Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
J Ped Surg Case Reports 3 (2015) 367e370
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports .com
A rare cause for severe recurrent lower gastrointestinal bleeding in a12 year old patient
D. Belsha a, M. Thomson a,*, O. Jackson b, D. Hughes c, M. Cohen d, G. Murthi b
aDepartment of Paediatric Gastroenterology, Sheffield Children Hospital, Western Bank, Sheffield S102TH, UKbDepartment of Paediatric Surgery, Sheffield Children Hospital, Western Bank, Sheffield S102TH, UKcDepartment of Paediatric Radiology, Sheffield Children Hospital, Western Bank, Sheffield S102TH, UKdDepartment of Paediatric Histopathology, Sheffield Children Hospital, Western Bank, Sheffield S102TH, UK
a r t i c l e i n f o
Article history:Received 25 April 2015Received in revised form10 June 2015Accepted 13 June 2015
Key words:Duplication cystLower gastrointestinal hemorrhageRecurrent bleeding
* Corresponding author. Sheffield Children’s Hospittreonterology, UK.
E-mail address: [email protected] (M. Tho
2213-5766/� 2015 The Authors. Published by Elsevierhttp://dx.doi.org/10.1016/j.epsc.2015.06.006
a b s t r a c t
The cause for severe, recurrent lower gastrointestinal (LGI) bleeding in children can usually be diagnosedreadily by means of the commonly used investigative/diagnostic techniques such as colonoscopy,laparoscopy � laparotomy. Occasionally less commonly used investigations may be necessary to look formore elusive causes of LGI bleeding such as capsule endoscopy, angiography, technetium-99m (99m Tc)-labeled red blood cell (RBC) scintigraphy, cross-sectional imaging such as CT/MRI (including angiog-raphy) and laparotomy combined with on-table small bowel enteroscopy. We report a case of severe,recurrent LGI bleeding that had occurred over several years, where the cause remained elusive despitenumerous investigations and interventions. The etiology of this was eventually found to be a gastricduplication cyst infiltrating into adjacent transverse colon and causing bleeding from peptic ulceration inthe colon. The process by which this diagnosis was made and the lessons learned are discussed.� 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Case report Subsequently, from 9 years of age per rectal bleeding was more
An 11 year old female patient was transferred to our unit for asecond opinion in view of severe, recurrent and obscure LGIbleeding.
The first presentation of LGI bleed was at 6 weeks of age withintermittent history of fresh unaltered blood in her stool. Assump-tion of cow’s milk enteropathy was made and hence she was startedon hydrolyzed formula. At five months of age she was passing freshblood with clots and hence she was referred to the gastroenterologyteam. Upper GI endoscopy and ileo-colonoscopy were normal. Shehad a further large fresh PR bleeding with clots during infancy andmini-laparotomy occurred which excluded Meckel’s diverticulum.Over the following 8 years her presentations were infrequent andtended to be associated with viral illness (one to two per year). Inattempts to diagnose the cause of the LGI bleeding multiple in-vestigations occurred including: 2 upper GI endoscopies, 2 ileo-colonoscopies, double balloon enteroscopy (DBE), and 2 wirelesscapsule endoscopies. One capsule video revealed blood apparentlyin the distal ileum but no further diagnostic information.
al, Centre for Paediatric Gas-
mson).
Inc. This is an open access article u
significant leading to hemoglobin drop of 30e50 g/l on multipleoccasions necessitating blood transfusions. Bleeding episodes wereusually preceded by a few days’ history of poor appetite, weight lossand significant peri-umbilical pain which persisted until bleedingceased. A CT angiogram was normal but a formal catheter angio-gram suggested a right colonic source with a vascular blush. At age9.5 years a laparotomy with entire small bowel enteroscopy wasperformed with no diagnostic yield. Her small bowel appearednormal at laparotomy, except that therewas blood in the colon fromthe cecum distally. In view of the recurrent nature of the bleedingand the transfusion dependency (7 transfusions between 9 and 10.5years of age), a right hemi-colectomy from the terminal ileum to thehepatic flexure was performed at 10.5 years. She remained well fora fewmonths but then she had a further bleed. Shewas given 20mgof omeprazole daily throughout this period and subsequently.
Between 10 and 11 years of age she had two normal abdominalultrasounds and a red cell scan. The red cell scan showed a blush inthe pelvis which may have been from the transverse colon butrepeat colonoscopy was normal, albeit on two occasions goodmucosal visualization was prevented by the presence of largeamounts of blood in the colon.
Table 1 demonstrates the summary of investigations performedbefore the definitive diagnosis was reached. At 11.5 years a qua-ternary opinion was sought following further large per-rectal
nder the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

D. Belsha et al. / J Ped Surg Case Reports 3 (2015) 367e370368
bleeding. After effective bowel clear-out colonoscopy revealed acolonic stricture with an adjacent polypoid lesion and ulceration ataround 30 cm from the anal verge. Injected contrast (on-table)showed an apple-core appearance of the stricture.
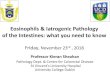
This was followed by a dual-injection single-phase (Afghantrauma protocol) contrast-enhanced CT abdomen which revealed a3e4 cm diameter rounded lesion with a fluid-filled center and astratified wall (Fig. 1), which was consistent with a duplication cystarising from the stomach or colon.
A few days later a further severe LGI bleed necessitated anemergency laparatomy. This was preceded by a colonoscopy andthe stricture was tattooed with methylene blue to facilitate serosalidentification at laparotomy. Upper GI endoscopy showed a 2 cmdome-shaped indentation into the stomach with no mucosal in-vasion or erosion (Fig. 2). At laparotomy a gastric duplication cystarising from the greater curve of the stomach was identified.Dissection revealed that this cyst was not communicating with thestomach but was infiltrating and fistulising into the adjacent colon
Fig. 1. Abdominal CT scan (coronal view) demonstrat
at the splenic flexure, resulting in an associated stricture of thecolon (Fig. 3). Stapled resection/anastomosis of the splenic flexurestricture was performed. The gastric duplication cyst was resectedby means of a stapled partial gastrectomy. Post-operative periodwas uneventful and patient was discharged one week later. Nofurther bleeding has been reported 6 months later. Histopatho-logical examination of the specimen showed regenerative changes,sub-mucosal fibrosis and ulcerated mucosa of the resected part oftransverse colonwith a duplication cyst showing perforated gastricduplication cyst with fundic type mucosa (Figs. 4 and 5).
2. Discussion
Significant LGI bleeding is usually investigated by means of analgorithm of sequential investigations and a cause can usually befound [1]. The appearance of a gastric duplication cyst in olderchildren can present a diagnostic dilemma. Due to their uncommonoccurrence there is no established diagnostic algorithm to aid in the
ing the position of the duplication cyst (arrow).

Fig. 2. Endoscopic appearance of the sub-mucosal bulge of the duplication cystthrough the greater curvature.
Fig. 4. Histological finding of the resected transverse colon: regenerative changes andsub-mucosal ulceration.
D. Belsha et al. / J Ped Surg Case Reports 3 (2015) 367e370 369
diagnosis and treatment of such a potentially life threatening GIbleeding.
Duplication cysts are defined by a smooth muscle coat, an inti-mate attachment to the native GI tract and a GI mucosal lining [2].Gastric duplication cysts are rare and account for only 4e8% of allduplication anomalies affecting the intestinal tract [3]. A majority ofduplication cysts occurred in females regardless of age with afemale to male ratio range from 2:1 to 4:1 reported to date [4].Occasionally identified by antenatal scan [5], the usual presentingsymptoms include PR bleeding, bowel obstruction, abdominal painor an abdominal mass usually in infancy but less commonly in olderchildren. Complications include torsion of pedunculated cysts,malignant changes, hemorrhage, pancreatitis and fistula formation.Gastrointestinal bleeding is a rare presenting feature and may becaused by peptic ulcer formation due to the cyst containing gastricmucosa. The bleeding can be painless, brisk and life threatening,with the first bleed occurring usually early in life [6].
Fig. 3. Intraoperative gastric duplication cyst fistulising into the transverse colon.
Amouei et al. reported a paediatric patient with hematemesisand melena and endoscopic appearance of a large sub-mucosalmass in the fundus of stomach with a large 3 cm2 ulcer noted with asignificant artery at its base e differential diagnoses consideredincluded leiomyoma or gastrointestinal stromal tumor (GIST) [7].
Interestingly, a review of the article reveals only 3 other similarcases where a gastric duplication cyst caused fresh LGI bleeding byinfiltrating into the adjacent colon [8e10]. The first described a 5month old with severe lower gastrointestinal bleeding due to agastric cyst eroding into the transverse colon [8], whereas anothercase reported an intra-pancreatic gastric duplication cyst causingmassive lower gastrointestinal bleeding in an 8 month old resultingfrom a peptic ulceration of the adherent jejunum [9]. Surridge et al.[10] describe rectal bleeding in a 13 month old from a perforatedgastric duplication cyst that had eroded into the right lobe of theliver as well as the hepatic flexure of the colon. Although it isdifficult to diagnose GDC preoperatively, recent imaging modalitieshave provided some informative findings. CT scan and endoscopicultrasound (EUS) are the best ways to identify GDC [11]. It is of note
Fig. 5. Fundic type mucosa of gastric duplication cyst.

Table 1Summary of the investigations performed prior to the definitive diagnosis.
Upper gastrointestinal endoscopy and ileo-colonoscopy (3 episodes)Mini-laparotomyWireless capsule endoscopy (3 episodes)Laparoscopy with double balloon enteroscopy laparotomy and on-table small
bowel enteroscopyCT angiographyRed cell-labeled bleeding isotope scan
D. Belsha et al. / J Ped Surg Case Reports 3 (2015) 367e370370
that the duplication cyst was not identified during the mini-lapa-rotomy the year before the diagnosis. Possible explanations for thismight be the cyst was in development, was varying in size atdifferent times or that the left-side of the colon was not examined.
Why the gastric duplication preferentially infiltrates into theadjacent colon rather than into the gastric lumen remains unclear.In this case it was clear at laparotomy that this was a gastricduplication as it shared muscle and serosal layers with the stomachand the involvement with the colon was only secondary to fistuli-sation. It is known that colonic duplication cysts can contain gastricmucosa but this is not the case here.
Once a gastric duplication cyst is detected, surgical excision ofthe entire gastric cyst remains the treatment of choice in allcomplicated intra-abdominal enteric duplications [3].
Other bleeding duplication cysts are well documented in theliterature. Duodenal duplication cysts can lead to GI bleeding as aresult of peptic ulceration of the ectopic gastric mucosa within thecyst and eroding the duodenal wall [12]. Ileal duplication cysts canpresent with LGIB of varying severity e stool occult blood positivitywith anemia to fresh bleeding per rectum. Diagnosis can be madeby Tc(99m) pertechnecium scan, DBE and laparotomy [13]. Rectalduplication cyst can present at times with per rectal bleedingdescribed in adults [14].
We feel that in this case the diagnosis e which had remainedelusive over a period of 11 years e may have been aided by acombination of disease progression leading to the development ofsignificant changes in the colon enabling visualization at colonos-copy and on cross-sectional imaging of the abdomen (CT scan). Theprevious CT did not detect the lesion probably because it was per-formed as an angiogram (with no portal venous phase) and becausethe scan area was limited and did not include the whole upperabdomen.
The second consideration is that previous colonoscopies suf-fered from poor vision due to acute bleeding and blood obscuringthe abnormal mucosal appearances. Referral to a different team ofclinicians who are approaching the problem as newmay have beena factor.
A review of the management preceding referral to the quater-nary GI bleeding unit reveals the following possible lessons:
� The importance of ‘starting again’ with referrals from other ter-tiary centers;
� Colonoscopy with good mucosal visualization and bowel prepa-ration that is adequate;
� Lesion recognition on concurrent upper GI endoscopy; and that� CT angiography alone is not good enough for anatomical lesion
identification.
A dual injection CT scan with simultaneous arterial and venousphase contrast can be used to identify lesions as well as delineatethe mesenteric vessels.
In conclusion, this case demonstrates the challenges in diagnosingrare conditions despite the availability of a variety of investigationmodalities at the disposal of the paediatric gastroenterologist andsurgeon. Amulti-disciplinary approach, teamwork and the sharing ofdifficult problems between teams and institutions is best practice andis most likely to yield a positive and safe result.
References
[1] Ghosh S, Watts D, Kinnear M. Management of gastrointestinal haemorrhage.Postgrad Med J 2002 Jan;78(915):4e14. Review.
[2] Chang HC, Huang SC, Wu RC, Yu MC. Duodenal duplication cyst: a rare cause ofgeriatric gastrointestinal bleeding. J Chin Med Assoc 2011;74:233e6.
[3] D’Journo XB, Moutardier V, Turrini O, Guiramand J, Lelong B, Pesenti C, et al.Gastric duplication in an adult mimicking mucinous cystadenoma of thepancreas. J Clin Pathol 2004 Nov;57(11):1215e8.
[4] Kim DH, Kim JS, Nam ES, Shin HS. Foregut duplication cyst of the stomach.Pathol Int 2000 Feb;50(2):142e5.
[5] Ford WD, Guelfand M, López PJ, Furness ME. Laparoscopic excision of a gastricduplication cyst detected on antenatal ultrasound scan. J Pediatr Surg 2004Oct;39(10):e8e10.
[6] Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etio-logic, and radiologic considerations. Radiographics 1993;13:1063e80.
[7] Amouei A, Pourrashidi AB, Rahnama A. Foregut duplication cyst as a rare causeof hematemesis: a case report. J Pak Med Stud 2013;3(3):123e6.
[8] Da Costa JM, Mariz CM, de Sousa JA, Gonzaga RA, de Sousa RM, dos Santos NT.Gastric duplication presenting rectal bleeding. A clinical case supportingMcLedtchie’s theory. Arq Gastroenterol 1993 Apr-Sep;30(2e3):62e4.
[9] Rao KL, Sunil I, Pimpalwar A, Vaiphei K, Chowdhary S. Intrapancreatic gastricduplication cyst presenting as lower gastrointestinal bleeding. J Pediatr Surg2003 Feb;38(2):243e4.
[10] Surridge CA, Goodier MD. Gastric duplication cyst: a cause of rectal bleeding ina young child. Afr J Paediatr Surg 2014 Jul-Sep;11(3):267e8.
[11] Theodosopoulos T,Marinis A, KarapanosK, VassilikostasG, DafniosN, Samanides L,et al. Foregut duplication cysts of the stomachwith respiratory epithelium.World JGastroenterol 2007 Feb 28;13(8):1279e81.
[12] Pandey S, Srivastava A, Lal R, Yachha SK, Poddar U. Enteric duplication cysts inchildren: a target in algorithm for evaluation of lower gastrointestinalbleeding. Indian J Gastroenterol 2014 May;33(3):285e8.
[13] Ko SY, Ko SH, Ha S, KimMS, Shin HM, Baeg MK. A case of a duodenal duplicationcyst presenting as melena. World J Gastroenterol 2013 Oct 14;19(38):6490e3.
[14] Jackson KL, Peche WJ, Rollins MD. An unusual presentation of a rectal dupli-cation cyst. Int J Surg Case Rep 2012;3(7):314e5.