Embed Size (px)
Citation preview


A Multi-Disciplinary Approach
Targeted Therapies in the Management of Non-Small Cell Lung Cancer

Course Faculty
Medical Oncologists:
Dr. Barb Melosky – British Columbia Cancer Agency, Vancouver, BC
Dr. Jeff Rothenstein – Lakeridge Health Oshawa, Oshawa, ON
Dr. Sunil Verma – Odette Cancer Center, Toronto, ON
Radiation Oncologist:
Dr. Patrick Cheung – Odette Cancer Center, Toronto, ON
Pathologists:
Dr. Ming Tsao – Princess Margaret Hospital, Toronto, ON

Disclosures
• Dr. Barb Meloskyo Advisory Board – Astra Zeneca, Roche, Boehringer Ingelheim, Pfizer, Lilly
• Dr. Jeff Rothensteino Advisory Board – Lilly, BMS; Grants/honorarium – Novartis; Clinical trials –
Roche, BMS, AstraZeneca, Boehringer Ingelheim, Novartis
• Dr. Sunil Vermao Advisory Board – AstraZeneca, Roche, Boehringer Ingelheim, Novartis, Lilly
• Dr. Patrick Cheungo None to declare
• Dr. Ming Tsaoo Grants/honorarium – Pfizer, Merck, Roche, AstraZeneca, Boehringer
Ingelheim

Course Objectives
1. To review the evidence for use of biomarkers to help make treatment decisions for patients with advanced non small cell lung cancer
2. To discuss the current opportunities and challenges in integrating biomarkers in clinical care of lung cancer patients
3. To review the latest evidence on targeted therapies incorporating biomarkers
4. To discuss the emerging roles of radiotherapy in the management of metastatic NSCLC.

Course Outline
• Module 1: Case Study & NSCLC Treatment Overview
• Module 2: Molecular Testing in NSCLC
• Module 3: EGFR/TKI: Evidence
• Module 4: ALK Inhibitors: Evidence

Module 2: Molecular Testing in NSCLC
Targeted Therapies in the Management of Non-Small Cell Lung Cancer: A Multi-
Disciplinary Approach
Dr. Ming TsaoPathologist, Princess Margaret Hospital, Toronto, ON

EGFR and ALK Testing in Non-Small Cell Lung Cancer

Module 2 Objectives
• Assess the guidelines and molecular testing procedures for selecting EGFR and/or ALK lung cancer patients.
• Describe the diagnostic procedures for molecular testing in NSCLC patients including sample selection, techniques and other requirements.
• Review Canadian algorithm and resources for molecular testing in NSCLC patients.

Current Biomarkers for FDA-Approved Therapies for NSCLC Patients
ALK = anaplastic lymphoma kinase; EGFR = epidermal growth factor receptorNSCLC = non-small-cell lung cancer; TKI = tyrosine kinase inhibitor
Agent Patient selection Tumour type
Bevacizumab
Histology Non-squamous
Pemetrexed
EGFR TKIsEGFR mutations
(first-line)Predominantly in adenocarcinoma Crizotinib
CeritinibALK (& ROS1)rearrangements
Nivolumab None Non-Small Cell
Pembrolizumab PD-L1 (22C3) Non-Small Cell

EGFR Mutation Rates: Low in Squamous Cell Carcinoma
Number of studies
Number of patients
MutationPositive
% Mutation Prevalence
Sex
Female 46 4858 1886 38.8
Male 46 3574 853 23.8
Smoking
Never 40 2913 1509 51.8
Ever 40 4755 834 17.5
Ethnicity
East Asian 27 3178 1483 46.6
Caucasian 19 5254 1256 23.9
Histology
Adeno ca 44 7718 2544 33
Squamous ca 17 278 14 5
Adenosquamous ca 4 14 5 36
Large cell ca 10 21 3 14
Adapted from Lindeman et al, J Thorac Oncol 2013;8:823-59; Mascaux et al, Thoracic Oncology: IASLC Multidisciplinary Approach, Chapter 18

EGFR Mutation Rates in East Asian Patients: Highest Among Female/Never-
SmokersMale Female Ever-smoker Never-
smoker
Hsieh (Taiwan) 23% 72% 21% 66%
Chou (Taiwan) 52% 72% 44% 69%
Yang (Taiwan) 55% 64% 37% 62%
Wu (Taiwan) 57% 65% 54% 65%
Kosaka (Japan) 36% 62% 30% 68%
Tokumo (Japan) 33% 67% 27% 73%
Takano (Japan) 53% 69% 51% 68%
Han (S. Korea) 9% 33% 13% 26%
Shigematsu (USA) 18% 54% 13% 56%
IPASS (many countries) 49% 63% - -

ALK Re-arranged Lung Cancer:Also Low in Squamous Cell Carcinoma
5.2 5.7
11.1
1.3
9
4.8
NSCLC ADC(unselected)
ADC(selected)
SCC ADSC NSCLC-Others
NSCLC (N=4025)
ADC (N=6775)
SCC (n=1411)
ADSC (n=78)
NSCLC-Others (n=376)
Number of Tumors Tested (n=12,665)
Estimated Prevalence Rate (% tested)
NSCLC: non-small cell lung cancer; ADC: adenocarcinoma; SCC: squamous cell carcinoma; ADSC: adenosquamous carcinoma
Adapted from IASLC ATLAS of ALK Testing in Lung Cancer , Chapter 2, 2013
Guideline for Molecular Testing in Lung Cancer from CAP/IASLC/AMP
• Aim: To establish evidence-based recommendations for the molecular analysis of lung cancers
• Systematic review conducted by: the College of American Pathologists (CAP), the International Association for the Study of Lung Cancer (IASLC), and the Association for Molecular Pathology (AMP)
Lindeman NI, et al. J Thorac Oncol. 2013;8:823–59; Lindeman NI, et al. Arch Pathol Lab Med. 2013;137:828–60; Lindeman NI, et al. J Mol Diagn. 2013;15:415–53

ASCO Endorsement

Patient Selection
Clinical factors: None
Histology:
• Adenocarcinoma or NSCLC with adenocarcinoma
component
• Small samples for which an adenocarcinoma component
cannot be excluded
• Pure Squamous and neuroendocrine carcinomas be tested
only in never smokers and young patients

1st Step in Mutation/FISH Testing
Shiau CJ, et al. J Thorac Oncol 2014 (7):9:947-56
Pathologist must review HE slide and mark areas for analysis

What (samples) to Test?
• Primary or metastatic lesions are suitable
• In most instances, available paraffin embedded diagnostic tumor samples:
o Resection specimens: patients with recurrence after previous surgery
o Needle core or aspiration (including EBUS) biopsy: for newly diagnosed advanced cancer patients
o Re-biopsy/effusion: for patients without readily available samples
• Cytology specimens
o Smear (air dried > alcohol fixed)
o Cytospin slide
o Cell block / gel block (FFPE)

Primary: 62%
Lymph node: 4%
Metastatic: 27%
Pleural fluid: 5%
Others: 2%
ONTARIO PROVINCE-WIDE EXPERIENCE
Shiau CJ, et al. J Thorac Oncol 2014 (7):9:947-56

Excision: 37%
Small biopsy: 40%
Cytology: 23%
ONTARIO PROVINCE-WIDE EXPERIENCE
Shiau CJ, et al. J Thorac Oncol 2014 (7):9:947-56

What are the Sample Requirements?
• Molecular Testing:
o At least 5 to 10 unstained slides at 4 microns plus an H and E with tissue being at least 0.25cm2 and at minimum 30% tumor cellularity
o Will work on paraffin embedded cytological material such as FNAs, as long as the tumor cellularity is sufficient
o Decalcified samples have lower rate of success for molecular testing and should be avoided.
• FISH
o At least 2 to 3 unstained sections on charged slides at 4 micron thickness
• IHC
o 2-3 unstained 4 micron tissue sections on charged slides for IHC plus an H&E
o Should not be more than 3 weeks after cutting
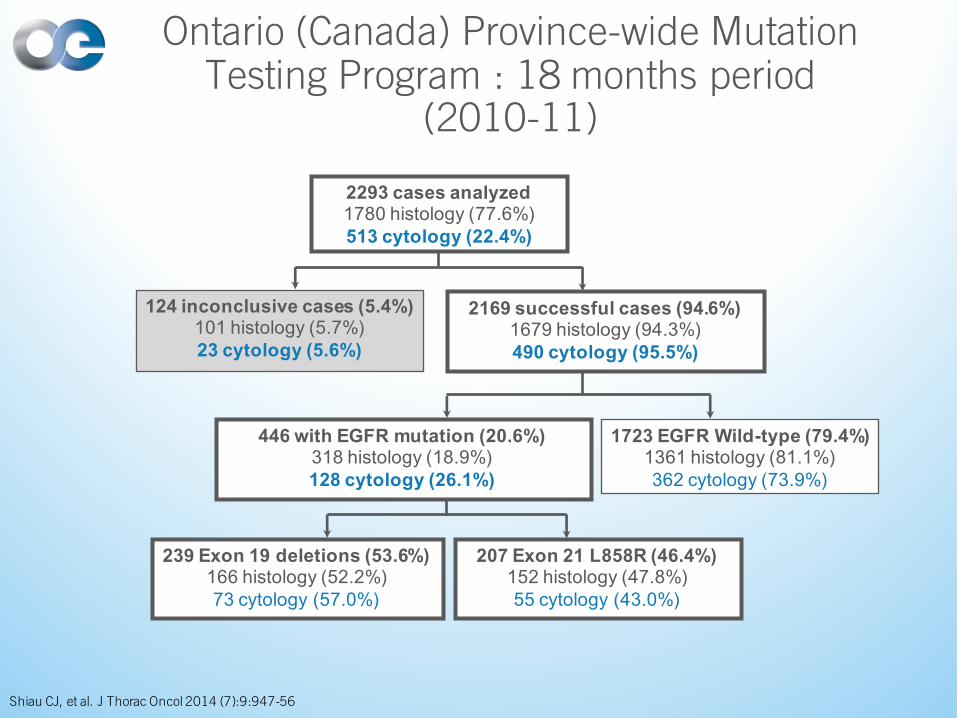
2293 cases analyzed1780 histology (77.6%)513 cytology (22.4%)
124 inconclusive cases (5.4%)101 histology (5.7%)23 cytology (5.6%)
239 Exon 19 deletions (53.6%)166 histology (52.2%)73 cytology (57.0%)
1723 EGFR Wild-type (79.4%)1361 histology (81.1%)362 cytology (73.9%)
207 Exon 21 L858R (46.4%)152 histology (47.8%)55 cytology (43.0%)
446 with EGFR mutation (20.6%)318 histology (18.9%)128 cytology (26.1%)
2169 successful cases (94.6%)1679 histology (94.3%)490 cytology (95.5%)
Ontario (Canada) Province-wide Mutation Testing Program : 18 months period
(2010-11)
Shiau CJ, et al. J Thorac Oncol 2014 (7):9:947-56

Testing in Cytology Specimens
Variable n (%) Successful test (%)Abundant 143 (27.8) 140 (97.9)Moderate 128 (25.0) 127 (99.2)
Small-clusters 118 (23.0) 112 (94.9)Minimal 83 (16.2) 73 (88.0)
Shiau CJ, et al. J Thorac Oncol 2014 (7):9:947-56

EGFR Mutation: PCR/Direct Sequencing
Minimum >30% tumor cellularityMay potentially miss up to 30% of mutations

Mutation Tests with Increased Sensitivity
Method% Tumor DNA
required
Targeted or screening
method
EGFR mutations
detected
Detection of
deletions and
insertions
Sanger direct sequencing 25 screening Known and new yes
Real time/Taqman PCR 10 targeted Known only no
High Resolution Melting Analysis 5-10 screening Known and new yes
COBAS (Roche) 5-10 targeted Known yes
Pyrosequencing 5-10 screening Known only yes
SNaPshot PCR 1-10 targeted Known only yes
Cycleave PCR 5 targeted Known only yes
Fragment length and RFLP analysis 5 Screening/targeted Known only yes
Allelic specific PCR/Scorpions ARMS 1 targeted Known only no
MassARRAY 1 targeted Known only yes
PNA-LNA PCR clamp 1 targeted Known only no
Denaturing HPLC 1 screening Known and new yes
Massively parallel/NGS 0.1 screening Known and new yes
Mascaux et al, Thoracic Oncology: IASLC Multidisciplinary Approach, Chapter 18

Must Test EGFR Mutations
Sharma SV, et al. Nat Rev Cancer 2007;7:169-81
90%

Desirable to Test EGFR Mutations
Sharma SV, et al. Nat Rev Cancer 2007;7:169-81
Lesscommonmutationstodetect

V1E13;A20E20;A20
E20ins18;A20E6;A20
E6ins33;A20E14;ins11del49A20
T3;A20
KI24;A20
KI15;A20
E6;A19
E2;A20E2;ins117A20E3;ins69A20
E14;del12A20E14;del36A20
E17;ins30A20E17ins61;ins34A20
E15del19;del20A20E18;A20
V2
V3aV3bV4
V5bV5a
V7V6
V8aV8b
“V5”“V4”
E17ins68;A20
EML4–ALK
KIF5B–ALK
TFG–ALK
KI17;A20
PTPN3-ALK
KLC1–ALK KL9;A20
ALKkinasedomain
Ou SH, et al. Oncologist 2012;17:1351–75
ALK – Multiple Variants Detectable by FISH

ALK Gene Rearrangement:FISH with Break Apart Probes
~12 MbALK EML4
e20

Optimized IHC to Detect ALK Fusion Protein Requires Signal Amplification
• Advantage: routinely used in pathology practice, fast and cost-effective
IASLC ATLAS of ALK Testing in Lung Cancer , Chapter 4, 2013

Canada Algorithm for Routine ALK Testing
Cutz et al. J Thorac Oncol 2014;9(9):1255-63
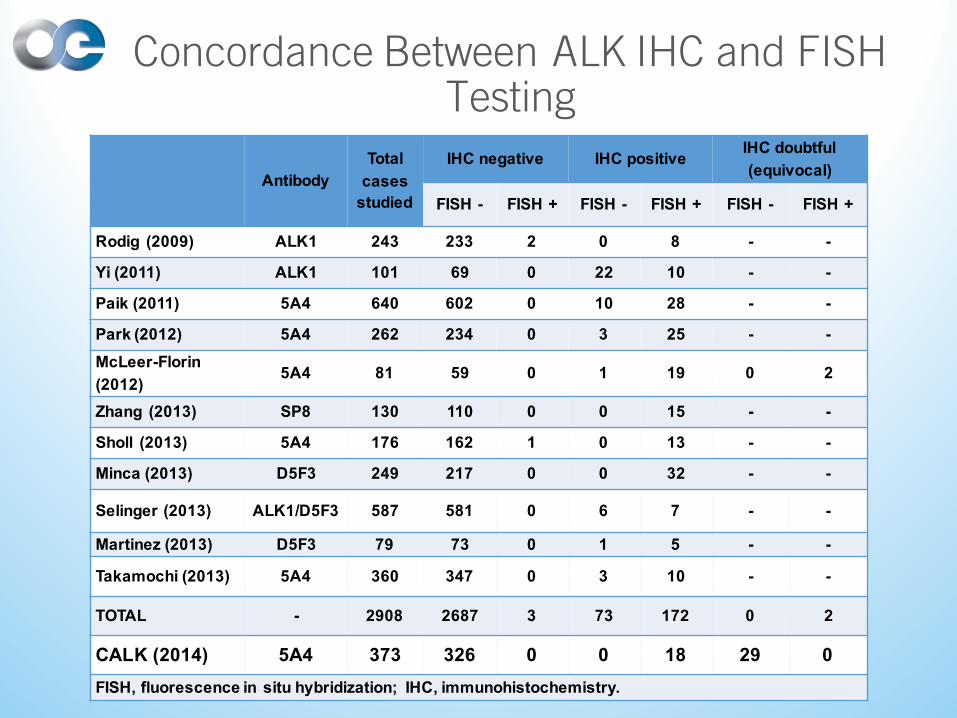
AntibodyTotal
cases studied
IHC negative IHC positive IHC doubtful (equivocal)
FISH - FISH + FISH - FISH + FISH - FISH +
Rodig (2009) ALK1 243 233 2 0 8 - -
Yi (2011) ALK1 101 69 0 22 10 - -
Paik (2011) 5A4 640 602 0 10 28 - -
Park (2012) 5A4 262 234 0 3 25 - -McLeer-Florin (2012)
5A4 81 59 0 1 19 0 2
Zhang (2013) SP8 130 110 0 0 15 - -
Sholl (2013) 5A4 176 162 1 0 13 - -
Minca (2013) D5F3 249 217 0 0 32 - -
Selinger (2013) ALK1/D5F3 587 581 0 6 7 - -
Martinez (2013) D5F3 79 73 0 1 5 - -
Takamochi (2013) 5A4 360 347 0 3 10 - -
TOTAL - 2908 2687 3 73 172 0 2
CALK (2014) 5A4 373 326 0 0 18 29 0FISH, fluorescence in situ hybridization; IHC, immunohistochemistry.
Concordance Between ALK IHC and FISH Testing


Current EGFR Testing Program
Physician
Request Testing for First line Rx with
gefitinib Holding Lab
Testing Lab
Prepare sample and ship to testing lab
Complete EGFR test and send results to
physician

Sample delivery to testing centre
Pathologist to QC the HE slides
Lab performance of the assay
Reporting of results
Turn Around Time
Test requested by Oncologist
1-2 days
7-10 days
Total: 10-21 days(average 14 days)
1-7 days
1-2 daysPrepare HE &
unstained section
Macro-dissectionDNA isolation
Mutation assay
Sample delivery to testing centre
Pathologist to QC the HE slides
Lab performance of the assay
Reporting of results
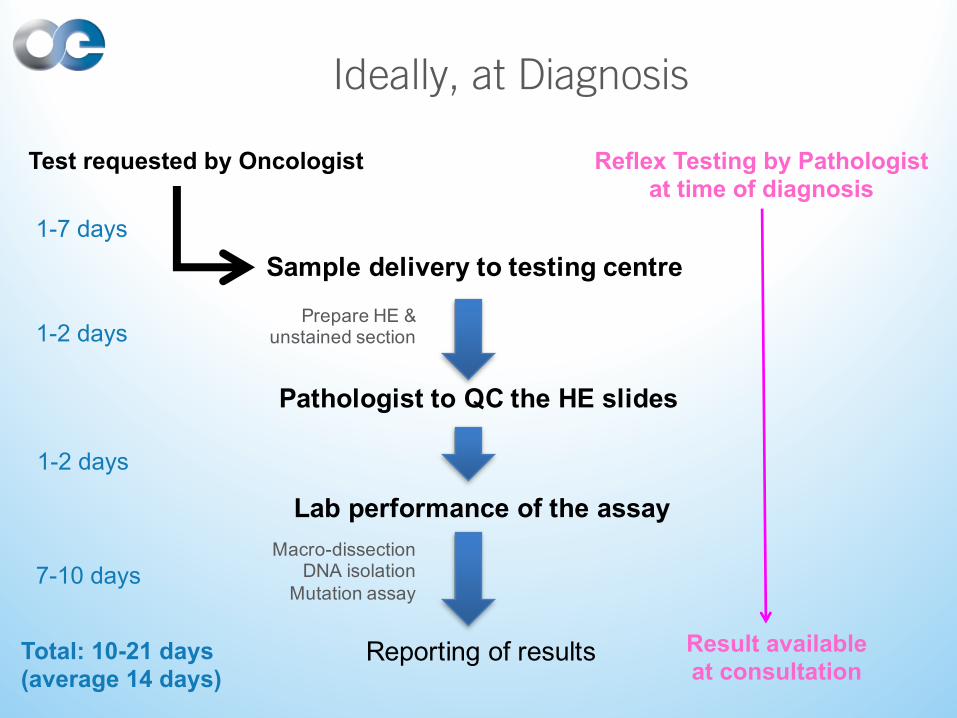
Ideally, at Diagnosis
Test requested by Oncologist
1-2 days
7-10 days
Total: 10-21 days(average 14 days)
1-7 days
Reflex Testing by Pathologist at time of diagnosis
Result available at consultation
1-2 daysPrepare HE &
unstained section
Macro-dissectionDNA isolation
Mutation assay

Next Generation Testing:High Throughput and Multiplex Platforms
• Mass spectrometry
(Sequenom)
• SNaPShot multiplex PCR (Applied Biosystems)
• Next Gen Sequencing: MiSeq, HiSeq, Ion Torrent, etc.

Next Generation Testing: Plasma circulating tumour cells and ctDNA
CTC = circulating tumour cell Haber & Velculescu. Cancer Disc June 2014

Where to Test?
Accredited clinical laboratory using validated assays!






























