Embed Size (px)
Citation preview

A national perspective on A national perspective on progressprogress
Professor Brian DuerdenProfessor Brian DuerdenInspector of Microbiology and Infection Inspector of Microbiology and Infection
Control,Control,Department of Health, London Department of Health, London

2007 -The challenge of HCAI2007 -The challenge of HCAI
MRSA bacteraemiaMRSA bacteraemia– 2001/2 7291 (Q Av)18232001/2 7291 (Q Av)1823– 2002/3 7426 (Q Av)18562002/3 7426 (Q Av)1856– 2003/4 7700 (Q Av)19252003/4 7700 (Q Av)1925– 2004/5 7212 (Q Av)18082004/5 7212 (Q Av)1808– 2005/6 7097 (Q Av)17732005/6 7097 (Q Av)1773– 2006/7 2006/7 Q1 Q1 1741 1741 Q2 1651Q2 1651 Q3 1542Q3 1542
Q4Q4 14471447
6381 6381 – 2007/8 Q1 13032007/8 Q1 1303
C. difficile C. difficile infectioninfection– 2001 220082001 22008– 2002 289862002 28986– 2003 355372003 35537– 2004 436722004 43672– 2005 498502005 49850(voluntary reporting, England, (voluntary reporting, England,
Wales, NI)Wales, NI)
– 20042004 44314 44314– 2005 517672005 51767– 2006 556812006 55681– 2007 2007 Q1 15639Q1 15639– Q2 13660Q2 13660 +2890 +2890
(<65)(<65)(England, mandatory)(England, mandatory)

Responsibility for HCAIResponsibility for HCAI
CliniciansClinicians– Safe patient careSafe patient care– DiagnosisDiagnosis– TreatmentTreatment– PreventionPrevention– ControlControl
Board/CEx/DIPCBoard/CEx/DIPC– Corporate Corporate
environmentenvironment– Make it happenMake it happen
Government/DHGovernment/DH– Set standardsSet standards– Ensure priorityEnsure priority– Monitor outcomeMonitor outcome– LegislationLegislation– Performance Performance
managementmanagement
Reducing HCAI….Reducing HCAI….
Change the mindsetChange the mindsetFrom: From: 1) create a system to deliver specialist clinical 1) create a system to deliver specialist clinical
carecare2) take measures to prevent infection 2) take measures to prevent infection
To:To:1) create a safe environment for patient care1) create a safe environment for patient care2) deliver specialist clinical care within that 2) deliver specialist clinical care within that
environmentenvironment
Getting Ahead of the Curve - 2002Getting Ahead of the Curve - 2002
Priorities identifiedPriorities identified
HCAIHCAI– bacteraemia (MRSA, GRE)bacteraemia (MRSA, GRE)– C. difficile C. difficile associated diarrhoeaassociated diarrhoea– surgical site infectionsurgical site infection
TuberculosisTuberculosis
Blood-borne & sexually transmitted viruses (and Blood-borne & sexually transmitted viruses (and others!)others!)
Antimicrobial resistanceAntimicrobial resistance

And then……….And then……….
POLITICSPOLITICS
(and the media hype)(and the media hype)

HCAI 2003 - 04HCAI 2003 - 04
Winning Ways Winning Ways - December 2003- December 2003– Strategy for HCAIStrategy for HCAI
NAO Report - NAO Report - July 2004July 2004– Critical of slow progressCritical of slow progress
Towards Cleaner Hospitals and Lower Towards Cleaner Hospitals and Lower Rates of Infection Rates of Infection - July 2004- July 2004– Action planAction plan

MRSA TargetMRSA Target
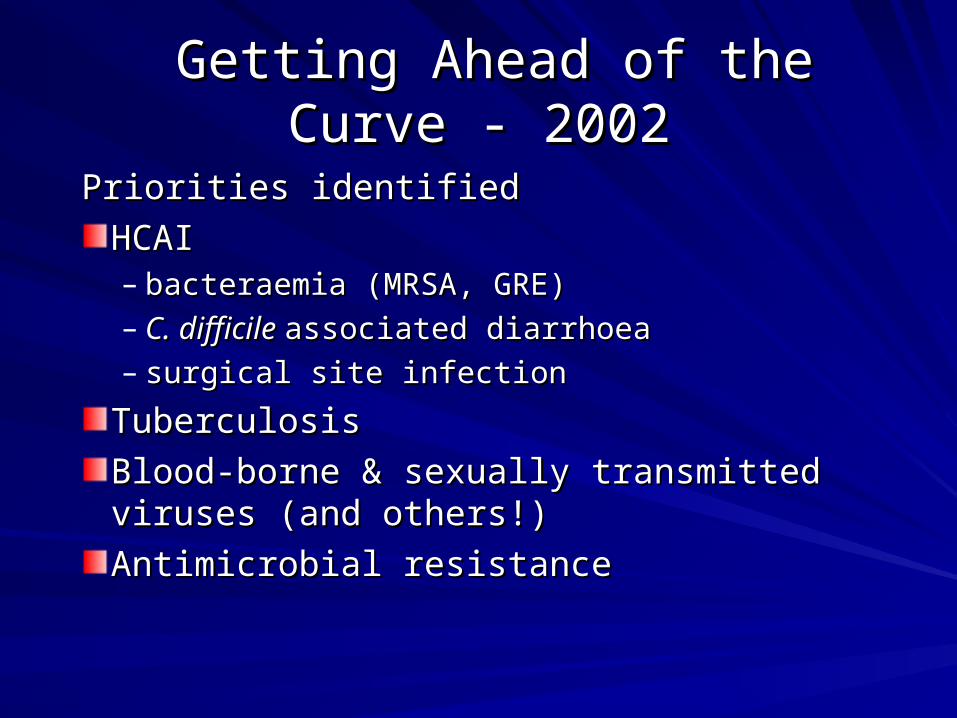
‘‘Halve MRSA infections by 2008’Halve MRSA infections by 2008’– MRSA bacteraemiaMRSA bacteraemia– Baseline 2003-04; Start date April 2005Baseline 2003-04; Start date April 2005– Monthly returnsMonthly returns– 3-monthly publication from Jan 20073-monthly publication from Jan 2007– Monthly submission and DH/SHA reviewMonthly submission and DH/SHA review
Depends upon mandatory surveillance Depends upon mandatory surveillance being accurate and timely – CEx sign-offbeing accurate and timely – CEx sign-off
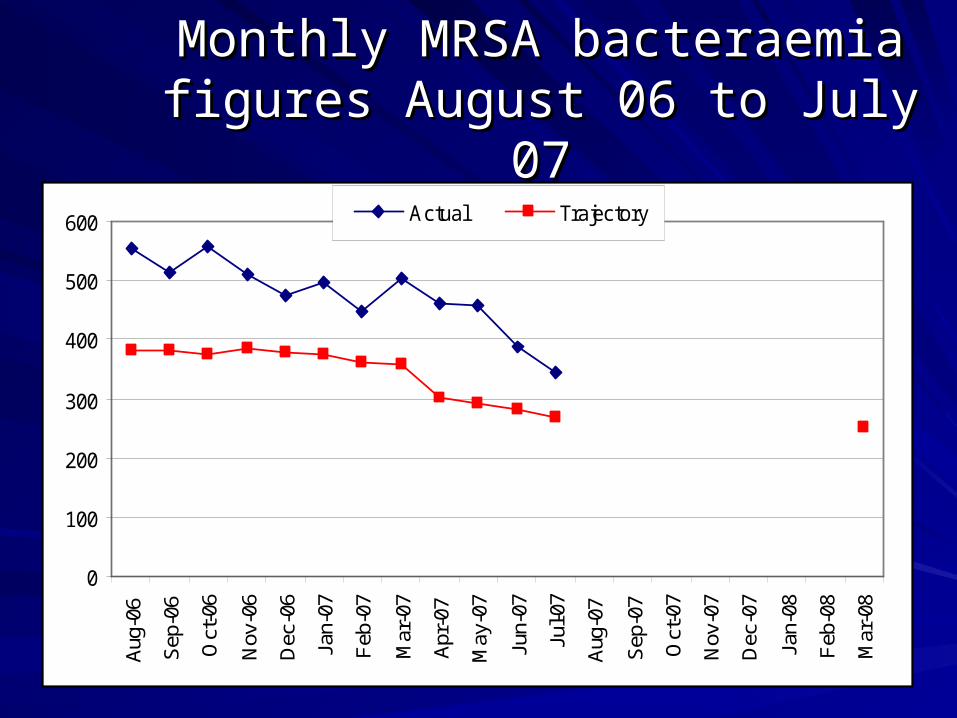
Monthly MRSA bacteraemia Monthly MRSA bacteraemia figures August 06 to July 07figures August 06 to July 07
0
100
200
300
400
500
600
Aug
-06
Sep
-06
Oct
-06
Nov
-06
Dec
-06
Jan-
07
Feb
-07
Mar
-07
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Sep
-07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb
-08
Mar
-08
Actual Trajectory

MRSA reportingMRSA reporting
TimelinessTimeliness– CEO lock down CEO lock down – Data entry in timeData entry in time– Use voluntary screen to record info to focus Use voluntary screen to record info to focus
efforteffort
Extenuating circumstancesExtenuating circumstances– DuplicatesDuplicates– Repeats in untreatable patientsRepeats in untreatable patients– Responsible Trust (eg, renal satellite units)Responsible Trust (eg, renal satellite units)

What do the data tell us?What do the data tell us?Men >65 yrs are 43% of MRSA bacteraemias Men >65 yrs are 43% of MRSA bacteraemias – (15% of all admissions nationally) (15% of all admissions nationally)
80% of MRSA bacteraemias are in emergency admissions80% of MRSA bacteraemias are in emergency admissions
– (37% of total admissions)(37% of total admissions)
35% have been in hospital during the previous month 35% have been in hospital during the previous month
Length of stay over 7 days increases riskLength of stay over 7 days increases risk
10% of MRSA bacteraemias come from nursing homes10% of MRSA bacteraemias come from nursing homes
– 17% for pre-48 hour cases. 17% for pre-48 hour cases.
30% diagnosed in first 48hrs 30% diagnosed in first 48hrs
– but 65% of these patients have touched health care setting in recent pastbut 65% of these patients have touched health care setting in recent past
Risk factorsRisk factors
– 14% - chronic wounds14% - chronic wounds
– 14% - central lines; 10% peripheral lines14% - central lines; 10% peripheral lines
– 8% pneumonia8% pneumonia

Healthcare Associated InfectionsHealthcare Associated Infections
MRSA - MRSA - not the only one!not the only one!
Clostridium difficileClostridium difficile
Glycopeptide resistant enterococciGlycopeptide resistant enterococci
ESBL-producing ESBL-producing E. coliE. coli etc etc
Acinetobacter baumanniiAcinetobacter baumannii
NorovirusNorovirus

C. difficileC. difficile “new superbug” hits the national “new superbug” hits the national press Mon. June 6press Mon. June 6thth 2005. Jeremy Laurance – 2005. Jeremy Laurance –
Health Editor, The IndependentHealth Editor, The Independent

C. difficile C. difficile voluntary reporting 1991 – 2005: voluntary reporting 1991 – 2005: England, Wales and Northern IrelandEngland, Wales and Northern Ireland
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
year
nu
mb
er
of
rep
ort
s

Mandatory surveillance 2004 - 7Mandatory surveillance 2004 - 7
January 2004January 2004– All NHS Trusts in EnglandAll NHS Trusts in England– Report all cases of Report all cases of C. difficile C. difficile diseasedisease
Toxin +ve diarrhoeaToxin +ve diarrhoea
– Patients over 65 years (over 2 years from April 2007)Patients over 65 years (over 2 years from April 2007)
ResultsResults– 2004 : 44,3142004 : 44,314– 2005 : 51,7672005 : 51,767– 2006 : 55,6812006 : 55,681– 2007 : Q1 156392007 : Q1 15639– Q2 13660 + 2890 (<65y)Q2 13660 + 2890 (<65y)

C. difficile C. difficile deaths 1999-2005deaths 1999-2005
19991999 20012001 20022002 20032003 20042004 20052005
DC DC mentionsmentions
975975 1,2141,214 1,4281,428 1,7881,788 2,2472,247 3,8073,807
UCUC 531531 691691 756756 958958 1,2451,245 2,0742,074
% as % as UCUC
5454 5757 5353 5555 5555 5454
Office of National Statistics

Deaths in CDIDeaths in CDI
HCC assessmentHCC assessment– DefinitelyDefinitely– ProbablyProbably– PossiblyPossibly– Unlikely Unlikely – NoNo
What should we What should we measure?measure?
Clinical experienceClinical experience– 5-10% direct cause5-10% direct cause– 5-10% probable 5-10% probable
contributorycontributory
– 30-day mortality 30%30-day mortality 30%– 60-day mortality 60-day mortality
35-40%35-40%
C. difficile C. difficile profile 2005-06profile 2005-06Public, media, politiciansPublic, media, politiciansHCC/HPA Survey published Dec. 2005HCC/HPA Survey published Dec. 2005– NHS Trusts not following guidance NHS Trusts not following guidance – Antibiotic policies; prevention; management; Antibiotic policies; prevention; management;
infection control; reportinginfection control; reporting
Advisory letter from CMO/CNO Dec 2005Advisory letter from CMO/CNO Dec 2005Saving Lives Saving Lives HII (care bundle) June 2006HII (care bundle) June 2006HCC report on Stoke Mandeville July 2006HCC report on Stoke Mandeville July 2006CMO/CNO/CPhO/CEx letter Dec 2006CMO/CNO/CPhO/CEx letter Dec 2006

CMO/CNO/CPhO/CEx guidance: Dec 2006CMO/CNO/CPhO/CEx guidance: Dec 2006
Antibiotic prescribingAntibiotic prescribing– Limit broad spectrum agentsLimit broad spectrum agents– Limit IV Limit IV andand oral courses oral courses
Prompt diagnostic tests – Toxins A+BPrompt diagnostic tests – Toxins A+B– isolates for typing if outbreak suspected isolates for typing if outbreak suspected
Isolation/segregation/cohorting of casesIsolation/segregation/cohorting of cases
Infection control – handwashing, gloves, gownsInfection control – handwashing, gloves, gowns
Decontamination/cleaning – increaseDecontamination/cleaning – increase– Chlorine-based disinfectantChlorine-based disinfectant

C. difficile C. difficile local targetslocal targets
Effective April 2007Effective April 2007
PCT/Acute Trust agreementPCT/Acute Trust agreement– Part of annual contractsPart of annual contracts
Sliding scale of percentage reductionsSliding scale of percentage reductions
SHA monitoringSHA monitoring
How do we change bad habits?How do we change bad habits?
ManagementManagement– emphasis on infection control emphasis on infection control
Enhanced surveillance (HPA)Enhanced surveillance (HPA)– MRSA & MRSA & C. difficileC. difficile
Clinical practice protocolsClinical practice protocolsCleanliness and hygieneCleanliness and hygiene– hand hygienehand hygiene– environmental cleaningenvironmental cleaning
TrainingTrainingTargets and performance management Targets and performance management
Management priority & responsibilityManagement priority & responsibility
HCAIHCAI– NOTNOT just the Infection Control Team just the Infection Control Team– Trust BoardTrust Board– Chief ExecutiveChief Executive– Clinical ownershipClinical ownership– ALL STAFFALL STAFF
DIPC is the focusDIPC is the focus– ResponsibilityResponsibility– Authority – clinical and managerialAuthority – clinical and managerial– Resource allocationResource allocation

WW Action area 6.Management WW Action area 6.Management and organisationand organisation
Chief Executive’s responsibilitiesChief Executive’s responsibilities– Core part of Clinical Governance and Patient Core part of Clinical Governance and Patient
Safety programmesSafety programmes– Promote low levels of HCAIPromote low levels of HCAI
Ensure actions are takenEnsure actions are taken
– Aware of legal responsibilities to identify, Aware of legal responsibilities to identify, assess and control risks of infectionassess and control risks of infection
– Appoint Director of Infection Prevention and Appoint Director of Infection Prevention and ControlControl

DIPC roleDIPC role
Senior management – Board/CEx reportSenior management – Board/CEx reportProfessional credibilityProfessional credibility– Special expertiseSpecial expertise
Reporting line for ICTReporting line for ICTPolicy implementationPolicy implementationPerformance managementPerformance managementResource allocationResource allocationA champion & a manager!!A champion & a manager!!
Improved Improved C. difficile C. difficile surveillancesurveillance
Individual web entry; started April 1, 2007Individual web entry; started April 1, 2007
All patients over 2 yearsAll patients over 2 years
Core dataCore data– Identifier; age; sexIdentifier; age; sex– Date of sampleDate of sample– Location of patientLocation of patient– Reporting laboratoryReporting laboratory– [from Jan. 08 – in/outpatient; admission date] [from Jan. 08 – in/outpatient; admission date]
C. difficile C. difficile voluntary pagevoluntary page
Risk factorsRisk factors– Health services contactHealth services contact– Antibiotic historyAntibiotic history– SpecialtySpecialty– Augmented careAugmented care– Emergency or electiveEmergency or elective
Suggest 2 – 4 weeks, 4 times a year?Suggest 2 – 4 weeks, 4 times a year?
Local assessment; national poolingLocal assessment; national pooling

Providing the tools Providing the tools
CleanCleanyouryourhands hands campaigncampaignPEAT inspections for cleanlinessPEAT inspections for cleanlinessSaving Lives & Essential StepsSaving Lives & Essential StepsRoot Cause Analysis toolRoot Cause Analysis tool– bacteraemia-specific version – Sept 2006bacteraemia-specific version – Sept 2006
MRSA screening advice - October 2006MRSA screening advice - October 2006C. difficile C. difficile guidance - December 2006guidance - December 2006
…………..and now……...and now…….

……..legislation..legislation
Health Act 2006Health Act 2006–Statutory Code of Practice Statutory Code of Practice –Compliance assessed by the Compliance assessed by the
Healthcare CommissionHealthcare CommissionAnnual healthcheckAnnual healthcheck120 unannounced spot checks120 unannounced spot checksImprovement noticesImprovement notices

‘‘Saving lives’ Saving lives’ toolkittoolkit
Two componentsTwo components– Self assessment tool – Self assessment tool –
now revised to reflect CoP core dutiesnow revised to reflect CoP core duties– 7 High Impact Interventions (Care Bundle 7 High Impact Interventions (Care Bundle
approach)approach)
- plus guidance notes- plus guidance notes

High Impact InterventionsHigh Impact Interventions (revised June 2007) (revised June 2007)
1.1. Central venous cathetersCentral venous catheters2.2. Peripheral line carePeripheral line care3.3. Dialysis cathetersDialysis catheters4.4. Surgical site managementSurgical site management5.5. Urinary cathetersUrinary catheters6.6. Ventilator managementVentilator management7.7. Clostridium difficileClostridium difficile

SL GuidanceSL Guidance
October 2006 October 2006 – MRSA screening MRSA screening
June 2007June 2007– Blood Culture protocolBlood Culture protocol– Antimicrobial prescribing frameworkAntimicrobial prescribing framework
September 2007September 2007– Isolation and cohortingIsolation and cohorting

Environmental hygieneEnvironmental hygiene
Hospitals should be clean!Hospitals should be clean!
Role of matrons & ward sistersRole of matrons & ward sisters
Routine cleaningRoutine cleaning– Hand-contact areasHand-contact areas
Enhanced cleaning in infected areasEnhanced cleaning in infected areas– Use of disinfectantsUse of disinfectants
Deep cleaning after discharge of infected patientDeep cleaning after discharge of infected patient
Cleaning of the bed and bed spaceCleaning of the bed and bed space
Medical equipmentMedical equipment

TrainingTrainingBMJ BMJ eeLearningLearning– C. difficileC. difficile video CPD module video CPD module
DoctorsNetDoctorsNet– CPD moduleCPD module
Dialogue withDialogue with– Undergraduate DeansUndergraduate Deans– Tomorrow’s Doctors Tomorrow’s Doctors review group (GMC)review group (GMC)– Royal CollegesRoyal Colleges– Postgraduate DeansPostgraduate Deans

Target performance managementTarget performance management
DH Task ForceDH Task Force– Reviews MRSA bacteraemia and Reviews MRSA bacteraemia and C. difficle C. difficle
figuresfigures– Monitors programme activitiesMonitors programme activities– Identifies Trusts for Identifies Trusts for SL SL reviews and visitsreviews and visits
SHA performance managersSHA performance managers– Monthly review of Trust performanceMonthly review of Trust performance
PCT commissioners – PCT commissioners – C. difficileC. difficile

Improvement programmeImprovement programme
National Performance Improvement National Performance Improvement Network (PIN)Network (PIN)– Meets 3 times a yearMeets 3 times a year
Saving Lives Saving Lives self assessment reviewsself assessment reviews
Improvement visitsImprovement visits– DH team;DH team; 2-day interviews2-day interviews– Develop local action/recovery planDevelop local action/recovery plan– Support implementationSupport implementation

Summer 2007Summer 2007
Saving Lives Saving Lives issue 2 (June)issue 2 (June)– C. difficile C. difficile care bundle updatedcare bundle updated– Antimicrobial prescribing – best practiceAntimicrobial prescribing – best practice
ImprovementImprovement Team (formerly MRSA)Team (formerly MRSA)– Double funding (and size!)Double funding (and size!)– Extend remit to Extend remit to C. difficileC. difficile
DIPC –DIPC – review review SACAR report – SACAR report – J Antimicrob Chemother J Antimicrob Chemother suppl Aug 2007suppl Aug 2007
– Antimicrobial frameworkAntimicrobial framework

Antibiotic policy - preventionAntibiotic policy - prevention
Restrict use of broad spectrum agentsRestrict use of broad spectrum agentsPromote aminoglycosides (gentamicin etc)Promote aminoglycosides (gentamicin etc)Reasons for prescribing recordedReasons for prescribing recordedStop dates – review by pharmacistsStop dates – review by pharmacistsProphylaxis – single doseProphylaxis – single doseAudit, training and reviewAudit, training and reviewRole of Antimicrobial Prescribing Role of Antimicrobial Prescribing Team/CommitteeTeam/Committee

Announcements Sept-Oct 2007Announcements Sept-Oct 2007
National CD target - 30% reduction by 2011National CD target - 30% reduction by 2011CMO PL on Death CertificationCMO PL on Death CertificationDeep cleaning (PM)Deep cleaning (PM)Matrons & Clinical Directors report to Boards Matrons & Clinical Directors report to Boards quarterlyquarterlyDress code – bare below the elbowDress code – bare below the elbowMRSA screening – universal (asap)MRSA screening – universal (asap)Isolation and cohorting guidance Isolation and cohorting guidance Regulator powers: fines and ward closuresRegulator powers: fines and ward closures

Dress code (mainly for doctors)Dress code (mainly for doctors)
Bare Below the Elbow (BBE)Bare Below the Elbow (BBE)– Short sleevesShort sleeves– No wrist watchNo wrist watch– No wrist or hand jewellery (except plain wedding No wrist or hand jewellery (except plain wedding
band)band)
– Sleeves/cuffs and jewellery are impediments to Sleeves/cuffs and jewellery are impediments to hand hygiene and aseptic procedureshand hygiene and aseptic procedures
No ties (except bow ties) – No ties (except bow ties) – they are readily contaminated they are readily contaminated and not washed!and not washed!No white coats!No white coats!Scrubs where appropriate, eg, theatre, ICU/HDU, A&EScrubs where appropriate, eg, theatre, ICU/HDU, A&E

October 2007 HCC ReportOctober 2007 HCC Report
Maidstone & Tonbridge WellsMaidstone & Tonbridge Wells– Major outbreak Oct 2005 – Sept 2006Major outbreak Oct 2005 – Sept 2006– Not reported to HPU until April 2006Not reported to HPU until April 2006– Misleading public announcements in JuneMisleading public announcements in June– SHA initiated review in early July and SHA initiated review in early July and
immediately referred to HCCimmediately referred to HCC
FindingsFindings– Very serious failures of management and Very serious failures of management and
clinical careclinical care

National recommendationsNational recommendations
C. difficile C. difficile regarded as a diagnosis in own rightregarded as a diagnosis in own rightCommissioners to ensure acute trusts have Commissioners to ensure acute trusts have guidelines in placeguidelines in placeEducation and training of junior doctorsEducation and training of junior doctors– Improve recording on Death CertificatesImprove recording on Death Certificates
Reinforce antibiotic stewardship messagesReinforce antibiotic stewardship messagesNHS/HPA to agree clear and consistent NHS/HPA to agree clear and consistent arrangements for monitoring rates of CDIarrangements for monitoring rates of CDIBoards to understand role and responsibility of Boards to understand role and responsibility of DIPC and receive regular informationDIPC and receive regular information

A wake-up call……..A wake-up call……..
We must no longer accept these infections We must no longer accept these infections as ‘normal’as ‘normal’PatientsPatients– Can be very illCan be very ill– Can dieCan die– Stay in hospital longerStay in hospital longer– May need major surgeryMay need major surgery
Significant NHS resources can be better Significant NHS resources can be better usedused

Goal (Government/DH) - useGoal (Government/DH) - use
Political imperativePolitical imperativeMeasurementMeasurementTarget settingTarget settingProfessional supportProfessional supportPerformance management ANDPerformance management ANDLegislation Legislation
To change human behaviour (clinical & To change human behaviour (clinical & managerial) tomanagerial) toOvercome the challenge of HCAIOvercome the challenge of HCAI