Embed Size (px)
Citation preview

Arch Gynecol Obstet (2011) 284:1179–1188
DOI 10.1007/s00404-010-1819-0GENERAL GYNECOLOGY
A structured questionnaire improves preoperative assessment of endometriosis patients: a retrospective analysis and prospective trial
Andreas Hackethal · Catharina Luck · Ann-Kathrin von Hobe · Kosai Eskef · Frank Oehmke · Lutz Konrad
Received: 30 November 2010 / Accepted: 13 December 2010 / Published online: 1 January 2011© Springer-Verlag 2010
AbstractPurpose To determine whether a structured questionnairecan improve preoperative assessment of patients with endo-metriosis.Methods Hospital records for patients with endometriosiswere evaluated retrospectively to determine the complete-ness of information. A structured electronic questionnairewas developed and used to assess preoperatively patientswith suspected or proved endometriosis. Data from bothassessments were compared.Results Data analysed retrospectively showed that therewere valid answers for 89.2% of questions on a standardpatient history template, but information was available foronly 46.3% of parameters considered speciWc to endometri-osis. Data from 69 patients investigated by structured elec-tronic questionnaire gave improved rates of 90.3% forstandard patient history items and 88.5% for endometriosis-speciWc parameters. SigniWcant improvement in validanswers was achieved in 66.7%.Conclusions A structured questionnaire improved thedocumentation of endometriosis-speciWc parameters. Fur-ther studies are needed to ensure that it enhances the eVec-tiveness of preoperative counselling and decisions aboutsurgery.
Keywords Endometriosis · Diagnosis · Patient history · Structured questionnaire · Surgical intervention
Introduction
In endometriosis, uterine mucous membrane tissue growsoutside the uterus, resulting in chronic, inXammatory reac-tions which cause pain and scar formation [1, 2]. Reportedprevalence rates for endometriosis are 4–12% in women ofchildbearing age, 33% in those with chronic pelvic pain and20–71% in those who are infertile [3–5]. Endometriosis isconsidered to be an inherited condition in which a geneticpredisposition may be inXuenced by several diVerent envi-ronmental factors [6–8]. The condition can have anextremely adverse eVect on the quality of life of patientsand their partners [9, 10]. Its symptoms and clinical presen-tation range widely. Patients may be asymptomatic or havesymptoms ranging from mild dysmenorrhoea or infertilityto devastating chronic pain [11]. The typical symptoms ofGerman women with endometriosis are summarised inTable 1 [12].
At present, a suspected diagnosis of endometriosiscan only be conWrmed by histology [13]. A signiWcantpositive correlation has been reported between painsymptoms at presentation and the localisation of deepinWltrating endometriosis requiring extensive, time-con-suming surgical treatment [14]. Preoperative patientassessment and examination aim to conWrm the diagno-sis and assist with mapping the lesions. Thus, carefulassessment of symptoms and pain are extremely impor-tant if patients are to receive eVective and speciWcpreoperative counselling and preparation. We endeav-oured to determine whether the quality of clinical andsymptom-speciWc information held for our patients with
A. Hackethal (&) · C. Luck · A.-K. von Hobe · K. Eskef · F. Oehmke · L. KonradDepartment of Obstetrics and Gynaecology, Justus-Liebig-University of Giessen, Klinikstrasse 32, 35385 Giessen, Germanye-mail: [email protected]
123

1180 Arch Gynecol Obstet (2011) 284:1179–1188
endometriosis, and therefore the quality of preoperativeassessment, could be improved by the introduction of astructured questionnaire.
Materials and methods
Retrospective analysis
We searched the database of patients treated at the Univer-sity Hospital of Giessen between 2006 and 2008 and identi-Wed those with a postoperative diagnosis of endometriosis(ICD-10: N85.0) and its subgroups (Table 2). The patients’medical notes were identiWed from the hospital archives forfurther evaluation.
When a patient is admitted to our clinic, the gynaecolo-gist in charge completes a patient history form comprisingquestions on the patient’s general and gynaecological his-tory. The results of examinations at admission and dis-charge are also noted. Data on laboratory investigations,radiological examinations and medication are available onthe hospital intranet system (KAOS). Until the end of 2007,inpatient medical notes were handwritten and stored in thepatient’s Wle. However, since then, they have been included
in the KAOS system. We accessed the KAOS system, tocollect preoperative and postoperative data on patients withendometriosis.
Literature search
We performed a search on MEDLINE and PubMed usingthe phrases “diagnosis of endometriosis” and “question-naire for diagnosis of endometriosis” to identify clinicaland scientiWc parameters which might be important in con-Wrming the diagnosis or making it more speciWc. The key-words and the relevant literature and cross references wereevaluated.
Questionnaire development and trial
The patient data we had identiWed were entered in an elec-tronic database. The database and relevant results from theliterature search were used to develop a structured elec-tronic questionnaire which asked not only about the pres-ence of endometriosis-speciWc symptoms but included avisual analogue scale to give an indication of their severity.The questionnaire (see Appendix) was used routinelybetween October 2009 and April 2010 in patients who pre-sented to our clinic with suspected or known endometriosis.It was produced as a PDF Wle in Microsoft Windows andcould be completed by the patient on a laptop with a directlink to the database. A Xow chart summarising the data col-lection procedure is shown in Fig. 1.
Statistical analysis
The data collected before and after questionnaire develop-ment were then analysed to determine whether the elec-tronic questionnaire improved patient assessment andtherefore treatment planning. The study data generatedwere descriptive and statistical comparisons betweengroups’ mean were done by chi squared test. A p < 0.05was considered signiWcant. For statistical analysis, we usedSPSS version 18.0 for Windows.
Ethical approval
The study was approved by the university’s ethicscommittee.
Results
Retrospective group data
We identiWed from the hospital records 248 patients with apostoperative diagnosis of endometriosis (ICD 10) who had
Table 1 Symptoms of endometriosis and their prevalence in Germanwomen (12)
Symptom Prevalence (%)
Primary and secondary sterility 60–80
Secondary dysmenorrhoea 50–60
Menstruation associated pain within the pelvis 30–40
Dyspareunia 15–30
Menstrual cycle irregularities 5–15
Table 2 DiVerent diagnoses (ICD10) associated with endometriosisin patients treated between 2006 and 2008
a More than one diagnosis per patient was possible
ICD-10 Diagnosis Number of patientsa
N80.0 Uterine endometriosis 87
N80.1 Ovarian endometriosis 92
N80.2 Tubal endometriosis 12
N80.3 Endometriosis of pelvic peritoneum 99
N80.4 Endometriosis of recto-vaginal space and vagina
29
N80.5 Bowel endometriosis 34
N80.6 Endometriosis of scar 2
N80.8 Other endometriosis 32
N80.9 Endometriosis not further deWned 25
123

Arch Gynecol Obstet (2011) 284:1179–1188 1181
undergone 268 surgical procedures during the study period.The records of 245 patients were retrieved from thearchives and data from 236 of these patients were eligiblefor evaluation. Electronic data for all patients were avail-able through the KAOS system. Table 2 summarises thenumbers associated with diVerent ICD-10, N80 diagnosesin patients treated between 2006 and 2008.
The mean § SD age of the women was 37.8 § 9.3 yearsand their mean § SD body mass index (BMI) was24.4 § 5.5.
Patients with known endometriosis comprised 35.6%(84/236) of the retrospective group. Table 3 summarises theavailability of selected patient data and the main results forboth groups, while Table 4 summarises the documentationof endometriosis-speciWc symptoms. A total of 36.8% (86/234) had previously undergone surgery because of endome-triosis—58.1% (50/86) were operated once and 41.9% (36/86) had multiple surgeries for endometriosis. In total, 158
procedures for endometriosis had been performed (118laparoscopies, 32 laparotomies and 8 unknown approaches).The typical symptoms associated with endometriosis werechronic pelvic pain 73.8% (107/145), dysmenorrhoea 65.2%(92/141) and dyspareunia 54.3% (19/35).
Prospective group data
The structured electronic questionnaire was completed by84.1% (69/82) of patients. The mean § SD age of the sub-jects in this group was 32.7 § 9.3 years and their BMI was23.6 § 4.8.
Patients with known endometriosis made up 72.7% (48/66) of this group. In three patients, surgery did not showendometriosis 5.3% (3/57). Typical complaints associatedwith endometriosis were dysmenorrhoea 87.5% (56/64),dyspareunia 64.5% (40/62) and chronic pelvic pain 58.7%(37/63).
Fig. 1 Flow chart describing the collection of data and the development of the electronic questionnaire
Table 3 Selected parameters from the records of endometriosis (EM) patients treated in 2006–2008 (retrospective group) and those assessed withthe structured electronic questionnaire between October 2009 and April 2010 (prospective group)
a Items explicitly included in patient history form
Parameters Retrospective group Prospective group p value valid answers between groups
% (Valid answers/total) % (Symptom applicable/total)
% (Valid answers/total) % (Symptom applicable/total)
Previous EM 100 (236/236) 35.6 (84/236) 95.7 (66/69) 72.7 (48/66) 0.01
Previous surgery for EM 99.2 (234/236) 36.8 (86/234) 97.1 (67/69) 70.1 (47/67) 0.22
Previous abdominal surgerya 100 (236/236) 49.6 (117/236) 97.1 (67/69) 41.8 (28/67) 0.05
Infertility 63.0 (148/235) 43.2 (64/148) 79.7 (55/69) 32.7 (18/55) <0.001
Previous ART 7.6 (18/236) 83.3 (15/18) 75.4 (52/69) 11.5 (6/52) <0.001
OC medication 56.8 (134/236) 42.5 (57/134) 95.6 (65/68) 55.4 (36/65) <0.001
Irregular menstruationa 86.9 (205/236) 14.6 (30/205) 95.7 (68/69) 26.5 (18/68) 0.03
Length of menstrual cyclea 41.9 (99/236) 59.4 (41/69) 0.01
Bleeding character 16.9 (40/232) 65.2 (45/69) <0.001
Allergiesa 98.3 (232/236) 53.9 (125/232) 95.7 (66/69) 62.1 (41/66) 0.19
Family history EM 67.2 (158/235) 2.5 (4/158) 97.1 (67/69) 16.4 (11/67) <0.001
123

1182 Arch Gynecol Obstet (2011) 284:1179–1188
Categorising parameters
Tables 3 and 4 illustrate selected parameters, which can bedivided into two categories. The Wrst comprises sevenexplicitly asked items in the template of the patient historyform. The second category consists of 11 items which aredisease-speciWc and depend on the patient’s likely diagno-sis (i.e dysmenorrhoea, dyspareunia and haemochezia forendometriosis). An obvious diVerence in the quantity ofdocumented information was observed between these twocategories in the retrospectively analysed data. The fre-quency of answers from the template patient assessmentform was 89.2% when compared with 46.3% for the dis-ease-speciWc parameters. In contrast, the electronic ques-tionnaire used in the prospective study provided higherfrequencies of valid answers of 90.3% for patient assess-ment items and 88.5% for disease-speciWc parameters.
For the selected parameters, statistical signiWcantimprovement between valid answers and groups was docu-mented for 66.7% (12/18) items.
Discussion
The development and incorporation of a structured elec-tronic questionnaire to record the patient’s history and spe-ciWc complaints related to endometriosis increased thefrequency of valid answers in the template patient assess-ment and the disease-speciWc parameters.
An experienced doctor is able to assess and analyse rela-tively quickly the important patient data which may point tothe correct diagnosis. However, more inexperienced practi-tioners may not be aware of all the important relationshipsbetween symptoms and diseases. It is particularly true ofgeneralised symptoms, such as lower abdominal pain, thatthe patient’s history and their presenting complaints are thekey factors in making an accurate diagnosis and initiating
the proper treatment. Thus, a thorough assessment is neces-sary. In relation to speciWc symptoms, this study found thatchronic pelvic pain and dysmenorrhoea are symptoms inalmost 75% of patients with endometriosis and over 50%experienced pain during sexual intercourse. Lower abdomi-nal pain and chronic abdominal pain are considered themain symptoms of endometriosis and deep inWltratingendometriosis, respectively, and in the latter, the severity ofchronic pain is signiWcantly correlated with the depth ofinWltration [15, 16]. Dyspareunia and painful defecationtypically suggest the presence of deep inWltrating endome-triosis, although some researchers found a poor correlationbetween the severity of pain and the anatomical staging ofthe disease [17, 18]. Thus, thorough assessment of thesymptoms and their severity can help to approximate thesite of endometriosis before surgery.
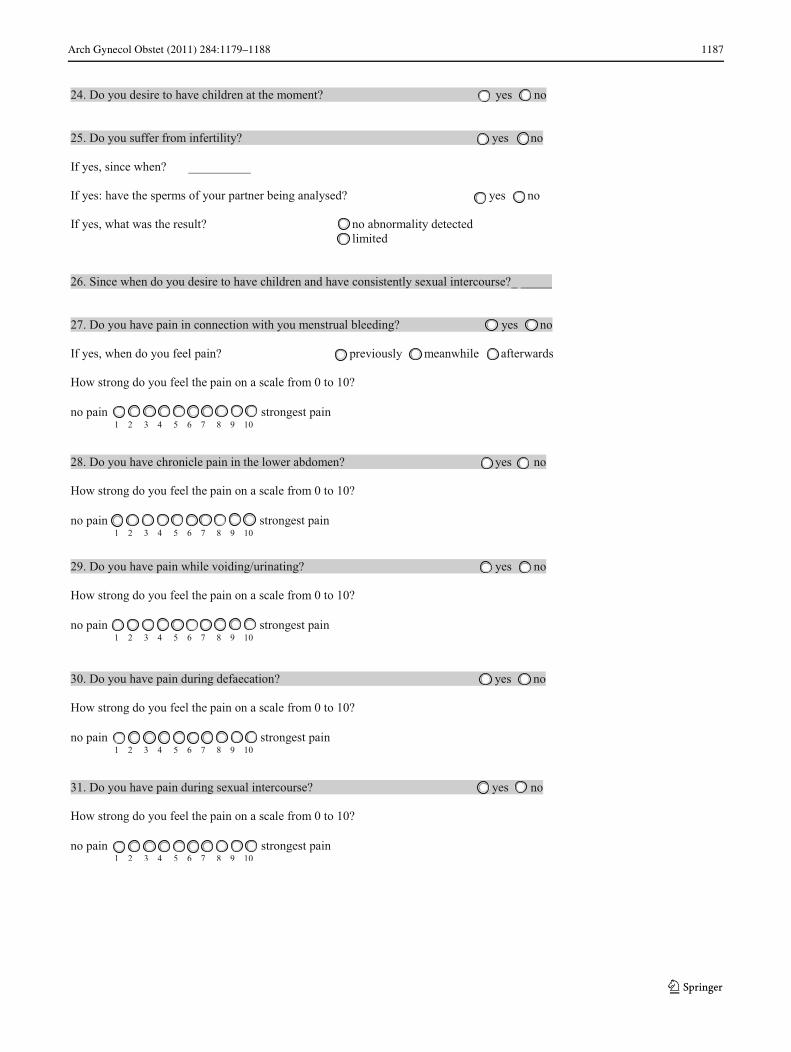
The preoperative assessment of pain through the use of astandardised questionnaire has been helpful in providingadequate exploration and counselling before laparoscopicsurgery for pelvic pain symptoms and bladder endometri-osis [17, 19]. It has been suggested that using a visual ana-logue scale to assess pain symptoms and their peak duringthe menstrual cycle may help in categorising these symp-toms and comparing them before and after surgery [20]. Wetherefore incorporated a visual analogue scale in the ques-tionnaire. Preoperative patient assessment and examinationaim at conWrming the diagnosis of endometriosis and theorgans involved. This information is particularly importantfor counselling the patient and organising appropriate inter-disciplinary surgical management where this is necessary.
Surgical excision of endometriotic nodules is consideredsuYcient to reduce pain and enhance fertility [21–23]. Therate of recurrence of endometriosis after surgical and con-servative treatment is between 2 and 47%. This rate is inXu-enced by how radical the surgery is, and this is largelydependent on the preoperative patient investigations [3, 24,25]. Again, an accurate assessment of the extent of the
Table 4 Selected documented symptoms that may be caused by endometriosis (EM) from the records of patients treated in 2006–2008 (retrospec-tive group) and those assessed with the structured electronic questionnaire between October 2009 and April 2010 (prospective group)
a Items explicitly included in patient history form
Parameters Retrospective group Prospective group p value valid answers between groups
% (Valid answers/total) % (Symptom applicable/total)
% (Valid answers/total) % (Symptom applicable/total)
Dysmenorrhoea 59.7 (141/236) 65.2 (92/141) 92.8 (64/69) 87.5 (56/64) <0.001
Chronic pelvic pain 61.4 (145/236) 73.8 (107/145) 91.3 (63/69) 58.7 (37/63) <0.001
Dysuriaa 95.8 (226/236) 10.2 (23/226) 94.2 (65/69) 18.5 (12/65) 0.39
Pain defecationa 94.5 (223/236) 9.0 (20/223) 95.7 (66/69) 34.8 (23/66) 0.39
Dyspareunia 14.8 (35/236) 54.3 (19/35) 89.9 (62/69) 64.5 (40/62) <0.001
Obstipationa 93.6 (221/236) 9.0 (20/221) 91.3 (63/69) 28.6 (18/63) 0.33
Haemochezia 2.5 (6/236) 33.3 (2/6) 94.2 (65/69) 15.4 (10/65) <0.001
123

Arch Gynecol Obstet (2011) 284:1179–1188 1183
lesions and the organs involved is essential to organiseinterdisciplinary and suYcient operation time.
The beneWts of a standardised electronic questionnairedesigned to record the patient’s history and assess theirsymptoms include the following: more complete dataassessment, ready availability of the documented data forfurther computer analysis, more objective data assessmentfrom the admitting doctor and more beneWcial use of thepatient’s waiting period. However, it is possible that usingan electronic questionnaire for assessing the patients’ his-tory and complaints might hinder inexperienced doctorsfrom becoming familiar with patient history assessment.Therefore, the doctor must review the questionnaire resultsfor completeness and plausibility during the admissionexamination and ask additional questions if necessary. Ourclinic specialises in endometriosis surgery and the consul-tants determine the surgical procedures. We are not able toevaluate retrospectively which symptoms or complaintshave been verbally assessed by the consultants without doc-umentation, and how far this information might have inXu-enced decisions on diagnosis and treatment.
The number of patients assessed in the questionnairestudy was relatively small and this too might aVect the
validity. Further studies are necessary to validate the ques-tionnaire for patients with endometriosis and correlate thepreoperative standardized data with postoperative results.Furthermore, the data of the visual analogue scale may onlybe evaluated with follow-up data.
In conclusion, the eVective assessment of a patient’smedical history and symptoms of endometriosis—a diversedisease presenting with a variety of symptoms—necessi-tates the following of a structured and standardised preop-erative procedure. The questionnaire we establishedimproved the documentation of the patient’s history andsymptoms. This should enhance the preoperative counsel-ling of patients, thereby allowing radical or interdisciplin-ary surgery if applicable. Furthermore, a standardised andstructured questionnaire may enhance retrospective datacollection and analysis.
Acknowledgments The authors thank Dr. phil. Marc Immenroth,Hamburg Germany for advice in data management and statisticalanalysis.
ConXict of interest We declare that we do not have a conXict ofinterest.
123

1184 Arch Gynecol Obstet (2011) 284:1179–1188
Appendix
123

Arch Gynecol Obstet (2011) 284:1179–1188 1185
123

1186 Arch Gynecol Obstet (2011) 284:1179–1188
123
Arch Gynecol Obstet (2011) 284:1179–1188 1187
123

1188 Arch Gynecol Obstet (2011) 284:1179–1188
References
1. Kennedy S, Bergqvist A, Chapron C, D’Hooghe T, Dunselman G,Greb R, Hummelshoj L, Prentice A, Saridogan E (2005) On behalfof the ESHRE Special Interest Group for Endometriosis andEndometrium Guideline Development Group. ESHRE guidelinefor the diagnosis and treatment of endometriosis. Hum Reprod20:2698–2704
2. Hassa H, Tanir M, Tekin B, Kirilmaz D, Sahin Mutlu F (2009)Cytokine and immune cell levels in peritoneal Xuid and peripheralblood of women with early- and late-staged endometriosis. ArchGyn Obstet 279:891–895
3. Guo SW, Wang Y (2006) The prevalence of endometriosis inwomen with chronic pelvic pain. Gynecol Obstet Invest 62:121–130
4. D`Hooge T, Debrock S, Hill JA, Meuleman C (2003) Endometri-osis and subfertility: is the relationship resolved? Semin ReprodMed 21:243–254
5. Buyalos RP, Agarwal SK (2000) Endometriosis-associated infer-tility. Curr Opin Obstet Gynecol 12:377–381
6. Montgomery GW, Nyholt DR, Zhao ZZ, Treloar SA, Painter JN,Missmer SA, Kennedy SH, Zondervan KT (2008) The search forgenes contributing to endometriosis risk. Hum Reprod Updat14:447–457
7. Koninckx PR, Braet P, Kennedy SH, Barlow PR (1994) Dioxin pol-lution and endometriosis: in Belgian. Hum Reprod 9:1001–1002
8. Javert CT (1949) Pathogenesis of endometriosis based on endome-trial homeoplasia, direct extension, exfoliation and implantation,lymphatic and hematogenous metastasis. Cancer 2:399–410
9. Oehmke F, Weyand J, Hackethal A, Konrad L, Omwandho C,Tinneberg HR (2009) Impact of endometriosis on quality of life: apilot study. Gynecol Endocrinol 25:722–725
10. Sinaii N, Cleary SD, Younes N, Ballweg ML, Stratton P (2007)Treatment utilization for endometriosis symptoms: a cross-sectionalsurvey study of lifetime experience. Fertil Steril 87:1277–1286
11. Ulrich U, Keckstein J (2005) Diagnosing endometriosis. ZentralblGynäkol 127:273–274
12. Schindler AE (1995) Endometriose und Fertilitätsstörungen.Frauenarzt 2:211–212
13. Bedaiwy MA, Falcone T (2004) Laboratory testing for endometri-osis. Clin Chim Acta 340:41–56
14. Fauconnier A, Chapron C (2005) Endometriosis and pelvic pain:epidemiological evidence of the relationship and implications.Hum Reprod Updat 11:595–606
15. Al-Jefout M, Dezarnaulds G, Cooper M, Tokushige N, LuscombeGM, Markham R, Fraser IS (2009) Diagnosis of endometriosis bydetection of nerve Wbres in an endometrial biopsy: a double blindstudy. Hum Reprod 24:3019–3024
16. Koninckx PR, Meuleman C, Demeyere S et al (1991) Suggestiveevidence that pelvic endometriosis is a progressive disease, where-as deeply inWltrating endometriosis is associated with pelvic pain.Fertil Steril 55:759–765
17. Chapron C, Barakat H, Fritel X, Dubuisson J-B, Bréart G, Faucon-nier A (2005) Presurgical diagnosis of posterior deep inWltratingendometriosis based on a standardized questionnaire. Hum Reprod20:507–513
18. Chapron C, Fauconnier A, Dubuisson JB, Barakat H, Vieira M,Bréart G (2003) Deep inWltrating endometriosis: relation betweenseverity of dysmenorrhoea and extent of disease. Hum Reprod18:760–766
19. Fedele L, Bianchi S, Carmignani L, Berlanda N, Fontana E,Frontino G (2007) Evaluation of a new questionnaire for the pre-surgical diagnosis of bladder endometriosis. Hum Reprod22:2698–2701
20. Chopin N, Vieira M, Borghese B, Foulot H, Dousset B, Coste J,Mignon A, Fauconnier A, Chapron C (2005) Operative manage-ment of deeply inWltrating endometriosis: results on pelvic painsymptoms according to a surgical classiWcation. J Minimal InvasGynec 12:106–112
21. Chapron C, Chopin N, Borghese B, Malartic C, Decuypere F,Foulot H (2004) Surgical management of deeply inWltrating endo-metriosis: an update. Ann NY Acad Sci 1034:326–337
22. Donnez J, SquiZet J, Pirard C, Jadoul P, Wyns C, Smets M (2002)The eYcacy of medical and surgical treatment of endometriosis-associated infertility and pelvic pain. Gynecol Obstet Invest54(Suppl 1):2–7
23. Kaiser A, Kopf A, Gericke C, Bartley J, Mechsner S (2009) TheinXuence of peritoneal endometriotic lesions on the generation ofendometriosis-related pain and pain reduction after surgical exci-sion. Arch Gyn Obstet 280:369–373
24. Vercellini P, Barbara G, Abbiati A, Somigliana E, Vigano P,Fedele L (2009) Repetitive surgery for recurrent symptomaticendometriosis: what to do? Eur J Obstet Gynecol Reprod Biol146:15–21
25. Busacca M, ChiaVarino F, Candiani M, Vignali M, Bertulessi C,Oggioni G, Parazzini F (2006) Determinants of long-term clini-cally detected recurrence rates of deep, ovarian, and pelvic endo-metriosis. Am J Obstet Gynecol 195:426–432
123