Embed Size (px)
Citation preview

Midwest Cardiovascular
Midwest Cardiovascular
Research Foundation
Research Foundation
Direct Thrombin Inhibitors and Direct Thrombin Inhibitors and GpGp 2b/3a Receptor Blockers in 2b/3a Receptor Blockers in
the Cardiac Cath Labthe Cardiac Cath Lab
Eric J Dippel, MD FACCEric J Dippel, MD FACC

Stable Angina
UnstableAngina
Non–Q-waveMI
Q-wave MI
Plaque Rupture
Adapted from Cannon CP. J Thrombolysis. 1995;2:205-218.

Thrombus FormationThrombus Formation


Events Leading to Thrombus FormationEvents Leading to Thrombus FormationAdhesion Activation Aggregation

Platelet ActivationPlatelet Activation
Resting PlateletResting Platelet Activated PlateletActivated Platelet
ThromboxaneThromboxane
Lysosomes (enzymes)
galactosidases
proteases
Lysosomes (enzymes)
galactosidases
proteases
Amine Storage Granules(Serotonin, ADP, ATP, Ca++)
Amine Storage Granules(Serotonin, ADP, ATP, Ca++)
α - Granules (secreted proteins)• Plasma proteins(fibrinogen, fibronectin, vWF, Factor V, plasminogen)
• Platelet-specific proteins(PF4, β -thromboglobulin proteins)
• Non platelet-specific proteins(thrombospondin, PDGF, amyloid protein precursor)
• Other(vascular permeability factor, IL-1, PADGEM)
α - Granules (secreted proteins)• Plasma proteins(fibrinogen, fibronectin, vWF, Factor V, plasminogen)
• Platelet-specific proteins(PF4, β -thromboglobulin proteins)
• Non platelet-specific proteins(thrombospondin, PDGF, amyloid protein precursor)
• Other(vascular permeability factor, IL-1, PADGEM)

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade


Ruptured PlaqueRuptured Plaque

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade

Coagulation CascadeCoagulation Cascade

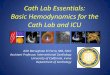
Targets for AntiTargets for Anti--ThromboticsThrombotics
Tissue factor
Plasma clottingcascade
Prothrombin
Thrombin
Fibrinogen Fibrin
Thrombus
Platelet aggregation
Conformational activation of GPIIb/IIIa
Collagen
Thromboxane A2
ADP
AT
AT
Aspirin
TiclopidineClopidogrel
GPIIb/IIIainhibitors
BivalirudinHirudin
Argatroban
FactorXa
LMWHHeparin
Pentasaccharides
Direct XaInhibitors
Fibrinolytics
Tissue Factor Inhibitors

Treatment of Occlusive Treatment of Occlusive Coronary ThrombusCoronary Thrombus
Fibrin
Plasminogenactivators– tPA– rPA– SK– TNK-tPA
Platelets
Antiplatelet therapy– Aspirin– Thienopyridines – GP IIb/IIIa inhibitors
Thrombin
Antithrombin therapy– Heparin– LMWH– Direct thrombin
Cannon CP. J Am Cannon CP. J Am CollColl Cardiol 1999;34:1395Cardiol 1999;34:1395--14021402

Cannon CP. J Am Coll Cardiol 1999;34:1395-1402
PlateletsPlatelets
FibrinFibrin
ThrombinThrombin
Thrombus occluding coronary arteryThrombus occluding coronary arteryThrombolyticThrombolytictherapytherapy
ExposesExposesclotclot--boundboundthrombinthrombin
New thrombinNew thrombingenerationgenerationPlatelet activationPlatelet activationCleaves fibrinogenCleaves fibrinogento fibrinto fibrin
PlasminPlasmin cleaves fibrincleaves fibrin
•• Lyses clotLyses clot↑↑ FDPsFDPs ((antiplateletantiplatelet
and anticoagulant)and anticoagulant)↓↓ FibrinogenFibrinogen
ReperfusionReperfusion
Activates plateletsActivates platelets
PAIPAI--1, thromboxane A1, thromboxane A22,,fibrinogenfibrinogen
↑↑ Platelet activationPlatelet activation↑↑ Thrombin productionThrombin production
VasoconstrictionVasoconstrictionInhibits plasminogen Inhibits plasminogen
activatorsactivators
Thrombus formationThrombus formationVessel reocclusionVessel reocclusion

Heparin RecipeHeparin Recipe
Kleiman. J Inv Card, Dec 2000.

Major Saccharide Components Major Saccharide Components in Pharmaceutical Heparinin Pharmaceutical Heparin
OO OO
OO
NNHHSSOO33--
OO OO
CCOO22--
OOHHOO
OOHH
OONNHHSSOO33
--OO
OOOO
CCOO22--
OOHHOOHH OO
OOHH
CCHH22OOSSOO33--
OOOOOO
NNHHSSOO33--
OOHH
OO
CCHH22
OO
OOSSOO33--CCOO22
--
OOOOSSOO33
--NNHHAAcc
OO
OOHH OOSSOO33--
OO
CCHH22
OOHHOO
OOHH
CCHH22OOSSOO33--
NNHHSSOO33--
OOSSOO33--
OOHHCCOO22--
OO OO
OO
OO
OOHHOO
OOHH
NNHHSSOO33--
OO
OOSSOO33--
CCHH22OOHH
CCHH22
CCOO22--
OOSSOO33--
OOSSOO33--
Trisulfated DisaccharideTrisulfated Disaccharide Disulfated DisaccharideDisulfated Disaccharide
OO OO
OOOOOO
NNHHSSOO33--
OOHH
OO
CCHH22
OO
OOSSOO --CCOO22--
OOOOSSOO33
--NNHHSSOO33
--
OO
OOHH OOSSOO33--
OO
CCHH22
OOHHOO
OOHH
CCHH22OOSSOO33--
NNHHSSOO33--
OOSSOO33--
OOHHCCOO22--
Antithrombin III Pentasaccharide Binding SitesAntithrombin III Pentasaccharide Binding Sites
33

HeparinHeparin
♦♦ NonNon--specific binding to circulating specific binding to circulating proteins, acute phase reactants, and proteins, acute phase reactants, and cellular binding sitescellular binding sites
♦♦ Directly activates plateletsDirectly activates platelets♦♦ Potentiates the platelet response to low Potentiates the platelet response to low
levels of agonists such as ADPlevels of agonists such as ADP♦♦ Unpredictable dose responseUnpredictable dose response

Antithrombotic Therapies and Platelet Antithrombotic Therapies and Platelet Aggregation in Aggregation in NormalsNormals
Xiao Z, Theroux P. Circ 1998;97:251-256
0
2
4
6
8
10
12
14 Saline UFH LMWH ARG
ADP (0.3125 μ M) TRAP (0.625 μ M)
Per
cent
Max
imum
* p < 0.05, ** p < 0.01 vs. control
**
*
*

Platelet Activation by Unfractionated HeparinPlatelet Activation by Unfractionated Heparin
(Normal Subjects) Knight CJ et al. Eur Heart J. 1998;19:1239
0
1
2
3
4
5
0 1 2 3 4 0
1
2
3
4
5Unstimulated ADP 1.0 ( μ mol.1-1)
0 1 2 3 4 Heparin / fragmin (units.ml-1)
Fibr
inog
en B
indi
ng In
dex UFH
LMWH

ProthrombinF 1.2
Va Ca ++
Xa Platelet
F1.2 Thrombin PlateletActivation
Fibrinogen AT III
TAT IIIFPA Fibrin 1

Thrombin Rebound After Cessation of Intravenous Heparin 0.5
0.4
0.3
0.2
0.1
0
14
12
10
8
6
4
2
0
F1.2FPA
Time 0 3 Hr 6 Hr 10 Hr 24 Hr
FPAF 1.2
(*p<0.03; **p<0.001)
1 Miller, Granger, Califf. Circ. 1993;88:I-202

Thrombin Generation Follows Heparin Thrombin Generation Follows Heparin Discontinuation in Patients with Acute Coronary Discontinuation in Patients with Acute Coronary SyndromesSyndromes
0
1
2
3
4
5 B a s e lin e IV H e p a r in W e a nD /C H e p a r in S C H e p a r in W e a n
Baseline 1 Hour 4 Hours 24 Hours
F1.2
(nM
)
1Becker RC. JACC 1999;34:1020

Disadvantages of UFHDisadvantages of UFH
Unfractionated HeparinUnfractionated Heparin
ThrombocytopeniaThrombocytopenia
PoorBioavailability
PoorBioavailability
AnticoagulantResponse Variations
AnticoagulantResponse Variations
BleedingBleeding
Stronger Drug
Interactions
Stronger Drug
Interactions

Heparin/AT complex inhibits thrombin and Factor Heparin/AT complex inhibits thrombin and Factor XaXaMust have adequate AT present for anticoagulant effectMust have adequate AT present for anticoagulant effect
Heparin/LMWH: mechanism of action Heparin/LMWH: mechanism of action Heparin/LMWH: mechanism of action
2
1
AntithrombinThrombin
Heparin
Pentasaccharidesequence
Antithrombin FactorXa
LMWH
Pentasaccharidesequence
Heparin chains with pentasaccharidesequence (~30%)
bind to AT causing a conformational
change
Thrombin inhibition requires “bridging”by heparin chain (at least 18 units)
LMWH has greater activity against Xathan thrombin
Antithrombin
X/E//109.a.1

HirudinHirudin: mechanism of action : mechanism of action
Binds directly to two sites on thrombinBinds directly to two sites on thrombin
Binding is highly specific and almost irreversibleBinding is highly specific and almost irreversible——very long halfvery long half--life may life may account for the high bleed rates seen with account for the high bleed rates seen with hirudinshirudins in clinical trialsin clinical trials
2
1
ThrombinHirudin
Inactivates both circulating and clot-bound thrombin—hirudin displaces thrombin from fibrin
Fibrin
X/E//110.a.1

Structure of Thrombin: Structure of Thrombin: Structure of Thrombin:
(Gly)4
C-terminal dodecapeptide(Exosite 1-binding portion)
2
1
Thrombin
Gly-Pro-Arg-Pro(active-site-binding portion)
Fibrin
A/E//20.b.1
Active SiteActive Site: cleaves fibrinogen and coagulation factors: cleaves fibrinogen and coagulation factors
ExositeExosite Site 1Site 1: activates platelets, activates protein C, anchors fibrinogen: activates platelets, activates protein C, anchors fibrinogen

Bivalirudin: mechanism of action Bivalirudin: mechanism of action Bivalirudin: mechanism of action
(Gly)4
C-terminal dodecapeptide(Exosite 1-binding portion)
2
1
Thrombin
Gly-Pro-Arg-Pro(active-site-binding portion)
Fibrin
Inactivates both circulating and clot-bound thrombin—bivalirudin competitively displaces thrombin from fibrin
Thrombin slowly cleaves Arg3-Pro4 bond, resulting in recovery of thrombin active site function
A/E//20.b.1

Direct Thrombin InhibitorsDirect Thrombin Inhibitors
AngiomaxAngiomax®® (bivalirudin)(bivalirudin)ReversibleReversible
PTCAPTCA25 min25 min
NovastanNovastan®® ((argatrobanargatroban))ReversibleReversible
HITHIT45 min45 min
RefludanRefludan®® (lepirudin)(lepirudin)IrreversibleIrreversible
IndicationIndication: HIT: HITTT1/21/2 = 1.3 hr= 1.3 hr
ThrombinThrombin

ArgatrobanArgatroban: mechanism of action: mechanism of action
ArgatrobanArgatroban only binds near the active site on thrombinonly binds near the active site on thrombin
ArgatrobanArgatroban has a short halfhas a short half--lifelife
2
1
ThrombinArgatroban
54% of argatroban binds to human serum proteins
X/E//111.a.1

Pharmacokinetic ProfilePharmacokinetic Profile
Infusion 2.5 mg/kg/h
[Biv
aliru
din]
Mea
n ng
/mL
Time from start of bivalirudin bolus (hours)
Bolus 0.75 mg/kg
0
2
4
6
8
10
12
14
0 2 4 6 8
t ½ = 25 min.Clearance = 3.4 mL/min/kg

Hemorrhagic outcomesHemorrhagic outcomes
0%
2%
4%
6%
8%
10%
Any majorbleed
3g/dL[Hgb]
Transfuse≥2U
5g/dL[Hgb]
RP or ICbleed
Heparin(N=2151)Bivalirudin(N=2161)
p < 0.001 p < 0.001 p < 0.001 p < 0.001 p = 0.020

20.0%
8.5%
12.7%
3.1%1.2% 1.9%
6.0%
0.0%0%
5%
10%
15%
20%
25%
None(≥90 mL/min)
Mild(60–89 mL/min)
Moderate(30–59 mL/min)
Severe(<30
mL/min)
Bleeding by renal functionBleeding by renal functionIn
cide
nce
of m
ajor
ble
edin
g
Robson, J Invas Cardiol. 2000, 12SupplF: 33F-36F
bivalirudin
heparin
B•A•T
n=275 n=454n=461 n=301n=250 n=12n=7n=256

Mechanical
Distal Embolization
Mechanical Plugging
Serotonin Release
Vasoconstriction
Plaque Rupture
Thrombus
Vasoconstrictive

Platelet aggregate
plugging a
small vessel
Platelet aggregate
plugging a
small vessel
Activated IIb/IIIa
stained red
Activated IIb/IIIa
stained red
Microvascular InjuryMicrovascular Injury

Comparing the Physical Comparing the Physical Differences of the Glycoprotein Differences of the Glycoprotein
2b/3a Inhibitors2b/3a Inhibitors
Platelet Surface
Fibrinogen
2b/3aaV/β3
MAC-1
abciximab
2b/3a
“Small Molecules”

Resting plateletGP IIb/IIIa receptors in
unreceptive state
Inhibition of platelet aggregation
GP IIb/IIIa receptors occupied by antagonistsAgonist
ADP, thrombin, collagen and others
GP IIb/IIIa receptor antagonist
Fibrinogen
Aggregating platelets
GP IIb/IIIa receptors occupied by fibrinogen which forms bridges between adjacent platelets
Response to Platelet Activation

Abciximab Eptifibatide TirofibanPlatelet-bound half-life Long Short Short
(hours) (seconds) (seconds)
Plasma half-life Short Long Long(minutes) (2.5 hr) (1.8 hr)
Drug-to-receptor ratio 1.5–2.0 250–2,5001 >2502
% of dose in bolus ~75%3 <2–5% <2–5%
Dosage adjustment inrenal insufficiency None Yes Yes
1 IMPACT-II and PURSUIT doses.2 RESTORE and PRISM- PLUS doses.3 For any individual receiving a weight-adjusted, 12-hour infusion.
Major Differences AmongMajor Differences AmongGPIIb/IIIa InhibitorsGPIIb/IIIa Inhibitors

Abciximab Eptifibatide Tirofiban↓ Thrombin generation ++ + +↑ Activated clotting time +35 sec +25 sec N/A
Reversibility* 12 hrs 4–6 hrs >4 hrsReversibility with platelets Yes No No
Major Differences AmongMajor Differences AmongGPIIb/IIIa InhibitorsGPIIb/IIIa Inhibitors
Anticoagulant Properties
*50% Return of platelet function without platelet transfusion

Total dose of small moleculeantagonist is a >100-fold
molar excess over GPIIb/IIIa
Total dose of small moleculeantagonist is a >100-fold
molar excess over GPIIb/IIIa
Total dose of abciximabis an ~twofold molar excess
over GPIIb/IIIa
Total dose of abciximabis an ~twofold molar excess
over GPIIb/IIIa
During Drug InfusionDuring Drug Infusion
80% 80%
80%
80%
80%
Numbers represent GPIIb/IIIa receptor occupancy and are an approximation
80%
80%80%
80%
AbciximabAbciximab Small MoleculeSmall Molecule

Platelet Transfusion Rapidly Normalizes Bleeding TimePlatelet Transfusion Rapidly Platelet Transfusion Rapidly Normalizes Bleeding TimeNormalizes Bleeding Time
Abciximab
-

Large pool of free drugto block transfused platelets
Very little free drug to blocktransfused platelets
Immediately After Platelet TransfusionImmediately After Platelet Transfusion
80% 80%
80%
80%
80%
0%
0%
20%
AbciximabAbciximab
80%
80%80%
80%
79%
80%
80%
Small MoleculeSmall Molecule
Numbers represent GPIIb/IIIa receptor occupancy and are an approximation

Months after randomizationIMPACT II: Lancet 1997; 349:1422-28, ACC 1999 Oral presentation, PURSUIT: NEJM 1998; 339:436-43, ESC 1998; Oral
Presentation,PRISM-PLUS: NEJM 1998; 338:1488-97, RESTORE: Circ. 1997; 96:1445-53, JACC 1998; 32:28-34, PARAGON A: Circ 1998; 97:2386-95 ESPRIT: SCAI 2000, Oral Presentation.
-1.0
-0.5
0.0
0.5
1.0
126 36241
.
Absolute Differences over Time
Effects of Small Molecule Therapy on Mortality%
cha
nge
vspl
aceb
o
IMPACT II (n = 4,010)
PURSUIT (n = 9,461)
RESTORE (n = 2,141)
PRISM+ (n = 1,570)
PARAGON A (n = 7,232)
ESPRIT (n = 2,007)

Absolute Differences over TimeAbsolute Differences over Time
-4.5
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0.5
1
Months since randomization1 126 36 4824
† p = 0.037* p = 0.071
‡ p = 0.202
Abciximab
CircEPIC: NEJM 1994; 330:956-61, Lancet 1994; 343:881-86, JAMA 1997; 278:479-84, CAPTURE: Lancet 1997; 349:1429-35, ACC 2000 oral pres
., EPILOG: Internal Data, Centocor, EPISTENT: Lancet 1998; 352:87-92, NEJM 1999; 341:319-27, Lancet 1999; 354:2019-24, RAPPORT:. 1998; 98:734-41, ERASER: Circ . 1999; 100; 799-806, ADMIRAL: ETC 2000, oral pres., Neumann : JACC 2000; 35:915-21
*†
‡
EPIC (B&I) (n = 1404)EPILOG (n = 2792)EPISTENT (n = 1603)ERASER (n = 225)
CAPTURE (n = 1265)RAPPORT (n = 483)
ADMIRAL (n = 300)Neumann(n = 401)
Effects of Abciximab Therapy on Mortality%
cha
nge
vspl
aceb
o

Mortality at Maximum Duration of Follow-Up: All Patients
Intention to Treat HR 0.83 (0.73–0.94)

Platelet Thrombi Cause Vessel Occlusion Platelet Thrombi Cause Vessel Occlusion at Site of Injury and Downstreamat Site of Injury and Downstream
Vasocconstriction
Mechanical Obstruction
Vasoconstriction
MechanicalObstruction
Platelet Aggregation
Platelet Attachment at Site of Endothelial Injury
Transient Platelet Aggregation

Stenting the Tip of the IcebergStenting the Tip of the Iceberg

Coronary TreeCoronary Tree----Stenting the Tip of the IcebergStenting the Tip of the Iceberg

3.7%1.0%In-hosp MACEIn-hosp MACE
Sirolimus (n=190)Sirolimus (n=190) Control (n=210)Control (n=210)
%
%
In-hospital MACE Out-of-hosp death|MI TVR (Non-TL) TLR
SIRIUS - Clinical EventsSIRIUS - Clinical EventsAll Events (to 270 days)All Events (to 270 days)
3.2%3.2% 3.8%3.8%TVR (Non-TL)TVR (Non-TL)
P<0.001P<0.001
4.7%4.7%
16.7%16.7%
TLRTLR
7.4%7.4% 7.2%7.2%2.4%2.4%
0.5%0.5%Out-of-hosp death|MIOut-of-hosp death|MI

MetaMeta--analysis of Balloon vs. Stent Trialsanalysis of Balloon vs. Stent Trials11
1.3 1.5
4.8
5.7
1 1
44.7
0
1
2
3
4
5
6
7BalloonStent
30 Day* 6 Month** 30 Day 6 MonthDEATH DEATH / MI
% P
atie
nts
p=0.970
1Kong, Hasselblad, Topol, Califf (submitted)
p=0.997
p=0.106p=0.343
* 3314 pts** 4345 pts (17 trials)

Mortality Follow-up - AbciximabLatest Follow-up in All Randomized Trials
8.6
2.6 2.4
6.7
2.8
4.5
7.3
8.5
6.8
1.71.0
6.3
0.0
4.13.3
6.0
0123456789
10
EPIC (3
years
)EPILOG (1
year)
EPISTENT (1 ye
ar)
CAPTURE (4 ye
ars)
ERASER (6 m
onths)
RAPPORT (6 m
onths)
ADMIRAL (6
months)
Neuman
n (1 ye
ar)
PlaceboAbciximab
% o
f Pat
ient
s
p = 0.037
EPIC: JAMA 1997; 278:479-84 , CAPTURE: Simoons, oral presentation, ACC 2000, EPILOG: Internal Data, Centocor,EPISTENT: Lancet 1999; 354:2019-24, RAPPORT: Circ. 1999; 98:734-41, ERASER Circ. 1999;100:799-806, Neumann: JACC 2000; 35(4):915-921, personal comm, JF Neumann; ADMIRAL: Montelescot, oral presentation, ACC 2000

10 5 0 5 10
Hemorrhage Death, MI, revasc
Heparin +ReoPro (100%)n = 64
Bivalirudin™ +ReoPro (24%)n = 144
% of patients with events at 7 days
75% reductionp-value <0.013
1.4% 2.8%
6.3% 7.8%
Clinical Results of CACHET BC Clinical Results of CACHET BC TrialTrial

REPLACE-2: Design
Multicenter international trial• United States 78% of patients• Europe 15%• Canada 7%• Double-blind, double dummy design
6002
Urgent or elective
PCIpatients
AspirinClopidogrel
Stent
Endpoints30-dayDeathMIRevascHemorrhage
Economics, ischemia6, 12m follow up
BivalirudinProvisional GPIIb/IIIa
Abciximabor
Eptifibatide
Heparin
2994
3008
Lincoff M et al. JAMA 2003

30-day endpoints
7.1%5.8%
4.1%
2.0%
5.2%
9.2%
6.6%
1.6%
3.5%
10.0%
2.4%
7.6%
Death, anyMI, revasc,
bleed
Death, anyMI, revasc
CKMB>3xULN
Major bleed Death, QMI,revasc
Death, QMI,revasc, bleed
Heparin + GPIIb/IIIa (N=3008)Bivalirudin (N=2994)
p=0.329 p=0.328 p=0.197 p<0.001 p=0.178 p=0.002
Lincoff AM et al JAMA 2003; 289: 853-863
All pre-specified endpoints of the trial were met

0 0.5 1 1.5 2
Risk ratio ±95% CIfor death at 6 months
BivalirudinREPLACE-2
N=6002
Mortality vs. heparin at 6 mo
Kong et al 2003Am J Cardiol 2003; 92: 651-5
12 trials – 20,186 patients (Odds ratio)
Karvourni et al 2003J Am Coll Cardiol 2003; 41: 26-32
19 trials 20,137 patients (Risk ratio)
GPIIb/IIIameta-analysis
0 0.5 1 1.5 2
Heparin betterNew Rx better Heparin betterNew Rx better
Odds ratio ±95% CIfor death at 6 months

Background: Current Management of ACSBackground: Current Management of ACS
Early invasive strategy if moderate-high risk1,2
Median time to cath 21 hours3
Revascularization with PCI or CABG1,2
55% PCI, 12% CABG, 33% medical mgt3
Triple anti-platelet therapy1,2
AspirinClopidogrel (initiated pre or post angiography)GP IIb/IIIa inhibitors- started upstream in all pts or in the CCL for PCI
Unfractionated or LMW heparin1,2,4
Early invasive strategy if moderate-high risk1,2
Median time to cath 21 hours3
Revascularization with PCI or CABG1,2
55% PCI, 12% CABG, 33% medical mgt3
Triple anti-platelet therapy1,2
AspirinClopidogrel (initiated pre or post angiography)GP IIb/IIIa inhibitors- started upstream in all pts or in the CCL for PCI
Unfractionated or LMW heparin1,2,4
1 Braunwald et al JACC 2002; 2 Bertrand et al. EHJ 2002; 3www.crusade.org; 4SYNERGY. JAMA 2004;292:45-541 Braunwald et al JACC 2002; 2 Bertrand et al. EHJ 2002; 3www.crusade.org; 4SYNERGY. JAMA 2004;292:45-54

In moderate-high risk patients with ACS undergoing an invasive strategy, compared to UFH or LMWH + GP IIb/IIIa inhibitors:
• Bivalirudin + GP IIb/IIIa inhibitors will result in less adverse ischemic events and less bleeding
• Bivalirudin alone will result in similar rates of ischemic events and markedly reduced bleeding
In moderate-high risk patients with ACS undergoing an invasive strategy, compared to UFH or LMWH + GP IIb/IIIa inhibitors:
• Bivalirudin + GP IIb/IIIa inhibitors will result in less adverse ischemic events and less bleeding
• Bivalirudin alone will result in similar rates of ischemic events and markedly reduced bleeding
Bivalirudin in ACS: Hypotheses

Moderate-high risk
ACS
Study Design – First RandomizationStudy Design – First Randomization
Ang
iogr
aphy
with
in 7
2h
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
UFH orEnoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
BivalirudinAlone
R*
*Stratified by pre-angiography thienopyridine use or administration*Stratified by pre-angiography thienopyridine use or administration
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800)
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800)
ACUITY Design. Stone GW et al. AHJ 2004;148:764–75ACUITY Design. Stone GW et al. AHJ 2004;148:764–75
Medicalmanagement
PCI
CABG

Moderate-high risk
ACS
Study Design – Second RandomizationStudy Design – Second Randomization
Ang
iogr
aphy
with
in 7
2h
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800)
Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800)
ACUITY Design. Stone GW et al. AHJ 2004;148:764–75ACUITY Design. Stone GW et al. AHJ 2004;148:764–75
Aspirin in allClopidogrel
dosing and timingper local practice
Aspirin in allClopidogrel
dosing and timingper local practice
Medicalmanagement
PCI
CABGBivalirudin
Alone
UFH or EnoxaparinUFH or EnoxaparinRoutine upstream
GPI in all ptsGPI started in
CCL for PCI onlyR
BivalirudinBivalirudin
RRoutine upstream
GPI in all ptsGPI started in
CCL for PCI only

11.7%11.8% 1.01 (0.90-1.12) <0.0010.93
0 1 2
Risk ratio±95% CI
Risk ratio±95% CI
Primaryendpoint
Primary Endpoint Measures (ITT)Primary Endpoint Measures (ITT)UFH/Enoxaparin + GPI vs. Bivalirudin + GPIUFH/Enoxaparin + GPI vs. Bivalirudin + GPI
Net clinical outcome
Ischemic composite
Major bleeding
Bivalirudin + IIb/IIIa betterBivalirudin + IIb/IIIa better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Bival+ IIb/IIIa
UFH/Enox+ IIb/IIIa RR (95% CI)
p value(non inferior)
(superior)
7.3%7.7% 1.07 (0.92-1.23) 0.0150.39
5.7%5.3% 0.93 (0.78-1.10) <0.0010.38
Upp
er b
ound
ary
non-
infe
riorit
y

0 1 2
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Risk ratio±95% CI
Risk ratio±95% CI
Primaryendpoint
Bivalalone
UFH/Enox+ IIb/IIIa RR (95% CI)
Net clinical outcome
Ischemic composite
Major bleeding
Primary Endpoint Measures (ITT)Primary Endpoint Measures (ITT)
Upp
er b
ound
ary
non-
infe
riorit
y
11.7%10.1% 0.86 (0.77-0.97) <0.0010.015
7.3%7.8% 1.08 (0.93-1.24) 0.020.32
5.7%3.0% 0.53 (0.43-0.65) <0.001<0.001
p value(non inferior)
(superior)
UFH/Enoxaparin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin Alone

Components of the Ischemic CompositeComponents of the Ischemic Composite
7.3%
1.3%
4.9%
2.3%2.7%2.4%
5.0%
7.7%
1.5% 1.6%
7.8%
5.4%
Ischemiccomposite
Death Myocardialinfarction
Unplannedrevasc forischemia
30 d
ay e
vent
s (%
)
UFH/Enox+GPI (N=4603) Bivalirudin+GPI (N=4604) Bivalirudin alone (N=4612)
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone
PSup = 0.32 PSup = 0.34 PSup = 0.35 PSup = 0.78

Major Bleeding EndpointsMajor Bleeding Endpoints
11.8%
5.7%
11.1%
5.3%3.0%
9.1%
All major bleeding Non CABG major bleeding(primary endpoint)
30 d
ay e
vent
s (%
)
Heparin+GPI (N=4603) Bivalirudin+GPI (N=4604) Bivalirudin alone (N=4612)
UFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin + GPI vs. Bivalirudin Alone
PSup=0.38 PSup<0.0001PSup=0.31 PSup<.001

0 1 2
Yes (n=3197)No (n=6008)
Low (0-2) (n=1291)Intermed (3-4) (n=4407)
High (5-7) (n=2449)
Elevated (n=5368)Normal (n=3841)
Risk ratio±95% CI
Risk ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
9.2%11.3%
12.2%11.1%
P Pint
0.76 (0.65-0.89)1.02 (0.86-1.21)
12.2%7.1%
13.3%9.4%
0.92 (0.80-1.06)0.75 (0.61-0.93)
0.230.01
<0.0010.83
0.35
0.02
0.18
13.0%8.6%
13.7%10.6%
0.96 (0.80-1.14)0.81 (0.69-0.95)
0.610.01 0.42
Biomarkers (CK/Trop)
ST Deviation
TIMI Risk Score
Pre Thienopyridine
6.4% 10.2% 0.63 (0.43-0.91) 0.019.4% 10.2% 0.92 (0.77-1.10) 0.34
13.9% 15.2% 0.92 (0.76-1.11) 0.36
Yes (n=5192)No (n=4023)
RR (95% CI)
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Net Clinical Outcome CompositeNet Clinical Outcome CompositeUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone

ConclusionsConclusions
♦♦ Heparin has significant limitationsHeparin has significant limitations–– Requires a cofactor (ATIII)Requires a cofactor (ATIII)–– NonNon--specific protein bindingspecific protein binding–– Variable dose responseVariable dose response–– Activates plateletsActivates platelets–– ThrombocytopeniaThrombocytopenia–– Thrombin reboundThrombin rebound–– Would not gain FDA approval in 2007Would not gain FDA approval in 2007

Conclusions Conclusions
♦♦ Low risk elective PCILow risk elective PCI–– Bivalirudin alone provides superior clinical Bivalirudin alone provides superior clinical
outcomes compared to UFH alone, and no outcomes compared to UFH alone, and no difference compared to UFH / difference compared to UFH / GpGp 2b3a2b3a
–– Provided they have been adequately preProvided they have been adequately pre--treated with ASA and Plavixtreated with ASA and Plavix
–– Bivalirudin alone has less bleeding than UFH / Bivalirudin alone has less bleeding than UFH / GpGp 2b3a2b3a

ConclusionsConclusions
♦♦ Moderate to high risk PCIModerate to high risk PCI–– No difference in ischemic complications No difference in ischemic complications
comparing bivalirudin alone comparing bivalirudin alone vsvs UFH / UFH / GpGp 2b3a 2b3a vsvs bivalirudin / bivalirudin / GpGp 2b3a2b3a
–– Provided patients are adequately preProvided patients are adequately pre--loaded loaded with ASA and Plavixwith ASA and Plavix
–– Less bleeding with bivalirudin alone Less bleeding with bivalirudin alone vsvs UFH / UFH / GpGp 2b3a 2b3a vsvs bivalirudin / bivalirudin / GpGp 2b3a2b3a

““Death is a very Death is a very good way to cut good way to cut
down on expenses.down on expenses.””Woody AllenWoody AllenLove and DeathLove and Death