Embed Size (px)
Citation preview

646November 2006 Volume 32 Number 11
I n July 2003 the Accreditation Council for GraduateMedical Education (ACGME) set limits for residentduty hours1 Although the main driving force was to
reduce sleep deprivation and improve patient safety oneunintended consequence was the increase in the numberof handoffs during patient care The discontinuity of carethat thereby results has the potential to undermine thebeneficial effects of work hour limitations2 The safety ofthe hand-off process has been called into question by anumber of different sources and studies which suggestthat handoffs are often characterized by communicationfailures and environmental barriers3ndash6
The handoff is also the subject of a Joint Commissionon Accreditation of Healthcare Organizations NationalPatient Safety Goal which went into effect January 12006 Written as a new requirement of Goal 2 Improvethe Effectiveness of Communication Among Caregiversthis addition requires hospitals to implement a stan-dardized approach to hand-off communications andprovide an opportunity for staff to ask and respond toquestions about a patientrsquos care67 (Sidebar 1 page 647)Although the standard applies to all handoffs that occurbetween all personnel within all health care settings thefocus of this article is on the handoffs between residen-cy trainees at academic teaching hospitals Becausemedical trainees receive little to no formal training oreducation in communication during handoffs there isan inherent opportunity to influence the practice of
A Model for Building a StandardizedHand-off Protocol
National Patient Safety Goals
Background The Joint Commission has made aldquostandardized approach to hand-off communicationsrdquo aNational Patient Safety Goal
Method An interactive 90-minute workshop (hand-off clinic) was developed in 2005 to (1) develop a stan-dardized process for the handoff (2) create a checklistof critical patient content and (3) plan for dissemina-tion and training
Conclusion To date 7 of 10 residency programs haveparticipated Analysis of these protocols demonstratedthat the hand-off process is highly variable and discipline-specific Although all disciplines required a verbal handoff because of competing demands verbal commu-nication did not always occur In some cases the transferof professional responsibility was separated in time andspace from the transfer of information For example intwo cases patient tasks were assigned to other teammembers to facilitate timely departure of a postcall resi-dent (to meet resident duty-hour restrictions) but resultswere not formally communicated to anyone The hand-off clinic facilitated the incorporation of ldquoclosed-looprdquocommunication by requiring that follow-up on thesetasks be conveyed to the on-call resident
Discussion This model for design and implementa-tion can be applied to other health care settings
Article-at-a-Glance
Vineet Arora MD MAJulie Johnson MSPH PhD
Department EditorsMarcia M Piotrowski RN MS Peter Angood MD Paula Griswold
MS Gina Pugliese RN MS Sanjay Saint MD MPH Susan E Sheridan MIM MBA Kaveh G Shojania MD Readers may submit
National Patient Safety Goals inquiries and submissions to Steven Berman (sbermanjcahoorg) and Marcia Piotrowski (marciapiotrowskimedvagov)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
647
future physicians8 In addition as academic teachinghospitals continue to adopt systems to ensure that duty-hour restrictions are met an increased focus on theintegrity of the handoffs is crucial to patient safety dur-ing these times of transition
Although relatively little information about educa-tional initiatives exist in the medical literature to guideresident and staff hospital physicians in meeting thesestandards much can be learned from other high-riskindustries that have been engaged in studying andimproving handoffs From direct observations at theNational Aeronautics and Space Agency nuclear powerplants and transportation dispatch centers a frame-work of strategies for handoffs has emerged9 Certainstrategies such as standardization and face-to-face ver-bal update with interactive questioning resonate direct-ly with the hand-off requirement and are supported by
evidence and expert opinion as best practices associat-ed with improved hand-off comunication5710 Drawingon this literature as well as preliminary data we pres-ent a model for building a standardized hand-off proto-col to meet this National Patient Safety Goal We alsoreview our preliminary experience with the protocol atthe University of Chicago
Creating a Model for Standardized HandoffsThe handoff can be thought of as a communication ofinformation (content) that can take place through dif-ferent modalities which can include a written or verbalcomponent Two guiding principles underlie this modelFirst the standardized protocol for handoffs needs to betailored to discipline and organization That is recog-nize that what works in one discipline may not work in
November 2006 Volume 32 Number 11
Requirement 2E
Implement a standardized approach to ldquohand-offrdquo com-munications including an opportunity to ask andrespond to questions
Rationale for Requirement 2E
The primary objective of a ldquohand offrdquo is to provideaccurate information about a patientrsquos care treatmentand services current condition and any recent or antici-pated changes The information communicated during ahand off must be accurate in order to meet patientsafety goals In health care there are numerous types ofpatient hand offs including but not limited to nursingshift changes physicians transferring complete respon-sibility for a patient physicians transferring on-callresponsibility temporary responsibility for staff leavingthe unit for a short time anesthesiologist report topost-anesthesia recovery room nurse nursing andphysician hand off from the emergency department toinpatient units different hospitals nursing homes andhome health care critical laboratory and radiologyresults sent to physician offices
Implementation Expectations for Requirement 2E
1 The organizationrsquos process for effective ldquohand offrdquocommunication includes Interactive communicationsallowing for the opportunity for questioning betweenthe giver and receiver of patient information
2 The organizationrsquos process for effective ldquohand offrdquocommunication includes Up-to-date informationregarding the patientrsquos care treatment and servicescondition and any recent or anticipated changes
3 The organizationrsquos process for effective ldquohand offrdquocommunication includes A process for verification ofthe received information including repeat-back orread-back as appropriate
4 The organizationrsquos process for effective ldquohand offrdquocommunication includes An opportunity for thereceiver of the hand off information to review rele-vant patient historical data which may include previ-ous care treatment and services
5 Interruptions during hand offs are limited to mini-mize the possibility that information would fail to beconveyed or would be forgotten
Sidebar 1 Joint Commission National Patient Safety Goal 2Improve the Effectiveness of Communication Among Caregivers
Source Joint Commission on Accreditation of Healthcare Organizations 2007 National Patient Safety Goals Hospital Version Manual Chapter includingImplementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafetyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
648November 2006 Volume 32 Number 11
another given each disciplinersquos unique requirementsFurthermore what constitutes an effective handoff forone discipline may be different for the same discipline inanother organization Although certain components maybe generalizable the successful adoption of a standard-ized hand-off protocol is highly dependent on the degreeto which it is tailored for end users in an organizationalsetting It is the method by which you create the proto-colmdashand the method that is presented heremdashthat is gen-eralizable across disciplines and organizations
Second standardization is the core goal for bothhand-off process and content For example although anidentifiable safe protocol may be currently in use for themajority of handoffs in a certain discipline and organiza-tion it is the variability of the hand-off protocol that isthe target for improvement The four steps in our modelare outlined in Table 1 (above) and discussed in detailbelow
Develop a Standardized ProcessldquoThe first step is to draw a flow diagram Then every-
one understands what his job is If people do not see the
process they cannot improve itrdquo mdash WE Deming
Understanding handoffs as a process is importantbecause a high degree of process awareness often drivesthe design of the work By mapping the process themembers of the team can gain insight into how their col-leagues perceive the same tasks Ultimately systemsimprovement requires (1) appreciating the inherent linkbetween process and results and (2) identifying potentialareas for improvement with a focus on the system that is
producing the processes and outcomes of care11 ratherthan on the individual
Process mapping can be used to describe and analyzehow an individual clinician interacts with the system aswell as with others within that system Process mappingdescribes what an individual is required to do in termsof cognitive processes andor actions to achieve the sys-temrsquos goal It can be accomplished through observationsandor interviews that carefully break down the multiplesteps in the process
Process maps can be created at different levels ofgranularity from a high-level overview of the major stepsin the process to very detailed representation of eachspecific step or activity Detailed process maps are espe-cially helpful to standardize and improve processes Foruse as an improvement tool it is important to map thecurrent process not the desired process so that oppor-tunities for improvement can be identified Being explic-it about the processes can help clinicians shape whatthey know about their environment and to provideinsight into how to improve the process or overcomesome of the barriers
Everyday multiple types of handoffs occur in healthcare settings such as handoffs around shift changes ofnursing shifts referrals to specialty care and dischargefrom inpatient to outpatient care We found it valuableto select only one type of handoff for the process analy-sismdashthe handoff from postcall residents to on-call resi-dents This transition represents the period of time thata patient is cared for by a ldquocoveringrdquo resident who maybe unfamiliar with the patientrsquos hospital course aknown risk factor for preventable adverse events12 Inaddition our earlier work suggested that this handoffwas particularly vulnerable with the implementation ofrecent ACGME duty-hour restrictions5 The particularquestion that we posed to residents in the process map-ping exercise was ldquoHow does a postcall resident trans-fer the care of their patients to an oncoming residentrdquoWe specifically asked how the contentmdashthe criticalinformation required to care for patients during thecoverage periodmdashis transferred We also asked resi-dents to delineate the mechanism by which the on-coming resident formally accepts care of the patients(that is the oncoming resident starts accepting callsfrom a ldquovirtual pagerrdquo when they are on call postcall
1 Process
Create a process map
2 Content
Create a standard check-list
3 Implementation
Garner leadership and resident buy-in
4 Monitoring
Ensure the protocol is in place and identify andresolve barriers
Table 1 Model for Adoption of aStandardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
649
resident forwards their pager to the oncoming residentand so on)
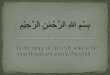
Figure 1 (above) includes a process mapping tutori-al that was used during the hand-off clinic Samplehand-off process maps for neurology and otolaryngolo-gy are included in Figure 2 (page 650) and Figure 3(page 651) respectively To analyze process maps sev-eral questions are important to address to generateimprovement ideas What is the goal of the process Does the process work as it should Are there obvious redundancies or complexities How different is the current process from the idealprocess
Although mapping the process is an important step indocumenting the standardized protocol for handoffs itcan also be instrumental in educating new interns aboutthe process Furthermore a process map can form thebasis of the performance measurement tool to monitorand assess adherence to the process
Build a Checklist of Necessary ContentIn addition to developing a standardized process it is
equally important to determine the critical content to betransferred in a patient handoff13 Omissions of contentare a major cause of failed communication during hand-offs5 A checklist of necessary information can helpteach others new to the handoff about the process and
November 2006 Volume 32 Number 11
Figure 1 This process mapping tutorial was used during the hand-off clinic
Process Map Tutorial
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
650November 2006 Volume 32 Number 11
serve as a monitoring tool in evaluating the contenttransferred In designing a checklist it is important tocustomize it for a specific discipline
When thinking about what content to include in achecklist one helpful tool is to interview the participantsin the hand-off process regarding the information thatthey desire or need (Figure 4 page 652) A good startingpoint is to ask the following question ldquoWhat are the maincontent pieces of a handoff in your disciplinerdquo Theanswers will likely result in a list of necessary patientcontent A more detailed interview can elicit content thatis part of an optimal handoff in addition to content thatmay be omitted in a suboptimal handoff To convert thiscontent into a checklist it is important to group this listinto larger categories of content and smaller subcate-gories in each major category as shown in the standard-ized content checklist for the pediatrics hand-off protocol (Figure 5 page 653) For example adminis-trative data or medications constitute large categorieswhereas name room number and admitting team orservice compose smaller subcategories under adminis-trative data Many programs may already use a templatefor written content which may facilitate the creation ofcategories and subcategories of content The checklist
will be perceived as more credible if it reflects technicaljargon or refers to organizational or program-specificnomenclature used in daily patient care For this reasoneliciting specific examples for how information is com-municated during the interview is particularly helpfulOperator experiencemdashthe experience of those partici-pating in the handoffmdashcan influence the design of thechecklist For example experienced physicians in hospi-tal practice may not require the extensive checklist usedby new interns Finally an acronym can serve as areminder for critical content but also as a motivationaltool to learn the new protocol14 For example theacronym we used for the checklist for psychiatry resi-dents was ldquopsychiatryrdquomdashrepresenting psychiatric histo-ry special instructions for you for me (the to-do list)courtlegal issues housing and social issues ifthenadministrative data and allergies therapeutics resultsof pertinent labs and radiology
Discuss Implementation StrategiesAn implementation plan begins with dissemination of
both the process map and the checklist of necessary con-tent Using an opinion leader in a residency program suchas a chief resident or program director can help facilitate
Figure 2 The hand-off process map for neurology is shown PGY postgraduate year
Process Map for Neurology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

647
future physicians8 In addition as academic teachinghospitals continue to adopt systems to ensure that duty-hour restrictions are met an increased focus on theintegrity of the handoffs is crucial to patient safety dur-ing these times of transition
Although relatively little information about educa-tional initiatives exist in the medical literature to guideresident and staff hospital physicians in meeting thesestandards much can be learned from other high-riskindustries that have been engaged in studying andimproving handoffs From direct observations at theNational Aeronautics and Space Agency nuclear powerplants and transportation dispatch centers a frame-work of strategies for handoffs has emerged9 Certainstrategies such as standardization and face-to-face ver-bal update with interactive questioning resonate direct-ly with the hand-off requirement and are supported by
evidence and expert opinion as best practices associat-ed with improved hand-off comunication5710 Drawingon this literature as well as preliminary data we pres-ent a model for building a standardized hand-off proto-col to meet this National Patient Safety Goal We alsoreview our preliminary experience with the protocol atthe University of Chicago
Creating a Model for Standardized HandoffsThe handoff can be thought of as a communication ofinformation (content) that can take place through dif-ferent modalities which can include a written or verbalcomponent Two guiding principles underlie this modelFirst the standardized protocol for handoffs needs to betailored to discipline and organization That is recog-nize that what works in one discipline may not work in
November 2006 Volume 32 Number 11
Requirement 2E
Implement a standardized approach to ldquohand-offrdquo com-munications including an opportunity to ask andrespond to questions
Rationale for Requirement 2E
The primary objective of a ldquohand offrdquo is to provideaccurate information about a patientrsquos care treatmentand services current condition and any recent or antici-pated changes The information communicated during ahand off must be accurate in order to meet patientsafety goals In health care there are numerous types ofpatient hand offs including but not limited to nursingshift changes physicians transferring complete respon-sibility for a patient physicians transferring on-callresponsibility temporary responsibility for staff leavingthe unit for a short time anesthesiologist report topost-anesthesia recovery room nurse nursing andphysician hand off from the emergency department toinpatient units different hospitals nursing homes andhome health care critical laboratory and radiologyresults sent to physician offices
Implementation Expectations for Requirement 2E
1 The organizationrsquos process for effective ldquohand offrdquocommunication includes Interactive communicationsallowing for the opportunity for questioning betweenthe giver and receiver of patient information
2 The organizationrsquos process for effective ldquohand offrdquocommunication includes Up-to-date informationregarding the patientrsquos care treatment and servicescondition and any recent or anticipated changes
3 The organizationrsquos process for effective ldquohand offrdquocommunication includes A process for verification ofthe received information including repeat-back orread-back as appropriate
4 The organizationrsquos process for effective ldquohand offrdquocommunication includes An opportunity for thereceiver of the hand off information to review rele-vant patient historical data which may include previ-ous care treatment and services
5 Interruptions during hand offs are limited to mini-mize the possibility that information would fail to beconveyed or would be forgotten
Sidebar 1 Joint Commission National Patient Safety Goal 2Improve the Effectiveness of Communication Among Caregivers
Source Joint Commission on Accreditation of Healthcare Organizations 2007 National Patient Safety Goals Hospital Version Manual Chapter includingImplementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafetyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006)
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
648November 2006 Volume 32 Number 11
another given each disciplinersquos unique requirementsFurthermore what constitutes an effective handoff forone discipline may be different for the same discipline inanother organization Although certain components maybe generalizable the successful adoption of a standard-ized hand-off protocol is highly dependent on the degreeto which it is tailored for end users in an organizationalsetting It is the method by which you create the proto-colmdashand the method that is presented heremdashthat is gen-eralizable across disciplines and organizations
Second standardization is the core goal for bothhand-off process and content For example although anidentifiable safe protocol may be currently in use for themajority of handoffs in a certain discipline and organiza-tion it is the variability of the hand-off protocol that isthe target for improvement The four steps in our modelare outlined in Table 1 (above) and discussed in detailbelow
Develop a Standardized ProcessldquoThe first step is to draw a flow diagram Then every-
one understands what his job is If people do not see the
process they cannot improve itrdquo mdash WE Deming
Understanding handoffs as a process is importantbecause a high degree of process awareness often drivesthe design of the work By mapping the process themembers of the team can gain insight into how their col-leagues perceive the same tasks Ultimately systemsimprovement requires (1) appreciating the inherent linkbetween process and results and (2) identifying potentialareas for improvement with a focus on the system that is
producing the processes and outcomes of care11 ratherthan on the individual
Process mapping can be used to describe and analyzehow an individual clinician interacts with the system aswell as with others within that system Process mappingdescribes what an individual is required to do in termsof cognitive processes andor actions to achieve the sys-temrsquos goal It can be accomplished through observationsandor interviews that carefully break down the multiplesteps in the process
Process maps can be created at different levels ofgranularity from a high-level overview of the major stepsin the process to very detailed representation of eachspecific step or activity Detailed process maps are espe-cially helpful to standardize and improve processes Foruse as an improvement tool it is important to map thecurrent process not the desired process so that oppor-tunities for improvement can be identified Being explic-it about the processes can help clinicians shape whatthey know about their environment and to provideinsight into how to improve the process or overcomesome of the barriers
Everyday multiple types of handoffs occur in healthcare settings such as handoffs around shift changes ofnursing shifts referrals to specialty care and dischargefrom inpatient to outpatient care We found it valuableto select only one type of handoff for the process analy-sismdashthe handoff from postcall residents to on-call resi-dents This transition represents the period of time thata patient is cared for by a ldquocoveringrdquo resident who maybe unfamiliar with the patientrsquos hospital course aknown risk factor for preventable adverse events12 Inaddition our earlier work suggested that this handoffwas particularly vulnerable with the implementation ofrecent ACGME duty-hour restrictions5 The particularquestion that we posed to residents in the process map-ping exercise was ldquoHow does a postcall resident trans-fer the care of their patients to an oncoming residentrdquoWe specifically asked how the contentmdashthe criticalinformation required to care for patients during thecoverage periodmdashis transferred We also asked resi-dents to delineate the mechanism by which the on-coming resident formally accepts care of the patients(that is the oncoming resident starts accepting callsfrom a ldquovirtual pagerrdquo when they are on call postcall
1 Process
Create a process map
2 Content
Create a standard check-list
3 Implementation
Garner leadership and resident buy-in
4 Monitoring
Ensure the protocol is in place and identify andresolve barriers
Table 1 Model for Adoption of aStandardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
649
resident forwards their pager to the oncoming residentand so on)
Figure 1 (above) includes a process mapping tutori-al that was used during the hand-off clinic Samplehand-off process maps for neurology and otolaryngolo-gy are included in Figure 2 (page 650) and Figure 3(page 651) respectively To analyze process maps sev-eral questions are important to address to generateimprovement ideas What is the goal of the process Does the process work as it should Are there obvious redundancies or complexities How different is the current process from the idealprocess
Although mapping the process is an important step indocumenting the standardized protocol for handoffs itcan also be instrumental in educating new interns aboutthe process Furthermore a process map can form thebasis of the performance measurement tool to monitorand assess adherence to the process
Build a Checklist of Necessary ContentIn addition to developing a standardized process it is
equally important to determine the critical content to betransferred in a patient handoff13 Omissions of contentare a major cause of failed communication during hand-offs5 A checklist of necessary information can helpteach others new to the handoff about the process and
November 2006 Volume 32 Number 11
Figure 1 This process mapping tutorial was used during the hand-off clinic
Process Map Tutorial
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
650November 2006 Volume 32 Number 11
serve as a monitoring tool in evaluating the contenttransferred In designing a checklist it is important tocustomize it for a specific discipline
When thinking about what content to include in achecklist one helpful tool is to interview the participantsin the hand-off process regarding the information thatthey desire or need (Figure 4 page 652) A good startingpoint is to ask the following question ldquoWhat are the maincontent pieces of a handoff in your disciplinerdquo Theanswers will likely result in a list of necessary patientcontent A more detailed interview can elicit content thatis part of an optimal handoff in addition to content thatmay be omitted in a suboptimal handoff To convert thiscontent into a checklist it is important to group this listinto larger categories of content and smaller subcate-gories in each major category as shown in the standard-ized content checklist for the pediatrics hand-off protocol (Figure 5 page 653) For example adminis-trative data or medications constitute large categorieswhereas name room number and admitting team orservice compose smaller subcategories under adminis-trative data Many programs may already use a templatefor written content which may facilitate the creation ofcategories and subcategories of content The checklist
will be perceived as more credible if it reflects technicaljargon or refers to organizational or program-specificnomenclature used in daily patient care For this reasoneliciting specific examples for how information is com-municated during the interview is particularly helpfulOperator experiencemdashthe experience of those partici-pating in the handoffmdashcan influence the design of thechecklist For example experienced physicians in hospi-tal practice may not require the extensive checklist usedby new interns Finally an acronym can serve as areminder for critical content but also as a motivationaltool to learn the new protocol14 For example theacronym we used for the checklist for psychiatry resi-dents was ldquopsychiatryrdquomdashrepresenting psychiatric histo-ry special instructions for you for me (the to-do list)courtlegal issues housing and social issues ifthenadministrative data and allergies therapeutics resultsof pertinent labs and radiology
Discuss Implementation StrategiesAn implementation plan begins with dissemination of
both the process map and the checklist of necessary con-tent Using an opinion leader in a residency program suchas a chief resident or program director can help facilitate
Figure 2 The hand-off process map for neurology is shown PGY postgraduate year
Process Map for Neurology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

648November 2006 Volume 32 Number 11
another given each disciplinersquos unique requirementsFurthermore what constitutes an effective handoff forone discipline may be different for the same discipline inanother organization Although certain components maybe generalizable the successful adoption of a standard-ized hand-off protocol is highly dependent on the degreeto which it is tailored for end users in an organizationalsetting It is the method by which you create the proto-colmdashand the method that is presented heremdashthat is gen-eralizable across disciplines and organizations
Second standardization is the core goal for bothhand-off process and content For example although anidentifiable safe protocol may be currently in use for themajority of handoffs in a certain discipline and organiza-tion it is the variability of the hand-off protocol that isthe target for improvement The four steps in our modelare outlined in Table 1 (above) and discussed in detailbelow
Develop a Standardized ProcessldquoThe first step is to draw a flow diagram Then every-
one understands what his job is If people do not see the
process they cannot improve itrdquo mdash WE Deming
Understanding handoffs as a process is importantbecause a high degree of process awareness often drivesthe design of the work By mapping the process themembers of the team can gain insight into how their col-leagues perceive the same tasks Ultimately systemsimprovement requires (1) appreciating the inherent linkbetween process and results and (2) identifying potentialareas for improvement with a focus on the system that is
producing the processes and outcomes of care11 ratherthan on the individual
Process mapping can be used to describe and analyzehow an individual clinician interacts with the system aswell as with others within that system Process mappingdescribes what an individual is required to do in termsof cognitive processes andor actions to achieve the sys-temrsquos goal It can be accomplished through observationsandor interviews that carefully break down the multiplesteps in the process
Process maps can be created at different levels ofgranularity from a high-level overview of the major stepsin the process to very detailed representation of eachspecific step or activity Detailed process maps are espe-cially helpful to standardize and improve processes Foruse as an improvement tool it is important to map thecurrent process not the desired process so that oppor-tunities for improvement can be identified Being explic-it about the processes can help clinicians shape whatthey know about their environment and to provideinsight into how to improve the process or overcomesome of the barriers
Everyday multiple types of handoffs occur in healthcare settings such as handoffs around shift changes ofnursing shifts referrals to specialty care and dischargefrom inpatient to outpatient care We found it valuableto select only one type of handoff for the process analy-sismdashthe handoff from postcall residents to on-call resi-dents This transition represents the period of time thata patient is cared for by a ldquocoveringrdquo resident who maybe unfamiliar with the patientrsquos hospital course aknown risk factor for preventable adverse events12 Inaddition our earlier work suggested that this handoffwas particularly vulnerable with the implementation ofrecent ACGME duty-hour restrictions5 The particularquestion that we posed to residents in the process map-ping exercise was ldquoHow does a postcall resident trans-fer the care of their patients to an oncoming residentrdquoWe specifically asked how the contentmdashthe criticalinformation required to care for patients during thecoverage periodmdashis transferred We also asked resi-dents to delineate the mechanism by which the on-coming resident formally accepts care of the patients(that is the oncoming resident starts accepting callsfrom a ldquovirtual pagerrdquo when they are on call postcall
1 Process
Create a process map
2 Content
Create a standard check-list
3 Implementation
Garner leadership and resident buy-in
4 Monitoring
Ensure the protocol is in place and identify andresolve barriers
Table 1 Model for Adoption of aStandardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
649
resident forwards their pager to the oncoming residentand so on)
Figure 1 (above) includes a process mapping tutori-al that was used during the hand-off clinic Samplehand-off process maps for neurology and otolaryngolo-gy are included in Figure 2 (page 650) and Figure 3(page 651) respectively To analyze process maps sev-eral questions are important to address to generateimprovement ideas What is the goal of the process Does the process work as it should Are there obvious redundancies or complexities How different is the current process from the idealprocess
Although mapping the process is an important step indocumenting the standardized protocol for handoffs itcan also be instrumental in educating new interns aboutthe process Furthermore a process map can form thebasis of the performance measurement tool to monitorand assess adherence to the process
Build a Checklist of Necessary ContentIn addition to developing a standardized process it is
equally important to determine the critical content to betransferred in a patient handoff13 Omissions of contentare a major cause of failed communication during hand-offs5 A checklist of necessary information can helpteach others new to the handoff about the process and
November 2006 Volume 32 Number 11
Figure 1 This process mapping tutorial was used during the hand-off clinic
Process Map Tutorial
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
650November 2006 Volume 32 Number 11
serve as a monitoring tool in evaluating the contenttransferred In designing a checklist it is important tocustomize it for a specific discipline
When thinking about what content to include in achecklist one helpful tool is to interview the participantsin the hand-off process regarding the information thatthey desire or need (Figure 4 page 652) A good startingpoint is to ask the following question ldquoWhat are the maincontent pieces of a handoff in your disciplinerdquo Theanswers will likely result in a list of necessary patientcontent A more detailed interview can elicit content thatis part of an optimal handoff in addition to content thatmay be omitted in a suboptimal handoff To convert thiscontent into a checklist it is important to group this listinto larger categories of content and smaller subcate-gories in each major category as shown in the standard-ized content checklist for the pediatrics hand-off protocol (Figure 5 page 653) For example adminis-trative data or medications constitute large categorieswhereas name room number and admitting team orservice compose smaller subcategories under adminis-trative data Many programs may already use a templatefor written content which may facilitate the creation ofcategories and subcategories of content The checklist
will be perceived as more credible if it reflects technicaljargon or refers to organizational or program-specificnomenclature used in daily patient care For this reasoneliciting specific examples for how information is com-municated during the interview is particularly helpfulOperator experiencemdashthe experience of those partici-pating in the handoffmdashcan influence the design of thechecklist For example experienced physicians in hospi-tal practice may not require the extensive checklist usedby new interns Finally an acronym can serve as areminder for critical content but also as a motivationaltool to learn the new protocol14 For example theacronym we used for the checklist for psychiatry resi-dents was ldquopsychiatryrdquomdashrepresenting psychiatric histo-ry special instructions for you for me (the to-do list)courtlegal issues housing and social issues ifthenadministrative data and allergies therapeutics resultsof pertinent labs and radiology
Discuss Implementation StrategiesAn implementation plan begins with dissemination of
both the process map and the checklist of necessary con-tent Using an opinion leader in a residency program suchas a chief resident or program director can help facilitate
Figure 2 The hand-off process map for neurology is shown PGY postgraduate year
Process Map for Neurology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

649
resident forwards their pager to the oncoming residentand so on)
Figure 1 (above) includes a process mapping tutori-al that was used during the hand-off clinic Samplehand-off process maps for neurology and otolaryngolo-gy are included in Figure 2 (page 650) and Figure 3(page 651) respectively To analyze process maps sev-eral questions are important to address to generateimprovement ideas What is the goal of the process Does the process work as it should Are there obvious redundancies or complexities How different is the current process from the idealprocess
Although mapping the process is an important step indocumenting the standardized protocol for handoffs itcan also be instrumental in educating new interns aboutthe process Furthermore a process map can form thebasis of the performance measurement tool to monitorand assess adherence to the process
Build a Checklist of Necessary ContentIn addition to developing a standardized process it is
equally important to determine the critical content to betransferred in a patient handoff13 Omissions of contentare a major cause of failed communication during hand-offs5 A checklist of necessary information can helpteach others new to the handoff about the process and
November 2006 Volume 32 Number 11
Figure 1 This process mapping tutorial was used during the hand-off clinic
Process Map Tutorial
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
650November 2006 Volume 32 Number 11
serve as a monitoring tool in evaluating the contenttransferred In designing a checklist it is important tocustomize it for a specific discipline
When thinking about what content to include in achecklist one helpful tool is to interview the participantsin the hand-off process regarding the information thatthey desire or need (Figure 4 page 652) A good startingpoint is to ask the following question ldquoWhat are the maincontent pieces of a handoff in your disciplinerdquo Theanswers will likely result in a list of necessary patientcontent A more detailed interview can elicit content thatis part of an optimal handoff in addition to content thatmay be omitted in a suboptimal handoff To convert thiscontent into a checklist it is important to group this listinto larger categories of content and smaller subcate-gories in each major category as shown in the standard-ized content checklist for the pediatrics hand-off protocol (Figure 5 page 653) For example adminis-trative data or medications constitute large categorieswhereas name room number and admitting team orservice compose smaller subcategories under adminis-trative data Many programs may already use a templatefor written content which may facilitate the creation ofcategories and subcategories of content The checklist
will be perceived as more credible if it reflects technicaljargon or refers to organizational or program-specificnomenclature used in daily patient care For this reasoneliciting specific examples for how information is com-municated during the interview is particularly helpfulOperator experiencemdashthe experience of those partici-pating in the handoffmdashcan influence the design of thechecklist For example experienced physicians in hospi-tal practice may not require the extensive checklist usedby new interns Finally an acronym can serve as areminder for critical content but also as a motivationaltool to learn the new protocol14 For example theacronym we used for the checklist for psychiatry resi-dents was ldquopsychiatryrdquomdashrepresenting psychiatric histo-ry special instructions for you for me (the to-do list)courtlegal issues housing and social issues ifthenadministrative data and allergies therapeutics resultsof pertinent labs and radiology
Discuss Implementation StrategiesAn implementation plan begins with dissemination of
both the process map and the checklist of necessary con-tent Using an opinion leader in a residency program suchas a chief resident or program director can help facilitate
Figure 2 The hand-off process map for neurology is shown PGY postgraduate year
Process Map for Neurology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

650November 2006 Volume 32 Number 11
serve as a monitoring tool in evaluating the contenttransferred In designing a checklist it is important tocustomize it for a specific discipline
When thinking about what content to include in achecklist one helpful tool is to interview the participantsin the hand-off process regarding the information thatthey desire or need (Figure 4 page 652) A good startingpoint is to ask the following question ldquoWhat are the maincontent pieces of a handoff in your disciplinerdquo Theanswers will likely result in a list of necessary patientcontent A more detailed interview can elicit content thatis part of an optimal handoff in addition to content thatmay be omitted in a suboptimal handoff To convert thiscontent into a checklist it is important to group this listinto larger categories of content and smaller subcate-gories in each major category as shown in the standard-ized content checklist for the pediatrics hand-off protocol (Figure 5 page 653) For example adminis-trative data or medications constitute large categorieswhereas name room number and admitting team orservice compose smaller subcategories under adminis-trative data Many programs may already use a templatefor written content which may facilitate the creation ofcategories and subcategories of content The checklist
will be perceived as more credible if it reflects technicaljargon or refers to organizational or program-specificnomenclature used in daily patient care For this reasoneliciting specific examples for how information is com-municated during the interview is particularly helpfulOperator experiencemdashthe experience of those partici-pating in the handoffmdashcan influence the design of thechecklist For example experienced physicians in hospi-tal practice may not require the extensive checklist usedby new interns Finally an acronym can serve as areminder for critical content but also as a motivationaltool to learn the new protocol14 For example theacronym we used for the checklist for psychiatry resi-dents was ldquopsychiatryrdquomdashrepresenting psychiatric histo-ry special instructions for you for me (the to-do list)courtlegal issues housing and social issues ifthenadministrative data and allergies therapeutics resultsof pertinent labs and radiology
Discuss Implementation StrategiesAn implementation plan begins with dissemination of
both the process map and the checklist of necessary con-tent Using an opinion leader in a residency program suchas a chief resident or program director can help facilitate
Figure 2 The hand-off process map for neurology is shown PGY postgraduate year
Process Map for Neurology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

651
this process During the dissemination phase other resi-dent physicians should be able to provide input into boththe process and the checklist The importance of produc-ing tangible documentsmdashthat is the process map andchecklistmdashcannot be understated These documents canbe distributed for everyonersquos input and clarification andcan help facilitate input on the hand-off protocol Forexample are there other steps that are missing Is thecontent checklist inclusive of the information neededThis input may dramatically improve the integrity andfuture buy-in of the standardized hand-off protocol
Keeping a record of the input or suggested revisionsand the response is important Once a general consensusis reached the process map and the checklist can berevised to incorporate suggested revisions The newprocess map and checklist can then be distributed andused to educate students and residents on the handoffThese documents can also be particularly helpful whenorienting new residents or students to the discipline
Develop a Plan for Monitoring and EvaluationTo determine the success of implementing a stan-
dardized hand-off protocol it is crucial that a plan formonitoring and evaluation be developed Choosing an evaluation strategy can be challenging The common-ly accepted gold standard of patient outcomes may be
particularly costly and difficult to determine More read-ily accessible measures such as stakeholder satisfactionand peer ratings of the quality of the hand-off processcan also be considered In addition periodic reviews ofthe handoff content and process through direct observa-tion can be performed using the process map and stan-dardized checklist Although direct observation may besubject to the Hawthorne effect using a variety of strate-gies to evaluate handoffs will address this concern Forexample in retrospective interviews participants arequeried regarding the quality of the process and contentof the handoff In a recent study critical incident analy-sis was used to ask residents if they had any difficultycaring for patients as a result of a poor sign-out beforetheir shift or duty5 An evaluation plan should alsoinclude sharing the information learned with the partici-pants of the process to solicit more improvements sug-gestions or comments on observed deficiencies Inessence this becomes a closed-loop process by whichhandoffs can be the target of continuous qualityimprovement efforts
Findings from the University of ChicagoHospitalsWe offered the hand-off clinic to individual residenciesthat take in-house call on an inpatient service The
November 2006 Volume 32 Number 11
Figure 3 The hand-off process map for otolaryngology is shown PGY postgraduate year
Process Map for Otolaryngology Standardized Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

652November 2006 Volume 32 Number 11
workshop employs a semistructured interview of resi-dents to do the following Develop a standardized process for the handoff usinga process mapping methodology Create a checklist of critical patient content Plan for dissemination and training
To date 7 of 10 residency programs have participatedWe used process analysis to highlight similarities differ-ences and areas for improvement among protocols Thehand-off process is highly variable and discipline-specif-ic Several themes emerged as highlighted in the follow-ing sections
Themes from the Process AnalysisRespect the Disciplinersquos Environment Culture
and Needs To tailor the hand-off protocol to its usersthe local environment in which the handoff is occurring(for example intensive care unit emergency room) andthe type of patients cared for need to be taken intoaccount
Although four of the seven residency programs hada designated hand-off location the other three con-ducted handoffs wherever convenient For exampleobstetrics and gynecology and psychiatry have an offi-cial meeting time and a dedicated room for handoffswhereas internal medicine handoffs occur wheneverconvenient for the on-call resident (for example emer-gency room call room ward) Only two programs hadmore senior residents present at the handoff althoughfor all seven programs senior residents andor attend-ings (usually during morning rounds or shortly after)provided input to the content of written sign-out sheetsused at the time of the handoff Similarly although con-tent checklists all contained some form of administra-tive data (for example patient name medical recordnumber room number) certain disciplines requiredunique elements of content For example pediatricssign-outs contained fields to describe custodialarrangements (for example parents statersquos office forchild and family services) whereas surgical sign-outs
Figure 4 Interviewing participants in the hand-off process regarding the information that they desire or need can
inform development of a hand-off checklist
Checklist Interview for Standard Handoff
1 Are there categories of content on a template that your programdiscipline usesIF YES For each category what is an example of what is said (or written) or a common patient careissue that occurs that this content is used for
2 In thinking about a time you participated (or observed) a ldquogoodrdquo handoff what types of informa-tion did you receive How was it helpful in caring for a patient or performing your dutyPROBE FOR ANY BIG CATEGORIES OF CONTENT What would staff say (or write) Can you give mesome specific examples
3 In thinking about a time you participated (or observed) a ldquopoorrdquo handoff what types of informationwere missing or inadequate How did it impair your ability to take care of patients or perform yourduty PROBE FOR ANY BIG CATEGORIES OF CONTENT What would you wish staff would have said (or written) Can you give me some specific examples
Write the names of all of the big categories that emerged on the back of this sheet Group like categories(to decrease redundancy) and think of a checklist acronym
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

653November 2006 Volume 32 Number 11
Figure 5 The standardized content checklist for the pediatrics hand-off protocol is shown GI gastrointestinal Pulm
pulmonary g gastrostomy trach tracheotomy CT computerized tomography HTN hypertension NPO nothing by
mouth IVF intravenous fluid Hgb hemoglobin Hct hematocrit PIV peripheral intravenous
Standardized Content Checklist for Pediatric Handoff
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

654November 2006 Volume 32 Number 11
contained fields for pre-operative and postoperativechecks Residents in one program described ldquoinforma-tion overloadrdquo and ldquobeing a slaverdquo to continuous updat-ing of the written sign-out A resident in a differentprogram stated that handoffs only occurred if acutepatient issues were present
Despite these variations all seven participating residency specialties use both a written summary orsign-out and a verbal exchange to execute a handoffHowever the amount of information recorded on thewritten sign-out and discussed at the verbal exchangediffer Cognitive-based specialties such as internal medi-cine and psychiatry appear to have a longer written sign-out sheet and a longer verbal exchange for each patientMeanwhile procedure-based specialties such as ortho-pedic surgery appear to have a more concise writtensign-out with verbal exchange for only those patientswith active issues
Aim to Understand and Reduce Variation
Although most residency program chief residents couldarticulate a protocol that was routinely followed theyalso referred to deviations from the protocol For exam-ple whereas all residents interviewed stated that verbalcommunication was required and should occur at thetime of the hand-off all residents acknowledged that itdid not always occur One surgical resident statedldquosometimes the on-call resident [receiving handoff] is inthe operating roomrdquo Indeed the most common causefor the exceptions was the competing demands of resi-dent work such that one of the participants was in theoperating room clinic in transit to or from an off-siteclinic or otherwise unavailable for a handoff Howeverat least one program chief stated that some residentscoming on duty were more likely to make themselvesavailable for verbal communication at the time of thehandoff than others
Highlight the Handoff as the Transfer of
Professional Responsibility The handoff is morethan just transfer of informationmdashit is also a transferof professional responsibility It is crucial that thehandoff indicate a clear transfer of professionalresponsibility When the transfer of professionalresponsibility occurs at the time or close to the time ofthe transfer of information this process is transparentand easily understood However in many cases the
transfer of professional responsibility was separated intime and space from the transfer of information Thisseparation can occur through a variety of differentmechanisms For example some residencies such as psychiatry designate a certain time at which the incoming residents actively transfer responsibilityof patients to themselves The on-call psychiatry resi-dent who starts at 530 pm transfers a virtual pagerto his or her own pager By contrast for other pro-grams departing residents may transfer their responsi-bility to someone else In the internal medicineresidency program departing residents forward theirpager to the on-call resident after they provide a verbalhandoff
Detect and Correct Vulnerabilities in the
Handoff A process map can be useful in assessing theintegrity of the handoff process By visualizing eachstep vulnerabilities in the process can be detected andimproved as occurred in the neurology and pediatricresidency programs Patient tasks were assigned toother team members to facilitate timely departure of a postcall resident to comply with resident duty-hour restrictions However in both cases no distinctmechanism was in place to communicate follow-up of these tasks such as their completion or results tothe on-call intern After examining the process maps the chief residents incorporated closed-loop communi-cation requiring that follow-up that was dividedamong the medical team be relayed back to the on-callresident
Implementation of the University of ChicagoHospitals Standardized Hand-off Protocols
Buy-in from senior leadership of stakeholders and ongoing education has been instrumental to theimplementation of standardized hand-off protocolsBecause this work deals with resident education andpatient care two stakeholders important to the success of implementation are the hospital leadershipand leaders of graduate medical education such asdeans and program directors With the support of the department of patient safety in March 2006 we presented this initiative to the patient care committeea subgroup of the hospitalrsquos board of trustees whichincluded senior institutional leaders We also briefed
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations
655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations

655
all residency and fellowship program directors at theinstitutionrsquos graduate medical education retreat inNovember 2005 At this briefing we reviewed the JointCommission National Patient Safety Goal and key lit-erature and introduced our model for a standardizedhand-off protocol A few days later with the assistanceof the department of patient safety we contacted thechief residents (by e-mail and pager) to schedule thehand-off clinics On its completion all participantsagreed that the protocol would help improve currenthand-off mechanisms and facilitate education of newinterns
The standardized protocols accompanied by anexplanation of the new National Patient Safety Goalwere disseminated to all incoming house staff duringthe orientation for new interns in June 2006 Residencyprograms are now expected to provide in-service ses-sions to their residents on the discipline-specific hand-off protocols during each academic year We continue towork with those residency programs that have not yetdeveloped standardized hand-off protocols and areexpanding our focus to nursing and other types of inter-disciplinary handoffs To date the major barrier for participation in the hand-off clinic is scheduling a timethat is convenient within the restraints of the residentsrsquoservice obligations To develop a formal monitoring and
evaluation process we have partnered with the IllinoisHospital Associationrsquos 18-month Patient Safety LearningCollaborative on Handoffs which currently has repre-sentatives from 26 Illinois hospitals
ConclusionThe model to standardize the handoff has the potentialto result in improved patient care Mapping the processand building a standardized checklist of content canfacilitate meeting the Joint Commission National PatientSafety Goal Using opinion leaders and involving resi-dents can be crucial to the success of disseminating thestandardized hand-off protocol to resident physicians inan academic teaching hospital
We thank the residents chief residents and program directors whohave participated in this initiative and Michelle Johnson RN BSNMBA and Krista Curell JD RN from the Department of PatientSafety and Risk Management at the University of Chicago Hospitals fortheir assistance with this initiative
J
November 2006 Volume 32 Number 11
1 Accreditation Council for Graduate Medical Education Resident
Duty Hours and the Working Environment httpwwwacgmeorgacWebsitedutyHoursdh_Lang703pdf (last accessed Sep 5 2006) 2 Fletcher KE Saint S Mangrulkar RS Balancing continuity of carewith residentsrsquo limited work hours Defining the implications Acad
Med 8039ndash43 Jan 20053 Volpp KG Grande D Residentsrsquo suggestions for reducing errors inteaching hospitals N Engl J Med 348851ndash855 Feb 27 20034 Cook RI Render M Woods DD Gaps in the continuity of care andprogress on patient safety BMJ 320791ndash794 Mar 18 20005 Arora V et al Communication failures in patient signout and sug-gestions for improvement a critical incident analysis Qual Saf Health
Care 14401ndash407 Dec 20056 Joint Commission on Accreditation of Healthcare Organizations2007 National Patient Safety Goals Hospital Version Manual
Chapter including Implementation Expectations httpwwwjointcommissionorgPatientSafetyNationalPatientSafeyGoals07_hap_cah_npsgshtm (last accessed Sep 5 2006) 7 Solet DJ et al Lost in translation Challenges and opportunities inphysician-to-physician communication during patient handoffs Acad
Med 801094ndash1099 Dec 2005
8 Horwitz LI et al Transfers of patient care between house staff oninternal medicine wards a national survey Arch Intern Med
1661173ndash1177 Jun 12 2006 9 Patterson ES et al Handoff strategies in settings with high conse-quences for failure Lessons for health care operations Int J Qual
Health Care 16125ndash132 Apr 200410 University HealthSystem Consortium (UHC) Best Practice
Recommendation Patient Hand Off Communication Oakbrook ILUHC White Paper May 2006 11 Mohr J Forming Operating and Improving Microsystems of Care(PhD diss) Hanover NH Center for the Evaluative ClinicalSciences Dartmouth College 2000 12 Petersen LA et al Does housestaff discontinuity of care increasethe risk for preventable adverse events Ann Intern Med 121866ndash872Dec 1 199413 Vidyarthi A et al Managing discontinuity to mitigate patientharm Strategies for a safe and effective sign-out J Hosp Med
1257ndash266 JulAug 200614 Stalder DR Learning and motivational benefits of acronym usein introductory psychology Teaching of Psychology 32(4)222ndash2282005
References
Vineet Arora MD MA is Assistant ProfessorDepartment of Medicine University of Chicago and JulieJohnson MSPH PhD is Assistant ProfessorDepartment of Medicine University of Chicago andDirector of Research American Board of MedicalSpecialties Evanston Illinois Please address correspon-dence to Vineet Arora varoramedicinebsduchicagoedu
Copyright 2006 Joint Commission on Accreditation of Healthcare Organizations