, which includes the right to food and other basic necessities. The public interest litigation initiated by the PUCL petition is known as “PUCL vs. Union of India and Others, Writ Petition (Civil) 196 of 2001”. The final judgment is still awaited, but meanwhile, the Supreme Court has issued a series of “interim orders” aimed at safeguarding various aspects of the right to food. The first major order, dated 28 November 2001, directed the government to fully implement nine food-related schemes (including ICDS) as per official guidelines. In effect, this order was converted into the benefits of these schemes as legal entitlements. It also directed the government to “universalize” the ICDS programme. It means every hamlet should have a functional Anganwadi centre, and that ICDS services should be extended to every child under six, every pregnant or nursing mother, and every adolescent girl.
The Court directives related to ICDS, however, received very little attention for several years. Virtually no serious action was taken to implement them until April and October 2004, meanwhile several hearings on ICDS were held in the Supreme Court and further orders were issued. For instance, the Supreme Court explicitly directed the government to expand the number of anganwadis from 6 lakhs to 14 lakhs, to ensure that every settlement is being covered. The Supreme Court orders of April and October 2004 gave a wake-up call to the government. As a result, universalization of ICDS was included in the National Common Minimum Programme of the UPA government in May 2004. The National Advisory Council submitted detailed recommendations for achieving “Universalization with Quality” in October 2004, and simultaneous follow-up recommendations in February 2005. The expenditure of the Central Government on ICDS was nearly doubled in the Union Budget 2005-06. However, there has been relatively little progress in terms of the situation on the ground. The expansion of ICDS is quite slow, and in most states there is little evidence of substantial quality improvement. This reflects the fact that Supreme Court orders and budget allocations are not enough. Ultimately, what is required is a broad based movement for the universalization of ICDS, involving not only the government but also the public at large.
As per the Supreme Court recommendations, under the consolidated child development program; the children under 6 years of age should be provided supplementary food on regular basis and should be given 30 calories or 8 to 10 grams of food containing proteins. But if the case is of malnourishment then the child should be given double amount of stated meals. But on the ground especially in the tribal populated area this concern is ignored, as supplying double amount of supplementary meals is not possible at the anganwadi
Moribund ICDS60
because of low quantity supply from government itself where the increased demand has not taken into consideration.
Apex Court has ordered the allocation of Rs. 2/-per child per day for supplementary nutrition food, State government is allocating budget on the same lines but the interesting point to be noted here is that there is no provision of extra budget for the transportation of SNP. It means that the expenditure on transportation and fuel for the same are included in the amount of Rs. 2/- per day per child, ultimately declining the per child expenditure on food. The SC Commissioners have also tried to raise the issue of malnutrition and non-compliance with the Court's orders in many letters to the State Government, but have received no response. And the malnutrition deaths continue in the state.
6.2 Steps of High Court of Madhya Pradesh in ICDS
A petition was filed by Mr. Sachin Kumar Jain a member of Right to Food Campaign Support group in November 2005 when the government of Madhya Pradesh was inviting big contractors to supply nutritional food supplements and violating its own policies. Highlights of the petition are as follows:
l The ground for petition was the order dated Oct 7th, 2004 of honorable Supreme Court case 196/2001 which stated that contractors shall not be allowed for supply of nutrition.
l Women and Child development department has invited sealed bids on 28-9-2005 from the eligible manufacturers/ producers for supply of Ready to Eat Energy food (Supplementary nutrition food) to various ICDS projects in various districts of M.P.
l The petitioner had drawn the attention of the administration towards the guidelines of the Hon'ble Supreme Court in his letter-dated 29.10.2005 and had requested to immediately stop the process of tender notification.
6.2.1 Response of Administration
In the above case the State Administration answered that the scheme was earlier started by the State Administration in the year 2003 where self-help groups supplied food. However, administration experienced that supply by self-help groups was not proper and successful and therefore it was decided by the Cabinet that self-help groups would supply food for 4 days and the manufacturers in all the districts would supply remaining 2 days food. It was also decided that if the self-help groups would able to make proper supply then they would given a chance for supplying food for all the days.
6.3 Orders of Supreme Court and Violation Continues
The Supreme Court directed on October 7th, 2004 that “contractors shall not be used for supply of nutrition in Anganwadis and preferably ICDS funds shall be spent by making use of village communities, self-help groups and Mahila Mandals for buying of grains and preparation of meals”.
l Besides the above order of Supreme Court Women and child development department involved manufacturers for the supply of supplementary nutrition food
Moribund ICDS61

for 3 days in a week in anganwadis of Gwalior district. The WCD of the district gave contracts to the private suppliers via following letters-
l Letter Q-19/ WCD/SNF/06/484 DATED- 22-2-06
l Letter-Q-19/WCD/SNF/06/374 DATED- 10-2-06
l According to the contract by WCD dated 19 January 2006 with Anil industries Indore for one year clearly mentioned the supply panjiri for 2 days and murmure for 2 days (i.e. 4 days in a week) in urban and rural projects of ICDS in Dewas district.
l In Ratlam district WCD department has made a contract with Ms. Anil industries, Indore on 1-3-06 for supplying supplementary nutrition for 4 days in week in urban areas of the District.
It is amply clear from the above facts that Court's order, whether it is Apex Court or High Court, are not decisive enough to resurrect the whole system but a collective effort from civil society is need of an hour for constantly pursuing the issue. The facet of accountability has been constantly ignored. Although the Supreme Court has stated that, in the case of starvation deaths and deaths due to malnutrition, the Chief Secretary of the concerned State and the Collectors are to be held liable. But the order seems too remained on the paper itself and not followed religiously in practice. It is high time that the order be complied with. As a general trend it was observed that whenever there is death reported, each time, lower level authorities like village level health worker or panchayat secretary are the first to be blamed for and may suspended at times. But the higher-level officials like the District Medical Officer, Collector etc, had never been held liable on the account. Such incidences are repeated owing to no stringent action against the concerned authorities.
Not only this is the case of Madhya Pradesh but also almost all the states across the country are facing more or less same deformity. Besides Madhya Pradesh, news about large-scale disruptions is coming from Jharkhand and Uttar Pradesh. Organization named CARE used to provide food to ICDS centres in large parts of Jharkhand, but the supply was abruptly discontinued in year 2002 following a dispute between the governments of US and India over the presence of genetically modified (GM) food in the supply. Failure to make reliable and alternative arrangements by the Jharkhand government led to major set back in the providing supplementary food to ICDS centres. In Uttar Pradesh food distribution to ICDS centres is often held up for months together for trivial reasons such as the failure to sanction tenders. But the most shocking part of the story is that none of this has led to furor, as hungry children have no voices.
Supreme Court Orders on ICDSSignificant amount of public attention has been drawn to the ICDS in recent years. This is partly due to interim orders passed by the Supreme Court in the 'right to food case', a writ petition currently pending before the Supreme Court of India (Civil Writ Petition 196/2001, People's Union for Civil Liberties v. Union of India and others). In this writ petition, the Supreme Court has taken the view that the denial of the 'right to food' amounts to the denial of the fundamental 'right to life and personal liberty' enshrined in Article 21 of the Constitution of India. The ICDS has since been recognised as central to safeguarding the 'right to food' of young children (up to six years of age), pregnant women, nursing mothers and adolescent girls. The noteworthy orders are highlighted here.
Box - 16
Moribund ICDS62
Order dated 28 November 2001l Each child up to 6 years of age should get 300 calories and 8-10 grams of protein.
l Each adolescent girl to get 500 calories and 20-25 grams of protein.
l Each pregnant woman and each nursing mother to get 500 calories and 20- 25 grams of protein.
l Each malnourished child to get 600 calories and 16-20 grams of protein.
l Every settlement is to have a disbursement centre called anganwadi.
Order dated 29 April 2004l All 0-6 year old children, adolescent girls, pregnant women and nursing mothers shall receive
supplementary nutrition for 300 days in the year.
Order dated 7 October 2004l The number of anganwadis shall be increased from 6 to 14 lakh in the country.
l The minimum norm for the provision of supplementary nutrition should be increased to Rs. 2/- per child per day.
l All sanctioned anganwadis shall be operationalize immediately.
l All SC/ST habitations shall have anganwadis as early as possible, and habitations with high SC/ST populations should receive priority in the placement of new anganwadis.
l Earnest efforts should be made to cover all slums under ICDS.
l ICDS services should never be restricted to BPL families (“BPL shall not be used as an eligibility criterion for ICDS”).
l Contractors shall not be used for the supply of supplementary nutrition.
l Local women's Self-Help Groups and Mahila Mandals should be encouraged to supply the supplementary food distributed in Anganwadis. They can make purchases, prepare the food locally, and supervise the distribution.
l The Central Government and States/UTs shall ensure that all amounts allocated are sanctioned in time so that there is no disruption whatsoever in the feeding of children.
l ICDS funds provided by the Central Government under the Pradhan Mantri Gramodaya Yojana (PMGY) should be fully utilised by the State Governments. Further these funds should supplement, and not substitute for, ICDS funds provided by the State Governments.
l All State Governments/UTs shall put on their websites, full data for the ICDS programme including where AWCs are operational, the number of beneficiaries category-wise, the funds allocated and used, and other related matters.
Order dated 13 December 2006This landmark judgment clearly orders the government to ensure "Universalization with Quality" in a time-bound manner and further strengthen the entitlements of children under six.
l The universalisation of the ICDS involves extending all ICDS services (Supplementary nutrition, growth monitoring, nutrition and health education, immunization, referral and pre-school education) to every child under the age of six, all pregnant women and lactating mothers and all adolescent girls.
l All 14 lakh AWCs shall be sanctioned and operationalized in a phased and even manner starting forthwith and ending December 2008. In doing so all SC/ST habitations must be identified on priority basis.
Moribund ICDS63
l Population norms for opening of AWCs must not be revised upward under any circumstances. While maintaining the upper limit of one AWC per 1000 population, the minimum limit for opening of a new AWC is a population of 300 may be kept in view. Further, rural communities and slum dwellers should be entitled to an "Anganwadi on Demand" (not later than three months) from the date of demand in cases where a settlement has at least 40 children under six but no anganwadi.
l The order also specifies the monetary allocation to be made per beneficiary under the ICDS scheme. The court instructed all State Governments and Union Territories to fully implement the ICDS scheme by, inter-alia-
v Allocating and spending at least Rs. 2/- per child per day for supplementary nutrition out of which the Central Government shall contribute Rs. 1 per child per day.
v Allocating and spending at least Rs. 2.70 for every severely malnourished child per day for supplementary nutrition out of which the Central Government shall contribute Rs. 1.35 per child per day.
v Allocating and spending at least Rs. 2.30 for every pregnant woman, nursing mother/adolescent girl per day for supplementary nutrition out of which the Central Government shall contribute Rs. 1.15.
l Chief Secretaries of all State Governments/UTs are directed to submit affidavit-giving details of all the habitations with a majority of SC/ST households, availability of AWCs in these habitations, and the plan of action for ensuring that all these habitations have functioning AWCs within two years.
l Chief Secretaries of all State Governments/UTs are directed to submit affidavits giving details of the steps that have been taken in regard to the order of this Court of October 7th, 2004 directing that "contractors shall not be used for supply of nutrition in Anganwadis and preferably ICDS funds shall be spent by making use of village communities, self-help groups and Mahila Mandals for buying of grains and preparation of meals". Chief Secretaries of all State Governments/UTs must indicate a time-frame within which the decentralization of the supply of SNP through local community shall be done.
Several of these orders are yet to be implemented in fully by the Central and State Governments. The most significant amongst these are orders to ensure that all children from 0-6 years, pregnant and nursing mothers and adolescent girls have access to ICDS services and further that all settlements, especially SC/ST settlements have access to an anganwadi. (For further details see Supreme Court Orders on the Right to Food: A Tool for Action, available from the secretariat of the right to food campaign.)
Moribund ICDS64
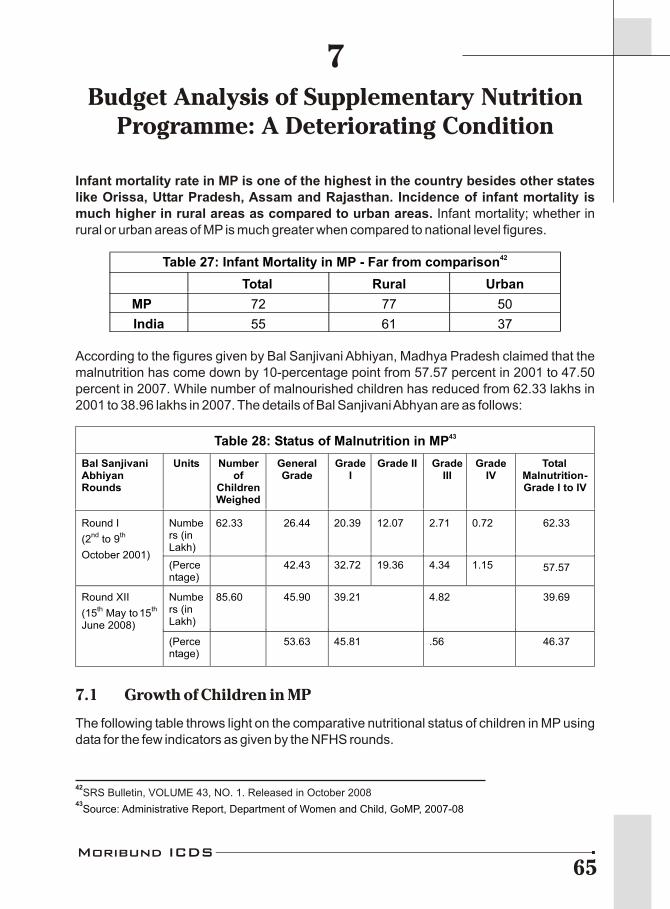
Budget Analysis of Supplementary NutritionProgramme: A Deteriorating Condition
7
Infant mortality rate in MP is one of the highest in the country besides other states like Orissa, Uttar Pradesh, Assam and Rajasthan. Incidence of infant mortality is much higher in rural areas as compared to urban areas. Infant mortality; whether in rural or urban areas of MP is much greater when compared to national level figures.
According to the figures given by Bal Sanjivani Abhiyan, Madhya Pradesh claimed that the malnutrition has come down by 10-percentage point from 57.57 percent in 2001 to 47.50 percent in 2007. While number of malnourished children has reduced from 62.33 lakhs in 2001 to 38.96 lakhs in 2007. The details of Bal Sanjivani Abhyan are as follows:
7.1 Growth of Children in MP
The following table throws light on the comparative nutritional status of children in MP using data for the few indicators as given by the NFHS rounds.
42Table 27: Infant Mortality in MP - Far from comparison
Total Rural Urban
MP 72 77 50
India 55 61 37
42SRS Bulletin, VOLUME 43, NO. 1. Released in October 2008
43Source: Administrative Report, Department of Women and Child, GoMP, 2007-08
43Table 28: Status of Malnutrition in MP
Bal Sanjivani Abhiyan Rounds
Units Number of
Children Weighed
General Grade
Grade I
Grade II Grade III
Grade IV
Total Malnutrition- Grade I to IV
Numbers (in Lakh)
62.33 26.44 20.39 12.07 2.71 0.72 62.33 Round I
(2nd
to 9th
October 2001) (Percentage)
42.43 32.72 19.36 4.34 1.15 57.57
Numbers (in Lakh)
85.60 45.90 39.21 4.82 39.69 Round XII
(15th May to15
th
June 2008)
(Percentage)
53.63 45.81 .56 46.37
Moribund ICDS65
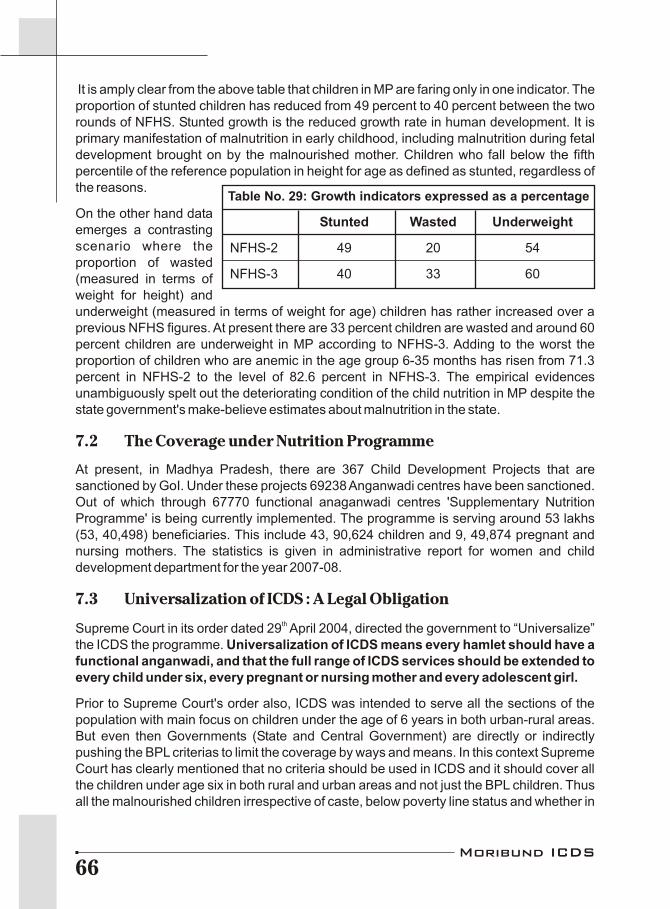
It is amply clear from the above table that children in MP are faring only in one indicator. The proportion of stunted children has reduced from 49 percent to 40 percent between the two rounds of NFHS. Stunted growth is the reduced growth rate in human development. It is primary manifestation of malnutrition in early childhood, including malnutrition during fetal development brought on by the malnourished mother. Children who fall below the fifth percentile of the reference population in height for age as defined as stunted, regardless of the reasons.
On the other hand data emerges a contrasting scenario where the proportion of wasted (measured in terms of weight for height) and underweight (measured in terms of weight for age) children has rather increased over a previous NFHS figures. At present there are 33 percent children are wasted and around 60 percent children are underweight in MP according to NFHS-3. Adding to the worst the proportion of children who are anemic in the age group 6-35 months has risen from 71.3 percent in NFHS-2 to the level of 82.6 percent in NFHS-3. The empirical evidences unambiguously spelt out the deteriorating condition of the child nutrition in MP despite the state government's make-believe estimates about malnutrition in the state.
7.2 The Coverage under Nutrition Programme
At present, in Madhya Pradesh, there are 367 Child Development Projects that are sanctioned by GoI. Under these projects 69238 Anganwadi centres have been sanctioned. Out of which through 67770 functional anaganwadi centres 'Supplementary Nutrition Programme' is being currently implemented. The programme is serving around 53 lakhs (53, 40,498) beneficiaries. This include 43, 90,624 children and 9, 49,874 pregnant and nursing mothers. The statistics is given in administrative report for women and child development department for the year 2007-08.
7.3 Universalization of ICDS : A Legal ObligationthSupreme Court in its order dated 29 April 2004, directed the government to “Universalize”
the ICDS the programme. Universalization of ICDS means every hamlet should have a functional anganwadi, and that the full range of ICDS services should be extended to every child under six, every pregnant or nursing mother and every adolescent girl.
Prior to Supreme Court's order also, ICDS was intended to serve all the sections of the population with main focus on children under the age of 6 years in both urban-rural areas. But even then Governments (State and Central Government) are directly or indirectly pushing the BPL criterias to limit the coverage by ways and means. In this context Supreme Court has clearly mentioned that no criteria should be used in ICDS and it should cover all the children under age six in both rural and urban areas and not just the BPL children. Thus all the malnourished children irrespective of caste, below poverty line status and whether in
Table No. 29: Growth indicators expressed as a percentage
Stunted Wasted Underweight
NFHS-2 49 20 54
NFHS-3 40 33 60
Moribund ICDS66

rural or urban area should be covered.
7.4 Resource Gap Analysis in the context of Universalization of ICDS
7.4.1 Required number of Anganwadi Centers
Projected population for Madhya Pradesh for 2007-08 is 68666478 that is around 6.87 44Crore . As per government norm one anganwadi centre should be opened per 400-800
population. Considering the maximum population of 800, there is a need of at least 85,833 anganwadi centers in MP. But going by the coverage figures given by WCD, GoMP, there is a gap of around 19.33 percent between required and sanctioned one. The gap increase to 21.04 percent when taken into consideration the number of functional anganwadi centers.
Going by Supreme Court's order for universalization of ICDS, there should be a functional anganwadi centre in every hamlet. Numbers of hamlets in Madhya Pradesh are around
461.27 lakhs . In that case MP should have 1.27 lakhs functional anganwadi centre in the state. When compared with sanctioned number of anganwadi centers the gap is of 45 percent, which gets widen further to around 47 percent in comparison with number of functional anganwadi centers.
7.4.2 A truth of beneficiaries covered
The projected population of children in age group 0-6 for Madhya Pradesh is 12081967, 47that is 1.20 crore approximately . The prevalent rate of malnutrition in the state, according
thto 10 round of Bal Sanjivani Abhiyan is 47.5 percent. Going by this there are around 57.39 lakh (57, 38,934) children in the state are suffering from malnourishment. State government
Required Number of Anganwadi Centre
85833 Required Number of
Anganwadi Centre
85833
Sanctioned anganwadi centers
69238
Functional anganwadi centers
67770
Gap 16595 (19.33%)
Gap
18063 (21.04%)
Hamlet-wise Number of anganwadi centers45
127397
Hamlet-wise Number of anganwadi centers
127397
Gap 58159 (45.00%) Gap 59627 (46.80%)
Table No. 30: Gap between the required number of anganwadi centers and the sanctioned one
44Projected population for the state for 2007-08 has been calculated by applying growth
rate on the projected population figure of 2006 as provided by the Census of India.45
As Supreme Court mentions it its orders that each hamlet should have anganwadi center.46
Source: National Habitation Survey, GoI, 2003.47
Projected population for the age group 0-6 for 2007-08 has been calculated on the basis of2001 population and then by applying the growth rate provided by Census of India.
Moribund ICDS67
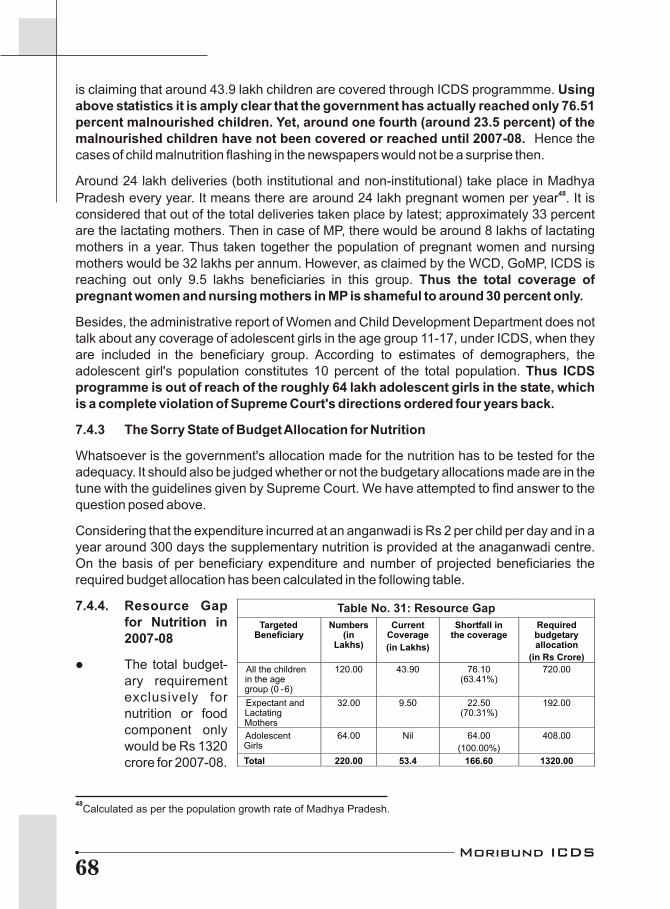
is claiming that around 43.9 lakh children are covered through ICDS programmme. Using above statistics it is amply clear that the government has actually reached only 76.51 percent malnourished children. Yet, around one fourth (around 23.5 percent) of the malnourished children have not been covered or reached until 2007-08. Hence the cases of child malnutrition flashing in the newspapers would not be a surprise then.
Around 24 lakh deliveries (both institutional and non-institutional) take place in Madhya 48Pradesh every year. It means there are around 24 lakh pregnant women per year . It is
considered that out of the total deliveries taken place by latest; approximately 33 percent are the lactating mothers. Then in case of MP, there would be around 8 lakhs of lactating mothers in a year. Thus taken together the population of pregnant women and nursing mothers would be 32 lakhs per annum. However, as claimed by the WCD, GoMP, ICDS is reaching out only 9.5 lakhs beneficiaries in this group. Thus the total coverage of pregnant women and nursing mothers in MP is shameful to around 30 percent only.
Besides, the administrative report of Women and Child Development Department does not talk about any coverage of adolescent girls in the age group 11-17, under ICDS, when they are included in the beneficiary group. According to estimates of demographers, the adolescent girl's population constitutes 10 percent of the total population. Thus ICDS programme is out of reach of the roughly 64 lakh adolescent girls in the state, which is a complete violation of Supreme Court's directions ordered four years back.
7.4.3 The Sorry State of Budget Allocation for Nutrition
Whatsoever is the government's allocation made for the nutrition has to be tested for the adequacy. It should also be judged whether or not the budgetary allocations made are in the tune with the guidelines given by Supreme Court. We have attempted to find answer to the question posed above.
Considering that the expenditure incurred at an anganwadi is Rs 2 per child per day and in a year around 300 days the supplementary nutrition is provided at the anaganwadi centre. On the basis of per beneficiary expenditure and number of projected beneficiaries the required budget allocation has been calculated in the following table.
7.4.4. Resource Gap for Nutrition in 2007-08
l The total budget-ary requirement exclusively for nutrition or food component only would be Rs 1320 crore for 2007-08.
48Calculated as per the population growth rate of Madhya Pradesh.
Targeted Beneficiary
Numbers (in
Lakhs)
Current Coverage
(in Lakhs)
Shortfall in the coverage
Required budgetary allocation
(in Rs Crore)
All the children in the age group (0 -6)
120.00 43.90 76.10 (63.41%)
720.00
Expectant and Lactating Mothers
32.00 9.50 22.50 (70.31%)
192.00
Adolescent Girls
64.00 Nil 64.00
(100.00%)
408.00
Total 220.00 53.4 166.60 1320.00
Table No. 31: Resource Gap
Moribund ICDS68
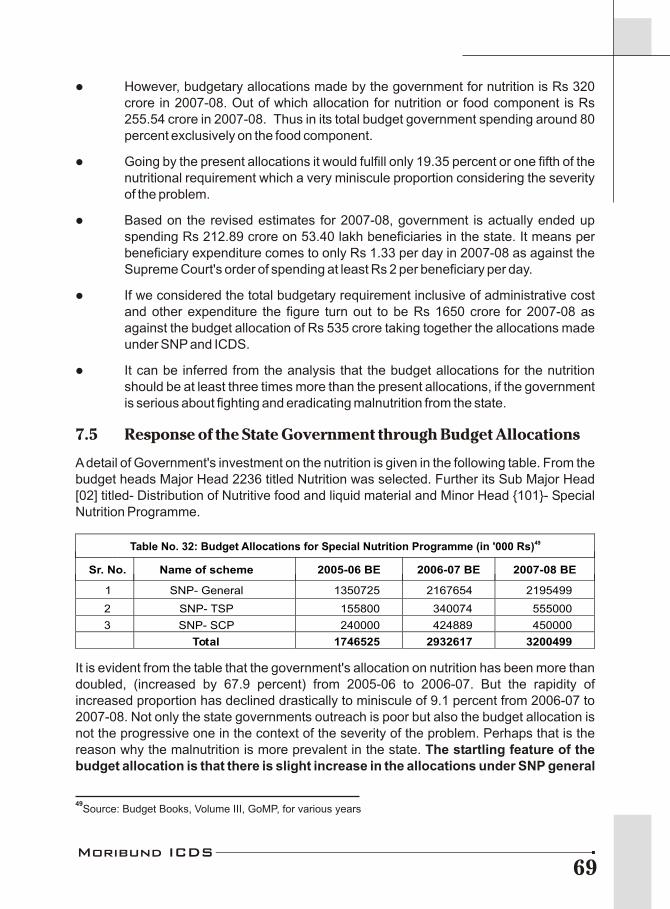
l However, budgetary allocations made by the government for nutrition is Rs 320 crore in 2007-08. Out of which allocation for nutrition or food component is Rs 255.54 crore in 2007-08. Thus in its total budget government spending around 80 percent exclusively on the food component.
l Going by the present allocations it would fulfill only 19.35 percent or one fifth of the nutritional requirement which a very miniscule proportion considering the severity of the problem.
l Based on the revised estimates for 2007-08, government is actually ended up spending Rs 212.89 crore on 53.40 lakh beneficiaries in the state. It means per beneficiary expenditure comes to only Rs 1.33 per day in 2007-08 as against the Supreme Court's order of spending at least Rs 2 per beneficiary per day.
l If we considered the total budgetary requirement inclusive of administrative cost and other expenditure the figure turn out to be Rs 1650 crore for 2007-08 as against the budget allocation of Rs 535 crore taking together the allocations made under SNP and ICDS.
l It can be inferred from the analysis that the budget allocations for the nutrition should be at least three times more than the present allocations, if the government is serious about fighting and eradicating malnutrition from the state.
7.5 Response of the State Government through Budget Allocations
A detail of Government's investment on the nutrition is given in the following table. From the budget heads Major Head 2236 titled Nutrition was selected. Further its Sub Major Head [02] titled- Distribution of Nutritive food and liquid material and Minor Head {101}- Special Nutrition Programme.
It is evident from the table that the government's allocation on nutrition has been more than doubled, (increased by 67.9 percent) from 2005-06 to 2006-07. But the rapidity of increased proportion has declined drastically to miniscule of 9.1 percent from 2006-07 to 2007-08. Not only the state governments outreach is poor but also the budget allocation is not the progressive one in the context of the severity of the problem. Perhaps that is the reason why the malnutrition is more prevalent in the state. The startling feature of the budget allocation is that there is slight increase in the allocations under SNP general
49Table No. 32: Budget Allocations for Special Nutrition Programme (in '000 Rs)
Sr. No.
Name of scheme 2005-06 BE 2006-07 BE 2007-08 BE
1 SNP- General 1350725 2167654 2195499
2 SNP- TSP 155800 340074 555000
3 SNP- SCP 240000 424889 450000
Total 1746525 2932617 3200499
49Source: Budget Books, Volume III, GoMP, for various years
Moribund ICDS69
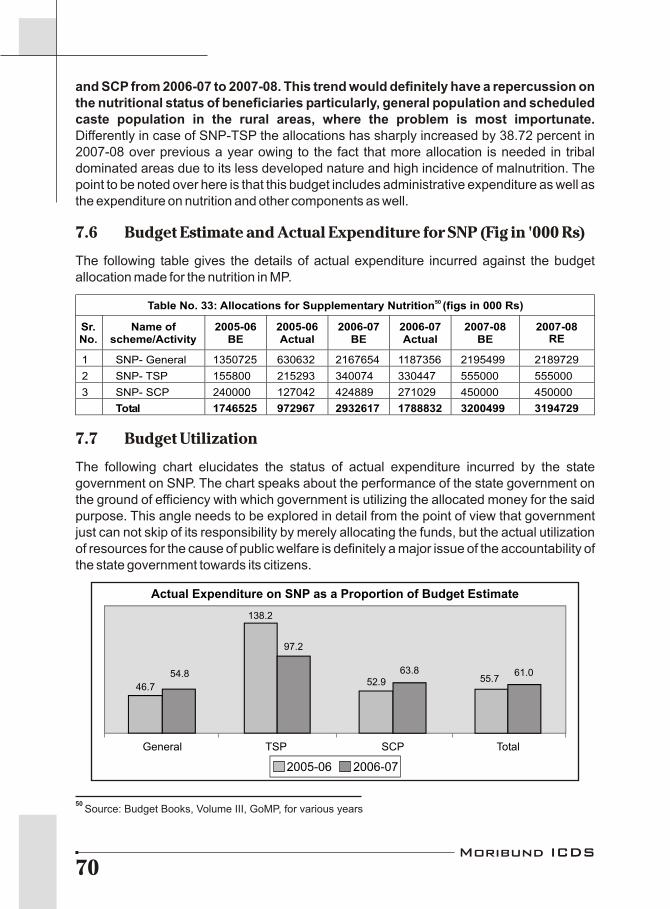
and SCP from 2006-07 to 2007-08. This trend would definitely have a repercussion on the nutritional status of beneficiaries particularly, general population and scheduled caste population in the rural areas, where the problem is most importunate. Differently in case of SNP-TSP the allocations has sharply increased by 38.72 percent in 2007-08 over previous a year owing to the fact that more allocation is needed in tribal dominated areas due to its less developed nature and high incidence of malnutrition. The point to be noted over here is that this budget includes administrative expenditure as well as the expenditure on nutrition and other components as well.
7.6 Budget Estimate and Actual Expenditure for SNP (Fig in '000 Rs)
The following table gives the details of actual expenditure incurred against the budget allocation made for the nutrition in MP.
7.7 Budget Utilization
The following chart elucidates the status of actual expenditure incurred by the state government on SNP. The chart speaks about the performance of the state government on the ground of efficiency with which government is utilizing the allocated money for the said purpose. This angle needs to be explored in detail from the point of view that government just can not skip of its responsibility by merely allocating the funds, but the actual utilization of resources for the cause of public welfare is definitely a major issue of the accountability of the state government towards its citizens.
50 Source: Budget Books, Volume III, GoMP, for various years
50 Table No. 33: Allocations for Supplementary Nutrition (figs in 000 Rs)
Sr.No.
Name of scheme/Activity
2005-06 BE
2005-06 Actual
2006-07 BE
2006-07 Actual
2007-08 BE
2007-08RE
1 SNP- General 1350725 630632 2167654 1187356 2195499 2189729
2 SNP- TSP 155800 215293 340074 330447 555000 555000
3 SNP- SCP 240000 127042 424889 271029 450000 450000
Total 1746525 972967 2932617 1788832 3200499 3194729
2005-06 2006-07
Actual Expenditure on SNP as a Proportion of Budget Estimate
General
46.7
54.8
138.2
97.2
52.963.8
55.761.0
TSP SCP Total
Moribund ICDS70

The above chart depicts a very disheartening picture of utilization of public funds. The overall actual expenditure although has increased in 2006-07 over the previous year, its utilization rate is very poor. The WCD department has been able to utilized only 61 percent of its budget allocation leading to exorbitant savings of around 40 percent in 2006-07. This has been very rightly pointed out by CAG report for Madhya Pradesh. Similar trend is observed in case of budget utilization for the general category and the utilization for dalit population. It is only the utilization for the tribal population showing at par budget utilization on paper. Higher utilization in 2005-06 is due to increased budget in revised estimates owing to supplementary budget. But the ground realities have many more reasons to question the performance as discussed in detail in the previous chapters. It's a total underutilization of the allocated funds indicating lack of efficiency of the concern government functionaries to spend what was budgeted for and indicates their insensitiveness towards the prime issue in the state.
7.8 ICDS in Budget Books
To locate ICDS sce in the budget books, one has to search for the Major Head 2235- titled Social Security and Welfare with Sub Major Head [02]- Social Welfare, Minor Head {102}- Child Welfare and then the Sub Head (658)-ICDS. Details of ICDS budgets are given in the following table. It is evident from the table that the budget allocation for ICDS has increased by almost 58 percent from Rs 104 crore in 2005-06 to Rs 253 crores in 2008-09. Budget allocation for 2007-08 shows the highest annual increment of about 63.2 percent over the previous year. Similarly, in the year 2006-07, both revised estimates and actual figures shows tremendous increase over of 85.4 % and 116.4 % respectively over the previous year. As far as budget allocation part is concerned over here the things are doing fine but the real crunch is noticed when it comes to budget utilization. The performance in the budget utilization is definitely on the lower side. There were unutilized funds to the tune of around 30 percent and 20 percent respectively in 2005-06 and 2006-07, although the utilization proportion has increased in 2006-07 over the previous year. However, the work does not really stopped here; the numerous reasons for the underutilization and the major defaulters in the system needs to further investigated using both primary and secondary researchemh.
Interestingly, under the object head of the ICDS programme # 34- Material and supply a fund of Rs 28 crore has been booked under the detail head 009- other expenditure in 2008-09. While if one compared these heads with that of Nutrition, its 004- value of ration or nutrition expenditure, with allocation of around Rs 216 crore. Therefore question arises out here is that whether it's a same nutritional component of ICDS or the something else? The fact needs to be corrected before going for detailed analysis.
But the interesting part is that this amount does not take into account nutritional component. Rather one has to search another major head 2236-titled Nutrition for identifying the component of Supplementary Nutrition Programme.
Table No. 34: Budgets of ICDS (excluding nutritional component)
Year Budget Estimates (BE)
Revised Estimates (RE)
Actual (AC)
2005-06 1048532 1065815 736131
2006 07 1322567 1976338 1593090
2007-08 2158264 2371907
2008-09 2530617
Moribund ICDS71
7.9 Latest addition
State government has launched another programme “Project Shaktiman” by the in 2007-08. Main objective of the programme is to eradicate malnutrition completely among the children of tribal dominated villages and other villages, as well as among the women. Presently, 39 blocks of 19 districts have been chosen for the implementation of the programme. On an average each anaganwadi centre provides nutrition of Rs 2 per child per day. But under the programme Project Shaktiman, state government from its side providing additional Rs 4, thus under the programme the expenditure on children would be Rs 6 per child per day. The names of the districts are: Vidisha, Dhar, Jhabua, Khargone, Barwani, Shadol, Anuppur, Umaria, Betul, Mandla, Dindori, Seoni, Balaghat, Sheopur, Shivpuri, Ashoknagar, Hoshangabad, Harda and Chhindwara. Government has set the target of reaching around 60,000 children. Although the programme has been launched in 2007-08, the concomitant budget allocations were found only in the year 2008-09, indicating a year's lag in actual programme implementation. Government has made allocation of Rs 16 crore for Project Shaktiman.
7.10 Criticism by Comptroller and Auditor General (CAG)
CAG in its report for 2005-06 had scorn off openly at the WCD of Madhya Pradesh government on poor implementation of ICDS while mentioning its observations. Some of the CAG remarks are summarized as follows:
1) Impact of welfare schemes for women and child was marginal especially on the health and nutritional status of children as more than 55 percent of children were malnourished in the state.
2) Nutritional support could not be provided to eligible beneficiaries due to low budget provisions.
3) Substantial and persistent savings were registered owing to poor budgetary and expenditure control.
4) Large number of posts remaining vacant and improper manpower planning affected implementation and monitoring of the scheme.
5) Due to inadequate budget provision and delay in the release of funds to districts offices, 52 to 62 percent children and 46-59 percent expectant and nursing mothers were remained deprived of the nutritional support.
Finally : It is the fact corroborated from the analysis once again that the pace of imple-
mentation of the nutrition programme is despicable, not only it can be overlooked as the routine poor implementation but needs a thorough brainstorming. Government has failed in preventing malnutrition deaths. The responsible agencies must be held accountable for the shameful deeds for the sake of saving the children from the deadliest situation. There is a complete violation of the Supreme Court's directions as far as beneficiaries covered and the amount being spent per beneficiary. Even after the four years of Supreme Courts orders the budget allocation are not proportionate to the needs of beneficiaries. One has to be very clear their mind that this overwhelming situation has not spurted out in a day or two but is out of sheer negligence that has been carried out in since the past.
Moribund ICDS72

Exceptions Are Always There…
8
So long we have seen that the Integrated Child Development Scheme has always been the sufferer of utter negligence even though ICDS is the only national programme to address the health, nutrition and pre-school needs of children under six years. Though children contributes about 15 % of the total population but still the rights of this most important section of our society has always been neglected or under estimated whether it is in policies or priorities of government and political leaders. This is perhaps because these young children do not form the vote bank so as to facilitate politicians. But in spite of all these adverse conditions, still there exist a hope that the very purpose of ICDS i.e. "to make the childhood a healthy one for transforming into a strong, healthy and all round physically fit younger generation" can be served to each and every child if the community participation is ensured. The care of young children cannot be left to the family alone it is also a social responsibility. Social intervention is required, both in the form of enabling parents to take better care of their children at home, and in the form of direct provision of health, nutrition, pre-school education and related services.
ICDS centers of Balaghat district and Khalwa block in Khandwa district of the State are setting the example before every one that occurrence of malnutrition can be controlled through proper implementation of ICDS scheme and most importantly by promoting community participation thus proving that exceptions are always there.
8.1 Balaghat : A district paving its own way
Balaghat district of Madhya Pradesh is setting an example for other districts to tackle the grass root problems with an innovative idea. The community of the district has attempted to sort out the issues by their own. Now, the malnutrition is no more a problem here, malnourished children have not to lose their life any more. Now the list of malnourished children is displayed at panchayat bhavan; the panchayat and community take the responsibility of saving as well as treatment of these children. Every malnourished child is identified at time and referred to NRC for sure. To promote the use of traditional food practices in such a manner that they fulfill are the nutritional requirements, “Grain Kits” are displayed in Anganwadi Centers. Similarly, “Maternity Kit” is being promoted to make aware women about health and hygiene.
All these initiatives taken by the people of Balaghat district are setting a modal for others and showing a new light of hope. The community is not only taking the responsibility to tackle the problem by their own but also making aware public leaders about the issues, especially the malnutrition and making them to act on the same. These steps of the district are no doubt setting as example, which must be replicated in other districts also. But the probing question is that will the State Administration ever recognize the initiative of Balaghat district?
Today even the most backward community residing in Balaghat district i.e. Baiga (which is also one of the 3 Primitive Tribal Group (PTG) in the State) is also well aware of the benefits
Moribund ICDS73

of vaccination, medicines and even institutional deliveries. The situation was not so favorable in Balaghat a few years back but continuous efforts of the district and its people make it possible.
Effort - 1
Sukwarobai Baiga from Baigatola of Gohra panchayat, which is 15 km far from Baihar block of the district, had already lost four of her children and now she is expecting for the 5th time. When Anganwadi worker and ANM tried to approach Sukwarobai for her immunization, she use to escape in the near by forest at the moment. Not only Sukwaro bai but also most of the women of the village were afraid of getting immunized and other health services. But due to the regular efforts of AWW and ANM to aware Sukwaro bai as well as all the villagers about the advantages of immunization and safe delivery, Sukwaro bai not only agreed to get immunized but also went for institutional delivery. Her newly born baby also got all the vaccinations on time and the result is healthy Sukwaro bai with healthy and YES alive baby!
Effort - 2
Similarly, the baigas of Karwahi panchayat use to affraid of and were far off the benefits of vaccination, institutional deliveries and other health services. Due to this the percentage of vaccination was about nil in the baigatola of karwahi panchayat but today about 98% vaccinations is done in this region. It seems to be untrue but all this is due to the restless efforts of Bansilaal Tilagaam, one of the panch along with Anganwadi worker of the village. This is not only the story of the mentioned two villages but there are a number of villages in Balaghat district, which are now well aware of the importance of health services. And the peoples have adopted a participatory approach to plan for a better maternal & child health, community health as well as vaccination programs.
Effort - 3
A health initiative named Integrated Nutrition and Health Project (INHP) was started in the four blocks of Balaghat district by a local organization called Community Development Center (CDC) with the help of CARE four years back. The ultimate aim of INHP program was to bring qualitative changes in the health status of children and women. Director of CDC Mr. Ameen Charles says that starting this project in Balaghat district was not an easy task because the district is a tribal populated area, which is far from the main stream of development. But still we accepted the challenge. The first task done by CDC was organizing orientation programs for Anganwadi workers so as to strengthen them, says Ameen. Besides this, the community was also being sensitized and mobilized about the health services and their benefits using banners, posters, short plays, hamlet meetings etc. The Government departments of WCD and Health plays important role in this project and because there is no co-ordination between these departments so the task becomes further challenging. Sometimes Anganwadi workers were performing well but were not getting the support of health workers due to which the health services and vaccination program were not functioning properly at village level. These situations make the task more challenging. The CDC members first of all tried and assured the presence of health workers in the sector meetings of anganwadi workers and vice-versa. This result was worth and meetings
Moribund ICDS74

resulted in creating a co-ordination between the two departments at grassroot level and at the same time the difficulties as well as needs related to the health status of villages were well identified. The efforts of INHP can be analyzed by the fact that there is a remarkable decrease in the level of malnutrition in Balaghat.
Mamta, one of the members of CDC told that previously the occurrence of malnutrition among children was high in the district and consequently the rate of child mortality was also high. Therefore, they (CDC team members) focused the issue of malnutrition and organized special workshops for Anganwadi workers (AWW) to tackle the problem. Anganwadi workers were told that the locally available food stuffs are sufficiently rich in protein, iron and fats and thus their nutritious value is also good, the only thing is the right utilization or consuming practices of these food stuffs. The hurdle before AWW was how to each the villagers about the right consuming practice of locally available foodstuffs. Making “Nutritious Food Kit” locally known as “Anaj Kit” then solved this problem. The kit contains samples of rice, maize, pulses (urad & tuar), gram, groundnut, murmure along with jaggery and oil. The kit was displayed in each Anganwadi Center and it really worked in teaching mothers as well as the community how and what to feed a malnourished child.
Effort - 4
According to health workers along with malnutrition deaths of kids the district was also facing the problem of maternal health. The rate of deaths of pregnant women was also quite noticeable in the district. So they started the counseling of pregnant women and told them about the advantages of institutional deliveries and disadvantages of home deliveries. Women were also told that if (in any case) home delivery is the only choice than one should take the help of trained dais (midwives). All the pregnant women were made to learn to make a “Health Kit” containing a fresh reel of thread, a fresh piece of cloth, soap, iron tablets and a new blade on every Mangal Diwas of Anganwadi Center. Also, all the expecting mothers were made to take oath on every Mangal Diwas that they will go for institutional deliveries anyhow and if in any case it is not possible than they will use the Health Kit during their deliveries.
Effort - 5
Anganwadi worker Vimla Meshram told that previously women use to dispose off the iron and folic acid tablets given to them but now they not only take the tablets timely but also promote their neighboring women to take the tablets regularly. In Madhya Pradesh probably Balaghat is the only district where Anganwadi workers are having there uniform. Here AWW are having a special status in the society, they are given respect and get proper support of community. Anganwadi Centers of the district are being developed as a Child Right's Center and the attendance of children in the Centers is also satisfactory.
Effort - 6
The process of innovative steps to tackle grassroot problems like malnutrition does not halt here, says project coordinator Mr. Satish Jain. We tried that the list of malnourished children get displayed at panchayat bhavans and the panchayat should take the responsibilities of these children. Though we have to face a lot of difficulties in starting but the regular efforts
Moribund ICDS75

and discussions with panchayat members made it possible and slowly & gradually panchayats also showed interest in the process and started to take the responsibilities of malnourished children. Along with panchayat leaders, parents/mothers committee was also sensitized about the issue. And now the list of malnourished children is displayed at panchayat bhavans. Now every malnourished child is the responsibility of the panchayat as well as community groups and they are ready to take all the possible stands to save the children life. Sarpanch of Boda panchayat Smt. Seema Meshram has invested money from her pockets to arrange milk and nutritious food for underweight children so as to bring them to normal grades.
The communities are also aware of severe malnutrition and its consequences and are promoted to take the severely malnourished children to NRCs.
Effort - 7
Nirmala Uike, the Anganwadi worker of village Chhinditola says that previously we find it quite difficult to work as an Anganwadi worker and to convince people to send their children as well as get associated with Anganwadi Centers. Also, we were not getting the proper support of health department but now there are no such difficulties. The coordination between WCD and Health Departments has made the things better and now we are having an identity and respect in society, we have a special uniform also. Now the women are conscious about their health and health facilities. The practice of breastfeeding to newly born child within half an hour of birth as well up to 2 years has also increased in the district.
On one hand when all across the State the issues of children deaths due to malnutrition are continuously being encountered at the same time the joint efforts of CDC and CARE have made it possible in Balaghat district to reduce the death tolls due to malnutrition. The INHP program has made the community conscious about the grassroot issues and a participatory approach has been developed among the community. The result of these efforts is that the level of malnutrition deaths in the district has decreased by 6 percents in last 2 years. All these efforts being practiced in Balaghat district have proved that if there is a will there is a way. The district has set an example that with a little attention and a proper coordination between the related departments any problem, even the huge malnutrition problem, can be handled with an ease. Now the point is whether our State administration will ever give attention to the brilliant attempt of Balaghat district so that it can be replicated in other districts also or not!
8.2 Mai's local initiative for Child Protection in Khandwa :
Effort - 8
Fokatpura tribal habitation of Khalwa. Almost all the children of this tribal hamlet visit Anganwadi regularly … they come…they play…. they learn….Shantabai is not a next of kin of these 74 children but she is known as "Mai" of these children. Four severely malnourished children were brought out of severity in this hamlet. For past one and half years none of the children here succumbed to death. Here this miracle was possible with the locally grown corn porridge and nutritional supplements made of groundnuts has
Moribund ICDS76

brightened the health of the children. What transformation can happen in children's lives by sheer committed efforts of a tribal woman in her village; this amazing truth is revealed in Fokatpura hamlet of Khalwa Block.
For past five yeas or more cases of serial deaths of smaller children due to malnutrition and infectious diseases have been recorded in this Korku tribe dominated Khalwa Block During this time in May 2007, unschooled Shantabai started an Anganwadi voluntarily at her doorsteps braving all needs, adversity and deprivations. Dozens of underfives in Shantabai's neighborhood were unable to reach the existing Anganwadi as it was more than a kilometer away and the children had to cross the highway bisecting the hamlet and the main village. Despite 74 children so prevented there was no Anganwadi center in this hamlet and Spandan's survey had identified 34 children to be malnourished with 4 of them being severe. In a way the Fokatpura initiative at child protection lacked an institutional effort. The situation demanded a new Anganwadi Center at Fokatpura that was not being heeded to. On 13th December 2006 Supreme Court in the case People's Union for Civil Liberty (PUCL) versus UOI & others directed that Anganwadis be started on demand within three months in those settlements (especially Dalit and Tribal hamlets) where children for some reason or other are unable to reach the existing center.
Spandan based on its survey and the said Supreme Court order demanded a new Anganwadi. At this time not waiting for the formal sanction, Shantabai and her husband started the Anganwadi at her home. As a matter of fact the Anganwadis in the state are seen merely as a formal and loose structure and the community and society view them as centers run as distribution of Dalia for the poor and disadvantaged children. But Shantabai has changed this perception of Anganwadi in past one and half year. When Spandan surveyed the children it was sure that the Administrative process will take time for this Anganwadi to begin. She would gather the children, ask her school going daughter to keep the children busy with songs and games. To encourage Shantabai's initiative, Spandan provided her a token support for some time. Shantabai dedicated more than half of her small house for the center, as she believed the situation of children in a small closed room would be like chickens in cage. Her family grows corn and groundnuts in their 3 acres land. They used part of this production for supplementary nutrition for children. The government of Madhya Pradesh has been continuously advocating the supply of supplementary nutrition in a centralized manner and through contractors despite Supreme Court's directives in 2004 that contractors or any company will not supply supplementary nutrition neither the supply will be centralized. Then the Mahila Mandals and Self Help Groups were assigned this responsibility. But the government of MP through an affidavit in the High Court tried to prove that these community based groups are incompetent in campaign against malnutrition and persisted with the centralized supply. It needs to be mentioned that companies prepare some supplementary nutrition at a place that is supplied to various places across the state.
In this system not only delays in supply were recorded but in many tribal pockets it was not used for being not according to the traditional food habits and in many places pests were found strolling in them. The frequent changes in nutritional policy by the state could not let a systematic process be established. Then in 2007 it was decided that Matra Sahyogini
Moribund ICDS77

Samiti (that has village women and the worker) will look after this system but in 2008 they were declared indulged in corruption. In such a scenario where the community understanding of nutrition is not believed upon, Shantabai presented an example of arresting malnutrition through corn and groundnuts. The Administrative processes and the norms for selection of an Anganwadi worker delimit the role of the community. Shantabai though initiated a process but she could not become an Anganwadi worker or helper, as she is unschooled. But she has no regrets, she just want to see children living graciously. The Anganwadi center at her home has been operating since past one and a half year but she has not been paid any rent. She still does not cry over but says for the initial six months DWCD did not provide any nutritional supplements and she fed the children from her field's corn and groundnuts; she did not receive any reimbursement of the same either. She herself fetches the drinking water. On this Shantabai says: "we shouldn't expect our daily bread from someone else." The children should get home food and not the shop food for those alone ticks the life. How long the government will feed the Company Foods.
In most parts of the country Anganwadi Center means Dalia Distribution Centers but here Shanta Bai's daughter Sumitra manages the pre school education. Not a single day passes by when the hamlet is not echoed with the chorus of Sumitra Didi and those 70 children and here there is no need to gather children; it is "Life Development Home" for them. Sumitra is a full time voluntary worker here. This family has become a pillar. ShantaBai's husband Bihari too is involved in this effort without any expectations. Bihari Bhai says: "Till the Department wants they can run Anganwadi at our home and when they need a place to construct the Center we will provide our land even. Children's love is our greatest property we are not interested in wealth…".
When we view this initiative in present context the greatest need seems to be that the community wisdom and role in their effort at protecting the child rights should be respected and not rejected. Even the UNICEF and the WHO in their joint statement has stressed that the permanent solution to malnutrition problem can be sought only by promoting community systems and Shanta Bai's efforts seems to be justifying this thought.
Moribund ICDS78

51A - Comprehensive Strategies
Children under six years of age need good nutrition, education and care in order to meet their full potential of health, well being and capacity for the rest of their lives. However, children under six (particularly those under two) and their needs rarely get any recognition in policies, programmes and budgets. Their feeding, development and care is assumed to be the responsibility only of the family.
Children are the future of society, and society has the responsibility for ensuring that they are given adequate and appropriate care. The only government programme that addresses the rights and needs of this age group is the Integrated Child Development Services (ICDS). However, the coverage of ICDS is quite limited, and the quality of the programme is also quite poor. “Universalisation with quality” is urgently required to protect the fundamental rights of children under the age of six.
The policy and programmes of the 'restructured' ICDS programme that is supposed to meet the nutritional, health, learning and development needs of children below six years of age, are in the process of being finalized. Any policy on Early Childhood Care and Development should focus on providing holistic and comprehensive care for children under six, and contain the following essential components:
l A system of food entitlements, ensuring that every child receives adequate food, not only in terms of quantity but also in terms of quality, diversity and acceptability. The food should be locally procured and produced by village communities, womens SHGs, mahila mandals or the most appropriate decentralised village forum.
l A system of child care that supplements care by the family and empowers women. Such care needs to also address their learning needs and must be provided by informed, interested adult carers, with appropriate infrastructure.
l A system of health care that provides prompt locally available care for common but life threatening illnesses. Such a system needs to address both prevention and management of malnutrition and disease.
Further early child care programmes should cater to the needs of the children of different age groups with different strategies. The three crucial age groups are:
l children 0-6 months of age the period of recommended exclusive breastfeeding,
l children 6 months to 3 years until entry into pre-school, and
l children 3 years to 6 years the pre-school years, until entry into school.
Strategies for Children under Six
9
Moribund ICDS79
51 It is a part of the paper on strategies for the children under six prepared by the working group on
children's right to food on the request of Planning Commission of India in the year 2007.
Based on this framework, the following are the ten essential interventions required to be put in place:
1. Universalised Maternity Entitlements
Women need adequate nutrition and care, including health care, during pregnancy, after delivery and when they breastfeed. They need skilled counselling and support to begin breastfeeding within the first hour. During the six months of exclusive breastfeeding, they need to stay close to their children, at the risk of losing their wages. Therefore it is necessary to have maternity entitlements that include:
l Compensation for staying home to breastfeed the very young child at the risk of losing wages or affecting their economic status, on the lines of the “Dr. Muthulakshmi Reddy Maternity Benefit Scheme” in Tamil Nadu, where women are given cash support of Rs 1,000 per month for six months starting from the 7th month of pregnancy, for care during pregnancy and after delivery.
l Adequate nutrition during pregnancy and lactation, including good quality supplementary nutrition for pregnant and lactating mothers through the ICDS.
l Adequate access to quality health care services.
l Adequate access to skilled counselling and support for early initiation of breastfeeding and exclusive breastfeeding.
2. Exclusive Breastfeeding for children up to six months
ICDS and the Health System should mainstream providing skilled counseling and support for women to practice exclusive breastfeeding for six months through adequate training of frontline workers such as ASHA, anganwadi workers and ANMs. Mitanins in Chhattisgarh have shown the way.
3. Skilled Counselling and nutritional support for children under three
Children require solid foods that are calorie-dense, including fats, after six months of age (complementary feeding). Nutritious and carefully designed take-home rations (THR) based on locally procured food should be provided as “supplementary nutrition” for children in this age group. Currently THRs are in the form of just grain this is inadequate.
Also, THRs must be combined with nutrition counselling and nutrition and health education sessions for mothers and family members to ensure that children of this age group are given appropriate and adequate foods at home. Further, skilled counselling is also required to educate the family on the psycho-social and learning needs of the child.
4. Pre-school and hot, cooked meals for all children in the age group of 3 years 6 years
Pre-school education is very significant in helping children to prepare for formal schooling. Pre-school education assists children both to enter school and to remain in the system. The ICDS must provide a centre-based play-school facility at the anganwadi with the worked trained in conducting preschool activities.
Moribund ICDS80
For these children a culturally acceptable, varied, adequate, energy meal that has multiple nutrients including micronutrients like Vitamin A and Zinc must be provided at the anganwadi centre. A hot cooked meal provided at a centre also has many benefits as it:
l serves as an incentive for regular attendance,
l promotes social equity,
l provides income support to poor households,
l acts as a form of nutrition education,
l tackles hunger and can contributes all nutrients required,
5. Day Care Centres or Crèches
Women across the country work long hours at paid and unpaid work, often starting to work very soon after delivery. They need support to provide adequate care and attention to their children. They need safe places or crèches, close to their work sites, run by trained workers, where they can keep their infants, and where their older children will receive hot cooked meals and health care.
Crèches must be designed to meet the varying needs of children of different age groups. Infants 0-6 months need to be breastfeed on demand. Children 6 months - 3 years of age 5-6 times small but nutritious and energy dense meals a day. Children 3-6 years of age need 3-4 small but nutritious meals a day. All these children also require organized play and learning in areas that are safe, to help them develop adequate motor and learning skills appropriate to their age, acquire concepts, language, habits and develop relationships with peers and adults.
To begin with a model of anganwadi-cum-crèches can be introduced to provide this service in the village. This would be mean that these centres are open full-time, with adequate staff, training and infrastructure. Existing crèche schemes such as the Rajiv Gandhi Crèche Scheme and provision for crèches under the NREGA must also be expanded and strengthened.
6. Second Anganwadi Worker for ICDS Centres
Adequate care of children under three, which includes skilled counselling on breastfeeding, nutrition and learning needs, combined with effective preschool education for children aged 3-6 years cannot be achieved without the involvement of two Anganwadi workers (along with the Anganwadi helper). The availability of at least two anganwadi workers at each anganwadi centre would make it possible for one of them to concentrate on providing the home-based services, while the other can provide centre-based activities such as pre-school. The helper would have a role to play in bringing the children, cooking and serving and keeping the centre clean.
7. Convergence between Health and WCD Department at all levels including provisioning of basic Health Care Services including Nutritional Rehabilitation Centres for highly malnourished children
Regular interventions like health screening and referral, growth monitoring, immunisation and de-worming must be carried out by the ICDS and health department together.
Moribund ICDS81
There are several factors that affect the nutritional status of children, including food and health factors Tackling malnutrition effectively will require that the health department and the ICDS work together at all levels. The ASHA programme offers great opportunities for convergence provided:
l ANMs / AWWs and ASHA to be trained and mentored together on tackling malnutrition.
l Nutrition Rehabilitation Centres located at PHCs should be the focal point of dealing with severe malnutrition.
l Block and District level Health, RCH and WCD officials should routinely monitor malnutrition together.
8. Investing in the ICDS workforce through training and capacity building
The training programmes should recognise pre-school education and nutrition counselling as essential components. Within the overall framework, training curriculum, material and approaches should be developed in a decentralised manner, to be appropriate to the specific state/district level. Anganwadi Training Centres should be allocated for capacity building in a specific region at the District or Sub-District level. A system for continuous field level support should be developed (for instance, identifying a relatively accessible Anganwadi centre and developing it as a local resource centre, where the supervisor/ trainer can facilitate peer learning through monthly cluster-level meetings).
9. Building a comprehensive monitoring and evaluation system
A more robust, regular and independent monitoring and evaluation system, where workers are not forced to under-report malnutrition. As things stand, the most reliable source of information on child nutrition is the National Family Health Survey (NFHS). However, the NFHS surveys have been conducted at intervals of 6-7 years. Further, these surveys are too small to produce nutrition indicators at lower levels of aggregation than the State level (e.g. the District level). Ideally, NFHS-type surveys should be conducted every five years on a scale that would allow the estimation of District-level health and nutrition indicators, and every year on a smaller scale. At the very least, national NFHS-type surveys should be conducted at intervals no larger than three years. Expert scrutiny of this issue is urgently required.
A high-level overseeing mechanism should be created which will serve as a strategic oversight, technical support and ensure convergence and accountability in the range of interventions concerned with child nutrition.
10. Improving governance and involving communities
Decentralisation is the key to reducing corruption. A decentralized approach is required, fostering participatory planning, community ownership, responsiveness to local circumstances, and the involvement of Panchayati Raj Institutions (PRIs).Key decisions, including decisions on recruitment and transfers should be taken locally. Procurement of food should be done at the village level without private contractors, as the Supreme Court
Moribund ICDS82
has ordered. Medicine kits and Pre-School Kits should be procured locally. Monitoring and evaluation should also be carried out at the block and district level with the active involvement of PRIs.
B - Strategies for the treatment of SAM
An Open letter to Policy Makers
We would like to share with you our position and concerns in relation to the strategies for addressing the issue of Severe Acute Malnutrition (SAM). Millions of young children in Madhya Pradesh are facing the prospects of lifelong disadvantages or even death in some cases, due to severe acute malnutrition. We therefore understand the urgency of the situation and the need for the government to respond to this at the earliest.
We would like to begin with saying that we agree that there is a need for a High Energy Therapeutic Food (which can also be in the form of RUTF) for the treatment of Severely Malnourished Children and this should be provided in required quantities to all SAM children. At the same time, it must be understood that the high energy therapeutic food or RUTF is just one of the components of a treatment protocol for SAM, which includes among other things early identification, treatment of infections and so on. Further, we also feel that it is critical to place SAM in broader context of prevention and management of all forms of malnutrition among children under 6.
The following are some of our specific concerns and comments on the strategies to address severe acute malnutrition in the state:
1. Local Production and No to commercialization of RUTF:
While accepting the need for a therapeutic food for the treatment for SAM we feel that principles of diversity (respecting cultural acceptability among different communities) and decentralization must be adhered to, while designing the RUTF that is to be used as part of the treatment protocol. The group working of children's right to food is in favor of local and decentralized production of RUTF and is against the entry of any kind of commercial interests, including through indirect processes or sub-contracting, into the production and distribution of RUTF.
To begin with, we suggest that a unit for production of therapeutic food for the treatment of SAM should be set up under a public sector undertaking or institution like the SANCHI Cooperative Group in the state.
You may also be aware that National Institute of Nutrition (NIN) is the apex body to provide knowledge and guidance on this issue. We suggest that the services of NIN should be sought by the state government for help in finalizing recipes and production processes for RUTF.
A system of using milk based F75 / F100 while at the NRCs and decentralized ready mixes for community management can be developed. SAM children with complications need to be provided proper institution (Nutritional Rehabilitation Centers and Primary Health
Moribund ICDS83

Centers) based services, while the uncomplicated cases can be treated in the community with support from the ICDS.
2. Need for a comprehensive package:
As mentioned earlier we strongly believe that the use of RUTF in isolation is not enough to reach the goal of elimination of malnutrition or even SAM from Madhya Pradesh. Our experience of studying the impact of RUTF in Khandwa district showed that a strong system of follow-up and monitoring is absolutely essential. While we understand that the response in Khandwa was to an emergency situation and therefore some important aspects could have been neglected, as part of a long term strategy we need to establish clear protocols for the treatment of SAM, including the use of RUTF.
Further, while once a child enters the category of SAM he/she needs to undergo the treatment protocol; we must also understand that the very reason for the child becoming severely malnourished is an outcome of socio-economic imbalance and chronic hunger. Since we are not addressing this situation, after the treatment the child will go back to the same conditions of access to food and is likely to become malnourished again. The other children in the family are also vulnerable. The group therefore feels that, while working on the treatment protocols for SAM children, the affected families should be given protection through food and employment entitlement based schemes (like AAY, NREGS, Social Security Pension etc.). Our analysis shows that having a social security net is a fundamental requirement to address malnutrition.
Similarly, the treatment protocol for SAM must identify promotion of breastfeeding up to two years of age as one of the non-negotiable components. The linkages of malnutrition with low breastfeeding are quite visible. In Madhya Pradesh also, malnutrition rises once the cycle of breast feeding is broken. While support must be provided for exclusive breast feeding for the children under the age of 6 months, those in the age group between 6-36 months should be provided with locally made and culturally accepted nutrition in the form of take home rations. Children in the 3 to 6 years age group can be provided hot cooked meals in the anganwadi centre.
In our view malnutrition is a complex problem, and therefore demands complex solutions as well. The strategy for prevention and management of malnutrition must also address issues such as access to quality institutional services, capacities of personnel (like ANM, AWW, MPW, ASHA etc.), quality of services, accountability, community participation, nutrition counseling and so on. The clinical treatment and nutritional care for SAM children will be a critical component of this larger framework and cannot be addressed in isolation.
3. Convergence and Responsibilities:
A system needs to be put in place at 3 levels:
1) Community for early identification and referral to medical institution
2) Nutrition Rehabilitation Centres once children are identified and brought to the institution
3) ICDS or in the community again for follow up of the treatment protocol.
Moribund ICDS84

The systems of co-ordination between the network of NRCs and ICDS centers need to be operationalised. It must be ensured the victims themselves are not blamed for failure in treatment, with arguments mothers of or parents of the child don't want to get their child treated, They themselves go back to home, what government can do? Any treatment strategy must be sensitive to the the limitations of the deprived families.
The Women and Child Development and the Health Department must co-ordinate in the treatment of SAM children. The health department has the responsibility of not only treating children with SAM in the institutions but their community outreach workers such as ANMs and ASHAs must be involved in the counseling and other processes taking place in the community. On the other hand the capacities of the ICDS needs to be built so that they can identify SAM children, ensure timely referral, counsel the families and are able to ensure the rehabilitation of children in the community after the treatment phase.
4. RUTF vs. RUF:
We are also concerned about RUTF being converted into RUF. While making the guidelines and protocol, we hope the state government will also take necessary steps to prevent this possible conversion. The department should clearly state in its nutrition policy that the provision of supplementary nutrition in anganwadis will be in line with the orders of the Supreme Court i.e. providing hot cooked meals for children in the 3 to 6 years age group and locally produced take home rations for younger children. As directed by the Court SHGs, community groups, Mahila Mandals etc. may be involved in this process.
We would like to conclude by reiterating that we believe that severe acute malnutrition is a serious concern in our state and the government must urgently set up systems to address this problem. In doing so it must be kept in mind that any strategy for the treatment of SAM must be within the larger framework of prevention and management of malnutrition for all children and ensuring health, nutrition and education services for all children under six. Further, while there is indeed a need for a therapeutic food for the treatment of SAM, this is only one of the components of the treatment protocol. Attempts must be made to provide therapeutic food (could be in the form of RUTF) which is produced within the state at as decentralized a manner as possible, which is free from the interference of any commercial interests. For this we recommend involving co-operative groups that are already in existence in the state. We do hope that these concerns are kept in mind while finalizing any strategy for SAM in the state.
Moribund ICDS85
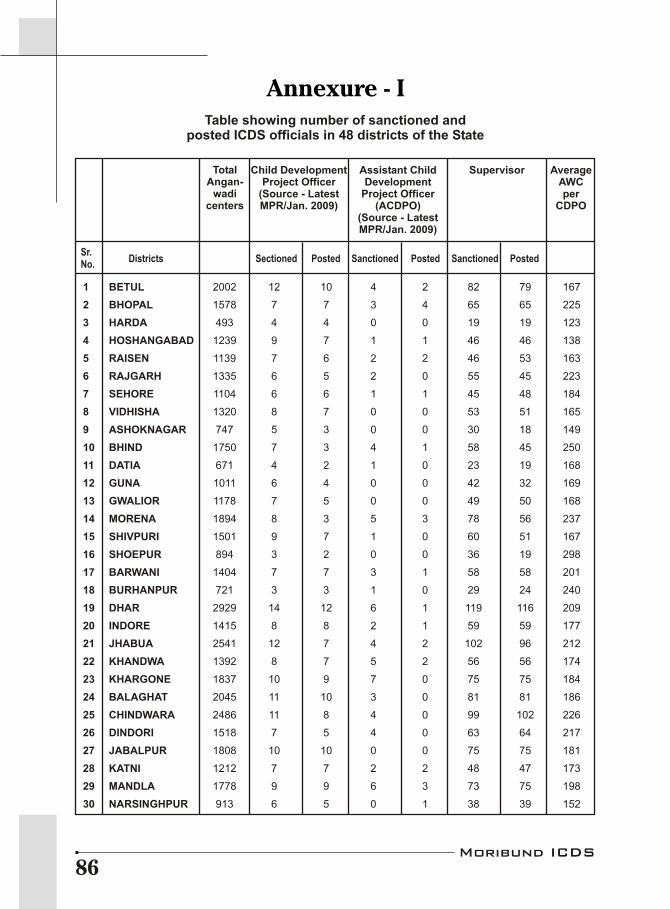
Annexure - I
1 BETUL 2002 12 10 4 2 82 79 167
2 BHOPAL 1578 7 7 3 4 65 65 225
3 HARDA 493 4 4 0 0 19 19 123
4 HOSHANGABAD 1239 9 7 1 1 46 46 138
5 RAISEN 1139 7 6 2 2 46 53 163
6 RAJGARH 1335 6 5 2 0 55 45 223
7 SEHORE 1104 6 6 1 1 45 48 184
8 VIDHISHA 1320 8 7 0 0 53 51 165
9 ASHOKNAGAR 747 5 3 0 0 30 18 149
10 BHIND 1750 7 3 4 1 58 45 250
11 DATIA 671 4 2 1 0 23 19 168
12 GUNA 1011 6 4 0 0 42 32 169
13 GWALIOR 1178 7 5 0 0 49 50 168
14 MORENA 1894 8 3 5 3 78 56 237
15 SHIVPURI 1501 9 7 1 0 60 51 167
16 SHOEPUR 894 3 2 0 0 36 19 298
17 BARWANI 1404 7 7 3 1 58 58 201
18 BURHANPUR 721 3 3 1 0 29 24 240
19 DHAR 2929 14 12 6 1 119 116 209
20 INDORE 1415 8 8 2 1 59 59 177
21 JHABUA 2541 12 7 4 2 102 96 212
22 KHANDWA 1392 8 7 5 2 56 56 174
23 KHARGONE 1837 10 9 7 0 75 75 184
24 BALAGHAT 2045 11 10 3 0 81 81 186
25 CHINDWARA 2486 11 8 4 0 99 102 226
26 DINDORI 1518 7 5 4 0 63 64 217
27 JABALPUR 1808 10 10 0 0 75 75 181
28 KATNI 1212 7 7 2 2 48 47 173
29 MANDLA 1778 9 9 6 3 73 75 198
30 NARSINGHPUR 913 6 5 0 1 38 39 152
Table showing number of sanctioned andposted ICDS officials in 48 districts of the State
TotalAngan-
wadicenters
Child DevelopmentProject Officer
(Source - LatestMPR/Jan. 2009)
Assistant ChildDevelopment
Project Officer(ACDPO)
(Source - LatestMPR/Jan. 2009)
Supervisor AverageAWCper
CDPO
Districts Sectioned Posted Sanctioned Posted Sanctioned PostedSr. No.
Moribund ICDS86

TotalAngan-
wadicenters
Child DevelopmentProject Officer
(Source - LatestMPR/2008)
Assistant ChildDevelopment
Project Officer(ACDPO)
(Source - LatestMPR/2008)
Supervisor AverageAWCper
CDPO
Districts Sectioned Posted Sanctioned Posted Sanctioned PostedSr. No.
31 SEONI 1718 9 9 7 6 70 72 191
32 ANOOPPUR 1007 4 4 7 1 47 47 252
33 REWA 2154 10 8 3 2 89 83 215
34 SATNA 1845 9 7 4 0 25 15 205
35 SHAHDOL 1192 6 5 4 2 48 48 199
36 SIDHI 2628 9 5 3 1 95 66 292
37 UMARIA 643 3 3 3 1 25 20 214
38 CHHATARPUR 1480 9 7 0 0 61 59 164
39 DAMOH 1057 8 7 2 1 43 46 132
40 PANNA 941 6 6 1 0 39 33 157
41 SAGAR 2007 13 7 0 0 84 84 154
42 TIKAMGARH 1218 7 3 1 2 50 42 174
43 DEWAS 1306 7 6 4 0 52 51 187
44 MANDSAUR 1125 6 4 2 0 42 24 188
45 NEEMUCH 715 4 1 0 0 29 16 179
46 RATLAM 1600 8 5 2 2 66 62 200
47 SHAJAPUR 1233 8 6 0 0 50 49 154
48 UJJAIN 1514 9 9 1 1 61 58 168
Total 69238 366 290 115 46 2738 2538 189
Moribund ICDS87

Prioritizing the nutritional needs of children (0 to 6 years) which comprise 16 percent population of the country, new norms have been released by Ministry of Women & Child Development in February 2009 to all the States/UTs laying down the new nutritional feeding norms for supplementary nutrition provided under ICDS.
The guidelines are trend setting but still there are some aspects which compel to think on the government's intention. On one hand the budget has been doubled and on the other hand the government has given a due recognition to the feeding habits of children under 2 years of age. The guidelines call for takeaway home rations (THR). It is clearly notified that the complementary food to children under three must be in a form that is palatable to the child and cannot be consumed by the entire family. The guide lines also emphasize the importance of hygiene, immunization and spreading the significant message of breastfeeding within one hour of birth.
The major thrusts have been given to following points in the revised guidelines
l Universalizing the ICDS scheme and priority must be given to the villages/habitations pre-dominantly inhabited by SC/ST/Minority community.
l Under the ICDS scheme, it must be ensured that the nutritional gap is effectively bridged and all children and women in the target group are brought under its coverage.
l Revising the existing cost of supplementary nutrition provided to children and women under ICDS scheme.
No doubt the revised guidelines are beneficial and are made keeping in focus the target groups (children and women) BUT at the same time there are some noteworthy loopholes in it which can not be passed up.
Financial Norms : The Government of India has revised the existing norms of Supplementary Nutrition Program which are as under
Annexure - IIRevised Nutritional and Feeding norms forSupplementary Nutrition in ICDS scheme
S. No. Category Pre-revised norms Revised norms w.e.f.(per beneficiary per day) 16/10/08
(per beneficiary per day)
1 Children (6-72 months) Rs. 2.00 Rs. 4.00
2 Severely underweight children Rs. 2.70 Rs. 6.00(6-72 months)
3 Pregnant women and Rs. 2.30 Rs. 5.00Lactating mothers
4 Weighted Average Rs. 2.06 Rs. 4.21
Moribund ICDS88
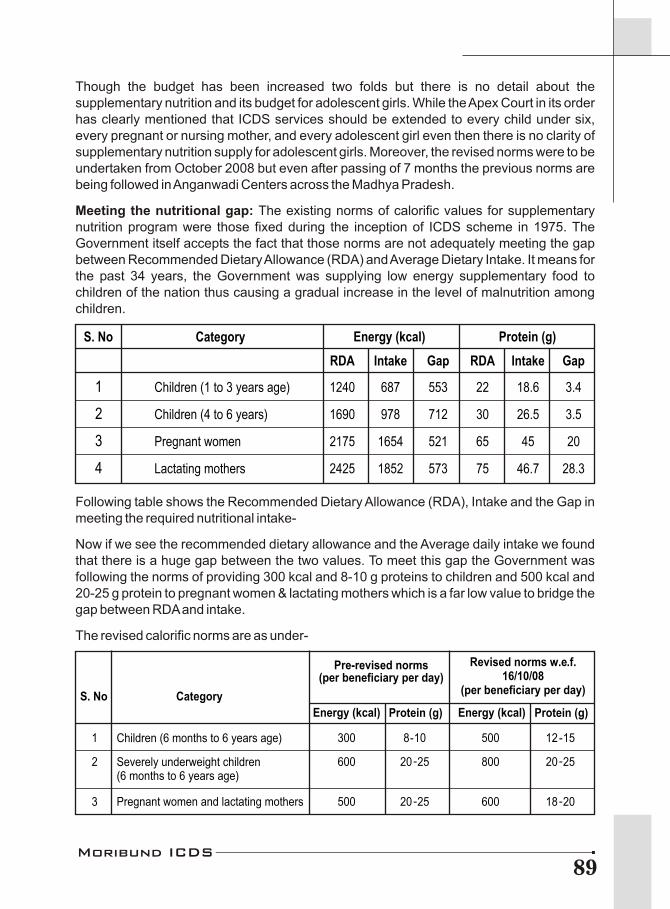
Though the budget has been increased two folds but there is no detail about the supplementary nutrition and its budget for adolescent girls. While the Apex Court in its order has clearly mentioned that ICDS services should be extended to every child under six, every pregnant or nursing mother, and every adolescent girl even then there is no clarity of supplementary nutrition supply for adolescent girls. Moreover, the revised norms were to be undertaken from October 2008 but even after passing of 7 months the previous norms are being followed in Anganwadi Centers across the Madhya Pradesh.
Meeting the nutritional gap: The existing norms of calorific values for supplementary nutrition program were those fixed during the inception of ICDS scheme in 1975. The Government itself accepts the fact that those norms are not adequately meeting the gap between Recommended Dietary Allowance (RDA) and Average Dietary Intake. It means for the past 34 years, the Government was supplying low energy supplementary food to children of the nation thus causing a gradual increase in the level of malnutrition among children.
Following table shows the Recommended Dietary Allowance (RDA), Intake and the Gap in meeting the required nutritional intake-
Now if we see the recommended dietary allowance and the Average daily intake we found that there is a huge gap between the two values. To meet this gap the Government was following the norms of providing 300 kcal and 8-10 g proteins to children and 500 kcal and 20-25 g protein to pregnant women & lactating mothers which is a far low value to bridge the gap between RDA and intake.
The revised calorific norms are as under-
S. No Category
RDA Intake Gap RDA Intake Gap
1 Children (1 to 3 years age) 1240 687 553 22 18.6 3.4
2 Children (4 to 6 years) 1690 978 712 30 26.5 3.5
3 Pregnant women 2175 1654 521 65 45 20
4 Lactating mothers 2425 1852 573 75 46.7 28.3
Protein (g)Energy (kcal)
Pre-revised norms (per beneficiary per day)
Revised norms w.e.f. 16/10/08
(per beneficiary per day)
S. No Category
Energy (kcal) Protein (g) Energy (kcal) Protein (g)
1 Children (6 months to 6 years age) 300
2
Severely underweight children(6 months to 6 years age)
600
3
Pregnant women and lactating mothers 500
8-10
20-25
20-25
500
800
600
12-15
20-25
18-20
Moribund ICDS89

Though the revised norms suggest that now onwards the calorific value of supplementary diet given to children and women under ICDS will be increased but from when these revised norms will be in action is not known!
Promoting Micronutrient fortified foods in ICDS scheme: The Central Government has recommended in the new guidelines that because the children of age group 6 months to 6 years are not capable of consuming a meal comprising 500 kcal energy and 12-15 g proteins therefore as an alternative the government has suggested that for children aged 6 months to 3 years Take Home Ration (THR) facility will be adopted and the parents will be given THR which could be in the form of Micronutrient Fortified Food or Energy-dense Food (which may be called Ready to Use Food, RUF). The parents will be advised to give this food in small frequent meals. Similarly, for children of age group 3 to 6 years it has been suggested that state/UTs governments may arrange to provide a morning snack in the form of milk/banana/egg/seasonal fruits/micronutrient Fortified Food etc.
Likewise, for severely malnourished children (of age groups 6 to 72 months) an additional 300 kcal energy and 8-10 g protein rich food (along with 500 kcal energy and 12-15 g protein rich food given at AWC) should be given in the form of Micronutrient Fortified Food and/or Energy-dense Food as THR.
We can see that the government is totally in favour of introducing Micronutrient Fortified Food or Energy-dense Food (which may be called Ready to Use Food) in ICDS system in one or the other way. This is clearly a hint that government has set a frame of mind for the commercial interest of private firms and sooner or later these private firms will be introduced in the food supply system of ICDS for supplying supplementary nutrition food. This will be a sheer violence of orders of Apex Court which has strictly denied the involvement of private firms in supplementary nutrition supply system for ICDS.
Let alone the children who could not consume the supplementary food at one sitting, the revised guidelines instruct to provide 600 kcal and 18-20 g protein rich food to pregnant and lactating mothers in the form of Micronutrient Fortified food and/or Energy-dense Food as THR. Are pregnant women and lactating mothers also not able to consume the prescribed amount of food in one sitting that government is recommending Energy-dense Food for them!
Such policies of government clearly shows that, even after very clear cut orders from the Supreme Court of India, there is a planned action to replace the traditional system of serving Hot-Cooked Supplementary Nutrition Food followed in ICDS networks with Ready to Use Foods (RUFs). Though it has been seen that for the treatment of severe malnutrition the Ready to Use Therapeutic Food (RUTF) has given some positive indications but it is also true that this RUTF is a medicated therapy and should be given under medical supervision with a definite protocol. Also this RUTF is not procured locally so its sustainability is again a question. Similarly, for the supply of Micronutrient Fortified Food or Energy-dense Food, we have to depend on private firms and thus its regular supply and sustainability will also be the things out of our control. Moreover, acceptability of these foods is yet to be proved.
Moribund ICDS90

Annexure - IIITables showing the ground realities of available facilities in the
studied 65 Anganwadi Centres of 10 districts in the State.
Table No. 1 - Infrastructure At Anganwadi centers
District Blocks No. of AWC Buildings
Yes No
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 3 7
Jhabua Petlavad 13 6 7
Tikamgarh Niwari 7 3 4
Panna Ajaygarh 5 1 4
Balaghat Laalbarra 5 3 2
Khandwa Khalwa 5 3 2
Hoshangabad Sohagpur 5 2 3
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 1 4
Bhopal Bhopal (Urban) 5 1 4
Total 65 24 41
Percentage 37 63
Moribund ICDS91
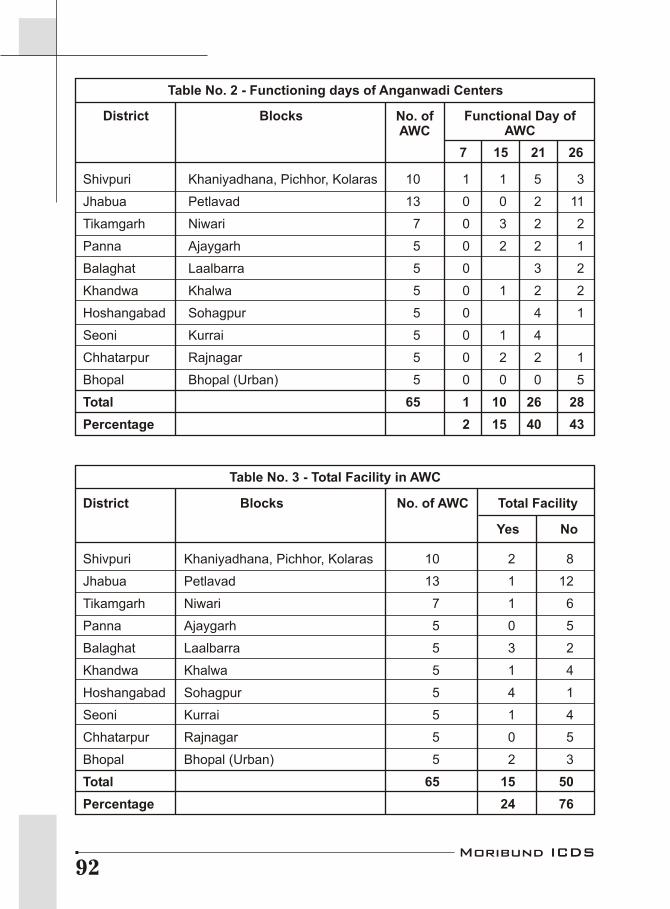
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 1 1 5 3
Jhabua 13 0 0 2 11
Tikamgarh Niwari 7 0 3 2 2
Panna Ajaygarh 5 0 2 2 1
Balaghat Laalbarra 5 0 3 2
Khandwa Khalwa 5 0 1 2 2
Hoshangabad Sohagpur 5 0 4 1
Seoni Kurrai 5 0 1 4
Chhatarpur Rajnagar 5 0 2 2 1
Bhopal Bhopal (Urban) 5 0 0 0 5
Total 65 1 10 26 28
Percentage 2 15 40 43
Petlavad
Table No. 3 - Total Facility in AWC
District Blocks No. of AWC Total Facility
Yes No
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 2 8
Jhabua 13 1 12
Tikamgarh Niwari 7 1 6
Panna Ajaygarh 5 0 5
Balaghat Laalbarra 5 3 2
Khandwa Khalwa 5 1 4
Hoshangabad Sohagpur 5 4 1
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 2 3
Total 65 15 50
Percentage 24 76
Table No. 2 - Functioning days of Anganwadi Centers
District Blocks
7 15 21 26
Functional Day ofAWC
No. ofAWC
Moribund ICDS92
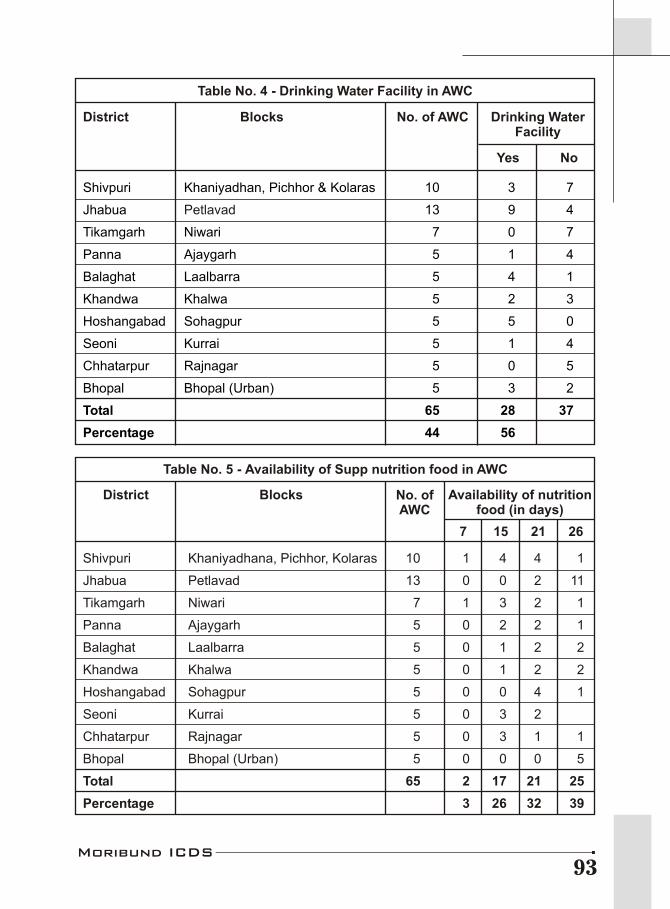
Table No. 4 -
District Blocks No. of AWC
Yes No
Petlavad
Drinking Water Facility in AWC
Drinking WaterFacility
Shivpuri Khaniyadhan, Pichhor & Kolaras 10 3 7
Jhabua 13 9 4
Tikamgarh Niwari 7 0 7
Panna Ajaygarh 5 1 4
Balaghat Laalbarra 5 4 1
Khandwa Khalwa 5 2 3
Hoshangabad Sohagpur 5 5 0
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 3 2
Total 65 28 37
Percentage 44 56
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 1 4 4 1
Jhabua 13 0 0 2 11
Tikamgarh Niwari 7 1 3 2 1
Panna Ajaygarh 5 0 2 2 1
Balaghat Laalbarra 5 0 1 2 2
Khandwa Khalwa 5 0 1 2 2
Hoshangabad Sohagpur 5 0 0 4 1
Seoni Kurrai 5 0 3 2
Chhatarpur Rajnagar 5 0 3 1 1
Bhopal Bhopal (Urban) 5 0 0 0 5
Total 65 2 17 21 25
Percentage 3 26 32 39
Petlavad
Table No. 5 - Availability of Supp nutrition food in AWC
District Blocks
7 15 21 26
Availability of nutritionfood (in days)
No. ofAWC
Moribund ICDS93
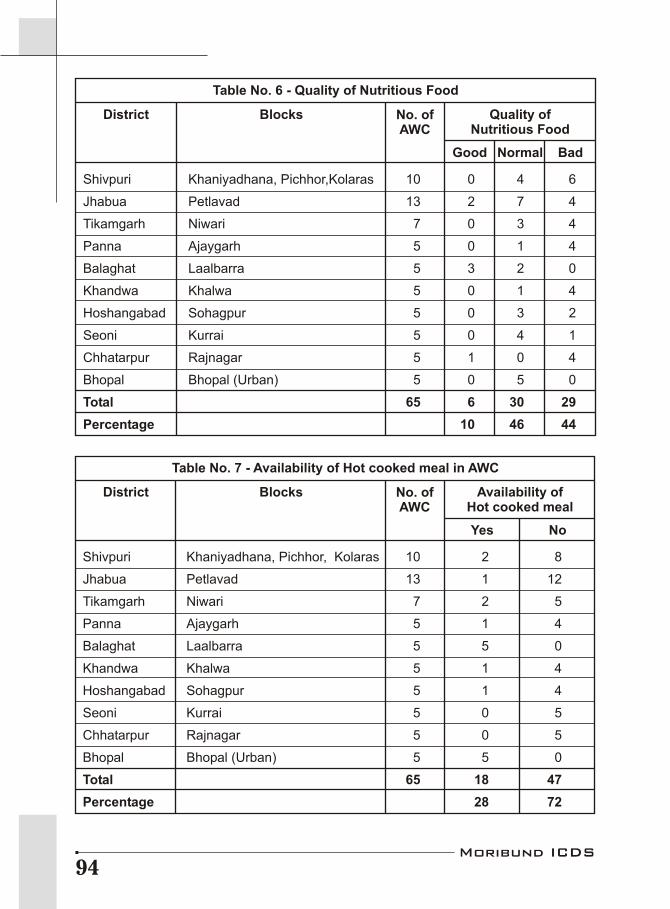
Shivpuri Khaniyadhana, Pichhor,Kolaras 10 0 4 6
Jhabua 13 2 7 4
Tikamgarh Niwari 7 0 3 4
Panna Ajaygarh 5 0 1 4
Balaghat Laalbarra 5 3 2 0
Khandwa Khalwa 5 0 1 4
Hoshangabad Sohagpur 5 0 3 2
Seoni Kurrai 5 0 4 1
Chhatarpur Rajnagar 5 1 0 4
Bhopal Bhopal (Urban) 5 0 5 0
Total 65 6 30 29
Percentage 10 46 44
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 2 8
Jhabua 13 1 12
Tikamgarh Niwari 7 2 5
Panna Ajaygarh 5 1 4
Balaghat Laalbarra 5 5 0
Khandwa Khalwa 5 1 4
Hoshangabad Sohagpur 5 1 4
Seoni Kurrai 5 0 5
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 5 0
Total 65 18 47
Percentage 28 72
Petlavad
Table No. 6 - Quality of Nutritious Food
Table No. 7 - Availability of Hot cooked meal in AWC
Good
Yes
Normal Bad
No
District
District
Blocks
Blocks
Quality ofNutritious Food
Availability ofHot cooked meal
No. ofAWC
No. ofAWC
Moribund ICDS94
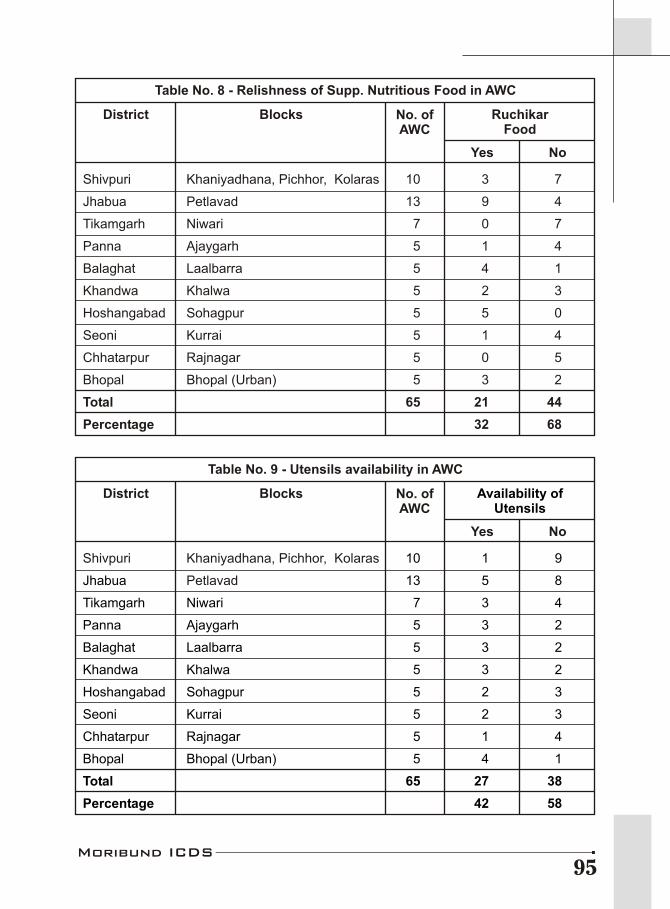
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 3 7
Jhabua 13 9 4
Tikamgarh Niwari 7 0 7
Panna Ajaygarh 5 1 4
Balaghat Laalbarra 5 4 1
Khandwa Khalwa 5 2 3
Hoshangabad Sohagpur 5 5 0
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 3 2
Total 65 21 44
Percentage 32 68
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 1 9
Jhabua 13 5 8
Tikamgarh Niwari 7 3 4
Panna Ajaygarh 5 3 2
Balaghat Laalbarra 5 3 2
Khandwa Khalwa 5 3 2
Hoshangabad Sohagpur 5 2 3
Seoni Kurrai 5 2 3
Chhatarpur Rajnagar 5 1 4
Bhopal Bhopal (Urban) 5 4 1
Total 65 27 38
Percentage 42 58
Petlavad
Table No. 8 - Relishness of Supp. Nutritious Food in AWC
Table No. 9 - Utensils availability in AWC
Yes
Yes
No
No
District
District
Blocks
Blocks
RuchikarFood
Availability ofUtensils
No. ofAWC
No. ofAWC
Moribund ICDS95
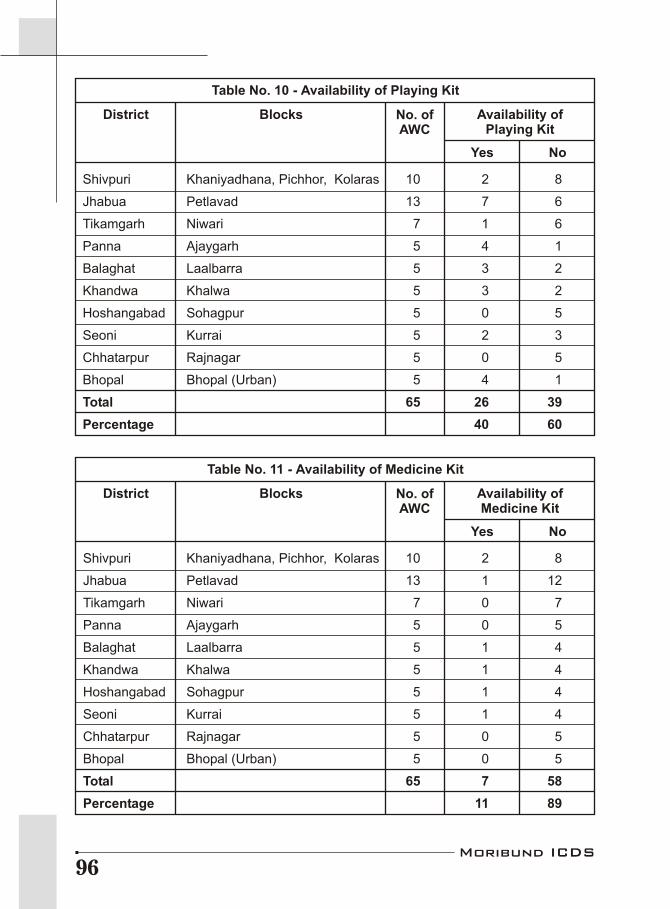
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 2 8
Jhabua 13 7 6
Tikamgarh Niwari 7 1 6
Panna Ajaygarh 5 4 1
Balaghat Laalbarra 5 3 2
Khandwa Khalwa 5 3 2
Hoshangabad Sohagpur 5 0 5
Seoni Kurrai 5 2 3
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 4 1
Total 65 26 39
Percentage 40 60
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 2 8
Jhabua 13 1 12
Tikamgarh Niwari 7 0 7
Panna Ajaygarh 5 0 5
Balaghat Laalbarra 5 1 4
Khandwa Khalwa 5 1 4
Hoshangabad Sohagpur 5 1 4
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 0 5
Bhopal Bhopal (Urban) 5 0 5
Total 65 7 58
Percentage 11 89
Petlavad
Table No. 10 - Availability of Playing Kit
Table No. 11 - Availability of Medicine Kit
Yes
Yes
No
No
District
District
Blocks
Blocks
Availability ofPlaying Kit
Availability ofMedicine Kit
No. ofAWC
No. ofAWC
Moribund ICDS96

Shivpuri Khaniyadhana, Pichhor, Kolaras 10 9 1
Jhabua 13 4 9
Tikamgarh Niwari 7 5 2
Panna Ajaygarh 5 5 0
Balaghat Laalbarra 5 5 0
Khandwa Khalwa 5 3 2
Hoshangabad Sohagpur 5 5 0
Seoni Kurrai 5 3 2
Chhatarpur Rajnagar 5 3 2
Bhopal Bhopal (Urban) 5 5 0
Total 65 47 18
Percentage 72 28
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 5 5
Jhabua 13 7 6
Tikamgarh Niwari 7 6 1
Panna Ajaygarh 5 4 1
Balaghat Laalbarra 5 5 0
Khandwa Khalwa 5 4 1
Hoshangabad Sohagpur 5 4 1
Seoni Kurrai 5 3 2
Chhatarpur Rajnagar 5 2 3
Bhopal Bhopal (Urban) 5 3 2
Total 65 43 22
Percentage 66 34
Petlavad
Table No. 12 - Availability of Salter machine
Table No. 13 - Availability of Adult Weighing Machine
Yes
Yes
No
No
District
District
Blocks
Blocks
Availability ofSalter machine
Availability of AdultWeighing Machine
No. ofAWC
No. ofAWC
Moribund ICDS97

Shivpuri Khaniyadhana, Pichhor, Kolaras 10 2 8
Jhabua 13 11 2
Tikamgarh Niwari 7 1 6
Panna Ajaygarh 5 0 5
Balaghat Laalbarra 5 4 1
Khandwa Khalwa 5 4 1
Hoshangabad Sohagpur 5 5 0
Seoni Kurrai 5 3 2
Chhatarpur Rajnagar 5 3 2
Bhopal Bhopal (Urban) 5 5 0
Total 65 38 27
Percentage 58 42
Petlavad
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 1 9
Jhabua 13 2 11
Tikamgarh Niwari 7 1 6
Panna Ajaygarh 5 1 4
Balaghat Laalbarra 5 3 2
Khandwa Khalwa 5 1 4
Hoshangabad Sohagpur 5 1 4
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 1 4
Bhopal Bhopal (Urban) 5 4 1
Total 65 16 49
Percentage 24 76
Petlavad
Table No. 14 - Availability of Growth Monitoring Register
Table No. 15 - Pre-school Education Facility
Yes
Yes
No
No
District
District
Blocks
Blocks
Availability of GrowthMonitoring Register
Pre-schoolEducation Facility
No. ofAWC
No. ofAWC
Moribund ICDS98
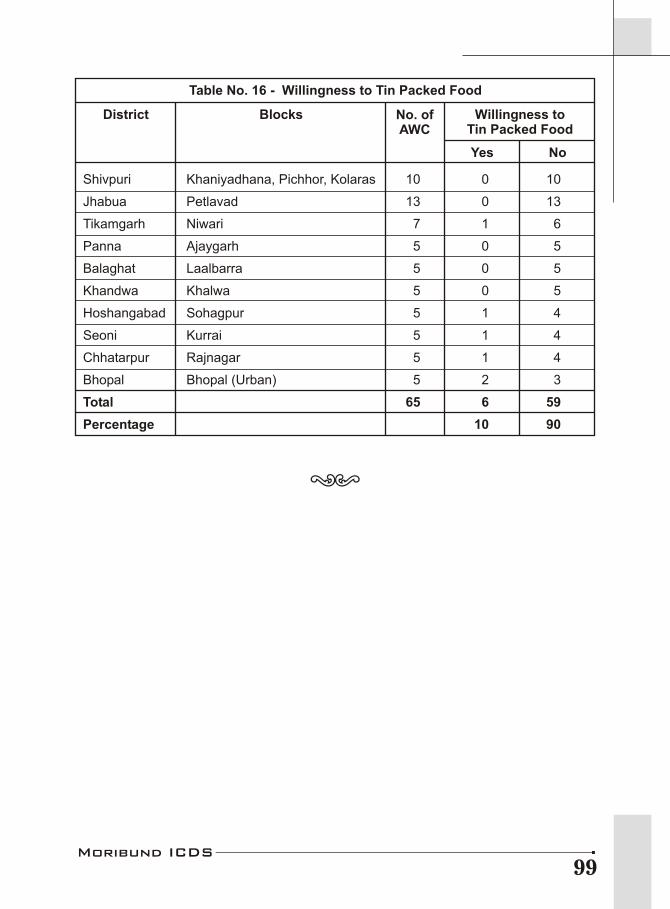
Shivpuri Khaniyadhana, Pichhor, Kolaras 10 0 10
Jhabua 13 0 13
Tikamgarh Niwari 7 1 6
Panna Ajaygarh 5 0 5
Balaghat Laalbarra 5 0 5
Khandwa Khalwa 5 0 5
Hoshangabad Sohagpur 5 1 4
Seoni Kurrai 5 1 4
Chhatarpur Rajnagar 5 1 4
Bhopal Bhopal (Urban) 5 2 3
Total 65 6 59
Percentage 10 90
Petlavad
Table No. 16 - Willingness to Tin Packed Food
Yes No
District Blocks Willingness toTin Packed Food
No. ofAWC
Moribund ICDS99
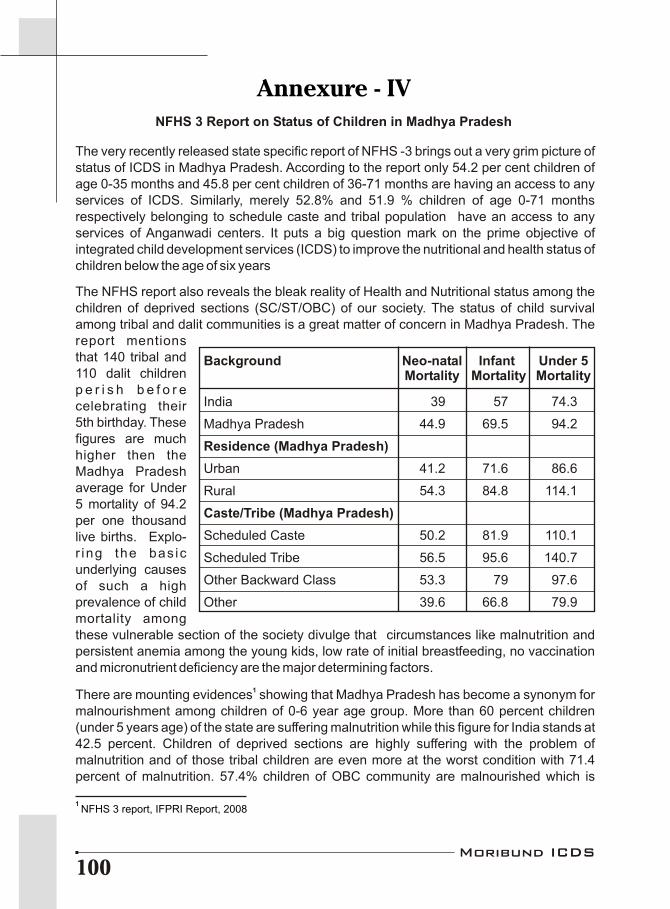
The very recently released state specific report of NFHS -3 brings out a very grim picture of status of ICDS in Madhya Pradesh. According to the report only 54.2 per cent children of age 0-35 months and 45.8 per cent children of 36-71 months are having an access to any services of ICDS. Similarly, merely 52.8% and 51.9 % children of age 0-71 months respectively belonging to schedule caste and tribal population have an access to any services of Anganwadi centers. It puts a big question mark on the prime objective of integrated child development services (ICDS) to improve the nutritional and health status of children below the age of six years
The NFHS report also reveals the bleak reality of Health and Nutritional status among the children of deprived sections (SC/ST/OBC) of our society. The status of child survival among tribal and dalit communities is a great matter of concern in Madhya Pradesh. The report mentions that 140 tribal and 110 dalit children p e r i s h b e f o r e celebrating their 5th birthday. These figures are much higher then the Madhya Pradesh average for Under 5 mortality of 94.2 per one thousand live births. Explo-r ing the bas ic underlying causes of such a high prevalence of child mortality among these vulnerable section of the society divulge that circumstances like malnutrition and persistent anemia among the young kids, low rate of initial breastfeeding, no vaccination and micronutrient deficiency are the major determining factors.
1There are mounting evidences showing that Madhya Pradesh has become a synonym for malnourishment among children of 0-6 year age group. More than 60 percent children (under 5 years age) of the state are suffering malnutrition while this figure for India stands at 42.5 percent. Children of deprived sections are highly suffering with the problem of malnutrition and of those tribal children are even more at the worst condition with 71.4 percent of malnutrition. 57.4% children of OBC community are malnourished which is
Background Neo-natal Infant Under 5Mortality Mortality Mortality
India 39 57 74.3
Madhya Pradesh 44.9 69.5 94.2
Residence (Madhya Pradesh)
Urban 41.2 71.6 86.6
Rural 54.3 84.8 114.1
Caste/Tribe (Madhya Pradesh)
Scheduled Caste 50.2 81.9 110.1
Scheduled Tribe 56.5 95.6 140.7
Other Backward Class 53.3 79 97.6
Other 39.6 66.8 79.9
Annexure - IVNFHS 3 Report on Status of Children in Madhya Pradesh
Moribund ICDS100
1 NFHS 3 report, IFPRI Report, 2008
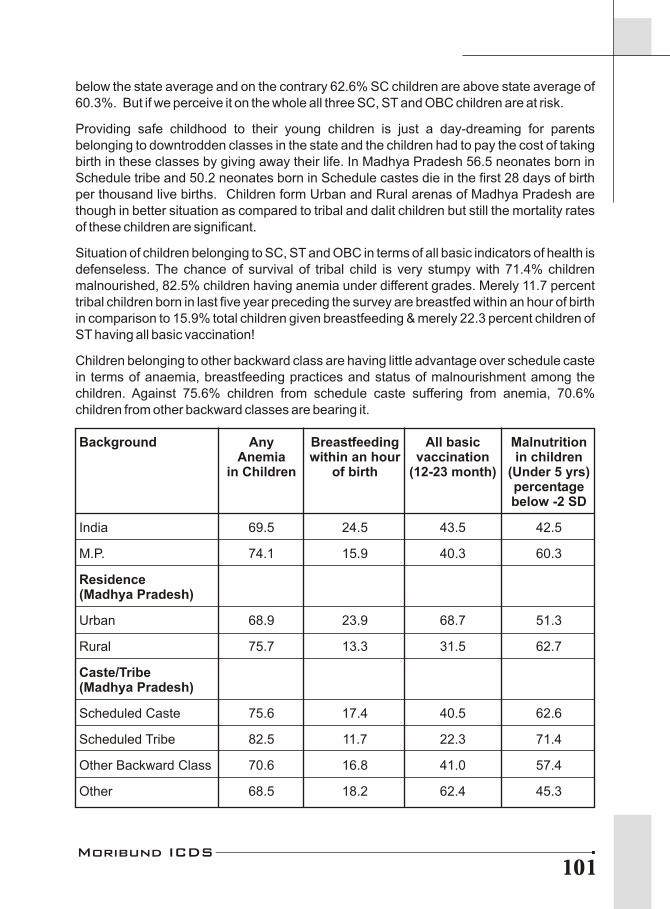
Moribund ICDS101
below the state average and on the contrary 62.6% SC children are above state average of 60.3%. But if we perceive it on the whole all three SC, ST and OBC children are at risk.
Providing safe childhood to their young children is just a day-dreaming for parents belonging to downtrodden classes in the state and the children had to pay the cost of taking birth in these classes by giving away their life. In Madhya Pradesh 56.5 neonates born in Schedule tribe and 50.2 neonates born in Schedule castes die in the first 28 days of birth per thousand live births. Children form Urban and Rural arenas of Madhya Pradesh are though in better situation as compared to tribal and dalit children but still the mortality rates of these children are significant.
Situation of children belonging to SC, ST and OBC in terms of all basic indicators of health is defenseless. The chance of survival of tribal child is very stumpy with 71.4% children malnourished, 82.5% children having anemia under different grades. Merely 11.7 percent tribal children born in last five year preceding the survey are breastfed within an hour of birth in comparison to 15.9% total children given breastfeeding & merely 22.3 percent children of ST having all basic vaccination!
Children belonging to other backward class are having little advantage over schedule caste in terms of anaemia, breastfeeding practices and status of malnourishment among the children. Against 75.6% children from schedule caste suffering from anemia, 70.6% children from other backward classes are bearing it.
Background Any Breastfeeding All basic MalnutritionAnemia within an hour vaccination in children
in Children of birth (12-23 month) (Under 5 yrs)percentage below -2 SD
India 69.5 24.5 43.5 42.5
M.P. 74.1 15.9 40.3 60.3
Residence(Madhya Pradesh)
Urban 68.9 23.9 68.7 51.3
Rural 75.7 13.3 31.5 62.7
Caste/Tribe(Madhya Pradesh)
Scheduled Caste 75.6 17.4 40.5 62.6
Scheduled Tribe 82.5 11.7 22.3 71.4
Other Backward Class 70.6 16.8 41.0 57.4
Other 68.5 18.2 62.4 45.3
The rural children are comparatively much more anemic (75.7 %) than the 69% urban anemic children. Schedule caste and schedule Tribe children are worst sufferers of aneamia in the state. More than eighty percent of tribal children undergoes through various stages of childhood aneamia. Similarly 4.6 % children from schedule caste are in the grip of death monster in the form of severe anaemia. These anemic children must be provided with additional nutritional foods to triumph over undernourishment but it is so unfortunate that merely 35.9% of children receive supplementary foods from Anganwadi centers in Madhya Pradesh.
Though micronutrients are required in very small amounts, the consequences of their absence are severe. Micronutrient deficiency in children also significantly contributes to childhood morbidity & mortality. According to WHO estimates approximately 50% of all anemia can be attributed to iron deficiency In Madhya Pradesh only 3.5 percentages of children of 6-59 months were given iron supplement in last seven days preceding the survey, which further reduced incase of children belonging to low wealth index to 2.3% & 1.8% for Muslim community children. Vitamin A deficiency (VAD) causes slow growth and development in children in addition to the manifestations of its deficiency in the eye. And NFHS-3 results shows that merely 14.1% children had received Vitamin A supplement in last six month preceding the survey and just 11.4% marginalized tribal children received the same in a given period.
In spite of such sky-scraping infant & child mortality no special efforts has been made for providing the better survival conditions to the children of State. The children from downtrodden classes of our society are the utter sufferer of the negligence of State towards health and nutrition policies.
Moribund ICDS102
Moribund ICDS103
AbbreviationAAY Antyoday Anna Yojana
ACDPO Additional Children Development Project Officer
ASHA Accredited Social Health Activist
ANM Auxiliary Nurse Midwife
AWC Anganwadi Centre
AWH Anganwadi Helper
AWW Anganwadi Worker
BIMARU Bihar, Madhya Pradesh, Rajasthan and Uttar Pradesh
BPL Below Poverty Line
CAG Comptroller and Auditor General
CC Cement Concrete
CDC Community Development Centre
CDPO Child Development Project Officer
CEFS Centre for Environment and Food Security
CHC Community Health Centre
CSOs Civil Society Organizations
DWCD Department of Women and Child Development
FAO Food and Agriculture Organization
GAIN Global Alliance for Improved Nutrition
GHI Global Hunger Index
GoI Government of India
GM Genetically Modified
HACCP Hazard Analysis and Critical Control Point
ICDS Integrated Child Development Services
ICSSR Indian Council of Social Science Research
IFPRI International Food Policy Research Institute
IMR Infant Mortality Rate
INHP Integrated Nutrition and Health Project
ISHI India State Hunger Index
ISO International Organization for Standardization
JCE Joint Commission of Enquiry
LHV Lady Health Worker
MDG Millennium Development Goals
MDM Mid Day Meal
MLA Member of Legislative Assembly
MMR Maternal Mortality Rate
MP Madhya Pradesh
MPCE Monthly Per Capita Expenditure
MPJSA Madhya Pradesh Jan Swasthya Abhiyan
MPR Monthly Progress Report
NFHS National Family Health Survey
NIWCYD National Institute of Women Child and Youth Development
NOAPS National Old Age Pension Scheme
MPW Multi Purpose Worker
NGO Non Governmental Organization
NRCs Nutritional Rehabilitation Centers
NREGS National Rural Employment Guarantee Scheme
NSSO National Sample Survey organization
PDS Public Distribution system
PHC Primary Health Centre
PMGY Pradhan Mantri Gramoday Yojana
PRHW Peoples' Rural Health Watch
PRIs Panchayat Raj Institutions
PTG Primitive Tribal Group
PUCL People's Union for Civil Liberty
RCH Reproductive Child Health
RUEF Ready to Use Energy Food
RUTF Ready to Use Therapeutic Food
SC Scheduled Caste
SCP Special Component Plan
SD Level Standard Deviation (for measuring malnutrition level)
SHC Sub Health Centre
SHG Self Help Group
SNP Supplementary Nutrition Programme
SRS Sample Registration Survey
ST Scheduled Tribe
TPDS Targeted Public Distribution System
TSP Tribal Sub Plan
UNICEF United Nations Children's Fund
UP Uttar Pradesh
USRN University School Resource Network of Jawaharlal Nehru University
UT Union Territories
WFP World Food Programme
WHO World Health Organization
WTO World Trade organization
Moribund ICDS104
ISBN - 978-81-908302-1-8
They are small but much more then a unit of Kilogram,
Millimeter, a tiny part of any group,
Beneficiary of a government scheme,
They are more then a man or woman!
You see them on streets
doing business for survival!
They bid every morning for today
at the cost of tomorrow!
You see them searching an opportunity
in bundle of garbage,
Which gives them a hope for food!
They have been restricted to keep
dreams, in their close eyes!
They should have an equal independent identity
but we have made them lost!
They can not be common,
They are more then anything now!
They should be treated as special in totality!
They should not survive by chance, but rightfully!
Don't you know them!
They are small but much more then a unit of Kilogram,
Millimeter, a tiny part of any group,
Beneficiary of a government scheme,
They are more then a man or woman!
You see them on streets
doing business for survival!
They bid every morning for today
at the cost of tomorrow!
You see them searching an opportunity
in bundle of garbage,
Which gives them a hope for food!
They have been restricted to keep
dreams, in their close eyes!
They should have an equal independent identity
but we have made them lost!
They can not be common,
They are more then anything now!
They should be treated as special in totality!
They should not survive by chance, but rightfully!
Don't you know them!
Neglect of them is a crime!!!Neglect of them is a crime!!!
They are more then us
Right to Food Campaign Madhya Pradesh Support GroupSanket - Centre for Budget Studies
&Vikas Samvad





























