Embed Size (px)
Citation preview

A infant withrecurrent bacterial infection and
persistent oral candidiasis
2011-01-26
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Age/Gender: 5-month-old boy
Body Height: 64cm (3rd-10th percentile)
Body Weight: 5 kg(< 3rd percentile)
Admission Date: May 28, 2004
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Birth history: G3P3, full term, BBW 3130 g, no perinatalinsult
At 3m/oAdmission because of UTI with E.coli infection
At 4m/o Admission due to oral candidiasis and poor appetite
At 5 m/orefer to our hospital with E.coli urosepsis,
bronchopneumonia, and persistent oral candidiasis
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Acute ill looking, poor muscle tone
Conscious: clear
Oral thrush over buccal mucosa
Paucity of lymph nodes and tonsils
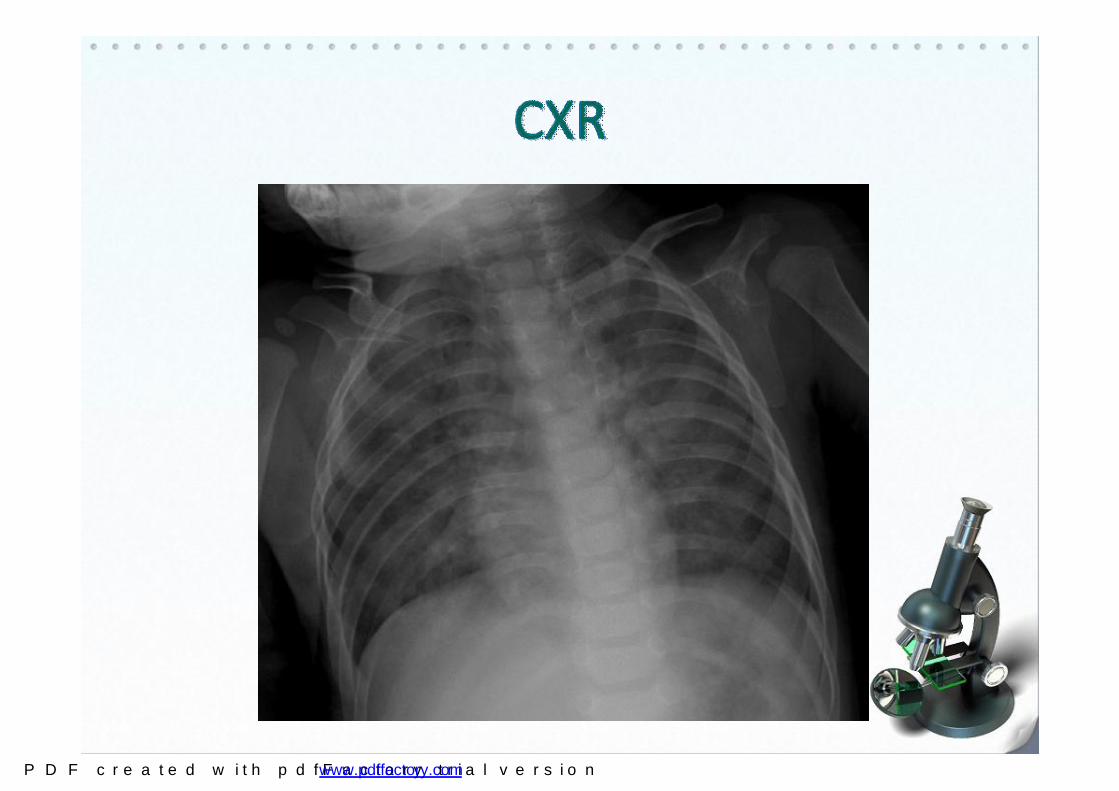
Tachypnea with O2 cannula supportnasal flaring, subcostal retractions, bilateral crackles
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
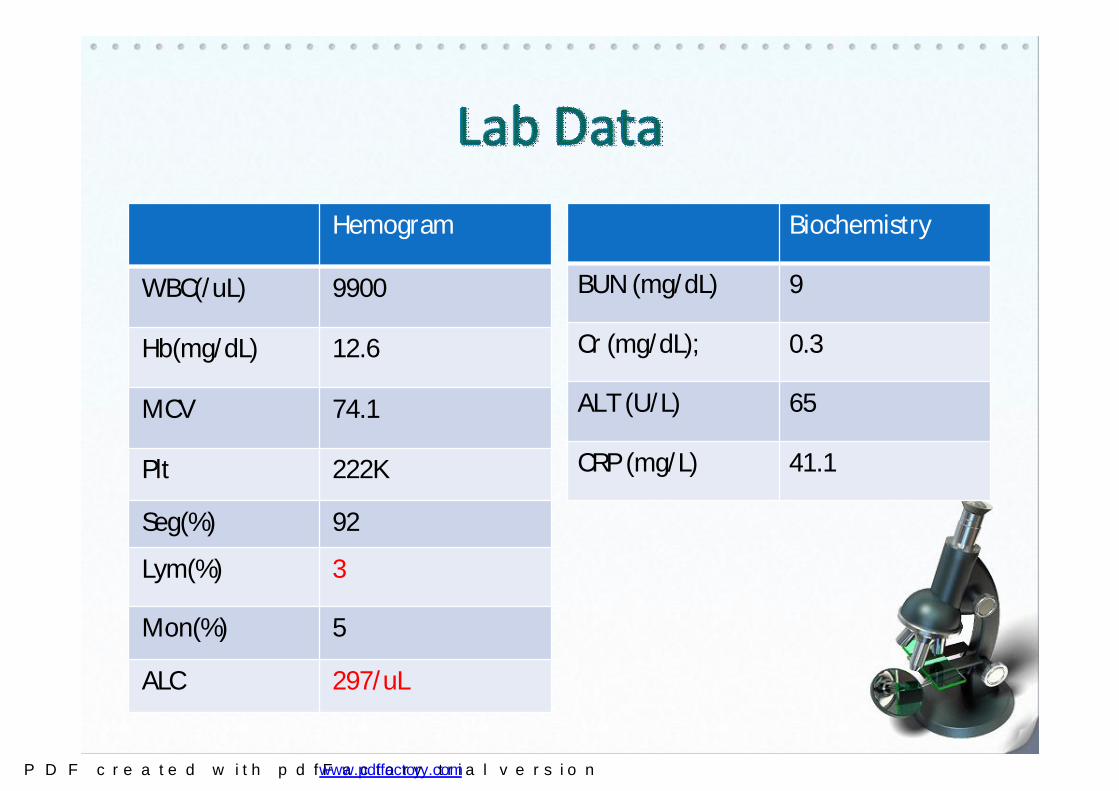
Hemogram
WBC(/uL) 9900
Hb(mg/dL) 12.6
MCV 74.1
Plt 222K
Seg(%) 92
Lym(%) 3
Mon(%) 5
ALC 297/uL
Biochemistry
BUN (mg/dL) 9
Cr (mg/dL); 0.3
ALT (U/L) 65
CRP (mg/L) 41.1
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

What are the impression& further management ?
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
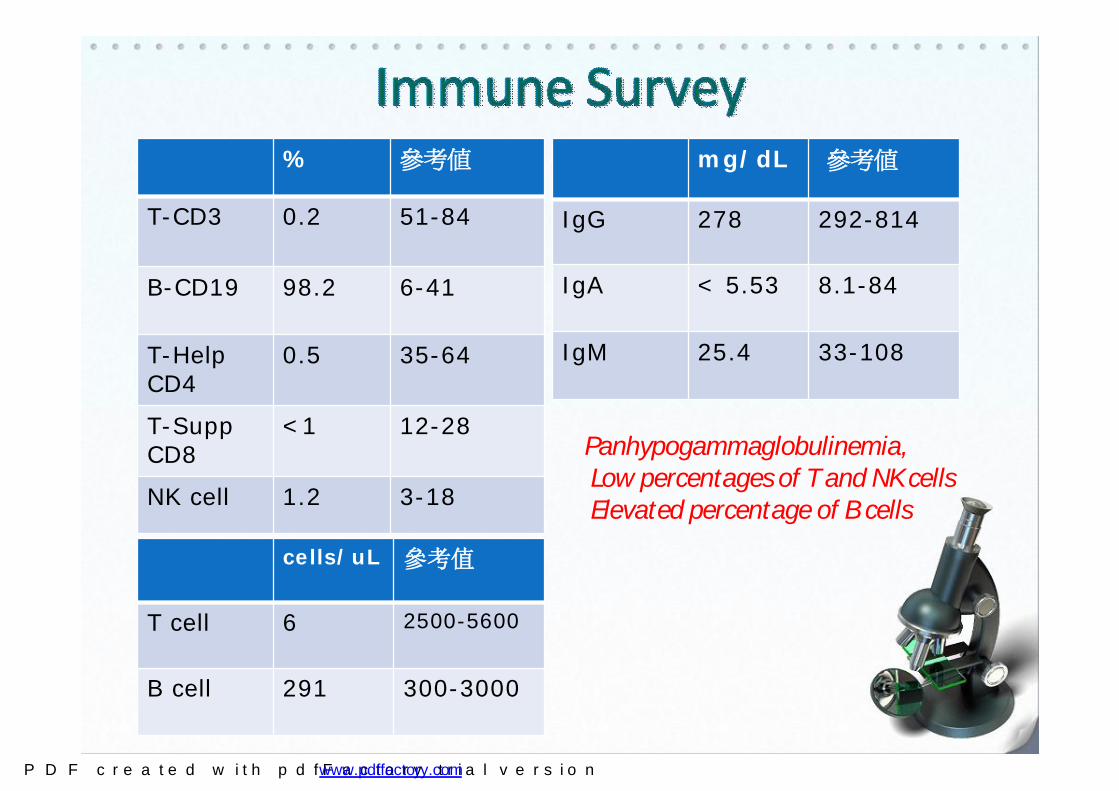
% 參考值
T-CD3 0.2 51-84
B-CD19 98.2 6-41
T-Help CD4
0.5 35-64
T-SuppCD8
<1 12-28
NK cell 1.2 3-18
mg/dL 參考值
IgG 278 292-814
IgA < 5.53 8.1-84
IgM 25.4 33-108
Panhypogammaglobulinemia,Low percentages of T and NK cellsElevated percentage of B cells
cells/uL 參考值
T cell 6 2500-5600
B cell 291 300-3000
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Primary immunodeficiencybased on recurrent infection, persistent candidiasis, failure to thrive, lymphopenia
Excluding secondary immunodeficiencies:Premature and newbornHereditary and metabolic diseasesImmunosuppressive agentsInfectious diseasesInfiltrative and hematologic diseasesSurgery and traumaMiscellaneous
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

PCR identified the presence of P. carinii in BAL fluid→Pneumocystis carinii (jirovecii) pneumonia
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

BCG scar?
Suppurative granulomatous inflammation with mycobacterial infection→Disseminated bacillus Calmette-Guerin disease
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
X
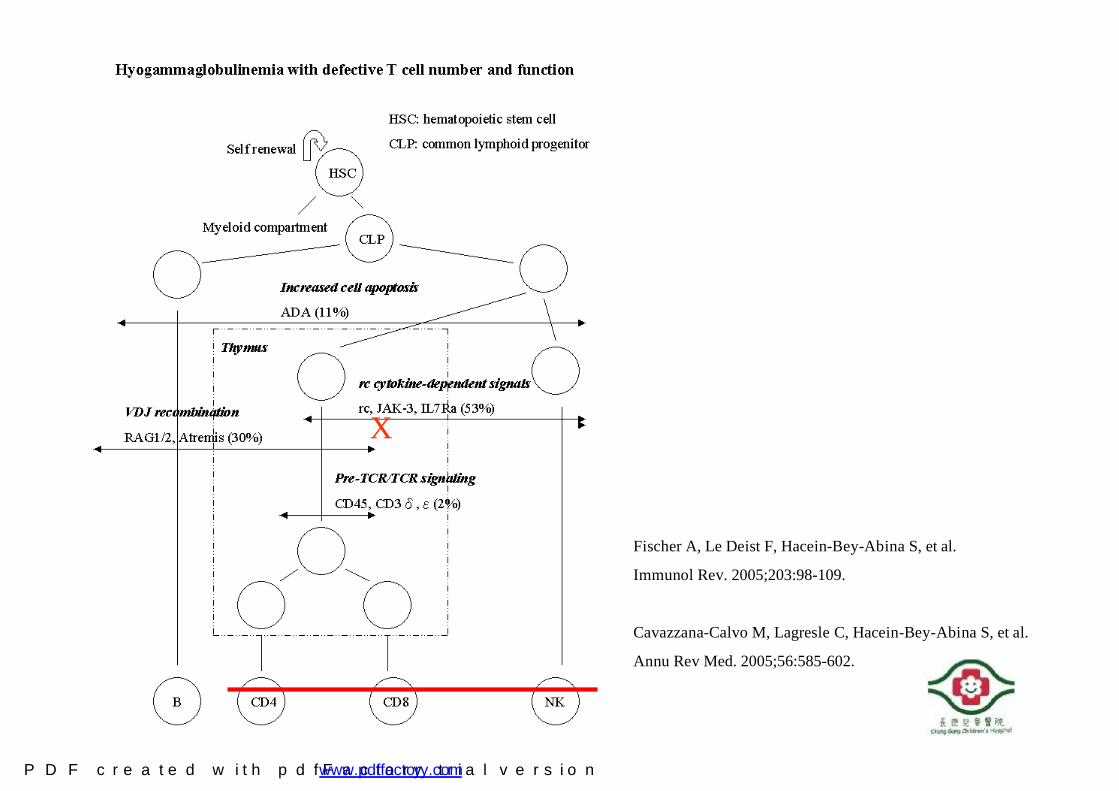
Fischer A, Le Deist F, Hacein-Bey-Abina S, et al.
Immunol Rev. 2005;203:98-109.
Cavazzana-Calvo M, Lagresle C, Hacein-Bey-Abina S, et al.
Annu Rev Med. 2005;56:585-602.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Role of γc receptor complexes for multiple cytokines
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Molecular study: Obviously decreased IL-2R common γ chain expression on rest CD4+ cells
Isotype control IL-2R γchainControl
Patient 18
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
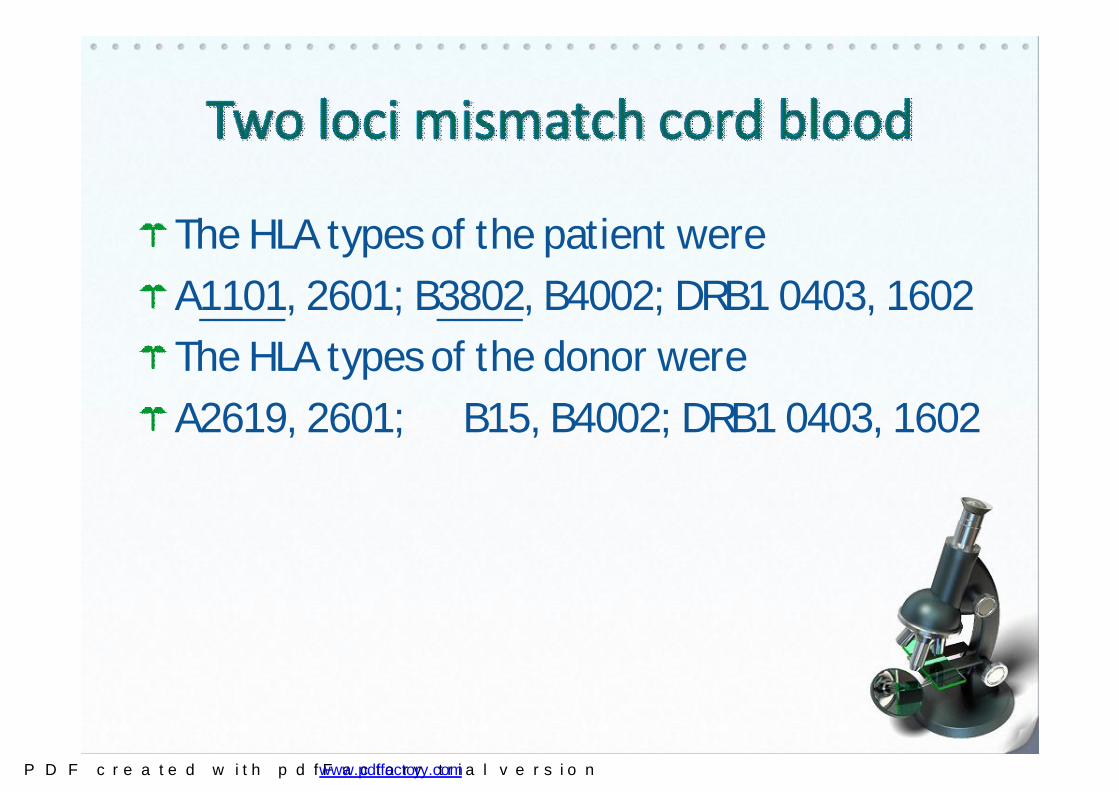
The HLA types of the patient were
A1101, 2601; B3802, B4002; DRB1 0403, 1602
The HLA types of the donor were
A2619, 2601; B15, B4002; DRB1 0403, 1602
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

PCPHepatitis due
to Barktar(primaquine)
Disseminated BCG disease (4 month)
Stop IVIG supply
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
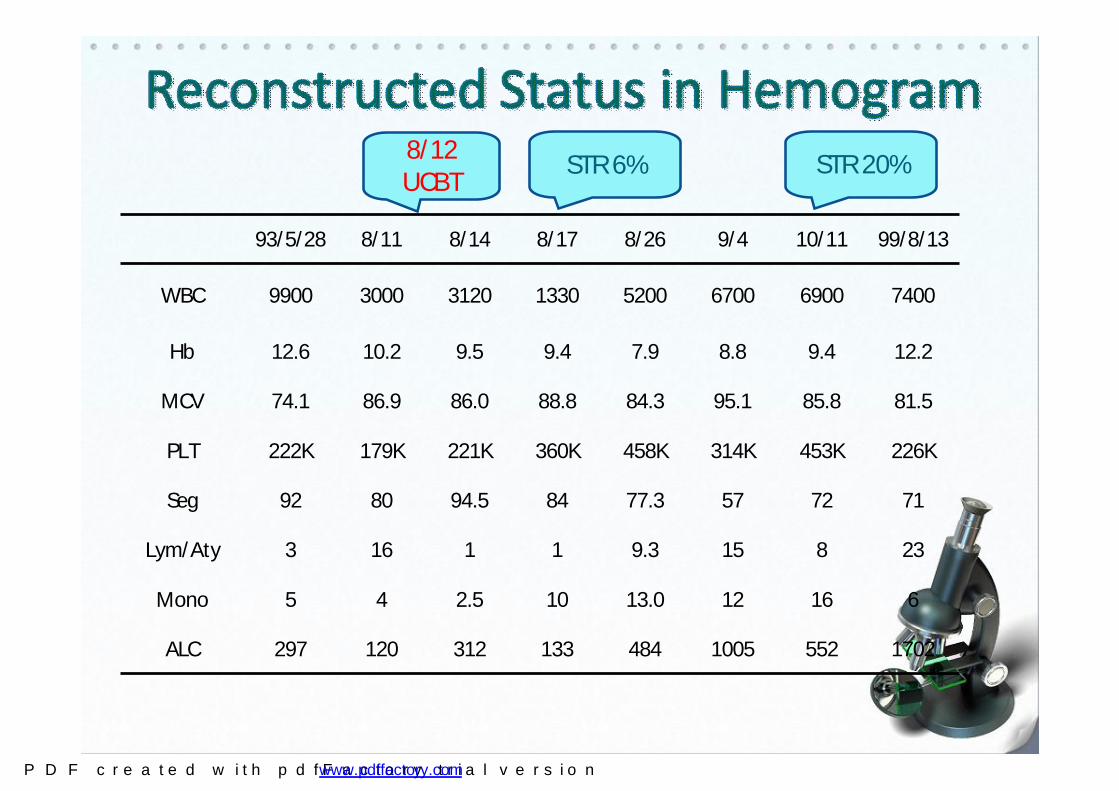
93/5/28 8/11 8/14 8/17 8/26 9/4 10/11 99/8/13
WBC 9900 3000 3120 1330 5200 6700 6900 7400
Hb 12.6 10.2 9.5 9.4 7.9 8.8 9.4 12.2
MCV 74.1 86.9 86.0 88.8 84.3 95.1 85.8 81.5
PLT 222K 179K 221K 360K 458K 314K 453K 226K
Seg 92 80 94.5 84 77.3 57 72 71
Lym/Aty 3 16 1 1 9.3 15 8 23
Mono 5 4 2.5 10 13.0 12 16 6
ALC 297 120 312 133 484 1005 552 1702
STR 6%8/12 UCBT
STR 20%
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Before After (2 Month ) After (6 Month)
T-CD3 0.2 68.8 68.5
B-CD19 98.2 1.0 22.2
T-Help CD4 0.5 52.7 44.6
T-SuppCD8
<142.3 28.5
NK cell 1.2 25 8.6
T cell 6 cells/uL 379 cells/uL 1846 cells/uL
B cell 291 cells/uL 5 cells/uL 602 cells/uL
CD 45 RO 0.5 62 9.4
CD 45 RA 97.9 38 30.8
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Before After2 Month
IgG 278 522
IgA < 5.53 < 6.13
IgM 25.4 94.1
After11 Month
After13 Month
837 966
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

BCG
0
10000
20000
30000
40000
50000
60000
2.50% 5.00% 2.50% 5.00% 2.50% 5.00% 2.50% 5.00%
Pre- Post-2M Post-6M Post-10M
Time (Month)
Del
ta c
pm
Patient Control 3 years later..
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

A 5-month-old boy
Failure to thrive, dyspnea, intermittent cyanosis for 1 month Pneumocystis carinii pneumonia and thymic hypoplasia
T-B+NK- type SCID identified with IL-2RG Arg226Cys mutation
Unrelated cord blood transplantation on 2007/8/8.Engraftment with mixed chimerism post-transplant three weeks. Good clinical condition without any medications
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
曾小弟參加2009年臍帶移植~希望再生六週年慶
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

A 4-month-old girl
Candidiasis over back, neck and genital area for 1 month. Interstitial pneumonia (pneumocystis carinii) T-B-NK+ SCID with RAG2 mutationHesitate to perform stem cell transplantation
Unrelated peripheral blood progenitor cells transplantation on 2009/12/25 while exacerbating respiratory distress
Deceased of sudden pneumomediastinum and subcutaneous emphysema despite of successful engraftment post-transplant 4 months
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Whitish patch or spot
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Discussion---on emphasis of early diagnosis
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

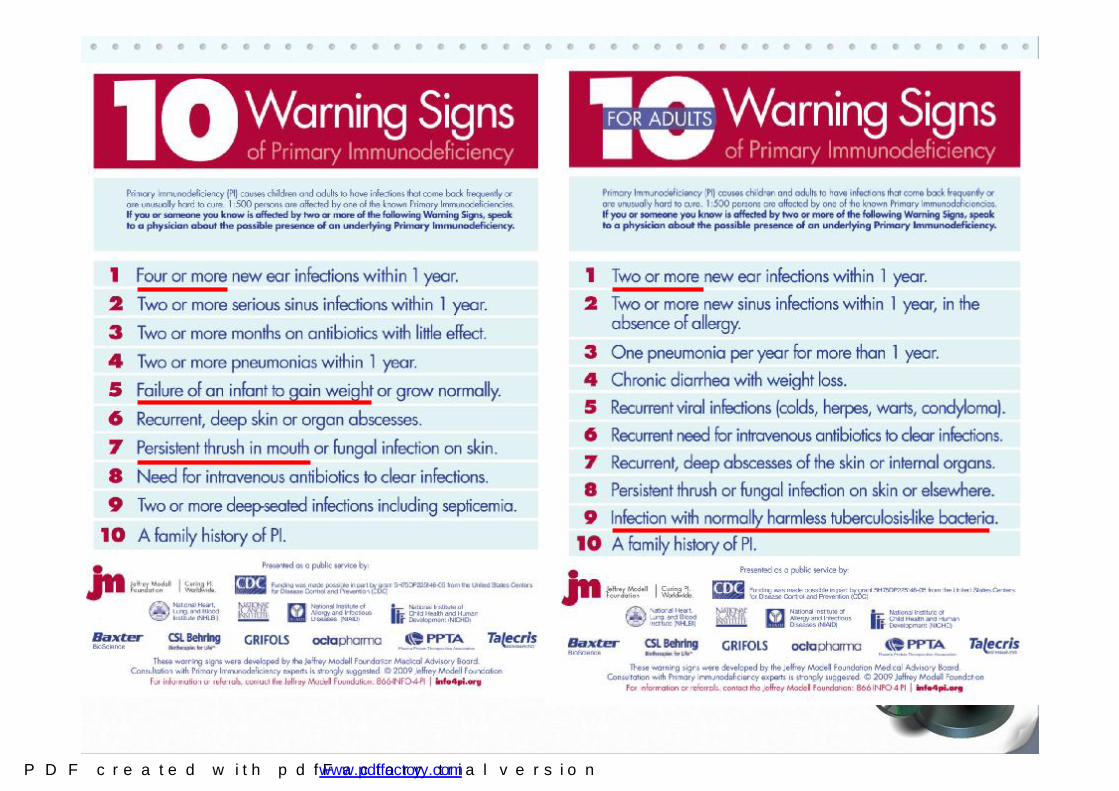
How to recognize PIDs earlier, especially SCID
• High suspicion by clinical features (warning signs)
• Prenatal diagnosis if families with identified genetic defects
• Newborn screening to quantify T-cell receptor excision circle
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Website http://www.cgmh.org.tw/chldhos/intr/c4a80/06index003.htm
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
• Intravenous immunoglobulins (IVIG):
hypogammaglobulinemia and recurrent infections
• Stem cell transplantation (bone marrow or cord blood) :
severe combined immunodeficiencies, severe T cell defects,
severe PMN defects
• Interferon-gamma (IFN-γ):
refractory recurrent mycobacteria or salmonella infections
• Granulocyte-colony stimulating factor (G-CSF):
intermittently neutropenia
• Prophylactic treatment:
T-cell and phagocytic defects to prevent opportunity infections
Basic principle of management:
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
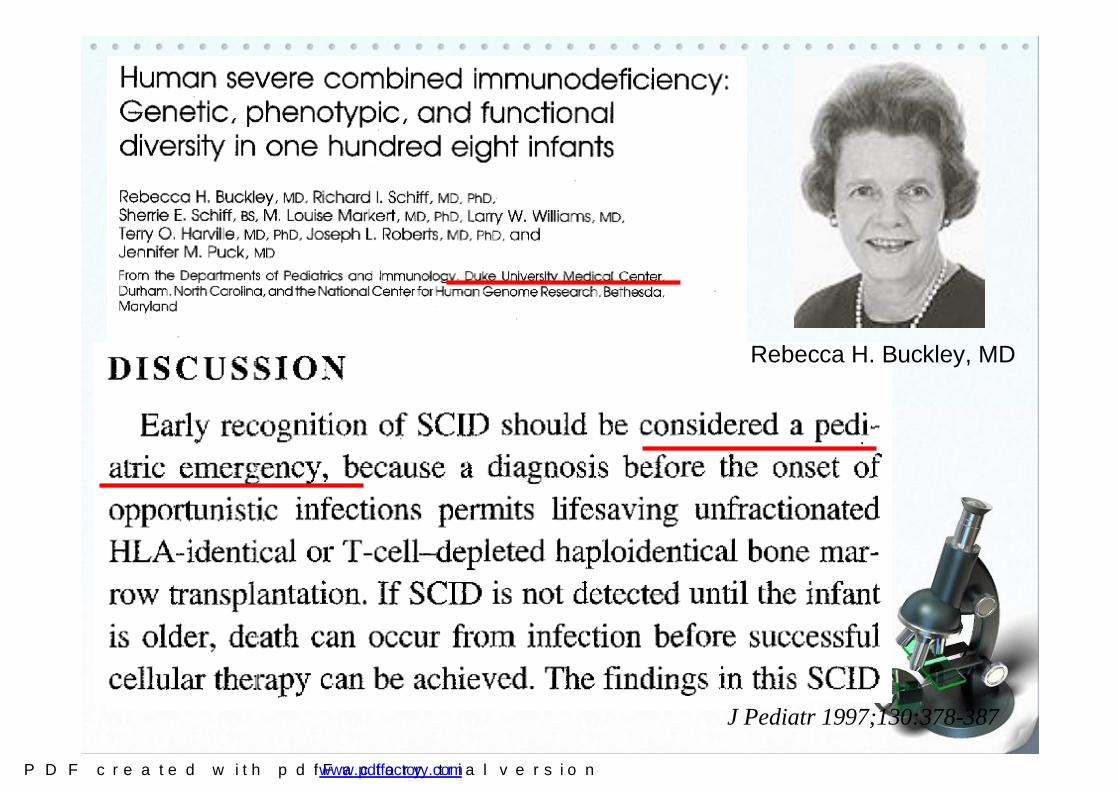
J Pediatr 1997;130:378-387
Rebecca H. Buckley, MD
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

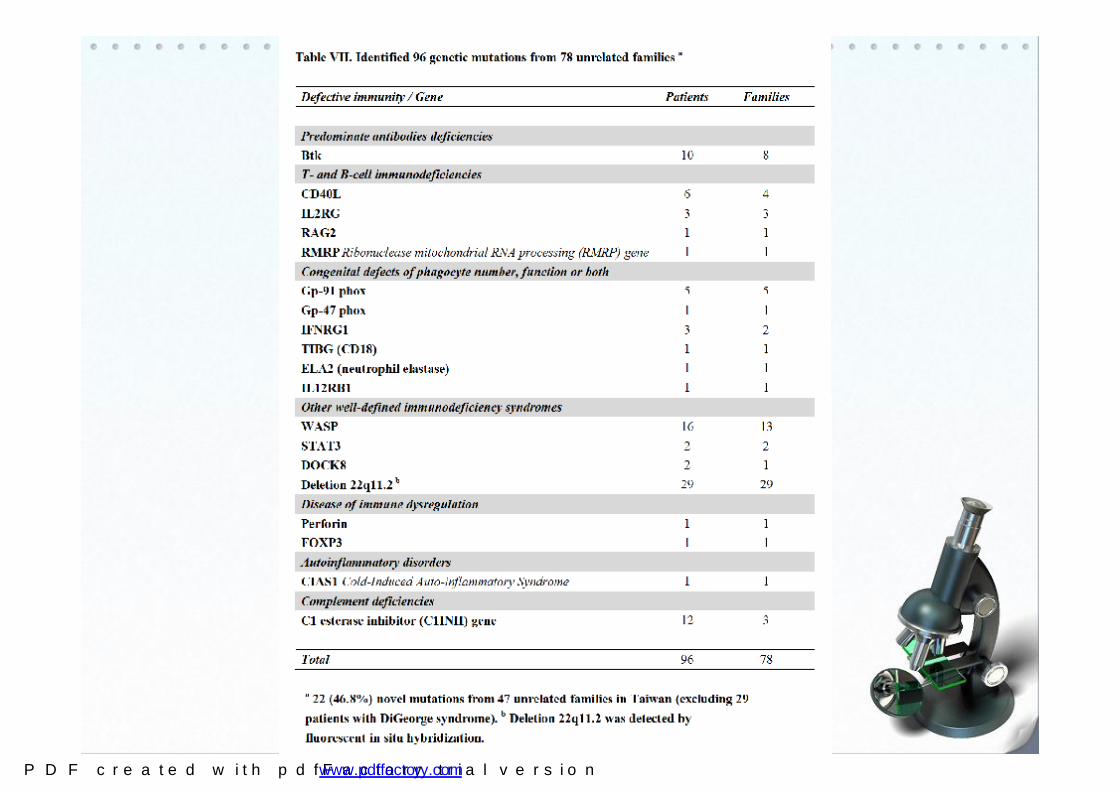
Other well-defined immunodeficiency syndromes 70 (35.5%) Predominate antibodies deficiencies 51 (25.9%)T- and B-cell immunodeficiencies 33 (16.8%)Congenital defects of phagocyte number, function or both 23 (11.7%) Complement deficiencies 15 (7.6%) Disease of immune dysregulation 4 (2.0%) Autoinflammatory disorders 1 (0.5%)Defects in innate immunity: None
Lee WI, Jaing TH, Hsieh MY, et al. J Clin Immunol. 2005; 25:162-73; 2006; 26:274-83 and update
Distribution of Taiwanese PIDs patients
(197 patients during 1985-2010)
Overview
7 mortality in 14 SCID
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

How to recognize PIDs earlier, especially SCID
• High suspicion by clinical features (warning signs)
• Prenatal diagnosis if families with identified genetic defects
• Newborn screening to quantify T-cell receptor excision circle
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
How to recognize PIDs earlier, especially SCID
• High suspicion by clinical features (warning signs)
• Prenatal diagnosis if families with identified genetic defects
• Newborn screening to quantify T-cell receptor excision circle
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

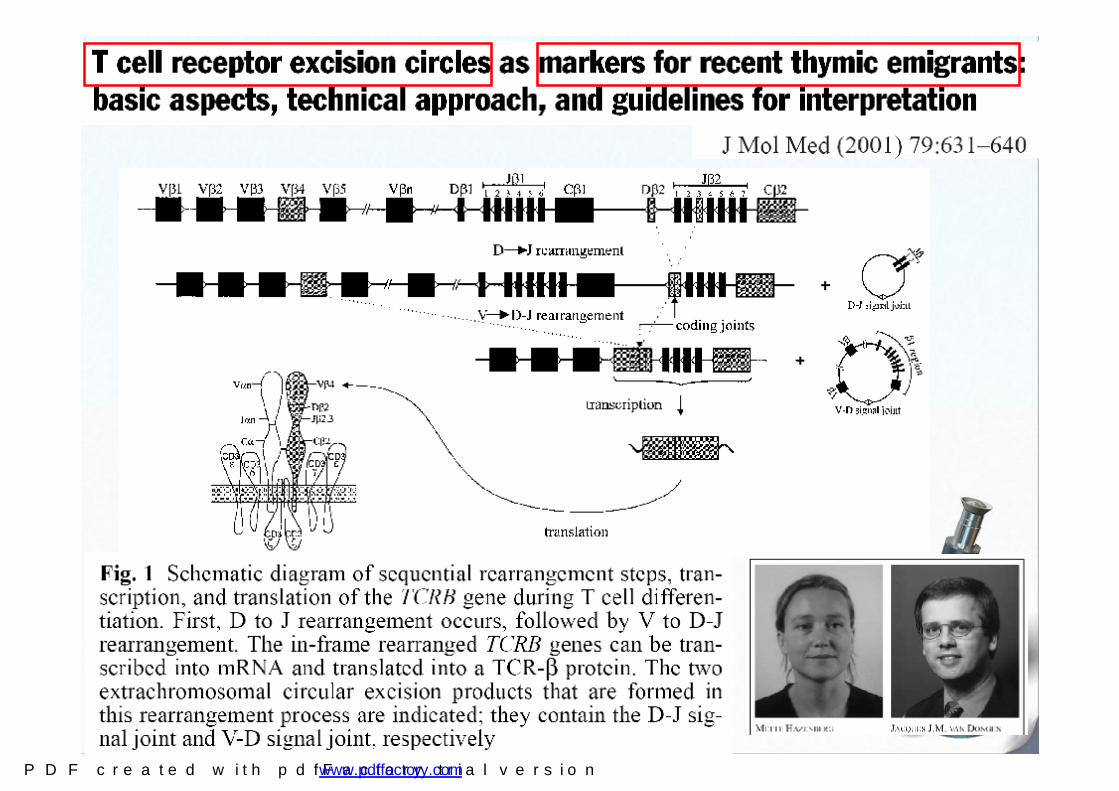
Methods of monitoring T cell reconstitution. Deletion of the TCRD locus from within the TCRA locus is a common requirement for productive rearrangement of the a-chain (A). The resultant signal joint (sj) T-cell rearrangement excision circlet (TREC) can be quantified by realtime polymerase chain reaction (PCR) allowing assessment of thymic output. Because episomal DNA does not replicate but remains stable over time, the TRECs are diluted out by cell divisions as the T cells age (B)
British Journal of Haematology, 2004,124, 407–420
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
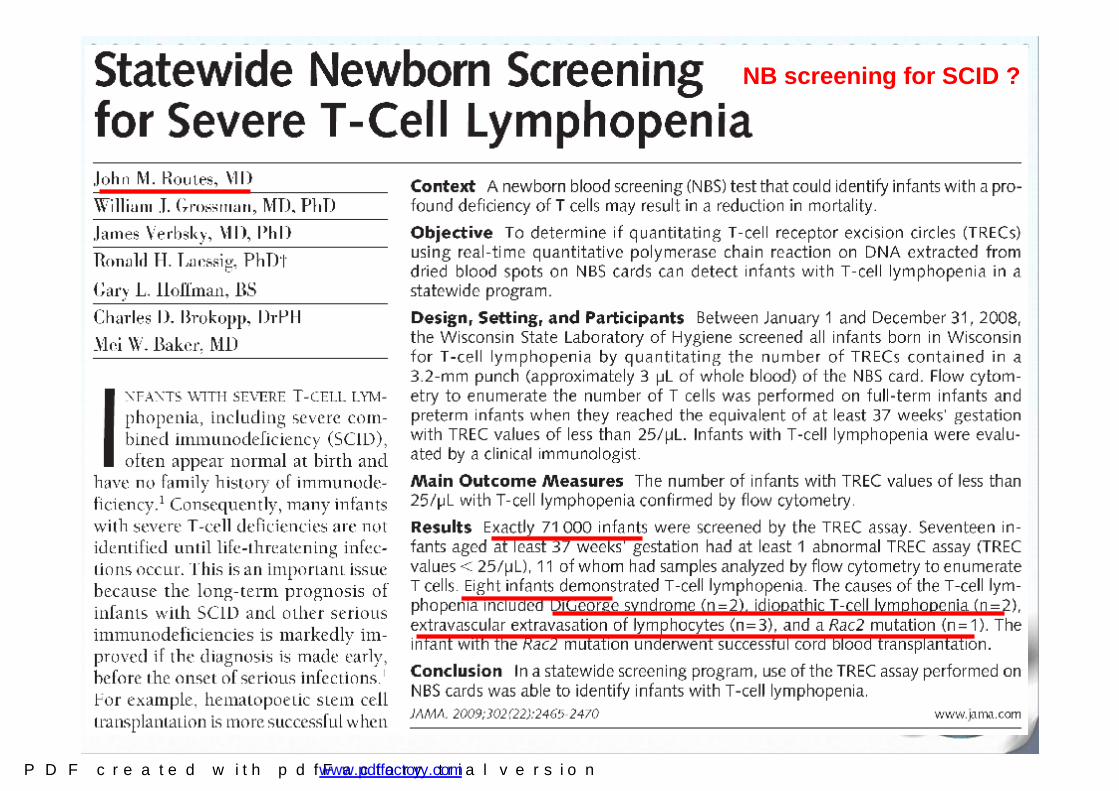
NB screening for SCID ?
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
For early recognize de novo SCID patients…
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Foundation from:
Chang-Gung Medical Research Progress Grant (CMRPG)
National Science Council Grant (NSC)
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Thanks for your attention !
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com




![Recurrent meningitis in children: etiologies, …centers.ju.edu.jo/en/idvc/LatestPublications/meningitis.pdfthen [2, 3]. The exact incidence of recurrent bacterial menin-gitis is not](https://img.dokumen.tips/doc/110x75/5e4093b072e3fb14b003bea4/recurrent-meningitis-in-children-etiologies-then-2-3-the-exact-incidence-of.jpg)



















![RoleofUropathogenicEscherichiacoliVirulenceFactorsin ...downloads.hindawi.com/journals/ijn/2012/681473.pdf · recurrent infection [65, 69]. Virulence factors located on the bacterial](https://img.dokumen.tips/doc/110x75/5f7bfeb88ced6b66fe07ec0b/roleofuropathogenicescherichiacolivirulencefactorsin-recurrent-infection-65.jpg)




