Embed Size (px)
Citation preview

DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al therapy for Lyme encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic
This information is current as of October 10 2007
httpwwwneurologyorgcontent7013992fullhtmllocated on the World Wide Web at
The online version of this article along with updated information and services is
0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology
A randomized placebo-controlled trialof repeated IV antibiotic therapy forLyme encephalopathy
BA Fallon MDJG Keilp PhDKM Corbera MDE Petkova PhDCB Britton MDE Dwyer MDI Slavov PhDJ Cheng MD PhDJ Dobkin MDDR Nelson PhDHA Sackeim PhD
ABSTRACT
Background Optimal treatment remains uncertain for patients with cognitive impairment thatpersists or returns after standard IV antibiotic therapy for Lyme disease
Methods Patients had well-documented Lyme disease with at least 3 weeks of prior IV antibiot-ics current positive IgG Western blot and objective memory impairment Healthy individualsserved as controls for practice effects Patients were randomly assigned to 10 weeks of double-masked treatment with IV ceftriaxone or IV placebo and then no antibiotic therapy The primaryoutcome was neurocognitive performance at week 12mdashspecifically memory Durability of bene-fit was evaluated at week 24 Group differences were estimated according to longitudinal mixed-effects models
Results After screening 3368 patients and 305 volunteers 37 patients and 20 healthy individu-als enrolled Enrolled patients had mild to moderate cognitive impairment and marked levels offatigue pain and impaired physical functioning Across six cognitive domains a significanttreatment-by-time interaction favored the antibiotic-treated group at week 12 The improvementwas generalized (not specific to domain) and moderate in magnitude but it was not sustained toweek 24 On secondary outcome patients with more severe fatigue pain and impaired physicalfunctioning who received antibiotics were improved at week 12 and this was sustained to week24 for pain and physical functioning Adverse events from either the study medication or the PICCline were noted among 6 of 23 (261) patients given IV ceftriaxone and among 1 of 14 (71)patients given IV placebo these resolved without permanent injury
Conclusion IV ceftriaxone therapy results in short-term cognitive improvement for patients withposttreatment Lyme encephalopathy but relapse in cognition occurs after the antibiotic is dis-continued Treatment strategies that result in sustained cognitive improvement areneeded Neurologyreg 200870992ndash1003
GLOSSARYCDC Centers for Disease Control and Prevention LMM longitudinal mixed-effects models NAART-R North AmericanAdult Reading Test-Revised PCS Physical Component Scale ITT intent-to-treat VAS visual analog scale WMS-III Wechsler Memory Scale
Lyme disease a tick-borne bacterial illness caused by Borrelia burgdorferi can inducecognitive deficits when it affects the CNS1 These deficits often mild to moderate inseverity extend across multiple domains of cognitive function including memory work-ing memory verbal fluency and psychomotor performance23 Although treatment with 4weeks of IV ceftriaxone usually results in marked improvement in a subgroup this treat-ment results in only partial or nonsustained benefit45 Posttreatment cognitive deficitsmay reflect residual effects of past infection continuing effects of current low-gradeB burgdorferi infection the presence of an unrecognized coinfection or incorrect diagno-
e-Pub ahead of print on October 10 2007 at wwwneurologyorg
From the Department of Psychiatry (BAF JGK KMC EP IS JC HAS) Department of Biostatistics (EP) Department ofNeurology (CBB) Department of Medicine (ED JD) and New York State Psychiatric Institute (BAF JGK KMC EP IS JCHAS) Columbia University New York and Department of Cell and Molecular Biology University of Rhode Island Kingston (DRN)
Primary location of research Columbia University Medical Center New York
This study was funded by a grant from NINDS to Dr Fallon (R01- NS38636)
Disclosure Roche Pharmaceuticals supplied ceftriaxone free of charge for this study but were not involved in any other aspect of the studyDr Fallon has given expert testimony at hearings related to Lyme disease and its treatment The other authors report no conflicts of interest
Supplemental data atwwwneurologyorg
Address correspondence andreprint requests to Dr BAFallon Columbia University1051 Riverside Drive Unit 69New York NY 10032baf1columbiaedu
Editorial page 986
ARTICLES
992 Copyright copy 2008 by AAN Enterprises Inc
sis Consequently clinicians are uncertainabout optimal treatment strategies For pa-tients in whom no other cause of symptomscan be found community practice varieswidely ranging from no treatment to pal-liative treatment to use of repeated or long-term antibiotic courses
To evaluate the benefit of additional IVantibiotic therapy we conducted a trial com-paring clinical improvement from 10 weeksof IV ceftriaxone vs IV placebo in patientswith previously treated Lyme disease whohad objectivememory impairment and a cur-rently positive IgGWestern blot
METHODS Study participants Between January 2000and April 2004 healthy volunteers (controls) and individualswith a history of Lyme disease (patients) between the ages of 18and 65 years were recruited follow-up evaluations were com-pleted byApril 2005 The institutional review boards at Colum-bia University and the New York State Psychiatric Instituteapproved the study and all participants provided written in-formed consent Evaluations were conducted at the New YorkState Psychiatric Institute and Columbia University MedicalCenter Treatments were conducted at each patientrsquos home Pa-tients met the following criteria (1) history of physician-documented erythema migrans or US Centers for DiseaseControl and Prevention (CDC)-defined manifestation of Lymedisease and a positive or equivocal ELISA confirmed by posi-tive Western blot serology67 (2) current positive IgG Westernblot using CDC surveillance criteria assessed using a single ref-erence laboratory (University Hospital of Stony Brook) (3)treatment for Lyme disease with at least 3 weeks of IV ceftriax-one completed at least 4 months before study entry (4) subjec-tive memory impairment that by participant report startedafter the onset of Lyme disease and (5) objective evidence ofmemory impairment as documented by the Wechsler MemoryScalendashIII8 compared with age- sex- and education-adjustedpopulation norms These study criteria were conservative andnarrow to enhance diagnostic confidence Prior IV antibiotictherapy was required to ensure that all patients had receivedtreatment considered adequate for neurologic Lyme disease bypublished guidelines910
The control sample of healthy volunteers had (1) nega-tive history of Lyme disease fibromyalgia or chronic fa-tigue (2) negative IgM and IgG Western blot for Lymedisease and (3) no evidence of memory impairment on neu-ropsychological testing
Patients and controls were excluded if their history re-vealed a prior learning disability or medical condition thatcould confound neuropsychological assessment Patientswith cephalosporin allergy or a history of major psychiatricdisorder before the onset of Lyme disease were also ex-cluded The control and patient samples were matched onthe mean variance and shapes of the distributions of ageand education and the distribution of gender
Study design Treatment The controlled phase of thisstudy consisted of 10 weeks of randomized treatment witheither IV ceftriaxone (2 gd) or IV placebo (09 normal
saline) and then 14 weeks off all antibiotics Ceftriaxonewas chosen because it is the recommended treatment forneurologic Lyme disease and has excellent penetration of thebloodndashbrain barrier9 A 10-week duration was chosen be-cause of reports of persistent or relapsing symptoms after 3weeks of IV ceftriaxone and because of case series suggest-ing that longer courses of antibiotic therapy may be moreeffective411 After week 24 treatment assignment was re-vealed by a research staff member not involved in data col-lection and no further constraints were placed onsubsequent care Participants underwent one follow-up as-sessment at week 48 This report concerns only the con-trolled phases of the study from baseline to week 24
Randomization Patients were assigned in a 21 ratio toIV ceftriaxone or IV placebo using permuted blocks of size20 based on a computer-based randomization list A 21 ran-domization schedule was used to encourage enrollment
Masking An unmasked off-site pharmacist who had nocontact with patients ensured that patients were sent theassigned treatment this pharmacist was the only unmaskedindividual during the 24 weeks of each patientrsquos maskedtreatment The neuropsychological technicians were notprivy to information about adverse events To assess successof masking patients were asked to guess treatment assign-ment at both the week 12 and 24 evaluations
Compliance with treatment Compliance and safetywere monitored by home infusion nurses who visited twiceweekly Patients had weekly telephone contact with a re-search physician and monthly in-person evaluations with thepatientrsquos private physician Study medication was packagedin pressured infusion devices numbered from 1 to 70 Boththe visiting nurse and the research physician recorded thenumber of completed infusions Patients who missed a dayrsquosdose were instructed to continue in consecutive sequence un-til all 70 doses were infused
Sample sizeThe target sample size of 45 Lymepatients (30randomized to active treatment and 15 randomized to placebo)provided at least 80power to detect an effect size of 11with atwo-sided test with 005 Power calculations were based onthe results of an uncontrolled pilot study4 with the outcomemeasure of memory assessed with the Buschke Selective Re-minding Test total verbal memory score Although cognitiveimprovement was expected in both visual and verbal memoryas well as in multiple other cognitive domains verbal memorywas selected for the power analysis given the lack of pilot datafor other aspects of cognition
Assessments Screening Subjects were screened for mem-ory impairment with the Wechsler Memory Scale (WMS-III)8 which measures immediate delayed and workingmemory in auditory and visual domains Demographicallyadjusted t scores were computed for all indices correctingfor the influence of sex ethnicity and education level Mem-ory impairment was defined as a t score of one or more SDbelow population norms on at least one of the six primaryWMS-III indices Premorbid IQ was estimated using the Ba-rona demographic formula12 and the North American AdultReading TestndashRevised (NAART-R)13
Outcome measures The primary clinical outcomemeasure assessed neurocognitive performance and theprimary biologic outcomes assessed brain structure andfunction Relative to the placebo and control groups IVantibiotic therapy was hypothesized to lead to superioroutcome in the memory domain scores as well as across
Neurology 70 March 25 2008 (Part 1 of 2) 993
cognitive domains The cognitive assessments sampled six do-mains motor function (finger tapping simple reaction timechoice reaction time) psychomotor function (Trail MakingAampB Digit Symbol) attention (Continuous Performance TestStroop task) memory (Buschke Selective Reminding Test [ver-bal memory] Benton Visual Retention Test [visual memory])working memory (A Not B Logical Reasoning Test N-BackTest) and verbal fluency (Controlled Oral Word AssociationTest and Category Fluency Test) Descriptions of these mea-sures may be found elsewhere1415 Scores on these tests were ztransformed relative to either published norms or a referencesample of healthy controls and were adjusted for the effects ofage gender and education Domain scores represent the aver-age of the z scores for the primary tests within each cognitivedomain To characterize overall performance the six domainscores were averaged to produce a cognitive ldquoindexrdquo score thisindexwas not used in the primarymixed-model analyses Brainimaging measures included MRI and PET scans these imagingresults will be reported elsewhere
Assessments of physical outcome included the rheumatolo-gistrsquos exam (trigger points total number of joints in pain at restor on movement) and self-report measures of fatigue (FatigueSeverity Scalendash1116) pain (McGill Pain QuestionnairendashShortForm17) and physical functioning (Short Formndash36 PhysicalComponent Scale [PCS]1819) Psychopathology was assessedwith respect to depression (Beck Depression Inventory20) anxi-ety (ZungAnxiety Scale21) mental functioning (SF-36MCS1819)and global symptoms (SCL-90 Global Symptom Index22)
Time of assessment Major assessments occurred at base-line week 12 and week 24 The primary end point for efficacyanalyses was week 12 The week 24 assessments evaluated du-rability of benefit Controls were assessed at the same timepoints to allow correction for the impact of practice effects onthe repeated neurocognitive measures The secondary outcomeself-report scales were collected at 4-week intervals (baselineand weeks 4 8 12 16 20 and 24) The rheumatologist examwas conducted at baseline week 12 and week 24 The lumbarpuncture (for patients) and neurology exam (for all partici-pants) were done only at baseline The neurologic exam as-sessed five areas cranial nerves reflexes sensory motor andassociated motor (cerebellar and basal ganglia) functions Forthe standardized neurology exam a summary score (0ndash5) indi-cated the number of areas with at least one minor or majorabnormal finding An objective neurologic abnormality wasconsidered major if it was associated with either a significantdeficit or impairment in the personrsquos functioning
Laboratory assessments Screening serum was sent forLyme IgM and IgGWestern blot testing Enrolled patients hadserum examined by IFA for signs of coinfection withAnaplasma phagocytophila (human granulocytic erhlichiosis)and Babesia microti (Babesiosis) Samples of whole blood andCSF were tested by PCR assay for B burgdorferi DNA usingthe plasmid ospA primer CSF was sent for cell count proteinglucose total gammaglobulin Lyme ELISA and oligoclonalbands Serum and CSF were sent for determination of Bb-specific intrathecal Ab production to University Hospital ofStony Brook using the whole-cell sonicate ELISA (positive cut-off 11) To determine whether viable B burgdorferi cellswere present spinal fluid was cultured in BSKII containingkanamycin (5 gmL) at 33degC and was checked weekly for upto 12 weeks
Statistical analysis Efficacy analyses were performed us-ing all randomized participants the intent-to-treat (ITT)
sample Lyme patient and healthy controls were comparedwith respect to demographic and baseline clinical character-istics using t tests for continuous measures and 2 tests forcategorical measures
Tests and estimates of differences between groups (IV anti-biotic IV placebo and healthy controls) with respect to themultivariate measure of cognition (six domains motor psy-chomotor working memory attention verbal fluency andmemory) over time (baselineweek 12 andweek 24)were basedon longitudinal mixed-effects models (LMM)23 which accountfor the correlation between the domains and between the re-peated observations over time24 The LMM included main ef-fects and all interaction terms Time was modeled as a nominalfactor rather than a continuous variable
Including all two- and three-way interactions the modelfor the covariance structure was selected based on maximiz-ing Bayesian information criteria2526 Keeping the model forthe covariance as selected stepwise backward eliminationwas used to select the ldquobestrdquo model for the mean structureInference regarding the comparison between the groups wasbased on the best model Significant omnibus tests for ITTdifferences among the three groups over time (two-sided
005) were followed by pairwise comparisons the p valuesfor these post hoc tests are reported unadjusted
Secondary outcome measures were analyzed with LMMsusing a similar strategy Healthy controls were not included be-cause practice effects were not of concern For the outcomenumber of joints with pain a Poisson variable an appropriategeneralized LMM23 was employed using log link As initiallyplanned the LMMs included the baseline value of the outcomeas a continuous covariate to account for heterogeneity in clini-cal characteristics and to remedy potential floor effects Thesignificance of the interaction terms was judged at a two-sided 015 to avoid the erroneous omission of potentially impor-tant effects for which the study was not powered the signifi-cance of a main effect for drug vs placebo was still judged at
005 To illustrate the impact on outcome of different base-line severity scores an estimate of the mean response based onthe best model for each outcome was computed at weeks 4 12and 24 for drug and placebo for hypothetical subjects withbaseline symptom severity equal to the lowest (first) or highest(third) quartile of the observed baseline severities The report-ing of outcomes for ldquolowrdquo and ldquohighrdquo baseline severity is forillustration purposes only the actual analysis based on LMMsincluded all patients and used baseline severity as a continuouscovariate without dichotomizing it into low and high valuesAll analyses were performed using SAS software version 925 theLMMswere fit using PROCMIXED and PROCGLIMMIX
To explore whether particular patient subgroups hadpreferential benefit from active treatment ANCOVAs testedfor associations between selected demographic clinical andlaboratory variables and the primary and secondary out-comes at week 12 and week 24 that had shown a treatmenteffect in the LMM analyses Treatment group baseline se-verity of the outcome measure and (dichotomous or contin-uous) potential predictor were examined as fully factorialbetween-subject factors
RESULTS Study population Healthy controls Of305 individuals contacted by telephone 58 wereinvited for on-site screening and 20 were en-rolled Reasons for exclusion included laboratoryabnormalities memory deficits on testing or
994 Neurology 70 March 25 2008 (Part 1 of 2)
other exclusions Of the 20 enrolled two partici-pants had impaired scores on baseline neuropsy-chological testing and were excluded
Patients Of 3368 initial clinic contacts 1439 wereexcluded because of insufficient prior IV treatmentand 1316 were excluded because the patient had notmet the CDC criteria for Lyme disease (figure)Among the remaining 613 patients 512 were ex-cluded because their serum was not IgG Westernblot positive and 20 were excluded for other rea-sons Of the 81 patients invited to Columbia forneuropsychological screening 31 did not have suffi-cient memory impairment 12 were not able to pro-vide adequate documentation of their clinicalhistory and one patient who had been deemed eligi-ble for the study withdrew for private treatment be-fore randomization Thirty-seven patients wererandomized to interventions representing 1 of allpatients screened for the study Of these 37 patientsfive withdrew from the study during the first 12weeks threewithin the first 3 weeks of therapy (twobecause of thrombus and one because of hemolyticanemia all three on antibiotic) one after 8 weeksbecause of a systemic infection (on placebo) andone after 10 weeks (on placebo) because of intolera-ble joint pain that required narcotic medications forrelief Three additional patients had adverse eventsthat required early termination of study medication(one at week 6 and two at week 8) but each of thesepatients continued in a masked fashion through tothe week 12 and 24 evaluations No patients with-
drew from the study between weeks 12 and 24
Laboratory results for enrolled patients Blood Allsamples were IgG WB positive and 18 of 37 wereIgM WB positive No patient samples were PCRpositive using the OspA primer assay None ofthe serum samples were IgM positive on either ofthe two coinfection tests whereas low positiveIgG results were noted on 4 of 37 (108) samplesfor Anaplasma phagocytophila and on 10 of 37(270) samples for Babesia microti
Cerebrospinal fluid Baseline lumbar punctureconducted in 33 of the 37 patients revealed few ab-normalities mildly elevated WBC (two samples)mildly elevated protein (four samples) and elevatedgammaglobulin (one sample) Positive results werenoted for 22 on Lyme ELISA 28 on IgG WB andnone on IgM WB For intrathecal Ab productionsamples tested positive for 4 of 31 (129) patientseach positive intrathecal sample was also seroposi-tive No patient had a positive CSF PCRWhen cul-tured one sample was positive for growth andrevealed spirochetes by both phase contrast anddark-field microscopy To exclude contaminationas an explanation the cellsrsquos DNA was extractedandwas used as a template for PCRamplification ofthe spoT gene Examination of the PCR ampliconby agarose gel electrophoresis revealed an approxi-mately 3-kbp band whereas a PCR amplicon fromwild-type strains was approximately 2 kbp Addi-tionally the B burgdorferi isolated from the CSFculture was able to grow when transferred intoBSKII containing kanamycin (5 gmL) plus strep-tomycin (100gmL) These results strongly suggestthat the B burgdorferi strain found in the CSF cul-ture was the result of contamination by a spoTmu-tant strain (WC07) of B burgdorferi containing adeletion of part of the spoT gene plus the insertionof a streptomycin resistance gene spoT mutantstrains were under investigation in the lab at thetime of the culture
Demographics and pretreatment clinical character-ization of patients and controls The patients andhealthy controls did not differ in the matchingvariables of age gender or education (table 1)The patientsrsquo clinical histories indicated that allhad rheumatologic symptoms and most had neu-rologic symptoms associated with cognitive com-plaints Nearly half (49) had had a prior lumbarpuncture only three of these patients had had ele-vated B burgdorferindashspecific intrathecal Ab pro-duction The total amount of prior antibiotictherapy for Lyme disease was extensive with57 of the patients in each treatment group hav-ing had more than 1 month of prior IV antibiotic
Figure Flow diagram of patient enrollment
Neurology 70 March 25 2008 (Part 1 of 2) 995
therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

A randomized placebo-controlled trialof repeated IV antibiotic therapy forLyme encephalopathy
BA Fallon MDJG Keilp PhDKM Corbera MDE Petkova PhDCB Britton MDE Dwyer MDI Slavov PhDJ Cheng MD PhDJ Dobkin MDDR Nelson PhDHA Sackeim PhD
ABSTRACT
Background Optimal treatment remains uncertain for patients with cognitive impairment thatpersists or returns after standard IV antibiotic therapy for Lyme disease
Methods Patients had well-documented Lyme disease with at least 3 weeks of prior IV antibiot-ics current positive IgG Western blot and objective memory impairment Healthy individualsserved as controls for practice effects Patients were randomly assigned to 10 weeks of double-masked treatment with IV ceftriaxone or IV placebo and then no antibiotic therapy The primaryoutcome was neurocognitive performance at week 12mdashspecifically memory Durability of bene-fit was evaluated at week 24 Group differences were estimated according to longitudinal mixed-effects models
Results After screening 3368 patients and 305 volunteers 37 patients and 20 healthy individu-als enrolled Enrolled patients had mild to moderate cognitive impairment and marked levels offatigue pain and impaired physical functioning Across six cognitive domains a significanttreatment-by-time interaction favored the antibiotic-treated group at week 12 The improvementwas generalized (not specific to domain) and moderate in magnitude but it was not sustained toweek 24 On secondary outcome patients with more severe fatigue pain and impaired physicalfunctioning who received antibiotics were improved at week 12 and this was sustained to week24 for pain and physical functioning Adverse events from either the study medication or the PICCline were noted among 6 of 23 (261) patients given IV ceftriaxone and among 1 of 14 (71)patients given IV placebo these resolved without permanent injury
Conclusion IV ceftriaxone therapy results in short-term cognitive improvement for patients withposttreatment Lyme encephalopathy but relapse in cognition occurs after the antibiotic is dis-continued Treatment strategies that result in sustained cognitive improvement areneeded Neurologyreg 200870992ndash1003
GLOSSARYCDC Centers for Disease Control and Prevention LMM longitudinal mixed-effects models NAART-R North AmericanAdult Reading Test-Revised PCS Physical Component Scale ITT intent-to-treat VAS visual analog scale WMS-III Wechsler Memory Scale
Lyme disease a tick-borne bacterial illness caused by Borrelia burgdorferi can inducecognitive deficits when it affects the CNS1 These deficits often mild to moderate inseverity extend across multiple domains of cognitive function including memory work-ing memory verbal fluency and psychomotor performance23 Although treatment with 4weeks of IV ceftriaxone usually results in marked improvement in a subgroup this treat-ment results in only partial or nonsustained benefit45 Posttreatment cognitive deficitsmay reflect residual effects of past infection continuing effects of current low-gradeB burgdorferi infection the presence of an unrecognized coinfection or incorrect diagno-
e-Pub ahead of print on October 10 2007 at wwwneurologyorg
From the Department of Psychiatry (BAF JGK KMC EP IS JC HAS) Department of Biostatistics (EP) Department ofNeurology (CBB) Department of Medicine (ED JD) and New York State Psychiatric Institute (BAF JGK KMC EP IS JCHAS) Columbia University New York and Department of Cell and Molecular Biology University of Rhode Island Kingston (DRN)
Primary location of research Columbia University Medical Center New York
This study was funded by a grant from NINDS to Dr Fallon (R01- NS38636)
Disclosure Roche Pharmaceuticals supplied ceftriaxone free of charge for this study but were not involved in any other aspect of the studyDr Fallon has given expert testimony at hearings related to Lyme disease and its treatment The other authors report no conflicts of interest
Supplemental data atwwwneurologyorg
Address correspondence andreprint requests to Dr BAFallon Columbia University1051 Riverside Drive Unit 69New York NY 10032baf1columbiaedu
Editorial page 986
ARTICLES
992 Copyright copy 2008 by AAN Enterprises Inc
sis Consequently clinicians are uncertainabout optimal treatment strategies For pa-tients in whom no other cause of symptomscan be found community practice varieswidely ranging from no treatment to pal-liative treatment to use of repeated or long-term antibiotic courses
To evaluate the benefit of additional IVantibiotic therapy we conducted a trial com-paring clinical improvement from 10 weeksof IV ceftriaxone vs IV placebo in patientswith previously treated Lyme disease whohad objectivememory impairment and a cur-rently positive IgGWestern blot
METHODS Study participants Between January 2000and April 2004 healthy volunteers (controls) and individualswith a history of Lyme disease (patients) between the ages of 18and 65 years were recruited follow-up evaluations were com-pleted byApril 2005 The institutional review boards at Colum-bia University and the New York State Psychiatric Instituteapproved the study and all participants provided written in-formed consent Evaluations were conducted at the New YorkState Psychiatric Institute and Columbia University MedicalCenter Treatments were conducted at each patientrsquos home Pa-tients met the following criteria (1) history of physician-documented erythema migrans or US Centers for DiseaseControl and Prevention (CDC)-defined manifestation of Lymedisease and a positive or equivocal ELISA confirmed by posi-tive Western blot serology67 (2) current positive IgG Westernblot using CDC surveillance criteria assessed using a single ref-erence laboratory (University Hospital of Stony Brook) (3)treatment for Lyme disease with at least 3 weeks of IV ceftriax-one completed at least 4 months before study entry (4) subjec-tive memory impairment that by participant report startedafter the onset of Lyme disease and (5) objective evidence ofmemory impairment as documented by the Wechsler MemoryScalendashIII8 compared with age- sex- and education-adjustedpopulation norms These study criteria were conservative andnarrow to enhance diagnostic confidence Prior IV antibiotictherapy was required to ensure that all patients had receivedtreatment considered adequate for neurologic Lyme disease bypublished guidelines910
The control sample of healthy volunteers had (1) nega-tive history of Lyme disease fibromyalgia or chronic fa-tigue (2) negative IgM and IgG Western blot for Lymedisease and (3) no evidence of memory impairment on neu-ropsychological testing
Patients and controls were excluded if their history re-vealed a prior learning disability or medical condition thatcould confound neuropsychological assessment Patientswith cephalosporin allergy or a history of major psychiatricdisorder before the onset of Lyme disease were also ex-cluded The control and patient samples were matched onthe mean variance and shapes of the distributions of ageand education and the distribution of gender
Study design Treatment The controlled phase of thisstudy consisted of 10 weeks of randomized treatment witheither IV ceftriaxone (2 gd) or IV placebo (09 normal
saline) and then 14 weeks off all antibiotics Ceftriaxonewas chosen because it is the recommended treatment forneurologic Lyme disease and has excellent penetration of thebloodndashbrain barrier9 A 10-week duration was chosen be-cause of reports of persistent or relapsing symptoms after 3weeks of IV ceftriaxone and because of case series suggest-ing that longer courses of antibiotic therapy may be moreeffective411 After week 24 treatment assignment was re-vealed by a research staff member not involved in data col-lection and no further constraints were placed onsubsequent care Participants underwent one follow-up as-sessment at week 48 This report concerns only the con-trolled phases of the study from baseline to week 24
Randomization Patients were assigned in a 21 ratio toIV ceftriaxone or IV placebo using permuted blocks of size20 based on a computer-based randomization list A 21 ran-domization schedule was used to encourage enrollment
Masking An unmasked off-site pharmacist who had nocontact with patients ensured that patients were sent theassigned treatment this pharmacist was the only unmaskedindividual during the 24 weeks of each patientrsquos maskedtreatment The neuropsychological technicians were notprivy to information about adverse events To assess successof masking patients were asked to guess treatment assign-ment at both the week 12 and 24 evaluations
Compliance with treatment Compliance and safetywere monitored by home infusion nurses who visited twiceweekly Patients had weekly telephone contact with a re-search physician and monthly in-person evaluations with thepatientrsquos private physician Study medication was packagedin pressured infusion devices numbered from 1 to 70 Boththe visiting nurse and the research physician recorded thenumber of completed infusions Patients who missed a dayrsquosdose were instructed to continue in consecutive sequence un-til all 70 doses were infused
Sample sizeThe target sample size of 45 Lymepatients (30randomized to active treatment and 15 randomized to placebo)provided at least 80power to detect an effect size of 11with atwo-sided test with 005 Power calculations were based onthe results of an uncontrolled pilot study4 with the outcomemeasure of memory assessed with the Buschke Selective Re-minding Test total verbal memory score Although cognitiveimprovement was expected in both visual and verbal memoryas well as in multiple other cognitive domains verbal memorywas selected for the power analysis given the lack of pilot datafor other aspects of cognition
Assessments Screening Subjects were screened for mem-ory impairment with the Wechsler Memory Scale (WMS-III)8 which measures immediate delayed and workingmemory in auditory and visual domains Demographicallyadjusted t scores were computed for all indices correctingfor the influence of sex ethnicity and education level Mem-ory impairment was defined as a t score of one or more SDbelow population norms on at least one of the six primaryWMS-III indices Premorbid IQ was estimated using the Ba-rona demographic formula12 and the North American AdultReading TestndashRevised (NAART-R)13
Outcome measures The primary clinical outcomemeasure assessed neurocognitive performance and theprimary biologic outcomes assessed brain structure andfunction Relative to the placebo and control groups IVantibiotic therapy was hypothesized to lead to superioroutcome in the memory domain scores as well as across
Neurology 70 March 25 2008 (Part 1 of 2) 993
cognitive domains The cognitive assessments sampled six do-mains motor function (finger tapping simple reaction timechoice reaction time) psychomotor function (Trail MakingAampB Digit Symbol) attention (Continuous Performance TestStroop task) memory (Buschke Selective Reminding Test [ver-bal memory] Benton Visual Retention Test [visual memory])working memory (A Not B Logical Reasoning Test N-BackTest) and verbal fluency (Controlled Oral Word AssociationTest and Category Fluency Test) Descriptions of these mea-sures may be found elsewhere1415 Scores on these tests were ztransformed relative to either published norms or a referencesample of healthy controls and were adjusted for the effects ofage gender and education Domain scores represent the aver-age of the z scores for the primary tests within each cognitivedomain To characterize overall performance the six domainscores were averaged to produce a cognitive ldquoindexrdquo score thisindexwas not used in the primarymixed-model analyses Brainimaging measures included MRI and PET scans these imagingresults will be reported elsewhere
Assessments of physical outcome included the rheumatolo-gistrsquos exam (trigger points total number of joints in pain at restor on movement) and self-report measures of fatigue (FatigueSeverity Scalendash1116) pain (McGill Pain QuestionnairendashShortForm17) and physical functioning (Short Formndash36 PhysicalComponent Scale [PCS]1819) Psychopathology was assessedwith respect to depression (Beck Depression Inventory20) anxi-ety (ZungAnxiety Scale21) mental functioning (SF-36MCS1819)and global symptoms (SCL-90 Global Symptom Index22)
Time of assessment Major assessments occurred at base-line week 12 and week 24 The primary end point for efficacyanalyses was week 12 The week 24 assessments evaluated du-rability of benefit Controls were assessed at the same timepoints to allow correction for the impact of practice effects onthe repeated neurocognitive measures The secondary outcomeself-report scales were collected at 4-week intervals (baselineand weeks 4 8 12 16 20 and 24) The rheumatologist examwas conducted at baseline week 12 and week 24 The lumbarpuncture (for patients) and neurology exam (for all partici-pants) were done only at baseline The neurologic exam as-sessed five areas cranial nerves reflexes sensory motor andassociated motor (cerebellar and basal ganglia) functions Forthe standardized neurology exam a summary score (0ndash5) indi-cated the number of areas with at least one minor or majorabnormal finding An objective neurologic abnormality wasconsidered major if it was associated with either a significantdeficit or impairment in the personrsquos functioning
Laboratory assessments Screening serum was sent forLyme IgM and IgGWestern blot testing Enrolled patients hadserum examined by IFA for signs of coinfection withAnaplasma phagocytophila (human granulocytic erhlichiosis)and Babesia microti (Babesiosis) Samples of whole blood andCSF were tested by PCR assay for B burgdorferi DNA usingthe plasmid ospA primer CSF was sent for cell count proteinglucose total gammaglobulin Lyme ELISA and oligoclonalbands Serum and CSF were sent for determination of Bb-specific intrathecal Ab production to University Hospital ofStony Brook using the whole-cell sonicate ELISA (positive cut-off 11) To determine whether viable B burgdorferi cellswere present spinal fluid was cultured in BSKII containingkanamycin (5 gmL) at 33degC and was checked weekly for upto 12 weeks
Statistical analysis Efficacy analyses were performed us-ing all randomized participants the intent-to-treat (ITT)
sample Lyme patient and healthy controls were comparedwith respect to demographic and baseline clinical character-istics using t tests for continuous measures and 2 tests forcategorical measures
Tests and estimates of differences between groups (IV anti-biotic IV placebo and healthy controls) with respect to themultivariate measure of cognition (six domains motor psy-chomotor working memory attention verbal fluency andmemory) over time (baselineweek 12 andweek 24)were basedon longitudinal mixed-effects models (LMM)23 which accountfor the correlation between the domains and between the re-peated observations over time24 The LMM included main ef-fects and all interaction terms Time was modeled as a nominalfactor rather than a continuous variable
Including all two- and three-way interactions the modelfor the covariance structure was selected based on maximiz-ing Bayesian information criteria2526 Keeping the model forthe covariance as selected stepwise backward eliminationwas used to select the ldquobestrdquo model for the mean structureInference regarding the comparison between the groups wasbased on the best model Significant omnibus tests for ITTdifferences among the three groups over time (two-sided
005) were followed by pairwise comparisons the p valuesfor these post hoc tests are reported unadjusted
Secondary outcome measures were analyzed with LMMsusing a similar strategy Healthy controls were not included be-cause practice effects were not of concern For the outcomenumber of joints with pain a Poisson variable an appropriategeneralized LMM23 was employed using log link As initiallyplanned the LMMs included the baseline value of the outcomeas a continuous covariate to account for heterogeneity in clini-cal characteristics and to remedy potential floor effects Thesignificance of the interaction terms was judged at a two-sided 015 to avoid the erroneous omission of potentially impor-tant effects for which the study was not powered the signifi-cance of a main effect for drug vs placebo was still judged at
005 To illustrate the impact on outcome of different base-line severity scores an estimate of the mean response based onthe best model for each outcome was computed at weeks 4 12and 24 for drug and placebo for hypothetical subjects withbaseline symptom severity equal to the lowest (first) or highest(third) quartile of the observed baseline severities The report-ing of outcomes for ldquolowrdquo and ldquohighrdquo baseline severity is forillustration purposes only the actual analysis based on LMMsincluded all patients and used baseline severity as a continuouscovariate without dichotomizing it into low and high valuesAll analyses were performed using SAS software version 925 theLMMswere fit using PROCMIXED and PROCGLIMMIX
To explore whether particular patient subgroups hadpreferential benefit from active treatment ANCOVAs testedfor associations between selected demographic clinical andlaboratory variables and the primary and secondary out-comes at week 12 and week 24 that had shown a treatmenteffect in the LMM analyses Treatment group baseline se-verity of the outcome measure and (dichotomous or contin-uous) potential predictor were examined as fully factorialbetween-subject factors
RESULTS Study population Healthy controls Of305 individuals contacted by telephone 58 wereinvited for on-site screening and 20 were en-rolled Reasons for exclusion included laboratoryabnormalities memory deficits on testing or
994 Neurology 70 March 25 2008 (Part 1 of 2)
other exclusions Of the 20 enrolled two partici-pants had impaired scores on baseline neuropsy-chological testing and were excluded
Patients Of 3368 initial clinic contacts 1439 wereexcluded because of insufficient prior IV treatmentand 1316 were excluded because the patient had notmet the CDC criteria for Lyme disease (figure)Among the remaining 613 patients 512 were ex-cluded because their serum was not IgG Westernblot positive and 20 were excluded for other rea-sons Of the 81 patients invited to Columbia forneuropsychological screening 31 did not have suffi-cient memory impairment 12 were not able to pro-vide adequate documentation of their clinicalhistory and one patient who had been deemed eligi-ble for the study withdrew for private treatment be-fore randomization Thirty-seven patients wererandomized to interventions representing 1 of allpatients screened for the study Of these 37 patientsfive withdrew from the study during the first 12weeks threewithin the first 3 weeks of therapy (twobecause of thrombus and one because of hemolyticanemia all three on antibiotic) one after 8 weeksbecause of a systemic infection (on placebo) andone after 10 weeks (on placebo) because of intolera-ble joint pain that required narcotic medications forrelief Three additional patients had adverse eventsthat required early termination of study medication(one at week 6 and two at week 8) but each of thesepatients continued in a masked fashion through tothe week 12 and 24 evaluations No patients with-
drew from the study between weeks 12 and 24
Laboratory results for enrolled patients Blood Allsamples were IgG WB positive and 18 of 37 wereIgM WB positive No patient samples were PCRpositive using the OspA primer assay None ofthe serum samples were IgM positive on either ofthe two coinfection tests whereas low positiveIgG results were noted on 4 of 37 (108) samplesfor Anaplasma phagocytophila and on 10 of 37(270) samples for Babesia microti
Cerebrospinal fluid Baseline lumbar punctureconducted in 33 of the 37 patients revealed few ab-normalities mildly elevated WBC (two samples)mildly elevated protein (four samples) and elevatedgammaglobulin (one sample) Positive results werenoted for 22 on Lyme ELISA 28 on IgG WB andnone on IgM WB For intrathecal Ab productionsamples tested positive for 4 of 31 (129) patientseach positive intrathecal sample was also seroposi-tive No patient had a positive CSF PCRWhen cul-tured one sample was positive for growth andrevealed spirochetes by both phase contrast anddark-field microscopy To exclude contaminationas an explanation the cellsrsquos DNA was extractedandwas used as a template for PCRamplification ofthe spoT gene Examination of the PCR ampliconby agarose gel electrophoresis revealed an approxi-mately 3-kbp band whereas a PCR amplicon fromwild-type strains was approximately 2 kbp Addi-tionally the B burgdorferi isolated from the CSFculture was able to grow when transferred intoBSKII containing kanamycin (5 gmL) plus strep-tomycin (100gmL) These results strongly suggestthat the B burgdorferi strain found in the CSF cul-ture was the result of contamination by a spoTmu-tant strain (WC07) of B burgdorferi containing adeletion of part of the spoT gene plus the insertionof a streptomycin resistance gene spoT mutantstrains were under investigation in the lab at thetime of the culture
Demographics and pretreatment clinical character-ization of patients and controls The patients andhealthy controls did not differ in the matchingvariables of age gender or education (table 1)The patientsrsquo clinical histories indicated that allhad rheumatologic symptoms and most had neu-rologic symptoms associated with cognitive com-plaints Nearly half (49) had had a prior lumbarpuncture only three of these patients had had ele-vated B burgdorferindashspecific intrathecal Ab pro-duction The total amount of prior antibiotictherapy for Lyme disease was extensive with57 of the patients in each treatment group hav-ing had more than 1 month of prior IV antibiotic
Figure Flow diagram of patient enrollment
Neurology 70 March 25 2008 (Part 1 of 2) 995
therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

sis Consequently clinicians are uncertainabout optimal treatment strategies For pa-tients in whom no other cause of symptomscan be found community practice varieswidely ranging from no treatment to pal-liative treatment to use of repeated or long-term antibiotic courses
To evaluate the benefit of additional IVantibiotic therapy we conducted a trial com-paring clinical improvement from 10 weeksof IV ceftriaxone vs IV placebo in patientswith previously treated Lyme disease whohad objectivememory impairment and a cur-rently positive IgGWestern blot
METHODS Study participants Between January 2000and April 2004 healthy volunteers (controls) and individualswith a history of Lyme disease (patients) between the ages of 18and 65 years were recruited follow-up evaluations were com-pleted byApril 2005 The institutional review boards at Colum-bia University and the New York State Psychiatric Instituteapproved the study and all participants provided written in-formed consent Evaluations were conducted at the New YorkState Psychiatric Institute and Columbia University MedicalCenter Treatments were conducted at each patientrsquos home Pa-tients met the following criteria (1) history of physician-documented erythema migrans or US Centers for DiseaseControl and Prevention (CDC)-defined manifestation of Lymedisease and a positive or equivocal ELISA confirmed by posi-tive Western blot serology67 (2) current positive IgG Westernblot using CDC surveillance criteria assessed using a single ref-erence laboratory (University Hospital of Stony Brook) (3)treatment for Lyme disease with at least 3 weeks of IV ceftriax-one completed at least 4 months before study entry (4) subjec-tive memory impairment that by participant report startedafter the onset of Lyme disease and (5) objective evidence ofmemory impairment as documented by the Wechsler MemoryScalendashIII8 compared with age- sex- and education-adjustedpopulation norms These study criteria were conservative andnarrow to enhance diagnostic confidence Prior IV antibiotictherapy was required to ensure that all patients had receivedtreatment considered adequate for neurologic Lyme disease bypublished guidelines910
The control sample of healthy volunteers had (1) nega-tive history of Lyme disease fibromyalgia or chronic fa-tigue (2) negative IgM and IgG Western blot for Lymedisease and (3) no evidence of memory impairment on neu-ropsychological testing
Patients and controls were excluded if their history re-vealed a prior learning disability or medical condition thatcould confound neuropsychological assessment Patientswith cephalosporin allergy or a history of major psychiatricdisorder before the onset of Lyme disease were also ex-cluded The control and patient samples were matched onthe mean variance and shapes of the distributions of ageand education and the distribution of gender
Study design Treatment The controlled phase of thisstudy consisted of 10 weeks of randomized treatment witheither IV ceftriaxone (2 gd) or IV placebo (09 normal
saline) and then 14 weeks off all antibiotics Ceftriaxonewas chosen because it is the recommended treatment forneurologic Lyme disease and has excellent penetration of thebloodndashbrain barrier9 A 10-week duration was chosen be-cause of reports of persistent or relapsing symptoms after 3weeks of IV ceftriaxone and because of case series suggest-ing that longer courses of antibiotic therapy may be moreeffective411 After week 24 treatment assignment was re-vealed by a research staff member not involved in data col-lection and no further constraints were placed onsubsequent care Participants underwent one follow-up as-sessment at week 48 This report concerns only the con-trolled phases of the study from baseline to week 24
Randomization Patients were assigned in a 21 ratio toIV ceftriaxone or IV placebo using permuted blocks of size20 based on a computer-based randomization list A 21 ran-domization schedule was used to encourage enrollment
Masking An unmasked off-site pharmacist who had nocontact with patients ensured that patients were sent theassigned treatment this pharmacist was the only unmaskedindividual during the 24 weeks of each patientrsquos maskedtreatment The neuropsychological technicians were notprivy to information about adverse events To assess successof masking patients were asked to guess treatment assign-ment at both the week 12 and 24 evaluations
Compliance with treatment Compliance and safetywere monitored by home infusion nurses who visited twiceweekly Patients had weekly telephone contact with a re-search physician and monthly in-person evaluations with thepatientrsquos private physician Study medication was packagedin pressured infusion devices numbered from 1 to 70 Boththe visiting nurse and the research physician recorded thenumber of completed infusions Patients who missed a dayrsquosdose were instructed to continue in consecutive sequence un-til all 70 doses were infused
Sample sizeThe target sample size of 45 Lymepatients (30randomized to active treatment and 15 randomized to placebo)provided at least 80power to detect an effect size of 11with atwo-sided test with 005 Power calculations were based onthe results of an uncontrolled pilot study4 with the outcomemeasure of memory assessed with the Buschke Selective Re-minding Test total verbal memory score Although cognitiveimprovement was expected in both visual and verbal memoryas well as in multiple other cognitive domains verbal memorywas selected for the power analysis given the lack of pilot datafor other aspects of cognition
Assessments Screening Subjects were screened for mem-ory impairment with the Wechsler Memory Scale (WMS-III)8 which measures immediate delayed and workingmemory in auditory and visual domains Demographicallyadjusted t scores were computed for all indices correctingfor the influence of sex ethnicity and education level Mem-ory impairment was defined as a t score of one or more SDbelow population norms on at least one of the six primaryWMS-III indices Premorbid IQ was estimated using the Ba-rona demographic formula12 and the North American AdultReading TestndashRevised (NAART-R)13
Outcome measures The primary clinical outcomemeasure assessed neurocognitive performance and theprimary biologic outcomes assessed brain structure andfunction Relative to the placebo and control groups IVantibiotic therapy was hypothesized to lead to superioroutcome in the memory domain scores as well as across
Neurology 70 March 25 2008 (Part 1 of 2) 993
cognitive domains The cognitive assessments sampled six do-mains motor function (finger tapping simple reaction timechoice reaction time) psychomotor function (Trail MakingAampB Digit Symbol) attention (Continuous Performance TestStroop task) memory (Buschke Selective Reminding Test [ver-bal memory] Benton Visual Retention Test [visual memory])working memory (A Not B Logical Reasoning Test N-BackTest) and verbal fluency (Controlled Oral Word AssociationTest and Category Fluency Test) Descriptions of these mea-sures may be found elsewhere1415 Scores on these tests were ztransformed relative to either published norms or a referencesample of healthy controls and were adjusted for the effects ofage gender and education Domain scores represent the aver-age of the z scores for the primary tests within each cognitivedomain To characterize overall performance the six domainscores were averaged to produce a cognitive ldquoindexrdquo score thisindexwas not used in the primarymixed-model analyses Brainimaging measures included MRI and PET scans these imagingresults will be reported elsewhere
Assessments of physical outcome included the rheumatolo-gistrsquos exam (trigger points total number of joints in pain at restor on movement) and self-report measures of fatigue (FatigueSeverity Scalendash1116) pain (McGill Pain QuestionnairendashShortForm17) and physical functioning (Short Formndash36 PhysicalComponent Scale [PCS]1819) Psychopathology was assessedwith respect to depression (Beck Depression Inventory20) anxi-ety (ZungAnxiety Scale21) mental functioning (SF-36MCS1819)and global symptoms (SCL-90 Global Symptom Index22)
Time of assessment Major assessments occurred at base-line week 12 and week 24 The primary end point for efficacyanalyses was week 12 The week 24 assessments evaluated du-rability of benefit Controls were assessed at the same timepoints to allow correction for the impact of practice effects onthe repeated neurocognitive measures The secondary outcomeself-report scales were collected at 4-week intervals (baselineand weeks 4 8 12 16 20 and 24) The rheumatologist examwas conducted at baseline week 12 and week 24 The lumbarpuncture (for patients) and neurology exam (for all partici-pants) were done only at baseline The neurologic exam as-sessed five areas cranial nerves reflexes sensory motor andassociated motor (cerebellar and basal ganglia) functions Forthe standardized neurology exam a summary score (0ndash5) indi-cated the number of areas with at least one minor or majorabnormal finding An objective neurologic abnormality wasconsidered major if it was associated with either a significantdeficit or impairment in the personrsquos functioning
Laboratory assessments Screening serum was sent forLyme IgM and IgGWestern blot testing Enrolled patients hadserum examined by IFA for signs of coinfection withAnaplasma phagocytophila (human granulocytic erhlichiosis)and Babesia microti (Babesiosis) Samples of whole blood andCSF were tested by PCR assay for B burgdorferi DNA usingthe plasmid ospA primer CSF was sent for cell count proteinglucose total gammaglobulin Lyme ELISA and oligoclonalbands Serum and CSF were sent for determination of Bb-specific intrathecal Ab production to University Hospital ofStony Brook using the whole-cell sonicate ELISA (positive cut-off 11) To determine whether viable B burgdorferi cellswere present spinal fluid was cultured in BSKII containingkanamycin (5 gmL) at 33degC and was checked weekly for upto 12 weeks
Statistical analysis Efficacy analyses were performed us-ing all randomized participants the intent-to-treat (ITT)
sample Lyme patient and healthy controls were comparedwith respect to demographic and baseline clinical character-istics using t tests for continuous measures and 2 tests forcategorical measures
Tests and estimates of differences between groups (IV anti-biotic IV placebo and healthy controls) with respect to themultivariate measure of cognition (six domains motor psy-chomotor working memory attention verbal fluency andmemory) over time (baselineweek 12 andweek 24)were basedon longitudinal mixed-effects models (LMM)23 which accountfor the correlation between the domains and between the re-peated observations over time24 The LMM included main ef-fects and all interaction terms Time was modeled as a nominalfactor rather than a continuous variable
Including all two- and three-way interactions the modelfor the covariance structure was selected based on maximiz-ing Bayesian information criteria2526 Keeping the model forthe covariance as selected stepwise backward eliminationwas used to select the ldquobestrdquo model for the mean structureInference regarding the comparison between the groups wasbased on the best model Significant omnibus tests for ITTdifferences among the three groups over time (two-sided
005) were followed by pairwise comparisons the p valuesfor these post hoc tests are reported unadjusted
Secondary outcome measures were analyzed with LMMsusing a similar strategy Healthy controls were not included be-cause practice effects were not of concern For the outcomenumber of joints with pain a Poisson variable an appropriategeneralized LMM23 was employed using log link As initiallyplanned the LMMs included the baseline value of the outcomeas a continuous covariate to account for heterogeneity in clini-cal characteristics and to remedy potential floor effects Thesignificance of the interaction terms was judged at a two-sided 015 to avoid the erroneous omission of potentially impor-tant effects for which the study was not powered the signifi-cance of a main effect for drug vs placebo was still judged at
005 To illustrate the impact on outcome of different base-line severity scores an estimate of the mean response based onthe best model for each outcome was computed at weeks 4 12and 24 for drug and placebo for hypothetical subjects withbaseline symptom severity equal to the lowest (first) or highest(third) quartile of the observed baseline severities The report-ing of outcomes for ldquolowrdquo and ldquohighrdquo baseline severity is forillustration purposes only the actual analysis based on LMMsincluded all patients and used baseline severity as a continuouscovariate without dichotomizing it into low and high valuesAll analyses were performed using SAS software version 925 theLMMswere fit using PROCMIXED and PROCGLIMMIX
To explore whether particular patient subgroups hadpreferential benefit from active treatment ANCOVAs testedfor associations between selected demographic clinical andlaboratory variables and the primary and secondary out-comes at week 12 and week 24 that had shown a treatmenteffect in the LMM analyses Treatment group baseline se-verity of the outcome measure and (dichotomous or contin-uous) potential predictor were examined as fully factorialbetween-subject factors
RESULTS Study population Healthy controls Of305 individuals contacted by telephone 58 wereinvited for on-site screening and 20 were en-rolled Reasons for exclusion included laboratoryabnormalities memory deficits on testing or
994 Neurology 70 March 25 2008 (Part 1 of 2)
other exclusions Of the 20 enrolled two partici-pants had impaired scores on baseline neuropsy-chological testing and were excluded
Patients Of 3368 initial clinic contacts 1439 wereexcluded because of insufficient prior IV treatmentand 1316 were excluded because the patient had notmet the CDC criteria for Lyme disease (figure)Among the remaining 613 patients 512 were ex-cluded because their serum was not IgG Westernblot positive and 20 were excluded for other rea-sons Of the 81 patients invited to Columbia forneuropsychological screening 31 did not have suffi-cient memory impairment 12 were not able to pro-vide adequate documentation of their clinicalhistory and one patient who had been deemed eligi-ble for the study withdrew for private treatment be-fore randomization Thirty-seven patients wererandomized to interventions representing 1 of allpatients screened for the study Of these 37 patientsfive withdrew from the study during the first 12weeks threewithin the first 3 weeks of therapy (twobecause of thrombus and one because of hemolyticanemia all three on antibiotic) one after 8 weeksbecause of a systemic infection (on placebo) andone after 10 weeks (on placebo) because of intolera-ble joint pain that required narcotic medications forrelief Three additional patients had adverse eventsthat required early termination of study medication(one at week 6 and two at week 8) but each of thesepatients continued in a masked fashion through tothe week 12 and 24 evaluations No patients with-
drew from the study between weeks 12 and 24
Laboratory results for enrolled patients Blood Allsamples were IgG WB positive and 18 of 37 wereIgM WB positive No patient samples were PCRpositive using the OspA primer assay None ofthe serum samples were IgM positive on either ofthe two coinfection tests whereas low positiveIgG results were noted on 4 of 37 (108) samplesfor Anaplasma phagocytophila and on 10 of 37(270) samples for Babesia microti
Cerebrospinal fluid Baseline lumbar punctureconducted in 33 of the 37 patients revealed few ab-normalities mildly elevated WBC (two samples)mildly elevated protein (four samples) and elevatedgammaglobulin (one sample) Positive results werenoted for 22 on Lyme ELISA 28 on IgG WB andnone on IgM WB For intrathecal Ab productionsamples tested positive for 4 of 31 (129) patientseach positive intrathecal sample was also seroposi-tive No patient had a positive CSF PCRWhen cul-tured one sample was positive for growth andrevealed spirochetes by both phase contrast anddark-field microscopy To exclude contaminationas an explanation the cellsrsquos DNA was extractedandwas used as a template for PCRamplification ofthe spoT gene Examination of the PCR ampliconby agarose gel electrophoresis revealed an approxi-mately 3-kbp band whereas a PCR amplicon fromwild-type strains was approximately 2 kbp Addi-tionally the B burgdorferi isolated from the CSFculture was able to grow when transferred intoBSKII containing kanamycin (5 gmL) plus strep-tomycin (100gmL) These results strongly suggestthat the B burgdorferi strain found in the CSF cul-ture was the result of contamination by a spoTmu-tant strain (WC07) of B burgdorferi containing adeletion of part of the spoT gene plus the insertionof a streptomycin resistance gene spoT mutantstrains were under investigation in the lab at thetime of the culture
Demographics and pretreatment clinical character-ization of patients and controls The patients andhealthy controls did not differ in the matchingvariables of age gender or education (table 1)The patientsrsquo clinical histories indicated that allhad rheumatologic symptoms and most had neu-rologic symptoms associated with cognitive com-plaints Nearly half (49) had had a prior lumbarpuncture only three of these patients had had ele-vated B burgdorferindashspecific intrathecal Ab pro-duction The total amount of prior antibiotictherapy for Lyme disease was extensive with57 of the patients in each treatment group hav-ing had more than 1 month of prior IV antibiotic
Figure Flow diagram of patient enrollment
Neurology 70 March 25 2008 (Part 1 of 2) 995
therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

cognitive domains The cognitive assessments sampled six do-mains motor function (finger tapping simple reaction timechoice reaction time) psychomotor function (Trail MakingAampB Digit Symbol) attention (Continuous Performance TestStroop task) memory (Buschke Selective Reminding Test [ver-bal memory] Benton Visual Retention Test [visual memory])working memory (A Not B Logical Reasoning Test N-BackTest) and verbal fluency (Controlled Oral Word AssociationTest and Category Fluency Test) Descriptions of these mea-sures may be found elsewhere1415 Scores on these tests were ztransformed relative to either published norms or a referencesample of healthy controls and were adjusted for the effects ofage gender and education Domain scores represent the aver-age of the z scores for the primary tests within each cognitivedomain To characterize overall performance the six domainscores were averaged to produce a cognitive ldquoindexrdquo score thisindexwas not used in the primarymixed-model analyses Brainimaging measures included MRI and PET scans these imagingresults will be reported elsewhere
Assessments of physical outcome included the rheumatolo-gistrsquos exam (trigger points total number of joints in pain at restor on movement) and self-report measures of fatigue (FatigueSeverity Scalendash1116) pain (McGill Pain QuestionnairendashShortForm17) and physical functioning (Short Formndash36 PhysicalComponent Scale [PCS]1819) Psychopathology was assessedwith respect to depression (Beck Depression Inventory20) anxi-ety (ZungAnxiety Scale21) mental functioning (SF-36MCS1819)and global symptoms (SCL-90 Global Symptom Index22)
Time of assessment Major assessments occurred at base-line week 12 and week 24 The primary end point for efficacyanalyses was week 12 The week 24 assessments evaluated du-rability of benefit Controls were assessed at the same timepoints to allow correction for the impact of practice effects onthe repeated neurocognitive measures The secondary outcomeself-report scales were collected at 4-week intervals (baselineand weeks 4 8 12 16 20 and 24) The rheumatologist examwas conducted at baseline week 12 and week 24 The lumbarpuncture (for patients) and neurology exam (for all partici-pants) were done only at baseline The neurologic exam as-sessed five areas cranial nerves reflexes sensory motor andassociated motor (cerebellar and basal ganglia) functions Forthe standardized neurology exam a summary score (0ndash5) indi-cated the number of areas with at least one minor or majorabnormal finding An objective neurologic abnormality wasconsidered major if it was associated with either a significantdeficit or impairment in the personrsquos functioning
Laboratory assessments Screening serum was sent forLyme IgM and IgGWestern blot testing Enrolled patients hadserum examined by IFA for signs of coinfection withAnaplasma phagocytophila (human granulocytic erhlichiosis)and Babesia microti (Babesiosis) Samples of whole blood andCSF were tested by PCR assay for B burgdorferi DNA usingthe plasmid ospA primer CSF was sent for cell count proteinglucose total gammaglobulin Lyme ELISA and oligoclonalbands Serum and CSF were sent for determination of Bb-specific intrathecal Ab production to University Hospital ofStony Brook using the whole-cell sonicate ELISA (positive cut-off 11) To determine whether viable B burgdorferi cellswere present spinal fluid was cultured in BSKII containingkanamycin (5 gmL) at 33degC and was checked weekly for upto 12 weeks
Statistical analysis Efficacy analyses were performed us-ing all randomized participants the intent-to-treat (ITT)
sample Lyme patient and healthy controls were comparedwith respect to demographic and baseline clinical character-istics using t tests for continuous measures and 2 tests forcategorical measures
Tests and estimates of differences between groups (IV anti-biotic IV placebo and healthy controls) with respect to themultivariate measure of cognition (six domains motor psy-chomotor working memory attention verbal fluency andmemory) over time (baselineweek 12 andweek 24)were basedon longitudinal mixed-effects models (LMM)23 which accountfor the correlation between the domains and between the re-peated observations over time24 The LMM included main ef-fects and all interaction terms Time was modeled as a nominalfactor rather than a continuous variable
Including all two- and three-way interactions the modelfor the covariance structure was selected based on maximiz-ing Bayesian information criteria2526 Keeping the model forthe covariance as selected stepwise backward eliminationwas used to select the ldquobestrdquo model for the mean structureInference regarding the comparison between the groups wasbased on the best model Significant omnibus tests for ITTdifferences among the three groups over time (two-sided
005) were followed by pairwise comparisons the p valuesfor these post hoc tests are reported unadjusted
Secondary outcome measures were analyzed with LMMsusing a similar strategy Healthy controls were not included be-cause practice effects were not of concern For the outcomenumber of joints with pain a Poisson variable an appropriategeneralized LMM23 was employed using log link As initiallyplanned the LMMs included the baseline value of the outcomeas a continuous covariate to account for heterogeneity in clini-cal characteristics and to remedy potential floor effects Thesignificance of the interaction terms was judged at a two-sided 015 to avoid the erroneous omission of potentially impor-tant effects for which the study was not powered the signifi-cance of a main effect for drug vs placebo was still judged at
005 To illustrate the impact on outcome of different base-line severity scores an estimate of the mean response based onthe best model for each outcome was computed at weeks 4 12and 24 for drug and placebo for hypothetical subjects withbaseline symptom severity equal to the lowest (first) or highest(third) quartile of the observed baseline severities The report-ing of outcomes for ldquolowrdquo and ldquohighrdquo baseline severity is forillustration purposes only the actual analysis based on LMMsincluded all patients and used baseline severity as a continuouscovariate without dichotomizing it into low and high valuesAll analyses were performed using SAS software version 925 theLMMswere fit using PROCMIXED and PROCGLIMMIX
To explore whether particular patient subgroups hadpreferential benefit from active treatment ANCOVAs testedfor associations between selected demographic clinical andlaboratory variables and the primary and secondary out-comes at week 12 and week 24 that had shown a treatmenteffect in the LMM analyses Treatment group baseline se-verity of the outcome measure and (dichotomous or contin-uous) potential predictor were examined as fully factorialbetween-subject factors
RESULTS Study population Healthy controls Of305 individuals contacted by telephone 58 wereinvited for on-site screening and 20 were en-rolled Reasons for exclusion included laboratoryabnormalities memory deficits on testing or
994 Neurology 70 March 25 2008 (Part 1 of 2)
other exclusions Of the 20 enrolled two partici-pants had impaired scores on baseline neuropsy-chological testing and were excluded
Patients Of 3368 initial clinic contacts 1439 wereexcluded because of insufficient prior IV treatmentand 1316 were excluded because the patient had notmet the CDC criteria for Lyme disease (figure)Among the remaining 613 patients 512 were ex-cluded because their serum was not IgG Westernblot positive and 20 were excluded for other rea-sons Of the 81 patients invited to Columbia forneuropsychological screening 31 did not have suffi-cient memory impairment 12 were not able to pro-vide adequate documentation of their clinicalhistory and one patient who had been deemed eligi-ble for the study withdrew for private treatment be-fore randomization Thirty-seven patients wererandomized to interventions representing 1 of allpatients screened for the study Of these 37 patientsfive withdrew from the study during the first 12weeks threewithin the first 3 weeks of therapy (twobecause of thrombus and one because of hemolyticanemia all three on antibiotic) one after 8 weeksbecause of a systemic infection (on placebo) andone after 10 weeks (on placebo) because of intolera-ble joint pain that required narcotic medications forrelief Three additional patients had adverse eventsthat required early termination of study medication(one at week 6 and two at week 8) but each of thesepatients continued in a masked fashion through tothe week 12 and 24 evaluations No patients with-
drew from the study between weeks 12 and 24
Laboratory results for enrolled patients Blood Allsamples were IgG WB positive and 18 of 37 wereIgM WB positive No patient samples were PCRpositive using the OspA primer assay None ofthe serum samples were IgM positive on either ofthe two coinfection tests whereas low positiveIgG results were noted on 4 of 37 (108) samplesfor Anaplasma phagocytophila and on 10 of 37(270) samples for Babesia microti
Cerebrospinal fluid Baseline lumbar punctureconducted in 33 of the 37 patients revealed few ab-normalities mildly elevated WBC (two samples)mildly elevated protein (four samples) and elevatedgammaglobulin (one sample) Positive results werenoted for 22 on Lyme ELISA 28 on IgG WB andnone on IgM WB For intrathecal Ab productionsamples tested positive for 4 of 31 (129) patientseach positive intrathecal sample was also seroposi-tive No patient had a positive CSF PCRWhen cul-tured one sample was positive for growth andrevealed spirochetes by both phase contrast anddark-field microscopy To exclude contaminationas an explanation the cellsrsquos DNA was extractedandwas used as a template for PCRamplification ofthe spoT gene Examination of the PCR ampliconby agarose gel electrophoresis revealed an approxi-mately 3-kbp band whereas a PCR amplicon fromwild-type strains was approximately 2 kbp Addi-tionally the B burgdorferi isolated from the CSFculture was able to grow when transferred intoBSKII containing kanamycin (5 gmL) plus strep-tomycin (100gmL) These results strongly suggestthat the B burgdorferi strain found in the CSF cul-ture was the result of contamination by a spoTmu-tant strain (WC07) of B burgdorferi containing adeletion of part of the spoT gene plus the insertionof a streptomycin resistance gene spoT mutantstrains were under investigation in the lab at thetime of the culture
Demographics and pretreatment clinical character-ization of patients and controls The patients andhealthy controls did not differ in the matchingvariables of age gender or education (table 1)The patientsrsquo clinical histories indicated that allhad rheumatologic symptoms and most had neu-rologic symptoms associated with cognitive com-plaints Nearly half (49) had had a prior lumbarpuncture only three of these patients had had ele-vated B burgdorferindashspecific intrathecal Ab pro-duction The total amount of prior antibiotictherapy for Lyme disease was extensive with57 of the patients in each treatment group hav-ing had more than 1 month of prior IV antibiotic
Figure Flow diagram of patient enrollment
Neurology 70 March 25 2008 (Part 1 of 2) 995
therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

other exclusions Of the 20 enrolled two partici-pants had impaired scores on baseline neuropsy-chological testing and were excluded
Patients Of 3368 initial clinic contacts 1439 wereexcluded because of insufficient prior IV treatmentand 1316 were excluded because the patient had notmet the CDC criteria for Lyme disease (figure)Among the remaining 613 patients 512 were ex-cluded because their serum was not IgG Westernblot positive and 20 were excluded for other rea-sons Of the 81 patients invited to Columbia forneuropsychological screening 31 did not have suffi-cient memory impairment 12 were not able to pro-vide adequate documentation of their clinicalhistory and one patient who had been deemed eligi-ble for the study withdrew for private treatment be-fore randomization Thirty-seven patients wererandomized to interventions representing 1 of allpatients screened for the study Of these 37 patientsfive withdrew from the study during the first 12weeks threewithin the first 3 weeks of therapy (twobecause of thrombus and one because of hemolyticanemia all three on antibiotic) one after 8 weeksbecause of a systemic infection (on placebo) andone after 10 weeks (on placebo) because of intolera-ble joint pain that required narcotic medications forrelief Three additional patients had adverse eventsthat required early termination of study medication(one at week 6 and two at week 8) but each of thesepatients continued in a masked fashion through tothe week 12 and 24 evaluations No patients with-
drew from the study between weeks 12 and 24
Laboratory results for enrolled patients Blood Allsamples were IgG WB positive and 18 of 37 wereIgM WB positive No patient samples were PCRpositive using the OspA primer assay None ofthe serum samples were IgM positive on either ofthe two coinfection tests whereas low positiveIgG results were noted on 4 of 37 (108) samplesfor Anaplasma phagocytophila and on 10 of 37(270) samples for Babesia microti
Cerebrospinal fluid Baseline lumbar punctureconducted in 33 of the 37 patients revealed few ab-normalities mildly elevated WBC (two samples)mildly elevated protein (four samples) and elevatedgammaglobulin (one sample) Positive results werenoted for 22 on Lyme ELISA 28 on IgG WB andnone on IgM WB For intrathecal Ab productionsamples tested positive for 4 of 31 (129) patientseach positive intrathecal sample was also seroposi-tive No patient had a positive CSF PCRWhen cul-tured one sample was positive for growth andrevealed spirochetes by both phase contrast anddark-field microscopy To exclude contaminationas an explanation the cellsrsquos DNA was extractedandwas used as a template for PCRamplification ofthe spoT gene Examination of the PCR ampliconby agarose gel electrophoresis revealed an approxi-mately 3-kbp band whereas a PCR amplicon fromwild-type strains was approximately 2 kbp Addi-tionally the B burgdorferi isolated from the CSFculture was able to grow when transferred intoBSKII containing kanamycin (5 gmL) plus strep-tomycin (100gmL) These results strongly suggestthat the B burgdorferi strain found in the CSF cul-ture was the result of contamination by a spoTmu-tant strain (WC07) of B burgdorferi containing adeletion of part of the spoT gene plus the insertionof a streptomycin resistance gene spoT mutantstrains were under investigation in the lab at thetime of the culture
Demographics and pretreatment clinical character-ization of patients and controls The patients andhealthy controls did not differ in the matchingvariables of age gender or education (table 1)The patientsrsquo clinical histories indicated that allhad rheumatologic symptoms and most had neu-rologic symptoms associated with cognitive com-plaints Nearly half (49) had had a prior lumbarpuncture only three of these patients had had ele-vated B burgdorferindashspecific intrathecal Ab pro-duction The total amount of prior antibiotictherapy for Lyme disease was extensive with57 of the patients in each treatment group hav-ing had more than 1 month of prior IV antibiotic
Figure Flow diagram of patient enrollment
Neurology 70 March 25 2008 (Part 1 of 2) 995
therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

therapy Patients reported having been symptom-atic with Lyme disease for a mean of 17 (SD 35)years before diagnosis and they reported havingbeen ill for a total of 90 (SD 68) years
Patients and controls on the screening measures Thegroups did not differ in estimated premorbid IQaccording to the Barona method (1115 [SD 62]for patients vs 1137 [SD 55] for controls) al-though healthy controls had superior IQ as esti-mated by the NAART (1089 [SD 81] for patientsvs 1159 [SD 60] for controls p 001) Therewere pronounced differences between the groupsin WMS-III scores for immediate memory (931
[SD 124] for patients and 1197 [SD 114] for con-trols p 001) and delayed (general) memory(947 [SD 102] for patients and 1221 [115] forcontrols p 001) The magnitude of these dif-ferences in memory substantially exceeded thedifference between the groups in estimated IQ
Patients and controls on postscreening measures Par-ticipants were entered into the study based on apredetermined level of impairment (patients) orlack of impairment (controls) using theWMS-IIIBecause Lyme disease typically affects multipleaspects of cognition227 patients and controlswere expected to differ at baseline on other cogni-
Table 1 Demographic and clinical characteristics of all participants by study group
Patients
Ceftriaxone group Placebo group Total Controls
Characteristic (n 23) (n 14) (n 37) (n 18)
Age in years mean (SD) 453 (137) 448 (127) 451 (132) 456 (113)
Female n () 140 (610) 80 (571) 220 (590) 130 (722)
Years of education mean (SD) 147 (24) 148 (27) 147 (25) 156 (24)
White n () 230 (100) 140 (100) 370 (100) 170 (944)
Employment n ()
Working full- or part-time 14 (609) 7 (500) 21 (570) 7 (339)
School full- or part-time 0 (00) 2 (143) 2 (54) 1 (55)
On leave from work or disabled 3 (130) 4 (286) 7 (189) 0 (00)
Other 6 (261) 1 (71) 7 (189) 10 (556)
Lyme disease symptom history n ()
Erythema migrans 13 (565) 7 (500) 20 (541)
Arthralgias or myalgias 23 (1000) 14 (1000) 37 (1000)
Arthritis 20 (870) 11 (786) 31 (838)
Facial nerve palsy 3 (130) 6 (429) 9 (243)
Meningitis or encephalitis 3 (130) 2 (143) 5 (135)
Polyneuropathy 18 (783) 11 (786) 29 (784)
Cognitive problems 23 (1000) 14 (1000) 37 (1000)
Months of prior IV antibiotics mean (SD) 25 (20) 19 (13) 23 (16)
Months of prior oral antibiotics mean (SD) 79 (102) 59 (76) 72 (92)
Rheumatology exam mean (SD)
No of joints with pain at rest or motion 59 (45) 64 (72) 61 (56)dagger 06 (07)dagger
No of fibromyalgia trigger points 14 (27) 23 (34) 18 (30)dagger 00 (00)dagger
No of tender joints 11 (24) 11 (21) 11 (23)dagger 01 (02)dagger
No of swollen joints 09 (16) 03 (83) 07 (14)dagger 00 (00)dagger
Neurology exam n ()
Sensory exam abnormality 16 (696) 11 (786) 27 (73)Dagger 4 (222)Dagger
Motor exam abnormality 8 (348) 6 (429) 14 (378) 2 (111)
Associated motor exam 7 (304) 5 (357) 12 (324) 3 (167)
Cranial nerves 3 (130) 4 (286) 7 (189) 2 (111)
Reflex exam 3 (130) 4 (286) 7 (189) 2 (111)
p 01dagger p 001Dagger p 0001
996 Neurology 70 March 25 2008 (Part 1 of 2)
tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

tive domains as well It was also expected basedon prior studies of posttreatment Lyme dis-ease52829 that the two groups might differ on sev-eral of the secondary clinical outcome measures
Patients and controls differed significantly onall clinical outcome measures both primary andsecondary Mean difference of at least one SD(moderate impairment) occurred in the psy-chomotor memory working memory and verbalfluency domains In the secondary measures theimpairment was severe in the physical measures(fatigue current pain physical functioning jointpain on exam) and was mild in the psychopathol-ogy measures (depression anxiety general symp-tom index mental component scale) Comparedwith published samples reports of pain were sim-ilar to those of postsurgery patients17 fatigue wassimilar to that of patients with multiple sclero-sis16 and limitations in physical functioning werecomparable with those of patients with conges-tive heart failure19 Individual subject scores onsecondary measures ranged from mild to severereflecting our enrollment criteria which did notpreselect patients based on a level of impairmentin these areas
Patients compared with controls had signifi-cantly more trigger points joints with pain andjoint swelling on rheumatologic exam (table 1) Pa-tients averaged 18 (SD 300) trigger points withonly one subject meeting the criteria for fibromyal-gia with more than 10 trigger points Joint pain wascommon elicited on exam in 35 patients with painonmotion (3437) beingmore common than tender-ness (1337 McNemar 2 1739 df 1 p 001) or swelling (1037 McNemar 2 2204df 1 p 001) The number of abnormal areason neurologic exam was greater in patients (mean18 12 median 2) than in controls (067 11median 0 t 33 df 53 p 001) Major neu-rologic abnormalities were infrequent in the pa-tients and absent in the controls (337 vs 018 p NS) However minor abnormalities on neuro-logic exam were found in 73 of the patients vs278 of the controls (Fisher p 001) most fre-quent was a mild sensory abnormality among thepatients
Completeness of follow-up Eighty-seven percent(3237) of patients and 100 (1818) of controlscompleted the week 12 acute-phase efficacy evalua-tion and week 24 follow-up durability evaluationrepresenting 20 patients in the ceftriaxone group 12in the placebo group and all healthy controls
Primary outcome Treatment effects on neuropsy-chological tests Arithmetic means and standarddeviations are given in table 2 The inference re-
garding ITT comparisons between the groupsover time is based on the best-fitting LMM thatcontained the main effects for group time anddomain and the two-way interactions of groupby time and group by domain (table 3)
The primary omnibus LMM analysis revealeda group-by-time interaction effect (p 004) in-dicating that with respect to cognition the groups(drug placebo and healthy controls) differed inchange over time (week 0 to week 12 week 12 toweek 24) across all domains The lack of a three-way interaction among group domain and timeindicates that differential improvement over timebetween the domains was not demonstrated ashad been hypothesized for memory and that thejoint effect of time and group can be describedwithout reference to a cognitive domain Becausethe primary omnibus p value was significant wethen conducted model-based estimation of the ef-fect of time within groups and pairwise compari-sons of the effect of time between the groupsThese comparisons demonstrated within-groupcognitive improvement (as measured by the sixcognitive domains) during the acute course oftreatment (from week 0 to week 12) for the pa-tients given ceftriaxone (p 001) but not for thepatients given placebo (p 015) or the healthycontrols (p 051) The cognitive improvementbetween baseline and week 12 in the drug-treatedpatients was better than in the healthy controls(p 001) and better than in the placebo-treatedpatients (p 0053)
During the antibiotic-free interval to week 24the patients initially on ceftriaxone lost the pref-erential cognitive gains seen at week 12 whereasthe two control groups (placebo and healthy vol-unteers) continued to show the same mild cogni-tive improvement as they had demonstrated in theacute phase At week 24 the within-group im-provement from baseline continued to be signifi-cant for the drug-treated group but it was alsonow seen in the placebo-treated group At week24 the between-group treatment effects were nolonger seen In summary the inability of the drug-treated group to sustain the distinguishing acute-phase improvement in cognition during thesubsequent antibiotic-free interval resulted in aloss of the differential treatment effect among thethree groups at week 24
Secondary outcomes Arithmetic means are pre-sented in table e-1 on the Neurologyreg Web site(wwwneurologyorg) and the best-fitting modelsfor each secondary outcome measure are pre-sented in table e-2 Table e-2 also provides model-based estimates of the means over time for
Neurology 70 March 25 2008 (Part 1 of 2) 997
subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

subjectsrsquo baseline severity scores corresponding tothe lowest or highest quartile of the distributionof baseline scores of all 37 patients These meansare obtained from the respective LMMs (given inthe right-hand side of table e-2) by substitutingthe selected baselines in the models When theLMM contained an interaction involving grouppost hoc comparisons between groups were per-formed within baseline severity level
The majority of the physical self-report mea-sures (fatigue current pain physical functioning)indicate interaction effects at week 12 favoringdrug over placebo as a function of baseline sever-
ity with the drug effect increasing with higherbaseline impairment Improvement continued toweek 24 but only for current pain and physicalfunctioning For example for physical function-ing as measured by PCS table e-2 indicates a two-way interaction (p 006) for baseline severityand treatment such that the beneficial effect ofdrug over placebo increased as baseline severityincreased model-based comparisons reveal themain effects of drug vs placebo (p 005) at highlevels of baseline severity As an illustration of theLMM results figure e-1 shows that among hypo-thetical subjects starting with a higher current
Table 2 Neuropsychological test results (raw scores) by domain treatment group and time
Baseline Week 12 Week 24
Mean (SD) Mean (SD) Effect size Mean (SD) Effect size
Drug group (n 23) (n 20) 12base (n 20) 24base
Motor 023 (134) 058 (088) 067 033 (105) 070
Psychomotor 021 (075) 019 (089) 054 012 (088) 056
Attention 012 (076) 015 (080) 027 018 (083) 036
Memory total 075 (107) 044 (129) 050 062 (130) 037
Buschke 113 (133) 079 (171) 042 098 (144) 031
Benton 036 (121) 008 (120) 025 026 (143) 016
Working memory 092 (109) 042 (094) 052 054 (089) 033
Fluency 073 (094) 038 (104) 055 030 (098) 11
Index 049 (063) 005 (074) 081 014 (068) 11
Placebo group (n 14) (n 12) (n 12)
Motor 006 (119) 006 (131) 013 036 (064) 049
Psychomotor 016 (061) 014 (057) 058 029 (071) 088
Attention 004 (120) 034 (070) 040 037 (092) 035
Memory total 036 (095) 020 (074) 006 022 (061) 003
Buschke 078 (137) 072 (144) 013 086 (126) 018
Benton 006 (109) 033 (073) 022 042 (062) 029
Working memory 032 (073) 037 (075) 034 004 (070) 037
Fluency 080 (038) 049 (039) 053 046 (044) 060
Index 028 (054) 009 (050) 030 006 (046) 072
Control group (n 18) (n 18) (n 18)
Motor 058 (063) 056 (068) 008 066 (068) 015
Psychomotor 098 (075) 093 (074) 011 118 (089) 038
Attention 035 (085) 060 (071) 043 065 (066) 059
Memory total 056 (043) 062 (049) 016 067 (055) 023
Buschke 038 (076) 072 (074) 051 072 (086) 046
Benton 073 (046) 052 (065) 032 062 (073) 017
Working memory 034 (069) 038 (064) 001 043 (070) 019
Fluency 048 (066) 057 (068) 018 059 (086) 021
Index 055 (040) 061 (036) 026 070 (037) 058
Benton negative scoring has been adjustedAn effect size of 02 reflects small improvement 05 reflects moderate improvement and 08 reflects large improvement40
998 Neurology 70 March 25 2008 (Part 1 of 2)
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
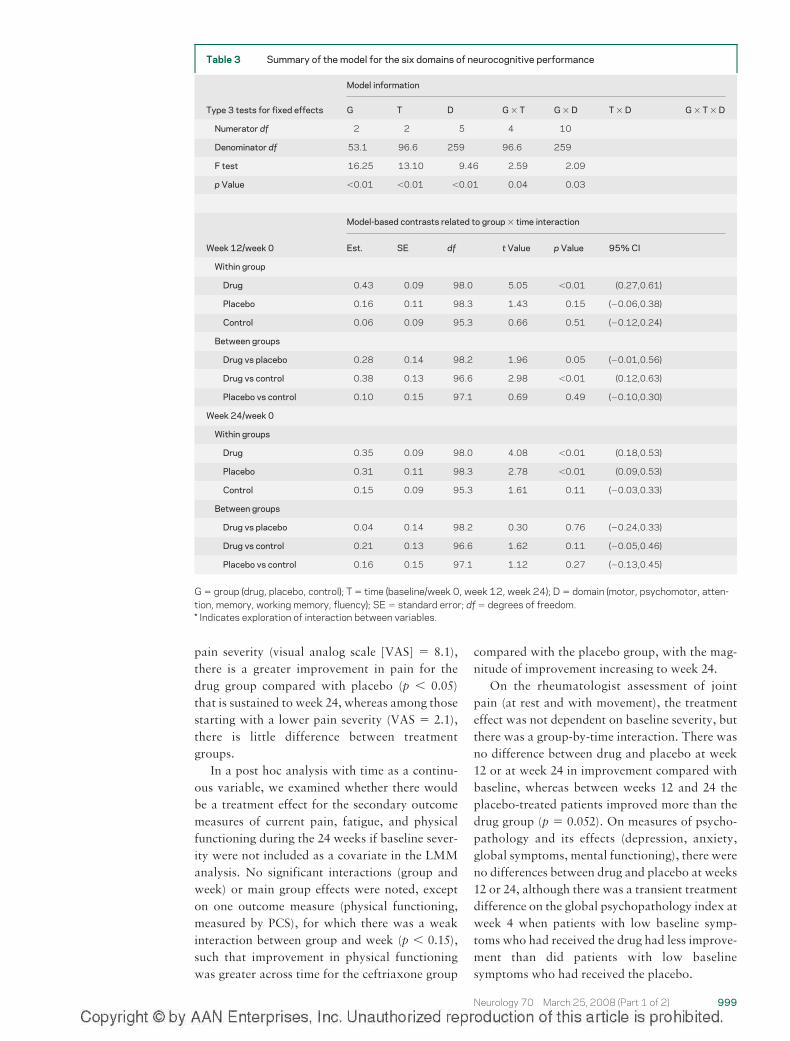
pain severity (visual analog scale [VAS] 81)there is a greater improvement in pain for thedrug group compared with placebo (p 005)that is sustained to week 24 whereas among thosestarting with a lower pain severity (VAS 21)there is little difference between treatmentgroups
In a post hoc analysis with time as a continu-ous variable we examined whether there wouldbe a treatment effect for the secondary outcomemeasures of current pain fatigue and physicalfunctioning during the 24 weeks if baseline sever-ity were not included as a covariate in the LMManalysis No significant interactions (group andweek) or main group effects were noted excepton one outcome measure (physical functioningmeasured by PCS) for which there was a weakinteraction between group and week (p 015)such that improvement in physical functioningwas greater across time for the ceftriaxone group
compared with the placebo group with the mag-nitude of improvement increasing to week 24
On the rheumatologist assessment of jointpain (at rest and with movement) the treatmenteffect was not dependent on baseline severity butthere was a group-by-time interaction There wasno difference between drug and placebo at week12 or at week 24 in improvement compared withbaseline whereas between weeks 12 and 24 theplacebo-treated patients improved more than thedrug group (p 0052) On measures of psycho-pathology and its effects (depression anxietyglobal symptoms mental functioning) there wereno differences between drug and placebo at weeks12 or 24 although there was a transient treatmentdifference on the global psychopathology index atweek 4 when patients with low baseline symp-toms who had received the drug had less improve-ment than did patients with low baselinesymptoms who had received the placebo
Table 3 Summary of the model for the six domains of neurocognitive performance
Model information
Type 3 tests for fixed effects G T D G T G D T D G T D
Numerator df 2 2 5 4 10
Denominator df 531 966 259 966 259
F test 1625 1310 946 259 209
p Value 001 001 001 004 003
Model-based contrasts related to group time interaction
Week 12week 0 Est SE df t Value p Value 95 CI
Within group
Drug 043 009 980 505 001 (027061)
Placebo 016 011 983 143 015 (006038)
Control 006 009 953 066 051 (012024)
Between groups
Drug vs placebo 028 014 982 196 005 (001056)
Drug vs control 038 013 966 298 001 (012063)
Placebo vs control 010 015 971 069 049 (010030)
Week 24week 0
Within groups
Drug 035 009 980 408 001 (018053)
Placebo 031 011 983 278 001 (009053)
Control 015 009 953 161 011 (003033)
Between groups
Drug vs placebo 004 014 982 030 076 (024033)
Drug vs control 021 013 966 162 011 (005046)
Placebo vs control 016 015 971 112 027 (013045)
G group (drug placebo control) T time (baselineweek 0 week 12 week 24) D domain (motor psychomotor atten-tion memory working memory fluency) SE standard error df degrees of freedom Indicates exploration of interaction between variables
Neurology 70 March 25 2008 (Part 1 of 2) 999
Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Variables associated with outcome measures Se-lected baseline variables were examined for inter-action effects with treatment group on thecognitive and self-report physical outcomes Like-lihood of improvement with ceftriaxone vs pla-cebo was not related to demographic variablesCSF values or clinical history (amount of priororal or IV antibiotic therapy the interval sincelast antibiotic course) Interaction effects betweenbaseline physical exam and treatment on outcomewere noted On joint exam patients with morejoints in pain at baseline had a preferential im-provement with ceftriaxone on the measures ofcognitive index at week 12 (p 006) and at week24 (p 004) and on the self-report measures offatigue (p 011) and pain (p 007) at week 24On neurologic exam patients with more areas ofabnormality at baseline had a preferential im-provement with ceftriaxone on the measure ofmemory at week 24 (p 011) and on the self-report measures of fatigue at week 12 (p 006)and week 24 (p 001) and physical functioningas measured by PCS (p 009) at week 24
Adverse events Five patients withdrew from thestudy because of adverse events two because ofthrombus (both on drug) one because of staphy-lococcal infection (on placebo) one because of anallergic reaction (on drug) and one because ofworsening joint pain (on placebo) that requirednarcotic pain medication Four patients remainedin the study despite adverse events that requiredeither early termination of study medication(three on drug two with allergic reactions andone with abdominal pain) or hospitalization (oneon drug cholecystectomy at week 16) for thesepatients ratings at weeks 12 and 24 continued tobe conducted without revealing treatment ran-domization The adverse reactions of seven ofthese nine patients were thought likely to havebeen directly related to the study treatment (pres-ence of a PICC line or medication) for a rate oftreatment-related adverse events of 6 of 23(261) among patients given IV ceftriaxone and1 of 14 (71) among patients given IV placeboall patients recovered fully
Masking Patients assigned to ceftriaxone did notdiffer from those assigned to placebo in their rateof guessing whether they had received active med-ication either at week 12 (684 vs 538 p
040) or at week 24 (750 vs 583 p 032)Analyses of covariance found no relationship tooutcome of a patientrsquos guess of medication vs pla-cebo and the actual treatment assignment at week12 At week 24 there were trends for patients who
believed that they had received active medicationto report less fatigue (p 008) and less impair-ment in physical function (p 005) but thismain effect was independent of actual treatmentassignment Finally patients who had severe sideeffects were not more likely to report a beneficialeffect from ceftriaxone indeed there was a trendfor patients with severe side effects to reportworsened physical functioning at week 12
Compliance Compliance was excellent Weeklynotes indicate that patients completed all 70doses except for those who terminated early Of37 patients who began treatment 30 completedthe full 10-week course (17 on ceftriaxone 13 onplacebo) Among the seven who did not completethe full course one person on placebo completed58 doses and among the six antibiotic noncompl-eters the total numbers of completed doses were5 11 19 35 54 and 58 patients with the latterthree totals returned for week 12 assessments
DISCUSSION This placebo-controlled double-masked trial tested the efficacy and safety of re-peated IV antibiotic treatment in a sample ofpatients with posttreatment Lyme encephalopa-thy Conservative inclusion criteria were used toattain high diagnostic confidence More than halfof the patients had prior courses of IV antibiotictherapy that exceeded the standard recommenda-tions for neurologic Lyme disease Although en-rollment required objective memory deficits thepatients had generalized mild to moderate cogni-tive deficits They also had more sensory andjoint abnormalities on physical exam and self-reports of marked pain fatigue and im-paired physical functioning replicating earlierfindings428
The primary result was that the three groups(ceftriaxone placebo health control) differed incognitive improvement over time (p 004) fa-voring ceftriaxone at week 12 but not at week 24At week 12 the end point for efficacy selected apriori patients given 10 weeks of IV ceftriaxonehad better within-group and between-group im-provement in cognition compared with theplacebo group or healthy controls This improve-ment was manifested broadly across several cog-nitive domainsmdashnot specific to the domain ofmemory Benefits from ceftriaxone exceeded thebenefits expected from retesting both in thehealthy controls and the placebo group For thedrug vs placebo comparison the borderline pvalue of 0053 reflects both the modest magnitudeof cognitive improvement and the small samplesize and it indicates that this finding has a slightly
1000 Neurology 70 March 25 2008 (Part 1 of 2)
elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

elevated risk of having occurred by chance 53vs 5 On self-report measures a benefit ofceftriaxone relative to placebo was observed atweek 12 for physical functioning current painand fatigue for those patients with greater sever-ity of symptoms at baseline
Durability of benefit was assessed at week 24after patients had been off of all treatment for 14weeks At this time point there was no differenceamong the three groups in cognitive improvementfrom baseline Sustained improvement howeverwas noted in physical functioning and currentpain among patients with greater baseline impair-ment suggesting that ceftriaxone may have bothshort- and long-term benefits for these symptomsA post hoc analysis suggested that the ceftriaxonegrouprsquos sustained improvement in physical func-tioning to week 24 could also be seen when base-line severity of impairment was not included as acovariate
Ceftriaxone has both infection-independentneuroprotective and infection-dependent antimi-crobial effects that could account for improve-ment in both primary and secondary measuresCeftriaxone upregulates the expression of gluta-mate transporters on the astroglia of rat brainswith neuroprotective effects30mdashpresumably be-cause of reduced extracellular glutamate a poten-tially neurotoxic neurotransmitter This couldexplain short-duration improvement in that con-tinued exposure to ceftriaxone would be requiredfor sustained upregulation of the glutamate trans-porter Another explanation for the observed re-lapse is that the course of ceftriaxone may havekilled some borrelia but it exerted little effect onother organisms in sequestered sites3132 There isone North American report of persistent B burg-dorferi by culture after antibiotic therapy33 andthere are several such European cases34-38 How-ever in our study the baseline CSF specimenswere PCR- and culture negative for B burgdorferi
Few variables at baseline showed consistentassociations with the primary or secondary out-come measures perhaps because of inadequatesample size which limits the power to detect in-teraction effects However the analysis suggeststhat the physical exam may be an important pre-dictor variable of short- and long-term responsebecause patients with more painful joints or moreareas of neurologic abnormality at baseline weremore likely to benefit from ceftriaxone than pla-cebo on various outcome measures
We did not find evidence that unmasking con-tributed significantly to the positive results in thisstudy because patients in each treatment group
did not differ in the rate of guessing assignment toceftriaxone Further patientsrsquo guesses had no re-lation with treatment response at the primaryoutcome time point of week 12 At week 24 al-though patientsrsquo guesses of ceftriaxone were asso-ciated with greater improvement in physicalfunctioning this was true for both the drug andplacebo groups when only those who guessedceftriaxone were included in the analysis a non-significant pattern continued to be evident ofgreater improvement in the drug group comparedwith the placebo group supporting a drug effectindependent of guess Third the presence of se-vere side effects was not associated with a morefavorable outcome on the primary or secondarymeasures at either week 12 or 24
How do these findings compare with those ofother placebo-controlled studies of posttreatmentLyme disease In two trials28 3 months of antibi-otics conferred no greater benefit than did pla-cebo on the primary SF-36 functional measure orthe secondary outcome measure of cognition In-ability to detect a treatment effect may reflect atrue failure of repeated antibiotic therapy or limi-tations of the study design (eg lack of severitystandard for study enrollment)2839 In contrast ina study of posttreatment Lyme disease for pa-tients with at least moderate fatigue improve-ment at 6 months on the Fatigue Severity Scalewas noted among 64 of patients who received 1month of IV ceftriaxone vs 185 who receivedIV placebo (p 0001)29 Improvements in cogni-tion or spinal fluid levels of OspA protein werenot detected but patients were not required tomanifest impairment on either of these measuresat study entry29 For post hoc comparison we re-analyzed our data using the post-Lyme fatiguersquosstudy enrollment criteria and we applied thesame definition for response (change 07 onFSS) Our results were compatible at 6 months667 of ceftriaxone-treated patients vs 25 ofplacebo-treated patients were responders (Fisherexact test p 005)
The strengths of this study were recruitment ofa rigorously diagnosed patient sample use ofquantitative measures of cognition with multiplealternative forms use of self-report instrumentsemployed in other trials to facilitate comparisoninclusion of a healthy control group to accountfor practice effects and the randomized placebo-controlled design that included a discontinuationphase to test durability Noteworthy is that thepattern of change and degree of cognitive im-provement during the 24 weeks were nearly iden-tical for the healthy volunteers and placebo-
Neurology 70 March 25 2008 (Part 1 of 2) 1001
treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

treated patients the healthy control grouptherefore served to increase the precision of theestimates of the treatment effect and to provideenhanced power for the overall analysis to detecttreatment effects in the active drug group thusreducing the risk of a type II error The primarylimitations of this study were its restrictive inclu-sion criteria (only 1 of screened patients wereenrolled) the relatively small sample size and thelack of posttreatment lumbar puncture or neuro-logic exam Therefore generalizability is uncer-tain to posttreatment Lyme patients withoutcognitive impairment or to seronegative patientswith persistent symptoms
Conclusions from this study are mixed At theprimary efficacy end point of week 12 IV ceftri-axone treatment resulted in greater improvementin cognition and among the more impaired inphysical functioning pain and fatigue Clinicalsignificance however depends on long-term ef-fects Notable were the long-term benefits for theceftriaxone group on physical functioning andpain among the more severely affected patients atbaseline because these are among the most trou-bling aspects of posttreatment Lyme disease28
However our primary interest in this study wason cognition for which the improvement was notsustained to week 24 Further adverse effects at-tributed to IV ceftriaxone occurred in 26 of pa-tients Therefore considering both the limitedduration of cognitive improvement and the risks10 weeks of IV ceftriaxone and then 14 weeks ofno antibiotic is not an effective strategy for sus-tained cognitive improvement Although certainsubgroups (patients with more joint or neurologicabnormalities) may experience long-term benefitfrom ceftriaxone the predictor analyses were ex-ploratory rather than hypothesis driven and theyrequire independent confirmation Pending suchconfirmation treatment strategies that are saferand more durable are needed
ACKNOWLEDGMENTNational Institutes of Neurological Disorders and Stroke (Al Kerza-Kwiatecki PhD Michael Nunn PhD) National Institute of Neuro-logical Disorders and Stroke DSMB (Justin McArthur MBBSAndrew Pachner MD Thomas Marcotte PhD Jorge Benach PhDRoland Martin MD Bruce Barton PhD) Columbia University re-search team (Megan Romano Dexterie Clemente MA Tani VieraMarcia Kimmeldorf PhD) Irving Center for Clinical Research at Co-lumbia University (Karen Marder MD Yakov Stern PhD MichaelJ Taylor PhD Robert Heaton PhD Wendy Coy PhD) Home CareServices Roche Pharmaceuticals participating private physicians (es-pecially Emilia Eiras MD Andrea Gaito MD Kornelia KeszlerMD and Kenneth Liegner MD) community leaders who helped ar-range screening clinics Patricia Smith Lyme Disease AssociationInc Time for Lyme Inc National Research Fund for Tick-BorneDiseases Phyllis Mervine MEd The Lyme Times Medical Diagnos-tic Laboratories University Hospital of Stony Brook Mel Evans
Richard Tilton PhD Steven Schutzer MD Allen Steere MD andMark Klempner MD
Received February 12 2006 Accepted in final form June 262007
REFERENCES1 Halperin JJ Krupp LB Golightly MG Volkman DJ
Lyme borreliosis-associated encephalopathy Neurol-ogy 1990401340ndash1343
2 Keilp JG Corbera K Slavov I Taylor MJ SackeimHA Fallon BA WAIS-III and WMS-III performance inchronic Lyme disease J Int Neuropsychol Soc 200612119ndash129
3 Logigian EL Kaplan RF Steere AC Chronic neuro-logic manifestations of Lyme disease N Engl J Med19903231438ndash1444
4 Fallon BA Tager F Fein L et al Repeated antibiotictreatment in chronic Lyme disease J Spirochetal Tick-borne Dis 19996117ndash122
5 Berglund J Stjernber L Ornstein K Tykesson-Joelsson K Walter H 5-y follow-up study of patientswith neuroborreliosis Scand J Infect Dis 200234421ndash425
6 Centers for Disease Control and Prevention (CDC)Case definitions for public health surveillanceMMWRMorb Mortal Wkly Rep 19903919ndash21
7 Centers for Disease Control and Prevention (CDC)Recommendations for test performance and interpreta-tion from the SecondNational Conference on SerologicDiagnosis of Lyme Disease MMWR Morb MortalWkly Rep 199544590ndash591
8 Wechsler D Wechsler Memory Scale Scale 3rd ed SanAntonio The Psychological Corporation 1997
9 Halperin JJ Logigian EL Finkel MF Pearl RA Prac-tice parameters for the diagnosis of patients with ner-vous system Lyme borreliosis (Lyme disease)Neurology 199646619ndash627
10 Wormser GP Nadelman RB Dattwyler RJ et al Prac-tice guidelines for the treatment of Lyme disease TheInfectious Diseases Society of America Clin Infect Dis200031(suppl 1)1ndash14
11 Donta ST Tetracycline therapy for chronic Lyme dis-ease Clin Infect Dis 199725(suppl 1)52ndash56
12 Barona A Reynolds C Chastain R A demographicallybased index of premorbid intelligence for the WAIS-RJ Consult Clin Psychol 198452885ndash887
13 Utti B North American Adult Reading Test agenorms reliability and validity J Clin Exp Neuropsy-chol 2002241123ndash1137
14 Sackeim HA Keilp JG Rush AJ et al The effects ofvagus nerve stimulation on cognitive performance inpatients with treatment-resistant depression Neuro-psychiatry Neuropsychol Behav Neurol 20011453ndash56
15 Keilp JG Sackeim H Mann JJ Correlates of trait im-pulsiveness in performance measures and neuropsy-chological tests Psychiatry Res 2005135191ndash201
16 Krupp LB LaRocca NG Muir-Nash J Steinberg ADThe fatigue severity scale Application to patients withmultiple sclerosis and systemic lupus erythematosusArch Neurol 1989461121ndash1123
17 Melzack R The short-form McGill Pain Question-naire Pain 198730191ndash197
1002 Neurology 70 March 25 2008 (Part 1 of 2)
18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

18 Ware JE Kosinski M Keller SD SF-36 Physical andMental Health Summary Scales A Userrsquos Manual Bos-ton The Health Institute 1994
19 Ware J Kosinski M SF-36 Manual for Users Version1 Boston The Health Institute 1994
20 Beck A Steer RA Beck Depression Inventory ManualSan Antonio Psychological Corporation 1987
21 Zung W A rating scale for anxiety disorders Psycho-somatics 197112371ndash379
22 Derogatis LR Rickels K Rock AF The SCL-90 and theMMPI a step in the validation of a new self-reportBr J Psychiatry 19761280ndash289
23 Diggle P Heagerty P Linag K-Y Zeger S Analysis ofLongitudinal Data Oxford Oxford University Press2002
24 Little RJA Rubin DB Statistical Analysis withMissingData 2nd ed Hoboken Wiley amp Sons Inc 2002
25 Cary N SASSTAT V9 Chicago SAS Institute Inc26 Schwarz G Estimating the dimension of a model Ann
Stat 19786461ndash46427 Krupp LB Masur D Schwartz J et al Cognitive func-
tioning in late Lyme borreliosis Arch Neurol 1991481125ndash1129
28 Klempner MS Hu LT Evans J et al Two controlledtrials of antibiotic treatment in patients with persistentsymptoms and a history of Lyme disease N Engl J Med200134585ndash92
29 Krupp LB Hyman LG Grimson R et al Study andtreatment of post Lyme disease (STOP-LD) a random-ized double masked clinical trial Neurology 2003601923ndash1930
30 Rothstein JD ReganMR Haenggeli C et al B-Lactamantibiotics offer neuroprotection by increasing gluta-mate transporter expression Nature 200543373ndash77
31 Singh SK Girschick J Molecular survival strategies ofthe Lyme disease spirochete Borrelia burdorferi LancetInfect Dis 20044575ndash583
32 Malawista SE Resolution of Lyme arthritis acute or pro-longed a new look Inflammation 200024493ndash504
33 Liegner KB Duray P Agricola M et al Lyme diseaseand the clinical spectrum of antibiotic responsivechronic meningoencephalomyelitides J SpirochetalTick-borne Dis 1997461ndash73
34 Schmidli J Hunziker T Moesli P Schaad UB Cultiva-tion of Borrelia burgdorferi from joint fluid threemonths after treatment of facial palsy due to Lyme bor-reliosis J Infect Dis 1988158905ndash906
35 Pfister HW Preac-Mursic V Wilske B Schielke E Sor-gel F Einhaupl KM Randomized comparison of ceftri-axone and cefotaxime in Lyme neuroborreliosisJ Infect Dis 1991163311ndash318
36 Oksi J Marjamaki M Nikoskelainen J Viljanen MKBorrelia burgdorferi detected by culture and PCR inclinical relapse of disseminated Lyme borreliosis AnnMed 199931225ndash232
37 Haupl T Hahn G Rittig M et al Persistence of Borre-lia burgdorferi in ligamentous tissue from a patientwith chronic Lyme borreliosis Arthritis Rheum 1993361621ndash1626
38 Preac-Mursic V Pfister HW Spiegel H et al First iso-lation of Borrelia burgdorferi from an iris biopsyJ Clin Neuroophthalmol 199313155ndash161
39 Kaplan RF Trevino RP Johnson GM et al Cognitivefunction in post-treatment Lyme disease do additionalantibiotics help Neurology 2003601916ndash1922
40 Cohen J Statistical Power Analysis for the BehavioralSciences 2nd ed New York Academic Press 1988
Neurology 70 March 25 2008 (Part 1 of 2) 1003
DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 10121201WNL0000284604611602d200870992-1003 Published Online before print October 10 2007Neurology
B A Fallon J G Keilp K M Corbera et al encephalopathy
A randomized placebo-controlled trial of repeated IV antibiotic therapy for Lyme
This information is current as of October 10 2007
ServicesUpdated Information amp
httpwwwneurologyorgcontent7013992fullhtmlincluding high resolution figures can be found at
Supplementary Material
00284604611602dDC1htmlhttpwwwneurologyorgcontentsuppl2008032201WNL00Supplementary material can be found at
References
httpwwwneurologyorgcontent7013992fullhtmlref-list-1at This article cites 32 articles 7 of which you can access for free
Citations
cleshttpwwwneurologyorgcontent7013992fullhtmlotherartiThis article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online





























