Embed Size (px)
Citation preview

A Nonparametric Analysis of the Transmission Rate of Human Immunodeficiency Virus fromMother to InfantAuthor(s): Wei-Yann Tsai, James J. Goedert, John Orazem, Sheldon H. Landesman, AryeRubinstein, Anne Willoughby and Mitchell H. GailSource: Biometrics, Vol. 50, No. 4 (Dec., 1994), pp. 1015-1028Published by: International Biometric SocietyStable URL: http://www.jstor.org/stable/2533440 .
Accessed: 25/06/2014 07:29
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
International Biometric Society is collaborating with JSTOR to digitize, preserve and extend access toBiometrics.
http://www.jstor.org
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

BIOMETRICS 50, 1015-1028 December 1994
A Nonparametric Analysis of the Transmission Rate of Human Immunodeficiency Virus from Mother to Infant
Wei-Yann Tsai,' James J. Goedert,2 John Orazem,3 Sheldon H. Landesman,4 Arye Rubinstein,5 Anne Willoughby,6 and Mitchell H. Gail2
'Division of Biostatistics, Columbia University, New York, New York 10032, U.S.A. 2Epidemiology and Biostatistics Program, National Cancer Institute,
Rockville, Maryland 20852, U.S.A. 3Department of Epidemiology and Biostatistics,
Memorial Sloan-Kettering Cancer Center, New York, New York 10021, U.S.A. 4State University of New York, Health Sciences Center at Brooklyn,
Brooklyn, New York 11203, U.S.A. 5Albert Einstein College of Medicine, Bronx, New York 10461, U.S.A.
6National Institute of Child Health and Human Development, Rockville, Maryland 20852, U.S.A.
SUMMARY
Infants born to mothers who are infected with the human immunodeficiency virus (HIV) may or may not become infected by perinatal transmission. Unfortunately, passively transferred maternal anti- bodies make it hard to determine the infant's infection status from HIV antibody testing, because shortly after birth it is not possible to distinguish passively transferred maternal antibodies from antibodies produced by an infected infant. Usually, the infection status is unobservable for each infant, unless the infant reaches the age of 15 months or develops an HIV-related disease such as the acquired immunodeficiency syndrome (AIDS). Traditionally, statistical analyses of the perinatal transmission rate of HIV are based on infants who had been born at least 15 months before the date of analysis. Such analyses can be both inefficient and biased. In this note, we define a mixture model underlying the onset time of AIDS and then obtain the nonparametric maximum likelihood estima- tors of the HIV transmission rate and of the distribution function of AIDS onset time for infected infants. Nonparametric tests are also derived for detecting differences in HIV transmission rates among different groups of infants. Finally, the methods are applied to the Mothers and Infants Cohort Study in New York City. The transmission rate of HIV from infected mothers to their infants was estimated to be 30.0% with 95% confidence interval (22.3%, 39.1%).
1. Introduction Not every child born to an HIV-infected mother will be infected, and an important aim of AIDS epidemiology is to determine the probability of perinatal HIV transmission and factors that influence the chance of transmission. Estimates of the transmission rate of HIV from infected mother to her infant range from 6% to 50% with wide confidence intervals (see Boylan and Stein, unpublished technical report, School of Public Health, Columbia University, 1990). Some of this uncertainty may be due to the use of methods of analysis that fail to take censoring and special data structure into account.
The population of children born to infected mothers is a mixture of infected and uninfected infants, and distinguishing them can be difficult. Direct measures of infection, like viral culture and the polymerase chain reaction (PCR) for HIV proviral sequences, are not routinely available and are of uncertain reliability. Moreover, the conventional HIV antibody test is not diagnostic of infection in the young infant, because a positive test may result from the passive transfer of maternal antibodies. Because maternal antibodies are eliminated over time, however, it is possible to define as uninfected those infants who remain clinically well and become consistently negative on the HIV
Key words: AIDS; HIV; Mixture model; Nonparametric analysis; Perinatal HIV transmission rate.
1015
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1016 Biometrics, December 1994
antibody test. Blanche et al. (1989) define an infant as uninfected if he or she remains free of clinical evidence of HIV infection and is antibody negative at 18 months of age. An infant is regarded as infected if either "clinical evidence of HIV infection" develops at or before 18 months or if antibody is present at 18 months. We discuss differing definitions of "clinical evidence of infection" in Section 5. Infants who are free of clinical evidence of HIV infection when censored to follow-up before 18 months of age have an indeterminate HIV status, regardless of whether they were antibody positive or negative when censored. Such censorship can occur because the child was born within 18 months of the end of follow-up ("administrative censoring"), because the investigators decide to end follow-up, the family migrates, or the family refuses to continue in follow-up ("refusal censoring"), or because the child dies of an illness not believed to be related to HIV disease. In this paper, we adopt the same definition for HIV infection as Blanche et al. (1989), except that we use 15 months in place of 18 months as the time when a definitive assessment of infection status is made.
Goedert et al. (1989) and the European Collaborative Study (1991) regarded an infant who was censored before 18 months (15 months in Goedert et al.) as uninfected if antibody to HIV was absent at the time of censorship. Some infants of this type might subsequently revert to antibody positive status at 18 months (or 15 months), either because of technical failures in the testing procedure or because maternal antibodies may have disappeared before the infected infant began to produce antibody. Treating such infants as uninfected will produce a lower estimate of the HIV transmission rate than treating them as indeterminate, as we and Blanche et al. do.
In this paper we shall analyze updated data from the Mothers and Infants Cohort Study (Goedert et al., 1989). As of April 1, 1991, the end of follow-up, 127 infants were free of clinical evidence of HIV infection when censored before 15 months of follow-up, 19 had developed clinical disease and had been born at least 15 months before April 1, 1991, 7 had developed clinical disease and were born fewer than 15 months before April 1, 1991, 15 were HIV antibody positive when studied at or after 15 months, and 65 were antibody negative when studied at or after 15 months. A simple estimator of the transmission rate, used by Blanche et al. (1989), confines the analysis to those children born at least 15 months before the end of follow-up (Blanche et al. used 18 months). The estimate of the probability of transmission, p, is the ratio of the number of such infants who were infected to the number who were infected plus the number who were uninfected and evaluated at or after 15 months. In this example, this estimate is (19 + 15)/(19 + 15 + 65) = .343.
Even though the simple estimate above is based on infants born at least 15 months before April 1, 1991, it is biased unless the probability of infection among those infants who were censored by death or refusal is the same as the probability of infection among all newborn infants, regardless of when censoring occurs. This condition is unlikely to be true because children who are censored without clinical evidence of HIV infection just before 15 months of age are less likely to be infected than newborns. The amount of this bias will be small if the amount of such censoring is small.
In this paper we propose an estimate of the probability of transmission, that takes into account infants who are administratively censored as well as those censored by refusal and death. In the previous example, the estimator of Blanche et al. (1989) makes no use of the 127 + 7 = 134 infants born within 15 months of April 1, 1991. The estimator we present uses these data. Like the estimator of Blanche et al., the estimator we propose is biased if the chance of censorship depends on infection status. Unbiasedness of the estimator we present also requires that the time to censorship be independent of the time to onset of clinical evidence of disease. These assumptions are discussed further in Sections 2 and 5.
In this note we give nonparametric estimators of p and of the survival distribution of the onset times of clinical evidence of HIV infection among infected infants, S(t). We also provide a simple test of the null hypothesis that the transmission ratesp1 andpo are the same in two groups of infants. In Section 2 we introduce notation and describe nonparametric maximum likelihood estimators ofp and S(t) together with confidence interval procedures based on asymptotic theory. A simple statistic P1 - Po is developed to test, = po for the two-sample problem. In Section 3, results of a simulation are presented to demonstrate that the confidence interval procedure for p has good coverage for samples of modest size and that the statistic b1 - p0 has good power. Data from the Mothers and Infants Cohort Study are analyzed using the methods developed in this note (Section 4), and critical assumptions and alternative methods of analysis are discussed in Section 5.
2. Notation, Assumption, and Estimators Let D indicate the infant's HIV infection status, where D = 1 if the infant is infected, and D = 0 if not. Let the random variable X denote the age at which clinical evidence of HIV occurs. If D = 0, we set X = mo. Therefore, p = Pr(D = 1) is the transmission rate of HIV from infected mothers to their infants, and S(t) = Pr(X > tID = 1) is the survival distribution of incubation periods to onset
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

An Analysis of Perinatal Transmission Rate of HIV 1017
of clinical evidence of HIV disease among infected infants. The major goals are to estimate the HIV transmission rate p and incubation survival distribution S(t).
If the HIV infection status is observable for each infant in a sample population, then the task of estimatingp and S(t) is straightforward. The usual methods of estimating a binomial probability can be used for the parameters. S(t) can be estimated by the product-limit (PL) estimator (Kaplan and Meier, 1958) applied to the subsample of infants who are infected. However, as mentioned in Section 1, the HIV infection status is unknown for the infants who are under 15 months old and have not developed clinical evidence of HIV infection. This inability to determine the infection status is not overcome by continuously following the infants under study until they reach the age of 15 months because some infants will be censored by "refusal" or by death unrelated to HIV infection as mentioned in Section 1.
For t < 15, the observable data are governed by the marginal survival distribution S*(t) = Pr(D = 1 or 0, X > t), which satisfies the mixture model
S*(t) =pS(t) + q, for 0 < t < 15,
where q = 1 - p. However, for t > 15, the infection status is assumed to be completely known, and the observable data for the onset times of AIDS are governed by the conditional survival distribution S(t)/S(15), which can be consistently estimated by applying the conventional PL estimator to the subsample of infants who are infected and did not develop AIDS by 15 months of age. Therefore we divide our statistical discussion concerningp and S(t) to consider separately the periods t < 15 and t > 15.
We assume that a censoring time, C, is independent of both (i) HIV infection status and (ii) the incubation period, X, among infected infants. These assumptions will be plausible if most censoring is "administrative." Some protocols require continued clinical follow-up through 15 months and a final HIV antibody test at 15 months, regardless of clinical status and HIV antibody status before 15 months of age. These protocols may also require that several attempts be made to contact the family by letter, phone, and home visits before designating the infant as lost, regardless of clinical status and antibody status when last seen. These procedures will tend to minimize the dependence of "refusal" censoring on HIV infection status and on X. In studies that do not take these precautions, censoring may depend on HIV infection status and X. For example, children with worsening HIV disease may require more medical attention and thus have a reduced chance of censorship. Also, if investigators stop following patients closely as soon as HIV antibody disappears, the chance of censoring is increased. Both these phenomena can cause censorship to be more likely in uninfected than infected infants. Deaths from causes thought to be unrelated to HIV disease are uncommon, but such deaths may induce the opposite type of dependence between C and infection status or X. Infants with HIV infection may be debilitated and therefore die sooner from illness thought to be unrelated to HIV. This phenomenon tends to make censorship more likely in infected than in uninfected infants. The impact of deviations from the independence assumptions is considered further in Section 5.
We denote the survival distribution of C by SC. The observed data from perinatal transmission studies are represented as N independent random vectors (Ti, 5i, D*), i = 1,..., N, where Ti = min(Xi, CQ) is the follow-up time for infant i, 5i = I(Xi = Ti) is the uncensored indicator, and D* is the infection indicator defined previously except that D* = -1 if infection status is indeterminate. Throughout, the function I(A) denotes the indicator function for the set A. Note that D* = -1 if and only if 5i = 0 and Ti < 15. Finally, let t1, ..., tK denote the ordered distinct follow-up times (censored or uncensored) among T1, .. ., TN. The goal, then, is to estimate the quantitiesp and S based on a random sample (Ti, 5i, D*), i = 1, ...,N.
First, Kaplan and Meier (1958) showed that the PL estimator 3* of S*, given by
3*(t)= I1[1 _d(ti) (1
is the nonparametric maximum likelihood estimator (NMLE) of S*(t) for t < 15, where d(t) = Yl(T = t, 5i = 1) is the number of infants observed to have AIDS at age t, and n*(t) = 2II(Ti > t) counts the number of infants at risk at time t-. Throughout, the sums without limits are over all observations. Similarly, the PL estimator Sc of the censoring survival distribution Sc, given by
S((t) = f - _____
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1018 Biometrics, December 1994
is the NMLE of Sc, where c(t) = X I(Ti = t, 5i = 0) is the number of censored infants at age t. Define the conditional survival distribution S15(t) = Pr(X > tX > 15, D = 1). The log-likelihood
of the observed data can be written as
t(q, S*, S15) = f1(q, S*) + 2(S15) + constant, (2)
where
l(q, S*) = > {I(D*= 1, Ti > 15) log[S*(15+) - q]
+ I(D*= 0, Ti > 15) log(q) - I(Ti > 15) log S*(15+)
+ I(8i = 1, Ti < 15) log[S*(TT-) - S*(Ti )]
+ I(8i = 0, Ti S 15) log S*(Ti)},
E2(S15) = > {I(D*= 1, 5i = 0, Ti > 15) log S15(Ti)
+ I(Di*= 1, 5i = 1, Ti > 15) log[S15(T7) -S15(Ti )]},
and S*(15+) is defined to bepS(15+) + q. For any well-defined function F(t), F(t+) denotes the limit of function F at t from the right and F(t-) denotes the limit from the left. Under the random censoring assumptions, q = Pr(D* = 0)/SJ(15). Therefore, it is natural to estimate q and S(t) by
nu q NS J15)' (3)
and
3(t) = g g
,for t, 15, (4)
where nu = Y2I(D* = 0). It is proved in the Appendix that q and S* maximize the log-likelihood el (q, S*) defined in (2). Let S15(t) be the PL estimator of S15 obtained from the subsample of infants who are infected and who did not develop AIDS by 15 months of age. This estimator is defined by
S15(t)= H E d(ti)] 15<ti--t
n t)
where n(t) = XJ(Ti ? t, D* = 1) is the number of infected infants at risk just prior to t. It is clear that S15 maximizes the log-likelihood E2(S15). Therefore, for t > 15, we may use S(t) = S(15)&15(t) to estimate S(t). Hence, p = 1 - q and S(t), for t ? 0, are also NMLEs.
As is true for the product-limit estimator (Efron, 1967), the estimators p and S are also "self- consistent." In particular, we prove in the Appendix that
n(0) P N'
and
F d(tk)] S*(t) - t 5
nkHi h(tk)J 1(
3(t) = Htk615 - n(tk)] 15 [ -(tk)] t>15,
where
n(t) = > {I(Di= 1) + I(Di= -1)pS(t)/IpS(t) + q]} (6)
is an estimate of the number of infected infants at risk just before time t. If n(t) were known, then the natural estimators of p and S would be given in equation (5). On the other hand, if p and S were known, then the natural estimator of n(t) would be given by equation (6). In this sense equations (5) and (6) are self-consistent.
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

An Analysis of Perinatal Transmission Rate of HIV 1019
If the censoring time and onset time of AIDS are independent and S,(15) > 0, then, by standard methods [see, for example, Breslow and Crowley (1974)] for t < 15, N/N (q - q, 3(t) - S(t)) converges weakly to a Gaussian process W = (W1, W2(t)) with mean zero and covariance structure given by
var(W1) = (S(15) - q)q - q f Sr7(X) dFsc(x)
cov(W2(s), W2(t)) =A(s, t) + S*(s)S*(t)(1 - q)f4 var(Wl) + B(s) + B(t),
cov(Wl, W2(t)) = B(t) + S*(t)(1 - q)-2 var(W1),
where
F,,(t) = Pr(Tj S t, 5i = 0) and FsU(t) = Pr(Tj < t, 5i = 1)
are subdistributions, and where
Sr(t) = Pr(Ti > t),
r min(s,t) A(s, t) = S*(s)S*(t)(1 - q)-2 J Sr2(x) dFsu(x)
B(t) - S*(t)2(lqf3q Sr2(x) dFs.(x).
We sketch the proof in the Appendix. These covariances can be estimated by replacing the unknown parameters and functions by their estimators. For example,
= &2(') N'{ ( 615) q-= q - [SO(x-)SO(x+)]-l dFc(x)}
is a consistent estimator of var(W1)/N, the asymptotic variance of q, where S'(t) = XJ(Tj ? t)/N and Ps--jt) = Y2I(Ti S t, 5i = O)/N are sample estimates of Sr and FsC, respectively. The second term of the asymptotic variance of q is a product of (q/Sc(15))2 and the asymptotic variance of Sc(15), which is provided by many statistical packages for survival analysis.
In many applications, we are also interested in comparing the HIV transmission rates between two subgroups. Based on the one-sample results, the statistic
T- Pi -Po &2(ij5) + &2(po)
can be used to test the null hypothesis Ho: Po = Pi, wherepi is the NMLE of the transmission rate of the ith group, i = 0, 1. Asymptotic normality of q implies that T will converge weakly to a standard normal distribution.
One may try to increase the power of the test Ho: Po = Pi by assuming SO(t) = S1(t), for t S 15, where Si is the survival distribution of AIDS onset time for infants in the ith group, i = 0, 1. Gray and Tsiatis (1989) called this the "proportional distribution assumption." This assumption may yield more powerful tests than the statistic T, because it leads to slightly better estimators of po and Pi. Following the approach of Gray and Tsiatis, we obtain a statistic U = U1 + U2, where U1 = ItiX15 w(ty)[d1(ti) - E(ti)] is a weighted log-rank statistic, U2 = nl+ - E1+ is a Mantel-Haenszel statistic for the fourfold table categorizing AIDS-free infants alive at 15 months as to infection status and group, w(t) = q/S*(t-) is a weight function, 1 - q and S* are, respectively, the NMLEs of transmission rate 1 - q and S* from the pooled sample, dj(ti) is the number of infants from the jth subgroup developing AIDS at time ti, E(t) = [do(t) + d1(t)]n*(t)/ [n*(t) + n*(t)] is the expected number of infants from the first subgroup developing AIDS at time t, n3(t) is the number of infants at risk just prior to t on subgroup], n1+ = Si from jth subgroup I(D1 = 1, T1 > 15) is the number of infected infants from the first subgroup who are free of AIDS at age 15 months, and F1 + = (n1? + n0?)n~l(15+)/ [n~l(15+) + n*O(15+)] is the expected number of infected infants from the first subgroup who are free of AIDS at age 15 months. Gray and Tsiatis (1989) obtain the statistic U1 under the condition that all data are censored at the end of 15 months. They also proved that the test
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1020 Biometrics, December 1994
U1 is optimal under the proportional distributions alternative, which is identical to the alternative hypothesisp1 - po = 0 X 0 in our notation. We expect that the test U is also optimal under the same alternative for the data collected in HIV perinatal transmission studies. However, simulations in Section 3 indicate that the statistic T is nearly as efficient as the statistic U in our setting, and T has the advantages that it is simple to compute and is free of the additional "proportional distribution" assumption.
3. Simulation Results We conducted a simulation study (Tables 1 and 2) to investigate the power of the statistic T, to compare that power with the power of the more elaborate statistic U, and to check whether the asymptotic theory in Section 2 holds in small samples. The simulated conditional distribution of onset of AIDS for infected infants was exponential with median 766 days. The censoring distribu- tions were exponential with medians 900 or 450 days. In all cases the sample size was 50 or 100 in each group. The values given in Table 1 are the percentages of 1,000 simulated samples for which the estimated 95% confidence interval contains the true transmission rate. The values given in Table 2a are the percentages of 1,000 simulated samples for which the test statistic T2 or U2 exceeded the 95th percentile of a chi-square distribution with 1 degree of freedom. The values given in Table 2b
Table 1 Estimated coverage probability (x 100) for nominal 95% confidence interval based on 1,000
simulations
Sample Infected proportion size Censoringa Methodb .2 .3 .4 .5 .6 .7 50 low P 92.5 93.8 94.0 92.6 93.9 93.3 50 low LO 96.0 96.2 95.6 94.6 95.8 96.2 50 high P 91.1 92.2 93.4 92.5 91.9 90.8 50 high LO 95.7 95.4 96.0 95.2 95.4 96.0
100 low P 93.0 94.2 94.4 93.5 95.4 94.0 100 low LO 94.9 95.4 95.0 94.7 96.4 95.4 100 high P 93.3 93.6 94.2 94.0 93.6 93.8 100 high LO 95.7 95.4 95.4 95.3 95.2 96.4
a Low and high censoring indicates exponential censoring with medians of 900 days and 450 days, respec- tively.
b p is the confidence interval based on the proportion estimate; LO is that based on the log-odds estimate:
log(p/4) + 1.96&/(pq).
Table 2a Simulated size (x 100) for nominal 5 % two-sided tests
Sample Infected proportions size Censoringa Testb (.2, .2) (.3, .3) (.4, .4) 50 low U 3.9 3.5 5.0 50 low T 4.6 3.9 5.8 50 low LO 3.4 2.7 4.8 50 high U 5.3 4.8 3.6 50 high T 5.7 6.4 5.2 50 high LO 3.8 4.3 4.3 100 low U 5.8 5.7 5.1 100 low T 6.3 6.1 5.6 100 low LO 5.9 5.6 5.2 100 high U 4.8 5.3 5.8 100 high T 5.7 5.2 6.9 100 high LO 4.5 4.8 6.0
a Low and high censoring indicates exponential censoring with medians of 900 days and 450 days, respec- tively.
b U is the modified Gray and Tsiatis test, T is based on the difference in proportionsp1 - p30, and LO is based on the difference in log-odds, log(p1/q1) - log(pO/q0).
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

An Analysis of Perinatal Transmission Rate of HIV 1021
Table 2b Simulated power (x 100) for 5% two-sided tests
Sample Infected proportions size Censoringa Testb (.20, .33) (.20, .50) (.30, .46) (.30, .63) (.40, .57) (.40, .73) 50 low U 32.9 79.6 36.4 87.5 29.2 83.0 50 low T 31.7 78.1 35.1 86.6 30.2 82.2 50 low LO 32.7 79.9 34.9 86.5 29.9 82.0 50 high U 18.6 62.2 24.7 69.5 26.6 69.6 50 high T 20.8 63.7 23.7 68.2 26.3 67.9 50 high LO 22.4 66.9 23.7 68.3 26.2 67.6
100 low U 43.6 96.9 49.0 98.0 53.5 97.6 100 low T 44.4 96.5 49.4 98.4 52.0 97.4 100 low LO 44.3 96.6 49.8 98.4 52.3 97.4 100 high U 38.6 93.3 41.8 94.5 40.5 92.8 100 high T 37.4 91.5 41.9 94.1 37.7 91.8 100 high LO 37.6 91.7 42.7 94.3 37.9 91.7
a Low and high censoring indicates exponential censoring with medians of 900 days and 450 days, respectively. b U is the modified Gray and Tsiatis test, T is based on the difference in proportions, and LO is based on the
difference in the log-odds of infection.
are the percentages of 1,000 simulated samples for which the test statistics exceeded the corre- sponding 95th percentile of the simulated distributions generated in Table 2a.
For sample size n = 50, the 95% confidence intervals for p ( b ? 1.96&(p)) have coverage probability less than nominal (Table 1). However, confidence intervals based on inverting the confidence intervals of log odds [log(p/4) ? &(p)/ (n q)] have the correct coverage, even for a sample size of 50. This suggests that confidence intervals based on the log odds will have near nominal coverage in samples of modest size.
The size of T is near nominal levels (Table 2a), but tends to exceed the size of U. To make appropriate power comparisons, we used empirically estimated 95th sample percentiles from the null simulations as critical values. Even after this adjustment, the statistic U shows no appreciable power advantage over the power of T or of a test based on the difference in log odds (Table 2b).
4. Example The updated data from the Mothers and Infants Cohort Study (Goedert et al., 1989) describe 233 infants born and in follow-up before April 1, 1991. Of these, 26 developed clinical evidence of HIV infection before 15 months of follow-up, and 15 were found to be infected after 15 months (Table 3).
Table 3 Summary of infection status data
Censored without clinical evidence of HIV infection Clinical evidence of HIV Free of clinical evidence of before 15 full months of infection within 15 full HIV infection at the end of
follow-up months of follow-up 15 full months of follow-up 127 19 born at least 15 15 infected
months before the date of analysis
20 premature 3 premature 4 premature 73 full term 12 full term 11 full term 34 unknown a 4 unknowna 0 unknowna
7 born fewer than 15 65 uninfected months before the date of analysis
1 premature 13 premature 6 full term 45 full term 0 unknowna 7 unknowna
Totals 127 26 80
a Unknown gestational status.
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

Table 4 Data on the onset of clinical evidence of HIV infection from the Mothers and Infants Cohort Study
Onset Onset indicator indicator
Follow-up for clinical Follow-up for clinical time evidence of Infection Premature time evidence of Infection Premature (days) infection statusa statusb (days) infection statusa status
3.0 0 -1 0 164.0 0 -1 -1 5.0 0 -1 0 165.0 1 1 1 6.0 0 -1 -1 166.0 0 -1 -1 7.0 0 -1 0 168.0 1 1 0
15.0 0 -1 0 172.0 0 -1 -1 17.0 0 -1 0 181.0 1 1 1 20.0 0 -1 -1 181.1 0 -1 1 21.0 0 -1 - 1 182.0 1 1 0 21.0 0 -1 1 184.0 1 1 0 22.0 0 - 1 0 186.0 1 1 0 29.0 0 - 1 - 1 188.0 1 1 0 29.0 0 -1 -1 188.1 0 -1 0 34.0 1 1 1 189.0 1 1 0 35.0 0 -1 0 191.0 0 -1 0 35.0 0 -1 0 195.0 0 -1 1 38.0 0 -1 1 196.0 0 -1 -1 47.0 0 -1 0 200.0 0 -1 0 52.0 0 -1 0 206.0 0 -1 0 55.0 0 -1 -1 207.0 0 -1 1 58.0 0 -1 -1 207.0 0 -1 1 61.0 0 -1 0 213.0 0 - 1 0 67.0 1 1 0 226.0 0 -1 -1 68.0 0 -1 0 235.0 0 -1 -1 74.0 0 -1 0 237.0 0 -1 0 78.0 1 1 1 244.0 0 - 1 0 79.0 0 -1 -1 247.0 0 -1 -1 79.0 0 -1 0 253.0 0 - 1 0 80.0 0 -1 -1 254.0 0 -1 0 81.0 0 -1 0 256.0 0 - 1 -1 84.0 0 -1 0 257.0 0 -1 -1 86.0 1 1 -1 257.0 0 -1 0 91.0 1 1 0 257.0 0 - 1 0 95.0 0 -1 -1 261.0 0 -1 1 96.0 0 -1 -1 274.0 0 -1 -1 97.0 0 -1 0 280.0 0 -1 0
101.0 0 -1 -1 280.0 0 -1 0 109.0 1 1 0 282.0 0 - 1 1 115.0 1 1 0 285.0 0 -1 0 115.1 0 -1 0 288.0 0 -1 -1 115.1 0 -1 0 289.0 0 -1 -1 115.1 0 -1 0 295.0 0 -1 0 117.0 1 1 0 302.0 1 1 0 117.1 0 -1 0 305.0 0 -1 0 118.0 1 1 0 315.0 0 -1 -1 119.0 1 1 0 318.0 0 -1 0 126.0 1 1 1 332.0 1 1 0 128.0 1 1 - 1 343.0 0 - 1 1 128.1 0 -1 -1 343.0 0 -1 0 128.1 0 -1 0 364.0 0 -1 -1 132.0 1 1 - 1 364.0 0 - 1 1 133.0 0 -1 0 366.0 0 -1 0 143.0 0 -1 0 366.0 0 - 1 0 148.0 1 1 0 367.0 0 - 1 0 150.0 1 1 0 369.0 0 - 1 0 152.0 0 -1 0 370.0 0 -1 -1 152.0 0 - 1 0 372.0 0 - 1 0 161.0 0 - 1 - 1 379.0 0 - 1 0 161.0 0 - 1 - 1 388.0 0 - 1 0 164.0 0 - 1 - 1 396.0 0 - 1 0
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

Table 4 Continued
Onset indicator Onset indicator
for clinical for clinical Follow-up evidence of Infection Premature Follow-up evidence of Infection Premature time (days) infection statusa statusb time (days) infection statusa status
401.0 0 -1 1 402.0 0 -1 1 850.0 0 0 0 414.0 1 1 0 853.0 0 0 -1 427.0 0 -1 0 856.0 0 1 0 434.0 0 -1 0 896.0 0 0 1 440.0 0 -1 0 914.0 0 0 -1 442.0 0 -1 0 923.0 0 0 1 455.0+ 0 -1 1 923.0 0 0 1 455.0+ 0 -1 0 925.0 0 0 0 455.0+ 0 -1 0 929.0 0 0 -1 455.0+ 0 -1 -1 942.0 0 0 0 455.0+ 0 -1 0 957.0 0 0 0 455.0+ 0 -1 -1 964.0 0 0 0 455.0+ 0 -1 1 987.0 0 0 0 455.0+ 0 -1 0 998.0 0 0 0 455.0+ 0 -1 0 1,006.0 0 0 0 455.0+ 0 -1 1 1,014.0 0 1 0 455.0+ 0 -1 1 1,020.0 0 0 0 455.0+ 0 -1 0 1,031.0 0 0 0 455.0+ 0 -1 -1 1,033.0 0 0 0 455.0+ 0 -1 1 1,070.0 0 0 0 455.0+ 0 -1 0 1,075.0 0 0 1 455.0+ 0 -1 0 1,085.0 0 1 0 455.0+ 0 -1 0 1,095.0 0 0 0 455.0+ 0 -1 0 1,100.0 0 0 1 455.0+ 0 -1 0 1,105.0 0 0 0 455.0+ 0 -1 -1 1,166.0 0 0 0 455.0+ 0 -1 1 1,215.0 0 0 1 455.0+ 0 -1 0 1,222.0 0 1 0 455.0+ 0 -1 1 1,259.0 0 1 0 455.0+ 0 -1 0 1,276.0 0 0 -1 455.0+ 0 -1 0 1,283.0 0 1 1 455.0+ 0 -1 0 1,294.0 0 0 1 455.0+ 0 -1 0 1,295.0 0 0 0 455.0+ 0 -1 0 1,324.0 0 0 0 471.0 1 1 1 1,328.0 0 1 0 503.0 0 0 0 1,336.0 0 0 0 514.0 0 0 0 1,346.0 0 0 0 547.0 1 1 0 1,360.0 0 0 0 552.0 0 0 0 1,415.0 0 0 0 590.0 0 0 1 1,433.0 0 1 1 618.0 0 0 0 1,446.0 0 0 0 632.0 0 0 -1 1,468.0 1 1 1 634.0 0 0 0 1,516.0 0 1 0 644.0 0 0 1 1,571.0 0 0 0 649.0 0 0 0 1,585.0 0 0 0 655.0 0 0 1 1,590.0 0 0 0 697.0 0 0 -1 1,599.0 0 1 0 701.0 0 0 0 1,648.0 0 0 0 712.0 0 0 0 1,687.0 0 0 0 739.0 0 0 0 1,692.0 0 0 0 755.0 1 1 0 1,707.0 0 0 0 763.0 0 0 1 1,728.0 0 0 0 792.0 0 0 0 1,837.0 0 0 0 807.0 0 0 0 1,854.0 0 0 1 809.0 0 0 1 1,871.0 0 1 0 812.0 0 0 0 1,959.0 0 0 0 822.0 0 0 0 1,990.0 0 0 - 1 a O = not infected, 1 = infected, -1 = indeterminate. b 0 = full term, 1 = premature, -1 = unknown. + Follow-up time greater than 15 months and infection status indeterminate.
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1024 Biometrics, December 1994
"Clinical evidence of infection" includes both AIDS and less advanced disease, such as two or more of the signs in category P2A defined by the Centers for Disease Control (1987), including persistent fever, hepatomegaly, splenomegaly, and several other signs. These data describe the status of infants as of April 1, 1991, the last date of follow-up for this analysis. In constructing Table 3, we have treated the 28 infants whose infection status was indeterminate or unknown at the end of 15 months (day 455) as if they were censored without disease on day 455 (see Table 4 for detailed information). These 28 infants were not officially lost to follow-up, but had a missing or inconclusive HIV antibody test result at age 15 months. The full data set (Table 4) contains the times to onset of clinical disease or censoring, an onset indicator for the presence of clinical evidence of disease, an indicator of infection status (-1 if indeterminate or unknown), and an indicator of prematurity (-1 if unknown gestational status).
As mentioned in Section 1, the estimator of p given by Blanche et al. (1989) is based only on infants born at least 15 months before the analysis date. This estimate is (19 + 15)/(19 + 15 + 65) = 34.3% with standard error 4.77% (Table 3). This estimate is slightly higher than the NMLE, P = 30.0%, with 95% confidence interval (22.3%, 39.1%) and standard error 4.30%. Note that the NMLE is more precise than the estimate of Blanche et al. because it utilizes data from all 233 infants.
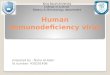
To determine whether infants born prematurely (S37 weeks gestation) are more likely to be infected, we used the procedures in this paper to estimates, = 33.2% with 95% confidence interval (17.1%, 54.3%) for premature infants andpo = 31.8% with 95% confidence interval (22.5%, 42.8%) for full-term infants. In view of these wide confidence intervals, there is no evidence that prema- turity is associated with higher risk, and the T statistic (Section 2) is only .12, corresponding to a two-sided significance level P = .90. The corresponding standardized deviate for the U test (Section 2) is .06, with P = .95. This latter statistic is based on the assumption of equal incubation survival distributions among infected premature infants and infected full-term infants (Figure 1). The incu- bation survival distribution for all infected infants (Figure 1) has a median of about 18 months.
-Combined (n = 233)
--Premature (n=42)
| --o | --Full term (n=147)
>% 0.8g
0 0.6
5 0.4
0.21 0 I I 0 200 400 600 800 1000 1200 1400
time to AIDS onset (days) Figure 1. AIDS onset-free survival for infected infants.
5. Discussion In this note we provide NMLEs of the HIV transmission rate, the conditional incubation survival distribution given that the infants are infected, and tests for the differences in HIV transmission rates. The NMLE of the infection rate is more efficient than estimates that only utilize infants with complete follow-up. Formal tests for the equality of conditional survival distributions, such as those
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

An Analysis of Perinatal Transmission Rate of HIV 1025
in Figure 1, were proposed and studied by Orazem (unpublished Ph.D. dissertation, Columbia University, 1991).
It is important to note that the validity of methods based on the NMLE depends on the assumptions that censoring time is independent of HIV infection status and of time to onset of clinical evidence of HIV disease. Administrative censoring will usually satisfy these assumptions, and "refusal censoring" will also tend to satisfy these assumptions provided protocols require continued follow-up to 15 months, regardless of intercurrent antibody status, as discussed in Section 2. Unbiasedness of the estimator used by Blanche et al. (1989) depends on the stronger assumption described in Section 1. Suppose, however, that follow-up is stopped in some infants as soon as the first negative antibody test is observed. Since the probability of infection is smaller in such infants than in the general population, the chance of censoring will be higher in uninfected than in infected infants. The estimator of p used by Blanche et al. (1989) and the one we propose will tend to overestimate the proportion infected, as the following example illustrates.
Suppose that 100 infants are born more than 15 months before the end of follow-up. Of these, suppose that 10 develop clinical evidence of AIDS within 15 months, 20 are censored when they first become seronegative before age 15 months, 20 remain clinically well but are HIV antibody positive when tested at 15 months, and 50 remain clinically well and antibody negative at 15 months. Suppose, further, that 2 of the 20 censored infants revert to seropositivity at 15 months, so that the true proportion infected isp = (10 + 2 + 20)/100 = .320. The procedure of Blanche et al. (1989) excludes the 20 censored children and yields the estimate (10 + 20)/80 = .375. The bias results from the fact that censored infants have a lower risk of infection (.10) than uncensored infants (.375). The NMLE of p given by equation (3) depends on the ordering of the times to clinical disease and the times to censoring. If all censoring times precede the first onset of clinical disease, equation (3) yields .375, the same result as the method of Blanche et al. If all censorings follow the last time of onset of clinical disease, the estimate is .357, which is less biased for the true value, .320. For other orderings, equation (3) yields estimates of p between .357 and .375. This example illustrates that if most children are followed only until they first become seronegative, the method proposed in this paper and the method used by Blanche et al. (1989) will be upwardly biased. On the other hand, this hypothetical example, and data presented by the European Collaborative Study (1991) and else- where, illustrate that an infant may be infected even though antibody disappears before 15 months. Assuming that all such infants are uninfected yields the estimate (10 + 20)/100 = .300, which underestimates the corrects = .320. Clearly, if one adopts the definition that an infant is uninfected only if he or she is clinically well and antibody free at 15 months, it is preferable to obtain antibody samples on all surviving disease-free children at 15 months, regardless of whether antibody disap- peared previously. If children are lost to follow-up inadvertently, despite vigorous attempts at continued follow-up regardless of intercurrent antibody test values as suggested in Section 2, the methods of Blanche et al. (1989) and estimates from equation (3) will be protected from bias resulting from a dependence between censoring and HIV infection status.
The NMLE of p makes no use of antibody measurements before 15 months. Methods that take advantage of this information might yield even more efficient estimates, but additional model assumptions are required. Currently, we are studying a model that assumes HIV antibody levels follow a Markov process. Another advantage of such models is that one may analyze data from protocols in which censoring does depend on intercurrent antibody levels. Instead of assuming that data are "missing completely at random," one can model the censoring process and assume only that data are "missing at random," conditional on current antibody level (Little and Rubin, 1987).
A major source of variability in estimated transmission rates arises from differences in the precise definition of "clinical evidence of HIV infection." In this paper, we have followed Goedert et al. (1989) in saying that there is clinical evidence of disease if either AIDS develops or if two or more nonspecific signs in category P2A defined by the Centers for Disease Control (1987) are present. The European Collaborative Group (1991) appears to adopt a stricter standard by requiring AIDS, death thought to be related to HIV infection, or detection of virus or viral antigen in two samples.
It may turn out that a few infants who were clinically well and antibody free at 15 months are infected. Additional follow-up is needed to determine the frequency of such infants. If there are appreciable numbers of such infants, the incubation distribution among infected infants may have a longer median than indicated in Figure 1, and estimates of the probability of transmission would need to be revised upward.
The fact that we establish the infection status at 15 months confers much more precision on our estimators of p than comparable applications of "cure models" for which there is never a definitive assessment of whether a "cure" has occurred. For testing p = Pi in the two-sample problem, the additional assumption SO = S1 can lead to a test with increased power in the cure model setting
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1026 Biometrics, December 1994
(Gray and Tsiatis, 1989). However, in the presence of the additional information on infection status at 15 months, the assumption SO = S1 does not lead to substantial increases in power, and we prefer the simpler test T that does not require this assumption.
ACKNOWLEDGEMENTS
We would like to thank the referees and editor for their comments that helped improve the paper considerably. W. Y. Tsai's work was supported in part by National Institutes of Health Grants NIAID-5-R29-AI29004-02 and Center Grant 5-P50-MH43520 NIMH NIDA (Anke A. Ehrhardt, Ph.D., Principal Investigator). This work was also supported by NIH Contract N01-HD-82913 with Westat, Inc. We thank Judy Walsh for expert computer programming and data base management.
RESUME'
Les enfants nes de mere infectee par le virus de l'immunodeficience humaine (VIH) peuvent ou non etre contamines par transmission perinatale. Malheureusement la transmission passive des anticorps maternels rend difficile la determination de l'etat de contamination de l'enfant par l'examen des anticorps anti-VIH, en raison de l'impossibilite d'une distinction precoce apres la naissance entre les anticorps transf6res passivement de la mere et les anticorps produits par un enfant contamine. Habituellement, l'etat de contamination n'est pas observable avant que l'enfant atteigne l'age de 15 mois ou bien ait developpe une maladie due au VIH tel que le syndrome de l'immunodeficience acquise (SIDA). Traditionnellement, les analyses statistiques du taux de transmission perinatale du VIH sont basees sur des enfants nes au moins 15 mois avant la date de l'analyse. De telles analyses peuvent etre a la fois inefficaces et biaisees. Dans cette note, nous definissons un module mixte sous-jacent a la date de debut du SIDA, et obtenons ainsi les estimateurs non parametriques du maximum de vraisemblance pour le taux de transmission du VIH et pour la fonction de repartition de la date de debut du SIDA des enfants contamines. On construit aussi des tests non parametriques pour detecter des differences de taux de transmission du VIH entre differents groupes d'enfants. Enfin, nos methodes sont appliquees a l'etude de cohorte Mere-Enfants de la ville de New-york. Le taux de transmission du VIH des meres infectees a leurs enfants a ete estime a 30%, avec un intervalle de confiance a 95% estime a [22.3%, 39.1%].
REFERENCES
Blanche, S., Rouzioux, C., Moscato, M-L., et al. (1989). A prospective study of infants born to women seropositive for human immunodeficiency virus type 1. New England Journal of Medicine 320, 1643-1648.
Breslow, N. and Crowley, J. (1974). A large-sample study of the life table and product limit estimation under random censorship. Annals of Statistics 3, 437-453.
Centers for Disease Control (1987). Classification system for human immunodeficiency virus (HIV) infection in children under 13 years of age. Morbidity and Mortality Weekly Report 36, 225-236.
Efron, B. (1967). The two-sample problem with censored data. In Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability IV, 831-853. Berkeley, California: University of California Press.
European Collaborative Study (1991). Children born to women with HIV-1 infection: Natural history and risk of transmission. Lancet 337, 253-260.
Goedert, J. J., Mendez, H., Drummond, J. E., et al. (1989). Mother-to-infant transmission of human immunodeficiency virus type 1: Association with prematurity or low anti-gp 120. Lancet 334, 1351-1354.
Gray, R. J. and Tsiatis, A. A. (1989). A linear rank test for use when the main interest is in differences in cure rates. Biometrics 45, 899-904.
Kaplan, E. L. and Meier, P. (1958). Nonparametric estimation from incomplete observations. Journal of the American Statistical Association 53, 457-481.
Little, R. L. A. and Rubin D. B. (1987). Statistical Analysis with Missing Data. New York: Wiley. Tsai, W. Y. (1986). Estimation of survival curves from dependent censorship model via a general-
ized self-consistent property with nonparametric Bayesian estimation application. Annals of Statistics 14, 238-249.
Turnbull, B. W. (1976) The empirical distribution function with arbitrarily grouped, censored and truncated data. Journal of Royal Statistical Society, Series B 38, 290-295.
Received October 1991; revised October 1992 and March 1993; accepted April 1993.
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

An Analysis of Perinatal Transmission Rate of HIV 1027
APPENDIX
Proof That 4 and S* Are NMLE
Setting
afi(q, S*) nu Y_ I(DW*= 1, Tj > 15) 0 =
I = q q S*(15+)-q
implies q = nuS*(15+)/n*(15+). It is easy to see that the PL estimator 3* maximizes the profile log-likelihood e1(nuS*(15+)/n*(15+), S*). Therefore q = nuS*(15)/n*(15+) = nu' (NS(15)) and 3*(t) for t < 15 maximize the log likelihood e1(q, S*).
Proof of Self-Consistency
Proof: (i) By the definition, we have
N - h(O) = E {I(D*= 0) + I(D*= -1)41/*(Tj)} = nu + E I(Di= -1)4N{Sc(T7-) - C(cji)}
n (7) = nu+ S(1 ){1-3c(15 )}
= 4N, which implies the first part of equation (5). The second equality in equation (7) is implied by the fact that N[Sc(Ti-) - SC(Tn) = S*(Ti) (ii) By the self-consistency property (Efron, 1967) of S*(t), we have
1 S*(t) I(D*= -1) 3*(t) = N 1 + N ST for t s 15. (8) N
Ti> t N T-tS*(Ti)
Since the equality in equation (8) holds only for t < 15, the following results are true for t S 15. Subtracting q from (8) and using the equations (4) and (7), we have
NS*(t) - N4
= E 1StI(Di1) I(D*= -1) {I(D= T 5 ) Ti>t Ti___t S*(T) )+ S()f
= 2 {I(Dt*=1)+I(Dt*=-1)R(T~)}+S(t) 2 I(Dt*=-1)S(=)
R(t) = pS(t)/[fr3(t) + q]
is an estimator of the conditional probability of being infected given that one is AIDS-free at time t. Dividing both sides by Np, we obtain
1 S&(ti) R*(Ti) h()T>t h() Ti __t-
f()no I(D 1l) +I(D 1-)f?(Tj)} + n() I(D 1-)5 .
By adapting Tsai's (1986) proof that the solution of a self-consistent equation coincides with the PL estimator, the second part of equation (5) is obtained.
Sketch of the Proof of Asymptotic Normality of q and S First we sketch the proof of asymptotic normality of QN = \/?(q - q). Decompose QN into three terms:
QN = AN-BN + RN,
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions

1028 Biometrics, December 1994
where AN = VN(4 - q)/Sc(15), BN = \N/q[Sc(15) - Sc(15)]ISC2(15), and RN = QN - AN + BN. It is easy to prove RN -* 0 as N -* oo. By using the theorems of Breslow and Crowley (1974), we may further decompose BN as BN = BiN + B2N + op(l), where BiN = qf15 S..V&Wd(Fs - Fsc)/Sc(l5) and B2N = qfO5 Sr2\/N(Sr - SN)dF C/S (15). From the properties of empirical processes, (AN, BN) converges to a random vector (A, B) having bivariate normal distribution with mean 0 and variance- covariance matrix given by var(A) = (1 - q)q/Sc2(15), var(B) = q2 f 05 S7-2(x) dFsc(x) and cov(A, B) = var(B). The asymptotic normality and variance of QN follow, and a similar decomposition yields the asymptotic Gaussian process of \/N(S - S).
This content downloaded from 185.2.32.106 on Wed, 25 Jun 2014 07:29:23 AMAll use subject to JSTOR Terms and Conditions