-
spine
J Neurosurg Spine Volume 23 • July 2015
caSe reportJ Neurosurg Spine 23:81–85, 2015
SchwannomaS in the presacral space are a rare vari-ant of these
neural tumors;6,9 by virtue of their loca-tion, they can cause a
variety of symptoms related mainly to their mass effect. They are
most often resected laparoscopically or, in the case of larger
masses, by lapa-rotomy.13 Unique patient circumstances, such as
morbid obesity, risk of hemorrhage, and previous morbidity, can
preclude these “traditional” approaches to resection. We report the
case of a presacral schwannoma resected via a minimally invasive
paracoccygeal exposure using tubular retractors and endoscopy—an
approach not previously de-scribed.
case reportHistory and Examination
A 49-year-old man with a history of worsening chronic low-back
pain and difficulty urinating had a presacral, solid, homogeneously
enhancing mass on MRI. A follow-up scan 3-months later revealed an
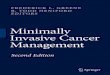
increase in tumor size.
Located to the left of the midline at the junction of S-1 and
S-2, the tumor had enlarged to 8 cm in diameter (Fig. 1).
The patient’s medical history included hypertension, Type 2
diabetes mellitus, morbid obesity (body mass index 41.5 kg/m2),
previous bilateral L4–5 and L5–S1 rhizoly-sis, and a previous
laparoscopic cholecystectomy. Given his body habitus, a
laparoscopic transperitoneal approach was recommended, but
morbidity from a previous laparo-scopic surgery led the patient to
refuse this approach. Con-sidering the anatomical location of the
tumor, the shortest route to the lesion was a pericoccygeal
approach, which would be easiest to perform using a minimally
invasive method with tubular retractors. Moreover, the patient’s
re-ligion precluded the use of blood products since he was a
Jehovah’s Witness.
OperationInformed consent was obtained, which included the
possibility of converting to an open procedure, if needed. The
patient was anesthetized, intubated, and placed in the
Submitted April 17, 2014. accepted November 12, 2014.iNclude
wheN citiNg
Published online April 24, 2015; DOI: 10.3171/2014.11.SPINE14396.diScloSure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper. Dr. Mendez has received teaching and product development consulting honoraria from Medtronic.
A minimally invasive pericoccygeal approach to resection of a
large presacral schwannoma: case reportosa emohare, mbbS, phd,
molly Stapleton, mS, pa-c, and alejandro mendez, md
Department of Neurosurgery, Regions Hospital, St. Paul, Minnesota
Resection of large presacral schwannomas can present a challenge. The posterior approach is commonly associated with coccygeal disarticulation, partial sacral resection, and muscular disarticulation, which can all result in significant morbidity. Minimally invasive surgery may obviate some of the morbidity traditionally associated with this approach. The authors present the case of a morbidly obese 49-year-old man with an enlarging presacral schwannoma. The patient refused laparoscopic resection because of the morbidity he had experienced with a previous laparoscopic surgery. The tumor was resected using a minimally invasive paracoccygeal approach, which affords improved access with minimal morbidity.http://thejns.org/doi/abs/10.3171/2014.11.SPINE14396Key
wordS
disarticulation; laparoscopic surgery; presacral schwannoma; surgical procedures; minimally invasive; sacral
81©AANS, 2015
Unauthenticated | Downloaded 06/08/21 12:08 PM UTC
-
o. emohare, m. Stapleton, and a. mendez
J Neurosurg Spine Volume 23 • July 201582
lateral decubitus position, with his right side up.
Antero-posterior and lateral fluoroscopy was used to guide the
location of the incision, which was about 6 cm long in the
pericoccygeal approach and about 4 cm lateral to the anus and 3–4
cm cephalic to it. The sacro-pelvic and coccygeal-pelvic ligaments
were exposed. The inferior fibers of these ligaments were released,
and with gentle blunt dissection, a surgical corridor was created
in the presacral space, anterior and cephalic to the ligaments.
Dilators were ad-vanced, a Medtronic direct lateral interbody
fusion retrac-tor system (Medtronic Sofamor Danek) was positioned,
and the retractor was secured to a table-mounted holder.
Neuromonitoring and a direct nerve stimulator were used during this
case. Prior to any cut or dissection, we would stimulate so as not
to damage any nerve roots.
The tubular retractor was slightly opened, allowing fur-ther
visualization of the inferior right-sided margin of the
tumor. We commenced endoscopic resection using a 0°
high-definition rhinoscope. The tumor had the character-istic
rubbery consistency of a schwannoma. It was cored using endoscopic
instruments, and electrocautery scissors were used to cut through
the capsule. Pituitary rongeurs were used to core the center of the
tumor, and dissectors were used to develop the tumor margin. During
surgery, we were able to stimulate the S-1 nerve root where the
tumor originated. The margins were clear, with a good plane and no
evidence of infiltration; they were peeled away, and brisk bleeding
was encountered from a branch of the iliac vein. Hemostasis was
ultimately obtained with bipolar cautery, compression, and Floseal
hemostatic ma-trix (Baxter Inc.). The patient remained
hemodynamically stable throughout. Once the bleeding was completely
con-trolled, residual edges of the tumor were removed and the
excision was completed. A drain was placed at the exci-sion site,
and the wound was closed in layers. Total surgi-cal time was 4
hours 9 minutes. Estimated blood loss was 1300 ml. The patient
awoke with no neurological deficits.
Postoperative CourseHis postoperative course was uneventful; he
main-
tained a hemoglobin level > 11 g/dl and was ambulating on
postoperative Day 1. The drain was removed, and the patient was
discharged on postoperative Day 4. Subse-quent pathology revealed
that the tumor stained diffusely positive for S100 and was negative
for smooth muscle ac-tin and CD34, and a low Ki 67 index was noted,
in keep-ing with a diagnosis of schwannoma. Postoperative MRI
showed gross-total resection with some peri-resection site changes.
The patient had a rapid recovery with no com-plications. Follow-up
MRI at 12 months showed the reso-lution of all postoperative
changes, with no evidence of residual tumor (Fig. 2).
discussionAlthough schwannomas are commonly slow growing
and painless, the mass effect of presacral schwannomas usually
constitutes the surgical indication. Patients with these lesions
are most often in their 2nd to 5th decades of life and tend to be
female.13,15 In the absence of a syn-dromic component to the tumor,
such as von Reckling-hausen’s disease, recurrence or malignant
transformation is unlikely, meaning that extensive resection is
curative.2,13 The lack of invasive growth exhibited by these tumors
and their thick capsular lining make presacral schwan-nomas
amenable to complete resection.4,7,9 Preoperative biopsy was not
performed in our featured case given the benign-appearing features
of the tumor, although there are divergent views regarding biopsy
for more atypical tumors.1 Generally, 3 potential approaches have
been de-scribed for presacral tumor resection: anterior or
abdomi-nal (whether open or laparoscopic), posterior, or a
com-bination.3,14,17 Resection of these tumors is increasingly
performed using laparoscopic techniques,12,17 although open
laparotomy may be performed in the case of larger tumors.14 A more
recent series advocated a posterior ap-proach to avoid the
abdominal morbidity associated with
Fig.
1. Axial (upper) and sagittal (lower) preoperative MR images of a mass lesion located in the presacral space.
Unauthenticated | Downloaded 06/08/21 12:08 PM UTC
-
pericoccygeal schwannoma resection
J Neurosurg Spine Volume 23 • July 2015 83
an anterior approach.14 Although the tumors presented in that
series were broadly comparable with the current case in terms of
their dimensions, most cases seemed to require disarticulation of
the coccyx and resection of part of the sacrum. The posterior
approach, in which a patient is placed in the prone jackknife
position, with excision of the coccyx, can be associated with
significant periopera-tive morbidity; in this context, extensive
sacral resection is not uncommon and has an attendant potential for
func-tional impairment.5,8,10,11 With this approach, neurological
dysfunction, especially neurogenic bladder, is the most frequently
reported complication,5,10,11 although infective complications,
hemorrhage, dysesthesia, and stool incon-tinence have also been
encountered.11 It has been report-
ed that lower sacral resections are associated with fewer
complications, as no permanent neurological morbidity has occurred
in patients whose sacral resection was be-low S-2.5 The coccyx may
be disarticulated either alone or with the attachment of the
gluteus maximus; when this happens, it is usually in combination
with a sacrectomy at the level of S4–5.8,16
The utility of the paracoccygeal approach has been examined,3 as
has the potential for detaching the coccyx, gluteus maximus, and
part of the sacrum. The patients and cadavers studied were
positioned in either the prone jackknife position or a lithotomy
position. In addition, the anococcygeal ligament and the levator
ani muscle were divided to enter the supra-levator space.3 The
minimally invasive paracoccygeal approach we present may reduce the
need for bony resection and is especially germane be-cause the
patient’s religious circumstances limited the op-tions for managing
morbidity or hemodynamic instability.
In this report, we presented a less destructive, less in-vasive
approach to these tumors. Because of the patient’s morbid obesity,
the transabdominal route was not ideal, and he opposed laparoscopy.
With the tumor located high in the presacral space, the traditional
posterior ap-proach would have required extensive sacral resection.
Our choice of directional approach was made because it is easier to
address pathology on the opposite ventral as-pect of the sacrum,
crossing the midline. This provides a view perpendicular to the
apex of the tumor as opposed to the tangential view obtained using
an ipsilateral approach (Figs. 3 and 4). The paracoccygeal approach
has been re-fined over the last 10–15 years with the introduction
of the axial presacral lumbar interbody fusion system (Axi-aLIF,
TranS1 Inc.). This approach provides quick, mini-mally invasive
access to the anterior junction of S1–2 with less morbidity while
the patient is prone. Modifications we made to this technique
included putting the patient in a lateral decubitus position to
allow the viscera to fall for-ward, away from the resection site,
and to decrease venous congestion. We worked from the right side
across the an-terior surface of the sacrum, with the tumor on the
left side, which provided a panoramic view of the inferior and
medial aspects of the tumor and allowed full visualization by
simply modifying the position of the retractor system a few degrees
at a time.
As in most minimally invasive endoscopic resections, the tumor
excision technique is different from the stan-dard open approach.
Here, the idea is to core the center of the tumor as much as
possible and then to let the thin residual skin collapse inward,
only then creating a plane between the tumor and adjacent tissues.
In our patient, the resection went extraordinarily well until we
created a vas-cular injury with significant blood loss. This is
something anyone attempting this technique should be aware of. It
took some time to control, working through a port 23 mm in diameter
and 15 cm long. Ultimately, we were able to control the bleeding
with no harm to the patient. When bleeding is encountered, possible
approaches to achieve hemostasis include using laparoscopic
hemostatic clips, long bipolar probes, electrocautery laparoscopic
scissors, and laparoscopic or thoracoscopic harmonic scalpels. The
first 3 tools were used in the present case. Postoperative
Fig.
2. Axial (upper) and sagittal (lower) MR images obtained at 12 months postoperatively, showing the absence of a mass lesion.
Unauthenticated | Downloaded 06/08/21 12:08 PM UTC
-
o. emohare, m. Stapleton, and a. mendez
J Neurosurg Spine Volume 23 • July 201584
imaging at 3 and 12 months demonstrated patency in the iliac
vein.
This technique remains in its infancy and requires fur-ther
development, such as the use of a laparoscopic har-monic scalpel or
laparoscopic vascular clips. A current limitation is patient
selection, as it is not appropriate for patients with previous
surgery in the area, those with peri-rectal pathology including
Crohn’s disease, potentially those with ulcerative colitis, and
those with abnormal vas-cular anatomy. Finally, the technique
provides a limited view of the sacral foramina, thus limiting its
application for extraforaminal tumors. Despite these shortcomings,
we believe it is an exciting and potentially very useful ap-proach
to presacral pathology.
conclusionsIn summary, presacral schwannoma is an uncommon
pathology that, in most cases, is resected abdominally. With
appropriate patient selection, a minimally invasive paracoccygeal
approach may offer minimal morbidity and relatively good
access—especially in morbidly obese pa-tients and those with
multiple comorbid conditions.
references 1. Bennert KW, Abdul-Karim FW: Fine needle
aspiration
cytology vs. needle core biopsy of soft tissue tumors. A
com-parison. Acta Cytol 38:381–384, 1994
2. Brady KA, McCarron JP Jr, Vaughan ED Jr, Javidian P: Be-nign
schwannoma of the retroperitoneal space: case report. J Urol
150:179–181, 1993
3. Buchs N, Taylor S, Roche B: The posterior approach for low
retrorectal tumors in adults. Int J Colorectal Dis 22:381–385,
2007
4. Canelles E, Roig JV, Cantos M, García Armengol J, Barreiro E,
Villalba FL, et al: [Presacral tumors. Analysis of 20 surgi-cally
treated patients.] Cir Esp 85:371–377, 2009 (Span)
5. Cody HS III, Marcove RC, Quan SH: Malignant retrorectal
tumors: 28 years’ experience at Memorial Sloan-Kettering Cancer
Center. Dis Colon Rectum 24:501–506, 1981
6. Daneshmand S, Youssefzadeh D, Chamie K, Boswell W, Wu N,
Stein JP, et al: Benign retroperitoneal schwannoma: a case series
and review of the literature. Urology 62:993–997, 2003
7. Dozois EJ, Jacofsky DJ, Dozois RR: Presacral tumors, in Wolff
BG, Fleshman JW, Beck DE, et al (eds): The ASCRS Textbook of
Colorectal Surgery. New York: Springer, 2007, pp 501–514
8. Hassan I, Wietfeldt ED: Presacral tumors: diagnosis and
management. Clin Colon Rectal Surg 22:84–93, 2009
9. Hughes MJ, Thomas JM, Fisher C, Moskovic EC: Imaging features
of retroperitoneal and pelvic schwannomas. Clin Radiol 60:886–893,
2005
10. Jackson RJ, Gokaslan ZL: Spinal-pelvic fixation in patients
with lumbosacral neoplasms. J Neurosurg 92 (1 Sup-pl):61–70,
2000
Fig.
3. Illustration of surgical approach to the tumor. Copyright Medical Surgical Illustration. Published with permission.
Fig.
4. Illustration of the anatomical relations of the tumor to neighbor-ing structures. Copyright Medical Surgical Illustration. Published with permission.
Unauthenticated | Downloaded 06/08/21 12:08 PM UTC
-
pericoccygeal schwannoma resection
J Neurosurg Spine Volume 23 • July 2015 85
11. Jao SW, Beart RW Jr, Spencer RJ, Reiman HM, Ilstrup DM:
Retrorectal tumors. Mayo Clinic experience, 1960-1979. Dis Colon
Rectum 28:644–652, 1985
12. Konstantinidis K, Theodoropoulos GE, Sambalis G, Geor-giou
M, Vorias M, Anastassakou K, et al: Laparoscopic resection of
presacral schwannomas. Surg Laparosc Endosc Percutan Tech
15:302–304, 2005
13. Mastoraki A, Toska F, Tsiverdis I, Kyriazi M, Tsagkas A,
Danias N, et al: Retroperitoneal schwannomas: dilemmas in
diagnostic approach and therapeutic management. J Gastro-intest
Cancer 44:371–374, 2013
14. Samarakoon L, Weerasekera A, Sanjeewa R, Kollure S: Gi-ant
presacral schwannoma presenting with constipation: a case report. J
Med Case Reports 6:285, 2012
15. White W, Shiu MH, Rosenblum MK, Erlandson RA, Wood-ruff JM:
Cellular schwannoma. A clinicopathologic study of 57 patients and
58 tumors. Cancer 66:1266–1275, 1990
16. Wolpert A, Beer-Gabel M, Lifschitz O, Zbar AP: The
man-agement of presacral masses in the adult. Tech Coloproctol
6:43–49, 2002
17. Yang CC, Chen HC, Chen CM: Endoscopic resection of a
presacral schwannoma. Case report. J Neurosurg Spine 7:86–89,
2007
author contributionsConception and design: Emohare, Mendez.
Acquisition of data: all authors. Analysis and interpretation of
data: Emohare, Mendez. Drafting the article: Emohare. Critically
revising the article: Emohare, Mendez. Reviewed submitted version
of manu-script: Emohare, Mendez. Approved the final version of the
man-uscript on behalf of all authors: Emohare.
Administrative/techni-cal/material support: all authors. Study
supervision: Mendez.
correspondenceOsa Emohare, Department of Neurosurgery, Regions
Hospital, 640 Jackson St., St. Paul, MN 55101. email:
[email protected].
Unauthenticated | Downloaded 06/08/21 12:08 PM UTC