Embed Size (px)
Citation preview
Vol. XVIII No. 1 J O U R N A L OF V A S C U L A R N U R S I N G PAGE 13
A performance improvement initiative: Development of a peripheral vascular pathway Cynthia K. Lewis, RN, MSN
Health care institutions today are being challenged to provide cost-
effective, quality care. High-cost Diagnostic Related Groups are being
targeted for performance improvement initiatives. A Peripheral Vascu-
lar Bypass Chartered Team was formed to review current practices and
identify opportunities for system improvements. Data analysis, the liter-
ature, and best practices were reviewed. Emphasis on the financial, clin-
ical, and quality outcomes are discussed in relation to a clinical path-
way and protocol development in an effort to better manage this
population. (J Vasc Nurs 2000;18:13-21,)
In March 1998 the Quality Council at a Midwestern center chartered a multidisciplinary team to improve the care provided for patients in the Diagnostic Related Group (DRG) 478: patients undergoing peripheral vascular bypass procedures. Identification of best practice (either based on the literature or consensus) was to be used to identify opportunities for standardization and to reduce costs by 25% while maintaining or improving the quality of care as measured by outcomes.
BACKGROUND DRG 478 is a relatively significant volume DRG for the med-
ical center (approximately 350 cases for the first three quarters of 1997). The majority of this DRG involves peripheral vascular procedures. Although length of stay was only slightly longer than expected, costs were exceeding revenues. The Surgical Ser- vices Outcome Facilitation Team had begun an investigation into the causes for this loss. Significant operating room costs were noted. Primarily general/vascular surgeons performed these pro- cedures; however, a small number of these procedures were also performed by cardiovascular surgeons. This patient population typically recovered in an intensive care unit (ICU) and then in a general surgical unit. Because this procedure had a relatively significant volume with a controlled group of practitioners and relatively controlled postoperative placement, the DRG was thought to lend itself well to a performance improvement initia- tive.
f
Project D e f i n i t i o n / / ~ f and Organization • breakthroughs in attitude Diagnostic Journey • organization • problem statement
• chartering team
Holding The Gains • confirm breakthrough G maintain quality
Remedial Journey • develop remedies • breakthroughs in practice
identify solution
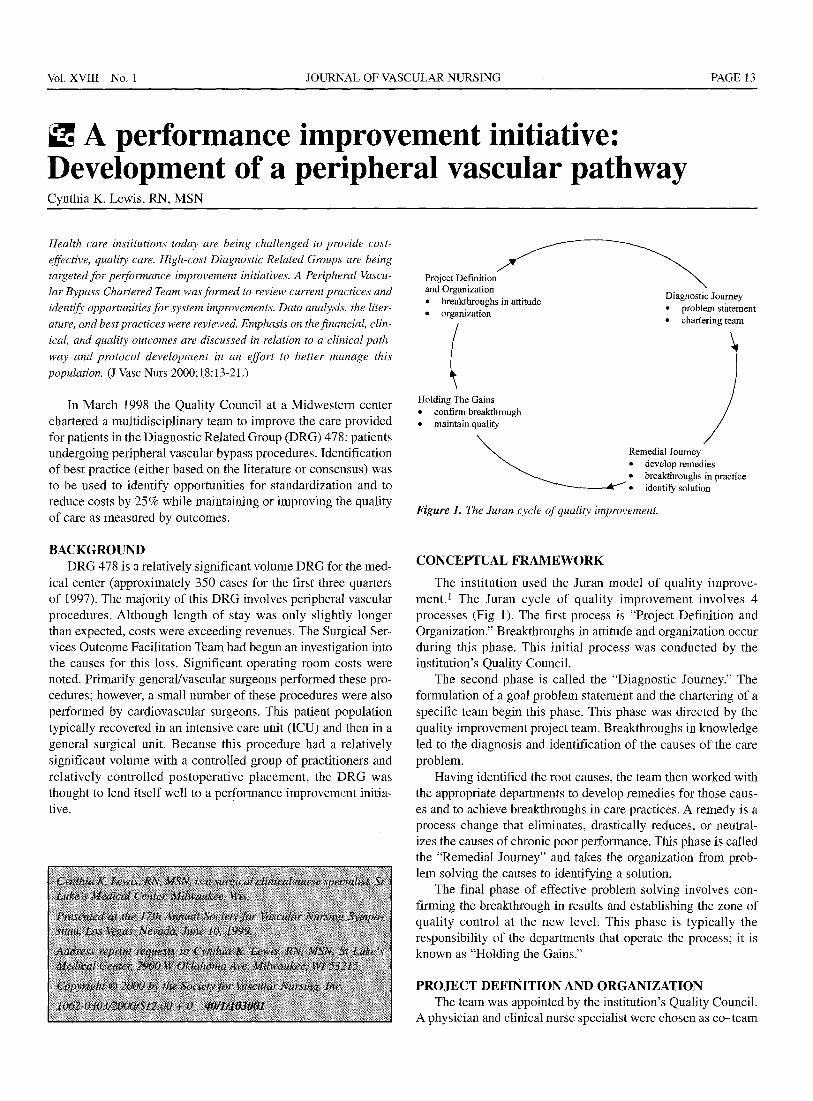
Figure 1. The Juran cycle of quality improvement.
CONCEPTUAL FRAMEWORK
The institution used the Juran model of quality improve- ment.1 The Juran cycle of quality improvement involves 4 processes (Fig 1). The first process is "Project Definition and Organization." Breakthroughs in attitude and organization occur during this phase, This initial process was conducted by the institution's Quality Council.
The second phase is called the "Diagnostic Journey." The formulation of a goal problem statement and the chartering of a specific team begin this phase. This phase was directed by the quality improvement project team. Breakthroughs in knowledge led to the diagnosis and identification of the causes o f the care problem.
Having identified the root causes, the team then worked with the appropriate departments to develop remedies for those caus- es and to achieve breakthroughs in care practices. A remedy is a process change that eliminates, drastically reduces, or neutral- izes the causes of chronic poor performance. This phase is called the "Remedial Journey" and takes the organization from prob- lem solving the causes to identifying a solution.
The final phase of effective problem solving involves con- firming the breakthrough in results and establishing the zone of quality control at the new level. This phase is typically the responsibility of the departments that operate the process; it is known as "Holding the Gains."
PROJECT DEFINITION AND ORGANIZATION The team was appointed by the institution's Quality Council.
A physician and clinical nurse specialist were chosen as co-team

TABLE II. TABLE I.
leaders. All other disciplines involved in the care of the periph- eral vascular bypass patients were identified as members. The multidisciplinary team included representatives from the sur- geons, anesthesiologists, radiologists, social service, physical therapy, pharmacy, home care, wound care, and all involved nursing areas. Nursing representatives from preadmission, same- day surgery, postanesthesia care, operating room, intensive care, and the respective surgical floors were included.
The team was led by the co-team leaders with support from a quality management facilitator. The team met every 2 weeks and was given a 6-month time line for completion of the project. The goal of the first meeting was to bring the team together and to discuss the roles and responsibilities for the team leaders, facilitator, and team members. Ground rules were identified and agreed on by the team.
The measures that the team was charged to consider from the Quality Council involved reviewing the average length of stay, average charges, costs stratified in the operating room, and per- centage of postoperative infections.
DIAGNOSTIC JOURNEY In reviewing the existing data, the team initially focused on
the two major categories included in DRG 478, vascular shunt and bypass, and angioplasty/atherectomy of noncoronary ves- sels, but later narrowed the scope to vascular shunt and bypass (ICD 9-CM code 39.29). Vascular shunt and bypass procedures were correlated with higher costs and a longer length of stay than angioplasty procedures. This step was necessary to determine the category for data retrieval.
Data analysis showed that 80% of the patients admitted under this category were elective admissions. Preadmission data showed that some angiography studies were being done within the 72 hours before admission, which had implications for reim- bursement. If radiologic tests occurred more than 72 hours before surgery, anticipated cost savings ranged from $780 to $2151.
Eighty-one percent of these patients had an ICU stay, of which 65.8% stayed in ICU for 24 hours. APACHE data (which identifies high-risk and low-risk patients requiring an ICU stay) showed that 68% of this population did not meet the ICU crite-
PAGE 14 JOURNAL OF VASCULAR NURSING MARCH 2000
ria. In addition, charge data demonstrated some equivalency in cost between the 24-hour stay in ICU and postanesthesia care unit (PACU)/floor after the operation. However, inconsistencies were identified in charges between two of the ICUs on the assignment of their acuity levels, which ultimately affects charges and cost. These inconsistencies in practice were identi- fied as educational opportunities for both the surgeons and the nursing staff.
The existing length of stay for this population was 9 days. Both physicians and nursing staff noted that often these patients did not require acute nursing care, yet were often not quite "ready" or able to go home. Home care and subacute care were used infrequently. In most circumstances, these patients did not meet the criteria for inpatient rehabilitation. Decreasing the length of stay to 4 to 5 days would account for almost a 25% cost savings. Readmissions within 30 days were less than 1% as a result of postoperative infections and less than 8% as a result of complications from comorbid conditions such as cardiac or res- piratory problems.
Pharmacy cost data were also reviewed. It became evident that an opportunity existed for standardization and dosing proto- cols for preoperative and postoperative antibiotics. Cefazolin was identified as the most cost-effective drug of choice. Before the operation, 1 g is given intravenously 30 minutes before inci- sion. After the operation, 1 g of Cefazolin is given every 8 hours for 24 hours. Vancomycin is used if the patient is allergic to peni- cillin or cephalosporin. Anesthesia charges and use did not reveal new opportunities for improvement. Operating room charges indicated that the greatest variability was the length of the operating time. However, opportunity existed for improving antibiotic dosing for long cases (>3 hours).
REMEDIAL JOURNEY The team then set out to review the existing literature to iden-
tify any other opportunities for improvement and best practice. The literature supported use of an ICU or an intermediate ICU for the first 24 hours after surgery. 2-s Unlike other populations, the peripheral vascular bypass patient is at risk for complications

Vol. XVIII No. 1 JOURNAL OF VASCULAR NURSING PAGE 15
St. Lukcs Medical Center A u r o r a H e a l t h C a r e ~
Milwaukee, Wisconsin
C A S E T Y P E : P E R I P H E R A L V A S C U L A R B Y P A S S
Nursing Diagnoses: Alteration in Tissue Perfusion - Knowledge Deficit
[ D A T E : P H A S E / D A Y : P R E - O P
KEY PATIENT OUTCOMES Date Time Symbol
0.1
0.2 0.3 0.4.
0.5
0.6
A S S E S S M E N T S
Initial NA Pre-admission testing completed >72 hours before surgery (include lab and P-~diologic
(Nurs/MD) OM #1 I ~ k n o w ~ e - - " - ' - ' T - - - i ~ a l ~ , t ~ I Patient verbalizes k n o w l e d ~ e n e r a l information and re aration for s u r e . (Nurs i
Patient verbalizes knowledge of specific information related to peripheral bypass surger ~ r a l Vascular Bypass Packet) (Nurs/MD) Patient/SO verbalizes anticipated discharge plan and assistance available at discharge. (Nurs/MD OM #2 . . . .
] Patient demonstrates exercises and verbalizes knowled e of ost-o them lans. (PT,
Collaborative Data Base completed/Standard of Care. (Nurs) Assess patient readiness for learning and barriers to learning: r l Reading E1 Lack of Family/SO Support [] Emotional [] Cognition [] Physical [] Other [] l.an ua e S ken I.an ua e: [] No barriers Triggers for potential diabetes education post-op. MD order required for consult (Nurs): [] Pt is not performing self blood sugar testing. [] Newly diagnosed diabetic. [] Present diabetic with educational needs or questions.
for Nutrition Services: (Nurs/NS) [] Poor appetite (for >6 days) prior to admission [] unintentional weight loss of more than 10 lbs. in 6 months [] Serum albumin <3.3g/dl Tri~jzers for Social Services: (Nurs/SS) [] Primary caregiver for spouse [] Lives alone and lack of support systems [] Decreased mobility/functioning prior to admission [] Past or current use of home care Triggers for pulmonaQ, rehab. (Nuts) Assess need for referral/resource for smoking cessation information.
121 home [] subacute care r"l home with home care [] inpatient rehab Review rehabilitation options (to include the above) (Nurs)
risk,anesthesi,'~a~thesiacontaeted/Standard of Care. (Nurs) ,y evaluation (PT)
I IIIII II1111 IIIII IIIII IIIII IIIII IIII IIII CASE TYPE: PERIPHERAL VASCULAR BYPASS
Figure 2. Peripheral vascular bypass pathway.
k~- forr~3athwz y ~ 134A8 .doc 10/22/98
© AHC X134~ (l l/gS)
after bypass within a 24-hour period. The institution does not have an intermediate ICU nor an observation unit; thus surgeons use the ICU not only for the technical aspects but also often for the close monitoring provided by the smaller nurse-patient ratio. The team was charged to identify the best place to care for this population after the operation. Risk factors that would predispose a patient to require intensive monitoring were identified through review of our APACHE risk data. Severe coexisting cardiac, cere- brovascular, respiratory, and neurovascular disease place the
patient at high risk for multiple early and late postoperative com- plications. 9-12 The team recommended to the hospital's adminis- trators the development of a step-down unit, which would pro- vide a setting to facilitate a 1:4 nurse-patient ratio. Hospital administration is reviewing and deliberating the concept of a step-down unit within the surgical inpatient unit.
At this point the team identified by consensus the opportuni- ties they wanted to address. These opportunities affected several phases along the continuum of care and are presented in Table I.
PAGE 16 JOURNAL OF VASCULAR NURSING MARCH 2000
St. Luke's Medical Center and St. Lukes's South Shore Patient Recovery Plan for Peripheral Vascular Bypass
AHC X14444 (11/98)
:: .... ~ ~ n A d m l s s l o n : : : I t S n f g e r y i - :Sufge l ;y Surgery
What N u r s ~ v e . Surgical Nursing Unit Unit will I go to? l ~mng in ~e ~ = . = ursurge~ you,will go I
' I Center at St. Luke's [ to the Recovery Room/Surgical [ [ _ Nursing Unit or to?e ICIJ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
What ~/fChest X-ray Frequent ~ ' s by IThe nurse will wash your incision with mild soap and water Tests/Treatments ~ L a b Wor!~, year nurse of your : tLeg up 11~]~on 2 pillows
will I have? ~ E K G *temperature *blood pressure IPhysical Therapy
~ P h y s i c a l * pulse t L e g exercises Therapy Evaluation * breathing
* incision t l V
What equipment/ tubes will I ~ IV Leg up on 2 pillows Ill11| Leg u p ~ l ~ on 2 pillows
have7 Foley catheter removed IV comes out
What will my ~ You will be on Up and waU~g with Up and walking with help O times activity be7 ~ bedrest after your help ~ ) times
• At At What will I eat?
What do I need
NOTHING BY MOUTH THE
NIGHT BEFORE Liquid Diet
SURGERY Progress your diet as tolerated
Review the information in your
Low Cholesterol Diet
I I A s k for pr~ ne j_uiee or laxaave i f no bowel movement
You will he You will be You will be to learn? folder. If you have questions I~!~N
ask your doctor or nurse, taught how to control your
pain,
taught how to care for your legs and • , ' . < Incision
given discharge instructions
How can I help Learn to rate your pain on a Pain medication Pain medication Ask for pain pills i Take a mild pain manage my pain? scale of 1 through 10 ~ will be given through your IV for discomfort reliever prior to
through your IV or by pills ~" ~ :: [ going home
What is my plan *Home [ Review for ~ Discharged to: • N~[I~W Peripheral *home
for discharge? *Home with home care dxscharge ~ V a s c u l a r Bypass 'qlomc/h,me care * Subacute care ~ - ~subacute care
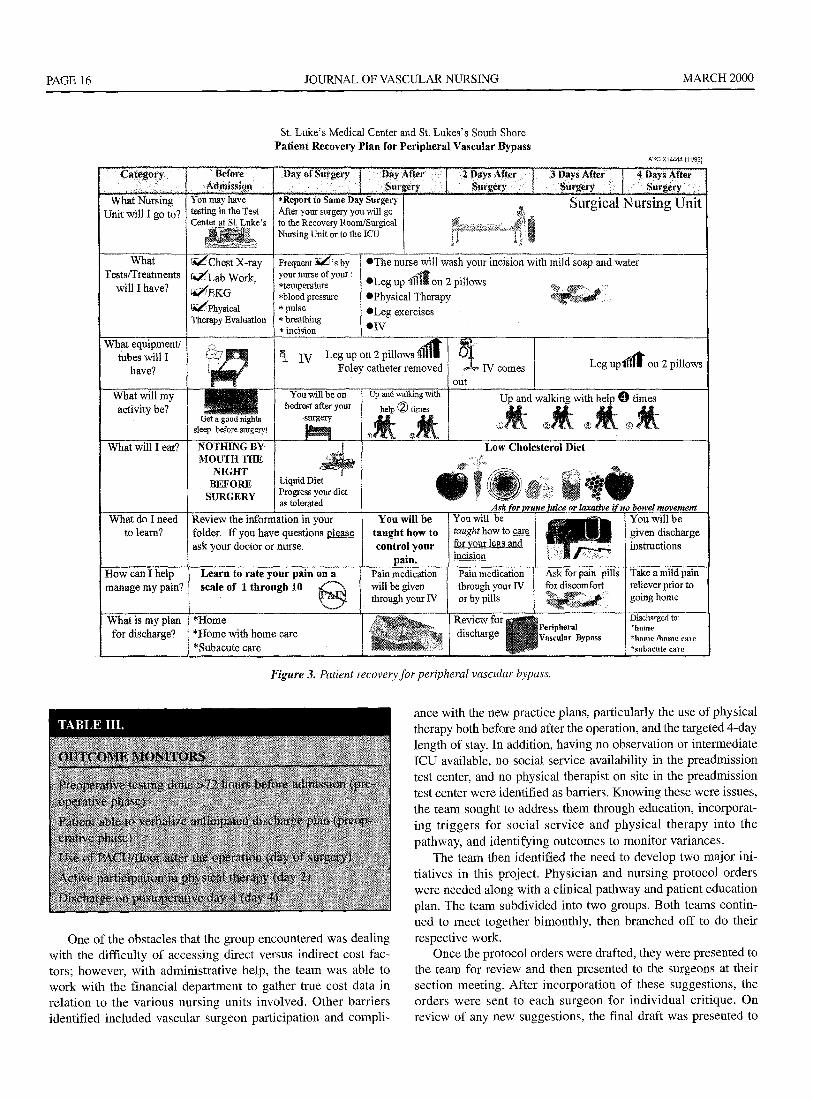
Figure 3. Patient recovery for peripheral vascular bypass.
One of the obstacles that the group encountered was dealing with the difficulty of accessing direct versus indirect cost fac- tors; however, with administrative help, the team was able to work with the financial department to gather true cost data in relat ion to the various nursing units involved. Other barriers identified included vascular surgeon participation and compli-
ance with the new practice plans, particularly the use of physical therapy both before and after the operation, and the targeted 4-day length of stay. In addition, having no observation or intermediate [CU available, no social service availability in the preadmission test center, and no physical therapist on site in the preadmission test center were identified as barriers. Knowing these were issues, the team sought to address them through education, incorporat- ing t r iggers for social service and phys ica l therapy into the pathway, and identifying outcomes to moni tor variances.
The team then identified the need to develop two major ini- tiatives in this project. Physician and nursing protocol orders were needed along with a clinical pathway and patient education plan. The team subdivided into two groups. Both teams contin- ued to meet together bimonthly, then branched off to do their
respective work. Once the protocol orders were drafted, they were presented to
the team for review and then presented to the surgeons at their section meeting. After incorporat ion of these suggestions, the orders were sent to each surgeon for individual critique• On review of any new suggestions, the final draft was presented to

Vol. XVIII No. 1 JOURNAL OF VASCULAR NURSING PAGE 17
St. Luke's Medical Center and St. Lukes's South Shore CARING FOR YOURSELF AT HOME AFTER YOUR LEG SURGERY
AHC X14445 (11/98)
CARING FOR
YOURSELF
TAKING YOUR
MEDICATION
~No smoking
V#Avoid foods high in fat ~Control your blood pressure
¢~Conserve yottr energy ¢r Pace your activities
EATING HEALTHY
FEELING GOOD
• Eat at least 5 servings of fruits and vegetables daily
,Eat slowly ,Eat less fatty foods
•Loose any excess weight
ANXIOUS? • Share your feelings with family members and
¢r Know your limits ~Be ok with it!
Keep your hospital discharge instruction sheet handy. It has phone numbers you may" need,
R e v i e w your Per ipheral Bypass folder often,
P e r i p h e r a l V a s c u l a r
Bypas s
Take your medication as prescribed N
.Drink plenty of fluids
Take short walks daily Rest between activities Avoid prolonged
Eat a balanced d i e t ~',mNOoKING!!!
~Eat a balanced diet
•Take medicine as ordered
• Take care of your legs and feet fl-iends • Use controlled breathing
CARING FOR YOUR
standing Avoid extreme hot & cold tempera tures
Avoid sitting ~ Wash feet daily
FEET with your legs
crossed
CALLING YOUR
DOCTOR
Keep legs up when sitting or laying I
C A L L YOUR DOCTOR IF um'elieved by medication ~ - - ~ - - i increased redness or drainage
TABLE IV.
File toenails straight across
Were" shoes that fit properly a5 Were" clean socks daily
• You have fever above 101 degrees F
Figure 4. Caring for yourself at home after your leg surgery.
the team. Both preoperative and postoperative order sets were developed (Table II). Once finalized, the orders were put into the hospital computer for system retrieval.
The pathway group developed a clinical pathway, variance tool, patient recovery plan, and patient education folder. The clinical pathway identified triggers for discharge planning to ini- tiate the plan before admission (Fig 2). In addition, a patient edu- cation sheet on discharge options was developed in collaboration with social service. The unit social worker would open the case for discharge planning on postoperative day 1. However, the ini- tial discussion was to occur during the preadmission interview by the registered nurse. A physical therapy exercise sheet was also developed in collaboration with physical therapy. The lead- ership of both the preadmission test center and physical therapy were committed to making the initiative a success. The need for physical therapy on site in the preadmission test center was iden- tified not only for this population but also for the other initiatives with the orthopedic population. After deliberation by the leader- ship group, a physical therapist is now available in test center 3 days a week and on call the other 2 days.
In addition to the pathway, patient education materials were compiled into a folder. This folder provided general preoperative information and disease-specific information on peripheral arte- rial disease, diet, and postoperative management of their legs. Two patient recovery plans were also developed. One addressed

PAGE 18 JOURNAL OF VASCULAR NURSING MARCH 2000
the preoperative and postoperative course; the other addressed home care management (Figs 3 and 4).
The team as a whole had chosen 5 major outcomes to monitor with this population: preoperative testing including laboratory and radiologic tests done >72 hours before admission, verbaliza- tion by the patient of the anticipated discharge plan, PACU/floor used after the operation, participation in physical therapy, and discharge on postoperative day 4 (Table III). The pathway was presented to the team for critique. These outcomes were then developed into a scanable variance form.
Next the team identified potential barriers to implementation of the order set and pathway. The use of the protocol orders by the general surgeons and cardiovascular surgeons was a possible compliance barrier. In addition, acceptance by the physicians of physical therapy on postoperative day 1 and acceptance of the planned discharge with home care or to a subacnte facility to support the 4-day length of stay were also identified as major compliance barriers (Table IV). These barriers were addressed by developing an education time line for nursing staff, physi- cians, physical therapy, and social service.
The team set out to develop the education time line for all dis- ciplines involved in the care of the peripheral vascular bypass patient. The protocol order set and pathway needed to be pre- sented in a timely and efficient manner. During a 2-week period, education sessions were held for staff to attend. In addition, team leaders presented the initiatives at the surgeons' section meet- ings. The pathway and order set were set to be initiated on Feb- ruary 4, 1999.
The final meeting of the team was a celebration meeting. This meeting was held a few weeks before the implementation date. The team worked exceedingly hard in reviewing data, identify- ing the opportunities, and implementing the plan of action. In addition, the team members exemplified teamwork in progress. A breakfast celebration was provided along with award recogni- tion by the institution's Quality Council to recognize and demon- strate appreciation for all their efforts.
HOLDING THE GAINS The outcome data are currently sent to the nursing co-team
leader on a monthly basis. The outcomes are graphed and moni- tored to identify both successes and obstacles of the project. Variances are listed for each outcome. Cost, length of stay, and patient demographics are also provided. This data is then shared with each respective nursing area so they can trend and monitor their success and compliance. The data is also shared with the surgeons at their section meetings. Both the surgeons and the nurses "hold the gains" to the success of this improvement project.
To date (January 1999-April 1999), there have been 44 patients on the Peripheral Vascular Bypass Pathway. The average length of stay has decreased from 9.91 days in 1998 to 7 days. Costs have decreased 29% as a result of the decrease in length of stay. ICU use remains high at 90% and accounts for a 1-day stay. The team's goal is to decrease the use of ICU to 60% to 70%.
In relation to the 5 major outcomes, percentages regarding outcomes being met, variances, and documentation rates are
monitored monthly. Several recurrent variances are becoming evident.
Outcome 1: Preadmission testing completed earlier than 72 hours before testing has been met 45% of the time. Variances have occurred (51%), most often as a result of the patient/family not being available.
Outcome 2: Patient/significant other verbalizing the antici- pated discharge plan and assistance available at discharge during the preadmission interview has been met 27% of the time. Vari- ances have occurred (10%), most often as a result of patient/fam- ily indecision regarding discharge planning.
Outcome 3: PACU/floor used for postoperative care has been met 15% of the time. Variances have occurred (40%), most often as a result of physician requests for ICU. The length of stay in the ICU averages 1 day. Before project implementation, the ICU length of stay averaged 1 to 3 days.
Outcome 4: The patient actively participating in physical therapy exercises/ambulation has been met 22% of the time. Variances have occurred (38%) most often as a result of physical therapy not being ordered by the physician and patient factors such as impaired physical mobility, medical instability, fatigue, and pain.
Outcome #5: Being discharged on day 4 has not been met. Variances have occurred (40%), most often as a result of medical instability, physical mobility barriers, and discharge/transfer delay because of physician request or receiving facility delay.
Home care (25%), subacute care (10%), rehabilitation facili- ties (20%), and home/self-care (46%) have been used to facilitate timely discharges. Home care and subacute use have increased 10% since the implementation of the orders and pathway.
Patient satisfaction scores for this population remain consis- tently high, between 90% and 100%. Patient satisfaction data are monitored on a quarterly basis. The data are an institution indicator that is reviewed overall and also according to specific procedures. The Quality Management Department provides this data to the co-team leader.
Nursing compliance with documentation has been identified as an issue with all the inpatient pathways. Currently the docu- mentation rate with the Peripheral Vascular Bypass Pathway is greater than 60%. Although this is a much better compliance rate than with the other pathways, documentation is certainly a nursing accountability, which holds legal ramifications. Unit- specific data is forwarded to the unit clinical nurse specialist for review. Documentation issues and outcome data need to be addressed with the unit nursing staff for corrective actions, which falls within the role accountabilities of the clinical nurse specialist to provide reeducation of the pathway and outcomes monitored.
The Peripheral Vascular Bypass Pathway will now serve as a template for taking this initiative to the other 4 corporate hospi- tals in the surrounding area. The multidisciplinary team approach to identify best care practices and system processes has proved successful with many high-cost DRG procedures. The Peripher- al Vascular Bypass Initiative is demonstrating positive results in relation to financial, quality, and satisfaction outcomes. Outcome

Vol. XVIII No. 1 JOURNAL OF VASCULAR NURSING PAGE 19
management by nursing, physicians, and other disciplines is the key to providing cost-effective, quality care. In the present health care arena, we all will be held accountable for providing the best care possible as measured by positive patient outcomes.
REFERENCES 1. Goonan K. The Juran prescription. Clinical quality man-
agement. San Francisco: Jossey-Bass Publishers Inc; 1995. p. 135-61.
2. Alan S. Perioperative nursing interventions for intravascular stent placements. AORN J 1995;61:689-98.
3. Capasso V, Cote K. The management of patients undergoing arterial reconstructive surgery. Med Surg Nurs 1993 ;2:11-20.
4. Chandra M, Wagner W. ICU care after infra-inguinal arterial surgery: an analysis of indications and outcomes. Am Surg 1995;61:904-8.
5. Gordon P, Sykes M. Determining outcomes of a lower extremity vascular reconstruction program. Semin Periopera- tire Nuts 1997;6:149-61.
6. Jasinkowski N. The unique needs of a distal bypass patient. RN 1982;44-8.
7. Ng RLH, Gilles TE. Iliofemoral versus femorofemoral bypass: a 6-year audit. Br J Surg 1991;79:101l-3.
8. Beattie DK, Golledge J. Quality of life assessment in vascu- lar disease: towards a consensus. Eur J Vasc Endovasc Surg 1997;13:9-13.
9. Bruni K, Hoosier-Paty D. The .quality of life of the limb- threatened patient after lower-extremity revascularization. J Vasc Nurs 1996;14:99-103.
10. Dunlop E Sayers RD. The effect of a surveillance programme on the patency of synthetic infrainguinal bypass grafts. Eur J Vasc Endovasc Surg 1996;11:441-5.
l l .Benson J, Karmody A. In situ artery bypass. AORN J 1987;45:40-55.
12. Kratschmer G, Wenzl E. Vein bypass surgery for femoro- popliteal arteriosclerosis: influence of different risk factors on patient survival and the importance of anticoagulant treat- ment. Eur J Vasc Surg 1988;2:77-81.
CALL FOR MANUSCRIPTS
Journal of Vascular Nursing welcomes manuscripts that provide nurses and other health care professionals with information to foster expert clinical practice in vascular nursing. Please submit manuscripts to Janice D. Nunnelee, PhD, RN, CS/ANR CVN, at the fol- lowing address:
Janice D. Nunnelee, PhD, RN, CS/ANR CVN West County Family Practices
14377 Woodlake #300 Chesterfield, MO 63017
For details about the Journal's editorial policy and manuscript preparation, see the Infor- mation for Authors pages in the front of this issue.





























