Embed Size (px)
Citation preview

17
A Study of Variations in the Position of Vermiform Appendix1 2
Geethanjali HT , Lakshmi Prabha Subhash1 2
Assistant Professor , Professor & HOD Dept. of Anatomy, SSMC, Tumkur, ,
ABSTRACT
Acute appendicitis is one of the most common causes of 'Acute abdomen' needing emergency surgery. A variation in the position of the appendix, along with the degree of inflammation makes the clinical presentation of appendicitis inconsistent and variable. This cross sectional study was done in 52 cadavers used for routine dissection for undergraduates. Variations in position, length of appendix, and length of mesoappendix were determined. Pelvic position was most commonly seen in 36.54%,followed by Retrocaecal 32.69%, Post-ileal 11.53%, Pre-ileal 9.62%, Subcaecal 5.77%, Rt Paracolic 1.92% and Retrocolic1.92%. The average length of appendix was 6.47cms in males and 5.34cms in females. Mesoappendix reached the tip in 69.23% of cases. Results of this study indicates a very large variability of anatomy of vermiform appendix, which together with other factors( age, sex, degree of inflammation etc.) form a complete spectrum of clinical presentation of acute appendicitis.
Key words; Vermiform appendix; mesoappendix ; position; length.
INTRODUCTION
Vermiform appendix, considered a
vestigial organ is present only in humans, some anthropoid apes and a wombat (a nocturnal burrowing Australian marsupial). Sub-Primate forms exhibit a contracted caput caeci, associated with the sub mucosal lymphoid follicles of varying size, termed an appendix for descriptive
1purposes.
The Appendix is a narrow worm like structure present in the right iliac fossa, arising from the posteromedial wall of the caecum about 2 cms below the ileo-caecal junction and has no constant anatomical position. The length of appendix varies from 2 to 20 cms with an average
2of 9 cms. Microscopically, the vermiform appendix is a muscular tube containing a large
3amount of lymphoid tissue . The appendix is suspended by a peritoneal fold called mesoappendix covering its variable length and carrying the blood supply to the organ, by
appendicular artery, a branch derived from 2
ileocolic artery. Failure of the mesoappendix to reach the tip reduces the vascularization to the tip of the organ making it more liable to become
4 gangrenous .
The attachment of the base of appendix remains fairly constant, but the tip can be found anywhere in Retrocaecal, Pelvic, Subcaecal, Para
3caecal, Post ileal and Preilealpositions (Fig1). Appendicitis in different positions may mimic other diseases in retrocolic – colitis, Post ileal-ureteric colic, Pelvic inflammatory disease, torsion of ovarian cyst & Ruptured tubal
8gestation, Sub hepatic- hepatitis, biliary colic .
The only invariable feature is its origin from the caecum at the site of coalescence of all three
2 taenia coli. Though considered by most to be a vestigial organ, its importance in surgery is mainly due to its propensity for inflammation that results in the clinical syndrome known as acute appendicitis, and is the most common cause of
1“acute abdomen” in young adolescents.
A variation in the position of the appendix, along with the degree of inflammation makes the clinical presentation of appendicitis notoriously inconsistent. Misdiagnosis in different age groups
5 is from 10 to 33%. Despite extraordinary advances in modern radiographic imaging and diagnostic laboratory investigations, the diagnosis of appendicitis remain essentially clinical requiring a mixture of observations, clinical acumen and surgical sense added with a
1thorough knowledge of anatomical variations.
The aim of this study was to determine the frequency of the various positions of the appendix, the average length, extent of mesoappendix and to correlate the same with the available literature.
MATERIALS AND METHODS
This study was done in 52 cadavers in the age group of 55 to 70 years used for routine dissection for undergraduate students.After noting down its position, the length of appendix and mesoappendix were measured using vernier
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)

Fig 1: Showing different positions of appendix
18
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)
A Study of Variations in the Position of Vermiform Appendix
Fig 2: Schematic diagram of development of appendix

19
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)
A Study of Variations in the Position of Vermiform Appendix
Table 1: Positions of Appendix
Sex Pelvic Retro caecal
Post ileal
Pre ileal
Sub caecal
Rt.Para colic
Retro colic
Total
M ale 09 (17.30%)
09 (17.30%)
03(5.77%) 03 (5.77%)
02 (3.85% )
01 (1.92%)
01 (1.92%)
28
Female 10 (19.23%)
08 (15.38%)
03 (5.77%)
02 (3.85%)
01 (1.92% )
- - 24
Tota l
19 (36.54%)
17 (32.69%)
06 (11.53%)
05 (9.62%)
03 (5.77% )
01 (1.92%)
01 (1.92%)
52
Fig 3: Incidence of various positions of Appendix in our study
Table2: Average length of differently located appendices
Position Avg length male (cm s)
Avg length fem ale (cm s)
Pelvic 6.4 6.3
Retrocaecal 4.8 4.2
Post ileal 5.8 6.0
Pre ilea l 4.8 4.7
Subcaecal 5.4 5.5
Retrocolic 10.3 -
Average length of Appendix 6.47 5.34
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)20
A Study of Variations in the Position of Vermiform Appendix
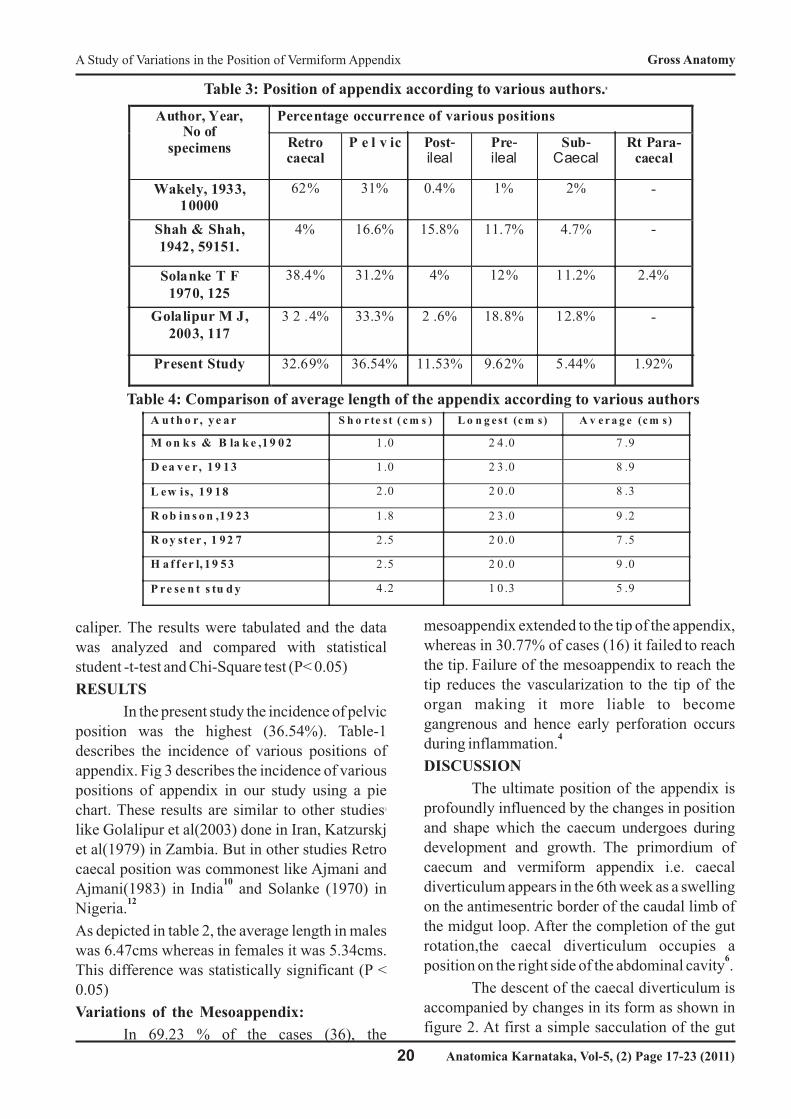
8Table 3: Position of appendix according to various authors.
Table 4: Comparison of average length of the appendix according to various authors
Author, Year, No of
specimens
Percentage occurrence of various positions
Retro caecal
P e l v ic Post-ileal
Pre- ileal
Sub-Caecal
Rt Para-caecal
Wakely, 1933, 10000
62% 31% 0.4% 1% 2% -
Shah & Shah, 1942, 59151.
4% 16.6% 15.8% 11.7% 4.7% -
Solanke T F 1970, 125
38.4% 31.2% 4% 12% 11.2% 2.4%
Golalipur M J, 2003, 117
3 2 .4% 33.3% 2 .6% 18.8% 12.8% -
Present Study 32.69% 36.54% 11.53% 9.62% 5.44% 1.92%
A u t h o r, y e a r S h o r te st ( c m s ) L o n g e st (c m s) A v e r a g e (c m s)
M o n k s & B la k e ,1 9 0 2 1 .0 2 4 .0 7 .9
D ea v e r, 1 9 1 3 1 .0 2 3 .0 8 .9
L ew is, 1 9 1 8 2 .0 2 0 .0 8 .3
R o b in s o n ,1 9 2 3 1 .8 2 3 .0 9 .2
R o y st er , 1 9 2 7 2 .5 2 0 .0 7 .5
H a f f er l, 1 9 5 3 2 .5 2 0 .0 9 .0
P re se n t s tu d y 4 .2 1 0 .3 5 .9
caliper. The results were tabulated and the data was analyzed and compared with statistical student -t-test and Chi-Square test (P< 0.05)
RESULTS
In the present study the incidence of pelvic position was the highest (36.54%). Table-1 describes the incidence of various positions of
appendix. Fig 3 describes the incidence of variouspositions of appendix in our study using a pie
3chart. These results are similar to other studies like Golalipur et al(2003) done in Iran, Katzurskj et al(1979) in Zambia. But in other studies Retro caecal position was commonest like Ajmani and
10Ajmani(1983) in India and Solanke (1970) in
12Nigeria.
As depicted in table 2, the average length in males was 6.47cms whereas in females it was 5.34cms. This difference was statistically significant (P < 0.05)
Variations of the Mesoappendix:
In 69.23 % of the cases (36), the
mesoappendix extended to the tip of the appendix,
whereas in 30.77% of cases (16) it failed to reach the tip. Failure of the mesoappendix to reach the
tip reduces the vascularization to the tip of the organ making it more liable to become gangrenous and hence early perforation occurs
4during inflammation.
DISCUSSION
The ultimate position of the appendix is profoundly influenced by the changes in position and shape which the caecum undergoes during
development and growth. The primordium of caecum and vermiform appendix i.e. caecal diverticulum appears in the 6th week as a swelling on the antimesentric border of the caudal limb of the midgut loop. After the completion of the gut rotation,the caecal diverticulum occupies a
6position on the right side of the abdominal cavity .
The descent of the caecal diverticulum is accompanied by changes in its form as shown in figure 2. At first a simple sacculation of the gut
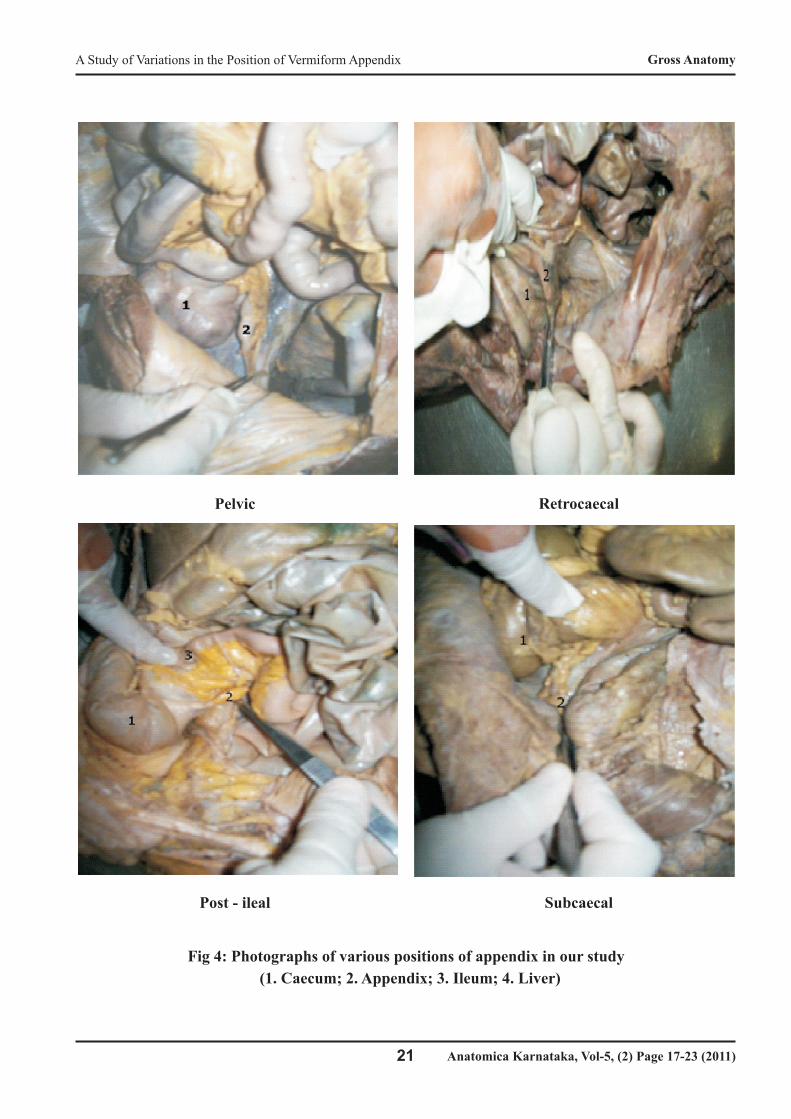
Post - ileal Subcaecal
Pelvic Retrocaecal
21
Fig 4: Photographs of various positions of appendix in our study
(1. Caecum; 2. Appendix; 3. Ileum; 4. Liver)
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)
A Study of Variations in the Position of Vermiform Appendix

22
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)
A Study of Variations in the Position of Vermiform Appendix
Retrocolic Right Paracolic
wall(figII-1), the caecal diverticulum elongates
and its proximal end grows more rapidly than its
distal, assuming a conical shape(figII-2), the
aecum and the appendix not being definitely
demarcated one from the other. Later, by the more
rapid enlargement of the proximal and the relative
constriction of the distal end, the appendix 7becomes differentiated from the caecum. With the
appearance of the taeniae, the caecum, becomes
sacculated. At first symmetrical, the right caecal
sacculation enlarges, while the left one
diminishes(figII-3). At the same time the anterior
wall which is subject to less resistance, grows
more rapidly than the posterior. This method of asymmetrical growth of the caecum is As shown
in Table 4 the present study reveals an average of
5.9cms in length. This can be probably attributed
to the shorterheight of the Asians, compared to the
other races where the other studies chad been 14
done. Among the specimens studied, it appears
that the males have a longer vermiform appendix
than the females. The anomalies besides the
position like agenesis of appendix and duplication
of appendix were not found in the present study.
The position of the appendix posterior to
the caecum is due to the disposition of its
bloodvessels within mesoappendix from the
dorsal aspect. The artery to the appendix is
derived either from ileo-caecal artery or from it
sposterior caecal branch and occupies a posterior
position.
In the case of such a mobile part of the gut as the
appendix, and taking into account the rapid and
extensive changes which the neighbouring parts
undergo, together with the changes in position
which the appendix itself undergoes as it follows
the caecum, it is obvious that it must be subject to
more or less accidental circumstances which will
modify its ultimate position and account for the
many and various positions in which it may be 5
found.
Conclusion
The present study determined the most common position, length and mesentery of the appendix in this area. Therefore, it can help the surgeons to make optimal diagnosis and treatment of appendicitis.
REFERENCES1) Bhasin S K, Khan A B, Vijay Sharma S,Saraf R; Vermiform Appendix and Acute Appendicitis, JK Science J, 2007; 9(4): 167-170.2) Snell R S. Clinical Anatomy. 7th edn.Baltimore: Lippincot William and Wilkins; 2004. pp215-217.3) Golalipur M J, Arya B, Azarhoosh R, JahanshahiM; Anatomical variations of

vermiform appendix in South East Caspian sea [Go r g o a n - I r a n ] , J .An a t S o c I n d i a ,2003; 52(2): 141- 143.4) Rahman MM, Khalil M, Sultana SZ, MannanS,Nessa A, Ahamed MS; Extent of mesoappendix inBangladeshi people J Bangladesh Soc Physiol,2009; 4(1): 20-23.5) Karpelowsky J S, Bickler S, Rode H; Appendicitis – pitfalls and medicolegal implications, South Afr Med J, 2006; 96(9): 866-872.6) Moore KL and Persaud T V N; Before we are born- Essentials of embryology and birth defects.5 t h e d n . W. B . S a u n d e r s c o m p a n y . Philadelphia1998. 273-280.7) Wakely CPS; The position of the vermiform appendix as described by analysis of 10.000 cases, Journal of Anatomy, 1933; 67: 277-283.8) Dr. Thyagaraj J, A Study of Anatomicalposition in normal population and in inflamed cases. [Thesis]. Bangalore Medical College; RGUHS, 2005.9) Shah MA, Shah M; The position of vermiform appendix, Ind Med Gaz, 1945; 8: 494-495.
10) Ajmani MLAjmani K; The position, length and arterial supply of vermiform appendix, Anatomischeranzeiger, 1983;153(4):369-374.
11) Sabiston DC, Townsend, Courtney M;Sabiston’s textbook of surgery, the biological basis of modern surgical practice. in: Appendix. 16th edn. Vol 2. W.B. Saunders& Co. Philadelphia.2001, pp 918.
12) Solanke TF; The position, length and content of the vermiform appendix in Nigerians, British Journal of Surgery, 1970.57:100-102.
13) Denjalic A, Delic J, Delic-Custendil S, Muminagic S. Variations in position and place of formation of appendix vermiformis found in the course of open appendicectomy. Med Arh. 2009;63(2):100-101
14) Chaisiwamongkol K,Chantaupalee T, Techataweewan N, Toomsan Y, AranateerakulT, Teepsawang S, Iamsaard S, Srikulwong:Position Variation of Vermiform Appendix inNortheast Thai Cadavers. Srinagar ind MedJ,
2010;25(3):250-255.
Address for Communication
Geethanjali HT,Assistant Professor,Dept. of Anatomy, SSMC, Tumkur,Ph 09964468415.
23
Gross Anatomy
Anatomica Karnataka, Vol-5, (2) Page 17-23 (2011)
A Study of Variations in the Position of Vermiform Appendix




![VARIATIONS GOLDBERG [ARIA et 30 variations] · Title: VARIATIONS GOLDBERG [ARIA et 30 variations] Author: Bach, Johann Sebastian - Arranger: Montreuille, Pierre - Publisher: Montreuille,](https://img.dokumen.tips/doc/110x75/610885d0028fe95f64358299/variations-goldberg-aria-et-30-variations-title-variations-goldberg-aria-et.jpg)