Embed Size (px)
Citation preview

R E S EARCH ART I C L E
CANCER IMAG ING
http://stm.sciencem
Dow
nloaded from
A mouse-human phase 1 co-clinical trial of aprotease-activated fluorescent probe for imaging cancerMelodi Javid Whitley,1,2 Diana M. Cardona,3 Alexander L. Lazarides,4 Ivan Spasojevic,5,6
Jorge M. Ferrer,7 Joan Cahill,8 Chang-Lung Lee,8 Matija Snuderl,9* Dan G. Blazer III,10
E. Shelley Hwang,10 Rachel A. Greenup,10 Paul J. Mosca,10 Jeffrey K. Mito,1,2 Kyle C. Cuneo,8
Nicole A. Larrier,8 Erin K. O’Reilly,11 Richard F. Riedel,5 William C. Eward,12 David B. Strasfeld,7
Dai Fukumura,9 Rakesh K. Jain,9 W. David Lee,7 Linda G. Griffith,13 Moungi G. Bawendi,14
David G. Kirsch,1,8†‡ Brian E. Brigman12‡
Local recurrence is a common cause of treatment failure for patients with solid tumors. Intraoperative detectionof microscopic residual cancer in the tumor bed could be used to decrease the risk of a positive surgical margin,reduce rates of reexcision, and tailor adjuvant therapy. We used a protease-activated fluorescent imaging probe,LUM015, to detect cancer in vivo in a mouse model of soft tissue sarcoma (STS) and ex vivo in a first-in-humanphase 1 clinical trial. In mice, intravenous injection of LUM015 labeled tumor cells, and residual fluorescencewithin the tumor bed predicted local recurrence. In 15 patients with STS or breast cancer, intravenous injectionof LUM015 before surgery was well tolerated. Imaging of resected human tissues showed that fluorescence fromtumor was significantly higher than fluorescence from normal tissues. LUM015 biodistribution, pharmacokineticprofiles, and metabolism were similar in mouse and human subjects. Tissue concentrations of LUM015 and itsmetabolites, including fluorescently labeled lysine, demonstrated that LUM015 is selectively distributed to tu-mors where it is activated by proteases. Experiments in mice with a constitutively active PEGylated fluorescentimaging probe support a model where tumor-selective probe distribution is a determinant of increased fluores-cence in cancer. These co-clinical studies suggest that the tumor specificity of protease-activated imaging probes,such as LUM015, is dependent on both biodistribution and enzyme activity. Our first-in-human data support futureclinical trials of LUM015 and other protease-sensitive probes.
ag.o
by guest on November 1, 202
rg/
INTRODUCTIONSurgical resection is the primary treatment modality for most solid tu-mors diagnosed beforemetastatic spread. In patients with soft tissue sar-coma (STS) of the extremity and breast cancer, organ-sparing surgeryalone prevents local recurrence in about two-thirds of patients (1–3). Lo-cal recurrence is due to residual cancer in the tumor bed, the risk ofwhich is inferred by histopathological evaluation for the presence of tu-mor cells on the surface of the excised margin (1, 4). Intraoperative fro-zen margin assessment is limited by time and prone to sampling error,leading to false-negative results in up to 23% of cases (5). An intra-
1Department of Pharmacology and Cancer Biology, Duke University Medical Center,Durham, NC 27710, USA. 2Medical Science Training Program, Duke University MedicalCenter, Durham, NC 27710, USA. 3Department of Pathology, Duke University MedicalCenter, Durham, NC 27710, USA. 4School of Medicine, Duke University Medical Center,Durham, NC 27710, USA. 5Department of Medicine, Duke University Medical Center,Durham, NC 27710, USA. 6PK/PD Core Laboratory, Duke Cancer Institute, DukeUniversity Medical Center, Durham, NC 27710, USA. 7Lumicell Inc., Wellesley, MA02481, USA. 8Department of Radiation Oncology, Duke University Medical Center,Durham, NC 27710, USA. 9Edwin L. Steele Laboratory, Department of RadiationOncology, Massachusetts General Hospital and Harvard Medical School, Boston, MA02114, USA. 10Department of Surgery, Duke University Medical Center, Durham, NC27710, USA. 11Duke Translational Medicine Institute, Regulatory Affairs Group, DukeUniversity Medical Center, NC 27710, USA. 12Department of Orthopaedic Surgery,Duke University Medical Center, Durham, NC 27710, USA. 13Department of BiologicalEngineering, Massachusetts Institute of Technology, Cambridge, MA 02142, USA.14Department of Chemistry, Massachusetts Institute of Technology, Cambridge, MA02142, USA.*Present address: Department of Pathology, NYU Langone Medical Center, New York,NY 10016, USA.†Corresponding author. E-mail: [email protected]‡Co-senior authors.
www.Scie
0
operative technique to accurately identify microscopic residual diseasewithin the tumor bed could be used to decrease the risk of a positive sur-gical margin, reduce the rate of re-resection, and tailor adjuvant therapy.
Emerging approaches to detect microscopic residual disease withinthe tumor bed include spectroscopy and optical imaging. Raman spec-troscopy measures the scattering properties of tissues, and tumor-targeted Raman reporters like gold nanostars can provide excellenttumor-to-normal tissue contrast (6, 7). Fluorescence optical imagingresolvesmolecular features, and nonspecific fluorescent imaging probessuch as methylene blue and indocyanine green provide contrast be-tween tumor and normal tissues and are currently in clinical trials.Themean tumor-to-background ratio (TBR) with these imaging agentsranges from 1.2 to 8.5 in mouse and human studies (8–10). To increasethe TBR, targeted (11–13) and activatable fluorescent probes havealso been developed. Activatable probes are optically silent until cleavedby proteases that are overexpressed by tumors, such as cathepsinproteases (14–16). In a previous study, we used the LSL-KrasG12D/+;p53flox/flox (KP) and Braf Ca/+; p53flox/flox (BP) mouse models of STSand a wide field-of-view imaging system to detect cathepsin-activatedfluorescence in tumor cells (17). Residual fluorescence in the tumor bedcorrelated with local recurrence, and image-guided surgery improvedoutcomes for mice. This intraoperative imaging system has also beenused in canine patients with spontaneous tumors (18).
Although protease-activated probes have shown promise preclini-cally, translation has been hindered by suboptimal preclinical modelsand limited funding for probe synthesis, toxicity studies, and phase1 clinical trials. We were able to overcome these hurdles, among others,to translate protease-activated probes into the operating room. Here, we
nceTranslationalMedicine.org 6 January 2016 Vol 8 Issue 320 320ra4 1

R E S EARCH ART I C L E
Dow
specifically explored the use of LUM015, anovel PEGylated protease-activated far-redfluorescent imaging probe. Preclinical tox-icity studies of LUM015 were performedin rats and indicated a wide margin ofsafety. We report here a first-in-humanphase 1 trial of LUM015 to test the safetyof the probe in patients undergoing sur-gery for STS and breast cancer as well asLUM015 pharmacokinetics. Co-clinicalstudies inmicewere conducted to optimizethe dose and timing of LUM015 adminis-tration and to investigate the in vivomech-anisms of tumor specificity. Our studiessupport further clinical development ofLUM015 in clinical trials with intraopera-tive imaging of the tumor bed.
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
nloaded from
RESULTS
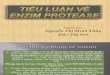
LUM015 forms two differentoptically active metabolitesLUM015 consists of a commercially availa-ble fluorescence quencher molecule (QSY21)attached through a GGRK peptide to a20-kD polyethylene glycol (PEG) and a Cy5fluorophore (Fig. 1A). LUM015 is optical-ly inactive, but upon proteolytic cleavageby cathepsins K, L, and S (and, to someextent, B), the quencher is released (frag-ment 1) to create the optically active frag-ment 2 (Fig. 1B). Additional cleavage ofLUM015 or fragment 2 yields the opti-cally active fragment 3 (Fig. 1A). High-performance liquid chromatography (HPLC)revealed distinct peaks for fragments 2and 3 (Fig. 1C). The low-level fluorescencedetected from LUM015 itself is from ~1%Cy5 fluorescence not absorbed by thequencher. Patient plasma samples showeda strong peak corresponding to fragment3 as well as a smaller peak representingfragment 2 and uncleaved LUM015 (Fig.1D), and human plasma profiles showedfragment 3 levels increasing during the first8 hours after injection followed by clear-ance at a slower rate (Fig. 1E).
We then injected mice with and with-out primary STS tumors with LUM015andmeasured [fragment 3]plasma over timeafter administration. At 1 hour, the con-centration of fragment 3 in plasma peakedin mice with tumors, but by 2 hours, plas-ma levels were similar to mice with notumor, suggesting that fragment 3 wasappreciably produced in nontumor tissues(Fig. 1F). In tumor tissue,most of LUM015
QSY21
Cy5
PEG QSY21NH
Lys
H2NO
NHO
Cy5
PEG
Lys
H2NO
NHO
Cy5
OH
LUM015Optically inactive
Fragment 1Optically inactive
Fragment 2Optically active
Fragment 3Optically active
Proteolyticcleavage
A
B
Fragment 3Fragment 2
LUM015
C
D
E
F
P = 0.09
Fig. 1. Cy5-Lys is the major fluorescent LUM015 metabolite. (A) Expected LUM015 cleavage products:Fragment 1 contains the quencher QSY21, and optically active fragments 2 and 3 contain the Cy5 fluoro-
phore. (B) In vitro protease (0.5 mM) activation of LUM015 (5 mM). Fluorescence was measured at multipletime points with peak excitation at 650 nm and fluorescence emission collection at 675 nm (n = 6 replicatesper enzyme). (C andD) HPLC analysis of pure LUM015 (25 ng/ml), fragment 2 (25 ng/ml), and fragment 3(2.5 ng/ml) (C) and a representative patient plasma sample collected from patient 14 at 8 hours after intra-venous administration of LUM015 (1.5mg/kg) (D). (E and F) Plasma profiles of fragment 3 in three patients(E) and in tumor-bearing and non–tumor-bearing mice (n = 6 mice per group) (F) each injected withLUM015 (1.5 mg/kg). P value determined by unpaired t test.www.ScienceTranslationalMedicine.org 6 January 2016 Vol 8 Issue 320 320ra4 2

R E S EARCH ART I C L E
was metabolized, whereas in blood, muscle, liver, and kidney tissue,half or more of LUM015 remained uncleaved (fig. S1). In contrastto fragment 3 being the major metabolite after in vivo administrationof LUM015 to patients, fragment 2 was the predominant cleavageproduct in vitro.
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from
LUM015 fluorescently labels tumorcells in miceTo test the specificity of LUM015 fortumor cells, we administered LUM015(3.5 mg/kg) via tail vein injection into16 mice with primary STS in the lowerextremity. This dose of LUM015 was chosenon the basis of preclinical studies performedwith other protease-activatable probes inthe samemouse model (17). Six hours later,we resected the STS and normal musclefrom the contralateral leg. Fluorescenceimaging of the resected tissues revealeda mean tumor fluorescence that wasnearly fivefold higher than that of muscle(Fig. 2A). In a mouse model of breastcancer, LUM015 fluorescence was signif-icantly greater in tumor than in muscle(Fig. 2B).
Because tumors consist of cancer andstromal cells, we next investigated to whatextent LUM015 labeled these cells usingmice with tumors that express yellow flu-orescent protein (YFP). After 6 hours, tu-mors resected from mice injected withLUM015 had a significantly higher pro-portion of Cy5+ fluorescent cells comparedto control animals given saline (Fig. 2C).About 62% of the LUM015-labeled cellswere YFP+ tumor cells, and less than 10%wereCD11b+ tumor-associatedmonocytesandmacrophages (Fig. 2C), indicating thatmost Cy5-labeled cells were tumor cells.Polymerase chain reaction (PCR) genotyp-ing of genomic DNA from the Cy5+ cellsthatwereYFP−/CD11b− revealed thatmostof these cells were tumor cells, which acti-vated LUM015 but may have lost expres-sion of the YFP marker, mixed togetherwith some CD11b− stromal cells (fig. S2A).Conversely, in pure populations of YFP+/CD11b+ cells, the proportion of Cy5+ cellswas higher in the tumor cell populationthan in the monocyte population, but theefficiency of labeling in tumor cells wasabout 20% in mice (fig. S2).
Having demonstrated that LUM015fluorescently labels sarcoma cells, we nextused an autochthonous mouse model ofSTS with marginal resection to determineif residual fluorescence in the tumor bed af-ter surgical removal of the tumor predicted
www.Scie
local recurrence. Residual fluorescence within the tumor bed was de-termined intraoperatively as fluorescence exceeding 80% of theminimum signal from the excised tumor (fig. S3) (17). After imagingthe tumor bed, the surgical wound was closed, and the mice weremonitored for local recurrence–free survival. All mice positive for
A Muscle Sarcoma
Tumor cells
PBS LUM015Monocytes/macrophages
0.4 8.8
8.0
62
YFP
Cy5
YFPCD11
b
C
D
Muscle TumorB
Fig. 2. LUM015 fluorescentlylabels tumor cells in mousemodels of STS and breast can-cer. (A and B) Mean measuredfluorescence in primary sarco-ma (n = 16) (A) or orthotopicbreast cancer (n = 23) (B) andmuscle. P values determinedby unpaired t test. Representa-tive fluorescence images ofresected normal muscle andtumors are shown along withcorresponding hematoxylin andeosin (H&E) histology. Thesame contrast scale was applied
nceTranslationalMedicine.org 6 January 201
to both fluorescence images in each pair. Scale bars, 5 mm for fluorescence images; 500 mm for H&Eimages in (A); 100 mm for H&E images in (B). (C) Representative flow cytometric analysis of resected mousetumors expressing tumor cell–specific YFP after intravenous administration of phosphate-buffered saline(PBS) or LUM015 (3.5 mg/kg). Of the tumors frommice treated with LUM015, Cy5+ cells (red box, cells withfluorescence >2 × 102) and YFP+ tumor cells (yellow box) were sorted and quantified (nPBS = 2 mice,nLUM015 = 3 mice). In the Cy5+ cells, the proportions of YFP+ tumor cells and CD11b+ tumor–associatedmacrophages were further quantified (n = 3 mice). P values were determined by unpaired t test. (D) Thecorrelation between residual fluorescence within the sarcoma tumor bed measured before wound closureand local recurrence–free survival in mice. P value determined by log-rank test.
6 Vol 8 Issue 320 320ra4 3

R E S EARCH ART I C L E
http://stm.s
Dow
nloaded from
residual fluorescence at the time of surgery developed local recur-rence of their tumors within 70 days of surgery. In comparison, onlyone-third of the mice without residual fluorescence in the tumorbed experienced local recurrence within 200 total days of follow-up(Fig. 2D).
LUM015 is safe in humansAfter demonstrating that LUM015 selectively labeled sarcoma and breastcancer in mice, we performed a first-in-human phase 1 clinical trial ofLUM015. This trial enrolled 15 patients, 12 with STS and 3 with invasiveductal carcinoma (IDC) of the breast. Four of the 12 STS patients hadundifferentiated pleomorphic sarcoma (UPS), and the other eightrepresented several different STS subtypes. The tumor subtypes,grade, size, and anatomic locations are described in Table 1. LUM015was administered to six patients at a 0.5 mg/kg dose, six patients at a1.0 mg/kg dose, and three patients at a 1.5 mg/kg dose, according to amodified 3 + 3 design (NCT01626066). These human doses werechosen on the basis of the estimated effective dose of 3.5 mg/kg inmice, which often corresponds to a lower effective dose in humansowing to differences in the ratio of body surface area to bodyweight (19).Surgical removal of the tumors immediately followed by ex vivo fluo-rescence imaging of the resected specimens was done either the sameday as probe injection (at ~6 hours) or the following day (at ~30 hours).Tissue samples imaged ex vivowere biopsied for subsequent histologicalanalysis.
www.Scie
LUM015 was well tolerated by study subjects, and no adverse phar-macological activity or hypersensitivity reactions occurred during thestudy (table S1). All subjects experienced green chromaturia, whichwas expected based on the blue color of LUM015. Two sarcoma patientshadwound healing complications, which is within the expected range forthis patient population and not considered related to LUM015; both ofthese patients had received preoperative radiation therapy, which isknown to delay wound healing in STS patients (20). Patient 11 experi-enced a minor transient elevation of liver function tests for aspartateaminotransferase at 59 U/liter (normal range, 15 to 41) and alaninetransaminase at 58 mg/dl (normal female range, 14 to 54) 8 hours afterLUM015 administration, which was determined to be only possibly re-lated to the investigational probe and therefore did notmeet the criteriafor adverse pharmacological activity, as defined by the clinical protocol(table S2).Notably, the tissue imaged for patient 10 did not include tumor,and therefore, this patient was excluded from tumor tissue analyses.
Co-clinical studies in mice and humans showsimilar pharmacokineticsBlood samples were collected frommice and patients at regular intervalsafter intravenous administration of LUM015, and liquid chromatography–tandemmass spectrometry (LC-MS/MS)wasused tomeasure [LUM015]plasma
at these time points. Summary pharmacokinetic parameters suggestinga linear dose response in humans are reported in fig. S4. Plasma clear-ance profiles for mice and humans injected with a 1.5 mg/kg dose of
ciencemag.org
Table 1. Enrolled patients in first-in-human phase 1 clinical trial ofLUM015. Imaging time was measured as the number of hours elapsedbetween LUM015 injection and imaging of the resected tissues with the
LUM device. Histological descriptors are based on clinical surgical pathol-ogy reports. ER, estrogen receptor; PR, progesterone receptor; RT, radia-tion therapy.
by gu/
Patient
e
LUM015 dose(mg/kg)
Imaging time(hours)
Tumor type
n
Tumorgrade
ceTranslationa
Tumor volume(cm3)
lMedicine.org 6 Jan
Neoadjuvanttherapy
uary 2016 Vol 8
Tumor site
st on
1 0.5 30.1N
Well-differentiatedliposarcoma
Low
10.5 × 8.5 × 6.2 None Retroperitonealovem
2 0.5 28.5 UPS High 13.5 × 8.3 × 6.5 25 × 2 Gy RT Thighbe
3 0.5 28.5 UPS High 18.0 × 9.0 × 6.0 25 × 2 Gy RT Upper armr 1,
4 1.0 30.920
Malignant peripheral nervesheath tumor
Intermediate
2.5 × 1.6 × 1.5 25 × 2 Gy RT Upper arm20
5 1.0 26.9 Myxoinflammatoryfibroblasticsarcoma/hemosideroticfibrolipomatous tumor
Low
31.0 × 20.0 × 1.3 None Leg6
1.0 26.5 UPS High 3.6 × 2.9 × 1.2 None Upper arm7
1.0 4.8 Metastatic clear cellsarcomaHigh
4.0 × 2.9 × 2.8 None Inguinal lymph node8
1.0 7.2 UPS High 13.0 × 6.5 × 7.1 25 × 2 Gy RT Upper arm9
1.0 8.3 IDC: ER+/PR−/Her2+ High 3.7 None Breast10
1.5 9.6 IDC: ER+/PR+/Her2− Intermediate 7.5 × 2.5 ×1.5 None Breast11
1.5 5.1 Metastatic spindle cellsarcomaLow
0.9 None Thigh12
1.5 7.3 Myxofibrosarcoma High 11.0 × 6.5 × 6.5 None Thigh13
0.5 9.6 Synovial sarcoma High 20.0 × 12.0 × 6.0 25 × 2 Gy RT Thigh14
0.5 8.5 Spindle cell sarcoma High 7.5 25 × 2 Gy RT Thigh15
0.5 7.3 IDC: ER+, PR+, Her2− High 2.4 × 1.6 × 1.4 None BreastIssue 320 320ra4 4

R E S EARCH ART I C L E
byhttp://stm
.sciencemag.org/
Dow
nloaded from
LUM015 were similar (Fig. 3A). Tumor fluorescence in the first sixhumans imaged at 30 hours was lower than fluorescence measured inmice at 6 hours, but in both mice and humans, absolute tumor fluores-cence was significantly higher when measured 6 hours after LUM015administration compared to 30 hours (Fig. 3B). In contrast, we did notfind a significant effect of imaging time on the tumor-to-normal tissuefluorescence ratio (T/N) in humans ormice (Fig. 3C). Thus, the imagingtime point was shortened to 6 hours after LUM015 administration forthe remainder of the phase 1 trial. Furthermore, at 6 hours, the fluores-cence ratio (tumor/normal) measured in humans administered thehighest LUM015 dose (1.5 mg/kg) was significantly higher than thosemeasured in the two lower-dose cohorts (Fig. 3D).
LUM015 fluorescence is tumor-selective in STS and breastcancer patientsTo determine if preoperative administration of LUM015 results intumor-specific fluorescence, we compared the absolute fluorescence inthe tumor with the absolute fluorescence in adjacent normal tissue fromall patients (Table 1), except for patient 10. The presence or absence ofcancer in the samples was confirmed by subsequent histological analysisby a pathologist blinded to the imaging data (table S3). Normal muscle,adipose, or breast tissue from the margin of tissue resected around thetumor was used for the normal tissue comparison unless otherwise notedin table S3. Three representative examples of ex vivo imaging from apatient with a high-grade UPS of the thigh, a patient with a high-grademyxofibrosarcoma of the thigh, and a patient with a high-grade IDC ofthe breast are shown (Fig. 4, A to C). UPS is the most common type ofSTS in the trial and is phenotypically most similar to the mouse modelin our preclinical studies. Myxofibrosarcoma is locally aggressive, andcomplete resections are challenging; thus, these patientsmay particular-ly benefit from this intraoperative imaging technology.
www.Scie
For each patient, we imaged one to six tumor and normal tissuesites that were histologically confirmed, and the mean fluorescencevalue is reported. Overall, tumor fluorescence was significantly higherthan matched normal tissue fluorescence with a mean tumor/normalfluorescence ratio of 4.1 (Fig. 4D). The tumor/normal fluorescence ratiowas less than or equal to 1 in two of the patients, both of whom wereimaged at the 30-hour imaging time point and had low-grade sarcomas(well-differentiated liposarcoma and myxoinflammatory fibroblasticsarcoma/hemosiderotic fibrolipomatous tumor). Furthermore, wefound that across all patients, the means of absolute tumor, muscle,and adipose fluorescence values were significantly different (Fig. 4E).
Biodistribution and protease activation contribute totumor fluorescenceAfter determining that fragment 3—with Cy5, no PEG—was themajorLUM015metabolite in human plasma (Fig. 1), wemeasured the con-centrations of both fragments and intact LUM015 in human tissues(table S4) and in a cohort of 18mice injectedwith LUM015 (1.5mg/kg).At 6 hours, [fragment 3]tumor correlated significantly with tumor fluo-rescence in mice and in humans (Fig. 5A). A similar analysis of frag-ment 2 showed a weaker correlation with tissue fluorescence (Fig. 5A).To measure the contribution of proteolytic probe activation to tumor-selective fluorescence, we calculated the fraction of LUM015 and itsme-tabolites that were present in the optically active state for each mousesample. In themouse cohort, sarcomas had a fraction of activated probe(FAP)of 0.38,whichwas about 50%higher thannormalmuscle (Fig. 5B).In human tumor samples imaged at 6 hours, tumors had a FAP of 0.26,whichwas about 60%higher compared to normal tissues (Fig. 5B), butthis difference did not reach statistical significance, even at 30 hours.
In the mouse STS cohort and the human STS patients imaged at6 hourswith normalmuscle available for comparison (patients 8, 11, 12,
nceTranslationalMedicine.org
guest on Novem
ber 1, 2020
13, and 14; table S3), tumor/muscle fluo-rescence ratioswere correlatedwith the cor-responding activation ratio; however, thiscorrelation was significant only for themouse samples (Fig. 5C). In an analysis in-clusive of all patients, there was a significantcorrelation between fluorescence and acti-vation (fig. S5A). Tomeasure the contribu-tion of biodistribution to tumor-selectivefluorescence, the total concentration ofLUM015 and its cleavage products, [totalprobe (TP)], was determined for each sam-ple. In both the mouse and human STScohorts, sarcomas had a [TP] that wasgreater than normalmuscle (Fig. 5D). Ad-ditionally, [TP] was higher in human tu-mors imaged at 6 hours when comparedto tumors imaged at 30 hours (fig. S5B).Furthermore, we found that tissue fluores-cence and [TP] had a significant positivecorrelation in the mouse cohort, the hu-man STS cohort, and the overall humandata set (Fig. 5, E and F).
To image tumors with a probe that doesnot require protease activation, we injectedSTS-bearing mice with either LUM015 orLUM033, a constitutively active fluorescent
A B
D
C
Fig. 3. Comparative LUM015pharmacokinetics inmouseandhuman subjects. (A) LUM015 plasma clearance profile inmouse andhuman subjects administered a 1.5mg/kg dose ofLUM015. [LUM015]plasma is given as a fraction of the maxi-mum concentration and shown on a log scale. (B) Tumor flu-orescence in patients andmice at the 6- and 30-hour imagingtime points (n = 5mice and 3 humans per dose cohort). P =0.02 for imaging time, as determined by two-way analysisof variance (ANOVA). (C) Tumor/normal fluorescence ratioin mice and humans at the 6- and 30-hour imaging timepoints. P = 0.6 for imaging time, as determined by two-way ANOVA. (D) Tumor/normal fluorescence ratio measuredin humans andmice by dose (nmouse-1.5, 3.5 = 5; nhuman-0.5, 1.0 = 3;nhuman-1.5 = 2). P values for dose cohort comparisons deter-
mined by Tukey’s multiple comparisons test. P = 0.02 for dose effect on human subset determined byone-way ANOVA.
6 January 2016 Vol 8 Issue 320 320ra4 5

R E S EARCH ART I C L E
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from
imaging probe identical to fragment 2 (also from Lumicell Inc.). Six hoursafter injection, resected tumors had a tumor/normal fluorescence ratiotwofold higher for LUM015 than for LUM033 (Fig. 5G). Therefore,protease activation may serve to double the level of tumor-to-normalcontrast that is achieved by tumor-selective biodistribution alone. Thesefindings suggest that tumor-selective distribution of LUM015 is a criticaldeterminant of T/N, which is further enhanced by tumor-specific pro-tease activation.
Because biodistribution is one of two major determinants of tumor-specific fluorescence measured after administration of LUM015, we usedimmunofluorescence and immunohistochemistry to further examine thedistribution of LUM015 to tumor and normal tissues. As a control for
www.ScienceTranslationalMedicine.org
immunofluorescence, we used formalin-fixed paraffin-embedded (FFPE) sectionsof tumor tissue from human sarcoma pa-tients not injected with LUM015. Patientswho had been injected with LUM015showed a positive signal for PEG, whereasthe control tissues did not (Fig. 6A). In abreast cancer sample from patient 15 thatcontained both areas of tumor and adja-cent normal tissue, PEG signal localizedto areas of tumor, with less intense stainingin normal tissue (Fig. 6B). Areas adjacentto tumor containing a lymphocytic infil-trate were also negative for PEG staining.The amount of PEG staining was signifi-cantly less in normalmuscle and breast tis-sues compared to sarcomas andbreast cancer,respectively (Fig. 6,CandD).These results forPEG staining, together with the quantifica-tion of LUM015 and its metabolites, sug-gest that tumor-selective distribution ofLUM015may serve to delineate the tumormarginwhile protease activation intensifiesthe contrast between tumor and normaltissue types for intraoperative imaging.
DISCUSSION
There is an unmet need for a real-timemethod to determine the presence of mi-croscopic residual cancer within the tu-mor bed at the time of surgery, whichcould reduce the need for re-resection,lower the rates of local recurrence, andper-sonalize adjuvant therapy. A particularlyattractive approach to detect residual dis-ease is fluorescence imaging because it canbe functionally and/or molecularly targetedand provide cellular resolution with pene-tration depths of up to several millimeters(11). Protease-activated fluorescent imag-ing probes were first introduced more than15 years ago to provide optical contrast be-tween tumor andnormal tissues (14, 21–23).Many of these probes have been tested in
preclinical models. This is the first study to use these probes to imagehuman cancers and investigate the relative importance of protease activa-tionversusbiodistribution for achieving tumor-to-normal tissue contrast.
We show here that the PEGylated, protease-activated probe LUM015specifically labels tumors in amousemodel of STS aswell as inhumanswithSTS and breast cancer. Flow cytometric studies of tumors from LUM015-injected mice showed that most fluorescently labeled cells were tumorcells, and less than 1/10 were tumor-associated monocytes and macro-phages. The labeling of tumor-associated macrophages likely occurs be-cause these cells also express high levels of proteases (24), and theintraoperative identification and removal of these cells may, in fact, bebeneficial to patients because these cells are associated with tumor
T
M
MRI Gross resectionarcoma Normal muscleA
MRI Gross resectionNormal muscleB
TN
Mammogram Gross resectionInvasive ductal carcinoma Normal breastC
D E
UPS
IDC
Other STS
T
M
Fig. 4. Tumor-selective fluorescence in patients receiving intravenous LUM015 before resection.(A to C) Representative human subjects with UPS of the thigh (A, patient 2), myxofibrosarcoma of the
thigh (B, patient 12), and IDC of the breast (C, patient 9). From left to right: gadolinium-enhancedmagnetic resonance imaging, gross tissue resection containing tumor (T) and normal muscle (M), H&Ehistology of imaged tumor tissue, fluorescence image of tumor tissue obtained with the LUM device,H&E staining of imaged muscle, fluorescence image of muscle obtained with the LUM device. (D) Tumortissue fluorescence and fluorescence measured from adjacent normal tissue in the same patient (n = 14).P value determined by paired t test. (E) Distribution of tumor, muscle, and adipose tissue fluorescenceacross all patients (ntumor = 14, nmuscle = 10, nadipose = 11). P = 0.04 for tissue type effect determined byone-way ANOVA. P values for tumor to muscle and adipose comparison determined by unpaired t test.6 January 2016 Vol 8 Issue 320 320ra4 6

R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.org
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from
Fac[fvsth[f[fFtaa3pmmnthte[fatis(Emnstiom6oP
A
B
C D
E
G
F
ig. 5. Tumor-selective distribution andctivation of LUM015. (A) Tumor fluores-
ence as a function of [fragment 3]tumor andragment 2]tumor (nhuman = 14, nmouse = 16). PaluesdeterminedbyF teston the linear regres-ionmodel. (B) The FAPwas determined usinge following equation: ([fragment 2 (nM)]tissue +ragment 3 (nM)]tissue)/([LUM015 (nM)]tissue +ragment 2 (nM)]tissue + [fragment 3 (nM)]tissue).AP data are shown for muscle and tumorissue samples from human (n = 5, patients 8nd 11 to 14) and mouse (n = 18) STS subjectsnd from all human subjects imaged at 6 and0 hours (n = 14). P values determined by un-aired t test. (C) Correlation between the tumor:uscle fluorescence ratio and the FAP ratio in theouse and human STS cohorts (nhuman = 5,mouse = 16). P value determined by F test one linear regression model. (D) The [TP] in theissue (innM)wasdeterminedusingthe followingquation: [LUM015]tissue + [fragment 2]tissue +ragment 3]tissue. [TP] data are shown for musclend tumor tissue samples fromhuman (n=5, pa-ents 8 and 11 to 14) and mouse (n = 18) STSubjects. P values determined by unpaired t test.and F) Tumor fluorescence versus [TP] in theouse and human STS cohorts (nhuman = 5,mouse = 16) (E) and in tumor andnormal tissueamples from all human subjects (n = 14 perssue type) (F). P values determined by F testn the linear regression models. (G) Tumor/uscle fluorescence ratios measured in micehours after injection with equimolar amountsf LUM015or LUM033 (nLUM015=11,nLUM033=9).value determined by unpaired t test.6 January 2016 Vol 8 Issue 320 320ra4 7

R E S EARCH ART I C L E
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from
progression and metastasis (25, 26). In mice injected with LUM015,residual fluorescence within the tumor bed was highly predictive oflocal recurrence, suggesting that this intraoperative imaging system couldbe useful to guide surgery and tailor adjuvant therapy.
In a first-in-human phase 1 trial in patients undergoing surgical re-section of STS or breast cancer, we found that LUM015 is safe and well-tolerated at a dose that allows for detection of tumor-specific fluorescence.We observed that the plasma clearance profile of LUM015 in humansand mice is similar. On the basis of allometric scaling, we expectedthat the clearance rate would be significantly slower in humans (27, 28)so that a greater interval of time between LUM015 administration andtumor resection would be required to allow for optimal tumor-to-normaltissue contrast. Our results are consistent with the findings that stan-dard allometric scaling does not accurately predict human pharmaco-kinetic parameters for PEGylated compounds (29). On the basis ofthis information, we modified the phase 1 clinical trial to include im-aging at the 6-hour time point, resulting in higher tumor fluorescencein human cancers than imaging at 30 hours.
www.ScienceTranslationalMedicine.org
Consistent with data from mice anddogs (18),whenpatientswith STSorbreastcancer were injected with LUM015 beforesurgery, we found tumor tissue fluores-cence measured ex vivo to be significantlyhigher than fluorescence measured fromadjacent normal tissues. It is important tonote that this study included patients withboth sarcoma and breast cancer, and thatwithin these tumors, different subtypeswere included. A T/N of greater than1 was measured in 12 of 14 patients, in-dicating that LUM015 may be effectivefor fluorescent labeling of many differ-ent types of cancer. However, the humanT/N reported in this study were mea-sured in ex vivo bulk tissue, and futureclinical trials with LUM015 with in vivotumor bed imaging will be necessary todefine a clinically meaningful T/N cut-off. Nevertheless, the in vivo tumor bedimaging inourmouse experiments suggeststhat LUM015 can provide a sufficient T/Nfor detecting residual cancer.
Tissue measurements of LUM015,PEG, and its metabolites showed that se-lective biodistribution in tumors was animportant factor in tumor-selective imag-ing. Tumor-specific protease activationserves to enhance the contrast that is es-tablished with differential distribution, sug-gesting that by targeting the tumor throughboth mechanisms simultaneously, a largertumor-to-normalcontrast isachieved.How-ever, in mice, we found that the genera-tion of fragments in vivo did not requirethe presence of cancer and could be formedin isolated blood, muscle, liver, and kidney.This suggests that protease activation doesnot fully account for the tumor/normal
ratio, and instead is established in part by tumor-selective accumulationthrough the enhanced permeability and retention effect.
This study shows that preoperative administration of LUM015 topatients with sarcoma or breast cancer results in tumor-specific flu-orescence that can be detected upon ex vivo imaging of resected tissues.However, future clinical studies will be needed to measure fluorescencein vivo, specifically residual cancer cells at the tumor margins. We re-port in vivo imaging data frommice and show that intraoperative imag-ing with LUM015 predicts local recurrence with high specificity. However,somemicewithnegative residual fluorescence did develop local recurrence.Therefore, it will be necessary to optimize fluorescence thresholdingmethods to increase the sensitivity of the systemwhilemaintaining highspecificity.
This work presents a first-in-human phase 1 clinical trial of an in-travenously administered, protease-activated fluorescent intraoperativeimaging probe.We have shown that LUM015 is safe for use in humansand generates tumor-specific fluorescence. These studies support futureclinical trials of LUM015 using intraoperative imaging of the tumor bed
A +LUM015−LUM015
B
Normal muscle Sarcoma
Normal breast Invasive ductal carcinoma
C D
UPS IDC Other STS
TT
N
PEGHoechst
PEGHoechst
Fig. 6. Visualizing tumor-selective LUM015 biodistribution. (A) PEG immunofluorescence of humantumor samples from LUM015-injected patients (+LUM015 representative image from patient 2) and from
uninjected patients (−LUM015 representative image from n = 3 patients) with UPS. (B) PEG immuno-fluorescence of margin tissue from LUM015-injected breast cancer patient 15. T, tumor tissue; N, normalbreast tissue. The corresponding H&E histology is shown. (C) Immunohistochemistry for PEG in normalmuscle tissue, normal breast tissue, and tumor tissue. Representative images of normal muscle and UPS(patient 2) as well as normal breast and IDC (patient 9). (D) Quantification of PEG staining intensity in tumorsand normal tissues (n = 14 per tissue type; 1 tumor and 1 normal tissue sample from each patient exceptpatient 10). P value determined by Mann-Whitney test.6 January 2016 Vol 8 Issue 320 320ra4 8

R E S EARCH ART I C L E
and comparing imaging results with histopathology. A feasibility studyof intraoperative imaging with the LUM system has recently started forbreast cancer patients (NCT02438358), but it may be possible to use theprobe for patients with other cancers, such as sarcoma (as demonstratedin mice) and gastrointestinal cancers. Our co-clinical studies in miceand humans reveal that pharmacokinetic and pharmacodynamic param-eters are conserved across species, which may aid in the translation ofother preclinical imaging agents for human use.
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from
MATERIALS AND METHODS
Co-clinical study designIn this co-clinical study, data regarding the pharmacokinetics, specificity,and mechanism of action of LUM015 were gathered in both mice andhumans. Preclinical studies in themice provided justification for a phase1 clinical trial in humans. During the clinical trial, parallel mouse studieswere conducted to further explore clinical observations regardingLUM015 pharmacokinetics and the mechanism of tumor-selective flu-orescence. The objective of the controlled laboratory experiments was touse a primary mouse model of STS and orthotopic models of breastcancer to investigate the in vivo activity of LUM015 and explore themechanism of LUM015 distribution and activation in vivo.
All animal studies were performed in accordance with protocolsapproved by the Duke University and Massachusetts General HospitalInstitutional Animal Care and Use Committees. Sample sizes wereselected before initiating the study based on previous intraoperative im-aging studies conducted in the laboratory (17), and power calculationswere performed as described previously (30). Data collection wasstopped if a smaller sample size achieved statistical significance. Nooutliers were excluded in this study. The mice in this study were notrandomized to their treatments and were selected on the basis of avail-ability. The investigators were not blinded when performing tissue flu-orescence measurements.
The primary objective of the single institution, open-label, nonran-domized phase 1 trial (NCT01626066) was to determine a safe andrecommended dose of LUM015 that labels tumors. Secondary objec-tives included obtaining ex vivo imaging information of the tumor andany adjacent normal tissue as well as collecting pharmacokinetic/pharmacodynamic information. Patients with the diagnosis of STSor breast cancer scheduled for tumor resectionwere included. Patientstreated with neoadjuvant radiation therapy were included in the studybased on our previous data that radiation therapy does not alter thefluorescence from protease-activated imaging probes in a mouse modelof STS (31). The sample sizewas determined on the basis of amodified3 + 3 dose escalation design to provide information on the relationshipbetween dose and fluorescence signal while observing patients foradverse pharmacological activity. No outliers were excluded in thisstudy. Informed consent was obtained from each patient, and thestudy was approved by the Duke University School of Medicine andCopernicus Institutional Review Boards. The study was also run underan Investigational New Drug application filed with the U.S. Food andDrug Administration. A safety monitoring committee was formed toprotect the rights, safety, and welfare of participants, and additionalmonitoring was done by the Duke Cancer Institute (DCI) Safety Over-sight Committee.
Patients underwent standard operative and perioperative treatment.Resected patient tissues underwent standard surgical pathology proce-
www.Scie
dures before being imaged and sampled for the study with the guidanceof a clinical pathologist blinded to the fluorescence imaging measure-ments. Safety evaluations, described in Supplementary Materials andMethods, were conducted before and after peripheral intravenousadministration of LUM015 at three predetermined doses: 0.5, 1.0, or1.5 mg/kg. LUM015 was administered either the day before or on themorning of surgery. LUM015was supplied free of charge fromLumicellInc. Patient blood samples were collected before and after LUM015 ad-ministration for pharmacokinetic/pharmacodynamic studies.
Fluorescent agent administration and imagingMicewere administeredLUM015orLUM033via tail vein injectionwhentumors reached about 1000mm3 (4 to 5mm in diameter). Blood samplesfor pharmacokinetic studies were obtained from the submandibular vein.After a specified time interval, the animals were euthanized, and tissueswere removed for fluorescence imaging and other analyses. For the localrecurrence study, tumors were removed and intraoperative assessmentof residual fluorescence was performed as described previously (17). Thehandheld LUM imaging device was described previously (17), and thespecifications are provided in Supplementary Materials and Methods.Normal and tumor tissues were identified grossly, and the imaging tipwas applied to the tissue to obtain two to three images of the same loca-tion. The tissue was biopsied at the site of imaging for identification ofthe tissue type by histological analysis (H&E) and measurement ofLUM015 and its metabolites (fragment 2 and Cy5-Lys).
Image processing was performed using a custom script developedin theMatlab programming environment (MathWorks) using standardcorrections for background and signal distribution (32), described inSupplementary Materials and Methods. Mean pixel intensities derivedfrom theMatlab script are reported in this study. For visual representa-tion of images, the contrast and brightness of images were adjusted asdescribed previously (17) so that the reader can appreciate the differ-ences in fluorescence intensities between tumor and normal tissue.
Histological analysis, immunohistochemistry,and immunofluorescenceFFPE sample tissues were sectioned to create 5-mm-thick slides forH&Estaining, PEG immunohistochemistry, and immunofluorescencestudies. Staining and quantification methods are described in Supple-mentary Materials and Methods. Slides were reviewed by a clinical pa-thologist specializing in STS (D.M.C.), who was blinded to tissuefluorescence measurements.
Flow cytometryKPYmice harboring primary sarcomaswere injectedwith either LUM015(3.5 mg/kg) or PBS vehicle, and tumors were collected 6 hours after injec-tion. Cells were dissociated from tumors according to methods describedpreviously (33). Total cells dissociated from tumors were incubated withrat anti-mouseCD16/32 immunoglobulinG (IgG) (BDPharmingen) andphycoerythrin-Cy5–conjugated anti-mouse CD11b IgG (eBioscience).Data were collected from at least 200,000 cells by FACSCanto (BD Phar-mingen) and analyzedbyFlowJo (Tree Star Inc.).GenomicPCRanalysis toshow recombination of the mutant Kras allele was performed with thefollowing primers: (i) 5′-GTCTTTCCCCAGCACAGTGC-3′; (ii) 5′-CTCTTGCCTACGCCACCAGCTC-3′; (iii) 5′-AGCTAGCCACCAT-GGCTTGAGTAAGTCTGCA-3′. The wild-type Kras allele yields a622-bp band, the unrecombined LSL-KrasG12D allele yields a 500-bpband, and the recombined 1-loxP-KrasG12D allele yields a 650-bp band.
nceTranslationalMedicine.org 6 January 2016 Vol 8 Issue 320 320ra4 9

R E S EARCH ART I C L E
http://stD
ownloaded from
Plasma and tissue metabolite measurementsConcentrations of LUM015 and its metabolites in plasma andtissue samples were determined using LC-MS/MS as well as HPLCwith fluorescence detection (HPLC-FD). A detailed methodology ispresented in Supplementary Materials and Methods.
StatisticsResults are presented asmeans ± SEMunless otherwise indicated. Beforeanalysis, all data were displayed graphically to determine whether para-metric or nonparametric tests should be used. Two-tailed Student’s t testwas performed to compare themeans of two groups, and amatchedpair ttest was used when comparing fluorescent measurements from the samepatient. A Mann-Whitney test was performed to compare the means oftwo groups when data were distributed nonparametrically. Two-wayANOVA was performed to examine the interaction between twoindependent variables such as dose and imaging time, and one-wayANOVA was used when measuring the effect of only one variable, suchas tissue type. These were followed by Bonferroni or Tukey’s post hocmultiple comparison tests for pairwise comparisons of individual treat-ments or tissue types. For local recurrence studies, Kaplan-Meier analysiswas performed with the log-rank test for statistical significance. To findthe correlation of two different measurements from the same sample, wedetermined thePearson coefficient (r) and r2. Significancewas assumedatP < 0.05. All calculations were performed using Prism 6 (GraphPad).
by guest on Novem
ber 1m
.sciencemag.org/
SUPPLEMENTARY MATERIALS
www.sciencetranslationalmedicine.org/cgi/content/full/8/320/320ra4/DC1Materials and MethodsFig. S1. In vitro incubation of LUM015 with mouse tissues.Fig. S2. The percentage of tumor cells that are Cy5+ after administration of LUM015.Fig. S3. In vivo detection of residual fluorescence within the mouse tumor bed.Fig. S4. Summary pharmacokinetic data from mice and humans.Fig. S5. Contribution of protease-activation and LUM015 distribution for tumor-selectivefluorescence.Table S1. No adverse pharmacological activity of LUM015 in humans.Table S2. Liver function tests.Table S3. Ex vivo imaging of human tissues.Table S4. Correlating tissue fluorescence with metabolite concentration.References (34–40)
, 2020
REFERENCES AND NOTES
1. P. W. Pisters, D. H. Leung, J. Woodruff, W. Shi, M. F. Brennan, Analysis of prognostic factorsin 1,041 patients with localized soft tissue sarcomas of the extremities. J. Clin. Oncol. 14,1679–1689 (1996).
2. B. Fisher, S. Anderson, J. Bryant, R. G. Margolese, M. Deutsch, E. R. Fisher, J.-H. Jeong,N. Wolmark, Twenty-year follow-up of a randomized trial comparing total mastectomy,lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer.N. Engl. J. Med. 347, 1233–1241 (2002).
3. J. C. Yang, A. E. Chang, A. R. Baker, W. F. Sindelar, D. N. Danforth, S. L. Topalian, T. DeLaney,E. Glatstein, S. M. Steinberg, M. J. Merino, S. A. Rosenberg, Randomized prospective studyof the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of theextremity. J. Clin. Oncol. 16, 197–203 (1998).
4. M. S. Anscher, P. Jones, L. R. Prosnitz, W. Blackstock, M. Hebert, R. Reddick, A. Tucker,R. Dodge, G. Leight Jr., J. D. Iglehart, et al., Local failure and margin status in early-stagebreast carcinoma treated with conservation surgery and radiation therapy. Ann. Surg.218, 22–28 (1993).
5. J. C. Cendán, D. Coco, E. M. Copeland III, Accuracy of intraoperative frozen-section analysisof breast cancer lumpectomy-bed margins. J. Am. Coll. Surg. 201, 194–198 (2005).
6. S. Harmsen, R. Huang, M. A. Wall, H. Karabeber, J. M. Samii, M. Spaliviero, J. R. White, S. Monette,R. O’Connor, K. L. Pitter, S. A. Sastra, M. Saborowski, E. C. Holland, S. Singer, K. P. Olive,
www.Scien
S. W. Lowe, R. G. Blasberg, M. F. Kircher, Surface-enhanced resonance Raman scatteringnanostars for high-precision cancer imaging. Sci. Transl. Med. 7, 271ra7 (2015).
7. Y. Liu, J. R. Ashton, E. J. Moding, H. Yuan, J. K. Register, A. M. Fales, J. Choi, M. J. Whitley,X. Zhao, Y. Qi, Y. Ma, G. Vaidyanathan, M. R. Zalutsky, D. G. Kirsch, C. T. Badea, T. Vo-Dinh, Aplasmonic gold nanostar theranostic probe for in vivo tumor imaging and photothermaltherapy. Theranostics 5, 946–960 (2015).
8. Q. R. J. G. Tummers, F. P. R. Verbeek, B. E. Schaafsma, M. C. Boonstra, J. R. van der Vorst,G.-J. Liefers, C. J. H. van de Velde, J. V. Frangioni, A. L. Vahrmeijer, Real-time intraoperativedetection of breast cancer using near-infrared fluorescence imaging and Methylene Blue.Eur. J. Surg. Oncol. 40, 850–858 (2014).
9. N. Kosaka, M. Mitsunaga, M. R. Longmire, P. L. Choyke, H. Kobayashi, Near infrared fluorescence-guided real-time endoscopic detection of peritoneal ovarian cancer nodules using intra-venously injected indocyanine green. Int. J. Cancer 129, 1671–1677 (2011).
10. R. A. Sheth, R. S. Arellano, R. N. Uppot, A. E. Samir, L. Goyal, A. X. Zhu, D. A. Gervais,U. Mahmood, Prospective trial with optical molecular imaging for percutaneous interven-tions in focal hepatic lesions. Radiology 274, 917–926 (2015).
11. R. Weissleder, Molecular imaging in cancer. Science 312, 1168–1171 (2006).12. G.M. vanDam,G. Themelis, L.M.A. Crane, N. J. Harlaar, R. G. Pleijhuis,W. Kelder, A. Sarantopoulos,
J. S. de Jong, H. J. G. Arts, A. G. J. van der Zee, J. Bart, P. S. Low, V. Ntziachristos, Intraoperativetumor-specific fluorescence imaging in ovarian cancer by folate receptor-a targeting: First in-human results. Nat. Med. 17, 1315–1319 (2011).
13. Y. Ardeshirpour, M. Hassan, R. Zielinski, J. A. Horton, J. Capala, A. H. Gandjbakhche,V. Chernomordik, In vivo assessment of HER2 receptor density in HER2-positive tumors bynear-infrared imaging, using repeated injections of the fluorescent probe. Technol. CancerRes. Treat. 13, 427–434 (2014).
14. R. Weissleder, C.-H. Tung, U. Mahmood, A. Bogdanov Jr., In vivo imaging of tumors withprotease-activated near-infrared fluorescent probes. Nat. Biotechnol. 17, 375–378(1999).
15. J. E. Koblinski, M. Ahram, B. F. Sloane, Unraveling the role of proteases in cancer. Clin. Chim.Acta 291, 113–135 (2000).
16. M. M. Mohamed, B. F. Sloane, Cysteine cathepsins: Multifunctional enzymes in cancer. Nat.Rev. Cancer 6, 764–775 (2006).
17. J. K.Mito, J. M. Ferrer, B. E. Brigman, C.-L. Lee, R. D. Dodd,W. C. Eward, L. F. Marshall, K. C. Cuneo,J. E. Carter, S. Ramasunder, Y. Kim, W. D. Lee, L. G. Griffith, M. G. Bawendi, D. G. Kirsch, Intra-operative detection and removal of microscopic residual sarcoma using wide-field imaging.Cancer 118, 5320–5330 (2012).
18. S. Bartholf DeWitt, C. Eward,W. C. Eward, A. L. Lazarides, D. G. Kirsch, D.M.Cardona, B. E. Brigman,J. K. Mito, M. J. Whitley, J. M. Ferrer, D. B. Strasfeld, D. Lee, K. Concannon, G. Spodnick, E. Holmes,K. Miller, J. Berg, in The American College of Veterinary Surgeons 2014 Surgery Summitt (SanDiego, California, 2014).
19. E. J. Freireich, E. A. Gehan, D. P. Rall, L. H. Schmidt, H. E. Skipper, Quantitative comparisonof toxicity of anticancer agents in mouse, rat, hamster, dog, monkey, and man. CancerChemother. Rep. 50, 219–244 (1966).
20. B. O’Sullivan, A. M. Davis, R. Turcotte, R. Bell, C. Catton, P. Chabot, J. Wunder, R. Kandel,K. Goddard, A. Sadura, J. Pater, B. Zee, Preoperative versus postoperative radiotherapy insoft-tissue sarcoma of the limbs: A randomised trial. Lancet 359, 2235–2241 (2002).
21. E. Segal, T. R. Prestwood, W. A. van der Linden, Y. Carmi, N. Bhattacharya, N. Withana,M. Verdoes, A. Habtezion, E. G. Engleman, M. Bogyo, Detection of intestinal cancer by local,topical application of a quenched fluorescence probe for cysteine cathepsins. Chem. Biol.22, 148–158 (2015).
22. C. Bremer, C.-H. Tung, R. Weissleder, In vivo molecular target assessment of matrix metal-loproteinase inhibition. Nat. Med. 7, 743–748 (2001).
23. E. S. Olson, T. Jiang, T. A. Aguilera, Q. T. Nguyen, L. G. Ellies, M. Scadeng, R. Y. Tsien,Activatable cell penetrating peptides linked to nanoparticles as dual probes for in vivofluorescence and MR imaging of proteases. Proc. Natl. Acad. Sci. U.S.A. 107, 4311–4316(2010).
24. T. Quillard, K. Croce, F. A. Jaffer, R. Weissleder, P. Libby, Molecular imaging of macrophageprotease activity in cardiovascular inflammation in vivo. Thromb. Haemost. 105, 828–836(2011).
25. C. E. Lewis, J. W. Pollard, Distinct role of macrophages in different tumor microenviron-ments. Cancer Res. 66, 605–612 (2006).
26. E. Y. Lin, A. V. Nguyen, R. G. Russell, J. W. Pollard, Colony-stimulating factor 1 promotesprogression of mammary tumors to malignancy. J. Exp. Med. 193, 727–740 (2001).
27. G. W. Caldwell, J. A. Masucci, Z. Yan, W. Hageman, Allometric scaling of pharmacokineticparameters in drug discovery: Can human CL, Vss and t1/2 be predicted from in-vivo ratdata? Eur. J. Drug Metab. Pharmacokinet. 29, 133–143 (2004).
28. T. Kolokotrones, S. Van, E. J. Deeds, W. Fontana, Curvature in metabolic scaling. Nature 464,753–756 (2010).
29. W. P. Caron,H. Clewell, R. Dedrick, R. K. Ramanathan,W. L. Davis, N. Yu,M. Tonda, J. H. Schellens,J. H. Beijnen, W. C. Zamboni, Allometric scaling of pegylated liposomal anticancer drugs.J. Pharmacokinet. Pharmacodyn. 38, 653–669 (2011).
ceTranslationalMedicine.org 6 January 2016 Vol 8 Issue 320 320ra4 10

R E S EARCH ART I C L E
by guehttp://stm
.sciencemag.org/
Dow
nloaded from
30. W. D. Dupont, W. D. Plummer Jr., Power and sample size calculations. A review and com-puter program. Control. Clin. Trials 11, 116–128 (1990).
31. K. C. Cuneo, J. K. Mito, M. P. Javid, J. M. Ferrer, Y. Kim, W. D. Lee, M. G. Bawendi, B. E. Brigman,D. G. Kirsch, Imaging primary mouse sarcomas after radiation therapy using cathepsin-activatable fluorescent imaging agents. Int. J. Radiat. Oncol. Biol. Phys. 86, 136–142 (2013).
32. D. L. Taylor, Y.-l. Wang, Fluorescence microscopy of living cells in culture, in Methods in CellBiology, L. Wilson, Ed. (Academic Press, San Diego, CA, 1989), vol. 29, pp. 1–328.
33. M. Sachdeva, J. K. Mito, C.-L. Lee, M. Zhang, Z. Li, R. D. Dodd, D. Cason, L. Luo, Y. Ma, D. Van Mater,R. Gladdy, D. C. Lev, D. M. Cardona, D. G. Kirsch, MicroRNA-182 drives metastasis of primarysarcomas by targeting multiple genes. J. Clin. Invest. 124, 4305–4319 (2014).
34. E. L. Jackson, N.Willis, K. Mercer, R. T. Bronson, D. Crowley, R. Montoya, T. Jacks, D. A. Tuveson,Analysis of lung tumor initiation and progression using conditional expression of oncogenicK-ras. Genes Dev. 15, 3243–3248 (2001).
35. D. Dankort, E. Filenova, M. Collado, M. Serrano, K. Jones, M. McMahon, A new mousemodel to explore the initiation, progression, and therapy of BRAFV600E-induced lung tu-mors. Genes Dev. 21, 379–384 (2007).
36. J. Jonkers, R. Meuwissen, H. van der Gulden, H. Peterse, M. van der Valk, A. Berns, Syner-gistic tumor suppressor activity of BRCA2 and p53 in a conditional mouse model for breastcancer. Nat. Genet. 29, 418–425 (2001).
37. S. Srinivas, T. Watanabe, C.-S. Lin, C. M. William, Y. Tanabe, T. M. Jessell, F. Costantini, Crereporter strains produced by targeted insertion of EYFP and ECFP into the ROSA26 locus.BMC Dev. Biol. 1, 4 (2001).
38. D. G. Kirsch, D. M. Dinulescu, J. B. Miller, J. Grimm, P. M. Santiago, N. P. Young, G. P. Nielsen,B. J. Quade, C. J. Chaber, C. P. Schultz, O. Takeuchi, R. T. Bronson, D. Crowley, S. J. Korsmeyer,S. S. Yoon, F. J. Hornicek, R. Weissleder, T. Jacks, A spatially and temporally restricted mousemodel of soft tissue sarcoma. Nat. Med. 13, 992–997 (2007).
39. Y. Huang, J. Yuan, E. Righi, W. S. Kamoun,M. Ancukiewicz, J. Nezivar, M. Santosuosso, J. D. Martin,M. R. Martin, F. Vianello, P. Leblanc, L. L. Munn, P. Huang, D. G. Duda, D. Fukumura, R. K. Jain,M. C. Poznansky, Vascular normalizing doses of antiangiogenic treatment reprogram theimmunosuppressive tumor microenvironment and enhance immunotherapy. Proc. Natl.Acad. Sci. U.S.A. 109, 17561–17566 (2012).
40. E. I. Ager, S. V. Kozin, N. D. Kirkpatrick, G. Seano, D. P. Kodack, V. Askoxylakis, Y. Huang, S. Goel,M. Snuderl, A. Muzikansky, D. M. Finkelstein, D. T. Dransfield, L. Devy, Y. Boucher, D. Fukumura,R. K. Jain, Blockade of MMP14 activity in murine breast carcinomas: Implications for macro-phages, vessels, and radiotherapy. J. Natl. Cancer Inst. 107, djv017 (2015).
Acknowledgments: We thank Y. Ma, N. Williams, and L. Luo for valuable assistancewith histology,animal/human tissue imaging, and mouse colony management, respectively. We thank J. Kahnfor her technical assistance with the mice in the breast cancer studies. We thank P. O’Donnell ofthe University of Kentucky, F. Hornicek of the Massachusetts General Hospital, S. Yoon of the
www.Scien
Memorial Sloan Kettering Cancer Center, and R. Noveck of Duke University for serving on thepatient safety committee for the phase 1 study. We thank B. Peterson for guidance on statisticaldesign of the clinical trial. Funding: Supported in part by the American Society of Clinical On-cology Advanced Clinical Research Award (D.G.K.), NIH T32 grant #T32GM007171 (M.J.W. andJ.K.M.), National Cancer Institute Small Business Innovation Research award #1U43CA165024(W.D.L.), National Center for Advancing Translational Science of the NIH grant #UL1TR001117(E.K.O.), and Duke Comprehensive Cancer Center Support Grant 5P30-CA-014236-38. Authorcontributions: M.J.W. participated in the design and execution of the clinical protocol, de-signed and performed experiments, analyzed and interpreted data, and wrote themanuscript.D.M.C., A.L.L., I.S., C.-L.L., M.S., and J.K.M. designed and performed experiments, analyzed andinterpreted data, and contributed to the writing of the manuscript. J.M.F., D.B.S., W.D.L., L.G.G.,and M.G.B. participated in the design of the clinical protocol, designed experiments, and ana-lyzed and interpreted data. J.C. participated in the design of the clinical protocol, identifiedhuman subjects, and participated in sample procurement. D.G.B., E.S.H., R.A.G., and P.J.M. iden-tified human subjects and participated in sample procurement. K.C.C., N.A.L., E.K.O., R.F.R., andW.C.E. participated in the design of the clinical protocol and edited the manuscript. E.K.O.drafted, submitted, and maintained the investigational new drug (IND) related to the phase1 study. D.F. and R.K.J. analyzed and interpreted data and contributed to the writing of themanuscript. R.F.R. and B.E.B. served on the safety monitoring committee. D.G.K. participated inthe design of the clinical protocol, held the IND, designed and oversaw the laboratory studies,interpreted the data, and wrote the manuscript. B.E.B. designed and supervised the clinical pro-tocol, participated in sample procurement, and edited the manuscript. Competing interests:W.D.L. is a cofounder and the CEO of Lumicell Inc., a company that is commercializing LUM015and the LUM imaging system. M.G.B. is a cofounder of Lumicell Inc. and is a member of itsscientific advisory board. L.G.G. and D.G.K. are members of the Lumicell Inc. scientific advisoryboard. W.D.L., M.G.B., and J.M.F. are co-inventors of LUM015 under U.S. patent application20140301950. W.D.L., M.G.B., J.M.F., and D.G.K. are co-inventors of the handheld imaging deviceunder U.S. patent 20140301950-A1. Data and materials availability: LUM015 and LUM033 canbe obtained from Lumicell Inc.
Submitted 15 July 2015Accepted 11 November 2015Published 6 January 201610.1126/scitranslmed.aad0293
Citation: M. J. Whitley, D. M. Cardona, A. L. Lazarides, I. Spasojevic, J. M. Ferrer, J. Cahill, C.-L. Lee,M. Snuderl, D. G. Blazer III, E. S. Hwang, R. A. Greenup, P. J. Mosca, J. K. Mito, K. C. Cuneo, N. A. Larrier,E. K. O’Reilly, R. F. Riedel, W. C. Eward, D. B. Strasfeld, D. Fukumura, R. K. Jain, W. D. Lee, L. G. Griffith,M. G. Bawendi, D. G. Kirsch, B. E. Brigman , A mouse-human phase 1 co-clinical trial of a protease-activated fluorescent probe for imaging cancer. Sci. Transl. Med. 8, 320ra4 (2016).
st o
ceTranslationalMedicine.org 6 January 2016 Vol 8 Issue 320 320ra4 11
n Novem
ber 1, 2020

imaging cancerA mouse-human phase 1 co-clinical trial of a protease-activated fluorescent probe for
Fukumura, Rakesh K. Jain, W. David Lee, Linda G. Griffith, Moungi G. Bawendi, David G. Kirsch and Brian E. BrigmanMito, Kyle C. Cuneo, Nicole A. Larrier, Erin K. O'Reilly, Richard F. Riedel, William C. Eward, David B. Strasfeld, DaiChang-Lung Lee, Matija Snuderl, Dan G. Blazer III, E. Shelley Hwang, Rachel A. Greenup, Paul J. Mosca, Jeffrey K. Melodi Javid Whitley, Diana M. Cardona, Alexander L. Lazarides, Ivan Spasojevic, Jorge M. Ferrer, Joan Cahill,
DOI: 10.1126/scitranslmed.aad0293, 320ra4320ra4.8Sci Transl Med
probes are now poised for further adaptation to tumor resections, signaling the presence of residual cancer.types of tumor tissues. With favorable biodistribution and pharmacokinetics also demonstrated, protease-activatedsarcoma model, and in a so-called ''co-clinical trial'' in 15 patients, it was safe and cleaved as expected in different intraoperatively. Their probe, called LUM015, was able to signal the presence of cancer in vivo in a mousebe activated in the presence of these cathepsins, thus allowing surgeons to distinguish tumor margins
. developed an imaging probe that couldet alremodel their surroundings for tumor growth and metastasis. Whitley Cancer cells secrete more of the protease cathepsin than healthy cells, partly as a way to enzymatically
Protease probe tested in humans
ARTICLE TOOLS http://stm.sciencemag.org/content/8/320/320ra4
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2016/01/04/8.320.320ra4.DC1
CONTENTRELATED
http://stm.sciencemag.org/content/scitransmed/12/542/eaay0712.fullhttp://stm.sciencemag.org/content/scitransmed/9/410/eaal4291.fullhttp://stm.sciencemag.org/content/scitransmed/7/271/271ra7.fullhttp://stm.sciencemag.org/content/scitransmed/5/216/216rv4.fullhttp://stm.sciencemag.org/content/scitransmed/6/260/260ra148.fullhttp://stm.sciencemag.org/content/scitransmed/3/110/110ra119.fullhttp://stm.sciencemag.org/content/scitransmed/6/260/260ra149.full
REFERENCES
http://stm.sciencemag.org/content/8/320/320ra4#BIBLThis article cites 38 articles, 10 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
Copyright © 2016, American Association for the Advancement of Science
by guest on Novem
ber 1, 2020http://stm
.sciencemag.org/
Dow
nloaded from