Embed Size (px)
Citation preview
1/26/2014
1
A Practical Optometric Approach To A Practical Optometric Approach To
HeadachesHeadaches
Leonid Skorin, Jr., OD, DO, MS, FAAO, FAOCOLeonid Skorin, Jr., OD, DO, MS, FAAO, FAOCO
Mayo Clinic Health System in Albert LeaMayo Clinic Health System in Albert Lea
Assistant Professor of OphthalmologyAssistant Professor of Ophthalmology
Mayo Clinic College of MedicineMayo Clinic College of Medicine
[email protected]@mayo.edu
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
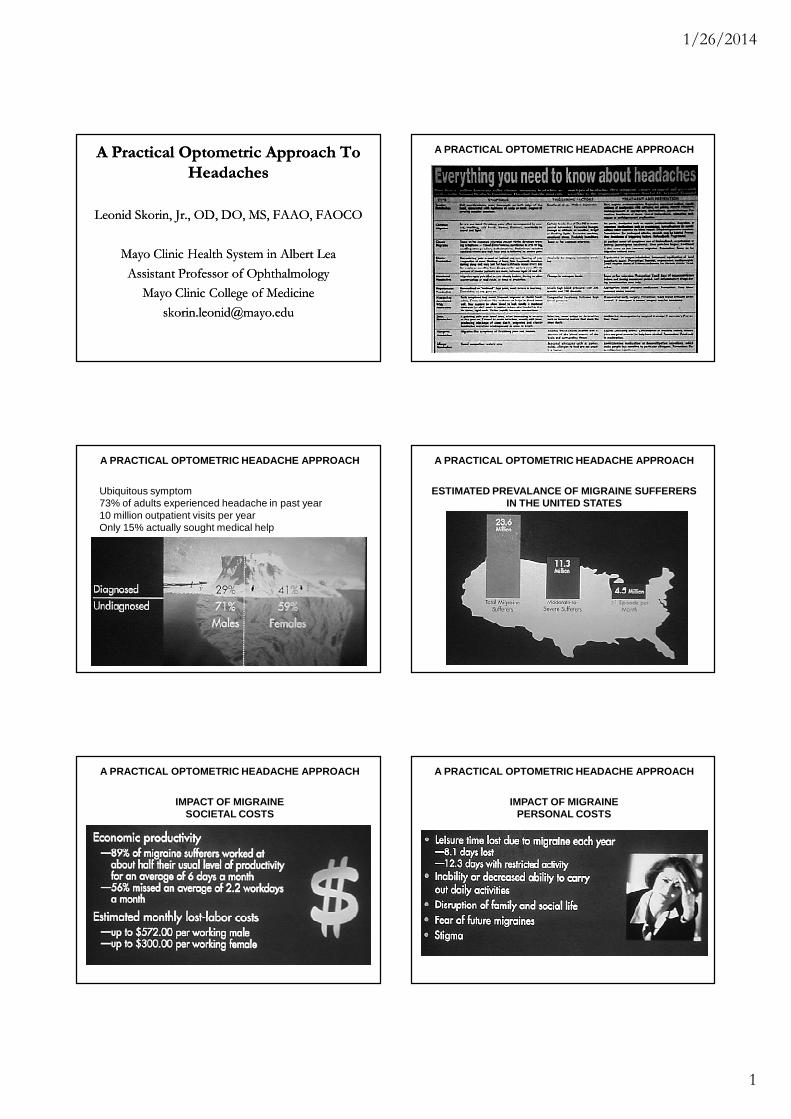
Ubiquitous symptom73% of adults experienced headache in past year10 million outpatient visits per yearOnly 15% actually sought medical help
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
ESTIMATED PREVALANCE OF MIGRAINE SUFFERERS IN THE UNITED STATES
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
IMPACT OF MIGRAINESOCIETAL COSTS
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
IMPACT OF MIGRAINEPERSONAL COSTS

1/26/2014
2
A PRACTICAL OPTOMETRIC HEADACHE APPROACH A PRACTICAL OPTOMETRIC HEADACHE APPROACH
IMPACT OF MIGRAINEHEALTH SURVEY SCORES FOR MIGRAINE AND OTHER CHRONIC
CONDITIONS
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
HEADACHE CLASSIFICATION
International Headache Society criteria1. Primary headache disorders
MigraineTension-typeCluster
2. Secondary headache disordersHeadache is symptomatic of an underlying condition such as temporal arteritis, brain tumor, stroke
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
BASIS OF DIFFERENTIAL HEADACHE DIAGNOSIS
THOROUGH PATIENT INTERVIEW
APPROPRIATE GENERAL EXAMINATION
ADEQUATE NEUROLOGIC EXAMINATION
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
HEADACHE DIAGNOSISP - Provokes, PalliatesQ - QualityR - RegionS - Severity, Associated signs/symptomsT - Timing
1. Onset2. Frequency3. Duration
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
Pathophysiology
Vascular
Neural
Unified or neurovascular
Serotonin (5-HT) neurotransmission

1/26/2014
3
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
POTENTIAL TRIGGERS OF MIGRAINE:
DRUGSHORMONESSENSORY STIMULICARBON MONOXIDEEMOTIONAL STRESSFOODS AND BEVERAGESENVIRONMENTAL CHANGESCHRONOBIOLOGIC CHALLENGES
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE PREVALENCE BY AGE AND SEX
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE CLASSIFICATION
Migraine without aura (common migraine)
Migraine with aura (classic migraine)
Complicated migraine1. Ophthalmoplegic migraine2. Basilar migraine3. Migraine equivalents
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE WITHOUT AURA (COMMON MIGRAINE)
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE WITH AURA (CLASSIC MIGRAINE)
A PRACTICAL OPTOMETRIC HEADACHE APPROACH

1/26/2014
4
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
OPHTHALMOPLEGIC MIGRAINE
ONSET BEFORE AGE 10
3RD, 6TH, OR 4TH NERVEPARESIS
POSITIVE FAMILY HISTORY
PERMANENT WITH REPEATEPISODES
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE EQUIVALENTS
ACEPHALGIC MIGRAINEEPISODIC, TRANSIENT DYSFUNCTION OF AN ORGAN OR SYSTEMNO ACCOMPANYING HEADACHE
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE TREATMENT
Nonpharmacologic1. Eliminate trigger factors2. Stress management3. Biofeedback4. Acupuncture
Physical TechniquesPhysical Techniques
�� Massage, acupressureMassage, acupressure
�� Acupuncture + OTC painkillers: 44% < HAAcupuncture + OTC painkillers: 44% < HA
�� Trigger point injectionsTrigger point injections
�� Muscle stretching exercisesMuscle stretching exercises
�� Osteopathic manipulationOsteopathic manipulation
�� Chiropractic spinal manipulationChiropractic spinal manipulation
Peripheral Nerve StimulationPeripheral Nerve Stimulation
�� Eon Mini IPGEon Mini IPG
�� Stimulation of occipital nerves for intractable chronic Stimulation of occipital nerves for intractable chronic migraine: changes the pain signalmigraine: changes the pain signal
�� 41% reduction in overall disability41% reduction in overall disability
�� 89% of patients would recommend to others89% of patients would recommend to others
�� 27% reduction in number of headache days27% reduction in number of headache days
�� 68% improved quality of life68% improved quality of life
HomeopathicHomeopathic
�� Feverfew Feverfew –– herb, 50herb, 50--100 mg daily, (100 mg daily, (parthenolideparthenolide))
Can cause oral ulcers, tongue irritation, lip swelling.Can cause oral ulcers, tongue irritation, lip swelling.
�� Riboflavin Riboflavin –– Vitamin BVitamin B22 –– 400 mg daily400 mg daily
Increases energy efficiency of mitochondria.Increases energy efficiency of mitochondria.
�� Vitamin B Complex Vitamin B Complex –– BB66 25 mg, B25 mg, B1212 400 mcg, 400 mcg,
folic acid 2 mg: 50% < HAfolic acid 2 mg: 50% < HA
�� Butterbur Butterbur –– herb, 75 mg BID x 4 months: 50% <HAherb, 75 mg BID x 4 months: 50% <HA
Use the brand Use the brand PetadolexPetadolex..
�� Magnesium 600 mg daily: 50% < HAMagnesium 600 mg daily: 50% < HA
Start with 200 mg daily, slowly increase to 600 mg.Start with 200 mg daily, slowly increase to 600 mg.

1/26/2014
5
Botulinum Toxin InjectionBotulinum Toxin Injection
�� Peripheral effect Peripheral effect –– muscle relaxantmuscle relaxant
�� Central effect Central effect –– inhibits release of trigeminal inhibits release of trigeminal
cellcell--mediated neurotransmittersmediated neurotransmitters
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE TREATMENT
Symptomatic (Abortive)
1. Over-the-counter medicationa. Aspirinb. Acetaminophenc. Non-steroidal anti-inflammatory drugs
Motrin Migraine PainAdvil Migraine
d. Combination drugs: Excedrin Migraine
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE TREATMENT
Symptomatic (Abortive)2. Prescription medication
a. Combination drugs with narcoticb. Ergotamine tartratec. Dihydroergotamine: Migranald. Narcotics: Stadol NSe. Midrin
Selective Serotonin Receptor AgonistsSelective Serotonin Receptor Agonists
�� ImitrexImitrex ((sumatriptansumatriptan))
�� ZomigZomig ((zolmitriptanzolmitriptan))
�� AmergeAmerge ((naratriptannaratriptan))
�� MaxaltMaxalt ((rizatriptanrizatriptan))
�� AxertAxert ((almotriptanalmotriptan))
�� FrovaFrova ((frovatriptanfrovatriptan))
�� RelpaxRelpax ((eletriptaneletriptan))
�� TreximetTreximet ((sumatriptansumatriptan/naproxen)/naproxen)
Selective Serotonin Receptor AgonistsSelective Serotonin Receptor Agonists
�� Efficacy: if first triptan does not work, try Efficacy: if first triptan does not work, try
another another –– may require trial and errormay require trial and error
�� Onset: injection Onset: injection –– 1010--15 minutes15 minutes
nasal spray nasal spray –– 15 minutes15 minutes
troche troche –– no faster than oral tabletsno faster than oral tablets
�� Route: nasal spray or injection for N/VRoute: nasal spray or injection for N/V
�� Duration: longest acting Duration: longest acting –– Frova and AmergeFrova and Amerge
A PRACTICAL OPTOMETRIC HEADACHE APPROACH

1/26/2014
6
A PRACTICAL OPTOMETRIC HEADACHE APPROACH
MIGRAINE TREATMENT
Prophylactic (Preventive)a. Beta blockersb. Tricyclic antidepressantsc. Nonsteroidal anti-inflammatory drugsd. Calcium channel blockerse. Monoamine oxidase inhibitors: Nardilf. Anticonvulsants: Depakote, Depakene, Topamax
Topamax 50% < HA by 6 weeks
A PRACTICAL OPTOMETRIC HEADACHE APPROACH