Embed Size (px)
Citation preview

728 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
A Laparoscopic Telesurgical WorkstationMurat CenkCavusoglu, Frank Tendick, Michael Cohn, and S. Shankar Sastry
Abstract—Medical robotics and computer aided surgery in gen-eral, and robotic telesurgery in particular, are promising applica-tions of robotics. In this paper, various aspects of telesurgery arestudied. After a general introduction to laparoscopic surgery andmedical applications of robotics, the UC Berkeley/EndoroboticsInc./UC San Francisco Telesurgical Workstation, a master-slavetelerobotic system for laparoscopic surgery, is introduced, fol-lowed by its kinematic analysis, control, and experimental results.Later some conceptual and future issues on telesurgery arediscussed, including teleoperation and hybrid control, focusingon the special requirements of telesurgery.
Index Terms—Laparoscopy, medical robotics, minimally inva-sive surgery, telesurgery.
I. INTRODUCTION
M EDICAL robotics and computer assisted surgery arenew and promising fields of study that aim to augment
the capabilities of surgeons by taking the best from robots andhumans.
In this joint project between the Robotics and IntelligentMachines Laboratory, University of California, Berkeley, En-dorobotics Inc., and the Department of Surgery, Universityof California, San Francisco, a telesurgical workstation isbeing developed for use in laparoscopic surgery [1]. Thecurrent design is a six degree-of-freedom (DOF) manipulator,instrumented with a gripper, controlled by a six DOF mastermanipulator.
Research on medical robotics at UC Berkeley includesthe development of an endoscopic manipulator [2], [3], earlydesigns of millirobotic manipulators for laparoscopy [4], andstudies on tactile sensing [5]–[7].
A. What is Laparoscopic Surgery?
Laparoscopic surgery is a revolutionary technique [8]. Itis minimally invasive, i.e., the surgery is performed withinstruments inserted through small incisions (less than 10 mmin diameter) rather than by making a large incision to exposethe operation site. The main advantage of this technique isthe reduced trauma to healthy tissue, which is the leading
Manuscript received November 25, 1997; revised March 31, 1997. This pa-per was recommended for publication by Editor R. H. Taylor upon evaluationof the reviewers’ comments. This work was supported in part by NASA underGrant STTR-NAS-1-20288, NSF under Grant IRI-95-31837, and ONR underMURI Grant N14-196001001200.
M. C. Cavusoglu and S. S. Sastry are with the Department of ElectricalEngineering and Computer Sciences, University of California, Berkeley, CA94720 USA.
F. Tendick is with the Department of Surgery, University of California,San Francisco, CA 94143-0475 USA. He is also with the Department ofBioengineering, University of California, Berkeley, CA 94720 USA.
M. Cohn is with Endorobotics, Inc., Berkeley, CA 94709 USA.Publisher Item Identifier S 1042-296X(99)05400-2.
cause of post-operative pain and long hospital stay of thepatient. The hospital stay and rest periods, and therefore theprocedure’s cost, are significantly reduced with minimallyinvasive surgery, at the expense of more difficult techniquesperformed by the surgeon.
Minimally invasive operations include laparoscopy (abdom-inal cavity), thoracoscopy (chest cavity), arthroscopy (joints),pelviscopy (pelvis), and angioscopy (blood vessels). The firstmajor laparoscopic surgery, for colecystectomy (removal ofgall bladder), was performed in 1985 by M¨uhe in (West)Germany. In less than a decade, there was a quick shiftfrom open surgery to laparoscopic surgery in relatively simpleprocedures, with 67% of cholecystectomies performed laparo-scopically in the U.S. in 1993 [9]. Adoption of laparoscopictechniques has been slower in more complex procedures,largely because of the greater difficulty due to the surgeon’sreduced dexterity and perception.
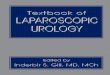
In laparoscopic surgery, the abdominal cavity, which isexpanded by pumping carbon dioxide inside to open aworkspace, is observed with a laparoscope inserted throughone of the incisions. The laparoscope itself is composed ofa chain of lens optics to transmit the image of the operationsite to the CCD camera connected to its outer end, and opticalfibers to carry light to illuminate inside. A monoscopic imageof the operation site is displayed on a high resolution CRTscreen. The instruments used for the operation are speciallydesigned long and thin instruments with trigger-like handles.They are inserted through trocars placed at the incisions toair seal the abdomen. The instruments have only four DOF(see Fig. 1), preventing the ability to arbitrarily orient theinstrument tip [10]. Dexterity is significantly reduced becauseof the lost DOF’s and motion reversal due to the fulcrum at theentry point. Force feedback is reduced due to the friction at theair tight trocar and the stiffness of the inflated abdominal wall.There is no tactile sensing, on which surgeons highly dependin open surgery to locate arteries and tumors hidden in tissue.
Minimally invasive surgery itself is telemanipulation as thesurgeon is physically separated from the workspace. Therefore,telerobotics is a natural tool to extend capabilities in laparo-scopic surgery. With the telesurgical workstation, the goal isto restore the manipulation and sensation capabilities of thesurgeon which were lost due to minimally invasive surgery.The six DOF slave manipulator, controlled through a spatiallyconsistent and intuitive master, will restore the dexterity, theforce feedback to the master will increase the fidelity of themanipulation, and the tactile feedback will restore the losttactile sensation.
Other work in the literature on telesurgical systems forabdominal surgery include the telesurgical system for open
1042–296X/99$10.00 1999 IEEE

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 729
Fig. 1. Four-DOF available in conventional laparoscopic instruments.
surgery with four DOF manipulators developed at SRI Inter-national [11] (a laparoscopic version has also been developed),the telerobotic assistant for laparoscopic surgery developed byTaylor et al. [12], and the telesurgery experiments performedbetween JPL, Pasadena, CA, and Polytechnic University ofMilan, Italy [13], and between Nagoya and Tokyo in Japan[14].
There are other successful medical applications of robotics,including systems for orthopedic surgery [15], microsurgeryand stereotactic neurosurgery [16], eye surgery [17], andradiotherapy [18]. See [19] and [20] for good reviews.
This paper will first introduce the UC Berke-ley/Endorobotics/UCSF Telesurgical Workstation, performits kinematic analysis, give information about control issues,describe the implemented control algorithm, and presentexperimental results. Finally, a short discussion on conceptualand future issues on telesurgery will be presented includingteleoperation and hybrid control issues.
II. DESCRIPTION OF THESYSTEM
A. Design Requirements
The goal of the design is to add a two DOF wrist to extendthe four DOF available through the fulcrum, and therefore giveenough dexterity to perform complex skills, especially suturingand knot tying, in the minimally invasive setting. The slavemust be small enough to fit through incisions typically 10 mmwide, but also able to apply forces large enough to manipulatetissue and suture. It must have sufficient workspace to spansignificant regions in the abdominal cavity and suture at almostarbitrary orientations, yet have a wrist short enough in length towork in constrained spaces. System bandwidth should permitnatural motions by the surgeon and haptic feedback withsufficient fidelity. Of course, the system must be safe to beused inside a patient.
Performance goals in the design of the millirobot are givenin Table I.1 These values are estimated for a suturing task,force and movement requirements for driving a needle throughtissue and tying a knot. The diameter of the instrument ischosen to fit the standard 10 and 15 mm diameter trocars. Itis preferable not to have larger diameters as it causes greater
1Courtesy of Endorobotics Inc.
TABLE IPERFORMANCE GOALS FOR THE MILLIROBOT
damage to healthy tissue. It is not necessary to go smaller than10 mm for laparoscopic surgery as there are other instruments,for example staplers, that require a 10 mm trocar. The wrist-to-gripper length is determined by the clearance betweenthe abdominal wall and the key organs when the abdomenis pressurized. Torque and force requirements are estimatedfrom measurements on instruments performing suturing in anopen surgical setting. A 270of roll rotation is required fordriving the needle through tissue in a single movement withoutregrabbing it. 90 of wrist flexion with 360 of gross rotationis necessary for suturing at the desired orientations. Thebandwidth requirement is set to accommodate the bandwidthof intentional hand movements.
B. Current Prototype
To meet the design requirements, the slave manipulator iscomposed of two parts (Fig. 2). The first part is the grosspositioning stage located outside the body. It is responsiblefor positioning the millirobot, which is the second part of theslave robot. The gross stage controls the same four DOF asthose available in conventional laparoscopic instruments. Asthe gross stage is located outside the body, there is not atight space limitation. A parallel arrangement is chosen forincreased rigidity and a small footprint. Three linear joints,which are connected to the base of the robot with gimbalarrangements, hold a small platform that carries the tool armand the motor rotating it. Two of the linear joints are connectedto the platform with three DOF ball joints whereas the thirdone is connected with a two DOF joint. All four actuators ofthe gross positioning stage are DC servo motors. In the linearjoints, power is transmitted by lead screws connected to themotors. The roll axis through the entry port is direct drive.
The second part of the slave, the millirobot, is located insidethe patient and consequently must be small yet capable ofproducing a wide range of motion and relatively large forces.To meet these requirements, it has a two DOF wrist, with yawand roll axis rotations, and a gripper (Fig. 3). It is 10 mm indiameter. The wrist-to-gripper length is 10 cm. The yaw axis

730 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
(a)
(b)
Fig. 2. Slave manipulator of the Berkeley/Endorobotics/UCSF laparoscopicworkstation.
is actuated by tendons driven by a DC servo motor locatedoutside the body. The roll axis and the gripper are actuated
Fig. 3. Millirobotic wrist.
TABLE IIMILLIROBOT TEST RESULTS
hydraulically through pairs of bladders which are inflated withwater. The water section is separated from the rest of thehydraulic circuit, outside the body, via a set of diaphragms.The millirobot is designed to be disposable, and the bladderswill be driven by sterile saline solution to avoid problems incase of leaks.
Table II gives the experimentally determined open loopperformance results of the actual slave manipulator. All thedesign goals are exceeded except for the range of roll rotationas a result of actuator design limitations.
The master manipulator (See Fig. 4) is a six DOF serialrobot. A commercial four DOF force reflecting joystick (Im-mersion Impulse Engine 3000) with three actuated axes isequipped with an additional two DOF (one actuated) anda stylus handle. The additional two DOF was necessary tocontrol the six DOF slave manipulator. There are positionmeasurements in all six joints and the four actuated joints giveforce feedback in translational directions and the roll axis. Thetorque feedback on the roll axis is especially important to feelwhen the needle enters and leaves the tissue while suturing.The stylus handle was chosen to give a more dextrous interfacefor precise manipulation.
The major safety feature present in this prototype of the sys-tem is the heartbeat check by the robot. The robot continuouslymonitors a heartbeat signal sent by the control program, andcuts the power to all of the actuators in case this signal is lost,which means a computer failure. Additional safety features tobe implemented in the second version of the robot will bediscussed later in this paper.

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 731
Fig. 4. Master manipulator of the laparoscopic workstation.
III. K INEMATICS
For feedforward control of the system, the inverse kinemat-ics of the slave manipulator and the forward kinematics ofthe master manipulator are needed. The forward kinematicsof the slave are also necessary for position error-based forcefeedback.
The hybrid parallel-serial structure of the slave manipulatoris an unusual design which complicates the solution of theinverse kinematics. We will present the calculation of theforward kinematics of the slave manipulator to show theworkspace of the robot. The details of the calculations areincluded as the techniques used are neither standard norobvious. The master manipulator is a straightforward designand therefore briefly described for completeness.
For the kinematic analysis, the product of exponentialsformulation is used. Refer to [21] for a full treatment.
A. Slave Manipulator Inverse Kinematics
In inverse kinematics, the problem is to solve for the jointangles2 of actuated joints, given (3), the desiredconfiguration of the tool relative to the fulcrum.
2For brevity, we use the termanglesto specify the values of generalizedjoint variables, which can be angles or lengths.
Fig. 5. Parallel and serial parts of the slave robot.
Notation: The joint variables of the actuated joints are:lengths of linear joints, , , , roll and yaw rotations ofthe millirobot, and , and gross stage rotation.
To simplify the inverse kinematics calculations, the slavekinematics can be divided into two parts: the serial portioninside the body and parallel portion outside the body. Theserial part is composed of the fulcrum, which is modeled with aspherical joint and a translational joint, and the two DOF wrist.The parallel part of the slave consists of the three arms holdingthe base of the tool arm, and the tool arm itself (Fig. 5).
In the inverse kinematics calculations, first the serial partwill be solved, which will give the angles of the wrist jointsand the desired configuration of the parallel part. Then theparallel part will be solved to calculate the lengths of the linearjoints and the tool arm rotation.
1) Serial Part: Using the naming convention and the zeroconfiguration shown in Fig. 6, the kinematic configuration ofthe serial part is characterized by the following twists3
(1)
and the reference configuration
(2)
which gives the forward kinematics map as
(3)
The inverse kinematics of the serial part is straightforwardas it is a kinematically simple configuration.
Lemma 1—Inverse Kinematics of the Serial Part:Given thedesired configuration
(4)
(5)
atan (6)
atan (7)
where
(8)
3ei denotes theith standard basis vector forR6.

732 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
Fig. 6. Naming convention and the zero configuration of the serial part.
Here, note that has two solutions, and can have anyvalue when , which is a singular configuration.
Then
(9)
will be used in the solution of the parallel part, since, ,and form the fictitious ball joint at the entry point.
2) Parallel Part: The parallel part of the slave consists ofthree arms connected to a triangular platform which holds themillirobot. Two of the arms have six DOF, whereas the thirdone has only five. In each of the arms, only one DOF, thetranslational joint, is actuated. The solution of the inversekinematics for the parallel part requires finding the lengthsof these translational joints and calculating the rotation of thetool arm. In the solution, one proceeds to solve the inversekinematics of the five DOF arm, then uses this to calculatethe lengths of the prismatic joints in the other two arms, andthe amount of rotation.
Specification of the Configuration:Fig. 7 gives a side viewof the parallel part, showing the joint naming conventions andvarious points and coordinate frames used in the calculations.In the figure, joints 1–5 are on the five DOF arm, and joint 6is the rotation of the tool arm. The serial part of the inversekinematics gives the direction, which is determined from thespherical joint at the fulcrum, as
(10)
and the length :
(11)
As notation, the subscripts of points and vectors denote the co-ordinate frames in which they are expressed. The subscripts ofthe homogeneous transforms denote which coordinate framesthey transform. Also, is used to denote inner product.
The forward kinematics of the 5 DOF arm, choosing thezero configuration as overlapped with , are
(12)
where
(13)
The homogeneous transform between theand coordinateframes ( ), coordinates of the spherical wrists and
, and coordinates of the centers of the other two motorsand are all known as they are constant.
The point at which extension of the tool arm intersects the(imaginary) plane passing through the wrists on the tool baseis defined as . Note that has coordinates of the form
(14)
and (10) and (11) give
(15)
where is the length of the tool arm.Lemma 2—Inverse Kinematics of the Parallel Part:The
solution of the inverse kinematics of the parallel section aregiven by
(16)
atan (17)
(18)
atan
(19)
atan
(20)
(21)

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 733
Fig. 7. Kinematic diagram of the side view of parallel section\.
atan
(22)
(23)
(24)
(25)
atan (26)
The full derivation can be found in [22]. Inverse kinematicsof the parallel part have a single solution for each solution ofthe serial part.
B. Slave Forward Kinematics
In forward kinematics, the problem is to calculate , theconfiguration of the tool relative to the fulcrum, given, ,
, , , and , angles of the actuated joints. Similar to theinverse kinematics calculations, the problem can be dividedinto two parts, first the solution for the gross stage and secondthe millirobot.
The gross positioning stage of the slave manipulator hasa parallel structure, which complicates the solution of theforward kinematics. Usually it is not possible to find closed
form solutions for parallel manipulators.4 Rather, the problemis reduced to calculating the solution of a system of nonlinearalgebraic equations.
In the solution of the forward kinematics of the grosspositioning stage the kinematics is expressed in terms of thefulcrum coordinate frame . The coordinate transformationbetween and is specified with the twists
(27)
and the zero configuration
(28)
also shown in Fig. 8. These give the forward kinematics map
(29)
The linear joints give the following three constraints in thefour unknowns
(30)
(31)
(32)4The most classical and well-studied example of this type of manipulators is
the Stewart platform, which has no closed form solution available in literature[23].

734 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
Fig. 8. Naming convention and the zero configuration for the forward kinematics of gross stage.
where point is the center of the coordinate frame. Tosolve the problem, we need to use the constraint imposed bythe five DOF arm, which gives that-axes of the andcoordinate frames are coplanar
(33)
Equations (30)–(33) form a system of four nonlinear equa-tions in four unknowns, which does not have a closed formsolution, but can be solved numerically. For a given, , ,there is a unique solution for .
After the gross stage forward kinematics is solved, (3) giveswith
(34)
(35)
(36)
(37)
(38)
(39)
1) Workspace of the Slave Manipulator:The workspacereachable by the gross stage of the slave manipulator isshown in Fig. 9. The boundary of the reachable workspace isdetermined by six surfaces corresponding to the minimum andmaximum lengths of each of the three linear joints. The grossstage does not have a singularity in the workspace, but, theprecision of the manipulator is reduced at the outer boundaryof the workspace due to the larger moment arm.
C. Master Manipulator Forward Kinematics
The master manipulator is a simple serial structure. Usingthe naming convention and the zero configuration shown inFig. 10, the kinematics of the serial part are characterized bythe following twists:
(40)
and the zero configuration
(41)
which gives the forward kinematics map as
(42)
The calculation of the body Jacobian, which is also straight-forward, is not presented here due to the space limitations, butcan be found in [22].
IV. CONTROL
A. Open Loop Control Issues
The main bottleneck in the dynamics of the slave manip-ulator is the lag in the hydraulic actuators, which is due tothe transmission delay in the tubing, and the first order lagresulting from the RC effect of the tube-bladder configuration.A simple model for transmission delay in the pipes consid-ering the compressibility of water and elasticity of tubes, butneglecting the viscous effects present, gives the propagationvelocity of the pressure wave fronts as [24]
(43)
where is the propagation velocity, is the bulk modulus ofwater, is the density of water, is the diameter of the tube,
is the thickness of the tube, and is the linear modulusof elasticity of the tube material. The tubes connecting themanifolds to the bladders are composed of two sections. Thicksection tubes have 3.5 and are made of Nylon 11, with
0.5 10 psi. Thin section tubes have 2.2 and aremade of PTFE, which has – 10 psi. Calculations

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 735
Fig. 9. Reachable workspace of the slave manipulator gross stage.
using (43) estimate the time delay as 28.6 ms in the thicksection and 1.3–1.6 ms in the thin sections, which is very closeto the experimentally measured values of 32–38 ms determinedfrom the open loop frequency response data.
The parallel structure of the gross stage prevents designinga dynamics-based control algorithm (like a computed torquealgorithm). Backlash in the linear actuators of the gross stageis another important factor to keep in mind for the controllerdesign.
B. Control Algorithm
The overall structure of the proposed control design for thetelesurgical workstation is shown in Fig. 11. In the currentimplementation, which is shown in Fig. 12, joint level anglecontrol is used. Individual joints of the slave manipulatorare servoed with PID controllers to the joint trajectoriesdetermined from the solution of the slave inverse kinematicsand the master forward kinematics along the trajectory of themaster manipulator. The force and tactile loops and safetymonitor are not present. A small dead-band is used on the errorsignal for linear joints to avoid oscillations due to backlash.Anti-windup integral terms (with saturation) are used in thePID controllers. The sensor outputs are compensated for thenonlinear input–output characteristics.
V. EXPERIMENTAL RESULTS AND DISCUSSION
The robot has been successfully tested inex vivosuturingand knot tying tasks in master-slave mode. Experimental
Fig. 10. Naming convention and the zero configuration of the master ma-nipulator.
tracking responses are given in Fig. 13. The RMS error duringtracking for each of the joints are
mm mm mm (44)
Average latency in each of the joints is less than 5 ms, exceptfor the roll axis ( ), which has a latency of 135 ms. As can beseen from these results, the system achieves very good trackingperformance, except for the roll axis which did not perform

736 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
Fig. 11. Proposed control system block diagram.
Fig. 12. Current implementation of master-slave control.
within the specifications and needs to be improved. Bandwidthand time delay for the hydraulic actuators and the noise ofthe analog position sensor are the limiting factors for theperformance of the millirobot. Space restrictions prevented theuse of a digital encoder for the roll axis, so an analog positionsensor was employed instead. However, the limitations ofthe roll axis did not prevent the system from successfullyperforming theex vivo suturing and knot tying tasks, as thesystem was being operated in master-slave mode, and theoperator in the loop was easily able to compensate for theinaccuracies in the roll motion.
During the ex vivo experiments, suturing with a straightneedle was easier compared to the curved needle due tothe limited roll movement available. Although the parallelstructure of the gross stage prevents the use of dynamics-basedcontrollers, the powerful actuators used compensate for this,as can be observed from the tracking responses for the linearjoints ( , , and ).
The specifications adopted for the second version of thesystem are given in Table III.5 In addition to increasing theforce and torque requirements to more easily accommodatemanipulation ofin vivo tissue, the main design changes are onthe roll rotation and the wrist to gripper length. 270of roll
5Courtesy of Endorobotics Inc.
rotation requirement needs to be satisfied for faster and moreeffective suturing. The wrist joint to gripper length is reducedto 5 cm to increase the maneuverability of the manipulatorinside the abdomen.
The more comprehensive safety features not implemented inthis prototype controller will be included in the later designs.The independent high level controller, which should run ona separate computer and have an independent set of sensors,is necessary for safety monitoring. The mission of this safetycontroller is to monitor the overall system, override commandsthat violate the safety constraints, and to shut down the systemin case of failure. A possible low level control algorithm toavoid high interaction forces between the manipulator and theenvironment is discussed in Section VI-B. Increased safetymust also be included in the hardware design to compensatefor the potential problems in the actuator and sensor systems.
VI. CONCEPTUAL AND FUTURE ISSUES INTELESURGERY
A. Teleoperation for Telesurgery
The main concerns for the design and control of a telesur-gical system can be summarized as follows:
1) fidelity in force-torque feedback;2) stability-fidelity trade-off;

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 737
Fig. 13. Master-slave tracking response: dashed lines show the desired trajectory commanded by the master and the solid lines show the actualtrajectory of the slave.
TABLE IIIPERFORMANCE GOALS FOR THE SECOND VERISON OF THEMILLIROBOT
3) performance under time delay
which will affect the choice of control algorithm, hardware forsensing and computation, and the limitations of the technology.
Force feedback is important for telesurgery because of thehigh level of interaction with the environment. Although cur-rently there are no direct experimental results, the performanceincrease as a result of force feedback in conventional teleop-eration tasks [25]–[27] is a clear indication, as interaction intelesurgery is more critical and delicate.
As pointed out by several authors, [28]–[31], fidelity andstability are contradicting factors in teleoperation. Control al-gorithms available in the literature can be classified in terms ofthis trade-off [31]. For example, passive communication basedcontrol algorithms of [32]–[34] are optimized for stability and
have poor fidelity [35], whereas the control algorithms of [36],[37] for ideal kinesthetic coupling are optimized for fidelityand have poor stability.
In conventional teleoperation tasks, involving manipulationof rigid objects for assembly, the interaction with the rigidenvironment is the main source of this stability problem.However, the challenges of telesurgery are quite different fromconventional teleoperation applications. When manipulatingsoft tissue, stability is less of a problem while there is asignificant need for fidelity during telemanipulation. It isespecially important to be able to distinguish changes inenvironment stiffness, as with the interaction between theneedle and the tissue during suturing. For example detectingwhen the needle enters or leaves the tissue, can only be sensedby the change in the resistance that is felt by the instrument.It is also important to be able to locate arteries and lumpshidden under tissue by feeling the changes in the stiffness ofthe tissue.
For increased fidelity, the performance of model basedcontrollers will be needed, at the expense of increased com-putational burden. Especially, model based control (or at leastgravity compensation) on the master side is critical for betterfidelity and to avoid fatigue. Increased force fidelity of a forcesensor on the slave, compared to position error based forcefeedback, might be desirable.
For operation under short time delay, the compliance ofthe robot and the environment would be enough for stableoperation with limited kinesthetic force feedback and a safety

738 IEEE TRANSACTIONS ON ROBOTICS AND AUTOMATION, VOL. 15, NO. 4, AUGUST 1999
controller like that described in Section VI-B. The limitingfactor for telesurgery under time delay will be the fidelity ofteleoperation. Although the control algorithms stabilized viaremote site compliance are reported to perform reasonably wellfor conventional teleoperation tasks, they are not satisfactoryfor surgery because of the lost fidelity as a result of the reducedstiffness of the manipulator. Visual aids like predictive displayswill not be applicable as it is virtually impossible to fullymodel the environment. For larger time delays, supervisorycontrol seems to be the only feasible solution.
It is also important to study the kinesthetic perception of thehuman and to optimize the teleoperation system accordingly.The coupling between the master-slave system can be chosento minimize perceptual distortion rather than seeking an idealresponse which is marginally stable and practically impossibleto achieve. Also some variables of interaction can be amplifiedto improve sensation of manipulation for better performance.Although there are some studies in the literature on humanperception in the context of teleoperation [38], there is a lotof work that should be done.
B. Hybrid Control
One way to increase safety and performance in telesurgerywith time delay is to use a hierarchical controller, where thecommands of the surgeon transmitted with a time delay areoverlaid by a local low level controller at the remote sitewhich guarantees safety. Hybrid control design techniques canbe used to develop this low level controller to limit interactionforces under specified disturbances [39]. Such a controller canbe used in a supervisory control algorithm for teleoperationunder time delay to guarantee safety by eliminating excessiveinteraction forces.
VII. CONCLUSION
This study addressed various aspects of telesurgery. We firstintroduced the telesurgical workstation, a master-slave teler-obotic system designed considering the special requirementsof minimally invasive telesurgery, followed by its kinematicanalysis, control, and experimental evaluation. Later, someconceptual and future issues in telesurgery were discussed,including discussions on teleoperation and hybrid control.
Directions for Future Work:The future work will proceedin two areas. For the Telesurgical Workstation, the proposedcontrol algorithm will be implemented, with the force feedbackand safety monitor, followed by experimental studies to furtheranalyze the effectiveness of the robot and the control. A secondrobot is necessary for bimanual operation. A second version ofthe system is currently being developed, with modifications toimprove performance based on the evaluation of the currentsystem. This second system is being tested in animal trialsat the experimental surgery laboratory at the University ofCalifornia San Francisco. These results will be presented ina coming paper.
On the conceptual side, human kinesthetic perception willbe experimentally studied to further identify the design goalsfor an effective teleoperation system design. Along this line,we are currently studying the ability of the human operator to
detect the changes in the compliance of a surface. Also, furtherexperimental and theoretical studies are being conducted tocompare alternate robot and control designs under nonidealconditions, like presence of time delay or uncertainties in themanipulator models.
REFERENCES
[1] S. S. Sastry, M. Cohn, and F. Tendick, “Milli-robotics for remote,minimally invasive surgery,”J. Robot. Auton. Syst.,vol. 21, no. 3, pp.305–316, Sept. 1997.
[2] J. Wendlandt and S. S. Sastry, “Design and control of a simplifiedStewart platform for endoscopy,” inProc. IEEE Conf. Decision Contr.,1994, vol. 1, pp. 357–362.
[3] J. Wendlandt, “Milli robotics for endoscopy,” Memo M94/7, Univ.California, Berkeley, Jan. 1994.
[4] M. Cohn, L. S. Crawford, J. M. Wendlandt, and S. S. Sastry, “Surgicalapplications of milli-robots,”J. Robot. Syst.,vol. 12, no. 6, pp. 401–416,June 1995.
[5] M. B. Cohn, M. Lam, and R. S. Fearing, “Tactile feedback for teleop-eration,” in Proc. SPIE,1993, vol. 1833, pp. 240–254.
[6] B. L. Gray and R. S. Fearing, “A surface micromachined microtactilesensor array,” inProc. IEEE Int. Conf. Robot. Automat.,1996, vol. 1,pp. 1–6.
[7] R. S. Fearing, G. Moy, and E. Tan, “Some basic issues in teletaction,”in Proc. IEEE Int. Conf. Robot. Automat.,1997, vol. 4, pp. 3093–3099.
[8] L. W. Way, S. Bhoyrul, and T. Mori, Eds.,Fundamentals of Laparo-scopic Surgery. London, U.K.: Churchill Livingstone, 1995.
[9] E. Graves,Vital and Health Statistics,Nat. Health Survey 122, U.S.Dept. Health and Human Services, Hyattsville, MD, 1993.
[10] F. Tendick, R. W. Jennings, G. Tharp, and L. Stark, “Sensing andmanipulation problems in endoscopic surgery: Experiment, analysis andobservation,”Presence,vol. 2, no. 1, pp. 66–81, 1993.
[11] J. W. Hill, P. S. Green, J. F. Jensen, Y. Gorfu, and A. S. Shah,“Telepresence surgery demonstration system,” inProc. IEEE Int. Conf.Robot. Automat.,1994, pp. 2302–2307.
[12] R. H. Taylor, J. Funda, B. Eldridge, S. Gomory, K. Gruben, D. LaRose,M. Talamini, L. Kavoussi, and J. Anderson, “A telerobotics assistant forlaparoscopic surgery,”IEEE Eng. Med. Biol. Mag.,vol. 14, no. 3, pp.279–288, May/June 1995.
[13] A. Rovetta, R. Sala, X. Wen, and A. Togno, “Remote control intelerobotic surgery,”IEEE Trans. Syst., Man, Cybern. A,vol. 26, pp.438–443, July 1996.
[14] F. Arai, M. Tanimoto, T. Fukuda, K. Shimojima, H. Matsuura, and M.Negoro, “Multimedia tele-surgery using high speed optical fiber networkand its applications to intravascular neurosurgery—System configurationand computer networked implementation,” inProc. IEEE Int. Conf.Robot. Automat.,1996, vol. 1, pp. 878–883.
[15] R. H. Taylor, B. D. Mittelstadt, H. A. Paul, W. Hanson, P. Kazanzides,etal., “An image-directed robotics system for precise orthopaedic surgery,”IEEE Trans. Robot. Automat.,vol. 10, pp. 261–275, June 1994.
[16] S. Lavallee, J. Troccaz, L. Gaborit, P. Cinquin, A. L. Benabid, andD. Hoffmann, “Image guided operating robot: A clinical application instereotactic neurosurgery,” inComputer Integrated Surgery: Technologyand Clinical Applications,R. H. Taylor, S. Lavall´ee, G. Burdea, and R.Mosges, Eds. Cambridge, MA: MIT Press, 1995.
[17] P. S. Schenker, H. Das, and T. R. Ohm, “A new robot for high dexteritymicrosurgery,” in Computer Vision, Virtual Reality and Robotics inMedicine. First International Conference, CVRMed’95 Proceedings.,N.Ayache, Ed. Berlin, Germany: Springer-Verlag, 1995, pp. 115–122.
[18] R. Tombropoulos, A. Schweikard, J. C. Latombe, and J. R. Adler, “Treat-ment planning for image-guided robotic radiosurgery,” inComputerVision, Virtual Reality and Robotics in Medicine. First International Con-ference, CVRMed ’95 Proceedings,N. Ayache, Ed. Berlin, Germany:Springer-Verlag, 1995, pp. 131–137.
[19] P. Dario, E. Guglielmelli, B. Allotta, and M. C. Carrozza, “Robotics formedical applications,”IEEE Robot. Automat. Mag.,vol. 3, no. 3, pp.44–56, 1996.
[20] R. H. Taylor, S. Lavallee, G. Burdea, and R. Mosges, Eds.,Computer-Integrated Surgery: Technology and Clinical Applications.Cambridge,MA: MIT Press, 1996.
[21] R. M. Murray, Z. Li, and S. S. Sastry,A Mathematical Introduction toRobotic Manipulation. Orlando, FL: CRC, 1994.
[22] M. C. Cavusoglu, “Control of a telesurgical workstation,” Tech. Rep.,Memo M97/3, Electron. Res. Lab., Univ. California, Berkeley, May1997.

CAVUSOGLU et al.: A LAPAROSCOPIC TELESURGICAL WORKSTATION 739
[23] K. Liu, J. M. Fitzgerald, and F. L. Lewis, “Kinematic analysis of aStewart platform manipulator,”IEEE Trans. Ind. Electron.,vol. 40, pp.282–293, Apr. 1993.
[24] D. N. Roy,Applied Fluid Mechanics. New York: Ellis Horwood, 1988.[25] H. Das, H. Zak, W. S. Kim, A. K. Bejczy, and P. S. Schenker, “Operator
performace with alternative manual control modes in teleoperation,”Presence,vol. 1, no. 2, pp. 201–218, Spring 1992.
[26] W. S. Kim, B. Hannaford, and A. K. Bejczy, “Force-reflection andshared compliant control in operating telemanipulators with time delay,”IEEE Trans. Robot. Automat.,vol. 8, pp. 176–185, Apr. 1992.
[27] B. Hannaford, L. Wood, D. A. McAffee, and H. Zak, “Performanceevaluation of a six-axis generalized force-reflecting teleoperator,”IEEETrans. Syst., Man, Cybern.,vol. 21, pp. 620–633, May/June 1991.
[28] B. Hannaford, “A design framework for teleoperators with kinestheticfeedback,” IEEE Trans. Robot. Automat.,vol. 5, pp. 426–434, Aug.1989.
[29] , “Stability and performance tradeoffs in bi-lateral telemanipula-tion,” in Proc. IEEE Int. Conf. Robot. Automat.,1989, pp. 1764–1767.
[30] G. J. Raju, G. C. Verghese, and T. B. Sheridan, “Design issues in 2-portnetwork models of bilateral remote manipulation,” inProc. IEEE Int.Conf. Robot. Automat.,1989, pp. 1316–1321.
[31] D. A. Lawrence, “Stability and transperancy in bilateral teleoperation,”IEEE Trans. Robot. Automat.,vol. 9, pp. 624–637, Oct. 1993.
[32] G. Niemeyer and J. J. E. Slotine, “Stable adaptive teleoperation,”IEEEJ. Oceanic Eng.,vol. 16, pp. 152–162, Jan. 1991.
[33] R. J. Anderson and M. W. Spong, “Bilateral control of teleoperatorswith time delay,” IEEE Trans. Automat. Contr.,vol. 34, pp. 494–501,May 1989.
[34] , “Asymptotic stability for force reflecting teleoperators with timedelay,” Int. J. Robot. Res.,vol. 11, pp. 135–148, Apr. 1992.
[35] C. A. Lawn and B. Hannaford, “Performance testing of passive com-munication and control in teleoperation with time delay,” inProc. IEEEInt. Conf. Robot. Automat.,1993, pp. 776–783.
[36] Y. Yokokohji and T. Yoshikawa, “Bilateral control of master-slave ma-nipulators for ideal kinesthetic coupling—Formulation and experiment,”in Proc. IEEE Int. Conf. Robot. Automat.,1992, pp. 849–858.
[37] , “Bilateral control of master-slave manipulators for ideal kines-thetic coupling—Formulation and experiment,”IEEE Trans. Robot.Automat.,vol. 10, pp. 605–620, Oct. 1994.
[38] L. A. Jones and I. W. Hunter, “Analysis of the human opera-tor controlling a teleoperated microsurgical robot,” inProc. 6thIFAC/IFIP/IFORS/IEA Symp. Anal., Design Evaluation Man–MachineSyst.,1995, pp. 593–597.
[39] M. C. Cavusoglu, J. Yan, and S. S. Sastry, “A hybrid system approachto contact stability and force control in robotic manipulators,” inProc.12th IEEE Int. Symp. Intell. Contr. (ISIC’97),July 1997, pp. 143–148.
Murat Cenk Cavusoglu received the B.S. degreefrom Middle East Technical University, Ankara,Turkey, in 1995, the M.S. degree from the Uni-versity of California, Berkeley, in 1997, and iscurrently pursuing the Ph.D. degree at the ElectricalEngineering and Computer Sciences Department,University of California, Berkeley.
His research interests are medical robotics, virtualenvironments for training, and control systems.
Frank Tendick received the B.S. degree in aero-nautics and astronautics from the MassachusettsInstitute of Technology, Cambridge, the M.S. degreein mechanical engineering from the University ofCalifornia, Berkeley, and the Ph.D. in bioengineer-ing from the joint program at the University ofCalifornia, San Francisco, and Berkeley campuses.
He is now an Assistant Professor in the De-partment of Surgery, University of California, SanFrancisco, and the Department of Bioengineering,University of California, Berkeley. His interests
are in human-machine interfaces, teleoperation, and virtual environments,especially as applied to surgery.
Michael Cohn received the Ph.D. degree from theDepartment of Electrical Engineering and ComputerSciences, University of California, Berkeley.
He is currently with Endorobotics, Inc., Berkeley,CA, and also working as a Post-Doctoral Researcherat the Berkeley Sensor and Actuator Center, Univer-sity of California, Berkeley.
S. Shankar Sastryreceived the Ph.D. degree fromthe University of California, Berkeley, in 1981.
He was on the faculty of the Massachusetts Insti-tute of Technology (MIT), Cambridge, from 1980 to1982 and Harvard University, Cambridge, MA, as aGordon McKay Professor in 1994. He is currentlya Professor of Electrical Engineering and ComputerSciences and Director of the Electronics ResearchLaboratory, University of California, Berkeley. Hehas held visiting appointments at the AustralianNational University, Canberra, the University of
Rome, Scuola Normale, and University of Pisa, the CNRS Laboratory LAASin Toulouse, and as a Vinton Hayes Visiting Fellow at the Center for IntelligentControl Systems at MIT. His areas of research are nonlinear and adaptivecontrol, robotic telesurgery, control of hybrid systems, and biological motorcontrol. He is a coauthor ofAdaptive Control: Stability, Convergence andRobustness(Englewood Cliffs, NJ: Prentice-Hall, 1989),A MathematicalIntroduction to Robotic Manipulation(Orlando, FL: CRC, 1994), and theauthor ofNonlinear Control: Analysis, Stability(New York: Springer-Verlag,1999). He coeditedHybrid Control II and Hybrid Control IV, and HybridSystems: Computation and ControlSpringer Lecture Notes in ComputerScience, 1995, 1997, and 1998.
Dr. Sastry received the President of India Gold Medal in 1977, theIBM Faculty Development award for 1983–1985, the NSF PresidentialYoung Investigator Award in 1985, and the Eckman Award of the AmericanAutomatic Control Council in 1990. He was an Associate Editor of theIEEE TRANSACTIONS ONAUTOMATIC CONTROL, IEEE Control Magazine, IEEETRANSACTIONS ON CIRCUITS AND SYSTEMS, and theJournal of MathematicalSystems, Estimation and Controland is an Associate Editor of theIMA Journalof Control and Information, the International Journal of Adaptive Control andSignal Processingand theJournal of Biomimetic Systems and Materials.