Embed Size (px)
Citation preview

lthough grouped under a single drug class, skeletal muscle relaxants are a heteroge-neous group of structurally unrelated med-ications with variable pharmacologic and safety profiles.1-3 Skeletal muscle relaxants are used commonly for the treatment of
2 conditions: spasticity and local musculoskeletal spasms. Approximately 2 million Americans, including more than
300,000 people over 60 years of age, are prescribed mus-cle relaxants.3
Spasticity and spasms are distinct etiologies, and each con-dition responds differently to certain medications. Spasticity is a disorder of motor neurons that manifests as increased muscle tone and stiffness.4 Spasms are involuntary localized muscle contractions that arise from acute trauma or muscle strain.3,5 Although antispasmodics and antispasticity agents
Feature
A
A Review of Skeletal Muscle Relaxants For Pain ManagementSpasticity and spasm: 2 distinct reactions to motor neurons that require unique and sometimes complementary therapies.
Mena Raouf, PharmD PGY-1 Pharmacy residentVa tennessee Valley Healthcare SystemNashville, tennessee
Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHPPresident and Director, Scientific and Clinical affairs reMItIGate LLC Clinical Pharmacy Specialist in Pain Management Director, PGY2 Pain & Palliative Care Pharmacy Pain residencySamuel Stratton Va Medical Centeralbany, New York
1June 2016 | Pract icalPainManagement.com

generally are not interchangeable, diaz-epam (Valium) is approved by the Food and Drug Administration (FDA) for both conditions.6,7
In this article, the authors review the etiologies of, and treatment options for, painful spasticity and muscle spasm.
Skeletal Muscle SystemTable 1 highlights the basic differences between spasticity and spasms, includ-ing the etiology, symptoms, causes, and FDA-approved therapies.8
Two types of motor neurons regu-late skeletal muscle excitability: upper motor neurons (UMNs), which orig-inate from the cerebral cortex, and lower motor neurons (LMNs), which originate in the spinal cord and brain
stem.9-11 UMNs innervate the LMNs in the spinal cord, where they directly innervate skeletal muscles, and in the brain stem (cranial nerves), where they innervate the facial muscles. UMNs can stimulate or inhibit skeletal mus-cle contraction by direct innervation to LMNs. UMN lesions can result in muscle weakness, spasticity, or both, but LMN lesions may develop into muscle weakness and paralysis.
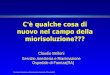
How Skeletal Muscle ContractsA single α-motor neuron can inner-vate up to 200 muscle fibers, forming a complex called motor unit (Figure 1, page 44).10 With movement, an action potential originates from the UMN in the motor cortex.9 This action
potential depolarizes the motor neu-ron terminal, resulting in the opening of voltage-gated calcium (Ca2+) chan-nels and the subsequent release of the neurotransmitter acetylcholine (Ach) into the synaptic cleft. In the synaptic cleft, Ach binds to nicotinic choliner-gic receptors on the muscle fiber mem-brane, leading to an influx of sodium (Na+) and a discharge of potassium (K) across the muscle fiber’s membrane, which results in depolarization of the muscle fiber.11 This depolarization opens voltage-gated Ca2+ channels on the sarcoplasmic reticulum (via ryan-odine and inositol triphosphate recep-tors), allowing for Ca2+ influx into the cytoplasm of striated muscle cells.12 The Ca2+ then binds to troponin C,
Table 1. Difference Between Spasticity and SpasmsDescription Spasticity4,10,13 Spasms3,5
Definition • Velocity-dependent increase in muscle tone caused by the increased excitability of the muscle stretch reflex
• Involuntary muscle contractions
Etiology • Central • Disorder of upper motor neurons
• Peripheral• Muscle sprain or injury • Nerve compression (eg, spinal stenosis)
Symptoms • Stiffness• Hypertonicity• Hyperreflexia
• Jerks• Twitches• Cramps
Causes • Multiple sclerosis• Cerebral palsy• Spinal cord injury• Traumatic brain injury• Motor neuron disease• Post-stroke syndrome
• Musculoskeletal pain• Fibromyalgia • Sciatica• Mechanical low back pain• Herniated disk• Spinal stenosis• Myofascial pain
FDA-approved agentsa
• Botulinum toxinb • Baclofen• Dantrolenec
• Diazepamd
• Riluzolee
• Tizanidine
• Carisoprodol• Chlorzoxazone• Cyclobenzaprine• Metaxalone• Methocarbamol• Orphenadrine
a See Tables 3 and 4 for more in-depth review of agents.b Indication depends on the product.c Also approved for prophylaxis and treatment of malignant hyperthermia.d Approved for treatment of both spasticity and muscle spasms.e Mainly used in patients with amyotrophic lateral sclerosis.
2
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

which exposes myosin-binding sites on actin filaments. A cross-link forms between actin and myosin, leading to muscle contraction. The pumping of Ca2+ back into the sarcoplasmic retic-ulum, using adenosine triphosphate, leads to cessation of contraction.
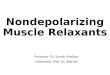
Neuromuscular SystemThere are 2 pathways that regulate skel-etal muscle excitability and contraction: the monosynaptic and polysynaptic reflex pathways.8,10,13 In the monosyn-aptic reflex, afferent signals from muscle cells return to the spinal cord, resulting in negative feedback on motor move-ments. The Golgi tendon (Figure 2), a proprioceptive sensory receptor organ, senses muscle tension and sends an inhibitory signal to the spinal cord.9 In the polysynaptic reflex, type IA afferent neurons synapse on inhibitory neurons in the dorsal horn and inhibit contrac-tion of the targeted area.8,10,13 For exam-ple, if a person touches a hot surface, the brain sends an excitatory signal to stimulate the bicep muscles to contract, allowing for the desired motion, and then sends an inhibitory signal to pre-vent the triceps from contracting to end the motion.
SpasticitySpasticity is defined as a velocity- dependent increase in muscle tone caused by the increased excitability of the muscle stretch reflex.4 Clinical manifestations include muscle stiffness, co-contraction of flexors and exten-sors, and increased resistance to muscle stretching. The etiology of spasticity is not fully known, but it is thought to be due to excessive stimulation or lack of inhibition of α-motor neurons, lead-ing to increased muscle tone.2,4
Spasticity is associated with increased activity of excitatory neurotransmit-ters or decreased activity of inhibitory neurotransmitters (Table 2, page 51).13
Causes of spasticity include multiple
sclerosis (MS), cerebral palsy, spinal cord injury, traumatic brain injury, and post-stroke syndrome.4,10,13
Antispasticity medications reduce muscle tone by acting either on the cen-tral nervous system (CNS) or directly on skeletal muscles (Figure 3, page 52).2 Agents that work on the CNS include baclofen (Gablofen, Lioresal, others), tizanidine (Zanaflex, others), gabapentinoids (gabapentin [Gralise, Horizant, others], pregabalin [Lyrica]), riluzole (Rilutek, others), and benzodi-azepines (diazepam [Diazepam Intensol, Valium, others]), whereas peripheral agents include dantrolene (Dantrium, Revonto, others), and botulinum toxin (Table 3, page 54).14-16
Central Agents Baclofen is a structural analogue of GABA that binds to GABAB recep-tors, which are coupled to presynaptic
and postsynaptic Ca2+ and K+ chan-nels.2,17 Therefore, baclofen acts pre-synaptically and postsynaptically to inhibit spinal reflexes. Presynaptic acti-vation of GABAB receptors results in hyperpolarization and decreased Ca2+ influx, which reduces glutamate release, leading to a decrease in α-motor neu-ron activity. Postsynaptic activation of GABAB increases K+ conductance in the IA afferent neuron terminals, hyperpo-larizing the membrane and enhancing presynaptic inhibition. Baclofen also is thought to inhibit substance P release into the spinal cord, which may reduce pain.18
Baclofen is available as an oral med-ication, as an intrathecal injection, or for use in an intrathecal pump; the lat-ter form is reserved for cases of severe spasticity.19 Baclofen has been evalu-ated for other conditions, including cluster headache, intractable hiccups,
Figure 1. Illustration of a motor unit.10
Reprinted with permission from Pathophysiology of Disease: An Introduction to Clinical Medicine, 7th ed. Copyright McGraw-Hill Companies, Inc. All rights reserved.
3
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

and nicotine, cocaine, and alcohol dependence.20-24
Common adverse effects (AEs) include dry mouth and transient sedation that subside with chronic use.17 Withdrawal syndrome has been reported following abrupt stoppage of intrathecal and/or oral baclofen.25,26 Symptoms associated with abrupt with-drawal of baclofen include auditory and visual hallucinations, agitation, delir-ium, anxiety, fever, tremors, tachycar-dia, and, potentially, seizures.25,26
Tizanidine is a centrally acting α2 agonist that is structurally similar to clonidine.2,6 Tizanidine inhibits pre-synaptic release of excitatory neu-rotransmitters, reducing the excitabil-ity of postsynaptic α-motor neurons.2
In addition, tizanidine can potentiate the actions of glycine.27 Tizanidine has been shown to suppress the polysyn-aptic reflex and reduce abnormal co- contraction of opposing muscle groups.28 Tizanidine also has been eval-uated as an adjunct for prophylaxis of several types of headache, including migraine and tension headache.29
Tizanidine is available as capsules and tablets, which are bioequivalent only when taken on an empty stom-ach.6 When tizanidine is administered with food, the amount absorbed from the capsule is approximately 80% of that of the tablet. In addition, food increases the plasma concentration of the tablet by 30% and decreases the plasma concentration of the capsule by
20%. Ingesting the contents of the cap-sule with applesauce results in a 15% to 20% increase in plasma concentration and area under the curve (AUC), com-pared to ingesting the capsule while fasting.
Tizanidine is metabolized through CYP1A2, and the inactive metabolites are excreted in the urine (60%) and feces (20%).6 CYP1A2 inhibitors, such as fluvoxamine and ciprofloxacin, can increase plasma levels of tizanidine and the incidence of AEs.30 Studies have shown that concurrent use of oral con-traceptives also increased the plasma concentration and hypotensive effects of tizanidine.31
AEs include weakness, dry mouth, increased spasm or tone, hypotension, and mild liver function test (LFT) elevations.6 Withdrawal symptoms, including reflex tachycardia, hyperten-sion, hypertonicity, tremor, and anxiety, have been reported with abrupt discon-tinuation.32 To minimize withdrawal symptoms, the manufacturer recom-mends that the dose be tapered slowly (2-4 mg/day), especially in patients receiving high doses (>20 mg/day) for long periods (>9 weeks).6
Gabapentinoids are anticonvulsant medications that have shown benefit as antispasticity agents in studies in involving patients with spinal cord injuries.2,33-35 Both gabapentin and pregabalin inhibit the α2δ subunit of L-type voltage-gated Ca2+ channels, which are thought to inhibit glutamate release.36,37 Both agents have demon-strated efficacy in treatment of neuro-pathic pain and spasticity in patients with MS.35,38
Gabapentin has been shown to have a dose-related efficacy in controlling spasticity at dosages of 1,200 mg to 3,600 mg/day.33 Gabapentin has vari-able interindividual bioavailability, and it exhibits saturable oral absorp-tion; its bioavailability decreases as the dose increases.2,36 Gabapentin also is
Figure 2. Illustration of the pathways regulating skeletal muscle contraction.9Copyright McGraw-Hill Companies, Inc. All rights reserved.
4
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

available in extended-release formu-lations with improved absorption, a tablet (Gralise),39 and a gastroreten-tive prodrug, gabapentin enacarbil (Horizant).40 Gralise is indicated for the management of postherpetic neu-ralgia,39 whereas Horizant is approved for the treatment of postherpetic neu-ralgia and moderate-to-severe primary restless legs syndrome.40
Pregabalin has a more predictable pharmacokinetic profile compared to gabapentin because it exhibits linear absorption.37 In a retrospective case series that evaluated pregabalin (75 to 300 mg bid) as a monotherapy for spas-ticity in 22 patients, 12 patients per-ceived improvements in spasticity, and 8 patients experienced AEs that lead to discontinuation.35
Overall, the role of gabapenti-noids as monotherapy for spasticity remains unclear. They may be beneficial adjuncts in patients who have spastic-ity and neuropathic pain.
Diazepam is the only benzodiaze-pine that is FDA approved for treat-ment of spasticity and muscle spasms.7 Diazepam binds to GABAA receptors
and potentiates GABAergic activity by increasing chloride conductance, which results in presynaptic inhibition in the spinal cord.2,7 Diazepam has demon-strated efficacy in the management of spasticity associated with spinal cord injury, hemiplegia, and MS. However, it is not often recommended as a first-line agent due to risks of sedation and a potential for dependence or abuse.
Diazepam is metabolized to the active metabolites desmethyldiazepam, temazepam, and oxazepam, the last 2 of which are available commercially.7 AEs include lethargy, sedation, anterograde amnesia, cognitive impairment, and dependence. Withdrawal syndrome can occur with abrupt cessation of diaze-pam, and may lead to seizures.
Riluzole is a glutamatergic drug that is indicated for treatment of spastic-ity associated with amyotrophic lateral sclerosis (ALS).41 The etiology of ALS is unknown, but 1 hypothesis is that neurons become vulnerable through genetic predisposition or environmen-tal factors, and excitotoxicity occurs secondary to excessive stimulation of glutamate receptors. Riluzole inhibits
voltage-gated Na+ channels on glutami-nergic nerve terminals, thereby inhib-iting glutamate release. Riluzole also regulates glutamate release and postsyn-aptic receptor activation. These actions also contribute to inhibition of gluta-mate release.2,41
Riluzole’s absorption is reduced by administration with high-fat meals, which results in a 20% reduction in AUC and a 45% reduction in peak plasma concentration.41 Riluzole undergoes hepatic metabolism through CYP1A2 followed by glucuronidation, and is excreted as glucuronide metab-olites in the urine (85%).41
In clinical trials, riluzole demon-strated disease-specific efficacy, showing benefit in patients with ALS but not patients with Huntington’s disease.42-45 Riluzole prolonged tracheostomy-free survival by 2 to 3 months in patients with ALS and showed a small benefi-cial effect on bulbar and limb func-tion but not on muscle strength.43,44 However, when evaluated in patients with Huntington’s disease, riluzole had no benefit in symptoms or neuropro-tection effects.45
Table 2. Neurotransmitters Involved in the Etiology of Muscle Spasticity and Spasm
• Gamma-Aminobutyric Acid (GABA). GABA, the primary inhibitory neurotransmitter in the nervous system, is released by interneurons within the dorsal and intermediate grey matter of the spinal cord and inhibit IA afferent neurons. Activation of GABA
A receptors increases chloride (Cl-) conduction, which hyperpolarizes the
cell and inhibits action potential formation. Activation of GABAB receptors also can reduce activity of adenylyl
cyclase and decrease calcium (Ca2+) influx into the cell. GABAB receptor activation has been shown to inhibit
the release of pain mediator substance P.14
• Glutamate. Glutamate, the primary excitatory neurotransmitter, increases Ca2+ influx into the postsynaptic cell. Glutamate is released by IA afferent fibers in the descending corticospinal tract. Glutamate also binds to α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA), kainate, and N-methyl-D-aspartate (NMDA) receptors, which mediate synaptic plasticity.
• Glycine. Glycine has both inhibitory and excitatory functions in the CNS. Activation of glycine s activates Cl- channels, as does GABA, which exerts inhibitory effects. Impaired glycine transmission has been linked to autism and hyperekplexia. Glycine is a co-agonist for N-methyl-D-aspartate, which increases neuronal excitation.
• Acetylcholine (Ach). Ach is the primary neurotransmitter responsible for transmitting signals between neurons and muscle fibers. It binds to skeletal muscle nicotinic receptors and increases conductance of sodium (Na+) and Ca2+, leading to depolarization and muscle contraction.
5
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

Common AEs reported during clin-ical trials included nausea, vomiting, dyspepsia, flatulence, dry mouth, and weight loss.41-44 Riluzole was reported to cause dose-related LFT elevations during clinical trials (3-fold increase in serum alanine transferase), and the manufacturer recommends using caution in patients with hepatic impairment.41,43
Peripheral Agents Dantrolene is a hydantoin derivative structurally related to phenytoin that blocks the ryanodine channel, which inhibits Ca2+ release from the sarcoplas-mic reticulum, thus reducing muscle contraction.12,46 Dantrolene has been
approved for “controlling the manifes-tations of clinical spasticity” that is the result of UMN disorders.46
AEs include skeletal muscle weak-ness, dyspnea, dysphasia, somnolence, and dose-dependent diarrhea. There have been reports of life-threatening hepatotoxicity.47,48 Dantrolene carries a black box warning of hepatotoxic-ity associated with high doses (>800 mg/day) and long-term use (3 to 12 months).46 Due to the risk of hepa-totoxicity, it is not commonly used in practice for treatment of chronic spasticity and is mainly reserved for acute conditions such as neuroleptic malignant syndrome and malignant hyperthermia.
Botulinum toxin (BTX) is pro-duced from Clostridium botulinum and is injected locally to inhibit presyn-aptic release of Ach in the neuromus-cular junction, resulting in paralysis of the muscle.49,50 The onset of effect varies depending on the indication but is typically 14 days for spasticity and cervical dystonia—the effect typically lasts approximately 3 months.50 The effect diminishes when motor neurons develop new nerve terminals that start releasing Ach.51 Resistance to the para-lytic effect could develop with repeated injections due to development of anti-bodies against the toxin.52,53 Adverse effects include rash and muscle weakness at the injection site, flu-like symptoms,
Figure 3. Two binding locations of antispasticity agents.CNS, central nervous system; CrCL, creatinine clearance estimate of renal function based on Cockcroft and Gault equation; GABA, gamma-aminobutyric acid; IR, immediate release; LFT, liver function tests; MDD, maximum daily dose; N/A, no information provided by the manufacturer; PK, pharmacokinetic; RYR1, ryanodine receptor 1Copyright McGraw-Hill Companies, Inc. All rights reserved.
6
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

and headache. There are 2 antigenically distinct sero-
types of BTX on the market: BTX-A and BTX-B. BTX-A is available as onabotulinumtoxinA (Botox), abob-otulinumtoxinA (Dysport), and inco-botulinumtoxinA (Xeomin).49,50 The only available BTX-B on the market is rimabotulinumtoxinB (Myobloc). Each agent has different FDA indica-tions. All agents are approved for cervi-cal dystonia; however, BTX-A has been shown to have a longer duration of effect than BTX-B.54 OnabotulinumtoxinA is approved for treatment of upper and lower limb spasticity, whereas abobotu-linumtoxinA is approved for upper limb spasticity.55,56
Muscle SpasmsA muscle spasm is a sudden involun-tary contraction of a muscle group that involves jerking and twitching.1,2,5 Unlike spasticity, which is a disorder of the CNS, muscle spasms arise from a variety of peripheral musculoskele-tal conditions, such as mechanical low back pain. Common skeletal muscle conditions that cause spasms include fibromyalgia, myofascial pain syn-drome, and mechanical low back or neck pain.1
Antispasm Agents Most of the agents discussed here are FDA approved for adjunctive use to treat muscle spasms and pain associ-ated with acute musculoskeletal con-ditions (Table 4, page 58). Health data from 2003 to 2004 revealed that cyclobenzaprine (Amrix, Fexmid, oth-ers), carisoprodol (Soma, others), and metaxalone (Metaxall, Skelaxin, oth-ers) accounted for more than 45% of medications prescribed for acute mus-culoskeletal pain.3
Although skeletal muscle relaxants are recommended for short-term use in the treatment of musculoskeletal pain, approximately 44.5% of users remain
on them for more than a year.3 Due to CNS depression, cyclobenzaprine, metaxalone, orphenadrine (Norflex, others), methocarbamol (Robaxin, others), carisoprodol, and chlorzox-azone (Lorzone, Parafon Forte DSC, others) are on the American Geriatrics Society’s Beers List of inappropriate drugs for elderly patients.5 Despite this, approximately 300,000 annual prescriptions for skeletal muscle relax-ants (15%) are issued to patients older than 65 years of age.3,5
Cyclobenzaprine has no direct activity on skeletal muscle, and its mechanism in myorelaxation has not been elucidated fully but is thought to be due primarily to its sedative effects.2,15,57 Cyclobenzaprine is highly sedating, which could be beneficial in patients with acute muscle spasms who are also experiencing difficulty sleep-ing, but the toxicity that comes with its significant anticholinergic risks can-not be overstated.1,15
Cyclobenzaprine is structurally similar to tricyclic antidepressants (TCAs), differing from amitriptyline by only 1 bond in the central ring.58 A meta-analysis evaluating cyclobenzap-rine in fibromyalgia patients showed that the medication was superior to placebo; however, it has been shown to be inferior to its chemically related TCA counterparts.59,60
Long-term use beyond 3 weeks is not recommended due to lack of data on efficacy for prolonged use.61
Cyclobenzaprine undergoes hepatic metabolism through CYP3A4, CYP1A2, and CYP2D6 and is mainly excreted in the urine as glucuronide conjugates and, to a lesser extent, as unchanged drug in the feces. Its AE profile is similar to amitriptyline and includes anticholinergic AEs (dry mouth, confusion, urinary retention), fatigue, tachycardia, and cardiac con-duction disturbances. It is not recom-mended in patients with arrhythmias
or cardiac conduction abnormalities. Methocarbamol is a centrally act-
ing muscle relaxant that is a carbamate derivative of guaifenesin (Liquibid, Mucinex, others).2,62 Its muscle relax-ant mechanism is unknown but is pre-sumed to be due to sedation. In a head-to-head trial comparing methocarba-mol to cyclobenzaprine, methocarba-mol was associated with less sedation (38% vs 58%), but the percentage of patients who stopped therapy due to AEs was similar for the 2 agents (6% vs 7%, respectively).63 The risk of respira-tory depression may be increased when patients also are taking opioids, benzo-diazepines, or barbiturates. A unique AE of the medication is brown or green urine discoloration. Muscle coordina-tion abnormalities and grand mal sei-zures also have been reported.
Similar to the other agents in this class, carisoprodol is a centrally acting muscle relaxant from the carbamate class.64 In animal studies, carisoprodol exhibited its muscle relaxant effects by altering interneuronal activity in the spinal cord and the descending reticu-lar formation of the brain.64 It also has been found to have analgesic proper-ties by reducing perception of pain.64
Carisoprodol undergoes exten-sive hepatic metabolism through CYP2C19 to several metabolites, including meprobamate, which exerts barbiturate-like activity at the GABAA receptors.65 Poor CYP2C19 metabo-lizers (prevalent in 5%-15% of Asians and 3%-5% of Caucasians and African Americans) have experienced up to a 4-fold increase in exposure to carisop-rodol and 50% reduction in exposure to meprobamate.66
AEs include drowsiness, headache, vertigo, insomnia, and an increased risk of respiratory depression, espe-cially in patients on concomitant opi-oids, benzodiazepines, or barbiturates. Compared to cyclobenzaprine, cariso-prodol is associated with less frequent
7
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

Table 3. Agents Used for Treatment of Spasticity
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic/Renal Impairment
Unique Adverse Effects Pharmacokinetics Drug Interactions
Baclofen 2,17-19
(Gablofen, Lioresal, others)
GABAB receptor agonist
Inhibits presynaptic and postsynaptic glutamate release
Starting dose: 5 mg orally 3 times daily
Increase by 5 mg per dose every 3 days
MDD: 80 mg
Hepatic: none
Renal: none
Transient dizziness that usually resolves with continued therapy, withdrawal syndrome with abrupt discontinuation
Metabolism: 15% of the dose undergoes hepatic deamination
Elimination: 70%-85% of the dose is renally excreted as unchanged drug in urine
CNS depressants
Tizanidine2,6,27-32 (Zanaflex, others)
Structurally similar to clonidine
Centrally acting alpha2 agonist
Inhibits presynaptic and postsynaptic alpha
1 motor
neurons
Could potentiate the actions of glycine
Starting dose: 2-4 mg orally 3 times a day
Titrate to MDD of 36 mg/day in 3 divided doses
Hepatic: avoid use; if used, reduce initial dose during titration
Renal: CrCl <25 mL/min: use with caution
Hypotension (20% decrease in blood pressure), mild LFT elevations (usually reversible), withdrawal syndrome with abrupt discontinuation
Bioavailability depends on formulation and food:
•Fasting: capsules and tablets are bioequivalent
•With meal: capsule has 25% less bioavailability than tablet
Metabolism: CYP1A2
Elimination: 60% urine and 20% feces
CNS depressants
↑ Exposure with CYP1A2 inhibitors (eg, fluvoxamine ciprofloxacin, oral contraceptives, verapamil)
↓ Exposure CYP1A2 inducers (eg, tobacco)
Gabapentin2,36,39,40
(Neurontin, Gralise, Horizant, others)
Inhibits α2δ subunit of L-type voltage-gated Ca2+ channels, which inhibits glutamate release
Gabapentin IR: 1,200 mg-3,600 mg/day in 3-4 divided doses
Horizant: 600 mg once or twice daily
Gralise: 300 to 800 mg once daily
Hepatic: none
Renal: CrCl >30-59 mL/min: 200-700 mg twice daily
CrCl >15-29 mL/min: 200-700 mg/day
CrCl ≤15 mL/min: 100-300 mg/day
Peripheral edema, weight gain, cognitive decline and memory loss
Nonlinear absorption with high intersubject variability
Eliminated in the urine as unchanged drug
CNS depressants
Pregabalin2,37
(Lyrica)
Inhibits α2δ subunit of L-type voltage-gated Ca2+ channels, which inhibits glutamate release
75-300 mg/day in 2-3 divided doses
Hepatic: none Renal: CrCl >30-59 mL/min: 300 mg/day in 2-3 divided doses
CrCl >15-29 mL/min: 150 mg/day in 1-2 divided doses
CrCl 15 mL/min: 75 mg daily
Peripheral edema, weight gain, cognitive decline, and memory loss; better tolerated than gabapentin
Linear absorption
More predicted PK profile compared to gabapentin
Eliminated in the urine as unchanged drug
CNS depressants
Diazepam 2,7 (Diazepam, Intensol, Valium, others)
GABAA receptor agonist
Increases chloride conductance, which results in presynaptic inhibition in the spinal cord
Starting dose: 2 mg orally 2-3 times daily or 5 mg at night for nocturnal spasticity
Target dose: 40-60 mg/day in divided doses
Renal: N/A
Hepatic: contraindicated in severe hepatic impairment
Cognitive impairment, potential for dependence or abuse, withdrawal syndrome with abrupt discontinuation
Metabolism: CYP3A4 and 2C19
Eliminated in the urine as glucuronide conjugates
CNS depressants
↑ Exposure with CYP3A4 inhibitors (eg, amiodarone, cyclosporine, fluconazole, fluoxetine, isoniazid, ketoconazole, ritonavir, verapamil)
CYP2C19 inhibitors (eg, celecoxib, chloramphenicol, fluoxetine, fluvoxamine, omeprazole)
↓ Exposure with CYP3A4 inducers (eg, carbamazepine, glucocorticoids, phenobarbital, phenytoin, rifampin, St. John’s wort)
CYP2C19 inducers (eg, carbamazepine, norethisterone, rifampin)
8
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

Table 3. Agents Used for Treatment of Spasticity
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic/Renal Impairment
Unique Adverse Effects Pharmacokinetics Drug Interactions
Baclofen 2,17-19
(Gablofen, Lioresal, others)
GABAB receptor agonist
Inhibits presynaptic and postsynaptic glutamate release
Starting dose: 5 mg orally 3 times daily
Increase by 5 mg per dose every 3 days
MDD: 80 mg
Hepatic: none
Renal: none
Transient dizziness that usually resolves with continued therapy, withdrawal syndrome with abrupt discontinuation
Metabolism: 15% of the dose undergoes hepatic deamination
Elimination: 70%-85% of the dose is renally excreted as unchanged drug in urine
CNS depressants
Tizanidine2,6,27-32 (Zanaflex, others)
Structurally similar to clonidine
Centrally acting alpha2 agonist
Inhibits presynaptic and postsynaptic alpha
1 motor
neurons
Could potentiate the actions of glycine
Starting dose: 2-4 mg orally 3 times a day
Titrate to MDD of 36 mg/day in 3 divided doses
Hepatic: avoid use; if used, reduce initial dose during titration
Renal: CrCl <25 mL/min: use with caution
Hypotension (20% decrease in blood pressure), mild LFT elevations (usually reversible), withdrawal syndrome with abrupt discontinuation
Bioavailability depends on formulation and food:
•Fasting: capsules and tablets are bioequivalent
•With meal: capsule has 25% less bioavailability than tablet
Metabolism: CYP1A2
Elimination: 60% urine and 20% feces
CNS depressants
↑ Exposure with CYP1A2 inhibitors (eg, fluvoxamine ciprofloxacin, oral contraceptives, verapamil)
↓ Exposure CYP1A2 inducers (eg, tobacco)
Gabapentin2,36,39,40
(Neurontin, Gralise, Horizant, others)
Inhibits α2δ subunit of L-type voltage-gated Ca2+ channels, which inhibits glutamate release
Gabapentin IR: 1,200 mg-3,600 mg/day in 3-4 divided doses
Horizant: 600 mg once or twice daily
Gralise: 300 to 800 mg once daily
Hepatic: none
Renal: CrCl >30-59 mL/min: 200-700 mg twice daily
CrCl >15-29 mL/min: 200-700 mg/day
CrCl ≤15 mL/min: 100-300 mg/day
Peripheral edema, weight gain, cognitive decline and memory loss
Nonlinear absorption with high intersubject variability
Eliminated in the urine as unchanged drug
CNS depressants
Pregabalin2,37
(Lyrica)
Inhibits α2δ subunit of L-type voltage-gated Ca2+ channels, which inhibits glutamate release
75-300 mg/day in 2-3 divided doses
Hepatic: none Renal: CrCl >30-59 mL/min: 300 mg/day in 2-3 divided doses
CrCl >15-29 mL/min: 150 mg/day in 1-2 divided doses
CrCl 15 mL/min: 75 mg daily
Peripheral edema, weight gain, cognitive decline, and memory loss; better tolerated than gabapentin
Linear absorption
More predicted PK profile compared to gabapentin
Eliminated in the urine as unchanged drug
CNS depressants
Diazepam 2,7 (Diazepam, Intensol, Valium, others)
GABAA receptor agonist
Increases chloride conductance, which results in presynaptic inhibition in the spinal cord
Starting dose: 2 mg orally 2-3 times daily or 5 mg at night for nocturnal spasticity
Target dose: 40-60 mg/day in divided doses
Renal: N/A
Hepatic: contraindicated in severe hepatic impairment
Cognitive impairment, potential for dependence or abuse, withdrawal syndrome with abrupt discontinuation
Metabolism: CYP3A4 and 2C19
Eliminated in the urine as glucuronide conjugates
CNS depressants
↑ Exposure with CYP3A4 inhibitors (eg, amiodarone, cyclosporine, fluconazole, fluoxetine, isoniazid, ketoconazole, ritonavir, verapamil)
CYP2C19 inhibitors (eg, celecoxib, chloramphenicol, fluoxetine, fluvoxamine, omeprazole)
↓ Exposure with CYP3A4 inducers (eg, carbamazepine, glucocorticoids, phenobarbital, phenytoin, rifampin, St. John’s wort)
CYP2C19 inducers (eg, carbamazepine, norethisterone, rifampin)
9
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

dry mouth but more frequent dizzi-ness.67 Of particular danger is the risk of psychological dependence with pro-longed use, which is likely due to the meprobamate metabolite.68 Withdrawal symptoms have been reported with abrupt cessation of therapy.
Orphenadrine is an anticholiner-gic agent that is structurally similar to diphenhydramine but has a stronger antagonistic effect on the histamine H1 receptor.69 Orphenadrine appears to inhibit antimuscarinic Ach and N-methyl-D-aspartate receptors in the CNS. It undergoes hepatic metabo-lism, and the metabolites are primarily eliminated in the urine. The most com-mon AEs are related to its anticholin-ergic profile and dose. AEs include dry mouth, sedation, constipation, ocular hypertension, palpitations, and sinus tachycardia. Rare cases of aplastic ane-mia have been reported but no causal relationship has been established.
The mechanism of action of metax-alone has not been established. It has no direct effect on skeletal muscles or nerve fibers, but CNS depression may be responsible for its effects.70 When taken with a high-fat meal, the bioavailability and AUC of metax-alone is increased. Metaxalone under-goes hepatic metabolism by CYP1A2, CYP2D6, CYP2E1, and CYP3A4, and its metabolites are excreted through the kidneys. Metaxalone is contraindi-cated in patients with renal or hepatic impairment. 70
AEs include dizziness, headache, nervousness, epigastric discomfort, and increased risk for respiratory depression in patients taking opioids, benzodiazepines, and barbiturates. Compared to other agents within the class, metaxalone has a relatively low risk of drowsiness or cognitive defects.71 Paradoxical muscle cramping has been documented with its use.71
Chlorzoxazone was FDA approved in 1958 as an adjunct for relief of dis-comfort associated with acute mus-culoskeletal conditions.72 Data from animal studies showed that it acts pri-marily at the level of the spinal cord and subcortical areas of the brain, which results in inhibition of multi-synaptic reflex arcs involved in mus-cle spasms. It undergoes hepatic glu-curonidation into an inactive metab-olite that is excreted in the urine.73 Chlorzoxazone can cause orange, red, or purple urine discoloration.72
AEs include dizziness, somnolence, and occasional overstimulation. Rare cases of idiosyncratic hepatocellular toxicity have been reported.74 The manufacturer recommends immediate discontinuation if symptoms, includ-ing fever, rash, dark urine, or jaundice ,develop. Periodic LFT monitoring is recommended for patients on chronic therapy.72
Table 3. Agents Used for Treatment of Spasticity
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic/Renal Impairment
Unique Adverse Effects Pharmacokinetics Drug Interactions
Dantrolene2,46-48 (Dantrium, Revonto, others)
Hydantoin derivative related to phenytoin
Blocks the RyR1 channel and inhibits Ca2+ release from the sarcoplasmic reticulum
Week 1: 25 mg once daily Week 2: 25 mg 3 times daily Week 3: 50 mg 3 times daily Week 4: 100 mg 3 times daily
MDD: 400 mg
Discontinue if efficacy is not evident in 45 days
Hepatic: contraindicated in liver disease
Renal: N/A
Dose-dependent hepatotoxicity, diarrhea
Metabolism: CYP3A4
Elimination: -Feces 50% -Urine 25%
CNS depressants
↑ Exposure with CYP3A4 inhibitors (eg, amiodarone, cyclosporine fluconazole, fluoxetine, isoniazid, ketoconazole ritonavir, verapamil)
↓ Exposure with CYP3A4 inducers (eg, carbamazepine, glucocorticoids, phenobarbital, phenytoin, rifampin, St. John’s wort)
Riluzole41-45
(Rilutek, others)
Inhibits voltage-gated Na+ channels on glutaminergic nerve terminals
Inhibits glutamate release and postsynaptic receptor activation
50 mg orally twice daily on empty stomach
Hepatic: N/A
Renal: N/A
Dose-related LFT elevations, decreased lung function, pruritus
Bioavailability decreased when coadministered with food
Metabolism: CYP1A2
Eliminated in the urine 85% as glucuronide metabolites
↑ Exposure with CYP1A2 inhibitors (eg, ciprofloxacin, fluvoxamine, oral contraceptives, verapamil)
↓ Exposure with CYP1A2 inducers (eg, tobacco)
Botulinum toxin 49-56 (various products)
Inhibits presynaptic release of acetylcholine in the neuromuscular junction
Dosing depends on product — Rash and muscle weakness at the injection site, flu-like symptoms, and headache — —
CNS, central nervous system; CrCL, creatinine clearance estimate of renal function based on Cockcroft and Gault equation; GABA, gamma-aminobutyric acid; IR, immediate release; LFT, liver function tests; MDD, maximum daily dose; N/A, no information provided by the manufacturer; PK, pharmacokinetic; RYR1, ryanodine receptor 1
(continued)
10
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

Table 3. Agents Used for Treatment of Spasticity
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic/Renal Impairment
Unique Adverse Effects Pharmacokinetics Drug Interactions
Dantrolene2,46-48 (Dantrium, Revonto, others)
Hydantoin derivative related to phenytoin
Blocks the RyR1 channel and inhibits Ca2+ release from the sarcoplasmic reticulum
Week 1: 25 mg once daily Week 2: 25 mg 3 times daily Week 3: 50 mg 3 times daily Week 4: 100 mg 3 times daily
MDD: 400 mg
Discontinue if efficacy is not evident in 45 days
Hepatic: contraindicated in liver disease
Renal: N/A
Dose-dependent hepatotoxicity, diarrhea
Metabolism: CYP3A4
Elimination: -Feces 50% -Urine 25%
CNS depressants
↑ Exposure with CYP3A4 inhibitors (eg, amiodarone, cyclosporine fluconazole, fluoxetine, isoniazid, ketoconazole ritonavir, verapamil)
↓ Exposure with CYP3A4 inducers (eg, carbamazepine, glucocorticoids, phenobarbital, phenytoin, rifampin, St. John’s wort)
Riluzole41-45
(Rilutek, others)
Inhibits voltage-gated Na+ channels on glutaminergic nerve terminals
Inhibits glutamate release and postsynaptic receptor activation
50 mg orally twice daily on empty stomach
Hepatic: N/A
Renal: N/A
Dose-related LFT elevations, decreased lung function, pruritus
Bioavailability decreased when coadministered with food
Metabolism: CYP1A2
Eliminated in the urine 85% as glucuronide metabolites
↑ Exposure with CYP1A2 inhibitors (eg, ciprofloxacin, fluvoxamine, oral contraceptives, verapamil)
↓ Exposure with CYP1A2 inducers (eg, tobacco)
Botulinum toxin 49-56 (various products)
Inhibits presynaptic release of acetylcholine in the neuromuscular junction
Dosing depends on product — Rash and muscle weakness at the injection site, flu-like symptoms, and headache — —
ConclusionSkeletal muscle relaxants represent a diverse pharmacotherapeutic group of medications across several chemical classes that are structurally dissimilar. These agents are effective for spasticity, skeletal muscle spasms, or both. Because of the breadth of pharmacologic mech-anisms and variable pharmacokinetics, the drugs have a huge range of AEs and potential drug interactions. Considering that these agents are most often used in the elderly and also as adjuvants for the treatment of chronic pain patients with multiple comorbidities who are likely receiving a polypharmaceutical regimen (including opioids), skeletal muscle drug selection for each patient requires care-ful attention to these factors.
Authors’ Bios: At the time of this writing, Mena Raouf was a PharmD candidate, 2016, at Albany College of Pharmacy and
Health Sciences, with a concentration in nephrology. He is currently a PGY-1 phar-macy resident at Veterans Administration (VA) Tennessee Valley Healthcare System.
Dr. Raouf completed an advanced pharmacy practice rotation in pain man-agement under the mentorship of Dr. Jeffrey Fudin at the Stratton VA Medical Center. He has been involved in devel-oping an automated software platform to assess pre-validated risk for opioid- induced respiratory depression to qualify patients for in-home naloxone.
Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHP, is president and direc-tor, Scientific and Clinical Affairs REMITIGATE LLC and a clinical pharmacy specialist at the Stratton VA Medical Center. He is an adjunct asso-ciate professor of Pharmacy Practice at Western New England University College of Pharmacy; adjunct associate professor of Pharmacy Practice at Albany College
of Pharmacy; adjunct assistant professor of Pharmacy Practice at the University of Connecticut School of Pharmacy. He is a diplomate of the American Academy of Pain Management, a fellow of the American College of Clinical Pharmacy and the American Society of Health-system Pharmacists. Dr. Fudin is a sec-tion editor for Pain Medicine, the offi-cial journal of AAPM. He is Founder/Chairman of Professionals for Rational Opioid Monitoring & Pharmacotherapy (PROMPT), a group that advocates in favor of safe opioid prescribing by encour-aging clinician education, proactive risk stratification, and appropriate therapeu-tic monitoring.
Dr. Fudin disclosed that his involve-ment with this article was not part of his official government duties. Practical Pain Management readers will recognize Dr. Fudin as one of the co-developers of the PPM Opioid Calculator.
11
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

Table 4. Agents Used for Treatment of Musculoskeletal Spasms
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic /Renal Impairment
Adverse Effects and Clinical Pearls Pharmacokinetics Drug Interactions
Cyclobenzaprine2,58,61
(Amrix, Fexmid, Flexeril, others)
Structurally similar to amitriptyline
CNS depressant acting primarily at the brain stem level
Reduces excitability of alpha and gamma motor neurons
5 mg orally 3 times daily
May increase to 7.5 mg or 10 mg 3 times daily for 2-3 weeks
May consider initially dosing at bedtime to gauge tolerance
Elderly: 5 mg orally and less frequent dosing
Hepatic:
Mild: 5 mg initial dosing and titrate with caution
Moderate-severe: use is not recommended
Renal: N/A
Anticholinergic effects (dizziness, dry mouth, constipation, urinary retention, ocular hypertension), palpitations, sinus tachycardia, cardiac conduction disturbances
Treatment is not recommended beyond 3 weeks; avoid in the elderly; use caution in patients with underlying cardiac conduction problems or arrhythmias; avoid in patients with closed angle glaucoma
Metabolism: CYPA12 (major), CYP3A4 and CYP2D6 (minor)
Elimination: Urine as glucuronide conjugates (major); feces as unchanged drug (minor)
CNS depressants
Serotonergic agents
↑ Exposure with CYP1A2 inhibitors (eg, ciprofloxacin, fluvoxamine, oral contraceptives, verapamil)
↓ Exposure with CYP1A2 inducers (eg, tobacco)
Methocarbamol62,63 (Robaxin, others)
Carbamate derivative of guaifenesin
Unknown mechanism but is thought to cause myo-relaxation via sedation
Initial dose: 1,500-2,000 mg orally 4 times daily for 2-3 days
Maintenance dose: 750-1,000 mg orally 3-4 times daily
Hepatic: N/A
Oral: N/A
Parenteral: use is contraindicated due to presence of propylene glycol in the formulation
Sedation, vertigo, confusion, headache, visual disturbances, amnesia, nausea, and dyspepsia; bradycardia, hypotension, syncope, muscle coordination abnormalities and grand mal seizures; urine discoloration (brown, green)
Metabolism: hepatic dealkylation, hydroxylation, conjugation
Elimination: urine
CNS depressants
Carisoprodol64-68 (Soma, others)
Interrupts interneuronal activity in the descending reticular formation and spinal cord
Metabolized to meprobamate, which exerts barbiturate-like activity at the GABA
A
receptors
250-350 mg orally 4 times daily
Hepatic: N/A; use with caution due to extensive hepatic metabolism
Renal: N/A
Drowsiness, headache, vertigo, insomnia; psychological dependence, withdrawal syndrome, respiratory depression when used with opioids, benzodiazepines, or barbiturates
Metabolism: CYP2C19
Elimination: renal and non-renal routes
↑ Exposure with CYP2C19 inhibitors (eg, celecoxib, chloramphenicol, fluoxetine, fluvoxamine, omeprazole)
↓ Exposure with CYP2C19 inducers (eg, carbamazepine, norethisterone, rifampin)
Orphenadrine69
(Norflex, others)
Anticholinergic receptor antagonist
H1 receptor antagonist
NMDA receptor antagonist
Structurally similar to diphenhydramine
100 mg orally twice dailyHepatic: N/A
Renal: N/A
Anticholinergic effects (dizziness, dry mouth, constipation, urinary retention, ocular hypertension, palpitations, sinus tachycardia); rare aplastic anemia
Metabolism: Hepatic N-didesmethylation and conjugation
Elimination: Urine
CNS depressants
Metaxalone 71,72 (Metaxall, Skelaxin, others)
Unknown mechanism but is thought to cause myorelaxation via sedation
800 mg orally 3-4 times daily
Hepatic: N/A; use is contraindicated with severe hepatic impairment
Renal: N/A; use is contraindicated with severe renal impairment
Dizziness (less frequent), irritability, nausea, gastrointestinal upset; contraindicated in patients with hepatic impairment
Paradoxical muscle cramps and respiratory depression when used with opioids, benzodiazepines, or barbiturates; contraindicated in serious liver or renal impairment
Co-administration with food increases bioavailability
Metabolism:
•CYP1A2•CYP2D6•CYP2E1•CYP3A4
Elimination: urine
CNS depressants
Increased risk for respiratory depression with opioids, benzodiazepines, barbiturates
Chlorzoxazone73-75 (Lorzone, Parafon Forte DSC, others)
Acts primarily on at the spinal cord and subcortical areas of the brain to inhibit multi-synaptic reflex arc
Initial dose: 250-500 mg orally 3-4 times daily
MDD: 750 mg orally 3-4 times daily
Hepatic: N/A
Renal: N/A
Dizziness, sedation, irritability, nausea, and gastrointestinal upset; respiratory depression when used with opioids, benzodiazepines, or barbiturates; rare idiosyncratic hepatotoxicity, urine discoloration (orange, red, or purple)
Metabolism: Hepatic glucuronidation
Elimination: urine
CNS depressants
Increased risk for respiratory depression with opioids, benzodiazepines, barbiturates
CNS, central nervous system; CrCL, creatinine clearance estimate of renal function based on Cockcroft and Gault equation; LFT, liver function test; MDD, maximum daily dose; N/A, no information provided by the manufacturer
12
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

Table 4. Agents Used for Treatment of Musculoskeletal Spasms
Medication Mechanism of Action Recommended Dosing Dose Adjustment for Hepatic /Renal Impairment
Adverse Effects and Clinical Pearls Pharmacokinetics Drug Interactions
Cyclobenzaprine2,58,61
(Amrix, Fexmid, Flexeril, others)
Structurally similar to amitriptyline
CNS depressant acting primarily at the brain stem level
Reduces excitability of alpha and gamma motor neurons
5 mg orally 3 times daily
May increase to 7.5 mg or 10 mg 3 times daily for 2-3 weeks
May consider initially dosing at bedtime to gauge tolerance
Elderly: 5 mg orally and less frequent dosing
Hepatic:
Mild: 5 mg initial dosing and titrate with caution
Moderate-severe: use is not recommended
Renal: N/A
Anticholinergic effects (dizziness, dry mouth, constipation, urinary retention, ocular hypertension), palpitations, sinus tachycardia, cardiac conduction disturbances
Treatment is not recommended beyond 3 weeks; avoid in the elderly; use caution in patients with underlying cardiac conduction problems or arrhythmias; avoid in patients with closed angle glaucoma
Metabolism: CYPA12 (major), CYP3A4 and CYP2D6 (minor)
Elimination: Urine as glucuronide conjugates (major); feces as unchanged drug (minor)
CNS depressants
Serotonergic agents
↑ Exposure with CYP1A2 inhibitors (eg, ciprofloxacin, fluvoxamine, oral contraceptives, verapamil)
↓ Exposure with CYP1A2 inducers (eg, tobacco)
Methocarbamol62,63 (Robaxin, others)
Carbamate derivative of guaifenesin
Unknown mechanism but is thought to cause myo-relaxation via sedation
Initial dose: 1,500-2,000 mg orally 4 times daily for 2-3 days
Maintenance dose: 750-1,000 mg orally 3-4 times daily
Hepatic: N/A
Oral: N/A
Parenteral: use is contraindicated due to presence of propylene glycol in the formulation
Sedation, vertigo, confusion, headache, visual disturbances, amnesia, nausea, and dyspepsia; bradycardia, hypotension, syncope, muscle coordination abnormalities and grand mal seizures; urine discoloration (brown, green)
Metabolism: hepatic dealkylation, hydroxylation, conjugation
Elimination: urine
CNS depressants
Carisoprodol64-68 (Soma, others)
Interrupts interneuronal activity in the descending reticular formation and spinal cord
Metabolized to meprobamate, which exerts barbiturate-like activity at the GABA
A
receptors
250-350 mg orally 4 times daily
Hepatic: N/A; use with caution due to extensive hepatic metabolism
Renal: N/A
Drowsiness, headache, vertigo, insomnia; psychological dependence, withdrawal syndrome, respiratory depression when used with opioids, benzodiazepines, or barbiturates
Metabolism: CYP2C19
Elimination: renal and non-renal routes
↑ Exposure with CYP2C19 inhibitors (eg, celecoxib, chloramphenicol, fluoxetine, fluvoxamine, omeprazole)
↓ Exposure with CYP2C19 inducers (eg, carbamazepine, norethisterone, rifampin)
Orphenadrine69
(Norflex, others)
Anticholinergic receptor antagonist
H1 receptor antagonist
NMDA receptor antagonist
Structurally similar to diphenhydramine
100 mg orally twice dailyHepatic: N/A
Renal: N/A
Anticholinergic effects (dizziness, dry mouth, constipation, urinary retention, ocular hypertension, palpitations, sinus tachycardia); rare aplastic anemia
Metabolism: Hepatic N-didesmethylation and conjugation
Elimination: Urine
CNS depressants
Metaxalone 71,72 (Metaxall, Skelaxin, others)
Unknown mechanism but is thought to cause myorelaxation via sedation
800 mg orally 3-4 times daily
Hepatic: N/A; use is contraindicated with severe hepatic impairment
Renal: N/A; use is contraindicated with severe renal impairment
Dizziness (less frequent), irritability, nausea, gastrointestinal upset; contraindicated in patients with hepatic impairment
Paradoxical muscle cramps and respiratory depression when used with opioids, benzodiazepines, or barbiturates; contraindicated in serious liver or renal impairment
Co-administration with food increases bioavailability
Metabolism:
•CYP1A2•CYP2D6•CYP2E1•CYP3A4
Elimination: urine
CNS depressants
Increased risk for respiratory depression with opioids, benzodiazepines, barbiturates
Chlorzoxazone73-75 (Lorzone, Parafon Forte DSC, others)
Acts primarily on at the spinal cord and subcortical areas of the brain to inhibit multi-synaptic reflex arc
Initial dose: 250-500 mg orally 3-4 times daily
MDD: 750 mg orally 3-4 times daily
Hepatic: N/A
Renal: N/A
Dizziness, sedation, irritability, nausea, and gastrointestinal upset; respiratory depression when used with opioids, benzodiazepines, or barbiturates; rare idiosyncratic hepatotoxicity, urine discoloration (orange, red, or purple)
Metabolism: Hepatic glucuronidation
Elimination: urine
CNS depressants
Increased risk for respiratory depression with opioids, benzodiazepines, barbiturates
CNS, central nervous system; CrCL, creatinine clearance estimate of renal function based on Cockcroft and Gault equation; LFT, liver function test; MDD, maximum daily dose; N/A, no information provided by the manufacturer
13
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com

References
1. Chou R, Peterson K. Drug Class Review: Skeletal Muscle Relaxants: Final Report [Internet]. http://www.ncbi.nlm.nih.gov/books/NBK10693/. Accessed May 30, 2016.
2. Kruidering-Hall M, Campbell L. Skeletal muscle relaxants. In: Katzung BG, Trevor AJ, eds. Basic & Clinical Pharmacology, 13th ed. New York, NY: McGraw-Hill; 2015.
3. Dillon C, Paulose-Ram R, Hirsch R, Gu Q. Skeletal muscle relaxant use in the United States: data from the third National Health and Nutrition Examination Survey (NHANES III). Spine. 2004;29(8):892-896.
4. Young RR. Spasticity: a review. Neurology. 1994;44(11 suppl 9):s12-s20.
5. Witenko C, Moorman-Li R, Motycka C, et al. Considerations for the appropriate use of skel-etal muscle relaxants for the management of acute low back pain. PT. 2014;39(6):427-435.
6. Tizanidine (Zanaflex) tablets [package insert]. Hawthorne, NY: Acorda Therapeutics, Inc.; November 2013.
7. Valium (diazepam) [package insert]. Nutley, NJ: Roche Laboratories, Inc.; January 2008.
8. Purves D, Augustine GJ, Fitzpatrick D, et al., eds. Neuroscience. 2nd ed. Sunderland, MA: Sinauer Associates; 2001.
9. Barrett KE, Boitano S, Barman SM, Brooks HL. Chapter 5. Excitable tissue: muscle. In: Barrett KE, Boitano S, Barman SM, Brooks HL, eds. Ganong’s Review of Medical Physiology, 24th ed. New York, NY: McGraw-Hill; 2012. http://accesspharmacy.mhmedical.com.acphs.idm.oclc.org/content.aspx?bookid=393&Section-id=39736743. Accessed May 30, 2016.
10. Lomen-Hoerth C. Nervous system disorders. In: Hammer GD, McPhee SJ (Eds). Pathophysiology of Disease: An Introduction to Clinical Medicine, 7th ed.. New York, NY: McGraw-Hill; 2013.
11. Lodish H, Berk A, Zipursky SL, et al. Molec-ular Cell Biology. 4th ed. New York, NY: W. H. Freeman; 2000.
12. Fill M, Copello JA. Ryanodine receptor calcium release channels. Physiol Rev. 2002;82(4):893-922.
13. Aminoff MJ. Neurologic causes of weakness and paralysis. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J (Eds). Harrison’s Principles of Internal Medicine, 19th ed. New York, NY: McGraw-Hill; 2015.
14. Ray NJ, Jones AJ, Keen P. GABA-B receptor modulation of the release of substance P from capsaicin-sensitive neurones in the rat trachea in vitro. Br J Pharmacol. 1991;102(4):801-804.
15. Chou R, Peterson K, Helfand M. Comparative efficacy and safety of skeletal muscle relaxants for spasticity and musculoskeletal conditions: a systematic review. J Pain Symptom Manage. 2004;28(2):140-175.
16. Rabchevsky AG, Kitzman PH. Latest approaches for the treatment of spasticity and autonomic dysreflexia in chronic spinal cord injury. Neu-rotherapeutics. 2011;8(2):274-282.
17. Baclofen [package insert]. Philadelphia, PA: Lannett Company, Inc.; December 2007.
18. Hwang AS, Wilcox GL. Baclofen, gamma-ami-nobutyric acid B receptors and substance P in the mouse spinal cord. J Pharmacol Exp Ther. 1989;248(3):1026-1033.
19. Gablofen (baclofen) injection [package insert]. St Paul, MN: CNS Therapeutics Inc.; February 2015.
20. Hering-Hanit R, Gadoth N. The use of baclofen in cluster headache. Curr Pain Headache Rep. 2001;5(1):79-82.
21. Guelaud C, Similowski T, Bizec JL, Cabane J, Whitelaw WA, Derenne JP. Baclofen therapy for chronic hiccup. Eur Respir J. 1995;8(2):235-237.
22. de Beaurepaire R. The use of very high-doses of baclofen for the treatment of alcohol-de-pendence: a case series. Front Psychiatry. 2014;5:143.
23. Franklin TR, Harper D, Kampman K et al. The GABA B agonist baclofen reduces cigarette consumption in a preliminary double-blind pla-cebo-controlled smoking reduction study. Drug Alcohol Depend. 2009;103(1-2):30-36.
24. Shoptaw S, Yang X, Rotheram-Fuller EJ, et al. Randomized placebo-controlled trial of baclofen for cocaine dependence: preliminary effects for individuals with chronic patterns of cocaine use. J Clin Psychiatry. 2003;64(12):1440-1448.
25. Terrence CF, Fromm GH. Complications of baclofen withdrawal. Arch Neurol. 1981;38(9):588-589.
26. Ross JC, Cook AM, Stewart GL, Fahy BG. Acute intrathecal baclofen withdrawal: a brief review of treatment options. Neurocrit Care. 2011;14(1):103-108.
27. Coward DM. Selective muscle relaxant prop-erties of tizanidine and an examination of its mode of action. Triangle. 1981;20:151-158.
28. Milanov I, Georgiev D. Mechanisms of tizanidine action on spasticity. Acta Neurol Scand. 1994;89(4):274-279.
29. Saper JR, Lake AE 3rd, Cantrell DT, Winner PK, White JR. Chronic daily headache prophylaxis with tizanidine: a double-blind, placebo con-trolled, multicenter outcome study. Headache. 2002;42(6):470-482.
30. Granfors MT, Backman JT, Neuvonen M, Neuvonen PJ. Ciprofloxacin greatly increases concentrations and hypotensive effect of tizanidine by inhibiting its cytochrome P450 1A2-mediated presystemic metabolism. Clin Pharmacol Ther. 2004;76(6):598-606.
31. Granfors MT, Backman JT, Laitila J, Neuvonen PJ. Oral contraceptives containing ethinyl estradiol and gestodene markedly increase plasma concentrations and effects of tizanidine by inhibiting cytochrome P450 1A2. Clin Phar-macol Ther. 2005;78(4):400-411.
32. Mörkl S, Bengesser SA, Schöggl H, Bayer D, Kapfhammer HP. [Tizanidine withdrawal symp-toms in stress cardiomyopathy]. Fortschr Neurol Psychiatr. 2015;83(3):170-173.
33. Priebe MM, Sherwood AM, Graves DE, Mueller M, Olson WH. Effectiveness of gabapentin in controlling spasticity: a quantitative study. Spinal Cord. 1997;35(3):171-175.
34. Gruenthal M, Mueller M, Olson WL, Priebe MM, Sherwood AM, Olson WH. Gabapentin for the treatment of spasticity in patients with spinal cord injury. Spinal Cord. 1997;35(10):686-689.
35. Bradley LJ, Kirker SG. Pregabalin in the treat-ment of spasticity: a retrospective case series. Disabil Rehabil. 2008;30(16):1230-1232.
36. Neurontin (gabapentin) [package insert]. New York, NY: Parke Davis; September 2015.
37. Lyrica (pregabalin) [package insert]. New York, NY: Pfizer; June 2012.
38. Mueller ME, Gruenthal M, Olson WL et al. Gabapentin for relief of upper motor neuron symptoms in multiple sclerosis. Arch Phys Med Rehabil. 1997;78(5):521-524.
39. Gralise (gabapentin) extended-release tablets. [package insert]. Menlo Park, CA: Depomed Inc; April 2012.
40. Horizant (gabapentin enacarbil) extended-re-lease tablets. [package insert]. Research Triangle Park, NC: GlaxoSmithKline; May 2013.
41. Rilutek (riluzole) [package insert]. Cary, NC: Covis Pharmaceuticals Inc.; April 2016.
42. Foran E, Trotti D. Glutamate transporters and the excitotoxic path to motor neuron degener-ation in amyotrophic lateral sclerosis. Antioxid Redox Signal. 2009;11(7):1587-1602.
43. Miller RG, Mitchell JD, Lyon M, Moore DH. Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Amyotroph Lateral Scler Other Motor Neuron Disord. 2003;4(3):191-206.
44. Bensimon G, Lacomblez L, Meininger V. A controlled trial of riluzole in amyotrophic lateral sclerosis. ALS/Riluzole Study Group. N Engl J Med. 1994 3;330(9):585-591.
45. Landwehrmeyer GB, Dubois B, de Yébenes JG, et al. Riluzole in Huntington’s disease: a 3-year, randomized controlled study. Ann Neurol. 2007;62(3):262-272.
46. Dantrium capsules (dantrolene sodium) [pack-age insert]. Rochester, MI: JHP Pharmaceuti-cals; October 2011.
47. Cornette M, Gillard C, Borlee-Hermans G. [Fatal toxic hepatitis associated with administration of dantrolene (author’s transl)]. Acta Neurol Belg 1980;80:336-347.
48. Ogburn RM, Myers RL, Burdick GE. Letter: Hepatitis associated with dantrolene sodium. Ann Intern Med. 1976;84:53-54.
49. Münchau A, Bhatia KP. Uses of botulinum toxin injection in medicine today. BMJ. 2000;320:161-165.
50. Lebeda FJ, Cer RZ, Stephens RM, Mudunuri U.Temporal characteristics of botulinum neuro-toxin therapy. Expert Rev Neurother. 2010;10(1) 93-103.
51. de Paiva A, Meunier FA, Molgó J, Aoki KR, Dolly JO. Functional repair of motor endplates after botulinum neurotoxin type A poisoning: biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc Natl Acad Sci U S A. 1999;96(6):3200-3205.
52. Carruthers A. Botulinum toxin products over-view. Skin Therapy Lett. 2008;13(6):1-4.
14
A Review of Skeletal Muscle Relaxants for Pain Management
PracticalPainManagement.com | June 2016

53. Benecke R. Clinical relevance of botulinum toxin immunogenicity. BioDrugs. 2012;26(2):e1-e9.
54. Comella CL, Jankovic J, Shannon KM, et al. Comparison of botulinum toxin serotypes A and B for the treatment of cervical dystonia. Neurology. 2005;65(9):1423–1429.
55. Botox (onabotulinumtoxinA) [package insert]. Irvine, CA: Allergan, Inc.; January 2016.
56. Dysport (abobotulinumtoxinA) [package insert].. Scottsdale, AZ: Medicis Pharmaceutical Corp.; July 2015.
57. Scheiner JJ. Cyclobenzaprine in the treatment of local muscle spasm. In: Clinical Evaluation of Flexeril (Cyclobenzaprine HCI/MSD). Minneapo-lis, Minn.: Postgraduate Medicine Communica-tions; 1978:39-48.
58. Wong EC, Koenig J, Turk J. Potential interfer-ence of cyclobenzaprine and norcyclobenzap-rine with HPLC measurement of amitriptyline and nortriptyline: resolution by GC-MS analysis. J Anal Toxicol. 1995;19(4):218-224.
59. Tofferi JK, Jackson JL, O’Malley PG. Treatment of fibromyalgia with cyclobenzaprine: a me-ta-analysis. Arthritis Rheum. 2004;51(1):9-13.
60. Carette S, Bell MJ, Reynolds WJ et al. Com-parison of amitriptyline, cyclobenzaprine, and placebo in the treatment of fibromyalgia. A
randomized, double-blind clinical trial. Arthritis Rheum. 1994;37(1):32-40.
61. Amrix (cyclobenzaprine hydrochloride) capsule, extended release [package insert]. North Wales, PA: Teva Pharmaceuticals USA, Inc.; June 2013.
62. Robaxin (Methocarbamol oral tablets), West-ward Pharmaceutical Corp, Eatontown, NJ; 2009.
63. Preston EJ, Miller CB, Herbertson RK. A double-blind, multicenter trial of methocarba-mol (Robaxin) and cyclobenzaprine (Flexeril) in acute musculoskeletal conditions. Today’s Ther Trends. 1984;1(4):1-11.
64. Soma (carisoprodol) [package insert]. Somerset, New Jersey; Meda Pharmaceuticals, Inc.; October 2009.
65. Berger FM, Kletzkin M, Ludwig BJ, Margolin S. The history, chemistry, and pharmacology of ca-risoprodol. Ann NY Acad Sci. 1960;86:90-107.
66. Dalén P, Alvan G, Wakelkamp M, Olsen H. Formation of meprobamate from carisoprodol is catalysed by CYP2C19. Pharmacogenetics. 1996;6(5):387-394.
67. Rollings HE, Glassman JM, Soyka JP. Manage-ment of acute musculoskeletal conditions— Thoracolumbar strain or sprain: a double-blind
evaluation comparing the efficacy and safety of carisoprodol with cyclobenzaprine hydrochlo-ride. Curr Ther Res. 1983;34(6):917-928.
68. Reeves RR, Burke RS. Carisoprodol: abuse potential and withdrawal syndrome. Curr Drug Abuse Rev. 2010;3(1):33-38.
69. Ophenadrine citrate [package insert]. Scha-umburg, Illinois: Sagent Pharmaceuticals; December 2009.
70. Metaxalone [package insert]. Bristol, Tennessee: King Pharmaceuticals, Inc.; April 2008.
71. Beebe FA, Barkin RL, Barkin S. A clinical and pharmacologic review of skeletal muscle relax-ants for musculoskeletal conditions. Am J Ther. 2005;12(2):151-171.
72. Lorzone (chlorzoxazone) [package insert]. Sayreville, NJ. Vertical Pharmaceuticals; September 2014.
73. Desiraju RK, Renzi NL Jr, Nayak RK, Ng KT. Pharmacokinetics of chlorzoxazone in humans. J Pharm Sci. 1983;72(9):991-994.
74. Powers BJ, Cattau EL Jr, Zimmerman HJ. Chlor-zoxazone hepatotoxic reactions. An analysis of 21 identified or presumed cases. Arch Intern Med. 1986;146(6):1183-1186.
15
A Review of Skeletal Muscle Relaxants for Pain Management
June 2016 | Pract icalPainManagement.com