Embed Size (px)
Citation preview

“A LITERARY STUDY OF MANSAVAHA SROTAS MOOLASTHANA AS
MENTIONED IN SUSHRUTA SAMHITA WITH SPECIAL REFERENCE TO
MODERN ANATOMY”
BY
DR. PRADNYA BHARAT PATIL MD Scholar
Dissertation submitted to the
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES KARNATAKA,
BANGALORE.
In partial fulfillment of the requirements for the degree of
AYURVEDA VACHASPATI
In
RACHANA SHAREERA
Under The Guidance of
Dr. RAHUL NITINALIAS RUGE MD (Ayu)
Associate Professor
Department of PG studies in Rachana Shareera
LATTHE EDUCATION SOCIETY'S
ACHARYA DESHABUSHAN AYURVEDIC MEDICAL COLLEGE
AND HOSPITAL, BEDHIKIHAL DIST- BELAGAVI
2017-2020







LIST OF ABBRAVATIONS USED
AÉ.U. ÌS AÉrÉÑuÉåïSè UWûxrÉ ÌSmÉÏMüÉç
Q. ÌlÉ. xÇÉ QûsWûlÉ ÌlÉoÇÉkÉç xÇÉaÉëWû
xÉÑ zÉÉ xÉÑ́ ÉÑiÉ zÉÉUÏUxjÉÉlÉ
ACL Anterior Crucial Ligament
ACL Anterior cruciate ligament
ASV AntiSnake Venom
DNA Deoxy Ribose Nucleic Acid
HIV Human Immunodeficiency virus
MCL Medial collateral ligament
mm millimeter
PCL Posterior cruciate ligament
PET Poly Ethylene Terephthalate
TB Tuberculosis
UV Ultra Violet
UVR Ultra Violet Radiation
UCL Ulnar collateral ligament
WSR with Special Reference

LIST OF TABLES
Sr.no Tables Page no
1
Type of skin,modern name,pramana
&adhishtana for disease
17
2
Types of tvaca according to different
tikakaras
18
3
Showing the comparison of thickness of
Tvaca according to Sushruta and
Dalhana
19
4
Tvaca and panchamahabhoot relation
24
5
Correlation of Ayurvedokta Tvaca Stara
with Modern sciences
27
6
Special Features of the Different Layers
of Epidermis
77
7
Cause and color of skin
80

LIST OF FIGURES
Sr no Figures Pages
1 Ligament 30
2 Articular ligament 32
3 Cricothyroid ligament 34
4 Periodontal ligament 35
5 Suspensory ligament of lens 35
6 Phrenoesophageal ligament 36
7 Suspensory ligament of breast 37
8 Anterior sacroiliac ligament 38
9 Posterior sacroiliac ligament 38
10 Sacrotuberous ligament 39
11 Sacrospinous ligament 39
12 Inferior pubic ligament 40

13 Superior pubic ligament 41
14 Suspensory ligament of penis 41
15 Anterior cruciate ligament 42
16 Lateral collateral ligament 43
17 Posterior cruciate ligament 44
18 Medial collateral ligament 45
19 Patellar ligament 45
20 Palmer radio carpal ligament 46
21 Dorsal radio carpal ligament 47
22 Ulnar collateral ligament 48
23 Radial collateral ligament 49
24 Peritoneal ligament 50
25 Flexor retinaculum 51
26 Extensor retinaculum 52

27 Lateral retinaculum 55
28 Medial patellar retinaculum 56
29 Keratinocyte 60
30 Melanocyte 61
31 Langerhans cell 62
32 Markel cell 63
33 Stratum basale 64
34 Stratum spinosum 65
35 Stratum granulosum 66
36 Stratum lucidum 67
37 Stratum corneum 68
38 Papilary layer 71
39 Reticular layer 72
40 Cross section of skin 75
41 Cross section of skin- Thick & thin skin
76

ABSTRACT
Ayurveda is a science which requires a lot of research to establish its
authenticity along with modern medical science. The first step in this is to define the
terms mentioned in Ayurvedic classics, especially the basic terms. The science cannot
be implemented methodically as long as the terms are not properly understood.
Rachana shareera is the subject which deals with a lot of anatomical terms and
defining these terms are important for application of the science. Snayu and tvaca is a
term which is explained elaborately in classical texts but yet it is unable to point out
exact structure related with it in human body. During this study, the references related
to the Snayu and tvacaare collected and tried to explain as a structure form. Literally
the term Snayu means to bind. It is explained as a structure which helps in binding the
joints and helps the body in weight bearing. Structurally it has been described
something similar to a fibrous in nature. Tvaca helps to regulate body temperature, &
permits the sensation of touch, heat &cold. Knowledge of snayu & tvaca is very
important for physicians as well as surgeons who are dealing with surgical removal of
foreign bodies.
Keywords- Snayu, tvaca, Sharir Rachana, fibrous structure.

1
1. INTRODUCTION
The Ayurveda is an ancient medical system that originates in india more than
five thousand years ago. It is considered as upveda of Atharvaveda. The term
Ayurveda is derived from the Sanskrit word Ayu which stands for the integrated
relation of body, sense, mind and the soul. Veda means science .This science is
concerned with life and hence called science of life. Shareera rachana is important
characteristic feature and compact the total science of biology.
Shareera Rachana is one of the basic subjects for the principles of
Ayurveda. It deals with the structure of a human body, its applied aspects & clinical
importance. Most of the structural entities explained in our Samhita are very difficult
to understand. It is very important to interpret the anatomical terms with reference to
the Samhita. There is a lacuna in this interpretation. Tvaca and Snayu Shareera is one
of such area which needs much more research.
Human anatomy (shareera rachana) is an important for allied health
sciences. It is one of the fundamental subject to the health science. The ayurvedic life
science is also based on the human anatomy and physiology (rachana & kriya),
without the knowledge of shareera rachana and kriya, the physician cannot become
perfect in the profession. So the ancient acharyas like Sushruta, Charaka and
Vagbhata were given importance to the knowledge of rachana shareera. The acharya
sushruta was mentioned in the shareerasthana of sushruta samhita, other acharyas are
also explained about the human anatomy in their samhitas.

2
Sushruta shareera sthana has great anatomical importance, therefore it
is said that, Shareera sthana of Sushrut Samhita is best. Strotas formulation takes
place in intrauterine life with appropriate Agni and differentiation takes place, Vayu is
responsible in generation of strotas. This process of differentiation of fertilized zygote
arises many strotas in which body entities take their origin. The term strotas means a
channel. It is derived from the root" susravane" meaning to exude, to ooze, to filter.
Strotas is unique concept of Ayurveda. According to Ayurveda the whole body is
made up of Srotas. The number of Srotas is as many as the number of cells, tissues
and organs put together. This explains that every human cell is possibly a Strotas.
The internal transport system of the body represented by strotamsi, has given a place
of fundamental importance in Ayurveda both in health and disease. Two types of
vyadhies are mentioned. When mamsavaha strotas get vitiated then some diseases
occur these are Aadhimamsa, Arbuda, Arsha, Adhijivha, Upakush, Galashundika,
Aalji, Galaganda, Gandamala, Arsha is mentioned in Mamsadoshaj vikar by Acharya
Sushruta. Srotas are channels of circulations. These channels carry the dhatus
undergoing transformation to their destination. Tissue elements are situated in
different parts of the body and each of them has channels to carry their particular
nourishment.
Mamsavaha Strotas have two roots viz. Snayu, tvaca .symptoms of
damage or injury of mansavaha strotas are shwayathu, mamsashosha and siragranthi
can occurs. Tvaca and snayu are moolasthana of mansavaha strotas. Tvaca as
diagnostic tool in clinical aspects & tvaca serving as prognostic tool. All In Ayurveda
snayu refers to the ligaments. The anatomical study of ligaments is known as

3
desmology. Muscular channels, which originate in the ligaments, tendons, and skin,
supply nutrients to all over the body. Impairment of these channels is due to regular
intake of heavy, greasy foods, excessive sleep, sleeping after meals, and sedentary
lifestyle. The symptoms of vitiation are usually benign tumors produced by the
muscular system, tonsillitis a swollen uvula, hemorrhoids, and swelling of the thyroid
glands and adenoids. The emotional symptoms are lack of mental clarity and nervous
tension.
The study of human anatomy is very much vital for preventive and
curative aspect. Sushrutacharya explains three moolsthana of mansavaha strotas but in
this we are going to study only two moolasthana i.e. tvaca and snayu. Knowledge of
snayu & tvaca is very important for physicians as well as surgeons who are dealing
with surgical removal of foreign bodies. Nowadays because of stressful life, food
habits the necessity of ayurveda principles play an important role for the benefit and
welfare of peoples, so the main purpose of ayurveda is the prevention of disease by
following the various majors and promotion of life.

4
2. OBJECTIVS
AIMS
1) To study the mansavaha strotas moolasthana as per classical texts and modern
anatomy.
OBJECTIVES
1) To elobrate the moolasthana of mansavahastrotas as per sushrutasamhita and
sushrutatikakaras.
2) To determine the action and functions of ligaments and differentiate tendons,
ligaments and muscles.
3) To study the modern anatomy of tvaca(skin) &snayu(ligament) in detail.

5
3. REVIEW OF LITERATURE
1.PREVIOUS WORK DONE
1) Structural study of mansa and rudhira wsr to the effect of vyayam.
2) A critical study of snayu sharer wsr to sushirsnayu.
3) Study of tvaca sharer wsr to vyanga.
4) A critical study of shareera terms snayu, kandara & rajju.
5) Study of Twak Shareer w.s.r to Kitibha Kustha
The literature review broadly divided in two groups mentioned in this topic-
1. Ayurvedic literature
2. Modern literature
1. Ayurvedic literature
We will describe the strotas and symptoms produced when these are injured at their
roots.
Mansavaha strotas(muscular system)-
qÉÉÇxÉuÉWå û²å iÉrÉÉåqÉÑïsÉxlÉÉrÉÑiuÉcÇÉU£üuÉWûɶÉkÉqÉlrÉÉ:
iɧÉÌuÉkÉxrɵÉrÉjÉÑqÉÉÇïxÉzÉÉåwÉ: ÍxÉUÉaÉëljÉrÉÉ qÉUhÉçÇcÉç: xÉÑ zÉÉ 9/12

6
Channels of muscle tissue are two, their roots are snayu (ligaments) and tvaca(skin)
and raktavahi dhamani when these are injured, swelling, emaciation/ wasting of
muscles and death occurs.
MANSAVAHA SROTAS DUSHTI KARANA-
Sevana of abhishyandi padarth.
Eating regularly of guru sthool padarth in excess quantity.
Diwaswap after eating.
MANSAVAHA SROTAS DUSHTI LAKSHANA-
Adhimansa
Arbud
Galshaluk
Galshundikavriddhi
Putimansa
Alaji
Galgand
Gandmala
Upjivika
There are two moolasthana of mansavahastrotas-
1) Snayu ( ligaments)
2) Tvaca ( skin)

7
1) Snayu
Snayu is a structure which performs the function of holding and binding the
various structures of human body like bones, muscles and adipose tissue.
Snayu is used as bow string owing to its strength. Detailed observation of
these structures reveals them as generally fibrous structures which are strong
enough to withstand a certain amount of tension. Observations of Snayuarma
show it as a white, tough structure.
An overall observation of these structures gives an impression that Snayu is a
fibrous structure visible in the body. Aponeurosis, ligament,tendons,
retinaculam, nerve, deep fascia and other fibrous structures in the body.
xlÉÉrÉÑ xÉÇZrÉÉ-
lÉuÉxlÉÉrÉÑzÉiÉÉÌlÉ | iÉÉxÉÉÇ zÉÉZÉÉxÉÑ wÉOûzÉiÉÉÌlÉ,
²å zÉiÉåå ̧ÉÇzÉcrÉ MüÉåwPå, aÉëÏuÉÉÇmÉëirÉÑkuÉçïÇ xÉmiÉÌiÉ xÉÑ.zÉÉ 5/29
Dosha that‘s why called the snayu. The word Snayuis formed from the word
root (Dhatu) Sna. Sna Dhatu when combined with un’ and yuk’ Pratyaya
forms the word Snayu. Snayu(ligaments) are nine hundreds in number of these
six hundred are in sakha (extrimities), two hundred and thirty in the kostha
(trunk) and seventy in griva( neck) and above.

8
Total Snayu–900
Sakha- 600
Kostha- 230
Greeva- 70
Vutpatti of snayu
Sna + una = snayu
Sna word denotes purity. It purifies the. From the unctuous portion of
MedasSnayuare formed.
Snayua rise from Khara Paaka.
Nirukti
Vachaspatya states Snayu as a Strilinga Shabda. The etymology is similar to
Sidhanta Kaumudi. Its function is binding the body.
Synonyms of Snayu
Snayu is said to be a structure which binds the Anga-Pratyanga Sandhi.
Relation between snayu&dhatu-
Snayu is updhatu of meda. From meda snayus are produced.
Snayubhava-
snayu is a pitruj avyava.

9
TYPES OF SNAYU-
xlÉÉrÉѶÉiÉÑÌuÉïkÉÉ ÌuɱɨÉÉxiÉÑ xÉuÉÉïï ÌlÉoÉÉåkÉ qÉå |
mÉëiÉÉlÉuÉirÉÉå uÉÚ¨ÉÉ¶É mÉÚjurÉ¶É xÉÑÍzÉUÉxiÉjÉÉ || xÉÑ.zÉÉ. 5/30
There are four kinds of Snayu-
1) Pratanavati snayu (long tendons)-These snayus are present in shakhas- limbs
and sandhis. Pratanvati means a tendril, a shoot, a low spreading plant, a
spreading creeper and branching out. These are said to be present In Shakha
and all Sandhi. So Pratanavati type of Snayu should be present in all joints
of body and extremities and they should be having branching pattern and
like a creeper. So the structures which resembles Pratanavati Snayu are-
Ligaments- As these are present in all joints.
Nerves- As these are like creepers and have branching pattern.
2) Vrattasnayu–These are circular in shape & are known as kandara. Vrutta
means round or circular.
These are cord like structures present in the body. Acharya Susruta also calls
Vrutta Snayu as Kandara. Kandara is called MahaSnayu or Mahanadi. It is
a cord like structure which is similar to Snayu but large in size. So Kandara
should be large circular or cord like structure. In human the structures
resembling Kandaraor Vrutta Snayu are-
Tendons- As these are cord like

10
Large Nerves cords- These are also cord like and resemble tendon.
3) Pruthusnayu (large &flat tendons)– These are present in chest sides, head
&back region. The word meaning of Pruthula is a broad, large or great. So
these should be structures which are Large, broad and flat resemble Pruthula
Snayu in our body are Aponeurosis Fascia.
4) Susira snayu(ring like tendons) are present in end of stomach & intestine &
urinary bladder. Sushira means porous, hollow, cavity etc. Acharya Susruta
explains that Sushira Snayu is present in the terminal part of regions like
Amashaya, Pakvashaya, Basti etc. So these are structures which are porous
like in nature and also present in the openings of hollow organs and hold
these hollow organs (viscera). So the structures which resemble Sushira
Snayu are sphincters and visceral ligament.
As a ship is constructed & its parts are assembled with different ropes, wires
& bolts, the bones & other parts of the living body also are constructed & bound by
900 different snayus.
Utility of snayu-
According to sushrut just as a boat built by wooden planks placed
side by side, when fastened tightly by ropes in many ways becomes capable of
carrying weight in water steered by a boatman, similarly the human body is able
to carry weight as long as the sandhi(bony joints) are fastened tightly by snayu in
many ways.Ligaments bind the muscle and joints help to keep them in their places
firmly and also strengthen.

11
2) Tvaca
The external covering of the body is called Twak or Twacha. A type
of Indriya which envelops the body is called Twagindriya or Sparshanendriya.
Synonym for Tvaca
1) Tvaca, 2) Asrugdhara
3) Charma, 4) Kruti
5) Parshan, 6) Ajin
7) Chavi, 8) Dehacharma
9) Chadian 10) Shariravaranam
11) Romabhumi 12) Asrugvara
13) Shariravarakam shastram
Twacha: This word is derived as Twacha Samvarane which means covering of the
body.
Charma: This word is derived from Chara which means movement i.e. nature of
moving. According to modern science, cells of epidermis are continuously being
produced, remain for some period and become dead and they are replaced by newly
produced cells. This mechanism can be correlated to Ayurveda Shiryate tat shareeram
law in this way Charma is related to movement so the name has given.

12
Sparshan: To give tactile sensation. Tvaca plays main role in perception of tactile
sensation.
Chhavi: It means to illuminate the complexion, Tvaca enlights colour of a person.
Chhadani: It means to cover Tvaca envelops all organs of the body.
Asrukdhara: It means to hold the blood inside the body. Thus Tvaca prevents
bleeding tendency.
Tvacabhava
Tvaca is a Matruja Bhava.
Tvaca Uttapati
iÉxrÉ ZÉsÉÑ LuÉÇ mÉëuÉÚ¨ÉxrÉ zÉÑ¢üzÉÉåÍhÉiÉxrÉÍpÉmÉcrÉqÉÉlÉxrÉ |
ZzÉÏUxrÉåuÉxÉÇiÉÉÌlÉMüÉ: xÉmiÉiuÉcÉÉåpÉuÉÎliÉ || xÉÑ. zÉÉ. 4/4
Acharya sushruta explained, when life induced by combination of shukra and shonita
in the garbhashaya, at the same time it undergoes rapid transformation and formation.
The seven layers of skin are formed during the embryonic period. The union of sukra
and shonit while being processed by heat gives rise to the formation of seven tvaca
(skin) Just like formation of cream when milk is boiled.
Formation and development of tvaca is took place during the
“Garbhanirmati” i.e. Process of formation and development of Garbha. Sushruta
depicts formation of Tvaca from the metabolization of Shukra & Shonita by Tridosha.
For better understanding of Twacha Uttapati in Brihattrayee the whole process of

13
formation of tvaca is compare with formation of creamy layer over the surface of
milk, when it is boiled and allowed to cooled down, formation of thick layer of skin
take place which is explained as Ksheerat Santaanika.Indu in his commentary
Shashilekha explains theappearance and arrangement of skin layers by giving an
illustration of Kadalidal i.e. Stem of Banana, which has several layers that are
arranged in systematic concentric manner. He states that Twacha is formed from the
Sara bhaaga (Prasaad) of Rakta dhatu, shiny and lustrous appearance of skin is due
to Rakta dhatu. Hemadri in his commentary Ayurved Rasayan depicts that whole
body is Panchmahabhautik and tvaca is formed by metabolization of Rakta dhatu by
its own dhatwagni, several layer of Tvaca are formed over outer surface of embryo.
According to Bhavaprakash tvaca is formed by Pachan that is metabolization of
Shukra and Rasa Dhatu.
Tvaca Uttapati Kala
Acharya describes Bala-Varna-Upachaya in sixth month of intrauterine life, As
Varna complexion is the attribute of skin it is clear that tvaca is formed in sixth
month of intrauterine life. According to Ashtang Sangraha & Hridya Uttapati of
Kesha, Roma, Nakha, Asthi, Snayu, Bala, Varna, Sira and Tvaca develops in sixth
month of intrauterine of life. As per modern all layers of skin is formed in fourth
month of intrauterine life.

14
Layers of tvaca-
iÉxrÉ ZÉsuÉå uÉÇmÉëuÉبÉxrÉ zÉÑ¢üzÉÉåÍhÉiÉxrÉÉÍpÉmÉcrÉqÉÉlÉxrÉ ¤ÉÏUxrÉåuÉ xÉliÉÉÌlÉMüÉ: xÉmiÉiuÉcÉÉåpÉuÉÎliÉ|
iÉÉxÉÉÇ mÉëjÉqÉÉÅuÉpÉÉÍxÉlÉÏ lÉÉqÉ, rÉÉxÉuÉÉïluÉhÉÉïlÉuÉpÉÉxÉrÉÌiÉ mÉÇcÉÌuÉkÉÉÇ cÉ NûÉrÉÉÇ mÉëMüÉzÉrÉÌiÉ,
xÉÉ uÉëÏWåûU¹ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ, ÍxÉkqÉmɱMühOûMüÉÍkɸÉlÉÉ; ̲iÉÏrÉÉsÉÉåÌWûiÉÉlÉÉqÉ, uÉëÏWwÉÉåQûzÉ pÉÉaÉmÉëqÉÉhÉÉ,
ÌiÉsÉMüÉsÉMülrÉcNûurÉQûaÉÉÍkɸÉlÉÉ: iÉ××ÌiÉrÉɵÉåiÉÉlÉÉqÉ, uÉëÏWu¬ÇÉSzÉpÉÉaÉmÉëqÉÉhÉÉ,
cÉqÉïSsÉÉeÉaÉssÉÏqÉwÉMüÉÍkɸÉlÉÉ: cÉiÉÑjÉÏï iÉÉqÉëÉ lÉÉqÉÉ uÉëÏW¹pÉÉaÉmÉëqÉÉhÉÉ, ÌuÉÌuÉkÉÌMüsÉÉxÉMÑü¸ÉÍkɸÉlÉÉ:
mÉçÇcÉqÉÏ uÉåÌSÌlÉ lÉÉqÉ uÉëÏWmÉÇcÉpÉÉaÉmÉëqÉÉhÉÉ, MÑü¸ÌuÉxÉmÉÉÍkɸÉlÉÉ: wÉ¸Ï UÉåÌWûÌlÉ lÉÉqÉ ÌuÉëÌWûmÉëqÉhÉÉ,
aÉëljrÉmÉcrÉoÉÑïSzsÉÏmÉSaÉsÉaÉlQûÉÍkɸÉlÉÉ; xÉmiÉÍqÉ qÉÉÇxÉkÉUÉ lÉÉqÉ ÌuÉëÌWû²rÉmÉëqÉhÉÉ, pÉaÉlkÉUÌuÉSìkrÉzÉÉåïÍkɸÉlÉÉ|
rÉSåiÉimÉëqÉÉhÉçÇ ÌlÉÌSïzÉiÉç ÇiÉlqÉÉÇxÉsÉåµÉuÉMüÉzÉwÉ ãlÉ sÉsÉÉiÉå xÉÑYzqÉÉQèû.aÉÑsrÉÉÌSzÉÑ; rÉiÉÉå uÉYzrÉirÉÑSUåzÉÑ
ÌuÉëÌWûqÉÑZÉålÉÉQèû.aÉÑziÉÉåUSUmÉëqÉhÉçÇqÉuÉaÉÉkÉçÇ ÌuÉbrÉÌSåÌiÉ ||
xÉÑ.zÉÉ. 4/4
1) Avabhasini
2) Lohita
3) Sveta
4) Tamra
5) Vedini
6) Rohini
7) Mansadhara

15
1) Avabhasini- The first layer is avabhasini. It is 1/18 of vrihipramana. It
is adhishtana for sidma, Padma, and kantak diseases. It is whitish black
color and brajakaagni lies in this layer. It reflects the complexion and the
quality of the Rasa dhatu. It also acts as a mirror: it indicates whether the
physiology as a whole is balanced or imbalanced, and whether there is
inner health or disorder. The avabhasini layer also reflects the aura of the
individual — if there is inner bliss, it shows on this layer. It does not have
its own color: it reflects the colors of the inner layers.
2) Lohita- The second layer is lohita. It is 1/16 of vrihipramana. It is
adhishtana for tilakalak, nyacha, vyanga diseases. It indicates the quality of
Rakta Dhatu (blood). If there is ama (impurities) in the blood, it impacts
the aura of the outer layer and accentuates sensitivity to the sun. The color
of this layer resembles molten iron.
3) Sveta-The third layer is sveta. It is 1/12 of vrihipramana. It is adhishtana
for charmadala, ajagalli, mashaqkadiseases. This is a white layer, and it
provides balance to skin color, lightening the darker colors of the inner
layers.
4) Tamra- The fourth layer is tamra. It is 1/8 of vrihipramana. It is
adhishtana for kilas and different varities of leprosy diseases. This layer
nurtures the upper layers of the skin. It supports the immune system. This is
the layer that helps the skin perform its function of being a "barrier." Skin
infections reflect an imbalance in this layer.

16
5) Vedini- The fifth layer is vedini. It is 1/5 of vrihi pramana. It is adhishtana
for visarpa and different varities of leprosy diseases. It is the center for
transformation of sensation like feeling of pain.
6) Rohini- The sixth layer is rohini. It is 1 vrihi pramana. It is adhishtana for
granthi, apachi, arbhuda, shlipada, and galganda diseases. This layer supports
healing and regeneration. Imbalance in this layer retards healing and the
disappearance of scars over time. A balanced diet, rich in nutritional value,
supports the rohini layer.
7) Mansadhara- The seventh layer is mansadhara. It is 2 vrihipramana. It is
adhishtana for bhagandar, vidradhi and arsha diseases. This innermost layer is
the platform for the skin's stability and firmness. When this layer is in balance,
the skin looks young and supple. A skin product that has a vayasthapana effect
nourishes this layer to help retard the aging process.

17
Table no.1
Type of skin,modern name,pramana & adhishtana for disease
Sr no Name of skin Modern name Pramana Adhishtana for
Diseases
1 Avabhasini Reflecting layer 1/18vrihi Sidma, Padma, and
Kantak
2 Lohita Reddish layer 1/16vrihi Tilakalak, nyacha,
Vyanga
3 Sveta White layer 1/12vrihi Charmadala, ajagalli,
Mashaqka
4 Tamra Pigment layer 1/8vrihi Kilas & kushta
5 Vedini Sensory layer 1/5vrihi Kushta & visarpa
6 Rohini Proliferating layer
1vrihi Granthi, apachi, arbuda, shlipada, & gandmala
7 Mansadhara Muscle
2 vrihi Bhagandar, vidradhi & arsha

18
Table no.2
Types of tvaca according to different tikakaras-
Sr
no
Sushruta
Samhita
Dr. Ghanekar Acharya
Dalhan
1 Avabhasini Avabhasini Avabhasini
2 Lohita Lohita Lohita
3 Shweta Shweta Shweta
4 Tamra Tamra Tamra
5 Vedini Vedini Vedini
6 Rohini Rohini Rohini
7 Mansdhara Mansdhara Mansdhara
Thickness of Tvaca:
In various Ayurvedic texts, there is a description of tvaca, its layers
and diseases occurring in each layer of tvaca. Sushruta Samhita is unique for
the description of Thickness of tvaca. Here, Sushruta describes thickness of
tvaca in the measurement of Vrihi Pramana. (Vrihi – Rice Grain) So,
Avabhasini tvaca is thick = 1/18th part of 1 Vrihi and likewise about other

19
layers of tvaca. But this measurement of tvaca is not throughout same for all
the body parts. It differs according to various body parts. The measurement of
thickness of tvaca mentioned above is applicable for only thick skin on
muscular parts of the body. It is not applicable for forehead and small fingers.
According to Dalhana, a commentator of Sushruta Samhita twenty parts of 1
rice grain should be done and then thickness of tvaca should be determined
e.g. Avabhasini tvaca is thick = 18/20 parts of 1 Vrihi.
Table no.3
Showing the comparison of thickness of tvaca according to Sushruta and
Dalhana:
Tvaca Sushruta Modern
measurement
Dalhana Modern
measurement
Avabhasini 1/18 0.055 18/20 0.90
Lohita 1/16 0.062 16/20 0.80
Shweta 1/12 0.083 12/20 0.60
Tamra 1/8 0.125 8/20 0.40
Vedini 1/5 0.200 5/20 0.20
Rohini 1 1 1 1
Mamsadhara 2 2 2 2
Total:3.525 Total: 5.9

20
So, according to Sushruta and Dalhana, there is a great controversy
regarding thickness of tvaca- Sushruta: 3.5 Vrihi
Dalhana: Appr 6 Vrihi
If practically observed and thickness of 1 vrihi is measured it becomes average
1mm. So, the thickness of tvaca told by Sushruta and Dalhana expressed in
modern measured will be: Sushruta: 3.5 mm Dalhana: Appr. 6 mm If we want
to compare this measurement with modern measurement (skin thickness = 1.5
to 4 mm), then Sushruta seems to be perfect and more accurate in telling
thickness of skin. Because according to Dalhana, it becomes 6mm which is
highly impossible.
Tvaca as diagnostic tool in clinical examination
WHO defined health as condition of complete physical, mental and social
wellbeing and not merely the absence of disease or infirmity. WHO also agree with
definition of Swastha purusha explained by Ayurveda, Sushruta defined Swastha
purusha as a person having balanced status of Dosha, Dhatu & Mala and all
metabolic activities are carried out by Agni in proper manner, along with having
cheerful status of Atma, Mana & Indriya that is all are performing their function
properly.As tvaca is included in indriya. Normal functioning tvaca is one of the
essential attribute of Swasthapurusha.
In Brittrayee three basic tools are described for clinical examination these are
Darshan (inspection) Sparshan (Palpation & Percussion) &Prashan (Interrogation by

21
history taking).Out of the entire three tools for clinical examination Darshan &
Sparshan parikshan is done by examining the appearance of tvaca and sensory
perception of patient. Tvaca is the reflection of internal body system as only by
examining the skin one can effectively make diagnosis. As earlier mentioned that we
can recognize Dosha, Dhatu and Mala Vriddhi- Kshaya only by Darshan and
Sparshan parikshan. Such as hyper pigmentation of skin in Vata Vriddhi.
Yellowishness of skin in Pitta vriddhi, Shitta sparsha & hypopigmentation of skin in
Kapha Vriddhi, Redness of skin in Rakta Vriddhi, Foul smelling of Tvaca in Sweda
Vriddhi.Similarlyloss in glory of skin &Shita sparsh in Pitta Kshaya. Dryness of skin
in Rasa Kshaya, Shaithilyata (loosness) &Rukshata (dryness) is seen in Rakta
Kshaya. Falling of Kesha and Nakha are observed in Asthi Kshaya. Cracks in tvaca &
loss or Destruction of Roma are noted in Sweda Kshaya. In Ayurveda pathogenesis of
diseases is depends on status of Dosha, Dhatu & Mala, so one can effectively make
diagnosis only by examining status of tvaca.
Modern science also emphasize on importance of skin as diagnostic tool, as many
diagnosis is made by examination of following features of skin:
Color & Pigmentation: following changes in skin color indicates few systemic
conditions.
1. Pallor: Anemia, Hemorrhage & Shock
2. Pale: Hypopitutarism, Hypogonadism
3. Albinism: Congential Absence of Haemosiderin pigment.
4. Cyanosis: Bluish discoloration of skin appears due to lack of oxygen supply to
blood corpuscles such as in Congestive Cardiac Failure & Valvular Septal Defect.

22
5. Jaundice: Yellowish Discoloration of skin, nail, & sclera.
Skin lesions and Eruption: Several skin lesions are observed in various
dermatological disorders such as: Vesicles, plaques, scales, papules, nodules,
papules & patches.
Hair & Nails: Clubbing of nails, oncolysis of nails, yellowish discoloration of nail
are indication of Congenital cardiac disorders, Anemia, Psoriatic nail…etc. Hair
fall and toothed hair roots are observed in Alopecia Aerata, patient on
chemotherapy.
Skin lesions in Sexually Transmitted diseases
Chancres in syphilis,Blisters in Herpes Zoster & Simplex, Candidial Infection in HIV.
Drug Hypersensitivity
Hypersensitivity reactions are notice after administering certain drugs such as:
Penicillin causes Urticaria, Methyl dopa & Phenyl butazone leads to eczema like
rashes, Sulphonyl urea, Indomethacin, Allopurinol causes Exfoliative dermatitis,
Prednisone leads to Acne.
Diagnostic test
Patch test done in Urticaria, Sensitivity test is done to rule out any drug
hypersensitivity before its administration for example penicillin & ASV. Montaux
test for confirming T.B.

23
Tvaca as Rogmarga
In Ayurvediya text three Roga marga are described, these are:
Bahaya Roga marga: Shakha, Raktaadi Sapta dhatu & Tvaca are included under
these Rog marga.
Madhyam Roga marga: Marma, Basti, Hridya, Murdha, Asthi, Snayu, Kandra are
included in these Rog marga.
Abhayantara Roga Marga: Kostha i.e. Mahastrotas, Sharir Madhaya &Pakvashaya
is mentioned in these Rog marga.
Tvaca is included in Bahaya Rog marga, it is one of the mode by means of which
disease exhibits itself.So brief attention should be given towards tvaca while
performing clinical examination.
Tvaca as vrana vastu
Acharya Sushruta mentions eight Vrana Vastu these are tvaca, Mansa, Shira,
Snayu, Asthi, Sandhi, Kostha& Marma. Vrana Vastu means the structure or place
where Vrana (wound) harbor itself. Sushruta state that Vrana limited to Twacha is
fast healing and easy to treat. So we can say that tvaca is an important diagnostic tool
in medicinal and surgical point of view.

24
Tvaca & Panchamahabhoota Relation:
Table no.4
Tvaca is also having Panchabhautik nature.
Sr. no
Element Structure
1 Parthiva Kesha, Loma
2 Aapya Rasa, Lasiak
3 Tejas Kanti, Varna
4 Vayviya Sparsha, Samvedna
5 Akashiya Lomakoopa, Sweda Vahi Nalika
Moolasthana of mansavaha strotas according to sushruta tikakaras-
Tikakaras of the following authors are important ones on the sushruta samhita.
1) Dr.Bhaskar Govind Ghanekar( Ayurvedrahasyadipeeka)
2) Shri.Dalhanacharya( Nibandhsangraha)
1) Dr.Bhaskar Govind Ghanekar( Ayurved Rahasya Dipeeka)
According to Dr.Bhaskar Ghanekar there is snayu and tvaca are moolasthana of
mansavaha strotas.
Snayu-
xlÉÉrÉѶÉiÉÑÌuÉïkÉÉ ÌuɱɨÉÉxiÉÑ xÉuÉÉïï ÌlÉoÉÉåkÉ qÉå |
mÉëiÉÉlÉuÉirÉÉå uÉÚ¨ÉÉ¶É mÉÚjurÉ¶É xÉÑÍzÉUÉxiÉjÉÉ ||
AÉ.U.ÌS. 5/38

25
There are 4 types of snayu
Pratanavati snayu (long tendons)-These snayus are present in
shakhas- limbs and sandhis. Vratta snayu–These are circular in
shape and cord like structure present in body.
Pruthu snayu (large &flat tendons) – Are present in chest sides, head &back region.
Susira snayu(ring like tendons) are present in end of stomach & intestine
& urinary bladder. Snayus are useful in seevan dravyas.
Functions of snayu
LuÉqÉåuÉë zÉUÏUåÅÎxqÉlÉ rÉÉuÉliÉ: xÉlkÉrÉ: xqÉ××iÉÉ:|
AÉrÉÑÍpÉuÉïQèû.aÉÑÍpÉoÉïkSÉxiÉålÉ pÉÉUxÉWûÉ lÉUÉ: ||
AÉ.U.ÌS.5/42
The main function of snayu is binding.
Tvaca-
iÉxrÉ ZÉsuÉå uÉÇmÉëuÉبÉxrÉ zÉÑ¢üzÉÉåÍhÉiÉxrÉÉÍpÉmÉcrÉqÉÉlÉxrÉ ¤ÉÏUxrÉåuÉ xÉliÉÉÌlÉMüÉ: xÉmiÉiuÉcÉÉåpÉuÉÎliÉ|
iÉÉxÉÉÇ mÉëjÉqÉÉÅuÉpÉÉÍxÉlÉÏ lÉÉqÉ, rÉÉxÉuÉÉïluÉhÉÉïlÉuÉpÉÉxÉrÉÌiÉ mÉÇcÉÌuÉkÉÉÇ cÉ NûÉrÉÉÇ mÉëMüÉzÉrÉÌiÉ,
xÉÉ uÉëÏWåûU¹ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ, ÍxÉkqÉmɱMühOûMüÉÍkɸÉlÉÉ; ̲iÉÏrÉÉsÉÉåÌWûiÉÉlÉÉqÉ, uÉëÏWwÉÉåQûzÉ pÉÉaÉmÉëqÉÉhÉÉ,
ÌiÉsÉMüÉsÉMülrÉcNûurÉQûaÉÉÍkɸÉlÉÉ: iÉ× ×ÌiÉrÉɵÉåiÉÉlÉÉqÉ, uÉëÏWu¬ÇÉSzÉpÉÉaÉmÉëqÉÉhÉÉ,
cÉqÉïSsÉÉeÉaÉssÉÏqÉwÉMüÉÍkɸÉlÉÉ: cÉiÉÑjÉÏï iÉÉqÉëÉ lÉÉqÉÉ uÉëÏW¹pÉÉaÉmÉëqÉÉhÉÉ, ÌuÉÌuÉkÉÌMüsÉÉxÉMÑü¸ÉÍkɸÉlÉÉ:
mÉçÇcÉqÉÏ uÉåÌSÌlÉ lÉÉqÉ uÉëÏWmÉÇcÉpÉÉaÉmÉëqÉÉhÉÉ, MÑü¸ÌuÉxÉmÉÉÍkɸÉlÉÉ: wÉ¸Ï UÉåÌWûÌlÉ lÉÉqÉ ÌuÉëÌWûmÉëqÉhÉÉ,
aÉëljrÉmÉcrÉoÉÑïSzsÉÏmÉSaÉsÉaÉlQûÉÍkɸÉlÉÉ; xÉmiÉÍqÉ qÉÉÇxÉkÉUÉ lÉÉqÉ ÌuÉëÌWû²rÉmÉëqÉhÉÉ, pÉaÉlkÉUÌuÉSìkrÉzÉÉåïÍkɸÉlÉÉ|

26
rÉSåiÉimÉëqÉÉhÉçÇ ÌlÉÌSïzÉiÉç ÇiÉlqÉÉÇxÉsÉåµÉuÉMüÉzÉwÉ ãlÉ sÉsÉÉiÉå xÉÑYzqÉÉQèû.aÉÑsrÉÉÌSzÉÑ; rÉiÉÉå uÉYzrÉirÉÑSUåzÉÑ
ÌuÉëÌWûqÉÑZÉålÉÉQèû.
aÉÑziÉÉåUSUmÉëqÉhÉçÇqÉuÉaÉÉkÉçÇ ÌuÉbrÉÌSåÌiÉ ||
AÉ.U.ÌS.4/3
According to Dr. Ghanekar there are 7 layers of tvaca.
1) Avabhasini- This is the first layer & having 1/18 of vrihipramana. Sidma,
Padma, and kantak diseases are adhishtana in this layer.it reflects the 5 types
of chhaya.
2) Lohita- This is second layer & having 1/16 of vrihipramana. It is adhishtana
for tilakalak, nyacha, vyanga diseases.
3) Sveta-This is the third layer& having 1/12 of vrihipramana. It is adhishtana for
charmadala, ajagalli, mashaqka diseases.
4) Tamra- This is the fourth layer & having 1/8 of vrihipramana. It is adhishtana
for kilas and different varities of leprosy diseases.
5) Vedini- This is the fifth layer & having 1/5 of vrihipramana. It is adhishtana
for visarpa and different varities of leprosy diseases.
6) Rohini- This is the sixth layer & having 1 vrihipramana. It is adhishtana for
granthi, apachi, arbhuda, shlipada, and galganda diseases.
7) Mansadhara- This is the seventh layer & having 2
vrihipramana. It is adhishtana for bhagandar vidradhi &
arsha diseases.

27
Table no.5
We can correlate Ayurvedokta Tvaca Stara with Modern sciences as per
mentioned by Dr.Ghanekar, which are as follows-
Sr. no Ayurvedokta
Twacha Stara
Correlate with
Modern Skin Layer
Epideris
1 Avabhasini Stratum Corneum
2 Lohita Stratum Lucidium
3 Shweta Stratum Granulosum
4 Tamra Stratum Malphighi
5 Vedini Papillary Layer
6 Rohini Reticular layer Dermis
7 Mansadhara Subcutaneous tissue Hypodermis
2) Shri.Dalhanacharya ( Nibandhsangraha)
qÉÉÇxÉuÉWåû²åiÉrÉÉåqÉÑïsÉxlÉÉrÉÑiuÉcÇÉU£üuÉWûɶÉkÉqÉlrÉÉ:|
iɧÉÌuÉkÉxrɵÉrÉjÉÑqÉÉÇïxÉzÉÉåwÉ : ÍxÉUÉaÉëljÉrÉÉ qÉUhÉçÇcÉç: ||
Q.ÌlÉ.xÇÉ 9/12
Channels of muscle tissue are two, their roots are snayu (ligaments) and
tvaca(skin)and raktavahi dhamani when these are injured, swelling, emaciation/
wasting of muscles and death occurs.

28
Snayu-
xlÉÉrÉѶÉiÉÑÌuÉïkÉÉ ÌuɱɨÉÉxiÉÑ xÉuÉÉïï ÌlÉoÉÉåkÉ qÉå |
mÉëiÉÉlÉuÉirÉÉå uÉÚ¨ÉÉ¶É mÉÚjurÉ¶É xÉÑÍzÉUÉxiÉjÉÉ ||
Q.ÌlÉ.xÇÉ 5/30
There are 4 types of snayu
1) Pratanavati snayu (long tendons)-These snayus are present in shakhas- limbs and
sandhis.
2) Vratta snayu–These are circular in shape and cord like structure present in body.
3) Pruthu snayu (large &flat tendons) – These are present in chest sides, head
&back region.
4) Susira snayu(ring like tendons) are present in end of stomach & intestine &
urinary bladder.
Tvaca-
iÉxrÉ ZÉsuÉå uÉÇmÉëuÉبÉxrÉ zÉÑ¢üzÉÉåÍhÉiÉxrÉÉÍpÉmÉcrÉqÉÉlÉxrÉ ¤ÉÏUxrÉåuÉ xÉliÉÉÌlÉMüÉ: xÉmiÉiuÉcÉÉåpÉuÉÎliÉ|
iÉÉxÉÉÇ mÉëjÉqÉÉÅuÉpÉÉÍxÉlÉÏ lÉÉqÉ, rÉÉxÉuÉÉïluÉhÉÉïlÉuÉpÉÉxÉrÉÌiÉ mÉÇcÉÌuÉkÉÉÇ cÉ NûÉrÉÉÇ mÉëMüÉzÉrÉÌiÉ,
xÉÉ uÉëÏWåûU¹ÉSzÉpÉÉaÉmÉëqÉÉhÉÉ, ÍxÉkqÉmɱMühOûMüÉÍkɸÉlÉÉ; ̲iÉÏrÉÉsÉÉåÌWûiÉÉlÉÉqÉ, uÉëÏWwÉÉåQûzÉ pÉÉaÉmÉëqÉÉhÉÉ,
ÌiÉsÉMüÉsÉMülrÉcNûurÉQûaÉÉÍkɸÉlÉÉ: iÉ××ÌiÉrÉɵÉåiÉÉlÉÉqÉ, uÉëÏWu¬ÇÉSzÉpÉÉaÉmÉëqÉÉhÉÉ,
cÉqÉïSsÉÉeÉaÉssÉÏqÉwÉMüÉÍkɸÉlÉÉ: cÉiÉÑjÉÏï iÉÉqÉëÉ lÉÉqÉÉ uÉëÏW¹pÉÉaÉmÉëqÉÉhÉÉ, ÌuÉÌuÉkÉÌMüsÉÉxÉMÑü¸ÉÍkɸÉlÉÉ:
mÉçÇcÉqÉÏ uÉåÌSÌlÉ lÉÉqÉ uÉëÏWmÉÇcÉpÉÉaÉmÉëqÉÉhÉÉ, MÑü¸ÌuÉxÉmÉÉÍkɸÉlÉÉ: wÉ¸Ï UÉåÌWûÌlÉ lÉÉqÉ ÌuÉëÌWûmÉëqÉhÉÉ,
aÉëljrÉmÉcrÉoÉÑïSzsÉÏmÉSaÉsÉaÉlQûÉÍkɸÉlÉÉ; xÉmiÉÍqÉ qÉÉÇxÉkÉUÉ lÉÉqÉ ÌuÉëÌWû²rÉmÉëqÉhÉÉ, pÉaÉlkÉUÌuÉSìkrÉzÉÉåïÍkɸÉlÉÉ|

29
rÉSåiÉimÉëqÉÉhÉçÇ ÌlÉÌSïzÉiÉç ÇiÉlqÉÉÇxÉsÉåµÉuÉMüÉzÉwÉãlÉ sÉsÉÉiÉå xÉÑYzqÉÉQèû.aÉÑsrÉÉÌSzÉÑ; rÉiÉÉå uÉYzrÉirÉÑSUåzÉÑ
ÌuÉëÌWûqÉÑZÉålÉÉQèû.
aÉÑziÉÉåUSUmÉëqÉhÉçÇqÉuÉaÉÉkÉçÇ ÌuÉbrÉÌSåÌiÉ ||
Q.ÌlÉ.xÇÉ. 4/4
According to the Dalhana tika in nibandhsangraha mentioned that there are 7 layers of
tvaca.
1) Avabhasini- It is the first layer of tvaca & the pramana is 1/18 of
vrihipramana. It is adhishtana for sidma, Padma, and kantak diseases.it reflects
the 5 types of chhaya.
2) Lohita- It is the second layer of tvaca & pramana is 1/16 of vrihipramana. It is
adhishtana for tilakalak, nyacha, vyanga diseases.
3) Sveta-It is the third layer of tvaca & pramana is 1/12 of vrihipramana. It is
adhishtana for charmadala, ajagalli, mashaqka diseases.
4) Tamra- It is the fourth layer of tvaca & pramana is 1/8 of vrihipramana. It is
adhishtana for kilas and different varities of leprosy diseases.
5) Vedini- It is the fifth layer of tvaca & pramana is 1/5 of vrihipramana. It is
adhishtana for visarpa and different varities of leprosy diseases.
6) Rohini- It is the sixth layer of tvaca & pramana is 1 vrihipramana. It is
adhishtana for granthi, apachi, arbhuda, shlipada, and galganda diseases.
7) Mansadhara- It is the seventh layer of tvaca & pramana is 2 vrihipramana. It is
adhishtana for bhagandar, vidradhi and arsha diseases.

30
2.Modern literature
1) ANATOMY OF LIGAMENT
A ligament is the fibrous connect tissue that connects bones to other bones. It is
also known as articular ligament, articular Laura, Fibrous ligament, or true
ligament.
Other ligaments in the body include the
Peritoneal ligament: a fold of peritoneum or other membranes.
Fetal remnant ligament: the remnants of a fetal tubular structure.
Periodontal ligament: a group of fibers that attach the cementum of teeth to the
surrounding alveolar bone.
Figure no 1- Ligament

31
Ligaments are similar to tendons and fasciae as they are all made of
connective tissue. The differences in them are in the connections that they make
ligaments connect one bone to another bone, tendons connect muscle to bone, and
fasciae connect muscles to other muscles. These are all found in the skeletal system of
the human body. Ligaments cannot usually be regenerated naturally; however, there
are periodontal ligament stem cells located near the periodontal ligament which are
involved in the adult regeneration of periodontal ligament.
Articular ligaments
"Ligament" most commonly refers to a band of dense regular connective tissue
bundles made of collagenous fibers, with bundles protected by dense irregular
connective tissue sheaths. Ligaments connect bones to other bones to form joints,
while tendons connect bone to muscle. Some ligaments limit the mobility of
articulations or prevent certain movements together.

32
Figure no 2- articular ligament
Capsular ligaments are part of the articular capsule that surrounds synovial
joints. They act as mechanical reinforcements. Extra-capsular ligaments join together
in harmony with the other ligaments and provide joint stability. Intra-capsular
ligaments, which are much less common, also provide stability but permit a far larger
range of motion. Cruciate ligaments are paired ligaments in the form of a cross.
Ligaments are viscoelastic.
They gradually strain when under tension and return to their original shape
when the tension is removed. However, they cannot retain their original shape when
extended past a certain point or for a prolonged period of time. This is one reason why
dislocated joints must be set as quickly as possible: if the ligaments lengthen too
much, then the joint will be weakened, becoming prone to future dislocations.
Athletes, gymnasts, dancers, and martial artists perform stretching exercises to
lengthen their ligaments, making their joints more supplied.

33
The term hypermobility refers to people with more-elastic ligaments, allowing
their joints to stretch and contort further; this is sometimes still called double-
jointedness.
The consequence of a broken ligament can be instability of the joint. Not all broken
ligaments need surgery, but, if surgery is needed to stabilize the joint, the broken
ligament can be repaired. Scar tissue may prevent this. If it is not possible to fix the
broken ligament, other procedures such as the Brunelli procedure can correct the
instability. Instability of a joint can over time lead to wear of the cartilage and eventually
to osteoarthritis.
Artificial ligaments-
One of the most often torn ligaments in the body is the ACL. The ACL is one
of the ligaments crucial to knee stability and persons who tear their ACL often seek to
undergo reconstructive surgery, which can be done through a variety of techniques
and materials. One of these techniques is the replacement of the ligament with an
artificial material. An artificial ligament is a reinforcing material that is used to
replace a torn ligament, such as the ACL. Artificial ligaments are a synthetic material
composed of a polymer, such as poly acrylonitrile fiber, polypropylene, PET
(polyethylene terephthalate).

34
Examples
Head and neck
Cricothyroid ligament
Figure no-3- cricothyroid ligament
The median cricothyroid ligament is a flat band of white connective
tissue that connects the front parts of the contiguous margins of the cricoid and
thyroid cartilages. It is a thick and strong ligament, narrow above and broad
below. Each lateral ligament is known as the conus elasticus.
Periodontal ligament-: The periodontal ligament, commonly abbreviated as
the PDL, is a group of specialized connective tissue fibers that essentially
attach a tooth to the alveolar bone within which it sits. It inserts into root
cementum one side and onto alveolar bone on the other.

35
Figure no 4- periodontal ligament
Suspensory ligament of the lens
Suspensory ligament of lens- a series of fibers that connect the ciliary
body of the eye with the lens,holding it in place. Upper eyelid - top,
movable, superior fold of skin that covers the front of the eyeball when closed,
including the cornea.
Figure no 5- suspensory ligament of lens

36
Thorax-
Phrenoesophageal ligament-
Figure no-6-phreno esophageal ligament
The phrenoesophageal ligament (phrenicoesophageal ligament or phrenoesophageal
membrane) is the ligament by which the esophagus is attached to the diaphragm.
The ligament allows independent movement of the diaphragm and esophagus during
respiration and swallowing.

37
Suspensory ligament of breast
Figure no 7- suspensory ligament of breast
Suspensory ligaments are connective tissue in the breast that help maintain
structural integrity.
Pelvis
Anterior sacroiliac ligament-
The anterior sacroiliac ligament consists of numerous thin bands,
which connect the anterior surface of the lateral part of the sacrum to the
margin of the auricular surface of the ilium and to the preauricular sulcus.

38
Figure no 8- Anterior sacroiliac ligament
Posterior sacroiliac ligament-
The posterior sacroiliac ligament is situated in a deep depression
between the sacrum and ilium behind; it is strong and forms the chief bond of
union between the bones.
Figure no 9-posterior sacroiliac ligament

39
Sacrotuberous ligament-
Figure no 10- Sacrotuberous ligament
The sacrotuberous ligament is a slender, fan-shaped ligament of the posterior
(back) pelvis located on either side of the body. This ligament arises midway
down the posterior side of the sacrum, which is located at the spinal base.
Sacrospinous ligament-
Figure no 11-Sacrospinous ligament

40
The sacrospinous ligament (small or anterior sacrosciatic ligament) is a thin,
triangular ligament in the human pelvis. The base of the ligament is attached to the
outer edge of the sacrum and coccyx and the tip of the ligament attaches to the spine
of the ischium, a bony protuberance on the human pelvis.
Inferior pubic ligament-
Figure no 12- Inferior pubic ligament
The inferior pubic ligament (arcuate pubic ligament, arcuate ligament of the pubis, or
subpubic ligament) is a thick, triangular arch of ligamentous fibers, connecting
together the two pubic bones below, and forming the upper boundary of the pubic
arch.

41
Superior pubic ligament-
The superior pubic ligament connects together the two pubic bones superiorly,
extending laterally as far as the pubic tubercles.
Figure no 13- Superior pubic ligament
Suspensory ligament of penis-
Figure no 14- Suspensory ligament of the penis
In males, the suspensory ligament of the penis is attached to the pubic symphysis,
which holds the penis close to the pubic bone and supports it when erect.

42
Knee
Anterior cruciate ligament-
Figure no 15- anterior cruciate ligament
The anterior cruciate ligament (ACL) is one of the key ligaments that help
stabilize our knee joint. The ACL connects our thighbone (femur) to our
shinbone (tibia). It's most commonly torn during sports that involve sudden
stops and changes in direction.

43
Lateral collateral ligament-
Figure no 16- lateral collateral ligament
The lateral collateral ligament is a thin band of tissue running along the
outside of the knee. It connects the thighbone (femur) to the fibula, which is
the small bone of the lower leg that runs down the side of the knee and
connects to the ankle. Like the medial collateral ligament, the lateral collateral
ligament's main function is to keep the knee stable.

44
Posterior cruciate ligament-
Figure no 17- posterior cruciate ligament
The posterior cruciate ligament (PCL) is a ligament within the knee. Ligaments are
tough bands of tissue that connect bones. The PCL similar to the anterior
cruciateligament (ACL) -connects the thigh bone (femur) to your shin bone (tibia).
Although it is larger and stronger than the ACL, the PCL can be torn.

45
Medial collateral ligament-
Figure no 18-medial collateral ligament
The medial collateral ligament is located on the inner aspect, or part, of
your knee, but it's outside the joint itself. Ligaments hold bones together and add
stability and strength to a joint. The MCL connects the top of the tibia, or
shinbone, to the bottom of the femur, or thigh bone.
Patellar ligament-
Figure no 19- patellar ligament

46
The patellar ligament is an extension of the quadriceps tendon. It extends from
the patella, otherwise known as the kneecap. A ligament is a type of fibrous
tissue that usually connects two bones.
Wrist
Palmar radio carpal ligament-
Figure no 20-palmar radio carpal ligament
The palmar radio carpal ligament (anterior ligament, volar radio carpal ligament)
is a broad membranous band, attached above to the distal end of the radius to the
scaphoid, lunate and the triquetrum of the carpal bones in the wrist. Some is
continued to the capitate.

47
Dorsal radio carpal ligament-
Figure no 21-Dorsal radio carpal ligament
The dorsal radio carpal ligament (posterior ligament) less
thick and strong than the volar, is attached, above, to the posterior border of
the lower end of the radius; its fibers are directed obliquely downward and
medialward, and are fixed, below, to the dorsal surfaces of the navicular (now
known as scaphoid), lunate and triquetral being continuous with those of the
dorsal inter carpal ligament.

48
Ulnar collateral ligament-
Figure no 22- ulnar collateral ligament
The ulnar collateral ligament (UCL or internal lateral ligament) is a thick
triangular band at the medial aspect of the elbow uniting the distal aspect of the
humerus to the proximal aspect of the ulna.

49
Radial collateral ligament-
Figure no 23- Radial collateral ligament
The radial collateral ligament (external lateral ligament, radial carpal collateral
ligament) extends from the tip of the styloid process of the radius and attaches to the
radial side of the scaphoid immediately adjacent to its proximal articular surface and
some fibers extend to the lateral side of the trapezium.
Peritoneal ligaments-
Peritoneal ligaments are folds of peritonium that are used to connect viscera to viscera
or the abdominal wall.There are multiple named ligaments that usually are named in
accordance with what they are.

50
Gastrocolic ligament
Gastrosplenic ligament
Gastrophrenic ligament
Phrenicocolic ligament
Splenorenal ligament
Coronary ligament
Hepatoduodenal ligament
Hepatogastric ligament
Figure no 24- peritoneal ligaments

51
Certain folds of peritoneum are referred to as ligaments. Examples include:
The hepato duodenal ligament,that surrounds the hepatic portal vein and other
vessels as they travel from the duodenum to the liver.
The broad ligament of the uterus, also a fold of peritoneum.
Retinaculum
A retinaculum is a band of thickened deep fascia around tendons that holds
them in place. It is not part of any muscle. Its function is mostly to stabilize a tendon.
The term retinaculum is derived from the Latin verb retinere (retain).
A retinaculum refers to any region on the body in which tendon groups
from different muscles pass under one connective tissue band. Specific retinacula
include-
In the wrist:
1) Flexor retinaculum of the hand-
Figure no.25- flexor retinaculum of hand

52
The flexor retinaculum (transverse carpal ligament or anterior annular
ligament) is a fibrous band on the palmar side of the hand near the wrist. It
arches over the carpal bones of the hands, covering them and forming the
carpal tunnel.
2) Extensor retinaculum of the hand-
Figure no 26- extensor retinaculum of hand
The extensor retinaculum (dorsal carpal ligament, or posterior annular
ligament) is an anatomical term for the thickened part of the antebrachial
fascia that holds the tendons of the extensor muscles in place. It is located
on the back of the forearm, just proximal to the hand.

53
In the ankle
1) Flexor retinaculum of foot-
The flexor retinaculum of foot (laciniate ligament, internal
annular ligament) is a strong fibrous band, extending from the bony ankle
prominence (malleolus) above, to the margin of the heelbone (calcaneus)
below, converting a series of bony grooves in this situation into canals for the
passage of the tendons of the flexor muscles and the posterior tibial vessels
and tibial nerve into the sole of the foot.
2) Peroneal retinacula-
The peroneal retinacula (singular: peroneal retinaculum) are
fibrous retaining bands which bind down the tendons of the peroneus longus
and brevis as they run across the side of the ankle. (Retinaculum is Latin for
retainer). These bands consist of superior and inferior fibers.
3) Superior extensor retinaculum of foot-
The superior extensor retinaculum of the foot (transverse
crural ligament) is the upper part of the extensor retinaculum of foot which
extends from the ankle to the heelbone.

54
4) Inferior extensor retinaculum of foot-
The inferior extensor retinaculum of the foot (cruciate crural
ligament, lower partofanterior annular ligament) is a Y-shaped band placed in
front of the ankle-joint, the stem of the Y being attached laterally to the
upper surface of the calcaneus, in front of the depression for the
interosseous talocalcaneal ligament; it is directed medialward as a double
layer, one lamina passing in front of, and the other behind, the tendons of the
peroneu tertius and extensor digitorum longus.
5) Superior fibular retinaculum-
The superior fibular retinaculum is one of two fibrous
bands that bind the peroneus longus and peroneus brevis muscle tendons that
run over the ankle's lateral side. ... Its fibers are connected to the lateral
malleolus (the bony projections at the outside of each ankle) and the
calcaneus's (heel bone) lateral surface.
6) Inferior fibular retinaculum-
A retinaculum refers to any region on the body where
tendon groups from different muscles pass under one connective tissue band.
The inferior retinaculum is responsible for stabilizing the tendons that extend
from the calf muscles as they run down the leg to reach both sides of the
ankle.

55
In the knee:
1) Lateral retinaculum
Figure no 27- Lateral retinaculum
The lateral retinaculum is the fibrous tissue on the lateral (outer) side of the
kneecap (patella). The kneecap has both a medial (on the inner aspect) and a
lateral (on the outer side) retinaculum, and these help to support the kneecap
in its position in relation to the femur bone underneath it.

56
1) Medial patellar retinaculum
Figure no 28-Medial patellar retinaculum
If a retinaculum is injured, it may lead to an impairment of tendon
functionally. If the peroneal retinaculum tears or stretches, it may cause the peroneal
tendons to detach from the fibula. This may cause damage to the tendons and impair
their functionality, leading to a condition known as peroneal tendon dysfunction.
Histology of retinaculum-
Structurally the retinaculum consists of three layers. The deepest layer,
the gliding layer consists of hyaluronic acid secreting cells. The thick middle layer
consists of interspersed elastin fibers, collagen bundles and fibroblasts. The most
superficial layer is made up of loose connective tissue which contains vascular
channels. Combined these three layers create a smooth gliding surface as well as
mechanically strong tissue which prevents tendon bowstringing.

57
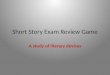
2) ANATOMY OF SKIN
The skin is the largest organ of the body, with a total area of about
20 square feet. The skin protects us from microbes and the elements, helps
regulate body temperature, and permits the sensations of touch, heat and cold.
Skin has three layers:
The epidermis, the outermost layer of skin, provides a waterproof barrier and
creates our skin tone.
The dermis, beneath the epidermis, contains tough connective tissue, hair
follicles, and sweat glands.
The deeper subcutaneous tissue (hypodermis) is made of fat and connective
tissue.
The skin‘s color is created by special cells called melanocytes, which
produce the pigment melanin. Melanocytes are located in the epidermis.
The human skin is the outer covering of the body and is the largest organ of the
integumentary The skin has up to seven layers of ectodermal tissue and guards the
underlying muscles, bones, ligaments and internal organs Human skin is similar
to most of the other mammals skin, and it is very similar to pig skin Though
nearly all human skin is covered with hair follicles, it can appear hairless. There
are two general types of skin, hairy and glabrous skin (hairless). The adjective
cutaneous literally means "of the skin" (from Latin cutis, skin).

58
Because it interfaces with the environment, skin plays an important immunity role in
protecting the body against pathogens and excessive water loss. Its other functions
are insulation, temperature regulation, sensation,
synthesis of vitamin D, and the protection of vitamin B floats. Severely damaged skin
will try to heal by forming scar tissue. This is often discolored and depigmented.
In humans, skin pigmentation varies among populations, and skin type can range from
dry to oily. Such skin variety provides a rich and diverse habitat for bacteria that
number roughly 1000 species from 19 phyla, present on the human skin.
STRUCTURE
Skin has mesodermal cells, pigmentation, such as melanin provided by melanocytes,
which absorb some of the potentially dangerous UV radiation in sunlight. It also
contains DNA repair enzymes that help reverse UV damage, such that people lacking
the genes for these enzymes suffer high rates of skin cancer. One form predominantly
produced by UV light, malignant melanoma, is particularly invasive, causing it to
spread quickly, and can often be deadly. Human skin pigmentation varies among
populations in a striking manner. This has led to the classification of peoples on the
basis of skin color. Terms of surface area, the skin is the second largest organ in the
human body (the inside of the small intestine is 15 to 20 times larger). For the average
adult human, the skin has a surface area of between 1.5-2.0 square meters. The
thickness of the skin varies considerably over all parts of the body, and between men
and women and the young and the old. An example is the skin on the forearm which

59
is on average 1.3 mm in the male and 1.26 mm in the female. His average square inch
of skin holds 650 sweat glands, 20 blood vessels, 60,000 melanocytes, and more than
1,000 nerve endings. The average human skin cell is about 30 micrometers in
diameter, but there are variants. A skin cell usually ranges from 25-40 micrometers
(squared), depending on a variety of factors.
Skin is composed of three primary layers: the epidermis, the dermis and the
hypodermis.
Epidermis-
Epidermis, "epi" coming from the Greek meaning "over" or "upon", is the outermost
layer of the skin. It forms the waterproof, protective wrap over the body's surface
which also serves as a barrier to infection and is made up of stratified squamous
epithelium with an underlying basal lamina.
The epidermis contains no blood vessels, and cells in the deepest layers are nourished
almost exclusively by diffused oxygen from the surrounding air and to a far lesser
degree by blood capillaries extending to the outer layers of the dermis.
The stratified, squamous, cornifying epithelium that is populated by 4 types of cells.
a. Keratinocytes
b. Melanocytes
c. Langerhans cells
d. Merkel cells

60
a) Keratinocytes:
Figure no 29- Keratinocytes
90% of epidermal cells are Keratinocytes they produce a protein called keratin. These
substances helps waterproof and protect the skin and underlying tissues from light,
heat, microbes, many chemicals. Anchoring junctions, desmosomes held
Keratinocytes to one another. Epidermal Keratinocytes undergoes characteristic
changes as they are progressively moved upward from basal of epidermis to the
chornified layer. Four interrelated cellular layer i.e. basal, spinosum, granular,
chornified can be recognized as successive stage of differentiation of germinal
Keratinocytes to chornified keratinocyte. Epidermal chornification is a form of
cellular differentiation that results in the formation of the outermost dead layer of
skin.

61
b) Melanocytes:
Melanocytes are dendritic cells Melanocytes are pigment producing cells of neuro
ectodermal origin. This cell synthesized melanin from tyrosin, a pigment responsible
for skin colour and essential for protection from UV light. Amount of the melanin in
Keratinocytes determines the skin colour. Facial differences in colour are the result
of metabolically active Melanocytes. Melanocytes appear microscopically as clear
cells in and immediately beneath the basal layer of epidermis.
Figure no 30-Melanocyte
The nucleus of a Melanocytes is smaller and more deeply basophilic then that
of Keratinocytes. The ratio of Melanocytes to Keratinocytes in the basal layer of
epidermis varies from 1:4 to 1:10 depending on the region of body example-
Melanocytes are more abundant in the skin of chicks then in that of abdomen. There
are two classes of integumentary melanin. Eumelanin produced in ellipsoidal
melanosomes (Eumelanosomes) account for the brown and black colours of both skin

62
and hair. Pheomelanin, produced in perikal melanosomes (pheomelanosome) account
for the lighter colour of hair, ranging from yellow to reddish brown.It is the amount of
melanin in Keratinocytes that determines the degree of pigmentation of skin and hair.
The principle function of melanin is to protect the skin from the
harmful effect of sunshine by scattering and observing UV.
c) Langerhans cells:-
Figure no 31-Langerhans cell
Are the macros phases like antigen producing cells located above the basal layer of
keratinocyte, which interact with hyper t cells with assisting with the immune
response may be a possible source of prostaglandin. Langerhans cells first described
by Paul Langerhans in 1868.although this cell constitute about 4% of the cell
population of epidermis, regional variation occurs in their distribution their number
varying between 460 and 1000 per (mm)sq of epidermis. The cross sectional

63
appearance of langerhans cell granules has been likened in shape to a tennis racket,
vesicular dilation at one end at a rod like segment. A langerhans cell plays an
important role in various immune process including allergic contact dermatitis,
immune tolerance and surveillance against neoplasio.
d) Merkel cells:
Figure no 32- Merkel cell
Merkel cells are non-pigmented dedrosides cytoplasmic dense core granules, which
function as touch receptors and also interact with separates t cells in assisting with
immune response. Endothelial cells are not found since the epidermis lack blood
vessels. Nutrient delivery and waste transport are by diffusion. There are capillary
networks in the papillary dermis which provide this function. Merkel cells make
contact with the flattened portion of ending of sensory neuron called as tactile
(merkel) disc and are thought to function in the sensation of touch. In 1875 fried rich

64
merkel identified unique cells of the basis of epidermal rate ridges that were in
contact with nerves fibrils. He named cells as ―TOUCH CELLS.
The names of 5 layers of epidermis from deepest to the most superficial are:
1) Stratum basale (basale-base):
Figure no 33- stratum basale
This layer is also called stratum germinativum to indicate its role in
germinating new cells.This single layer of cuboidal to columnar shaped cells contains
stem cells. Which are capable of continued cell division &melanocytes.The stem cells
multiply, producing Keratinocytes which push up towards the surface & become part
of more superficial layers.The nuclei of Keratinocytes degenerate &die. Eventually,
the cell remnants are shed from the surface layer of epidermis. During embryological
development, other stem cells are migrating into the dermis & give rise to sweat& oil
glands & hair follicles.The stratum basale also contain tactile cells (merkel cells) that

65
are sensitive to touch.
Function- The stratum basale also contains melanocytes, cells that produce melanin,
the pigment primarily responsible for giving skin its color. Melanin is transferred to
keranocytes in the stratum spinosum to protect cells from UV rays.
2) Stratum spinosum (spisum-throne like or prickly):
Figure no 34- stratum spinosum
This layer contains of prickle cells, which is composed of several layer of polyhedral
cells. From these plaques numerous fine fibrils radiate into the cell cytoplasm. Some
maintain that the fibrils do not exist as such in living unfixed cells. When the cells are
isolated these desmosomes are broken & surfaces of cells are beset with numerous
short than like processes, named prickle cells. These layers contain of 8-10 closely
fitted rows of polyhedral cells. These cells are able to synthesis protein but cannot
reproduce.

66
Long projections of melanocytes extend among the Keratinocytes, which take in
melanin by phygocytosis of these melanocyte projections.
Function- it is partly responsible for the skins strength and flexibility.
3) Stratum granulosum-
This layer is also known as granular layer. It comprises 2 or 3 layers of fusiform cells.
Which contain numerous granules which stain readily haematoxylin due to
accumulation of readily stainable granules of keratohyline in their cytoplasm.
Figure no 35- stratum granulosum
In this layer, keratin, the water proofing protein is produced. In the stratum
granulosum, the cells appears in various stages of degeneration & as a rule, break down
& cell death occurs.

67
Function- The cells of the stratum granulosum accumulate dense basophilic
keratohyalin granules. These granules contain lipids, which along with the
dermosomal connections help to form a waterproof barrier that functions to prevent
fluid loss from yhe body.
4) Stratum lucidum (lucidus- clear):
Figure no 36- stratum lucidum
This is clear layer appears in section as a homogeneous or deeply
seated layer, composed of closely packed cells in which traces of flattened nuclei may
be found. This layer consists of 3-4 rows of clear, flat dead cells. It is best seen in
regimen where the horizon is thick skin of the palms & soles of the feet.
Function- this is responsible for the capability of the skin to stretch. It also contains a
protein that is responsible for the degeneration of skin cells. This layer also lowers the
effects of friction in skin.

68
5) Stratum corneum(corneum- horny):
Figure no 37- stratum corneum
It is known as horny layer. It consists of several layers of horny,
epithelial cells, in which no nuclei are discernable & their protoplasm has been
converted into a material known as keratin. The outer most cells containing the tough
protein keratin are known as Keratinocytes. They consist of 25-30 rows of dead flat
cells. The cells are continuously shed & replaced by the newly divided cells. The
stratum corneum serves as an effective barrier against light, heat, bacteria & many
chemicals.
Function-The function is to form a barrier to protect underlying tissue from
infection, dehydration, chemicals and mechanical stress.
The daughter cells move up the strata changing shape and composition as they
die due to isolation from their blood source. The cytoplasm is released and the protein

69
keratin is inserted. They eventually reach the corneum and slough off (desquamation).
This process is called "keratinization". This keratinized layer of skin is responsible for
keeping water in the body and keeping other harmful chemicals and pathogens out,
making skin a natural barrier to infection.
Components
The epidermis contains no blood vessels, and is nourished by diffusion from
the dermis. The main type of cells which make up the epidermis are keratinocytes,
melanocytes, Langerhans cells and Merkel cells. The epidermis helps the skin to
regulate body temperature.
Layers
Epidermis is divided into several layers where cells are formed through
mitosis at the innermost layers. They move up the strata changing shape and
composition as they differentiate and become filled with keratin. They eventually
reach the top layer called stratum corneum and are sloughed off, or desquamated.
This process is called keratinization and takes place within weeks. The outermost
layer of the epidermis consists of 25 to 30 layers of dead cells.
Blood capillaries are found beneath the epidermis, and are linked to an
arteriole and a venule. Arterial shunt vessels may bypass the network in ears, the nose
and fingertips.
Genes and proteins expressed in the epidermis
About 70% of all human protein-coding genes are expressed in the skin.
Almost 500 genes have an elevated pattern of expression in the skin. There are less
than 100 genes that are specific for the skin and these are expressed in the epidermis.
An analysis of the corresponding proteins shows that these are mainly expressed in
keratinocytes and have functions related to squamous differentiation and
cornification.

70
Dermis
The dermis is the layer of skin beneath the epidermis that consists of
connective tissue and cushions the body from stress and strain. The dermis is tightly
connected to the epidermis by a basement membrane. It also harbors many nerve
endings that provide the sense of touch and heat. It contains the hair follicles, sweat
glands, sebaceous glands, apocrine glands, lymphatic vessels and blood vessels. The
blood vessels in the dermis provide nourishment and waste removal from its own cells
as well as from the Stratum basale of the epidermis.
The dermis is structurally divided into two areas:
1) A superficial area adjacent to the epidermis, called the papillary layer,
2) A deep thicker area known as the reticular layer.

71
1)Papillary layer:
Figure no 38- Papillary layer
The papillary layer consist of numerous highly sensitive & vascular eminences ,
termed papillae which rise perpendicularly .The papillae are minute conical
projections , having round or blunted extremities ,which may be surfaces of
epidermis. On the general surface of the body & especially in parts endowed with
slight sensibility, they are few in number & exceedingly minute. But upon the palmer
surfaces of hands & fingers & plantar surfaces of feet & toes, they are larger &
closely aggregated together & arranged in parallel curved lines forming elevated
ridges seen on the epidermis. Each ridge contains 2 rows of papillae & between the
rows the ducts of sweat gland pass outwards to open on the summits of the ridges.
Each papillae consist of very small & closely interlacing bundles of finely fibrillated
tissue, with a few elastic fibres, within this tissue there is a capillary loop & in some

72
papillae especially in palms of hands & fingers. There are tactile corpuscles. Papillary
layer has many small, elongated projections called rete peges, also contains loops of
capillaries & these projects into epidermis. Size & arrangement of dermal papillae
from ridge which are external surface of epidermis & provide attachment of epidermis
to dermis & its collagen fibres. In some dermal papillae are present meissner‘s
corpuscles, the nerve ending sensitive to light touch.
2) Reticular layer
Figure no 39- Reticular layer
The reticular region lies deep in the papillary region and is usually much
thicker. It is composed of dense irregular connective tissue, and receives its name
from the dense concentration of collagenous, elastic, and reticular fibers that weave
throughout it. These protein fibers give the dermis its properties of strength,
extensibility, and elasticity.
Also located within the reticular region are the roots of the hairs, sebaceous
glands, sweat glands, receptors, nails, and blood vessels.

73
Tattoo ink is held in the dermis. Stretch marks often from pregnancy and obesity, are
also located in the dermis. It consist of strong inter lacing bands, composed cheaply of
white fibrous tissue & containing some yellow elastic fibers, which vary in number in
different parts. In the deeper part the fasciculi are course & large intervals left by their
interlacement are occupied by adipose tissue & sweat glands. Below reticular layer,
there is subcutaneous areolar tissue which except in a few situations contains fat. The
connective tissue bands in reticular layer lie for the main part in parallel bundles so
that if conical object is stabbed through skin & then withdrawn it leaves a linear
wound since the fibers are forced apart with much rupture. The directions taken by the
parallel bundles vary in different part of the body & constitute what are termed the‖
cleavage lines‖, which heal with formation of scar tissue, whereas the incision across
these lines, owing to retraction of the several fibers lead to the formation of the broad
scar. The cleavage lines are arranged longitudinally in the skin of the limbs & more
or less horizontally in the trunk & neck. With increasing age the yellow elastic fibers
atrophy and the skin loses much of its elasticity and become wrinkled. If the skin
becomes much stretched (as by rapidly growing tumors, fat deposition or pregnancy)
the fibers in reticular layer may undergo partial rupture, followed by scar formation;
these areas may show on the surface as white streaks. These are commonly seen in the
anterior wall of abdominal wall after pregnancy and known as linear gravidarum. In
many regions the skin is separated from deep fascia or other structures by loose
areolar tissue and where the skin is freely movable over the deeper structures.
Elsewhere, however, the skin may be firmly anchored to structures like the
periosteum over‖ subcutaneous‖ parts of bones or to the deep fascia in regions related
to movements of underlying joints. In joints there are permanent creases known as
―flexure lines‖; they are particularly evident on the palm of the hand and flexor
surfaces of the digits, where they are arranged in relation to the movements of the
digits. The remaining reticular layer is made of dense irregular, collagenous tissue,
which allows strength & flexibility in every direction. The primary cell of this layer is
fibroblast, which produce the key structure of extra cellular matrix protein namely
collagen & elastin. These cells produce the key adhesive proteins used to attach
epidermal cells to the basement membrane & are used for epidermal cell migration &

74
replication. The fibronectin is a key fibroblast derived signal protein for the
orchestration of the healing ground substance or matrix. This is made of
polysaccharide protein complexes known as GAG or hyaluronic acid, which is semi
fluid that allows cells & connective tissue orientation, provide nutrients diffusion to
the cells & also provides scaffolding for cell migration. The space between interfacing
connective tissue fibers are occupied by adipose tissue, blood vessels, sweat glands,
nerves & hair follicles. It is attached to the underlined structure by the subcutaneous
layer of tissue.
Subcutaneous tissue(hypodermis)-
The subcutaneous tissue (also hypodermis and sub cutis) is not part of the
skin, and lies below the dermis of the cutis. Its purpose is to attach the skin to
underlying bone and muscle as well as supplying it with blood vessels and nerves. It
consists of loose connective tissue, adipose tissue and elastin. The main cell types are
fibroblasts, macrophages and adipocytes (subcutaneous tissue contains 50% of body
fat). Fat serves as padding and insulation for the body.

75
CROSS SECTION
Figure no.40- cross section of skin

76
Figure no 41- cross section of skin( thick and thin skin)

77
Table no.6
Special Features of the Different Layers of Epidermis –
Sr no Epidermis Cells Special feature
1 Stratum corneum (Horny layer)
Corneocytes
Stratified epithelial cells
Fibrous protein
keratin is present
2 Stratum lucidum Flattened epithelial cells Eleidin (Precursor
of keratin) is
present.
3 Stratum granulosum Flattened rhomboid cells
Three cells layered
Keratohyalin is
present in shape
of granules
4 Stratum spinosum (Prickle cell layer)
Several (3–5) cells thick.
Cell possess spine-like
Projection
Some melanocyte.
5 Stratum germinativum Polygonal cells—
Superficially.
Columnar or cuboidal
Epithelial cells— deep
Keratinocytes.
Melanocytes.

78
DEVLOPMENT
Skin color
Human skin shows high skin color variety from the darkest brown to the
lightest pinkish-white hues. Human skin shows higher variation in color than any
other single mammalian species and is the result of natural selection. Skin
pigmentation in humans evolved to primarily regulate the amount of UVR penetrating
the skin, controlling its biochemical effects.
The actual skin color of different humans is affected by many substances, although
the single most important substance determining human skin color is the pigment
melanin. Melanin is produced within the skin in cells called melanocytes and it is the
main determinant of the skin color of darker-skinned humans. The skin color of
people with light skin is determined mainly by the bluish-white connective tissue
under the dermis and by the hemoglobin circulating in the veins of the dermis. The
red color underlying the skin becomes more visible, especially in the face, when, as
consequence of physical exercise or the stimulation of the nervous system (anger,
fear), arterioles dilate.
There are at least five different pigments that determine the color of the skin.These
pigmentsare present at different levels and places
Melanin: It is brown in color and present in the basal layer of the epidermis.
Melanoid: It resembles melanin but is present diffusely throughout the
epidermis.
Carotene: This pigment is yellow to orange in color. It is present in the stratum

79
corneum and fat cells of dermis and superficial fascia.
Hemoglobin: It is found in blood and is not a pigment of the skin but develops a
purple color.
Oxyhemoglobin: It is also found in blood and is not a pigment of the skin. It
develops a red color.
There is a correlation between the geographic distribution of UVR and the
distribution of indigenous skin pigmentation around the world. Areas that
highlight higher amounts of UVR reflect darker-skinned populations,
generally located nearer towards the equator. Areas that are far from the
tropics and closer to the poles have lower concentration of UVR, which is
reflected in lighter-skinned populations there is a correlation between the
geographic distribution of UV radiation (UVR) and the distribution of
indigenous skin pigmentation around the world. Areas that highlight higher
amounts of UVR reflect darker-skinned populations, generally located nearer
towards the equator. Areas that are far from the tropics and closer to the poles
have lower concentration of UVR, which is reflected in lighter-skinned
populations.
In the same population it has been observed that adult human females are
considerably lighter in skin pigmentation than males. Females need more calcium
during pregnancy and lactation, and vitamin D which is synthesized from sunlight
helps in absorbing calcium. For this reason it is thought that females may have
evolved to have lighter skin in order to help their bodies absorb more calcium.

80
The Fitzpatrick scale is a numerical classification schema for human skin color,
developed in 1975 as a way to classify the typical response of different types of skin to
UV light.
Table no 7- cause and color of skin
Sr no Cause Color of skin
1 Always burns, never tans Pale, fair, freckles
2 Usually burns, sometimes tans Fair
3 May burn, usually tans Light brown
4 Rarely burns, always tans Olive brown
5 Moderate constitutional pigmentation Brown
6 Marked constitutional pigmentation Black
In the same population it has been observed that adult human females are
considerably lighter in skin pigmentation than males. Females need more calcium
during pregnancy and lactation, and vitamin D which is synthesized from sunlight
helps in absorbing calcium. For this reason it is thought that females may have
evolved to have lighter skin in order to help their bodies absorb more calcium.
Aging
As skin ages, it becomes thinner and more easily damaged. Intensifying this
effect is the decreasing ability of skin to heal itself as a person ages.
Among other things, skin aging is noted by a decrease in volume and
elasticity. There are many internal and external causes to skin aging. For example,

81
aging skin receives less blood flow and lower glandular activity.
A validated comprehensive grading scale has categorized the clinical findings of skin
aging as laxity (sagging), rhytids (wrinkles), and the various facets of photoaging,
including erythema (redness), and telangiectasia, depigmentation (brown
discoloration), solar elastosis (yellowing), keratoses (abnormal growths) and poor
texture.
Cortisol causes degradation of collagen accelerating skin aging.
Anti-aging supplements are used to treat skin aging.
Photo aging
Photo aging has two main concerns: an increased risk for skin cancer and the
appearance of damaged skin. In younger skin, sun damage will heal faster since the
cells in the epidermis have a faster turnover rate, while in the older population the
skin becomes thinner and the epidermis turnover rate for cell repair is lower which
may result in the dermis layer being damaged.
Functions
Skin performs the following functions:
1. Protection: an anatomical barrier from pathogens and damage between the
internal and external environment in bodily defense; Langerhans cellsin the
skin are part of the adaptive immune system.Perspiration contains lysozyme
that breaks the bonds within the cell walls of bacteria.
2. Sensation: contains a variety of nerve endings that react to heat and cold,
touch, pressure, vibration, and tissue injury.

82
3. Heat regulation: the skin contains a blood supply far greater than its
requirements which allows precise control of energy loss by radiation,
convection and conduction. Dilated blood vessels increase perfusion and heat
loss, while constricted vessels greatly reduce cutaneous blood flow and
conserve heat.
4. Control of evaporation: the skin provides a relatively dry and semi-
impermeable barrier to fluid loss.
Loss of this function contributes to the massive fluid loss in burns.
5. Aesthetics and communication: others see our skin and can assess our mood,
physical state and attractiveness.
6. Storage and synthesis: acts as a storage center for lipids and water, as well as
a means of synthesis of vitamin D by action of UV on certain parts of the skin.
7. Excretion: sweat contains urea, however its concentration is 1/130th that of
urine, hence excretion by sweating is at most a secondary function to
temperature regulation.
8. Absorption: the cells comprising the outermost 0.25–0.40 mm of the skin are
"almost exclusively supplied by external oxygen", although the "contribution
to total respiration is negligible" In addition, medicine can be administered
through the skin, by ointments or by means of adhesive patch, such as the
nicotine patch or iontophoresis. The skin is an important site of transport in
many other organisms.
9. Water resistance: The skin acts as a water-resistant barrier so essential
nutrients are not washed out of the body.

83
Skin flora
The human skin is a rich environment for microbes. Around 1000 species of bacteria
from 19 bacterial phyla have been found. Most come from only four phyla:
Actinobacteria (51.8%), Firmicutes (24.4%), Proteobacteria (16.5%), and
Bacteroidetes (6.3%). Propionibacteria and Staphylococci species were the main
species in sebaceous areas. There are three main ecological areas: moist, dry and
sebaceous. In moist places on the body Corynebacteria together with Staphylo
coccidominate. In dry areas, there is a mixture of species but dominated by b-
Proteobacteria and Flavobacteriales. Ecologically, sebaceous areas had greater species
richness than moist and dry ones. The areas with least similarity between people in
species were the spaces between fingers, the spaces between toes, axillae, and
umbilical cord stump. Most similarly were beside the nostril, nares (inside the nostril),
and on the back.
Reflecting upon the diversity of the human skin researchers on the human skin
observed "hairy, moist underarms lie a short distance from smooth dry forearms, but
these two niches are likely as ecologically dissimilar as rainforests are to deserts."
Microorganisms like Staphylo coccus epidermis‘s colonize the skin surface. The
density of skin flora depends on region of the skin. The disinfected skin surface gets
recolonized from bacteria residing in the deeper areas of the hair follicle, gut and
urogenital openings.

84
Clinical significance
1) Diseases of the skin include skin infections and skin neoplasms (including skin
cancer).
2) Dermatology is the branch of medicine that deals with conditions of the skin.
3) The skin is the body‘s largest organ, and it serves as a protective barrier. Its health
and surface appearance are determined by environmental factors as well as the
function of the components that comprise the layers below.
Hygiene and skin care
The skin supports its own ecosystems of microorganisms including yeasts and
bacteria which cannot be removed by any amount of cleaning. Estimates place the
number of individual bacteria on the surface of one square inch of human skin at 50
million, though this figure varies greatly over the average 20 square feet of human
skin. Oily surfaces such as the face may contain over 500 million bacteria per square
inch. Despite these vast quantities, all of the bacteria found on the skin surface would
fit into a volume the size of pea. In general the microorganisms keep one another in
check and are part of healthy skin. When the balance is disturbed, there may be an
overgrowth and infection, such as when antibiotics kill microbes, resulting in an
overgrowth of yeast. The skin is continuous with the inner epithelial lining of the
body at the orifices, each of which supports its own complement of microbes.
Sunlight, water and air play important role in keeping the skin healthy.

85
Oily skin
Oily skin is caused by over active sebaceous glands that produce a
substance called sebum, a naturally healthy skin lubricant. A high glycemic index diet
and dairy products consumption increase IGF-1 generation which in turn increases
sebum production. Over washing the skin does not cause sebum over production but
may cause dryness.
When the skin produces excessive sebum, it becomes heavy and
thick in texture. Oily skin is typified by shininess, blemishes and pimples. The oily
skin type is not necessarily bad, since such skin is less prone to wrinkling, or other
signs of aging, because the oil helps to keep needed moisture locked into the
epidermis.
The negative aspect of the oily skin type is that oily complexions are
especially susceptible to clogged pores, black heads and buildup of dead skin cells on
the surface of the skin. Oily skin can be sallow and rough in texture and tends to have
large,clearly visible pores everywhere, except around the eyes and neck.

86
ACTION & FUNCTIONS OF LIGAMENT
Ligaments attach two bones or cartilages, it helps in supporting and keeping the organ
in position, it is made of fibrous tissue.
1) One of the main functions of ligaments is mechanical as they passively stabilize
joints and help in guiding those joints through their normal range of motion when a
tensile load is applied. Ligaments exhibit nonlinear anisotropic mechanical behavior
and under low loading conditions they are relatively compliant, perhaps due to
recruitment of "crimped" collagen fibers as well as to viscoelastic behaviors and
interactions of collagen and other matrix materials. Continued ligament loading
results in increasing stiffness until a stage is reached where they exhibit nearly linear
stiffness and beyond this, ligaments continue to absorb energy until tensile failure.
2) Another ligament function relates to its visco elastic behavior in helping to provide
joint homeostasis. A ligament "load relaxes" which means that loads/stresses decrease
within the ligament if they are pulled to constant deformations. Ligaments
also"creep"which is defined as the deformation (or elongation) under a constant or
cyclically repetitive load. Creep is particularly important when considering joint
injury or reconstructive surgery as excessive creep could result in laxity of the joint
thus predisposing it to further injury.
3) A third function of ligaments is their role in joint proprioception, which is referred
to as the conscious perception of limb position in space. In joints such as the knee,
proprioception is pro-vided principally by joint, muscle and cutaneous receptors.
When ligaments are strained, they invoke neurological feed-back signals that activate

87
muscular contraction and this appears to play a role in joint position sense. Although
progress continues to be made to elucidate the role of proprioception in normal
ligament function.

88
DIFFERENCE BETWEEN TENDON & LIGAMENT & MUSCLES
1) TENDONS
Tendons are dense connective tissues and are dominated by regularly arranged
collagen fibers. They serve primarily to transfer the pull of muscles to bone. They also
play a fundamental role in locomotion, transferring the forces generated by our
muscles to the skeleton, and thus facilitating movement. In addition, they stabilize the
joint, and act as shock absorber to limit muscle damage. Some tendons have an
additional energy storing function which when stretched under load they then recoil.
This lessens the energetic cost of locomotion, as a reduced muscular effort is required
to return the limb to the starting position. Examples of energy storing tendons are the
human Achilles tendon and equine superficial digital flexor tendon. However, tendons
such as the human anterior tibialis tendon and the equine common digital extensor
tendon act purely to position the limb and are relatively inextensible to allow efficient
transfer of force from muscle to bone and precise placement of the limb.
Macroscopically healthy tendons are white in color and have a fibro-elastic
texture. They can vary remarkably in shape and size and in the way they are
attachedto the bone; some tendon can be rounded or cord- like, straplike bands appear
like, or flattened ribbons.The point of unification of tendon to the muscle is referred to
as the myo tendinous junction and the point of unification of tendon with bone as the
osteotendinous junction. The connection of the proximal tendon of a muscle to bone is
called the muscle origin, and the distal tendon connection is known as an
insertion.The myo tendinous is important for force transmission of contracted muscle

89
to tendon. At this region collagen fibers of tendon are inserted into deep recesses
formed by myocyte processes, which allows the tension that has been generated by
contractile proteins of muscle fibers to be transferred to the collagen fibrils. Enthesis
is the interface between tendon and bone and is classified in to four zones: fibrous
tissue, fibrocartilage, mineralised fibrocartilage and bone. The presence of
fibrocartilage in tendon is an adaptation to resist compression and/or shear forces
Connects skeletal muscles to bones.
Tough and elastic.
Proteoglycan content is less.
White in color.
Blood supply is good.
Fibroblasts lie in a continuous row.
The fibers are compact and present in Parallel bundles.

90
2) LIGAMENTS
Ligament is another dense regular connective, which joins bone to bone. Similar to
tendons, ligaments vary in size, form, orientation and location. Grossly, ligament
appears white, firm,homogenous and fibrous.Ligament can be categorized into at least
two major subgroups; those found in the musculoskeletal system and those connecting
other soft tissues, for instance the suspensory ligament in the abdomen. They are
named based on the point of bony attachment, shape, function, their relation to joints
or surfaces and their relationship to each other. Skeletal ligaments play essential roles
for accurate joint function. They passively stabilize the joint and are responsible for
guiding movement of the joint through a normal range of motion. They are
responsible for preventing or blocking abnormal joint movement within set limits.
Another function of articular ligament role in joint is in proprioception, which
provides feedback relating position space of the joint and contributes to the
coordinated movement of the limbs. Ligament contains different regions similar to
what has been previously described in tendon. For instance the anterior cruciate
ligament has a proximal origin from the femur and a distal insertion on the tibia. The
cruciate ligaments of the knee joint are examples of ligaments with direct enthesis at
both the femoral and tibial insertions, whilst medial collateral ligament has an indirect
enthesis at the tibial insertion.The formation of fibro cartilaginous matrix in both
tendon and ligament is thought to occur at sites that are under compression.
Connect bones to bones.
Elastic in nature.
Connects the end of the bones at joints.

91
Each joint contains many ligaments
Proteoglycan content is more.
Yellow in color.
Blood supply is poor
Fibroblasts are scattered.
They are not arranged in Parallel bundles but are compactly packed
3) MUSCLES
Muscles are allowing us to move our body. They enable our internal organs to
function. The human body has over 600 muscles which make up around 40
percent of our bodyweight. There are 3 types of muscles-
a. Skeletal muscle
b. Cardiac muscle
c. Smooth muscle
a) Skeletal muscle
Skeletal muscles move the external parts of the body and the limbs. Skeletal
muscles cover the bones and give our bodies their shape. There are about 320
pairs of identical bilateral muscles, when one muscle contracts the other
expands and this allows movement. Facial expression such as smiles, frowns,
mouth and tongue movements are all controlled by the skeletal muscles.

92
b) Cardiac muscle
Cardiac muscles are responsible for heartbeat. They only exist only in the
heart. The cardiac muscles work without stopping day and night. They work
automatically but they are similar in structure to the skeletal muscle. They
make the heart contract so that the heart can squeeze our blood and release so
that the heart can fill up with blood again.
c) Smooth muscle
Smooth muscles are responsible for movements in the stomach, intestine,
heart, arteries and hollow organs. These muscles are activate automatically.
The smooth muscles in the walls of the intestine contract and push food
forward. During child birth the smooth muscles in a women‘s uterus contract.
Our pupils shrink and expand depending on how much light there. These
movements depend on smooth muscle movements. Smooth muscles are also
present within the walls of the bladder, the bronchi, and the arrestors pill in the
skin which makes the hair stand up.
Muscles are highly vascular organ.
Muscle tissue is soft tissue.
Movement and regulation.
Posture & support
Body temperature regulation
Muscle contains special protein called contractile protein called myofilaments.
Muscles having high rate of metabolic activity.

93
Muscles having ability of contractility, extensibility, and elasticity.
Muscles having abundant supply of blood vessels and nerves.
Muscles transmits electrical impulses.

94
4. Methadology
MATERIALS AND METHODS
MATERIAL
1) Literature present in classical texts,tikakaras and in modern books available in
our institute.
METHODS
1) Study design
A) Literary study
Literary study-
All the information about mansavaha strotas and its moolasthana by sushruta
and its tikakaras was studied. Relation of snayu with other factors like
Dhatus was studied. Also did the study of thickness of tvaca told by Sushruta
and its tikakaras. Also the tvaca utpatti, utpatti kala,thickness of tvaca, tvaca
as diagnostic stool in clinical examination,Vrana vastu, tvaca as a prognostic
stool is also studied. In case of modern aspect of tvaca and snayu,all the
information regarding anatomy of skin and ligament is compiled from
different textbooks of anatomy. Finally the study of mansavaha strotas
moolasthana and its tikakaras is done.

95
METHOD OF SELECTION
1) Inclusion criteria
Literature available in sushrutasamhita and its tikakaras and in modern
texts.
2) Exclusion criteria
- Charaksamhita ,waghbhata And laghutrayee

Sample size of estimation-
It is not applicable for this study.

96
5. RESULTS
1) According to sushruta, there is snayu and tvaca are the moolasthana of
mansavaha strotas.
2) Also according to sushruta sanhita tikakaras, moolasthana of mansavaha strotas
is snayu and tvaca.
3) Acharya sushruta and its tikakaras mentioned that there are four kinds of
snayu viz. pratanvati snayu, vratta snayu, pruthu snayu and sushir snayu.
4) Snayus are the structures which maintain the body posture by joining the
mansa and asthi and provide the strength for the body to perform its activities.
5) These snayus are compared to ligaments.
6) Acharya sushruta and its tikakaras explained that, there are seven layers of
tvaca, these are avabhasini, lohita, sveta, tamra, vedini, rohini, mansadhara.
7) Tvaca is used as diagnostic tool in clinical examination, used as rogamarga and
vrana vastu.
8) Skin is composed of three primary layers: the epidermis, the dermis and the
hypodermis.
9) The epidermis having five layers these are the stratum basale, stratum
spinosum, stratum granulosum, stratum lucidum, stratum corneum. And
dermis having two layers, papillary layer and reticular layer.
10) Ligament is the fibrous connective tissue that connects bones to other bones
and helps in supporting and keeping the organ in position.
11) Tendon plays a fundamental important role in locomotion, transferring the
forces generated by muscles.
12) Muscles are allowing moving our body and also enabling internal organs to
function.

97
6. DISCUSSION
Discussion constitutes a critical stage in the development of thesis. Data observed
during the study are pooled together and on the basis of collected information
discussion will be done through various angles.
1) According to the definition, strotomula is considered as the prabhavsthana i.e. the
place of origin from where the particular commences or gets the nutrition.
2) In the vitiation of mansavaha strotasvarious diseases like arbuda,keela,alaji,etcare
produced which are pertained to skin(tvaca) which is said to be the moolsthana of
mansavaha strotas.
Snayu is another moolsthana of mansavaha strotas. Inmansakshaya
the function of snayu also gets diminished and hence the symptoms like sandhivedna,
sandhisphotana are produced.
3) Tvaca is also explained under eight tool of shadvidha rogi
pareeksha(sparshnendriya ), thus by examining the tvaca we can have a fair idea of
the disease. In this, Rasavaha srotas mainly vitiated because of abnormal functioning
of mana and mana has direct effect on tvaca. This makes mana a leading cause of
tvaca vikara. Descriptions of tvaca in classical texts and modern texts have
tremendous similarity between these two regarding numbers, layers, thickness etc.
4) The organ genesis of tvaca occur during paka of Shukra and Shonita by Agni,
seven types of tvaca gets formed on the surface of Garbha just like while heating milk
cream is formed on its surface. Snayu is a pitruj bhava and Tvaca is a Matruja Bhava
and it having predominance of Vayu mahabhoota and sparsha Vishishta guna.

98
5) Tvaca is the external covering of the body. It is also called ―sparshanendriya or
twagndriya‖ which envelops the body. It plays a great role in perception of sensations
like touch, pain, heat, cold.
6) Thickness of tvaca told by Sushruta and Dalhana is having great difference.
Sushruta seems to be more accurate in telling thickness of tvaca which is more or less
same to the thickness quoted in modern textbooks of Anatomy.
7) Tvaca reflects varna of an individual. Tvaca is one the gnyanendriyas which is
Vayaviya in nature. Its abode is Sparshanendriya which is responsible for the touch
sensation. In all Indriyas, Sparshanendriya is an entity that occupies all other Indriyas
also.
8)Tvaca is also useful as diagnostic tool in clinical examination.
9) Tvaca is considered as a rogmarga & it is
used as a vrana vastu.
10) Skin is having protective functions helps in general sensation helps in excretion of
waste products of metabolism synthesize Vitamin – D maintains water balance and
stores fats, water and salts.
11) Skin is divided into two layers outer epidermis and inner dermis. Epidermis is
divided into 5 layers and populated by 4 types of cells. Dermis is also divided into 2
layers. Skin is supplied by sebaceous glands which keep the skin surface oily and
sweat glands which excrete waste materials of the body through sweat.

99
12) The definition also proves the concept of Ayurveda that the Snayu which are strong
cord like structure made up of fine fibers, helps in binding the body parts together,
are known as ligaments.
13) Acharya Sushruta has also recommended that the Snayu should be protected along
with other vital structure like Marma, Sira, Sandhi etc., where it becomes necessary
to perform surgery.
14) Snayu are the fiber like material which can be used for suturing purpose in place of
thread.
15) Prathu Snayu which is mentioned by Acharya Sushruta to be present in Parshva, Ura,
Prishtha etc. regions are some special form of fascia or aponeuroses either entirely or
as a part of the muscle.
16) Ligaments are viscoelastic. They gradually strain when under tension and return to
their original shape when the tension is removed.
17) Ligaments play essential roles for accurate joint function.
18) Retinaculum consists of 3 layers i.e. Deepest layer, Gliding layer and superficial
layer. Combined these three layers create a smooth gliding surface as well as
mechanically strong tissue.
19) Tendons play a fundamental role in locomotion, transferring the forces generated by
our muscles to the skeleton, and thus facilitating movements.
20) Some tendons have an additional energy storing function which when stretched under
load they then recoil.

100
21) Ligaments appears white, firm, homogenous and fibrous which joins bone to bone.
22) Muscles are allowing us to move our body also enable our internal organs to function.
23) To understand patho-physiology and anato-physiologic changes, it is necessary to
evaluate and understand Srotas and its moolasthan.
24) The human anatomy (shareera rachana) is an important for allied health sciences. It
is one of the fundamental subject to the health science. The ayurvedic life science is
also based on the human anatomy and physiology (rachana & kriya), without the
knowledge of shareera rachana and kriya, the physician cannot become perfect in the
profession. The study of human anatomy is very much vital for preventive and
curative aspect. Knowledge of snayu & tvaca is very important for physicians as well
as surgeons who are dealing with surgical removal of foreign bodies.

101
7. CONCLUSION
The conclusions which can draw are as follows-
According to acharya sushruta there is moolasthana of mansavaha strotas is
snayu and tvaca. Also sushruta tikakaras Dr.Bhaskar ghanekar and
Dalhanacharya explains there is moolsthana of mansavaha strotas is snayu and
tvaca.
Strotomoola found to be the main functioning centre of particular strotas. Any
kind of vitiation of strotas either directly or through its dhatu leads to the
vitiation of its moola and when strotomoola is affected it leads to the vitiation
of strotas. Hence, it could be said that there is 'samavaya sambadha ' between
strotas and strotamoola. The term used prabhavsthana' used for strotomoola
Should be considered as either the origin place, storage place, controlling site,
conduction place, terminating place or site of manifestation for various strotas.
Acharya Sushruta had given emphasis on the anatomical aspect of the
strotomoola.
According to Acharya Sushruta, Dr.Bhaskar Ghanekar, and Dhalanacharya
there are seven layers of tvaca and in modern science also their number is
same.
The layers of tvaca described by Acharya Sushruta and tikakaras, their names
match with the layers of skin anatomically and physiologically.
It exhibits the image of the physiological and pathological imbalances of the body‘s internal
environment.

102
Acharya Sushruta, Dr.Ghanekar and Dalhanacharya even described thickness
of each layer of tvaca, which is more or less same to the thickness quoted in
modern science.
Dr. Ghanekar, co relates ayurvedic tvaca stara to modern skin layers.
After detailed study of various concepts about tvaca from various ayurvedic
literatures and modern science,we can state that tvaca is well established tool
in clinical examination, diagnostic & prognostic aspect in medical sciences.
Tvaca is considered as a rogamarga and it is used as a vrana vastu.
Indriya pancha panchak and factors causing pratyakasha gyan can be used as a
tool to understand the Gyangrahanprakriya of any sense organ.
The meaning ofSnayu is different in different contexts such as ligament in
binding bone and joints; tendon in binding the muscle and dura matter and
apponeurosis in binding the Meda.
Snayu (ligaments) presents in the human body are closely allied to the
biological air….. vata. Snayu is one of the extra articular or subsidiary tissues,
which plays an important role in the posture of human body.
Snayu is a structure which performs the function of holding and binding the
various structures of human body like bones, muscles and adipose tissue. It
is one among the updhatu which helps the Dharana
(kÉÉUhÉÉiÉ kÉÉiÉuÉÉ)(maintainence) of body.
Snayu is used as bow string owing to its strength. Detailed observation of
these structures reveals them as generally fibrous structures which are strong

103
enough to withstand a certain amount of tension. Observations of Snayu show
it as a white, tough structure. An overall observation of these structures gives
an impression that Snayu is a fibrous structure visible in the body.
Snayu which are better known as vital points in ayurvedic anatomy in specific
locations in the human body which are characterized by the predominance of
the ligaments.
According to acharya sushruta and tikakaras Snayu are of four kinds; we can
consider below mentioned entity.
Pratanavati Snayu –
Ligaments of the limbs and
nerve Vrutta Snayu -
Tendons and large nerve
cord PruthulaSnayu -
Aponeurosis and Fascia
SushiraSnayu -
Sphinctersand ligament of
viscera
Skin is one of the sensory organs and thus helps in knowledge. It is in a way
covering of the whole bodynot only externally but also internally.
Also the skin is useful for the protection, sensation, heat regulation, control of
evaporation, aesthetics and communication, storage & synthesis, excretion,
absorption and water resistance.

104
Modern anatomy explains there is three layers of skin i.e. Epidermis, Dermis
and hypodermis.
To get a proper idea of skin diseases one must know the normal echo texture.
Hence, normal condition of skin is necessary. Hence, the sharir rachana of
tvaca has to be studied in depth.
Ligaments attach two bones or cartilages; it helps in supporting and keeping the
organ in position.
Artificial ligaments possess unique advantages such as no donor site
morbidity, early recovery and no risk of disease transmission.
The periodontal ligament is a fibrous connective tissue, physically small but
functionally important tissue in tooth support.
Retinaculum is not a part of muscle but its function is to stabilize the tendon.
Tendons are elastic and connect skeletal muscles to bone.
Also ligaments are elastic in nature and connect the bone at joints.
In Ayurveda there is 900 muscles are explained but in modern anatomy there
are 600 muscles. Muscle is of 3 type‘s i.e. skeletal muscle, cardiac muscle and
smooth muscle which is useful for movements, proper functioning of body and
maintain the posture and supports the body.

105
8. SUMMARY
This present dissertation entitles ―A literary study of mansavaha strotas
moolsthana as mentioned in sushruta samhita with special reference to modern
anatomy consist of various sections. The sections are in order to achieve the result &
the convenience for review of literature, methodology, results, discussion, summary,
conclusion, bibliography.
Introduction
Introduction gives the information and importance of mansavahastrots and its
moolasthana.
Aim and objectives
Aim
1) To study the mansavaha strotas moolasthana as per classical texts and modern
anatomy.
Objectives
1) To elobrate the moolasthana of mansavaha strotas as per sushruta samhita and
sushruta tikakaras.
2) To determine the action and functions of ligaments and differentiate tendons,
ligaments and muscles.
3) To study the modern anatomy of tvaca(skin) &snayu(ligament) in detail.

106
Review of literature-
Review of literature deals with brief collection of ayurvedic literature on mansavaha
strotas and its moolasthanai. Snayu & tvaca and modern aspect of skin &ligaments.
Result-
Result is an important part of the dissertation described with the literature of the
mansavaha strotas and its moolasthana.
Discussion-
Discussion made on the basis of data obtained on the points of mansavaha
strotas moolasthana, its tikakaras and its modern anatomy.
Conclusion
Conclusion gives the final result of work by various angles and states the output
of the study.
References-
It gives information about books referred with the name of author, publication,
year, & edition are given.

107
9. REFERENCES
Books
1. Sushrutasamhita, k. k. shrikantmurty, 1
st edition, Choukhambaorientalia, 2001.
2. Drushtarthsharirmvol -2, Vd.P.G.Athwale,4th edition,Godavari publishers,nov
2003.
3. Shareerarachanavigyana,Vd. Shivajivavhal, 3rd
edition,Shantanuprakashan,2000.
4. Human anatomy vol-1, B.D.Chaurasia, 4th edition, C b s publishers, 2004.
5. Cunninghams manual of practical anatomy vol-1,G.J.Romanes,15th
edition,Oxford medical publication.
6. Sushrutasamhitavol 1,Kavirajdrambikadattashashtri,14th edition,Choukambha
Sanskrit sansthan.
7. Aayurvedarth anatomy,Dr. vinaymukeshkumarpandey,1 st edition, Aquaris
publication,2012.
8. Sareera rachana –anatomy of Ayurveda,Dr. M Rama sundararao,1 st
edition,2003.
9. A textbook of ayurvedic human anatomy, Dr. Giridharkanthi,1st
edition,Choukhamba orientalia,2008.
10. Susrutha Samhita. Ayurved Tatva Sandeepika hindi commentary Author:
Kaviraj Ambikadatta Shastri published by Chowkhambha Sanskrit Sansthan
Varanasi reprint edition Sushruta Samhita Sutrasthana ch. 2010.

108
11. SuśrutaSaṃhitā, with commentary of Dalhan. Edited by Vaidya Yadav ji
Trikram ji, Chaukahambha Orientalia, Varanasi 8th edition, 2005.
12. Sushruta sanhita, shri dalhanacharya virchatiya nibandhsangraga, edited by
acharya priyavat sharma Chaukahambha Orientalia, Varanasi 8th edition, and
2005.
13. Prof. Srikanth murthy K.R. sushrut samhita (sharer 4/4) chaukambha,
Varanasi,U.P. vol-1,2 edition 2004.
14. Sushruta Samhita: Ayurveda Rahasya Deepika Commentary by Dr. B.G.
Ghanekar, 13 edition, 1998, publication Meherehand Laxmandas, New Delhi.
15. Acharya Y.T. Sushruta Samhita with Nibhandha sangraha commentary of
Dalhanacharya. Varanasi (India): Chaukambha Sankrit Sansthan; 2007.
16. Suhruta Samhita:Dalhana Nibandha Sangraha Commentary, published by
krishnadas Academy.
17. Ghanekar S. commentary on Sushruth Samhita Sharirsthana ―Ayurved
Rahasya Deepika by Dr. Bhaskar Govind Ghanekar, published by
Meherchand prakashan Delhi reprinted edition, Sushruta Sharirsthana ch. 2007.
18. Gupta GK (Ed.). Ayurvediya Kriya Sharir Vigyan. Meerut: Utkarsha
Prakashan; 2016.
19. Acharya Y.T. SushrutaSamhita with Nibhandhasangraha commentary of
Dalhanacharya. Varanasi (India): Chaukambha Sankrit Sansthan; 2010.

109
20. Acharya Y.T. Sushruta Samhita with Nibhandha sangraha commentary of
Dalhanacharya. Varanasi (India): Chaukambha Sankrit Sansthan; 2010.
21. Sushutra, Ambika Dutta Shastri, Sushutra Samhita with Elaborated Ayurveda
Tatva Sandipika Hindi Commentary, Reprint 2009. Varanasi: Choukhambha
Sanskrit Sansthan, Volume 1, Sharir Sthan Chapter 4.
22. Clinical Anatomy – Richard S.Snell 7th edition 2003.
23. Principal of anatomy and physiology by Tortora Grabowski 10th edition 2003.
24. A.P.I. Text book of medicine by G.S. Sainani 1999.
25. Gray‘s Anatomy: By Henry Gray edited by Peter Williams and others.
Published by Churchill Livingstone Edinburgh, London, 37 th edition.

CONSENT FORM-
It is not applicable for this study


PROFORMA-
It is not applicable for this study.

MASTER CHART-
It is not applicable for this study.

ANNEXURES/PHOTOS/IMAGES-
Not necessary for this study.