Embed Size (px)
Citation preview

A STUDY OF EXPANDED INFECTIOUS FEVER - 100 CASES IN
A TERTIARY CARE HOSPITAL
Dissertation Submitted to
THE TAMILNADU Dr.M.G.R. MEDICAL UNIVERSITY
CHENNAI- 600 032
With Partial fulfillment of the requirement
for the award of degree of
M.D. DEGREE IN GENERAL MEDICINE
BRANCH – 1
Register Number : 201711210
THANJAVUR MEDICAL COLLEGE AND HOSPITAL
THANJAVUR
MAY 2020

CERTIFICATE FROM THE INSTITUTION
This is to certify that this dissertation entitled “A STUDY OF EXPANDED
INFECTIOUS FEVER - 100 CASES IN A TERTIARY CARE
HOSPITAL” submitted by Dr. RENGABASHYAM P appearing for M.D. Branch
I General Medicine Degree examination in May 2020 is a bonafide record of work
done by him under my direct guidance and supervision in partial fulfillment of
regulations of the Tamil Nadu Dr. M.G.R. Medical University, Chennai. I forward this
to the Tamil Nadu Dr.M.G.R. Medical University, Chennai, Tamil Nadu, India.
Prof. Dr. KUMUDHA LINGARAJ MD DA.,
The Honourable Dean
Thanjavur Medical College & Hospital
Thanjavur.
CERTIFICATE FROM THE HOD
This is to certify that this dissertation entitled “A STUDY OF EXPANDED
INFECTIOUS FEVER - 100 CASES IN A TERTIARY CARE
HOSPITAL” submitted by Dr.RENGABASHYAM P appearing for M.D. Branch
I General Medicine Degree examination in May 2020 is a bonafide record of work
done by him under my direct guidance and supervision in partial fulfillment of
regulations of the Tamil Nadu Dr. M.G.R. Medical University, Chennai. I forward this
to the Tamil Nadu Dr.M.G.R. Medical University, Chennai, Tamil Nadu, India.
Prof. Dr. K.NAMASIVAYAM MD .,
HOD and Professor of Medicine
Department of Internal Medicine
Thanjavur Medical College & Hospital
Thanjavur.
CERTIFICATE FROM THE GUIDE
This is to certify that this dissertation entitled “A STUDY OF EXPANDED
INFECTIOUS FEVER - 100 CASES IN A TERTIARY CARE
HOSPITAL” submitted by Dr.RENGABASHYAM P appearing for M.D. Branch
I General Medicine Degree examination in May 2020 is a bonafide record of work
done by him under my direct guidance and supervision in partial fulfillment of
regulations of the Tamil Nadu Dr. M.G.R. Medical University, Chennai. I forward this
to the Tamil Nadu Dr.M.G.R. Medical University, Chennai, Tamil Nadu, India.
Prof. Dr. G. BHASKAR MD .,
Associate Professor
Department of Internal Medicine
Thanjavur Medical College & Hospital
Thanjavur.
CERTIFICATE II
This is to certify that this dissertation work titled “A STUDY OF
EXPANDED INFECTIOUS FEVER - 100 CASES IN A TERTIARY
CARE HOSPITAL” Of the candidate Dr.RENGABASHYAM P with
registration number 201711210 for the award of M.D. in the branch of
GENERAL MEDICINE. I personally verified the urkund.com for the purpose
of plagiarism check. I found the uploaded thesis file contains from the
introduction to conclusion pages and result shows 10 percentage of plagiarism
in the dissertation.
Guide and Supervisor sign with Seal
ACKNOWLEDGEMENT
I would like to thank our respected Dean Prof.Dr.KUMUDHA
LINGARAJ MD DA., Thanjavur Medical college for permitting me to
utilize the facilities of Thanjavur Medical college and Hospital for this
dissertation.
I wish to express my respect and sincere gratitude to my
beloved teacher, Unit chief Prof. Dr.G.BHASKAR.M.D,Associate
Professor, Department of General Medicine for his valuable guidance,
support and encouragement during the study and also throughout
my course period.
My heartful thanks to unit Asst. Professors, Dr.S. HEMA
AKILANDESWARI M.D., Dr.S.VENNILA M.D., and Dr.N. RAMESH M.D,
for their valuable suggestions and support throughout the course of
the study.
I would like to express my whole hearted thanks to my
beloved father Mr.PIRAHALATHAN K and mother Mrs.MALARKODI P
for their constant support throughout my study and course period.
I extend my thanks to all my friends, batch mates, my
juniors and senior colleagues who supported me throughout my study
and course period.
I thank all the patients, who form the most vital part of my
work, for their extreme patience and co-operation, without whom this
project would have been a distant dream and I pray God for their
speedy recovery.
This acknowledgement is incomplete if I fail in my duty to
thank all the persons who have whole heartedly participated in the
study and have made the study complete
DECLARATION
I solemnly declare that the dissertation titled “A STUDY OF EXPANDED
INFECTIOUS FEVER - 100 CASES IN A TERTIARY CARE
HOSPITAL” is done by me at Coronary care unit, Thanjavur Medical College &
Hospital, Thanjavur during 2018-2019 under the guidance and supervision of
Prof.Dr.G.BHASKAR, MD
The dissertation is submitted to The Tamilnadu Dr. M.G.R. Medical University
towards the partial fulfillment of requirements for the award of M.D. Degree
(Branch I) in General Medicine.
Place; Thanjavur
Date:
Dr.RENGABASHYAM P
CONTENTS
CHAPTER
NO. TITLE
PAGE
NO.
1 INTRODUCTION 1
2 AIMS AND OBJECTIVES 2
3 REVIEW OF LITERATURE 4
4 MATERIALS AND METHODS 37
5 RESULTS AND INTERPRETATION 47
6 DISCUSSION 73
7 SUMMARY 85
8 SUMMARY 85
9 BIBLIOGRAPHY
10 PROFORMA`
11 MASTER CHART

1
INTRODUCTION
Infections are one of the leading cause of morbidity and mortality in
our country. The changing profile of infections need to be determined in
order to focus on specific investigative and therapeutic measures. This study
was undertaken to evaluate the changing profile in patients presenting with
infectious fevers.
2
AIM OF THE STUDY
To study the clinical and laboratory profile of patients with infectious
fever in the medical wards of Government Thanjvaur Medical College and
Hospital.
The groups analysed were:
1. Fever of less than 5 days with
a. Organ dysfunction
b. Temperature >40°C
2. Fever of more than 5 days with or without complications.

3
OBJECTIVES
1. To study the clinical profile like age, sex, fever duration and
associated systemic symptoms in patients with infectious fever.
2. To identify the common etiology of infectious fever.
3. The study the various complications of infectious fever and factors
contributing for it.
4. To analyze the causes of mortality in patients with infectious
fever.

4
REVIEW OF LITERATURE
FEVER1
Definition
Fever is an elevation of the body temperature that exceeds the normal
daily variation and occurs in conjunction with an increase in hypothalamic
set point, which controls the normal body temperature.
Mechanism
Once the hypothalamic set point is raised, neurons in the vasomotor
centre is activated and vasoconstriction commences, shunting of blood away
from the periphery decreasing heat loss. This mechanism increases the body
temperature by 1° to 2°C. Shivering begins at this point of time which further
increases the body temperature. Heat production by liver also increases.
Control of body temperature
Body temperature is controlled by hypothalamus. Neurous in both pre
optic anterior hypothalamus and the posterior hypothalamus receives two
kinds of signals; one from the peripheral nerves that reflect warmth and cold
receptors and other from the temperature of blood bathing the region, which

5
are integerated to maintain the normal body temperature. A normal body
temperature is ordinarily maintained despite environmental variations,
because of the balance between heat production and heat dissipation.
Normal Temperature
According to studies, the mean oral temperature is 36.8° ± 4°C (98.2
± 0.7°F) with low levels at 6 am and higher levels at 4 to 6 pm. In light of
these studies an AM temperature of >37.2°C (98.9°F) or a PM temperature
> 37.7°C (99.9°F) would define fever. Rectal temperatures are generally
0.4°C higher than oral readings. Lower oesophageal temperatures closely
reflect core temperature.
A fever of >41.5°C (>106.7°F) is called hyperpyrexia.
Fever Patterns
Intermittent fevers are temperature elevations that return to normal at
least once during most days.
Continous fevers do not vary more than 1°F. Remittent fevers do not
return to normal each day. Relapsing fevers are recurrent over days or weeks
and may have any undergoing fever pattern.
6
Studies of FUO (Fever of Unknown Origin)
Kejariwal et al.,2 in 2001 at Calcutta studied the etiological profile of
100 cases of FUO, the pattern was infections (53%) followed by neoplasm
(17%), collagen vascular diseases (11%), miscellaneous (5%) and
undiagonosed (14%).
De Kleijn et al.,3 in a study of 167 immunocompetent patients with
FUO found 43 (25.7%) had infections, 21 (12.6%) had neoplasms and 40
(24.0%) had inflammatory diseases.
Petersdorf et al.,4 in 1952 - 57, studied 100 cases, of which majority
(36%) were due to infections like, tuberculosis, abdominal abscess,
endocarditis, brucellosis and urinary tract infections. 26% were due to
lymphomas, leukemias and solid tumors. 15% were due to connective tissue
diseases.
Larson et al., 5 studied 105 cases of FUO patients of which infections
formed 30%. Malignancies formed 37% and 14.3% were due to connective
tissue disorders. Others were undiagnosed.
7
Knockaert et al., 6 studied 199 cases of FUO patients of which
infections formed 22.5%, followed by collagen vascular disorders (21.5%).
Neoplasms formed 7% while others were miscellaneous and undiagnosed.
Sharma et al., 7 studied 150 cases of FUO of which, infections formed
50%, followed by Neoplasms which formed 22%. 8% were due to collagen
vascular diseases, 15% formed miscellaneous causes and 5% were
undiagnosed.
Burke et al., 8 reviewed various studies on FUO and noted that
common treatable causes were tuberculosis, subacute bacterial endocarditis,
abscesses, salmonella and leptospirosis.
STUDIES ON ETIOLOGY OF FEVER
Definition: This entry lists major infectious diseases likely to be
encountered in countries where the risk of such diseases is assessed to be very
high as compared to the United States. These infectious diseases represent risks
to US government personnel traveling to the specified country for a period of
less than three years. The degree of risk is assessed by considering the foreign
nature of these infectious diseases, their severity, and the probability of being
affected by the diseases present. The diseases listed do not necessarily represent
8
the total disease burden experienced by the local population.
The risk to an individual traveler varies considerably by the specific location,
visit duration, type of activities, type of accommodations, time of year, and
other factors. Consultation with a travel medicine physician is needed to
evaluate individual risk and recommend appropriate preventive measures such
as vaccines.
Diseases are organized into the following six exposure categories shown
in italics and listed in typical descending order of risk. Note: The sequence of
exposure categories listed in individual country entries may vary according to
local conditions.
food or waterborne diseases acquired through eating or drinking on the
local economy:
Hepatitis A - viral disease that interferes with the functioning of the liver;
spread through consumption of food or water contaminated with fecal matter,
principally in areas of poor sanitation; victims exhibit fever, jaundice, and
diarrhea; 15% of victims will experience prolonged symptoms over 6-9
months; vaccine available.
Hepatitis E - water-borne viral disease that interferes with the functioning of
the liver; most commonly spread through fecal contamination of drinking

9
water; victims exhibit jaundice, fatigue, abdominal pain, and dark colored
urine.
Typhoid fever - bacterial disease spread through contact with food or water
contaminated by fecal matter or sewage; victims exhibit sustained high fevers;
left untreated, mortality rates can reach 20%.
vectorborne diseases acquired through the bite of an infected arthropod:
Malaria - caused by single-cell parasitic protozoa Plasmodium; transmitted to
humans via the bite of the female Anopheles mosquito; parasites multiply in
the liver attacking red blood cells resulting in cycles of fever, chills, and sweats
accompanied by anemia; death due to damage to vital organs and interruption
of blood supply to the brain; endemic in 100, mostly tropical, countries with
90% of cases and the majority of 1.5-2.5 million estimated annual deaths
occurring in sub-Saharan Africa.
Dengue fever - mosquito-borne (Aedes aegypti) viral disease associated with
urban environments; manifests as sudden onset of fever and severe headache;
occasionally produces shock and hemorrhage leading to death in 5% of cases.

10
Yellow fever - mosquito-borne viral disease; severity ranges from influenza-
like symptoms to severe hepatitis and hemorrhagic fever; occurs only in
tropical South America and sub-Saharan Africa, where most cases are reported;
fatality rate is less than 20%.
Japanese Encephalitis - mosquito-borne (Culex tritaeniorhynchus) viral
disease associated with rural areas in Asia; acute encephalitis can progress to
paralysis, coma, and death; fatality rates 30%.
African Trypanosomiasis - caused by the parasitic protozoa Trypanosoma;
transmitted to humans via the bite of bloodsucking Tsetse flies; infection leads
to malaise and irregular fevers and, in advanced cases when the parasites
invade the central nervous system, coma and death; endemic in 36 countries of
sub-Saharan Africa; cattle and wild animals act as reservoir hosts for the
parasites.
Cutaneous Leishmaniasis - caused by the parasitic protozoa leishmania;
transmitted to humans via the bite of sandflies; results in skin lesions that may
become chronic; endemic in 88 countries; 90% of cases occur in Iran,
Afghanistan, Syria, Saudi Arabia, Brazil, and Peru; wild and domesticated
animals as well as humans can act as reservoirs of infection.

11
Plague - bacterial disease transmitted by fleas normally associated with rats;
person-to-person airborne transmission also possible; recent plague epidemics
occurred in areas of Asia, Africa, and South America associated with rural
areas or small towns and villages; manifests as fever, headache, and painfully
swollen lymph nodes; disease progresses rapidly and without antibiotic
treatment leads to pneumonic form with a death rate in excess of 50%.
Crimean-Congo hemorrhagic fever - tick-borne viral disease; infection may
also result from exposure to infected animal blood or tissue; geographic
distribution includes Africa, Asia, the Middle East, and Eastern Europe; sudden
onset of fever, headache, and muscle aches followed by hemorrhaging in the
bowels, urine, nose, and gums; mortality rate is approximately 30%.
Rift Valley fever - viral disease affecting domesticated animals and humans;
transmission is by mosquito and other biting insects; infection may also occur
through handling of infected meat or contact with blood; geographic
distribution includes eastern and southern Africa where cattle and sheep are
raised; symptoms are generally mild with fever and some liver abnormalities,
but the disease may progress to hemorrhagic fever, encephalitis, or ocular
disease; fatality rates are low at about 1% of cases.
Chikungunya - mosquito-borne (Aedes aegypti) viral disease associated with
12
urban environments, similar to Dengue Fever; characterized by sudden onset
of fever, rash, and severe joint pain usually lasting 3-7 days, some cases result
in persistent arthritis.
water contact diseases acquired through swimming or wading in freshwater
lakes, streams, and rivers:
Leptospirosis - bacterial disease that affects animals and humans; infection
occurs through contact with water, food, or soil contaminated by animal urine;
symptoms include high fever, severe headache, vomiting, jaundice, and
diarrhea; untreated, the disease can result in kidney damage, liver failure,
meningitis, or respiratory distress; fatality rates are low but left untreated
recovery can take months.
Schistosomiasis - caused by parasitic trematode flatworm Schistosoma; fresh
water snails act as intermediate host and release larval form of parasite that
penetrates the skin of people exposed to contaminated water; worms mature
and reproduce in the blood vessels, liver, kidneys, and intestines releasing eggs,
which become trapped in tissues triggering an immune response; may manifest
as either urinary or intestinal disease resulting in decreased work or learning
capacity; mortality, while generally low, may occur in advanced cases usually

13
due to bladder cancer; endemic in 74 developing countries with 80% of infected
people living in sub-Saharan Africa; humans act as the reservoir for this
parasite.
aerosolized dust or soil contact disease acquired through inhalation of aerosols
contaminated with rodent urine:
Lassa fever - viral disease carried by rats of the genus Mastomys; endemic in
portions of West Africa; infection occurs through direct contact with or
consumption of food contaminated by rodent urine or fecal matter containing
virus particles; fatality rate can reach 50% in epidemic outbreaks.
respiratory disease acquired through close contact with an infectious person:
Meningococcal meningitis - bacterial disease causing an inflammation of the
lining of the brain and spinal cord; one of the most important bacterial
pathogens is Neisseria meningitidis because of its potential to cause epidemics;
symptoms include stiff neck, high fever, headaches, and vomiting; bacteria are
transmitted from person to person by respiratory droplets and facilitated by
close and prolonged contact resulting from crowded living conditions, often
with a seasonal distribution; death occurs in 5-15% of cases, typically within
24-48 hours of onset of symptoms; highest burden of meningococcal disease
occurs in the hyperendemic region of sub-Saharan Africa known as the
14
"Meningitis Belt" which stretches from Senegal east to Ethiopia.
animal contact disease acquired through direct contact with local animals:
Rabies - viral disease of mammals usually transmitted through the bite of an
infected animal, most commonly dogs; virus affects the central nervous system
causing brain alteration and death; symptoms initially are non-specific fever
and headache progressing to neurological symptoms; death occurs within days
of the onset of symptoms.
Shivakumar et al.,9 reported the study on etiology profile of fever, a study
carried out in Chennai during 2002 - 2003. Out of 195 diagnosed cases
tuberculosis formed 40% of cases, pneumonia 15.4%, meningitis and
malaria forming 12.8% each and leptospirosis forming 8.2%. The proportion
of undiagnosed cases was 46%.
Ruth D. Ellis et al.,10 studied to find out the etiological profile of fever in
the Thailand, which was carried out from 1999 to 2002. Etiologic diagnosis
was made in 48% cases. Malaria was the most common diagnosis accounting
for 25%, followed by leptospirosis, comprising about 17%. Other etiologic
diagnosis were intestinal infections, dengue fever and typhoid.
15
LITERATURE ON INDIVIDUAL FEVERS
MALARIA
PROBLEM STATEMENT
WORLD11
- 107 countries has areas of risk of malaria transmission.
- 3.2 billion people live in areas of risk of malaria transmission.
- 350 - 500 million malaria episodes occur annually.
- 1 million malaria deaths occur annually.
INDIA12
In 2006, there were 1.04 million vivax malaria cases and 0.46 million
falciparum cases reported in India. There were 890 deaths due to malaria.
MALARIAL SPECIES
There are four species of human malarial parasite i.e. Pl.vivax,
Pl.falciparum, Pl.malariae and P1.ovale. In India 60 - 65% of infections are
due to Pl.vivax and 35 to 45% are due to Plasmodium falciparum.
Antigenic diversity is present among different malarial parasites and
also within the species.
16
SEVERE MALARIA
Severe malaria is usually caused by Pl.falciparum but recently it has
been reported in Pl.vivax cases in Indian Subcontinent.
CLINICAL FEATURES
Uncomplicated malaria :
The clinical features of complicated malaria are common to all
species. Head ache, muscular ache, abdominal discomfort, lethargy and
lassitude often precede fever by about 2 days.
The fever in Plasmodium vivax and Plasmodium ovale regularises to
a two day cycle and in Plasmodium malaria to a 3 day cycle. The fever in
Pl.falciparum may never regularise to a classical tertian pattern.
DEFINITION OF SEVERE MALARIA BY WHO13
1. Renal failure : Sr.creatinine > 3 mgs / dl
Urine output < 400 ml / 24 hrs (or)
< 12 ml / hr
2. Severe Anaemia Hb% < 5 gms % (or)
Hct < 15%
3. Cerebral malaria : Unarousable coma with peripheral
parasitemia

17
4. Pulmonary Oedema or acute respiratory distress syndrome
5. Hypoglycemia : Blood sugar < 40 mg / dl
6. Shock - Systolic BP < 70 mm Hg (Adults)
< 50 mm Hg (Children - 1-5 yrs)
7. Acidemia - pH < 7.33, Hco3 < 15 mq / l
8. Spontaneous bleeding : Gums, Nose and GIT due to DIC
9. Macroscopic haemoglobinuria
10. Seizures > 3 episodes
11. Hyperparasitemia - More than 20%
12. Jaundice : Serum bilirubin > 3 mgs / dl is a marker of severe malaria,
only when combined with other vital organ dysfunction (i.e. cerebral
malaria and renal failure).
The 2000 WHO recommendation also include the following under
severe malaria.
1. Impairment of consciousness less marked than unarousable coma.
2. Prostration - Inability to sit unassisted in a child who is normally able
to do so. In a child not old enough to sit this is defined as inability to
feed.
18
STUDIES OF MALARIA
Bansode et al,14 conducted a prospective study of malaria at Bombay during
June 1993 to May 1994. All patients had fever, followed by head ache
(92%), vomitting (74%), cough (7%), diarrhoea (4.6%), icterus (3.8%) and
oliguria (1%) 70% were due to Plasmodium vivax and 30% due to
Pl.falciparum.
Madhu Muddaiah et al.,15 in mangalore in 2002 - 2004 studied the profile
of 190 admitted patients with smear positive malaria. Plasmodium vivax-
90, Plasmodium falciparum-71, mixed infections - 29. Jaundice occurred in
5 cases of vivax, 20 cases of falciparum and 3 cases of mixed infections.
Over all
28 (14.73%) had jaundice. Splenomegaly was seen in 30 (15.7%),
hepatosplenomegaly in 26 (13.6%), hepatomegaly in 8 (4.2%) and raised
serum creatinine in 14 (11.57%) cases.
Mohapatra et al.,16 from Berhampur has reported various atypical
presentation of malaria in their study of 110 cases of vivax malaria. They
were absence of malarial paroxysm (22.8%), migrainous head ache (4.5%),
myalgia (6.3%), episodic utricarial rash (1.8%), relative bradycardia
(13.6%) and postural hypotension (2.7%).
19
Chowta et al.,17 in 2003 studied 54 patients of both Plasmodium vivax
and Plasmodium falciparum and noted chloroquine resistance in 9(16%)
patients.
CHANGING TRENDS IN INDIA
The spectrum of severe falciparum malaria has changed world wide.
Currently a large proportion of cerebral malaria patients present with
multiple complications including acute renal failure and jaundice18.
Mohapatra et al.,16 in 2006 from Orissa observed that jaundice is an
important solitary complication. There were multiple complications and
majority had constellation of 3 complications. Cerebral malaria, jaundice
and renal failure (75.3%) were the most common combination. The mortality
rate was 14.6%, 21.3%, 30.9%, 38.5%, 100% and 100%, among patients
with 1, 2,
3, 4, 5 and 6 combinations respectively.
SEVERE VIVAX MALARIA
Pl.vivax is usually presumed to cause only uncomplicated malaria but
in the last few years there has been many reports regarding severe vivax
malaria. In a recent study from Bikaneer, Kochar et al.,19 reported 11 cases
20
of definite severe vivax malaria. In all these cases Plasmodium falciparum
infection was ruled out by PCR (polymerase chain reaction). All other
infectious causes were ruled out by appropriate tests. In this study the
manifestations observed were jaundice and hepatic dysfunction in four,
severe anaemia in four, cerebral malaria in three, ARDS in three, bleeding
diathesis in one and MODS (multi organ dysfunction syndrome) in five
patients. Recently in a monograph on treatment of malaria by WHO in 2006
the terminology of severe vivax malaria has been accepted seperately and it
had advocated the same regimen of treatment as for severe falciparum
malaria.
LEPTOSPIROSIS20
Epidemiology
It is caused by leptospira interrogans complex which has over 20
serogroups and more than 200 serovars. Rodents, domestic and wild animals
form the reservoir of infection, whereas domestic animals such as cattle,
dogs, pigs may act as carriers for several months (temporary carrier) and
rodents usually remain carrier through out life (permanent carrier).
1. Anicteric Leptospirosis
Presents with fever, head ache, body pain and biphasic illness. It has
abrupt onset with chills, rigor, fever, head ache and body pain. The most

21
characteristic finding on examination is severe myalgia and conjunctival
suffusion. A transient rash can occur. The septicemic phase subsides after 7
- 14 days. The second phase (immune phase) is characterized by severe
head ache and low grade fever lasting 4 - 30 days.
2. Icteric Leptospirosis
In some patients, the septicemic phase instead of subsiding progresses
to a severe icteric illness with renal failure. Some of the important clinical
features are as follows;
Kidneys : Renal involvement is the most serious complication and is
the commonest cause of death. Renal manifestations range from urinary
sediment changes (pyuria, haematuria and granular casts) to severe renal
failure. Renal manifestations are observed commonly in all forms of
leptospirosis regardless of the severity of disease or of the infecting sero -
group.
Liver : Jaundice is the most important clinical feature of severe illness.
Jaundice occurs between the fourth to sixth day but may occur as early as
the second day or as late as ninth day, deepens rapidly, reaching a peak
within a week. The liver is often enlarged and tender. Jaundice is mainly due
to hepatocellular damage. However, hepatocellular necrosis is usually mild
and additional factors include intrahepatic cholestasis and increased
22
bilirubin load from absorption of tissue haemorrhage. Marked elevation of
serum bilirubin with mildly elevated transaminases is characteristic. Death
is rarely due to hepatic failure.
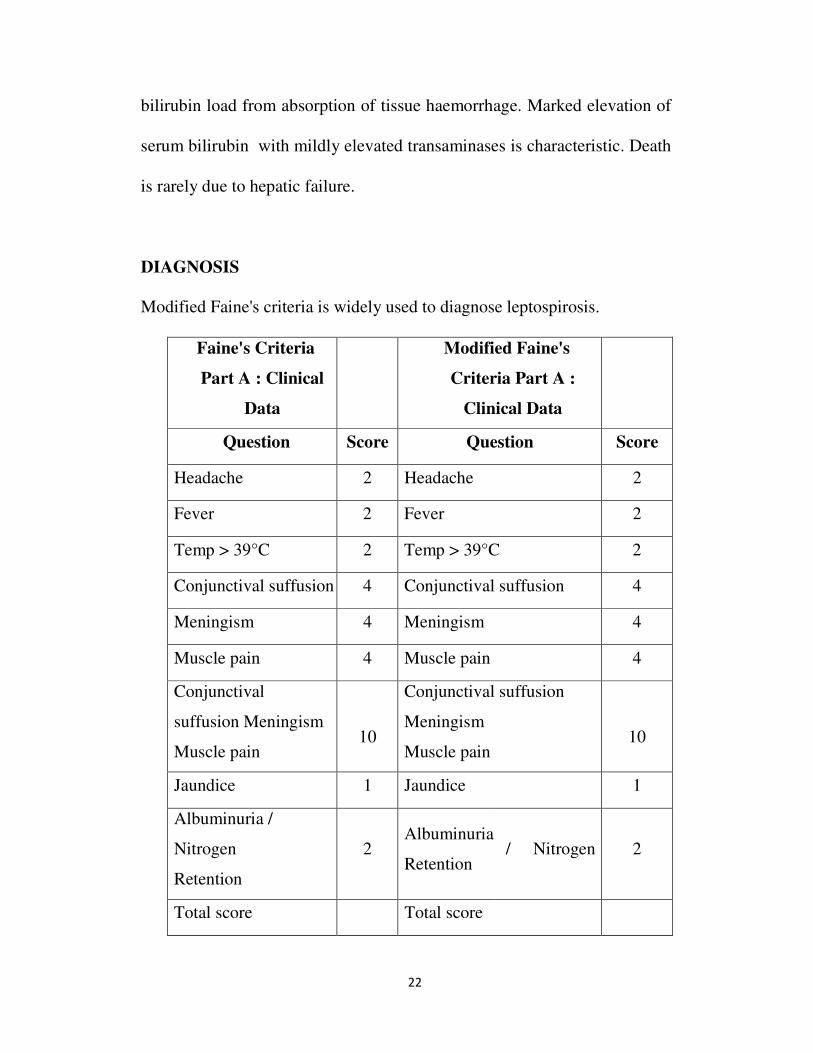
DIAGNOSIS
Modified Faine's criteria is widely used to diagnose leptospirosis.
Faine's Criteria
Part A : Clinical
Data
Modified Faine's
Criteria Part A :
Clinical Data
Question Score Question Score
Headache 2 Headache 2
Fever 2 Fever 2
Temp > 39°C 2 Temp > 39°C 2
Conjunctival suffusion 4 Conjunctival suffusion 4
Meningism 4 Meningism 4
Muscle pain 4 Muscle pain 4
Conjunctival
suffusion Meningism
Muscle pain
10
Conjunctival suffusion
Meningism
Muscle pain
10
Jaundice 1 Jaundice 1
Albuminuria /
Nitrogen
Retention
2 Albuminuria
Retention / Nitrogen 2
Total score Total score

23
Part B:
Epidemiological
factors
Part B : Epidemiological
factors
Contact with animals
or
Rainfall
Contact with contaminated
environment
Animal contact
Tota
5
contact with known 10
4
1
10
contaminated water
Part C :
Bacteriological and
Lab Findings
Part C : Bacteriological
and Lab Findings
Isolation of leptospira
in
culture-Diagnosis
certain
Isolation of leptospira in
culture - Diagnosis certain
Positive Serology
(MAT)
Leptospirosis
Endemic
Positive Serology
Single positive-Low
titre 2
ELISA IgM positive
SAT - Positive
MAT - Single high titre
Rising titre (Paired sera)
15
Single positive-High
titre 10 15
Leptospirosis Non 15
Endemic
24
Single positive-Low
titre 5
Total (A+B+C)
Single positive-High
titre 15 25
Rising titre (Paired
sera) 25
Total (A+B+C)
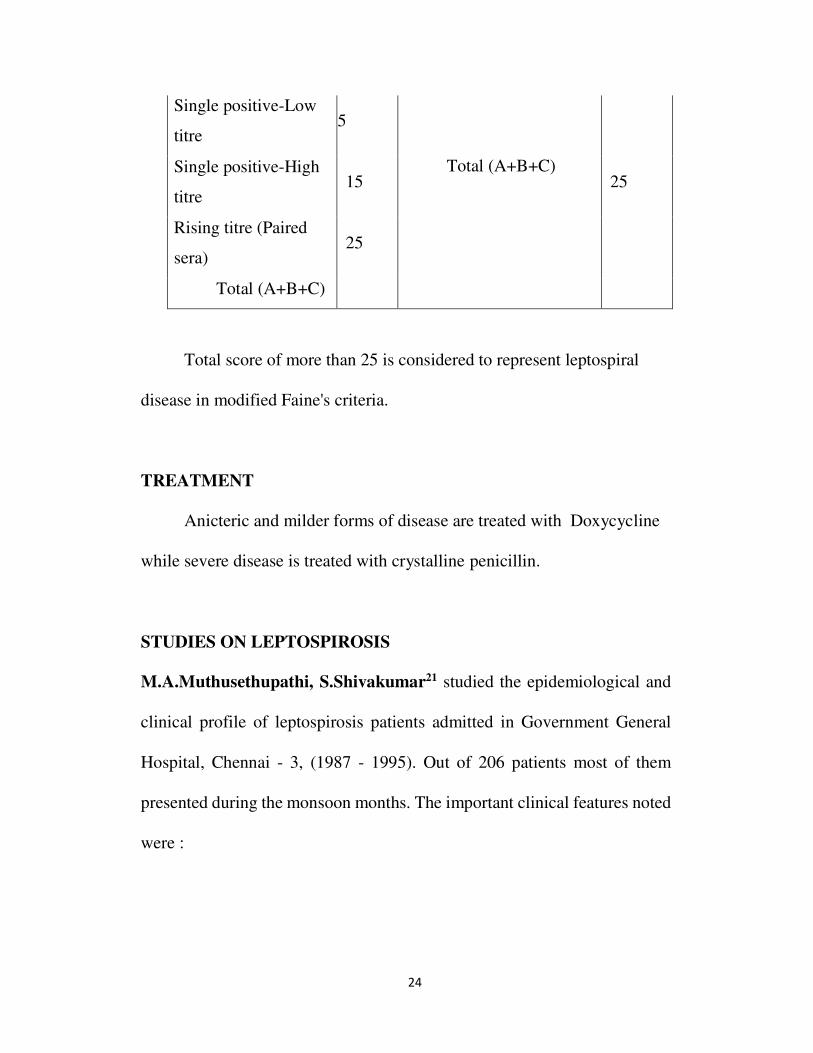
Total score of more than 25 is considered to represent leptospiral
disease in modified Faine's criteria.
TREATMENT
Anicteric and milder forms of disease are treated with Doxycycline
while severe disease is treated with crystalline penicillin.
STUDIES ON LEPTOSPIROSIS
M.A.Muthusethupathi, S.Shivakumar21 studied the epidemiological and
clinical profile of leptospirosis patients admitted in Government General
Hospital, Chennai - 3, (1987 - 1995). Out of 206 patients most of them
presented during the monsoon months. The important clinical features noted
were :
25
a. Fever - 100%
b. Jaundice - 83%
c. Renal failure - 79%
d. Myalgia - 79%
e. Conjunctival Suffusion - 43%
f. CNS - 43%
g. Bleeding tendencies - 28%
Autumnalis was the most common serogroup noted then.
Overall icteric leptospirosis constituted the common group with
83% and mortality was 15.5%.
Sumathi G. et al.,22 reported the serodiagnosis results of leptospirosis
from 1995 - 1997, during which microscopic agglutination test revealed
that the predominant serovar to be autumnalis (48.3%) and ictero
haemorrhagiae (31.1%).
In 2006, Shivakumar S23 reported that severe leptospirosis has
declined, mild leptospirosis has increased. He reports that in a recent study
of 106 cases of leptospirosis from North Chennai, jaundice occurred in
17.8% and renal failure occurred in 10.3% showing a decline in

26
complication. Fever, head ache and myalgia were the common presentation.
Only 2 patients were dialysed and there were no deaths. Contaminated
environment (98%) and rainfall (50%) were the important epidemiological
risk factors.
Muthusethupathi et al.,24 studied the clinical and serological profile
in 57 patients. All had fever followed by jaundice (84%), mylagia (82%),
acute renal failure (72%) and conjunctival suffusion (58%). 23 cases
underwent dialysis. Autumnalis was the serogroup most commonly
recorded.
Lecour et al.,25 studied 50 cases of leptospirosis and reported renal
failure in 62%, aseptic meningitis in 24% with leptospira ictero
haemorrhagiae responsible for 78% of cases.
TUBERCULOSIS
PROBLEM STATEMENT26
WORLD
9 million cases occur world wide annually 54
million people are infected annually
2.4 million deaths occur annually
27
INDIA
- 20% of the total cases in the world.
- 1.8 million cases occur annually
- 30,000 patients become smear positive every year.
- Death rate is 100 - 200 / lakh / year.
- It is mostly prevalent in the productive age group of 25 - 45 yrs.
Even though TB is a major global health problem, there are only
a few studies about the pattern and profile of its presentation.
Samal et al.,27 analysed clinical features and evaluated
changing trends in 110 non - drug resistant sputum positive
pulmonary tuberuclosis between 1987 - 1989. Majority had
haemoptysis (60.7%), cough (47.06%) and fever (44.7%). Other
symptoms were hoarseness of voice and loss of weight. 18% had
clubbing and 3.5% had lymphadenopathy. Radiologically 98% had
fibro caseous lesions, cavity in 60% and bilateral opacities in 59%.
Dehankar et al.,28 studied X-ray changes in pulmonary
tuberculosis. 27% had bilateral lesions, 27% had right lower lobe
apical segment lesion, and 14% in basal segment. Lingula and whole

28
left lower lobe was less commonly involved. 41% was AFB positive
on smear examination.
PNEUMONIA
Community acquired pneumonia continues to be a common and
serious disease in both developed and developing countries.
Bansal .S et al.,29 studied the clinical and bacteriological profile of
community acquired pneumonia in a tertiary care hospital at Himachal
Pradesh. 70 patients were studied. Patients older than 40 years were
predisposed. Etiological diagnosis was obtained in 53(75%) cases. Among
that 19 cases of Streptococcus pneumoniae, 12 cases of Klebsiella
pneumoniae, 9 cases of Staphylococcus aureus, 8 cases of Mycoplasma
pneumonia and 6 cases of Escherichia coli were grown in culture.
CO-INFECTION OF MALARIA AND LEPTOSPIROSIS
In many parts of the world where both malaria and leptospirosis are
endemic co-infection with both malaria and leptospirosis is common. Ruth
D Ellis in a study in Bangkok from 1999 to 2003, reported 5.12% of
coinfection of malaria and serologically proven leptospirosis in a total of
613 cases10.
29
ENTERIC FEVER
Chowta MN et al.,30 in mangalore studied the clinical profile and
antibiotic response in typhoid fever from 1999 - 2001. In his study of 44
cases he noted ciprofloxacin resistance in 18.1% of cases. Yew et al.,31 in
his study of clinical profile of enteric fever reported splenomegaly in 47%.
BACTERIAL MENINGITIS
Pomeroy et al.,32 studied the clinical profile of meningitis and
reported seizures in 30% of cases.
CONTRIBUTIONS OF INFECTIONS IN INDIAN STUDIES ON
FUO
Study Sharma
(1992)7
Handa
(1994)33
Dhawan
(1994)34
Agarwal
(1998)35
Infection 50% 48% 81% 61%
DENGUE
Dengue is a mosquito-borne viral disease that has rapidly spread in all
regions of WHO in recent years. Dengue virus is transmitted by female
mosquitoes mainly of the species Aedes aegypti and, to a lesser extent, Ae.
albopictus. This mosquito also transmits chikungunya, yellow fever and Zika
30
infection. Dengue is widespread throughout the tropics, with local variations in
risk influenced by rainfall, temperature and unplanned rapid urbanization.
Severe dengue was first recognized in the 1950s during dengue epidemics in
the Philippines and Thailand. Today, severe dengue affects most Asian and
Latin American countries and has become a leading cause of hospitalization
and death among children and adults in these regions.
Dengue is caused by a virus of the Flaviviridae family and there are 4
distinct, but closely related, serotypes of the virus that cause dengue (DEN-1,
DEN-2, DEN-3 and DEN-4). Recovery from infection by one provides lifelong
immunity against that particular serotype. However, cross-immunity to the
other serotypes after recovery is only partial and temporary. Subsequent
infections (secondary infection) by other serotypes increase the risk of
developing severe dengue.
Global burden of dengue
The incidence of dengue has grown dramatically around the world in
recent decades. A vast majority of cases are asymptomatic and hence the actual
numbers of dengue cases are underreported and many cases are misclassified.
One estimate indicates 390 million dengue infections per year (95% credible
interval 284–528 million), of which 96 million (67–136 million) manifest
clinically (with any severity of disease).36 Another study, of the prevalence of
31
dengue, estimates that 3.9 billion people, in 128 countries, are at risk of
infection with dengue viruses.37
Member States in three WHO regions regularly report the annual number
of cases. The number of cases reported increased from 2.2 million in 2010 to
over 3.34 million in 2016. Although the full global burden of the disease is
uncertain, the initiation of activities to record all dengue cases partly explains
the sharp increase in the number of cases reported in recent years.
Other features of the disease include its epidemiological patterns, including
hyper-endemicity of multiple dengue virus serotypes in many countries and the
alarming impact on both human health and the global and national economies.
Dengue virus is transported from one place to another by infected travelers.
CLASSIFICATION
The WHO classifies DF into two groups: Uncomplicated and severe.
Severe cases are linked to excessive hemorrhage, organ impairement, or severe
plasma escape, and the remaining cases are considered uncomplicated.38
According to the 1997 classification, dengue can be divided into
undifferentiated fever, DF, and DHF.39 DHF was further subdivided into grades
I–IV.
Grade I: Only mild bruising or a positive tourniquet test
Grade II: Spontaneous bleeding into the skin and elsewhere

32
Grade III: Clinical sign of shock
Grade IV: Severe shock - feeble pulse, and blood pressure cannot be recorded.
Here, grades III and IV comprise DSS.
CLINICAL MANIFESTATIONS
Undifferentiated fever
This stage is seen mostly in the primary infection but may also occur following
the initial secondary infection. Clinically, it is difficult to differentiate from
numerous other viral diseases and often remains undiagnosed.
Dengue fever
DF follows both primary and secondary infections, and is most
frequently encountered in adults and older children. Onset of symptoms is
characterized by a biphasic, high-grade fever lasting for 3 days to 1 week. 38
Severe headache (mainly retrobulbar), lassitude, myalgia and painful joint,
metallic taste, apetite loss, diarrhea, vomiting, and stomachache are the other
reported manifestations. Dengue is also known as breakbone fever because of
the associated myalgia and pain in joints.39 Of patients with DF, 50–82% report
with a peculiar cutaneous rash.40 The initial rash is the result of capillary
dilatation, and presents as a transient facial flushing erythema, typically
occuring before or during the first 1–2 days of fever. The second rash is seen
33
at 3 days to 1 week following the fever, and presents as a asymptomatic
maculopapular or morbilliform eruption. Sometimes, individual lesions may
merge and present as widespread confluent erythematous areas with pinpoint
bleeding spots and rounded islands of sparing, giving a typical appearance of
“white islands in a sea of red.”41 The cutaneous rash is usually asymptomatic,
and pruritis is reported only in 16-27% cases.42 Bleeding episodes are
infrequently seen in DF, although epistaxis and gingival bleeding, substantial
menstruation, petechiae/purpura, and gastrointestinal tract (GIT) hemorrhage
can occur.43
Dengue hemorrhagic fever
DHF is frequently seen during a secondary dengue infection. However, in
infants it may also occur durring a primary infection due to maternally attained
dengue antibodies.44
The proposed diagnostic criteria for DHF includes:45
• a.Clinical parameters: Acute-onset febrile phase – high-grade fever
lasting from 2 days to 1 week. Hemorrhagic episodes (at least one of the
following forms): Petechiae, purpura, ecchymosis, epistaxis, gingival
and mucosal bleeding, GIT or injection site, hematemesis and/or malena
Positive tourniquet and hepatomegaly.
34
• b. Laboratory parameters: Thrombocytopenia (platelet count
<100,000/cu mm)
The hemorrhagic episodes in DHF are associated with multifactorial
pathogenesis. Vasculopathy, deficiency and dysfunction of platelets and
defects in the blood coagulation pathways are the attributed factors. Decreased
production of platelets and increased destruction of platelets may result in
thrombocytopenia in DHF. The impaired platelet function causes the blood
vessels to become fragile and this results in hemorrhage.46
The clinical course of DHF is characterized by three phases: Febrile,
leakage, and convalescent phase. High-grade fever of acute onset along with
constitutional signs and facial erythema characterizes the commencement of
the febrile illness. The initial febrile illness is marked by a morbilliform rash
and hemorrhagic tendencies. The fever persists for 2 days to 1 week and then
drops to normal or subnormal levels when the patient either convalesces or
advances to the plasma leakage phase. 47 High plasma escape cases are marked
by frank shock with low pulse pressure, cyanosis, hepatomegaly, pleural and
pericardial effusions, and ascites. Severe ecchymosis and gastrointestinal
bleeding followed by epistaxis may also be noted in a few cases. Bradycardia,
confluent petechial rashes, erythema, and pallor are seen during this phase.
35
Dengue shock syndrome
DSS is defined as DHF accompanied by a unstable pulse, narrow pulse
pressure (<20 mmHg), restlessness, cold, clammy skin, and circumoral
cyanosis. Progressively worsening shock, multiorgan damage, and
disseminated intravascular coagulation account for a high mortality rate
associated with DSS. The shock persists for a short span of time and the patient
promptly recovers with supportive therapy.48
Dengue hemorrhagic fever
At first, symptoms of DHF may be mild, but they gradually worsen
within a few days. As well as mild dengue symptoms, there may be signs of
internal bleeding.
A person with Dengue hemorrhagic fever may experience:
• bleeding from the mouth, gums, or nose
• clammy skin
• damage to lymph and blood vessels
• internal bleeding, which can lead to black vomit and feces, or stools
• a lower number of platelets in the blood
• sensitive stomach
• small blood spots under the skin
• weak pulse

36
Without prompt treatment, DHF can be fatal.
Dengue shock syndrome
DSS is a severe form of dengue. It can be fatal.
Apart from symptoms of mild dengue fever, the person may experience:
• intense stomach pain
• disorientation
• sudden hypotension, or a fast drop in blood pressure
• heavy bleeding
• regular vomiting
• blood vessels leaking fluid
Without treatment, this can result in death.

37
MATERIALS AND METHODS
STUDY DESIGN: A PROSPECTIVE QUESTIONNAIRE BASED
OBSERVATIONAL STUDY
B. STUDY PLACE :DEPARTMENT OF MEDICINE, THANJAVUR
MEDICAL COLLEGE THANJAVUR.
C. STUDY PERIOD: JANUARY 2018- DECEMBER 2018
D. STUDY INSTRUMENTS
A. A predesigned, pretested, semi structured questionnaire. Containing items
on
a) Identification data i.e. age, gender , educational status, area of residence,
socio- economic status of study subjects
Patients getting admitted to medical wards of Government Thabjavur
Medical College and Hospital, Chennai, with fever and satisfying the below
criteria were taken up for study. Patients of age group more than 12 years,
both male and female were included.
INCLUSION CRITERIA
I. The following patients were included with number of days of fever less
than 5 days and temperature >40°C or following complications
38
a. With altered sensorium, seizures, signs of meningitis.
b. Clinical signs suggestive of pneumonic consolidation.
c. Signs suggestive of pleural effusion.
d. Polyarthralgia
e. Rash
f. Purpura / ecchymoses
g. Oliguria or serum creatinine > 1.5 mg/dl
h. Jaundice or serum total bilirubin > 1.5 mg/dl
II. Fever of more than 5 days with or without organ dysfunction
EXCLUSION CRITERIA
1. HIV seropositivity
2. Non - infectious causes of fever like hematological malignancy.
connective tissue disorders and solid tumours were excluded from
the study.
39
THE FOLLOWING DATA WERE ANALYSED
PROFORMA
Name : Age : Sex : I.P.
No : Occupation and address :
1. SYMPTOMATOLOGY
FEVER
* Duration, pattern
* Rigors
* Other associated factors
RESPIRATORY SYSTEM
* Cough with expectoration
* Chest pain, hemoptysis
* Wheeze
CARDIOVASCULAR SYSTEM
* Chest pain, breathlessness
* Palpitations, syncope
ABDOMEN
* Nausea, vomiting, abdominal pain
* Loose stools, constipation
* Abdominal distension
40
* Jaundice
GENITOURINARY TRACT
* High coloured urine / hematuria
* Burning micturition
* Decreased urine output
NERVOUS SYSTEM
* Altered sensorium, head ache
* Seizures, motor weakness
* Cranial nerve symptoms
* Symptoms of in co-ordination
LOCOMOTOR SYSTEM
* Joint swelling / pain
* Muscle pain, back ache
SKIN / MUCOSA
* Rashes, purpuric spots, ecchymosis
* Vesications
* Oral mucosal lesions
EAR
* Ear ache / discharge

41
OTHERS
* Loss of appetite and weight
* Sore throat, neck swelling
* Leg swelling
PAST ILLNESS
* H/o. TB, DM, Rheumatic fever, Rheumatic heart
disease, seizure disorder, sexually transmitted disease.
* H/o jaundice, blood transfusion
* H/o drugs, previous surgeries
PERSONAL HISTORY
* Smoking, alcohol, drug addiction
* Exposure (high risk behaviour)
FAMILY HISTORY
* H/o jaundice, tuberculosis
VITAL SIGNS
* Pulse
* Blood Pressure
* Temperature pattern
* Respiratory rate
42
2. GENERAL EXAMINATION
* Level of consciousness
* Temperature, hydration
* Clubbing, lymphadenopathy
* Rashes / petechiae / ecchymosis
* Pedal edema, arthritis
* Bony tenderness, spine tenderness
EXAMINATION OF
* Cardiovascular system
* Respiratory system
* Abdomen
* Nervous system
INVESTIGATIONS
* Blood : TC, DC, Hb%, PCV, ESR, Platelets
* Peripheral smear, cytology and parasites
* Blood urea, sugar
* Liver function test
* Blood culture and sensitivity
* ECG in all leads
* X-ray chest : PA view
* USG - abdomen

43
* Urine - albumin, sugar, deposits
* Urine - culture and
sensitivity If fever is >1 week
* Blood Widal
* Serology for Leptospirosis
* ELISA for HIV
In relevant cases, the following investigations were done :
* Sputum AFB, sputum culture and sensitivity, pleural
fluid analysis
* Mantoux test
* Smear / QBC for malarial parasite
* CSF analysis
* Bone marrow study
* CT scan : Brain, chest, abdomen etc
* Lymph node : FNAC / Biopsy
* ANA, RF
44
DIAGNOSTIC CRITERIA
1. Tuberculosis
Patient was diagnosed to have pulmonary tuberculosis if any of the
following criteria is satisfied.
* 2 initial sputum smear examination positive for AFB.
* Sputum smear examination positive for AFB and radiological
abnormalities consistent with active pulmonary tuberculosis.
* Symptoms suggestive of TB with atleast 3 sputum examination
negative for AFB and radiological abnormalities consistent with
active pulmonary tuberculosis.
Extrampulmonary tuberculosis was diagnosed based on one culture
positive specimen from the extrapulmonary site (or) histological evidence
(or) strong clinical evidence consistent with active extrapulmonary TB.
2. Pneumonia was diagnosed based on clinical features, radiological
findings, positive gram stain and sputum culture.
3. Meningitis was diagnosed based on clinical features, cytology, gram
stain and culture of CSF, CSF - AFB and biochemistry.
4. Malaria was diagnosed based on clinical features, peripheral smear
and quantitative buffy coat.

45
5. Leptospirosis was diagnosed based on clinical features, MSAT
(macroscopic slide agglutination test) with a 2+ (or) 3+ positivity with
modified Faine's score more than 25.
6. Enteric fever was diagnosed with WIDAL test, using a cut-off of
> 1/200 for O/H agglutinin titres, (or) a positive blood culture.
7. Rheumatic fever was diagnosed based on Modified Jones Criteria.
8. Infective endocarditis was diagnosed based on Duke's Criteria.
9. Liver abscess was diagnosed based on clinical features and
ultrasonography.
10. Chikungunya fever was diagnosed by symptoms of fever with
polyarthralgia during the epidemic.
11. Urinary tract infection was diagnosed based on symptoms and
positive urine culture.
12. Other diseases were clinically diagnosed and confirmed by
appropriate biochemical and radiological investigations.

46
STATISTICAL ANALYSIS
The collected data was entered in MS-Excel and was analyzed and
statistically evaluated using SPSS-17 version.
Quantitative data was expressed by mean and standard deviation and
qualitative data was expressed by the percentages and difference between the
proportions was observed by chi square test or Fischer exact test.
p< 0.05 was considered significant.
ETHICAL CONSIDERATIONS
1. The protocol of the thesis was approved by the ethical committee of
Thanjavur Medical College in December 2017.
2. Informed written consent was taken from all study subjects. No pressure
coercion was exerted on subjects for participation in the study.
3. Confidentiality and privacy was ensured at all stages
The subject was free to leave the study at any time and no questions were
asked. They were not be debarred from getting any medical services similar to
the participants.m
47
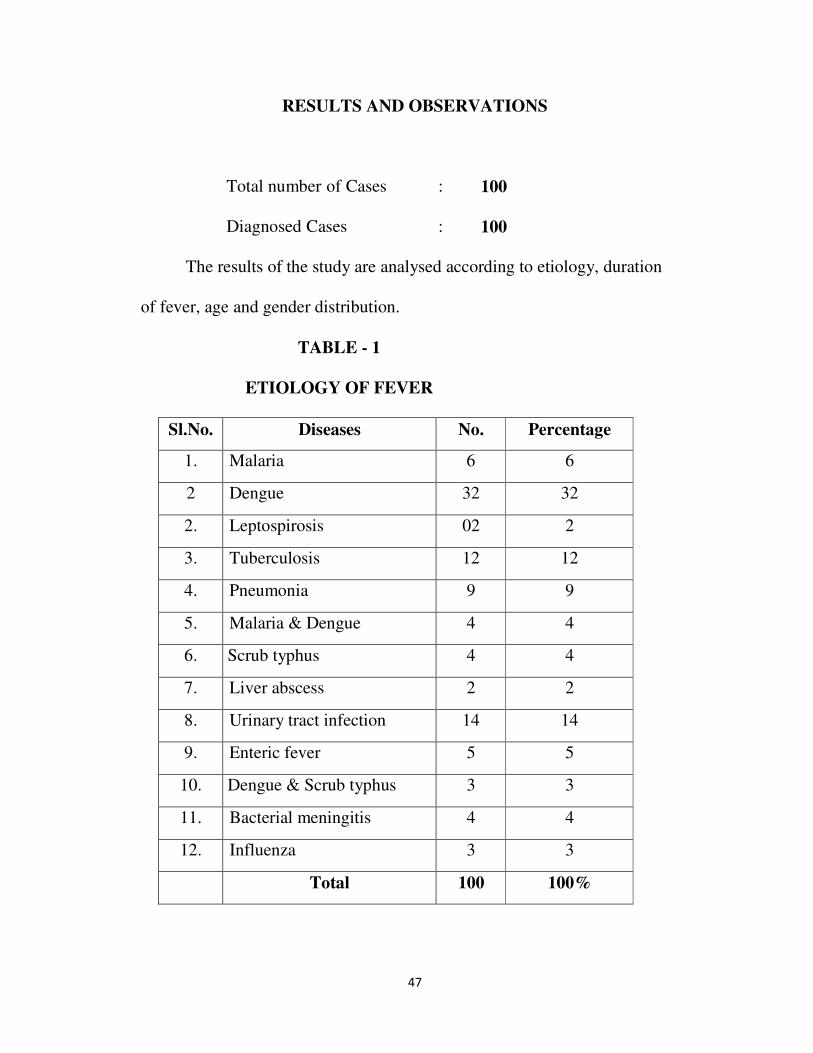
RESULTS AND OBSERVATIONS
Total number of Cases : 100
Diagnosed Cases : 100
The results of the study are analysed according to etiology, duration
of fever, age and gender distribution.
TABLE - 1
ETIOLOGY OF FEVER
Sl.No. Diseases No. Percentage
1. Malaria 6 6
2 Dengue 32 32
2. Leptospirosis 02 2
3. Tuberculosis 12 12
4. Pneumonia 9 9
5. Malaria & Dengue 4 4
6. Scrub typhus 4 4
7. Liver abscess 2 2
8. Urinary tract infection 14 14
9. Enteric fever 5 5
10. Dengue & Scrub typhus 3 3
11. Bacterial meningitis 4 4
12. Influenza 3 3
Total 100 100%
48
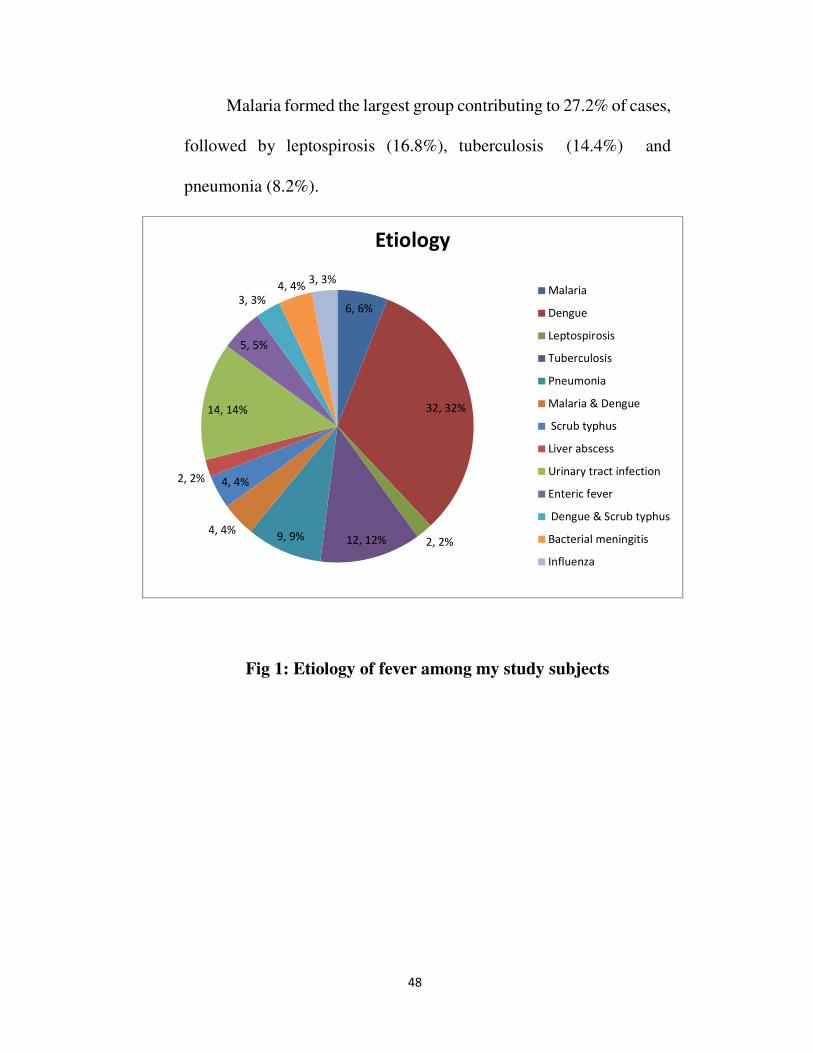
Malaria formed the largest group contributing to 27.2% of cases,
followed by leptospirosis (16.8%), tuberculosis (14.4%) and
pneumonia (8.2%).
Fig 1: Etiology of fever among my study subjects
6, 6%
32, 32%
2, 2%12, 12%9, 9%4, 4%
4, 4%2, 2%
14, 14%
5, 5%
3, 3%
4, 4%3, 3%
Etiology
Malaria
Dengue
Leptospirosis
Tuberculosis
Pneumonia
Malaria & Dengue
Scrub typhus
Liver abscess
Urinary tract infection
Enteric fever
Dengue & Scrub typhus
Bacterial meningitis
Influenza
49
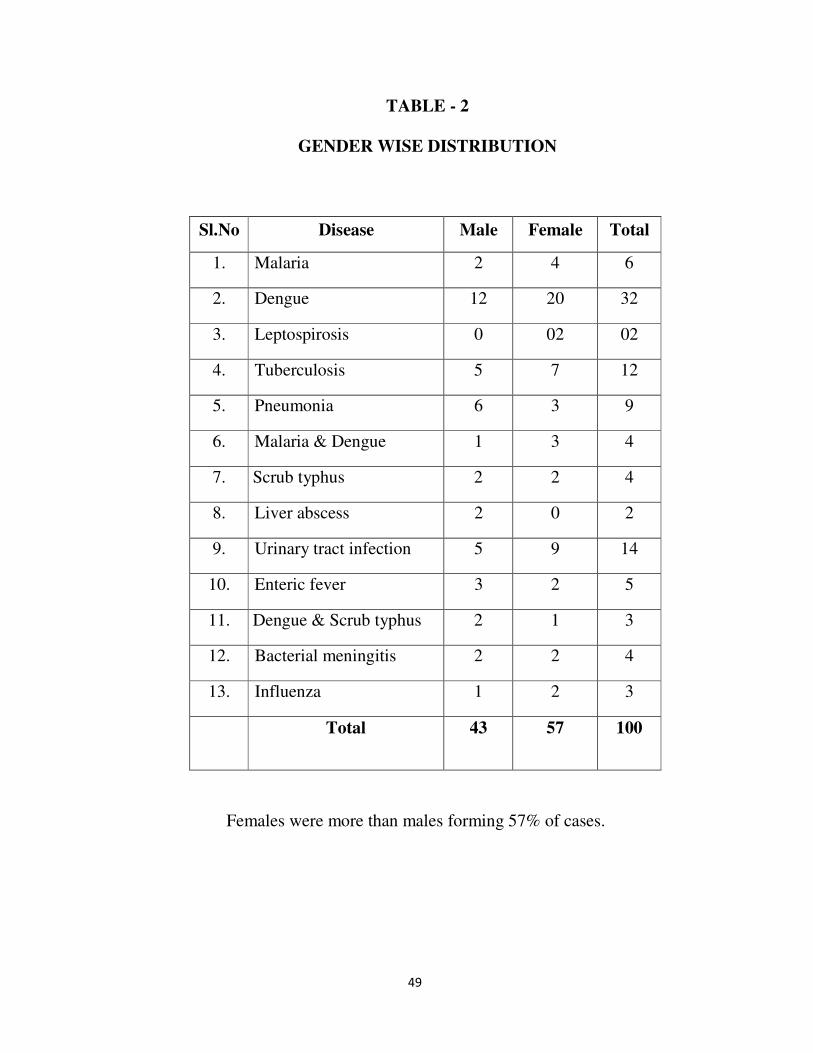
TABLE - 2
GENDER WISE DISTRIBUTION
Sl.No Disease Male Female Total
1. Malaria 2 4 6
2. Dengue 12 20 32
3. Leptospirosis 0 02 02
4. Tuberculosis 5 7 12
5. Pneumonia 6 3 9
6. Malaria & Dengue 1 3 4
7. Scrub typhus 2 2 4
8. Liver abscess 2 0 2
9. Urinary tract infection 5 9 14
10. Enteric fever 3 2 5
11. Dengue & Scrub typhus 2 1 3
12. Bacterial meningitis 2 2 4
13. Influenza 1 2 3
Total 43 57 100
Females were more than males forming 57% of cases.

50
TABLE - 3
AGE WISE DISTRIBUTION IN FEVER CASES
Sl.No. Disease Age in Years
14-20 21-40 41-60 >60
1. Malaria 0 2 4 0 6
2. Dengue 6 15 9 2 32
3. Leptospirosis 1 1 02
4. Tuberculosis 1 2 9 12
5. Pneumonia 1 3 5 9
6. Malaria & Dengue 1 3 0 4
7. Scrub typhus 1 3 4
8. Liver abscess 1 1 2
9. Urinary tract
infection 1 4 5 4 14
10. Enteric fever 1 1 3 5
11. Dengue & Scrub
typhus 3 3
12. Bacterial
meningitis 2 2 4
13. Influenza 3 0 0 0 3
Total 13 35 45 7
Age group of 41-60 constituted the most common age group
in our study forming about 42% of total cases studied.

51
TABLE - 4
FEVER DURATION AND DISEASE DISTRIBUTION
Sl.
No. Disease
<5
days
5-10
days
11-30
days
>30
days Total
1. Malaria 3 2 1 0 6
2. Dengue 3 27 2 0 32
3. Leptospirosis 0 2 0 02
4. Tuberculosis 9 3 0 12
5. Pneumonia 3 4 2 0 9
6. Malaria &
Dengue
3 1 0 4
7. Scrub typhus 4 0 4
8. Liver abscess 0 2 0 2
9. Urinary tract
infection
3 10 1 0 14
10. Enteric fever 5 0 5
11. Dengue & Scrub
typhus
3 3
12. Bacterial
meningitis
2 2 0 4
13. Influenza 2 1 0 3
Tota
l
14 70 16 0
Most cases were admitted with fever durations of 5 - 10 days, forming
70% of cases.
52
MALARIA
- 50% had fever less than 5 days
- 33% were male
- 33% were within 40 yrs. of age
- Total cases : 6
Plasmodium vivax: 4 cases
Plasmodium falciparum : 2
cases
Survived : 6 cases
Died : 0 cases
53
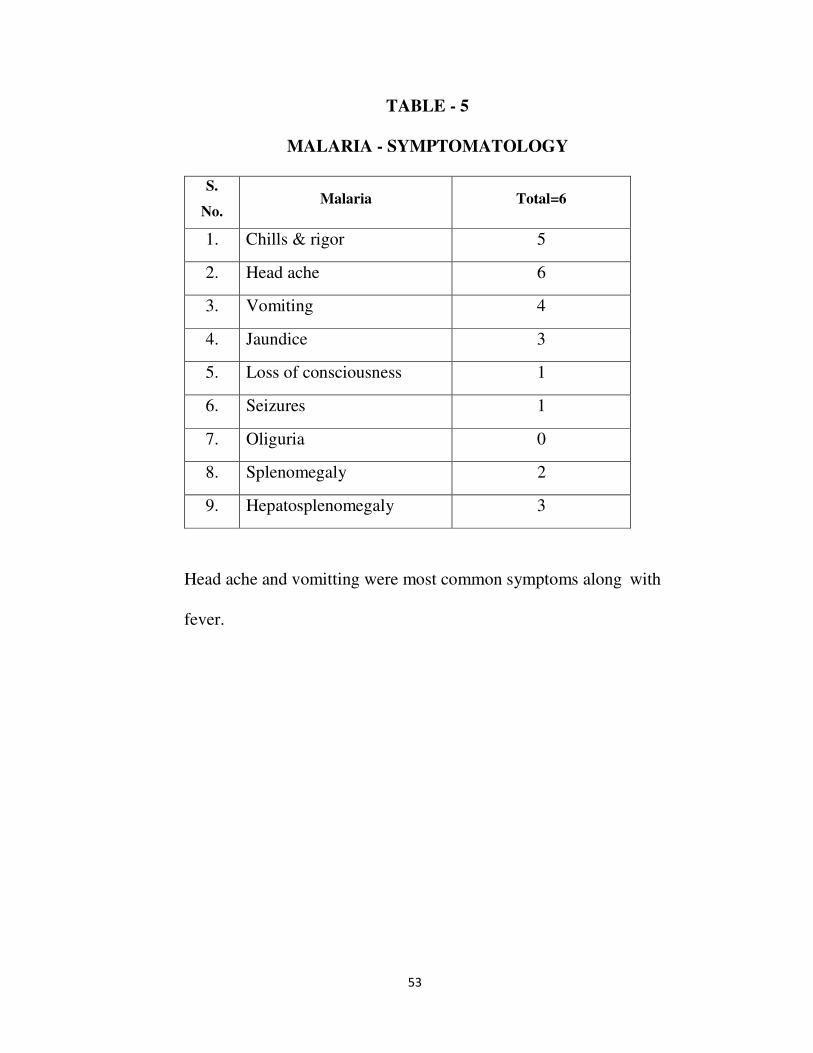
TABLE - 5
MALARIA - SYMPTOMATOLOGY
S.
No. Malaria Total=6
1. Chills & rigor 5
2. Head ache 6
3. Vomiting 4
4. Jaundice 3
5. Loss of consciousness 1
6. Seizures 1
7. Oliguria 0
8. Splenomegaly 2
9. Hepatosplenomegaly 3
Head ache and vomitting were most common symptoms along with
fever.
54
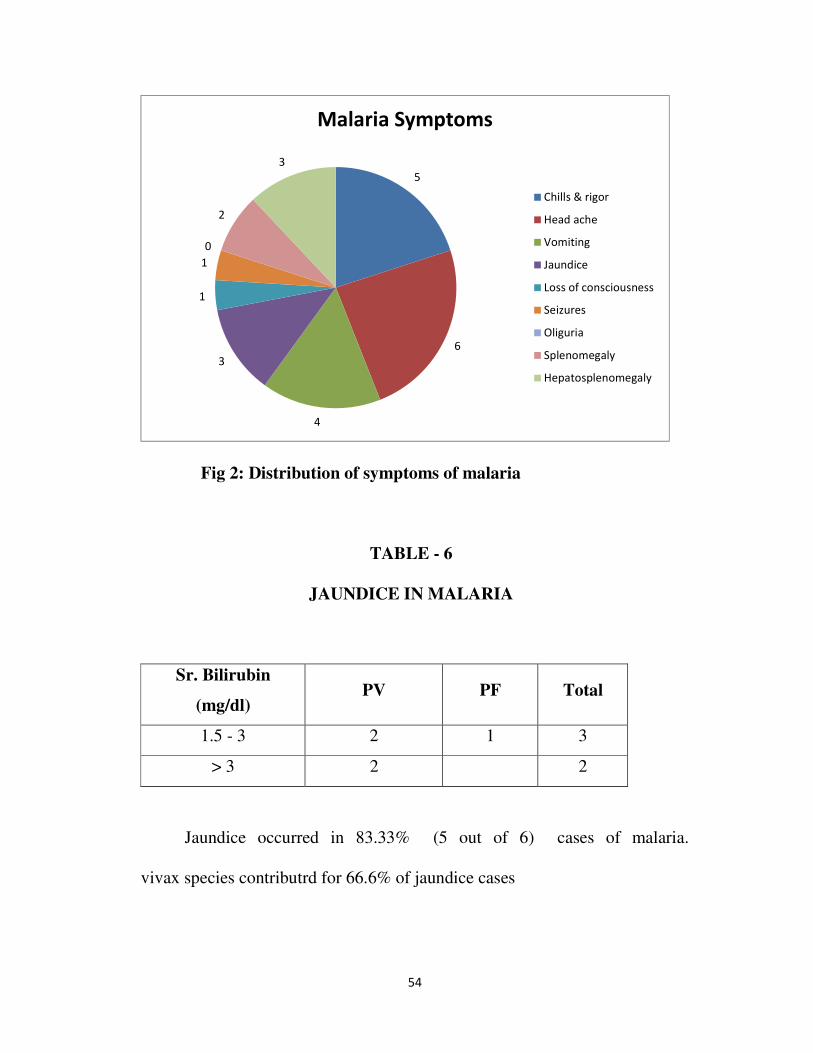
Fig 2: Distribution of symptoms of malaria
TABLE - 6
JAUNDICE IN MALARIA
Sr. Bilirubin
(mg/dl) PV PF Total
1.5 - 3 2 1 3
> 3 2 2
Jaundice occurred in 83.33% (5 out of 6) cases of malaria.
vivax species contributrd for 66.6% of jaundice cases
5
6
4
3
1
1
0
2
3
Malaria Symptoms
Chills & rigor
Head ache
Vomiting
Jaundice
Loss of consciousness
Seizures
Oliguria
Splenomegaly
Hepatosplenomegaly
55
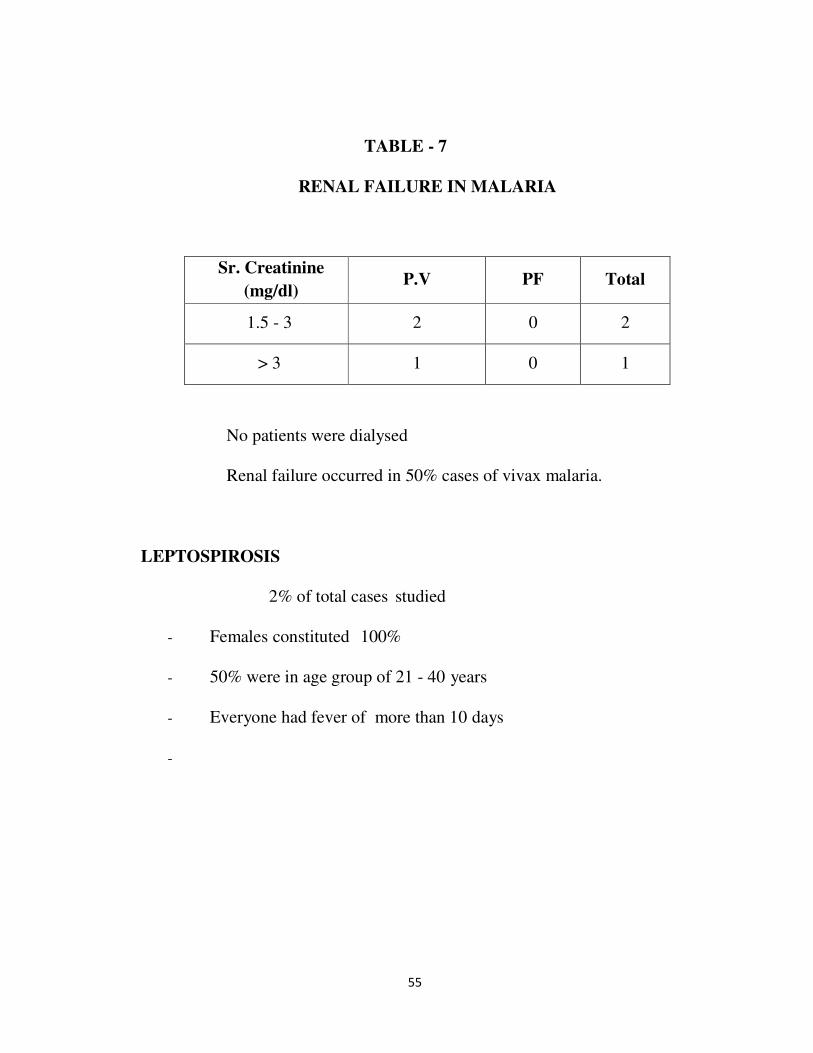
TABLE - 7
RENAL FAILURE IN MALARIA
Sr. Creatinine
(mg/dl) P.V PF Total
1.5 - 3 2 0 2
> 3 1 0 1
No patients were dialysed
Renal failure occurred in 50% cases of vivax malaria.
LEPTOSPIROSIS
2% of total cases studied
- Females constituted 100%
- 50% were in age group of 21 - 40 years
- Everyone had fever of more than 10 days
-
56
TABLE - 8
LEPTOSPIROSIS - SYMPTOMATOLOGY
Symptom Total Male Female
Myalgia - 1
Conj. Suffusion - 1
Jaundice -
Oliguria -
Myalgia and conjunctival suffusion were the most common
symptoms along with fever.
TABLE – 9
LEPTOSPIROSIS - TOTAL BILIRUBIN
Sr. Bilirubin
(mg/dl)
No. of
cases
1.5 - 3 1
> 3.0 0
Total 1 (50%)
About 50% of leptospirosis patients had icteric hepatitis.
57
TABLE - 10
LEPTOSPIROSIS – CREATININE
Sr.Creatinine
(mg/dl)
No. of
cases
1.5 - 3 0
> 3.0 0
Total
No cases of leptospirosis had renal failure TUBERCULOSIS
- 12% of cases contributed for Tb
- 75% had fever for less than 30 days
- 58.3% were females and 75% belongs to 41-60 age group
TABLE - 11
ORGAN WISE DISTRIBUTION AMONG
TUBERCULOSIS PATIENTS
Organ M F Total
Pulmonary 3 4 7 (58.4)
Pleural.effussion 2 2 4
Lymphadenitis 0 1 1
5 7 12
58.3% of the cases were pulmonary tuberculosis among total tuberculosis
cases.
58
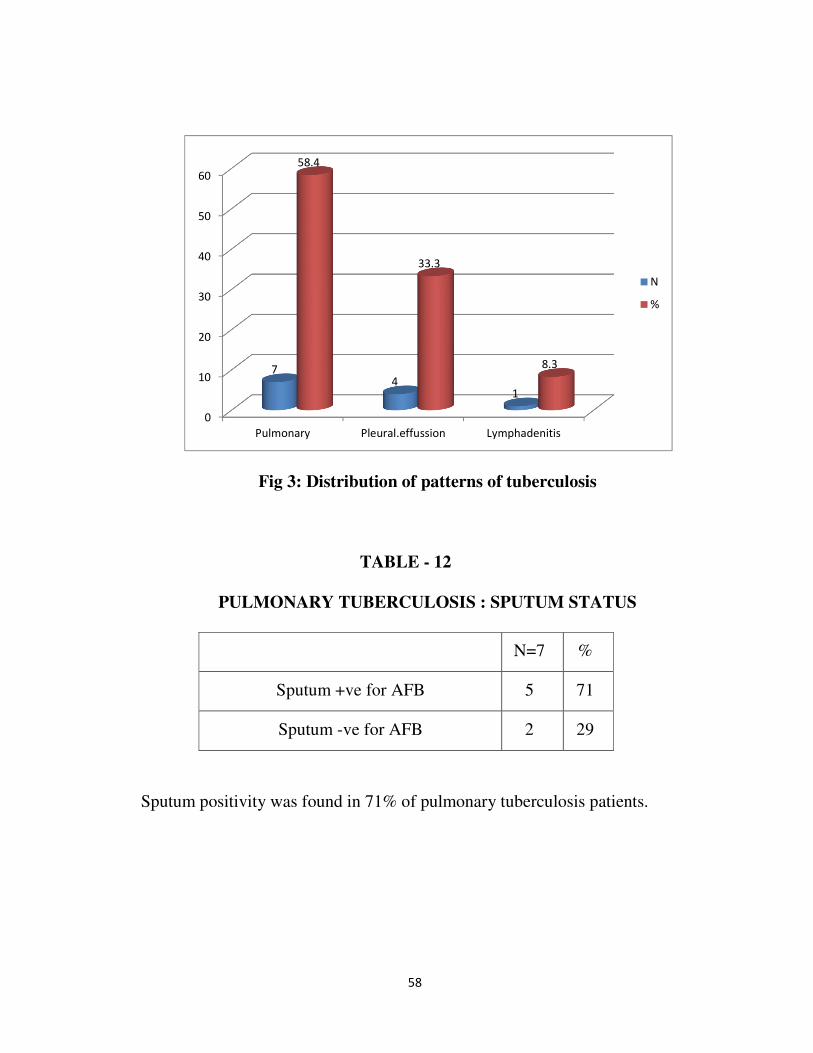
Fig 3: Distribution of patterns of tuberculosis
TABLE - 12
PULMONARY TUBERCULOSIS : SPUTUM STATUS
N=7 %
Sputum +ve for AFB 5 71
Sputum -ve for AFB 2 29
Sputum positivity was found in 71% of pulmonary tuberculosis patients.
0
10
20
30
40
50
60
Pulmonary Pleural.effussion Lymphadenitis
74
1
58.4
33.3
8.3
N
%

59
Fig 4: Distribution of sputum for AFB in my study subjects
TABLE - 13
PULMONARY TUBERCULOSIS - SYMPTOMATOLOGY
Symptom Total (7)
Cough with sputum 6
Breathlessness 3
Loss of weight and loss of
appetite 4
Haemoptysis 2
Sputum production was present in 85.8% of pulmonary
tuberculosis patients.
5
2
sputum for AFB
Positive
Negative

60
Fig 5: Distribution of symptoms of pulmonary tuberculosis
TABLE - 14
SIGNS - CREPITATIONS
Lobe No. Percenta
ge
Unilateral upper
lobe 8 66.6
Bilateral upper
lobe 3 25
Lower lobe 1 8.3
Total
Unilateral upper lobe crepitations were common.
0
10
20
30
40
50
60
70
80
90
Cough with
sputum
Breathlessness Loss of weight
and loss of
appetite
Haemoptysis
63 4 2
85.7
50
57.1
28.5
Number
Percent
61
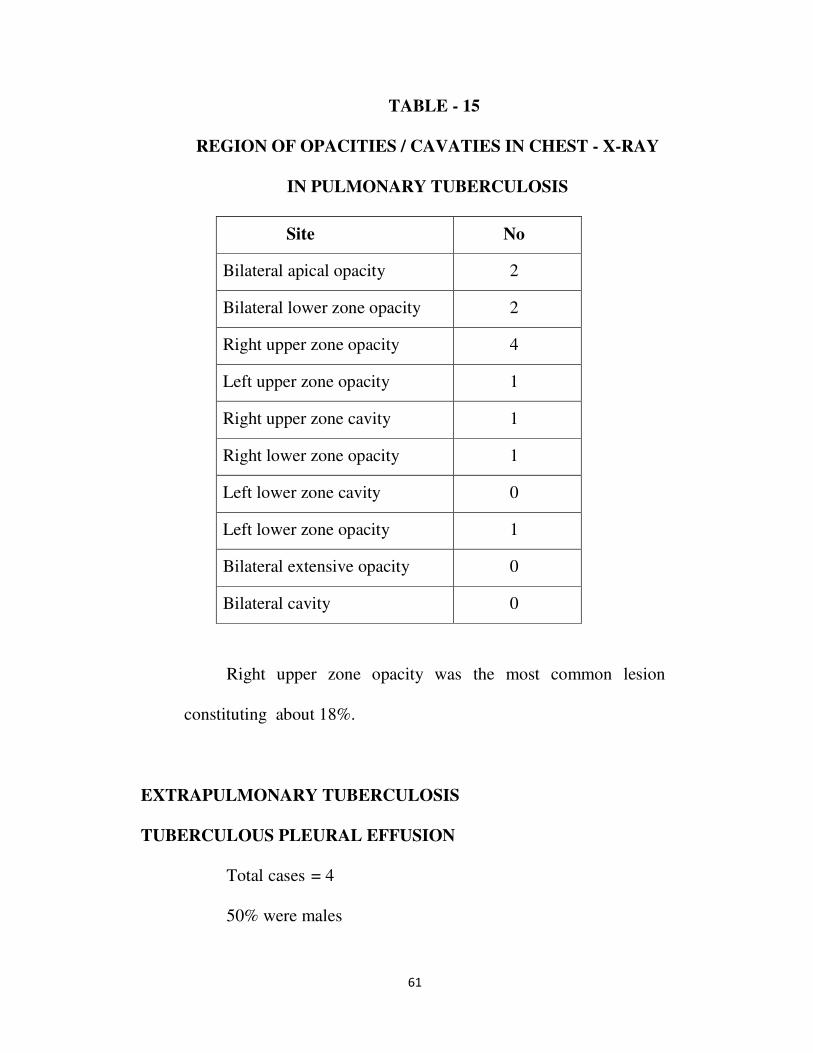
TABLE - 15
REGION OF OPACITIES / CAVATIES IN CHEST - X-RAY
IN PULMONARY TUBERCULOSIS
Site No
Bilateral apical opacity 2
Bilateral lower zone opacity 2
Right upper zone opacity 4
Left upper zone opacity 1
Right upper zone cavity 1
Right lower zone opacity 1
Left lower zone cavity 0
Left lower zone opacity 1
Bilateral extensive opacity 0
Bilateral cavity 0
Right upper zone opacity was the most common lesion
constituting about 18%.
EXTRAPULMONARY TUBERCULOSIS
TUBERCULOUS PLEURAL EFFUSION
Total cases = 4
50% were males

62
TABLE - 16
SYMPTOMATOLOGY IN TUBERCULOUS PLEURAL
EFFUSION
Symptoms No (%)
Cough with sputum 2 (50)
Loss of weight and
appetite 3 (75%)
Chest pain 1 (25)
Loss of weight and appetite were the most common symptoms
occurring in 75% of the cases.
TUBERCULOUS LYMPHADENITIS
1 Cases
- Had cervical lymphadenopathy with low grade fever
PNEUMONIA
Total Cases – 9
66, 6% were male
44.4% had fever for 5- 10 days
55.5% were in age group 40 - 60 years
63
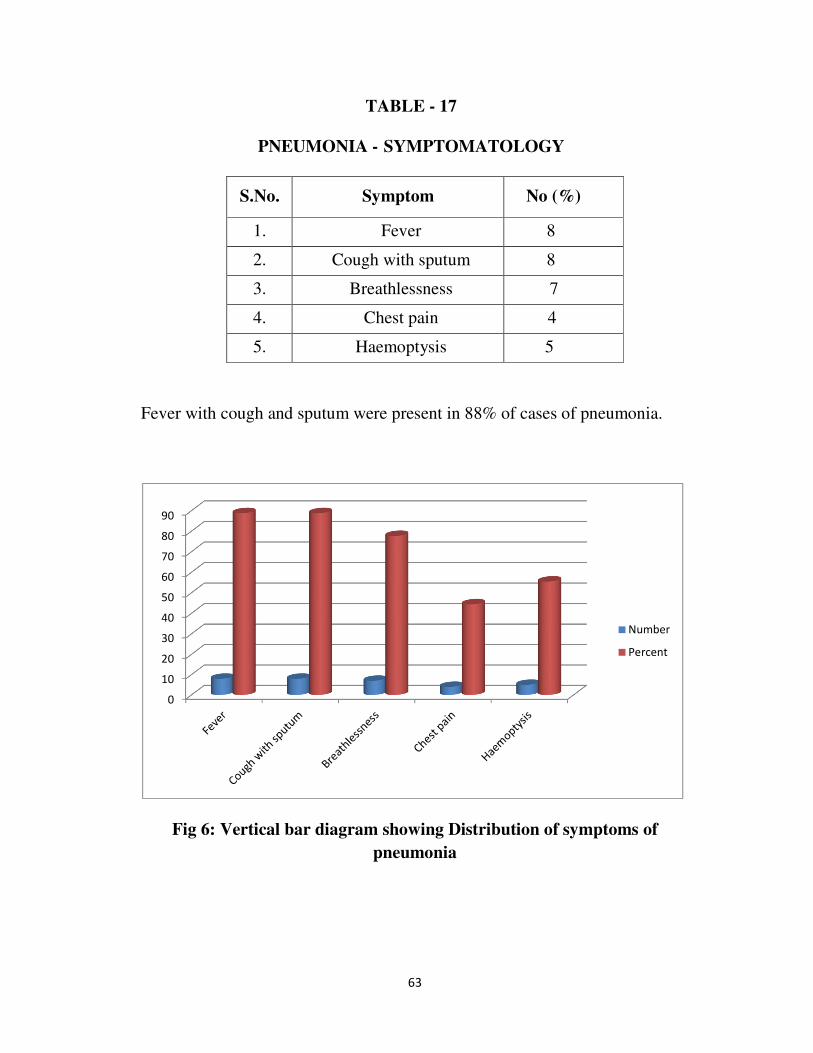
TABLE - 17
PNEUMONIA - SYMPTOMATOLOGY
S.No. Symptom No (%)
1. Fever 8
2. Cough with sputum 8
3. Breathlessness 7
4. Chest pain 4
5. Haemoptysis 5
Fever with cough and sputum were present in 88% of cases of pneumonia.
Fig 6: Vertical bar diagram showing Distribution of symptoms of
pneumonia
0
10
20
30
40
50
60
70
80
90
Number
Percent

64
TABLE - 18
PNEUMONIA - BACTERIOLOGICAL PROFILE
Sl.No. Organism No. (%)
1. K.pneumoniae 2 (22.2)
2. S.pneumonia 5(55.5)
3. E.Coli 1 (11.1)
4. S.aureus 1 (11.1)
Total 9
S. Pneumonia was the most common organism isolated constituting about
55.5% of isolates.
Fig 7: Distribution of bacteriological profile of pneumonia
2
5
1
1
Organism
K.pneumoniae
S.pneumonia
E.Coli
S.aureus
65
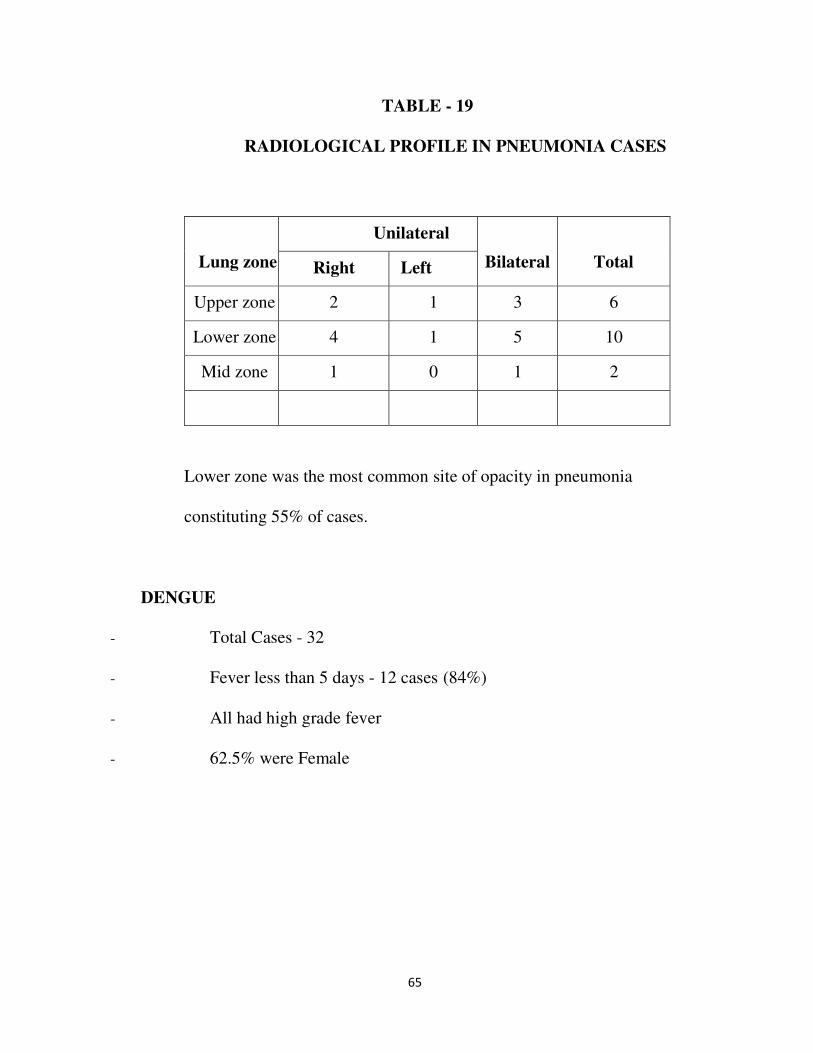
TABLE - 19
RADIOLOGICAL PROFILE IN PNEUMONIA CASES
Lung zone
Unilateral
Bilateral
Total Right Left
Upper zone 2 1 3 6
Lower zone 4 1 5 10
Mid zone 1 0 1 2
Lower zone was the most common site of opacity in pneumonia
constituting 55% of cases.
DENGUE
- Total Cases - 32
- Fever less than 5 days - 12 cases (84%)
- All had high grade fever
- 62.5% were Female
66
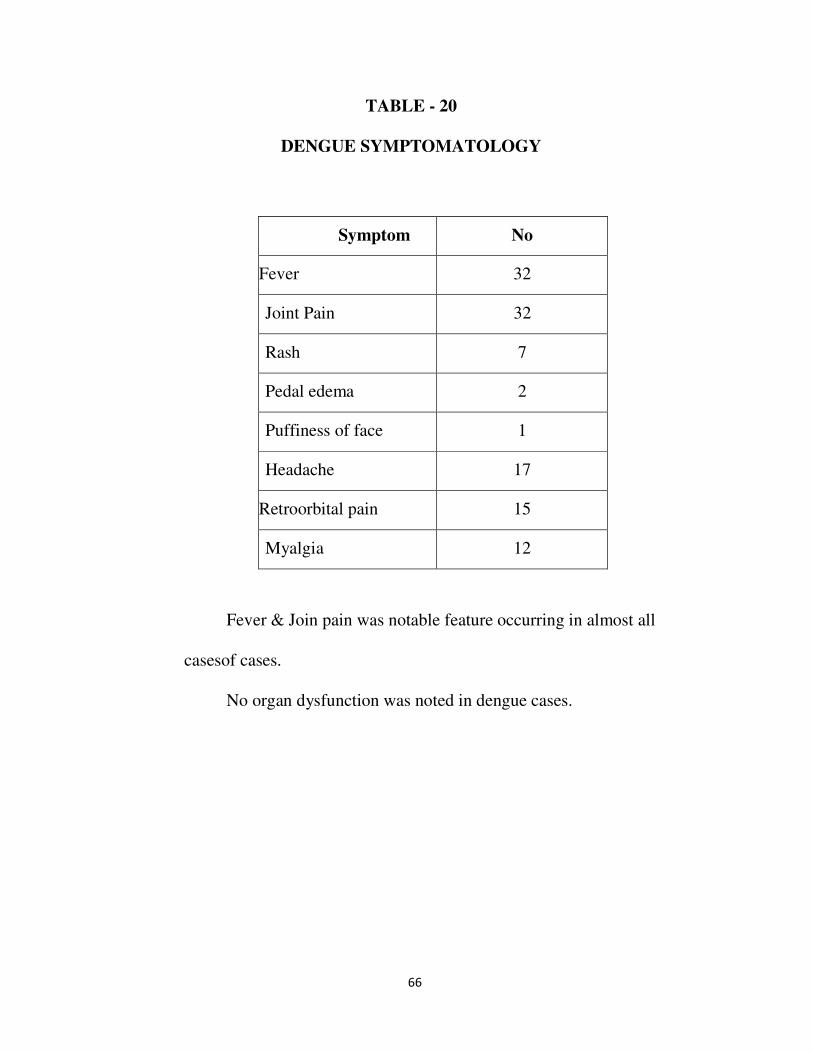
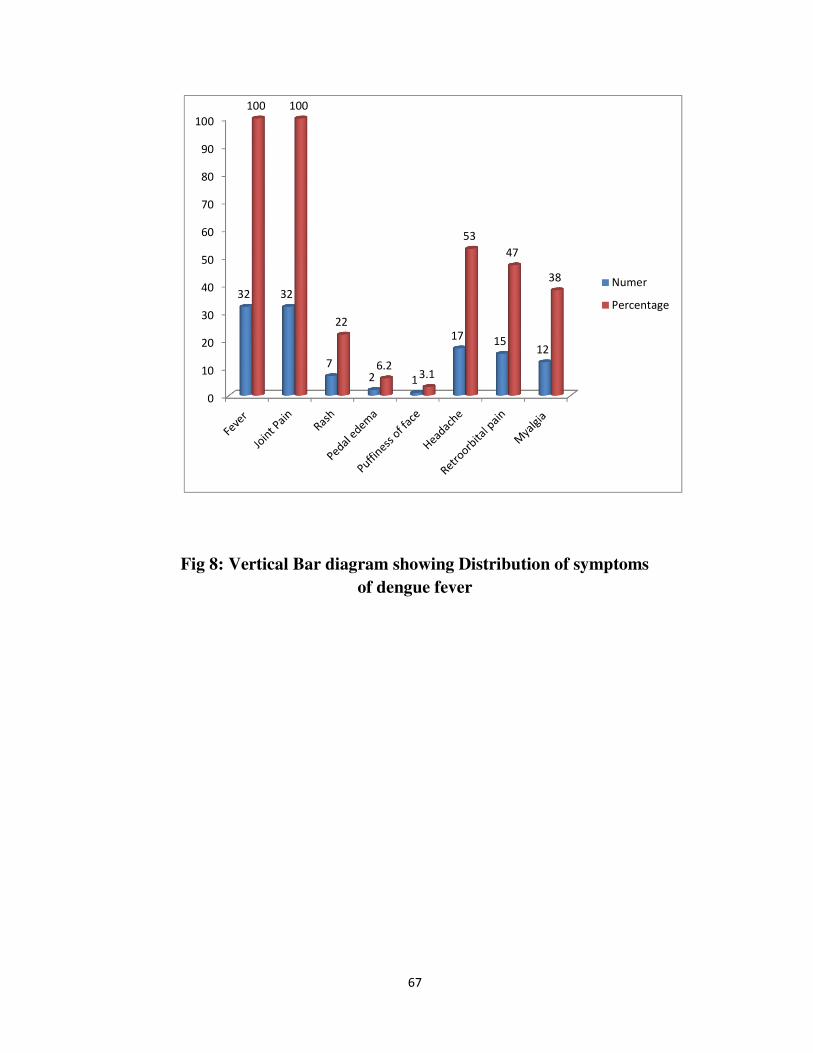
TABLE - 20
DENGUE SYMPTOMATOLOGY
Symptom No
Fever 32
Joint Pain 32
Rash 7
Pedal edema 2
Puffiness of face 1
Headache 17
Retroorbital pain 15
Myalgia 12
Fever & Join pain was notable feature occurring in almost all
casesof cases.
No organ dysfunction was noted in dengue cases.
67
Fig 8: Vertical Bar diagram showing Distribution of symptoms
of dengue fever
0
10
20
30
40
50
60
70
80
90
100
32 32
7
2 1
1715
12
100 100
22
6.23.1
53
47
38 Numer
Percentage
68
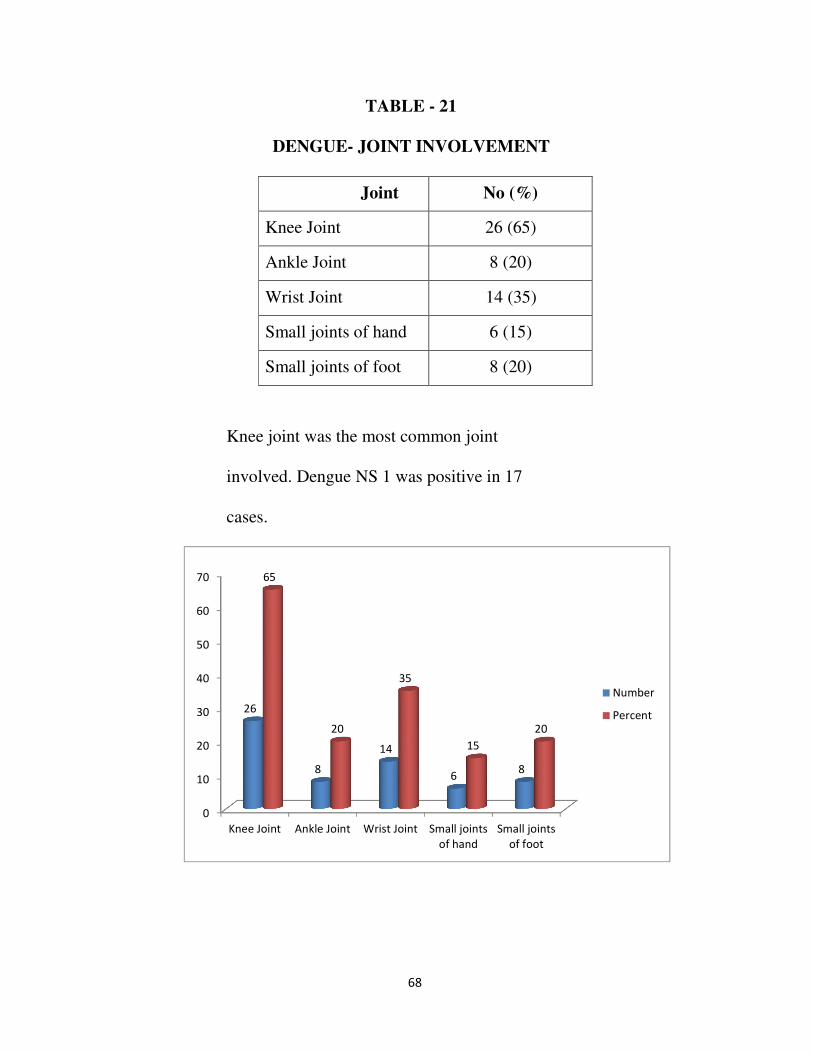
TABLE - 21
DENGUE- JOINT INVOLVEMENT
Joint No (%)
Knee Joint 26 (65)
Ankle Joint 8 (20)
Wrist Joint 14 (35)
Small joints of hand 6 (15)
Small joints of foot 8 (20)
Knee joint was the most common joint
involved. Dengue NS 1 was positive in 17
cases.
0
10
20
30
40
50
60
70
Knee Joint Ankle Joint Wrist Joint Small joints
of hand
Small joints
of foot
26
8
14
68
65
20
35
15
20
Number
Percent
69
LIVER ABSCESS
- Total Cases – 2
- Solitary abscess was present in 50% cases
- All of them had uncomplicated course
- 50% cases were managed conservatively and in 50% ultrasound
guided aspiration of the fluid was done.
BACTERIAL MENINGITIS
- Total Cases - 4
- Males were 50%
- 50% had fever 5 to 10 days
- All had meningeal signs
- 1 patient had features of raised intracranial tension
URINARY TRACT INFECTION
- Total Cases - 14
- 64% were females
- 50% had E.coli and 50% had klebsiella grown in culture
- Most common group was 20 - 40 yrs.
- All of them responded to ciprofloxacin and cefotaxim.
70
SCRUB TYPHUS FEVER
- Total Cases - 4
- Most of them were in age group of 41-60
- All of them had fever with rash
ORGAN DYSFUNCTION IN FEVER CASES
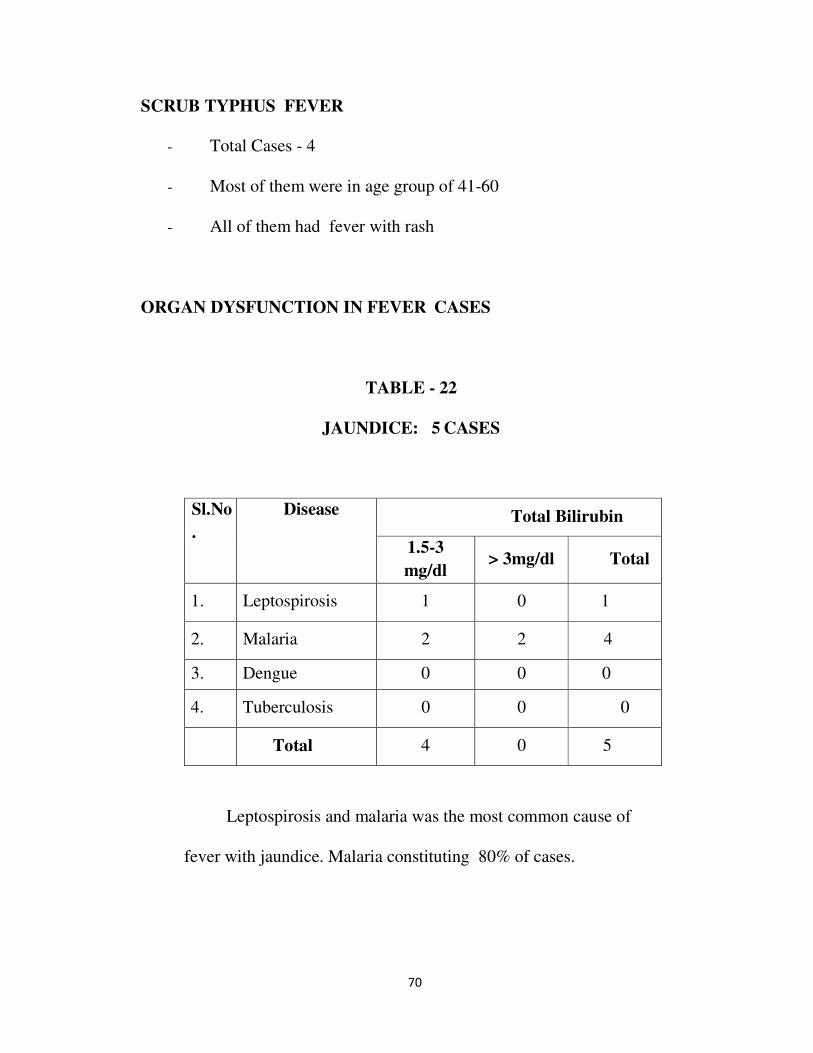
TABLE - 22
JAUNDICE: 5 CASES
Sl.No
.
Disease Total Bilirubin
1.5-3
mg/dl > 3mg/dl Total
1. Leptospirosis 1 0 1
2. Malaria 2 2 4
3. Dengue 0 0 0
4. Tuberculosis 0 0 0
Total 4 0 5
Leptospirosis and malaria was the most common cause of
fever with jaundice. Malaria constituting 80% of cases.
71
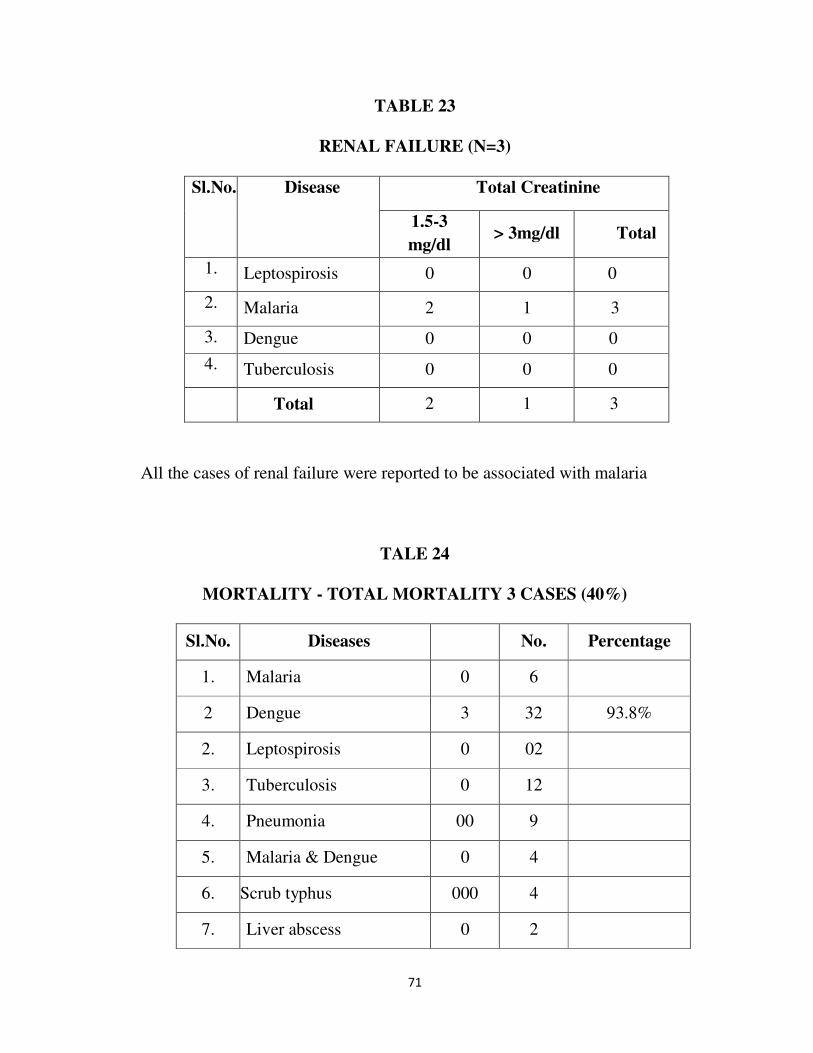
TABLE 23
RENAL FAILURE (N=3)
Sl.No. Disease Total Creatinine
1.5-3
mg/dl > 3mg/dl Total
1. Leptospirosis 0 0 0
2. Malaria 2 1 3
3. Dengue 0 0 0
4. Tuberculosis 0 0 0
Total 2 1 3
All the cases of renal failure were reported to be associated with malaria
TALE 24
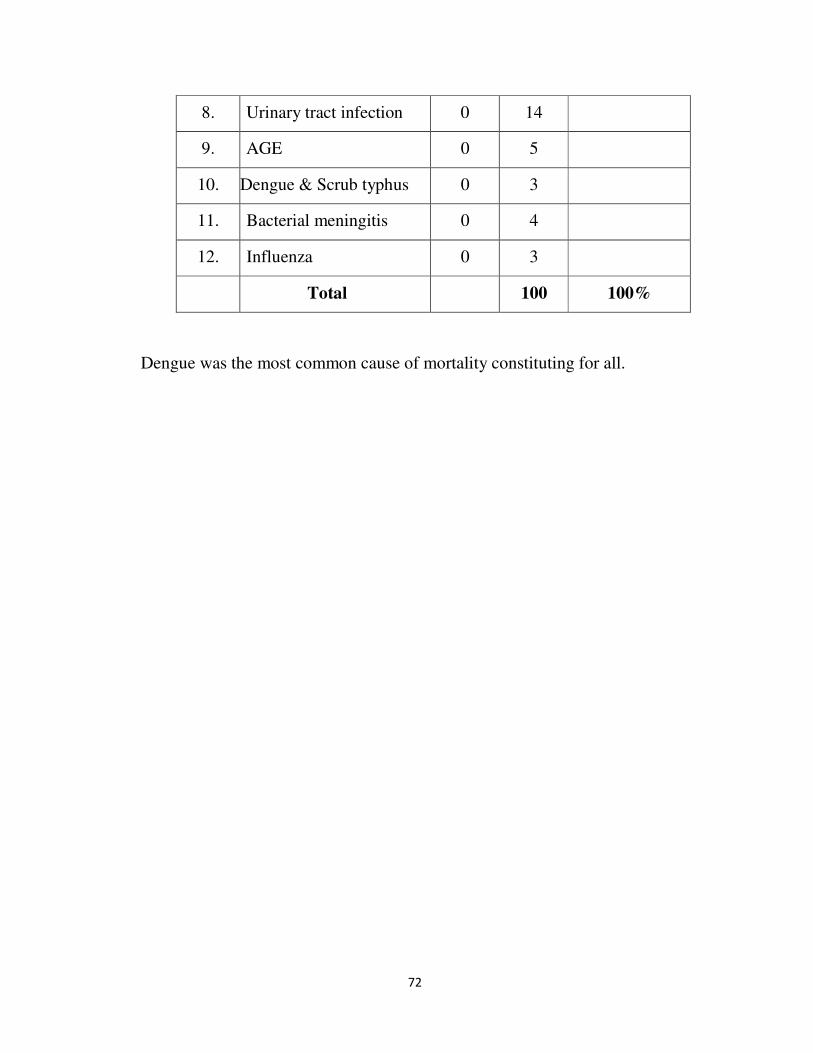
MORTALITY - TOTAL MORTALITY 3 CASES (40%)
Sl.No. Diseases No. Percentage
1. Malaria 0 6
2 Dengue 3 32 93.8%
2. Leptospirosis 0 02
3. Tuberculosis 0 12
4. Pneumonia 00 9
5. Malaria & Dengue 0 4
6. Scrub typhus 000 4
7. Liver abscess 0 2
72
8. Urinary tract infection 0 14
9. AGE 0 5
10. Dengue & Scrub typhus 0 3
11. Bacterial meningitis 0 4
12. Influenza 0 3
Total 100 100%
Dengue was the most common cause of mortality constituting for all.
73
DISCUSSION
100 patients, both male and female fulfilled the entry criteria and were
included in the study. The patients were clinically examined and investigated
following which all cases were diagnosed. However fever subsided in most
undiagnosed cases after empiric antimalarial and antibiotic therapy.
Among the total cases dengue was the major contributor forming 32%
of cases, followed by UTI 12% and tuberculosis (12%). Pneumonia formed
9%, co-infection with malaria and dengue formed 4%, liver abscess - 2%,
malaria 6%, enteric fever - 1%, scrup typhus - 4%, influenza - 3% and
bacterial meningitis - 4% (Table - 1).
74
COMPARISION WITH OTHER STUDIES OF INFECTIOUS FEVERS
Similar study on clinical profile of infections fevers was carried out in
Chennai in which there were more undiagnosed fevers9.
The increased numbers of diagnosed cases in the present study (100%)
in comparsion to previous study (54%) is probably due to increased
diagnostic facilities
Among the diagnosed cases number of malaria cases diagnosed in
present study was 6% while it was 12.8% in the previous study. The incidence
of malaria is due to use of peripheral smear and quantitative buffy coat method
which was carried out at malaria laboratory of Chennai Corporation..
Leptospirosis is diagnosed in the present study was 2% less than the
previous study (8.2%) due to awareness of the disease and picking up of
anicteric leptospirosis and increased diagnostic facilities for doing slide
agglutination test.
Scrub typhus fever which was not present in the previous study was
picked up in the present study due to the wide spread epidemic which
occurred from July 2018 - December 2018.
The incidence of other causes of fever are more or less the same.
A similar study on etiological profile of fever was carried out in
Thailand between 1999 - 2002, the results of which are similar to our study.
Malaria constituted 25% of diagnosed cases in their study, whereas in our
75
study it was 31%; leptospirosis was about 17%, in our study it constituted
19% of cases10.
MALARIA
Malaria was contributing for 6% of the total cases studied, which
amounted to 6 cases. Plasmodium vivax occurred in 4 (67%) cases,
Plasmodium falciparum occurred in 2(33%) cases and mixed infection is
nil. Hazara et al.,49 from calcutta has reported 73.3% PV and 26.7% PF in
their study of 225 cases. Tamil Nadu is in low risk category with regard to
Plasmodium falciparum infection.
CLINICAL FEATURES
In malaria, all 6 (100%) patients had fever. Typical paroxysms
occurred in very few patients. Fever was associated in 83% cases with chills,
in 83% head ache was severe and consistently associated with fever (Table
- 5). Mohapatra et al.,16 from Orissa reported migrainous head ache of 4.5%
in a study of 110 cases of vivax malaria.
CEREBRAL MALARIA
Cerebral malaria was a not a common complication noted in our study.
Omly 2 patients (33.3%) had neurological dysfunction in the form of altered
76
sensorium, loss of consciousness and generalized convulsions. 1 patients
(16%) had loss of consciousness. 1 (16%) had convulsions. (Table-5) .
Kochar50 reported generalised convulsion in 21.31% of 441 cases of cerebral
malaria from Rajasthan. 3 patients died of cerebral malaria all of which were
caused by Pl.vivax. Cerebral malaria was associated with DIC in one case
and one case was associated with jaumidce.
JAUNDICE
Jaundice occurred in 5(83%) cases when the serum bilirubin cut off of
more than 1.5 was taken. As per WHO criteria serum bilirubin of more than
3 mg% occurred in 2 cases (33%) (Table - 6). Bilirubinemia was
predominantly direct, with only slight elevation of transaminases.
It occurred in 26.6% cases of falciparum malaria and 8.33% cases of
vivax malaria. Hazara et al.,49 reported jaundice in 9.09% of PV cases and
40% of PF cases. Harris VK et al., from South India reported 37% of
jaundice in PF cases50. Kochar et al., from Rajasthan has reported jaundice
in 58.85% of PF cases in 200151.
RENAL FAILURE
Acute renal failure occurred in 3 (50%) cases. As per WHO criteria
severe renal failure occurred only in 1 (16) % of cases and all the cases were
77
due to PV (Table - 7). In our study it has been found that renal failure also
occurs in PV in significant numbers. This has been proved by kochar in his
study of 11 cases of complicated vivax malaria by documenting the presence
of PV and absence of PF by PCR study19. No patient was dialysed in our
study. In India reported incidence of ARF in Malaria is 17.8% from Delhi,
17.2% from Orissa, 13% from North East India and 5.9% from Mumbai52.
Madhu Muddaiah from Mangalore reported renal failure in 11.57% of
190 cases studied in 2002 - 200415.
TREATMENT
Cases of plasmodium vivax malaria with organ dysfunction like
jaundice, renal failure and cerebral malaria was treated with quinine and
other cases were treated with chloroquine. Among the cases treated with
chloroquine 1 (16%) showed chloroquine resistance while Chowta et al.,17
noted chloroquine resistance in 16% of the cases.
MORTALITY
There were no deaths in malaria.
78
LEPTOSPIROSIS
Leptospirosis contributed to 2% of total cases studied. All were
females 100%. Majority were in the age group of 21 - 40 years. Anicteric
leptospirosis was about 50% while icteric leptospirosis formed 50% of cases.
All of them were diagnosed using macroscopic slide agglutination > 2+
along with modified Faine's score of more than 25. Duration of fever was
more than 5 days in 80% cases.
In our study no patients had renal failure while it was 79%
(Muthusethupathi et al.,)54 and 49% (Edward et al.,)53 in other studies.
The decreased renal failure in present study is probably due to decreased
prevalence of serogroup autumnalis.
50% of patients had bilirubin of >1.5 mg/dl while it was 83%
(Muthusethupathi et al.,)54 95% (Edward et al.,)53 and 28% (Gendron
et al.,)55 in other studies.
All patients recovered with doxycycline and patients who had
complication was treated with crystalline penicillin. No mortality in
leptospirosis.
CO-INFECTION OF MALARIA AND DENGUE
A total of 4(4%) patients had co-infection with both malaria and
dengue. Similar study on fever profile conducted in Thailand showed a co-
79
infection of 5.5%10. An important observation was that of co- infection
patients had jaundice and renal failure.
TUBERCULOSIS
Tuberculosis was the third major contributor in our study constituting
12% of cases.
* 75% had fever for 5-10 days
* 41.7% were males and 58.3% females
* Pulmonary tuberculosis contributed 58.3% cases with
extrapulmonary TB forming 42.7% cases.
The contribution of tuberculosis was 54% (Sharma et al.,)7, 45%
(Agarwal)35 and 54% (Dhawan et al.,)34 in other studies.
PULMONARY TUBERCULOSIS
* Total - 7 cases
* Males constituted 43% and females 57%.
Among pulmonary tuberculosis, other symptoms along with fever was
sputum which was present in 6 cases (85.88%). Samal et al.,27 reported
cough with expectoration in 92.7% of pulmonary tuberculosis cases.
Haemoptysis was present in 25.5% while Samal et al.,27 reported in 20.3%
cases. Breathlessness was a complaint in 70.2% cases (Table - 13).

80
The most common radiological finding was unilateral upper zone
opacity (66.6%), while Samal et al.,27 most commonly reported bilateral
scattered opacities in all zones in 77.5% cases.
Sputum AFB positivity was present in 41.6% of cases while
Dehankar et al.,28 reported sputum positivity in 42.34%.
EXTRAPULMONARY TUBERCULOSIS
Tuberculous pleural effusion formed 33.3% of tuberculosis cases.
Most (50%) were male. Fever duration in maximum number of patients
between 5-10. Majority of them (56.25%) were in age group of 20 - 40 years.
Next to fever chest pain was the most common symptom.
The other groups of extra pulmonary TB which constituted a minority
was 1 cases of TB lymphadenopathy.
PNEUMONIA
Pneumonia formed significant number of cases in our study. It
constituted about 9% (9 cases). Majority (66.6%) were male. Majority had
fever of 5 - 10 days (44.4%).
Etiological diagnosis was obtained in 68.2% while Bansal et al.,
obtained etiological diagnosis in 75% of cases29.
81
Patients older than 40 years were more predisposed as in the study by
Bansal et al29. Cough with expectoration was present in 100% while
Narendra et al.,43 reported cough in 97.6%. In our study 77% had
breathlessness 44.4% had chest pain (Table - 17). Most of the organisms
isolated from the present study was s.pneumoniae and sensitive to
ciprofloxacin and gentamycin (Table - 18). Similar to study done in North
American studies44 in which S.pneumoniae was most common.
DENGUE
32% of cases in our study were due to Dengue fever. All of them had
polyarthralgia with majority involving the knee joint (81%) and small
joints of the hand (19%) (Table -21). Majority (84%) had fever less than 5
days duration. Headache 53.1% and retroorbital pain 47% were next most
common symptom followed by rash and myalgia. In the cases fever subsided
with antipyretics though there was prolonged joint pain.
LIVER ABSCESS
Liver abscess formed 2% of total cases. Most (75%) had fever of 5-
10 days; with females forming all cases. 50% were in the age group of 20 -
40 years.
82
Abdominal pain (100%) was the most common symptom along with
fever. Diagnosis was confirmed by ultrasonography.
50% cases was managed conservatively while 50% of cases were
aspirated with ultrasonogram guidance.
URINARY TRACT INFECTION
UTI formed 14% of total cases. Diagnosis was based on
symptomatology and urine culture. 60% were females. E.coli (50%) was the
most common organism and none of them had complications.
SCRUB TYPHUS FEVER
Scrub typhus formed 4% of cases.50% were males and all were more
than 40 years old.
ENTERIC FEVER
Enteric fever was present in 5% of cases all had fever more than 5
days. 80% were female. Along with fever headache, vomiting and diffuse
abdominal pain, splenomegaly was present in 40% of cases. Blood widal
was positive in 100% of cases.
40% of patients responded to ciprofloxacin, while 60% of patients
who did not respond to ciprofloxacin was treated with ceftriaxione. 1 had

83
(20%) elevated creatinine at admission which recovered after treatment.
BACTERIAL MENINGITIS
Bacterial meningitis cases were 4 (4%) in our study. 2 (50%) had
altered sensorium and none had seizures, while seizures was reported in 30%
by Pomeroy et al.,32 100% had neck stiffness and Kernigs Sign. 1 had
bilateral sixth nerve palsy. CSF examination showed predominant
polymorphs and Gram stain was negative in all the three. All had low sugar
and high protein and showed clinical improvement when cefotaxim 2 gm
was used.
ORGAN DYSFUNCTION IN FEVER CASES JAUNDICE
Of the total patients studied 3 patients (3%) had raised bilirubin of >1.5
mg %. Of these 2% (2 cases) had bilirubin >3 mg%. Of the total leptospirosis
constituted 20% of cases , and malaria 80% of cases (Table - 22).
84
RENAL FAILURE
Renal failure with creatinine >1.5 mg/dl was present in 75% (2 cases),
of which severe renal failure with creatinine >3 mg/dl was present in 25%
of total renal failure cases. Of the total renal failure cases was constituted by
malaria (Table - 17).
MORTALITY
The overall mortality is 3 cases of 100 cases, the most common cause
is dengue constituting for all deaths.

85
SUMMARY
1. 100 patients were analysed, 43% were males and 57% were females.
2. Etiology of febrile illness could be diagnosed in all cases.
3. The common causes of infectious fever were dengue (32%), folloed
by Urinary tract infection 14%, tuberculosis (12%) malaria (6%),
leptospirosis (2%and pneumonia (9%). Other causes were bacterial
meningitis 4% , influenza 3%, liver abscess (2%), scrub typhus (4%)
and enteric fever (5%).
4. Age group of 41-60 constituted the most common age group in our
study forming about 42% of total cases studied.
5. Most cases were admitted with fever durations of 5 - 10 days, forming
70% of cases.
6. Fever & Join pain was notable feature occurring in almost all cases
of cases.
7. No organ dysfunction was noted in dengue cases.
8. Knee joint was the most common joint involved.
9. Dengue NS 1 was positive in 17 cases.
10. Plasmodium vivax formed 67% of malaria cases while plasmodium
falciparum occured in 33%. Head ache and vomitting were most
common symptoms along with fever.
86
11. Common complications of malaria were jaundice and renal failure in
our study
12. In Leptospirosis cases, Myalgia and conjunctival suffocation were the
most common symptoms along with fever.
13. The most common presentation of tuberculosis was pulmonary
tuberculosis (58.3%). Extrapulmonary tuberculosis occured in 41.7%
14. Sputum positivity was found in 71% of pulmonary tuberculosis patients.
15. Sputum production was present in 85.8% of pulmonary tuberculosis
patients followed by breathlessness and loss of weight and appetite .
16. Pneumonia constituted about 9% of cases in our study, Fever with cough
and sputum were present in 88% of cases of pneumonia.
17. S. Pneumonia was the most common organism isolated constituting
about 55.5% of isolates followed by klebsiella
18. Urinary tract infection constituted about 14% cases, among which 50%
had E.coli and 50% had klebsiella grown in culture. All of them
responded to ciprofloxacin and cefotaxim.
19. All 4 cases of scrub typhus presented with fever with rash
20. Co-infection with malaria and dengue occurred in 4 (4%) patients.
21. Jaundice with fever occurred in 5(5%) patients. Leptospirosis
contributed to 20% and malaria to 80%.
22. Fever with renal failure occurred in 3(30%) patients. Malaria
87
contributed to all reported cases
23. Mortality was 3(3%) cases in the study, dengue contributing to all 3
cases

88
BIBLIOGRAPHY
1. Kasper al ed Harrison's principles of internal medicine 16th
edition by The McGraw - Hill companies, 104 - 108.
2. Kejariwal D. Sarkar N, Chakraborthi SK, et al., : Pyrexia of
unknown origin : a prospective study of 100 cases; Journal of
Postgraduate medicine, 2001, Vol.47, page 104 - 107.
3. De Kleijn; FUO - A prospective multicenter study of 167
patients with FUO, using fixed epidemiologic entry criteria.
Medicine 1997; 76; 392 - 400.
4. Peters Dorf; FUO : An old friend revisited. Arch. Int. Med.
1992; 152 - 21.
5. Larson; Diagnosis and followup of 105 FUO cases, Medicine,
1982; 61 : 269.
6. Knockaert; Fever of unkonwn origin in 1980. Arch Int. Med.
1992 : 152: 51
7. Sharma B.K, Kumar. Prolonged and undiagnosed fevers in north
India. Tropical and geographic medicine 1992; 14 : 22 - 6.
8. Burke et al., fever of unknown origin. Inf. Dis. Clin. Nov. 1996;
10;111- 125.

89
9. Shivakumar S, Emmanuel Bhaskar M, Jayachandran R, Sukumar
C; Clinical profile of infectious fevers (non - HIV). A prospective
study of 361 cases; J. Assoc. Phys. India, Vol.51, December 2003,
p.1257.
10. Ruth. D. Ellis, Fukuda M, McDaniel et al, Causes of fever in adults
on the Thai - Myanmar border. Am. J. Trop. Med. Hyg, 74(1),
2006, pp.108- 113.
11. Internet website www.rbm.who.int/wmr.2005. World Malaria
Report, 2005, home page.
12. Malaria site.com; Dr.B.S.Kakkilaya's Malaria website.home
page.
13. N.J.White, Malaria in Manson's Tropical Disease. 21 edition,
Ed. Gc Cook and A Zumla. ELST with Saunders. 2003 : 1205 -
95.
14. Ban sode et al., Clinical profile of malaria at Dr.B.A.M.
Hospital,
J Assoc Phys India, 1994; 42(12) : 1052.
15. Madhu Muddaiah and P.S.Prakash; A study of clinical profile of
malaria in a tertiary referral centre in South Canara; J. Vect. Borne
Dis. 43, March 2006, pp.29-33.
90
16. Mohapatra MK, Padhiary KN, Mishra DP et al., Atypical
Manifestations of Plasmodium Vivax Malaria. Indian J.
Malariol, 2002 : 391 (1-2) : 18- 25.
17. Chowta MN; Study of clinical profile of malaria at KMC
Hospital, Attavar, India. Journal of Clinical and Diagnostic
Research, 2007 June; 1 (3) : 110 - 115.
18. D.K.Kochar S.K.Kochar; Malaria in India; 62nd Annual
Conference of Association of Physicians of India, 2007,
Medicine update. Vol.(17), Page 645.
19. Kochar DK, Saxena V, Singh N et al., Plasmodium vivax
malaria,
Emerg Infect. Dis. 2005, 11(1); 132 - 4.
20. S.Shivakumar: Approach to Leptospirosis in India;
Ed.Battacharya,
Medicine update; Assam 2003; 699-703.
21. M.A.Muthusethupathi, S.Shivakumar; Leptospirosis in Madras,
India - A study of 206 cases (1987 - 95); First Meeting of the
International Leptospirosis Society, Nantes (France) 9 - 13
September 1996.
22. Sumathi G. Chinari Pradeep KS, Vimala Ranga Rao G,
Shivakumar S. - A three year experience in serodiagnosis of

91
leptospirosis (1995 - 1997); Indian J Med. Microbiol, (1999),
17(1) : 50 - 51.
23. Shivakumar S. : Leptospirosis in Chennai - Changing Clinical
Profile. J Assoc Phys. India. Vol.54, December 2006, 964 - 965.
24. M.A. Muthusethupathi, S. Shivakumar, R. Suguna;
Leptospirosis in Madras. A clinical and serological study. J.
Assoc. Phys. India, 1995, Vol.43, No.7, 456 - 458.
25. Leucour ; Human Leptospirosis - A review of 50 cases.
Infection 17 :8 - 12.
26. TB India 2007, RNTCP Status report : Central TB division,
Directorate General of Health Services: page. 10.
27. Samal; Pattern of Pulm. Tuberculosis in Adults in Western
Orissa. J. Assoc. Phys. India, 1990; 38(1) : 14,
28. Dehankar; Incidence of pulmonary tuberculosis in lower lung
fields. J. Assoc. Phys. India, 1990; 38(1) : 74.
29. S.Bansal, S. Kashyap, LS Pal and A.Goel; Clinical &
Bacteriological profile of community acquired pneumonia in
Shimla, Himachal Pradesh; Indian J. Chest Dis. Allied Sciences,
2004; 46 : 11 - 22.
92
30. Chowta MN, Chowta NK; Study of Clinical profile and
antibiotic response in typhoid fever : Indian J. Med. Microbiol.
2005; Vol.23, Issue 2, 125 - 127.
31. Yew; Typhoid fever in singapore. A review of 370 cases. J.
Trop. Med. Hyg. 1991; 94 : 352 - 7.
32. Pomeroy et al., Seizures and other neurological sequelae of
Bacterial meningitis in Children, N. Eng. J. Med., 1990; 323 :
1651.
33. Handa; PUO - Experience at a large teaching hospital in New
Delhi, J. Assoc. Phys. India 1994; 42 (12) : 1020.
34. Dhawan; A clinical study of Pyrexia of unknown origin. J.
Assoc. Phys. India, 1994; 42(12); 1021.
35. Agarwal; FUO in a Tertiary care hospital. J. Assoc. Phys. India,
1998; 46(1) : 30.
36. Geneva, Switzerland: World Health Organization; 2009. WHO.
Dengue: Guidelines for Diagnosis, Treatment, Prevention and
Control. Part 1.1.6: Dengue case classification; pp. 10–2.
37. Ranjit S, Kissoon N. Dengue hemorrhagic fever and shock
syndromes. Pediatr Crit Care Med. 2011;12:90–100.
38. Narayanan M, Aravind MA, Thilothammal N, Prema R,
Sargunam CS, Ramamurty N. Dengue fever epidemic in Chennai-
93
a study of clinical profile and outcome. Indian
Pediatr. 2002;39:1027–33.
39. Waterman SH, Gubler DJ. Dengue fever. Clin
Dermatol. 1989;7:117–22.
40. 24. Itoda I, Masuda G, Suganuma A, Imamura A, Ajisawa A,
Yamada K, et al. Clinical features of 62 imported cases of dengue
fever in Japan. Am J Trop Med Hyg. 2006;75:470–4.
41. Radakovic-Fijan S, Graninger W, Müller C, Hönigsmann H,
Tanew A. Dengue hemorrhagic fever in a British travel guide. J
Am Acad Dermatol. 2002;46:430–3.
42. Chadwick D, Arch B, Wilder-Smith A, Paton N. Distinguishing
dengue fever from other infections on the basis of simple clinical
and laboratory features: Application of logistic regression
analysis. J Clin Virol. 2006;35:147–53.
43. Kabra SK, Juneja R, Madhulika, Jain Y, Singhal T, Dar L, et al.
Myocardial dysfunction in children with dengue haemorrhagic
fever. Natl Med J India. 1998;11:59–61.
44. Halstead SB, Lan NT, Myint TT, Shwe TN, Nisalak A,
Kalyanarooj S, et al. Dengue hemorrhagic fever in infants:
Research opportunities ignored. Emerg Infect Dis. 2002;8:1474–
9.

94
45. National Institute of Communicable Diseases. Investigation and
Control of Outbreaks: Dengue and Dengue Hemorrhagic
Fever. 1997
46. Geneva: World Health Organization; 2001. World Health
Organization. Dengue and dengue haemorrhagic fever. Chapter 6.
WHO Report on Global Surveillance of Epidemic Prone Infectious
Diseases.
47. Srikiatkhachorn A, Krautrachue A, Ratanaprakarn W,
Wongtapradit L, Nithipanya N, Kalayanarooj S, et al. Natural
history of plasma leakage in dengue hemorrhagic fever: A serial
ultrasonographic study. Pediatr Infect Dis J. 2007;26:283–90.
48. Gurugama P, Garg P, Perera J, Wijewickrama A, Seneviratne SL.
Dengue viral infections. Indian J Dermatol. 2010;55:68–78.
49. Hazra, Chowdhury RS, Sala S.K., et al., Changing Scenario of
Malaria : A study at Calcutta. Indian J. Malariol, 1998: 35(2) : 111
- 6
50. Kochar DK, Subhakaran, BL Kumawat et al., Cerebral malaria
in Indian Adults; J. Assoc. Phys. India 2002; 50 : 234 - 241
51. Harris VK, Richard Vs Mathai E et al., A study on clinical
profile of Falciparum malaria in a tertiary care hospital in South
India. Indian J. Malariol, 2001 : 38(1-2) : 19-24.
95
52. Sharma AK, Arora M, Gupta H. et al., Malarial Acute Renal
Failure in Rajasthan. J. Assoc. Phys. India, 1998; 46 : 1001 -
1002.
53. Edward et al., Leptospirosis in Barbados. A clinical study. W.I.
Med. J. 1990; 39 : 27 - 34.
54. Muthusethu pathi, Shivakumar. Leptospirosis in Madras - A
clinical and serological study. J. Assoc. Phys. India 1995; 43(7)
: 456 - 58.
55. Gendron; Leptospirosis in French polynesia : 120 Case reports
Med. Trop. 52 : 21 - 7.
56. Narendra Kotwal; Pneumonia among army recruits. J. Assoc.
Phys. India 1998; 46(1) : 8
57. John barlett, Community Acquired Pneumonia. N. Eng. J. Med,
1995; 333 ; 1618 - 1623.
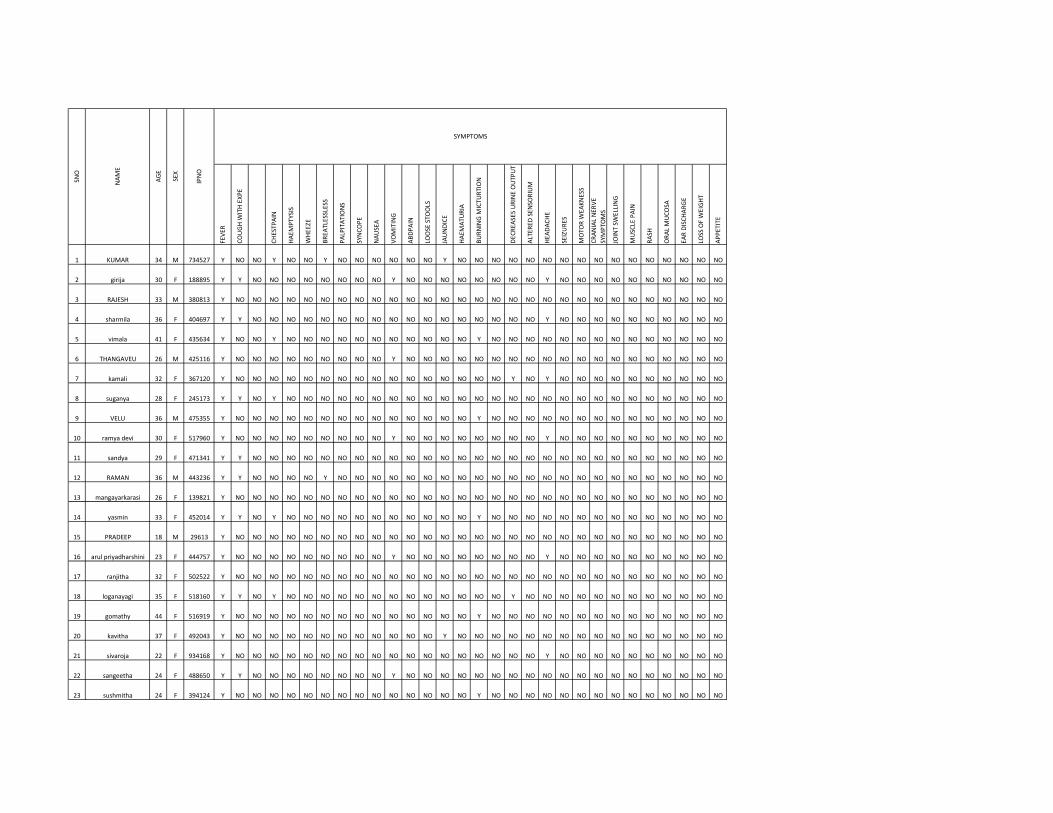
FE
VE
R
CO
UG
H W
ITH
EX
PE
CH
ES
TP
AIN
HA
EM
PT
YS
IS
WH
EE
ZE
BR
EA
TLE
SS
LES
S
PA
LPIT
AT
ION
S
SY
NC
OP
E
NA
US
EA
VO
MIT
ING
AB
DP
AIN
LOO
SE
ST
OO
LS
JAU
ND
ICE
HA
EM
AT
UR
IA
BU
RN
ING
MIC
TU
RT
ION
DE
CR
EA
SE
S U
RIN
E O
UT
PU
T
ALT
ER
ED
SE
NS
OR
IUM
HE
AD
AC
HE
SE
IZU
RE
S
MO
TO
R W
EA
KN
ES
S
CR
AN
IAL
NE
RV
E
SY
MP
TO
MS
JOIN
T S
WE
LLIN
G
MU
SC
LE P
AIN
RA
SH
OR
AL
MU
CO
SA
EA
R D
ISC
HA
RG
E
LOS
S O
F W
EIG
HT
AP
PE
TIT
E
1 KUMAR 34 M 734527 Y NO NO Y NO NO Y NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
2 girija 30 F 188895 Y Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
3 RAJESH 33 M 380813 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
4 sharmila 36 F 404697 Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
5 vimala 41 F 435634 Y NO NO Y NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
6 THANGAVEU 26 M 425116 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
7 kamali 32 F 367120 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO Y NO NO NO NO NO NO NO NO NO NO
8 suganya 28 F 245173 Y Y NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
9 VELU 36 M 475355 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
10 ramya devi 30 F 517960 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
11 sandya 29 F 471341 Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
12 RAMAN 36 M 443236 Y Y NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
13 mangayarkarasi 26 F 139821 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
14 yasmin 33 F 452014 Y Y NO Y NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
15 PRADEEP 18 M 29613 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
16 arul priyadharshini 23 F 444757 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
17 ranjitha 32 F 502522 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
18 loganayagi 35 F 518160 Y Y NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO
19 gomathy 44 F 516919 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
20 kavitha 37 F 492043 Y NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
21 sivaroja 22 F 934168 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
22 sangeetha 24 F 488650 Y Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
23 sushmitha 24 F 394124 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
SN
O
NA
ME
AG
E
SE
X
SYMPTOMS
IPN
O
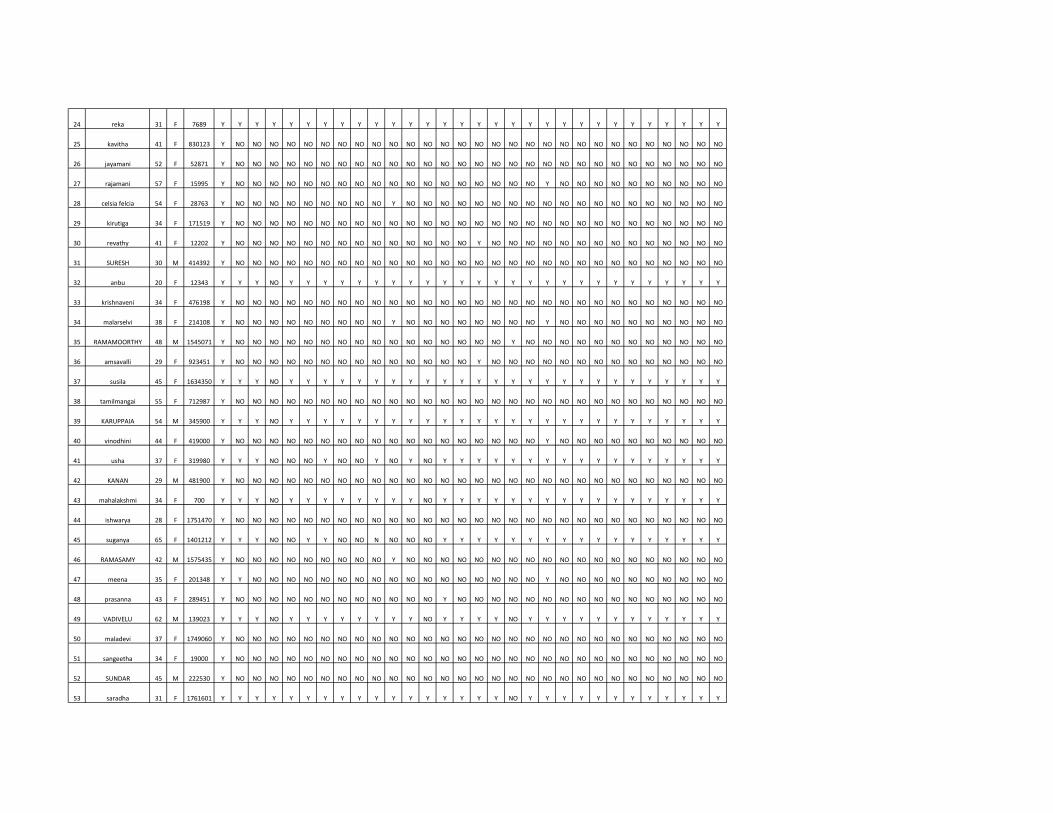
24 reka 31 F 7689 Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
25 kavitha 41 F 830123 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
26 jayamani 52 F 52871 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
27 rajamani 57 F 15995 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
28 celsia felcia 54 F 28763 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
29 kirutiga 34 F 171519 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
30 revathy 41 F 12202 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
31 SURESH 30 M 414392 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
32 anbu 20 F 12343 Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
33 krishnaveni 34 F 476198 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
34 malarselvi 38 F 214108 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
35 RAMAMOORTHY 48 M 1545071 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO
36 amsavalli 29 F 923451 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
37 susila 45 F 1634350 Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
38 tamilmangai 55 F 712987 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
39 KARUPPAIA 54 M 345900 Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
40 vinodhini 44 F 419000 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
41 usha 37 F 319980 Y Y Y NO NO NO Y NO NO Y NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
42 KANAN 29 M 481900 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
43 mahalakshmi 34 F 700 Y Y Y NO Y Y Y Y Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
44 ishwarya 28 F 1751470 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
45 suganya 65 F 1401212 Y Y Y NO NO Y Y NO NO N NO NO NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
46 RAMASAMY 42 M 1575435 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
47 meena 35 F 201348 Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
48 prasanna 43 F 289451 Y NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
49 VADIVELU 62 M 139023 Y Y Y NO Y Y Y Y Y Y Y Y NO Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
50 maladevi 37 F 1749060 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
51 sangeetha 34 F 19000 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
52 SUNDAR 45 M 222530 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
53 saradha 31 F 1761601 Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
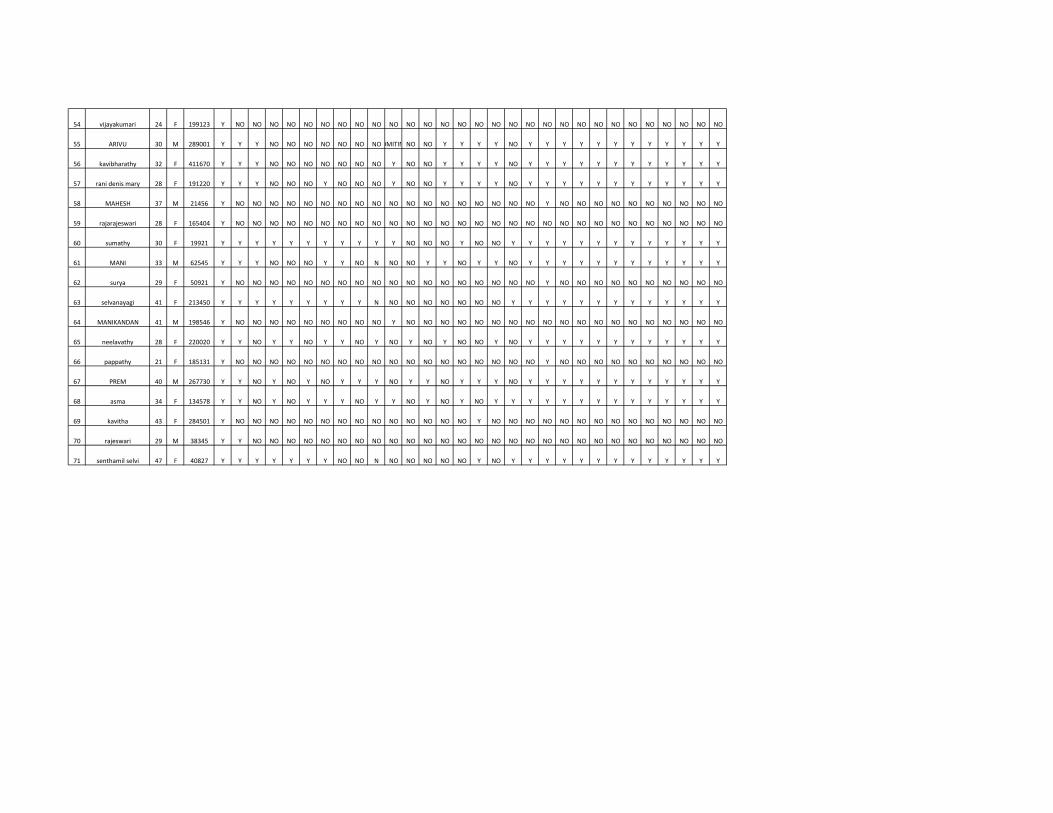
54 vijayakumari 24 F 199123 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
55 ARIVU 30 M 289001 Y Y Y NO NO NO NO NO NO NOVOMITING NO NO Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
56 kavibharathy 32 F 411670 Y Y Y NO NO NO NO NO NO NO Y NO NO Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
57 rani denis mary 28 F 191220 Y Y Y NO NO NO Y NO NO NO Y NO NO Y Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
58 MAHESH 37 M 21456 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
59 rajarajeswari 28 F 165404 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
60 sumathy 30 F 19921 Y Y Y Y Y Y Y Y Y Y Y NO NO NO Y NO NO Y Y Y Y Y Y Y Y Y Y Y Y Y
61 MANI 33 M 62545 Y Y Y NO NO NO Y Y NO N NO NO Y Y NO Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
62 surya 29 F 50921 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
63 selvanayagi 41 F 213450 Y Y Y Y Y Y Y Y Y N NO NO NO NO NO NO NO Y Y Y Y Y Y Y Y Y Y Y Y Y
64 MANIKANDAN 41 M 198546 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
65 neelavathy 28 F 220020 Y Y NO Y Y NO Y Y NO Y NO Y NO Y NO NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y
66 pappathy 21 F 185131 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
67 PREM 40 M 267730 Y Y NO Y NO Y NO Y Y Y NO Y Y NO Y Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
68 asma 34 F 134578 Y Y NO Y NO Y Y Y NO Y Y NO Y NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y
69 kavitha 43 F 284501 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
70 rajeswari 29 M 38345 Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
71 senthamil selvi 47 F 40827 Y Y Y Y Y Y Y NO NO N NO NO NO NO NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y
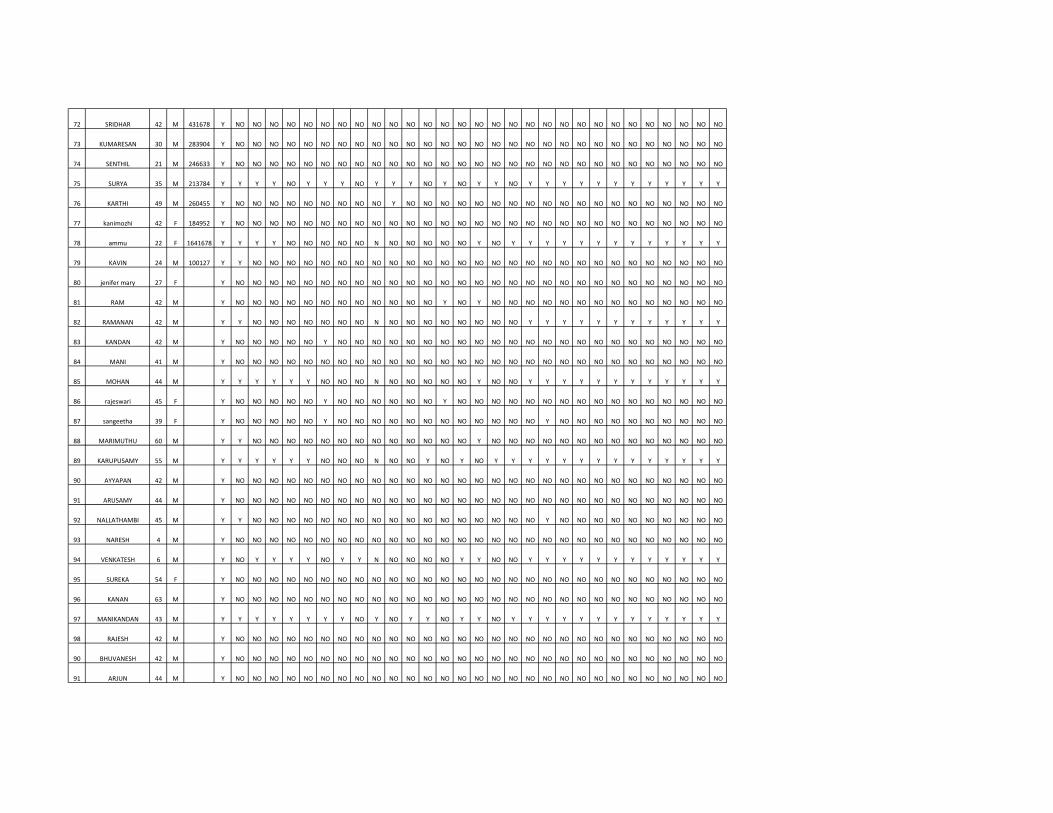
72 SRIDHAR 42 M 431678 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
73 KUMARESAN 30 M 283904 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
74 SENTHIL 21 M 246633 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
75 SURYA 35 M 213784 Y Y Y Y NO Y Y Y NO Y Y Y NO Y NO Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y
76 KARTHI 49 M 260455 Y NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
77 kanimozhi 42 F 184952 Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
78 ammu 22 F 1641678 Y Y Y Y NO NO NO NO NO N NO NO NO NO NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y
79 KAVIN 24 M 100127 Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
80 jenifer mary 27 F Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
81 RAM 42 M Y NO NO NO NO NO NO NO NO NO NO NO NO Y NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
82 RAMANAN 42 M Y Y NO NO NO NO NO NO NO N NO NO NO NO NO NO NO NO Y Y Y Y Y Y Y Y Y Y Y Y
83 KANDAN 42 M Y NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
84 MANI 41 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
85 MOHAN 44 M Y Y Y Y Y Y NO NO NO N NO NO NO NO NO Y NO NO Y Y Y Y Y Y Y Y Y Y Y Y
86 rajeswari 45 F Y NO NO NO NO NO Y NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
87 sangeetha 39 F Y NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
88 MARIMUTHU 60 M Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO
89 KARUPUSAMY 55 M Y Y Y Y Y Y NO NO NO N NO NO Y NO Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y Y
90 AYYAPAN 42 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
91 ARUSAMY 44 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
92 NALLATHAMBI 45 M Y Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO Y NO NO NO NO NO NO NO NO NO NO
93 NARESH 4 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
94 VENKATESH 6 M Y NO Y Y Y Y NO Y Y N NO NO NO NO Y Y NO NO Y Y Y Y Y Y Y Y Y Y Y Y
95 SUREKA 54 F Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
96 KANAN 63 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
97 MANIKANDAN 43 M Y Y Y Y Y Y Y Y NO Y NO Y Y NO Y Y NO Y Y Y Y Y Y Y Y Y Y Y Y Y
98 RAJESH 42 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
90 BHUVANESH 42 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO
91 ARJUN 44 M Y NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO NO

1 KUMAR
2 girija
3 RAJESH
4 sharmila
5 vimala
6 THANGAVEU
7 kamali
8 suganya
9 VELU
10 ramya devi
11 sandya
12 RAMAN
13 mangayarkarasi
14 yasmin
15 PRADEEP
16 arul priyadharshini
17 ranjitha
18 loganayagi
19 gomathy
20 kavitha
21 sivaroja
22 sangeetha
23 sushmitha
SN
O
NA
ME
PS
ME
AR
DIA
GN
OS
IS
FE
VE
R D
UR
AT
ION
SM
OK
ING
ALC
OH
OL
PU
LSE
BP
TE
MP
RR
TC
/1
00
0
DC
HB
PA
LTE
LET
LA
KH
S
MP
/MF B
LO
OD
U
RE
A
LF
T
BLO
OD
CU
LT
UR
E
EC
G
X R
AY
CH
ES
T
SP
UT
UM
FO
R A
FB
MA
NT
OU
X
CS
F
UR
INE
PU
S C
ELLS
NO NO 77 130/9038.1 N 11 DECREASED15NORMALNORMALND N N ND ND N D <5
NO NO 80 130/9838.8 T 9 NORMAL 1NORMALNORMALND N N ND ND N D 10-15DA
NO NO 6 120/7037.5 N 8 NORMAL1.5NORMALNORMALND N N ND ND N D 15-Jan
NO NO 86 110/9038.6 N 9 NORMAL 2NORMALNORMALND N N ND ND N D 5
NO NO 84 110/9038.5 N 5 NORMAL1.5NORMALNORMAL N N N NEGATIVE ND N DENGUE <5
NO NO 68 120/7039.2 N 6 NORMAL 1NORMALNORMALND N N ND ND N DENGUE <5
NO NO 78 130/8037.5 T 7 NORMAL1.5NORMALNORMALND NEFFUSION ND ND N DENGUE 6
NO NO 64 140/8037.8 N 8 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 8
Y NO 96 130/8038.3 N 5 NORMAL40NORMALNORMALND N N NEGATIVE ND N DENGUE 9
NO NO 52 130/8039.4 N 6 NORMAL65NORMALNORMALND N N ND ND N DENGUE 5
NO NO 65 130/8038.1 N 7 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 6
NO NO 68 130/8038.3 N 8 NORMAL1.5NORMALNORMALND NEFFUSION ND ND N DENGUE 8
NO NO 78 120/8038.6 N 6 NORMAL 2NORMALNORMAL N N N ND ND N DENGUE 10
NO NO 80 110/7038.9 T 10 NORMAL 2NORMALNORMALND N N ND ND N DENGUE 15
NO NO 90 110/7037.5 N 11 NORMAL2.4NORMALNORMALND N N NEGATIVE ND N DENGUE 20
Y NO 68 90/70 37.2 N 12 NORMAL 3NORMALNORMALND N N ND ND N ENTERIC 12
NO NO 76 80/60 37.5 N 12 NORMAL 3NORMALNORMALND N N ND ND N INFLUENZA 14
NO NO 78 130/8038.6 T 12 DECREASED3NORMALNORMAL N N N ND ND N INFLUENZA 15
NO NO 84 110/7038.1 N 14 NORMAL 3NORMALNORMALND N N ND ND N INFLUENZA 4
NO NO 88 120/80 38 N 6 NORMAL 2NORMALNORMALND N N NEGATIVE NDINCREASEDLIVER ABSCESS 6
Y NO 87 130/8037.8 N 5 NORMAL 2NORMALNORMALND N N ND ND N LIVER ABSCESS 7
NO NO 76 120/8038.9 N 7 NORMAL 2DETECTEDELEVATEDNORMALND N N ND ND N M 8
NO NO 74 120/8037.8 T 8 NORMAL 1DETECTEDELEVATEDNORMALND N N ND ND N MALARIA 10
VIT
ALS
INV
ES
TIG
AT
ION
S
PE
RS
ON
AL
HIS
TO
RY
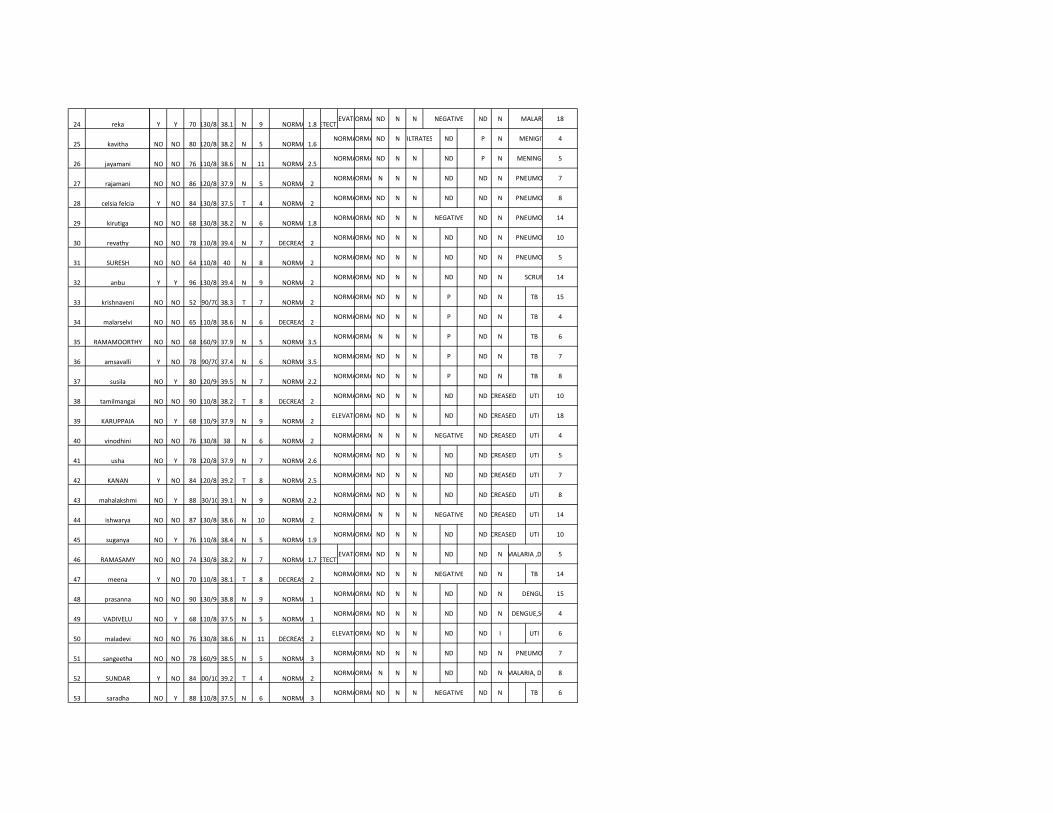
24 reka
25 kavitha
26 jayamani
27 rajamani
28 celsia felcia
29 kirutiga
30 revathy
31 SURESH
32 anbu
33 krishnaveni
34 malarselvi
35 RAMAMOORTHY
36 amsavalli
37 susila
38 tamilmangai
39 KARUPPAIA
40 vinodhini
41 usha
42 KANAN
43 mahalakshmi
44 ishwarya
45 suganya
46 RAMASAMY
47 meena
48 prasanna
49 VADIVELU
50 maladevi
51 sangeetha
52 SUNDAR
53 saradha
Y Y 70 130/8038.1 N 9 NORMAL1.8DETECTEDELEVATEDNORMALND N N NEGATIVE ND N MALARIA 18
NO NO 80 120/8038.2 N 5 NORMAL1.6NORMALNORMALND NINFILTRATES ND P N MENIGITIS 4
NO NO 76 110/8038.6 N 11 NORMAL2.5NORMALNORMALND N N ND P N MENINGITIS 5
NO NO 86 120/8037.9 N 5 NORMAL 2NORMALNORMAL N N N ND ND N PNEUMONIA 7
Y NO 84 130/8037.5 T 4 NORMAL 2NORMALNORMALND N N ND ND N PNEUMONIA 8
NO NO 68 130/8038.2 N 6 NORMAL1.8NORMALNORMALND N N NEGATIVE ND N PNEUMONIA 14
NO NO 78 110/8039.4 N 7 DECREASED2NORMALNORMALND N N ND ND N PNEUMONIA 10
NO NO 64 110/80 40 N 8 NORMAL 2NORMALNORMALND N N ND ND N PNEUMONIA 5
Y Y 96 130/8039.4 N 9 NORMAL 2NORMALNORMALND N N ND ND N SCRUB 14
NO NO 52 90/70 38.3 T 7 NORMAL 2NORMALNORMALND N N P ND N TB 15
NO NO 65 110/8038.6 N 6 DECREASED2NORMALNORMALND N N P ND N TB 4
NO NO 68 160/9037.9 N 5 NORMAL3.5NORMALNORMAL N N N P ND N TB 6
Y NO 78 90/70 37.4 N 6 NORMAL3.5NORMALNORMALND N N P ND N TB 7
NO Y 80 120/9039.5 N 7 NORMAL2.2NORMALNORMALND N N P ND N TB 8
NO NO 90 110/8038.2 T 8 DECREASED2NORMALNORMALND N N ND NDINCREASED UTI 10
NO Y 68 110/9037.9 N 9 NORMAL 2ELEVATEDNORMALND N N ND NDINCREASED UTI 18
NO NO 76 130/80 38 N 6 NORMAL 2NORMALNORMAL N N N NEGATIVE NDINCREASED UTI 4
NO Y 78 120/8037.9 N 7 NORMAL2.6NORMALNORMALND N N ND NDINCREASED UTI 5
Y NO 84 120/8039.2 T 8 NORMAL2.5NORMALNORMALND N N ND NDINCREASED UTI 7
NO Y 88 130/10039.1 N 9 NORMAL2.2NORMALNORMALND N N ND NDINCREASED UTI 8
NO NO 87 130/8038.6 N 10 NORMAL 2NORMALNORMAL N N N NEGATIVE NDINCREASED UTI 14
NO Y 76 110/8038.4 N 5 NORMAL1.9NORMALNORMALND N N ND NDINCREASED UTI 10
NO NO 74 130/8038.2 N 7 NORMAL1.7DETECTEDELEVATEDNORMALND N N ND ND N MALARIA ,DENGUE5
Y NO 70 110/8038.1 T 8 DECREASED2NORMALNORMALND N N NEGATIVE ND N TB 14
NO NO 90 130/9038.8 N 9 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 15
NO Y 68 110/8037.5 N 5 NORMAL 1NORMALNORMALND N N ND ND N DENGUE,SCRUB 4
NO NO 76 130/8038.6 N 11 DECREASED2ELEVATEDNORMALND N N ND ND I UTI 6
NO NO 78 160/9038.5 N 5 NORMAL 3NORMALNORMALND N N ND ND N PNEUMONIA 7
Y NO 84 200/10039.2 T 4 NORMAL 2NORMALNORMAL N N N ND ND N MALARIA, DENGUE8
NO Y 88 110/8037.5 N 6 NORMAL 3NORMALNORMALND N N NEGATIVE ND N TB 6

54 vijayakumari
55 ARIVU
56 kavibharathy
57 rani denis mary
58 MAHESH
59 rajarajeswari
60 sumathy
61 MANI
62 surya
63 selvanayagi
64 MANIKANDAN
65 neelavathy
66 pappathy
67 PREM
68 asma
69 kavitha
70 rajeswari
71 senthamil selvi
NO NO 87 120/8037.8 N 7 NORMAL 2NORMALNORMALND N N ND ND I ENTERIC 6
NO Y 76 110/8038.3 N 8 NORMAL 3NORMALNORMALND N N ND ND N DENGUE 4
NO Y 74 120/8039.4 N 9 NORMAL1.2NORMALNORMAL N NEFFUSION ND ND N DENGUE,SCRUB 5
NO Y 70 110/8038.1 T 7 NORMAL1.2DETECTEDELEVATEDNORMALND N N NEGATIVE ND N MALARIA 7
NO NO 90 130/8038.3 N 6 NORMAL 2NORMALNORMALND N N ND ND N PNEUMONIA 8
Y NO 68 120/8038.6 N 5 NORMAL 1NORMALNORMALND N N ND ND I UTI 14
NO Y 76 110/8038.9 N 6 NORMAL75NORMALNORMALND N N ND ND N DENGUE 10
NO Y 78 110/7037.5 N 7 NORMAL90NORMALNORMAL N N N ND ND N DENGUE,SCRUB 5
NO NO 84 90/60 37.2 T 8 NORMAL60NORMALNORMALND N N ND ND N DENGUE 5
NO Y 88 90/60 37.5 N 9 NORMAL 1NORMALNORMALND N N NEGATIVE ND N TB 6
NO NO 87 80/80 38.6 N 5 NORMAL 2NORMALNORMALND N N ND ND I PNEUMONIA 8
NO Y 76 110/7038.1 N 7 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 4
Y NO 74 110/70 38 N 8 NORMAL 3NORMALNORMALND NINFILTRATES NEGATIVE ND N TB 5
NO Y 70 120/8037.8 T 9 DECREASED2NORMALNORMALND N N ND ND N DENGUE 6
NO Y 90 110/7038.9 N 5 NORMAL1.1NORMALNORMAL N N N ND ND N PNEUMONIA 8
NO NO 68 110/8037.8 N 11 NORMAL1.1NORMALNORMALND N N ND ND N DENGUE 7
NO NO 76 110/8038.1 N 5 DECREASED2NORMALNORMALND N N NEGATIVE ND N TB 6
NO Y 78 130/8038.2 N 4 NORMAL 2NORMALNORMALND N N ND ND I UTI 8
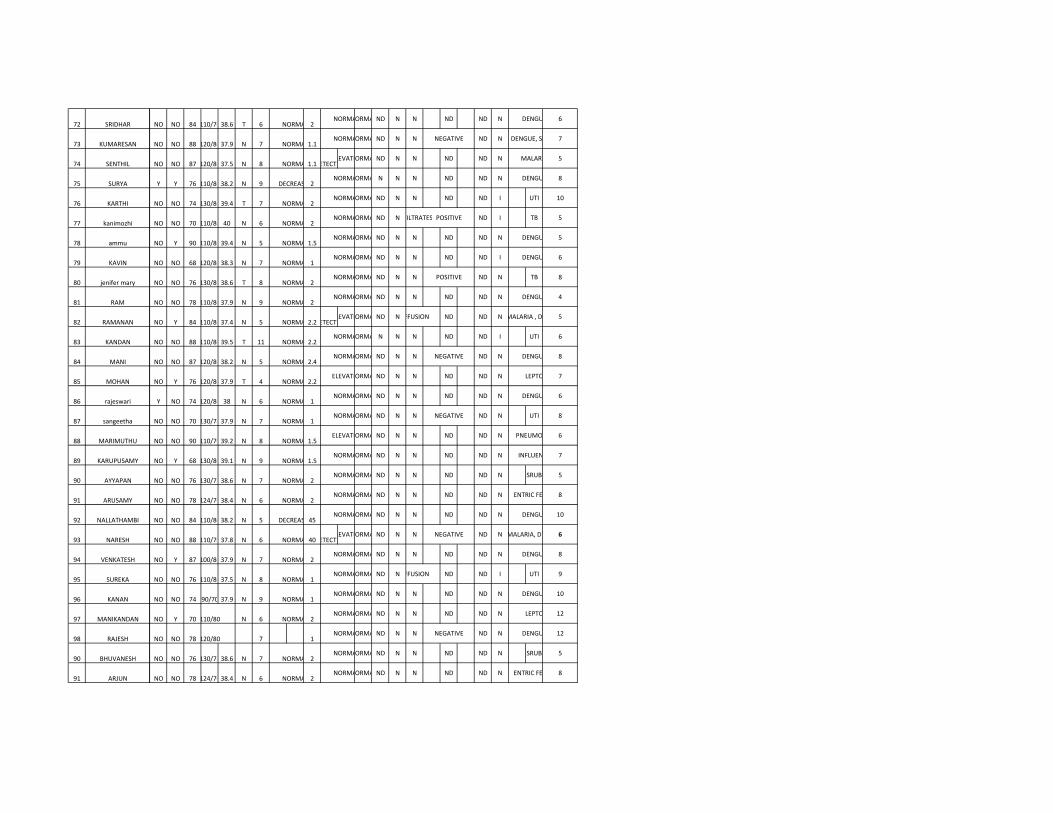
72 SRIDHAR
73 KUMARESAN
74 SENTHIL
75 SURYA
76 KARTHI
77 kanimozhi
78 ammu
79 KAVIN
80 jenifer mary
81 RAM
82 RAMANAN
83 KANDAN
84 MANI
85 MOHAN
86 rajeswari
87 sangeetha
88 MARIMUTHU
89 KARUPUSAMY
90 AYYAPAN
91 ARUSAMY
92 NALLATHAMBI
93 NARESH
94 VENKATESH
95 SUREKA
96 KANAN
97 MANIKANDAN
98 RAJESH
90 BHUVANESH
91 ARJUN
NO NO 84 110/7038.6 T 6 NORMAL 2NORMALNORMALND N N ND ND N DENGUE 6
NO NO 88 120/8037.9 N 7 NORMAL1.1NORMALNORMALND N N NEGATIVE ND N DENGUE, SCRUB7
NO NO 87 120/8037.5 N 8 NORMAL1.1DETECTEDELEVATEDNORMALND N N ND ND N MALARIA 5
Y Y 76 110/8038.2 N 9 DECREASED2NORMALNORMAL N N N ND ND N DENGUE 8
NO NO 74 130/8039.4 T 7 NORMAL 2NORMALNORMALND N N ND ND I UTI 10
NO NO 70 110/80 40 N 6 NORMAL 2NORMALNORMALND NINFILTRATES POSITIVE ND I TB 5
NO Y 90 110/8039.4 N 5 NORMAL1.5NORMALNORMALND N N ND ND N DENGUE 5
NO NO 68 120/8038.3 N 7 NORMAL 1NORMALNORMALND N N ND ND I DENGUE 6
NO NO 76 130/8038.6 T 8 NORMAL 2NORMALNORMALND N N POSITIVE ND N TB 8
NO NO 78 110/8037.9 N 9 NORMAL 2NORMALNORMALND N N ND ND N DENGUE 4
NO Y 84 110/8037.4 N 5 NORMAL2.2DETECTEDELEVATEDNORMALND NEFFUSION ND ND N MALARIA , DENGUE5
NO NO 88 110/8039.5 T 11 NORMAL2.2NORMALNORMAL N N N ND ND I UTI 6
NO NO 87 120/8038.2 N 5 NORMAL2.4NORMALNORMALND N N NEGATIVE ND N DENGUE 8
NO Y 76 120/8037.9 T 4 NORMAL2.2ELEVATEDNORMALND N N ND ND N LEPTO 7
Y NO 74 120/80 38 N 6 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 6
NO NO 70 130/7837.9 N 7 NORMAL 1NORMALNORMALND N N NEGATIVE ND N UTI 8
NO NO 90 110/7039.2 N 8 NORMAL1.5ELEVATEDNORMALND N N ND ND N PNEUMONIA 6
NO Y 68 130/8039.1 N 9 NORMAL1.5NORMALNORMALND N N ND ND N INFLUENZA 7
NO NO 76 130/7838.6 N 7 NORMAL 2NORMALNORMALND N N ND ND N SRUB 5
NO NO 78 124/7038.4 N 6 NORMAL 2NORMALNORMALND N N ND ND N ENTRIC FEVER 8
NO NO 84 110/8038.2 N 5 DECREASED45NORMALNORMALND N N ND ND N DENGUE 10
NO NO 88 110/7037.8 N 6 NORMAL40DETECTEDELEVATEDNORMALND N N NEGATIVE ND N MALARIA, DENGUE6
NO Y 87 100/8037.9 N 7 NORMAL 2NORMALNORMALND N N ND ND N DENGUE 8
NO NO 76 110/8037.5 N 8 NORMAL 1NORMALNORMALND NEFFUSION ND ND I UTI 9
NO NO 74 90/70 37.9 N 9 NORMAL 1NORMALNORMALND N N ND ND N DENGUE 10
NO Y 70 110/80 N 6 NORMAL 2NORMALNORMALND N N ND ND N LEPTO 12
NO NO 78 120/80 7 1NORMALNORMALND N N NEGATIVE ND N DENGUE 12
NO NO 76 130/7838.6 N 7 NORMAL 2NORMALNORMALND N N ND ND N SRUB 5
NO NO 78 124/7038.4 N 6 NORMAL 2NORMALNORMALND N N ND ND N ENTRIC FEVER 8