Embed Size (px)
Citation preview

Develop. Med. Child Nerirol. 1975, 17, 605-6 I3
A Home-visiting Intervention Programme with Jamaican Mothers and Children
Sallg M. Grantham-McGregor P. Desai
Introduction In Jamaica, as in most developing
countries, very young children from poor social backgrounds are subject to varying degrees of malnutrition and considerable morbidity from infections (Miall et ul. 1970, Grantham-McGregor er a/ . 1972). It has recently become apparent that, in addition, their mental development is in jeopardy: Hawke carried out develop- mental assessments of 65 children at one, two and three years of age and found a steady decline in their scores (Grantham- McGregor and Hawke 1971, Back et a/. 1972); and Wein (1971~) found that men- tal development of four-year-old school- entrants from lower socio-economic back- grounds was more than 18 months behind that of their middle-class counterparts.
Scant information is available on the quality of the home environments of lower socio-economic Jamaican families (Richardson 1972; Grantham-McGregor, in preparation), but the indications are that there is a lack of toys and books in the homes and that mothers are often poorly educated and do not provide the type of stimulation usually required to promote satisfactory psychological development. I t is almost certain that such environments are at least partly responsible for the poor
level of mental development found in many pre-school children from lower socio- economic backgrounds.
We therefore undertook a home-visiting project with the aim of helping mothers to interact with their three-year-old child- ren in such a way as to improve their mental development.
The study took place in suburban areas of the city of Kingston, near the University of the West Indies. The general standard of housing was low, with overcrowding and inadequate sanitation, but the areas were not among the very poorest in Kingston.
Methods The project included index and control
groups of mothers and their three-year-old children. The index group was formed by conducting a complete house-to-house census in a defined area and identifying all mothers or guardians who were not in full-time employment and who had child- ren of the appropriate age. Controls were similarly identified in an adjacent area with the same standard of housing. Children living in houses of an atypically high standard, or whose mothers or guardians had reached ‘0’-level standard of education, were not included. One child with brain damage was also excluded.
~ ___
MRC Epidemiology Unit, University of the West Indies, Kingston 7, Jamaica.
605
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1975, 17
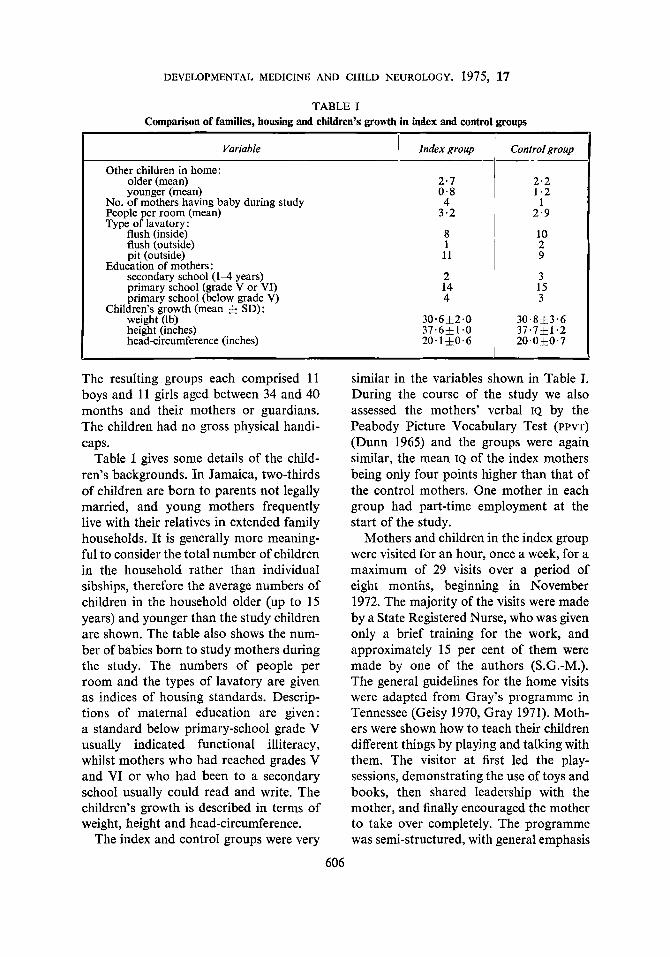
TABLE I Comparison of families, housing and children’s growth in index and control groups
I Variable
Other children in home: older (mean) younger (mean)
No. of mothers having baby during study People per room (mean) Type of lavatory:
flush (inside) flush (outside) pit (outside)
Education of mothers: secondary school ( 1 4 years) primary school (grade V or VI) primary school (below grade V)
Children’s growth (mean & SD): weight (Ib) height (inches) head-circumference (inches)
Index group
2.7 0 .8 4
3.2
8 1
11
2 14 4
Control group
2 . 2 1.2
1 2 . 9
10 2 9
3 15 3
The resulting groups each comprised 11 boys and 11 girls aged between 34 and 40 months and their mothers or guardians. The children had no gross physical handi- caps.
Table I gives some details of the child- ren’s backgrounds. In Jamaica, two-thirds of children are born to parents not legally married, and young mothers frequently live with their relatives in extended family households. It is generally more meaning- ful to consider the total number of children in the household rather than individual sibships, therefore the average numbers of children in the household older (up to 15 years) and younger than the study children are shown. The table also shows the num- ber of babies born to study mothers during the study. The numbers of people per room and the types of lavatory are given as indices of housing standards. Descrip- tions of maternal education are given: a standard below primary-school grade V usually indicated functional illiteracy, whilst mothers who had reached grades V and VI or who had been to a secondary school usually could read and write. The children’s growth is described in terms of weight, height and head-circumference.
The index and control groups were very
similar in the variables shown in Table J. During the course of the study we also assessed the mothers’ verbal IQ by the Peabody Picture Vocabulary Test (PPVT) (Dunn 1965) and the groups were again similar, the mean IQ of the index mothers being only four points higher than that of the control mothers. One mother in each group had part-time employment at the start of the study.
Mothers and children in the index group were visited for an hour, once a week, for a maximum of 29 visits over a period of eight months, beginning in November 1972. The majority of the visits were made by a State Registered Nurse, who was given only a brief training for the work, and approximately 15 per cent of them were made by one of the authors (S.G.-M.). The general guidelines for the home visits were adapted from Gray’s programme in Tennessee (Geisy 1970, Gray 1971). Moth- ers were shown how to teach their children different things by playing and talking with them. The visitor at first led the play- sessions, demonstrating the use of toys and books, then shared leadership with the mother, and finally encouraged the mother to take over completely. The programme was semi-structured, with general emphasis
606

SALLY M. GRANTHAM-MCGREGOR P. DESAI
on increasing the verbal interaction between mother and child and developing the child’s self-confidence and imagination. Specific emphasis was given to teaching basic concepts such as size, colour, shape and quantity. The concept-teaching was based on the curriculum developed by Palmer (1971) whilst working with deprived children in New York.
The books and toys used at each session were left in the home for a week, then exchanged and rotated to other families. Care was taken to select play materials relevant to the children’s environment; other than this the toys were similar to those found in most well-equipped nursery schools or play-groups, i.e. jigsaws, blocks, tea-sets, dolls and beads. Equipment found in the homes was also used when possible. Towards the end of the study mothers and children were taken in small groups to a nearby zoo to demonstrate the educational value of such an outing.
The control group of mothers and children were visited three times during the intervention period, to maintain con- tact and to make arrangements for evalua- tion sessions.
The IQS of all index and control children were assessed before and after intervention with the Griffiths Mental Development Scales for Babies and Young Children (Griffiths 1970), and the PPVT. Only four of the six component scales of the Griffiths Scales were used, namely Hearing and speech, Eye and hand co-ordination, Per- formance and Praciical reasoning. Part- way through the study the IQS of about half the index and half the control children were estimated, using the Grifiths test only (limited resources prevented the testing of the remaining ones).
S.G.-M. performed all initial and inter- mediate tests, but the final Griffiths tests were administered by a psychologist who neither knew the children’s former scores
607
nor was aware whether they were index or control chldren.
At the end of the study all mothers were asked a brief series of questions on child- rearing. Before final evaluations, the nurse graded the index mothers into three categories according to how well they had co-operated with the programme.
Results Three boys were lost from the study:
one index and one control whose families moved from the area, and one index child whose mother went out to work full-time. The number of visits made to the remain- ing 20 index families ranged from 22 to 29. Some of these visits were made in the absence of the mother or child. Five children had fewer than 20 visits with both mother or guardian and child present. However, a suitable substitute who lived with the child was found for four of them, so except for one boy who only had 14 satisfactory visits, all the children had at least 20 visits with both the child and a suitable adult present.
IQs and Changes in IQs Table I1 and Figure 1 show the IQ
scores of the index and control children before and after the intervention pro- gramme. Mean IQS of both groups were initially very similar, but after intervention the mean scores of the index children had risen by 13 points relative to the controls in both the Griffiths test and the PPVT. In both tests there was a tendency for index girls to improve more than boys, which was significant in the PPVT scores only (two-way analysis of variance: GriF
fiths test-experimental effect p< .01 experiment-sex interaction not significant; PPvr-experimental effect p< .01, experi- ment-sex interaction p < .05).
Before intervention there were dis- parities in the mean scores on the four sub-scales of the Griffiths test in both

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1975, 17
9 11 20
TABLE 1I IQs of index and control children before and after intervention
92 14 91 8 92 1 1
i Gri’ths Scales PP VT Group 1 Before Afrer Change Before 1 Afrer Change
1 Mean S D Mean S D
100 14 103 9 102 1 1
88 14 86 12 87 12
Mean S D
+ 8 8 +12 6 +10 7
- 2 9 - 4 7 - 3 8
Mean S D Mean S D Mean SD
- 3 14 $14 16 + 6 17
- 7 9 - 7 8 - 7 8
Index Males Females Both sexes
Control Males Females Both sexes
74 12 70 6 72 9
70 9 70 6 70 7
71 16 84 20 78 19
63 10 63 10 63 10
10 I 9 0 6 i i 90 9 21 1 90 8
p < -01). After intervention, the control children’s mean scores remained hetero- geneous but the index children’s scores had become almost uniform in each of the sub-scales; their greatest gains had been made where originally their scores were lowest, and vice versa (Fig. 2).
The results of testing part-way through the programme indicated that the index children’s Griffiths scores were still im- proving after six months of intervention (Fig. 3). It is uncertain whether improve- ment was still taking place at the end of the project.
Mean IQ
groups of children. They scored relatively highly in F (Practical reasoning) and D (Eye and hand co-ordination) and poorly in C (Hearing and speech) and E (Per- formance) (difference among four means in index and control groups combined
Index
3efore intervention After intervention 105’
100
95
90
85
80
75 I D I C - c o - o L n o m o 7 - - m I l l
E F c D E F Subscale of Griffiths test
Fig. 2. Mean scores of index and control children in the four subscales of the Griffiths test, before and after intervention. (C=Learning and speech, D=Eye and hand co-ordination, E=Perform- ance, F= Practical reasoning.)
Change in I Q Fig. 1. Changes in IQ (Griffiths test) among index and control children during intervention period.
608

SALLY M. GRANTHAM-MCGREGOR P. DESAI
1051
Y 0 9 5 4 /
Control group (n=l l ) 851 \ I
0 3 6 9 12 Time after start of intervention (mo.) Fig. 3. Mean scores in the Griffiths test of index and control children tested part-way through the study.
Factors AJ@cting Change in ZQ The changes in IQ of index children
varied considerably, so relationships be- tween these and certain other variables were sought.
Changes in IQ were significantly cor- related neither with the children’s initial IQ measurements in either of the tests nor with the number of home visits. Changes in the children’s PPVT scores were moder- ately correlated with their mothers’ verbal IQ as assessed by the PPVT (r == 0.52, p< .05), but changes in their Griffiths scores were not. The mothers’ degree of co-operation with programme was cor- related with the changes in the children’s Griffiths scores (Spearman’s rank corr. coeff., r = 0.56, p c . 0 1 ) (Table 111) but not with changes in the children’s PPVT
scores.
Reliability of Tests Over the six-month period between the
initial and interim tests, the scores on the Griffiths scales showed satisfactory test- retest correlations (r = .94) for the 11 control children. A similarly high correla- tion (r = -94) was found between the interim and final scores for the 11 control children, indicating consistency between the two testers. At the final evaluations, the children’s scores on the Griffiths Mental Development Scales were sig- nificantly correlated with those on the PPVT (r = .75, p<.Ol).
Questionnaire on Child-rearing The replies given by the mothers to the
questionnaire on child-rearing showed that the index mothers had a better under- standing of the importance of playing with their children and were more aware of their children’s level of development and the educational value of toys than were the control mothers (Table IV). They also had a better idea of how to involve three-year- olds in story reading, had a greater preference for the use of positive rather than negative motivation in disciplining their children, and participated more in their children’s ‘pretend’ games. Both groups of mothers actually spent the same amount of time with their children. In some instances the difference between the groups was only slight, but in every item but the last the differences favoured the index mothers, and the difference reached statistical significance in three items.
TABLE III Changes in Griffiths Scores of index children according to degree of co-operation of mothers
i Co-operation grading of mother
Mean Range Most co-operative . . .. .. . . .. ~ 7 Jr13.9 +5 to +19
+11.7 +4 to +23 Intermediate . . . . . . . . . . . . Least co-operative .. .. ..
I No. I Change in children’s fQs
1 - 5 . 1 -2 to +I4 ’ . I . I
609

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1975, 17
TABLE IV Differences in child-rearing practices between mothers of index and control children at end of intervention
period
Aspect of child-rearing
Awareness of importance of playing and chatting with child Awareness of child’s mental abilities Awareness of educational value of toys Awareness of appropriate method of reading to child Preference for positive rather than negative motivation Participation by child and mother in ‘pretend‘ games Actual time spent with child
Whether diflerences between groups in desired direction, and statistical signGcance
of difference (2 test)
Yes (P < .05) Yes (P < .05)
Yes (N.S.) Yes (N.S.) Yes (N.S.)
-
Yes (P < 4 5 )
No (-->
Discussion Many previous intervention programmes
have been criticised for errors in their experimental design. Both Jensen (1969) and Palmer (1970) report that children from impoverished homes are often in- hibited and do poorly at initial IQ testing, and therefore have artificially high gains at post-intervention testing when they are more at home with the test situation. We found that these Kingston children were very shy and inhibited, so great care was taken to put them at ease. They were brought several times to the testing centre, where they played and were given re- freshments, and testing was not carried out until they were considered to be relaxed. Another criticism is the lack of adequate control-groups (Jensen 1969, Tizard 1970); our control group was care- fully chosen and was tested as often as the index group. A third pitfall is that the evaluators of studies are often familiar with the children and involved in the intervention; final evaluations in this study were done by an independent tester. It would appear, therefore, that the IQ gains reported here are realistic ones.
A problem in testing children in Jamaica is that there are no indigenous tests for children under four years. This is the first reported use of the Griffiths test in Jam- aica. Its administration presented very few problems and the test-retest reliability
on this small sample was satisfactory. The children’s Griffiths scores correlated satis- factorily with their PPVT scores at four years of age (r = .75, p<*Ol), the latter having been used on larger samples of four-year-olds in Jamaica and found to be satisfactory, and also to correlate well with the Caldwell Pre-school Inventory (Cald- well 1965, Wein 1971a, b).
The Griffiths test was standardised in Britain, and designed so that the average scores of children in each sub-scale were the same. On initial testing, both index and control groups had significantly different scores in the different sub-scales. However, it was remarkable how similar the index children’s mean scores on each sub-scale had become by the end of the study. If changing the home environment to such a limited degree can significantly alter the children’s developmental profile, the pre- sence of the original pattern can hardly be used as evidence for or against genetic differences between them and the popula- tion used to standardise the test.
Another problem in evaluating pre- school programmes is defining the criteria for success. Although mental tests have recently fallen into disrepute in the United States, IQ scores are still the best single predictors of contemporary occupational and scholastic success (Kennedy 1969). More specifically, initial mental ability of pupils measured during the primary-
610

SALLY M. GRANTHAM-MCGREGOR P. DESAI
school grades accounts for more of the individual differences in subsequent school- performance than any other single variable (Wilson 1967). Zimiles (1968) and Tizard (1970) point out that IQ gains are a very narrow criterion when considering the total development of children, but there is no easy way of evaluating the many other benefits gained by both the child and his family. The children in this study almost certainly gained in self-confidence, and probably in many other ways. The younger sibIings were included in the visits and they too appeared to benefit. The mothers themselves generally enjoyed the \isits and learnt some of the ways they could assist their children to reach their ftill intellectual potential. Gray’s home-visiting project in Tennessee found that younger siblings showed a significant improvement com- pared with those in a control group (Gil- mer et d. 1970), and there was some sugges- tion that the mothers’ life-style actually improved during the project (Gray 1971). The index mothers in this study were not spending more time with their children than were the control mothers, so pre- sumably they were spending their time more usefully.
A gain of 13 points is a very promising one for such a limited and economical intervention programme. The input was deliberately minimised so that it would be feasible to repeat on a larger scale. Other studies have shown larger gains, but they had considerably greater inputs over longer periods of time (Weikart 1971, Heber et at. 1972, Levenstein 1974). It may be noted that the verbal IQ of the mothers was not related to the children’s change in JQ in the Griffiths test, even moth- ers with a relatively low IQ being able to help their children.
No attempt was made to improve the children’s health or nutritional status. Though none of them was severely or moderately malnourished, their median
61 1
and other percentiles of weight fell below the Boston standards (Stuart and Stephen- son 1959) for three-year-old boys and girls by about 1 and 2 lb respectively. They also had frequent minor infections. It is poss- ible that providing health and nutritional care might have further improved their performance.
The long-term effects of intervention obviously are important, and Gray and Klaus (1970) have shown that when famil- ies are included in such programmes the benefits last longer than when the children alone are involved. Results of the long- term follow-up on the children in this study are not yet available.
West-Indian immigrant school-children in Britain are having problems with the educational system (Coard 1971, Yule ef af. 1979, and Pollack (1972) has suggested that their mental development is falling be- hind that of their English peers as early as three years of age. It would be a disservice to the West-Indian community in Britain to dwell overmuch on the hypothesis (Jen- sen 1969) of a ‘biological difference’ in psychological function between blacks and whites, which was discussed in the Lancet (1973). This hypothesis tends to minimise the damage done to young children by the environment and thereby delays much- needed intervention programmes.
The results of this present study suggest that Jamaican mothers from lower socio- economic homes are a potentially valuable source of education for their young child- ren. Intervention at pre-school age need not be expensive if the mothers’ co- operation is fully used; apart from costs related to the research aspect of the pro- gramme, the major expenses were the salary of the nurse working full-time for eight months, El50 for toys and books, and transport. Where nurses or health-aides are already visiting at-risk families, as in

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1975, 17
SUMMARY In order to promote better mental development in three-year-old children from poor
Jamaican families, a home-visiting project was carried out with the aim of helping mothers to interact with and stimulate their children. Homes were visited once a week, and the use of toys and books was demonstrated to the mothers. The play equipment was then left with the family and exchanged at the following visit. After a maximum of 29 visits, the children had made significant gains (average 13 IQ points) compared with children in a previously matched control group. The mothers’ knowledge of child-rearing had also improved. Similar intervention programmes may be useful on a larger scale, and need not be expen- sive if full use is made of the mothers’ help.
R ~ S U M E Programme de visite ci domicile chez des mires et enfants Jnmaicains
Pour favoriser un meilleur diveloppement mental chez des enfants de trois ans de familles jamaicaines pauvres, un projet de visite a domicile a e t i entrepris dans le but d’aider les mkres A agir et stimuler leurs enfants. Les maisons Ctaient visitees une fois par semaine, l’usage de jouets et de livres expliquC aux mbres. L‘Cquipement de jeu Ctait alors IaissC dans la famille puis &change a la visite suivante. Aprbs un maximum de 29 visites, les enfants prtsentaient un gain significatif en moyenne de treize points de QI, compares a des enfants d‘un groupe contr6Ie antCrieurement appariC. Les connaissances Cducatives des mbres avaient Cgalement progresse. Les auteurs concluent que de semblables programmes d’intervention pourraient Ctre utiles sur une plus grande Cchelle et ne sont pas trop coateuses yi l’aide des meres est pleinement utilist.
ZUSAMMENFASSUNG Ein lnterventionsprogramm fiir Hausbesuehe bei Miittern und Kidern auf Jamaika
In der Absicht, eine bessere Entwicklung der dreijahrigen Kinder armer jamaikanischer Familien zu gewahrleisten, wurde ein Hausbesuchsprojekt mit der Unterstiitzung hilfsbe- reiter Mutter unternommen, mit diesen Kindern in Beziehung zu treten und sie zu stimul- ieren. Die Hauser wurden einmal wochentlich besucht, und den Muttern wurde der Ge- brauch von Spielzeug und Biichern demonstriert. Die Spielausrustung wurde dann bei der Familie belassen und beim nachsten Besuch ausgetauscht. Nach einem Maximum von 29 Besuchen zeigten die Kinder eine signifikante Zunahme von 13 IQ-Punkten im Vergleich zu Kindern einer vorher passenden Kontrollgruppe. Die Kenntnisse der Mutter in der Kin- dererziehung hatten ebenfalls zugenommen. Es wird festgestellt, daB ahnliche Interventions- programme mit einer grol3eren Breite niitzlich sein konnten, ohne teuer zu sein, wenn die Hilfsbereitschaft der Mutter vollkommen ausgeschopft wird.
RESUMEN Un programa de intervencidn con visitas a domiciIio para madres y niiios de Jamaica
Con el objeto de promover el mejor desarrollo mental en niiios de tres aiios pertenecientes a familias pobres de Jamaica, se realiz6 un proyecto de visitas a domicilio con el objeto de ayudar a las madres a interaccionar y estiniular a sus niiios. Los domicilios fueron visitados una vez a la semana y fuC mostrada a las madres la utilizaci6n de juguetes y libros. El
612

SALLY M. GRANTHAM-MCGREGOR P. DESAI
equipo de juego se dejo con la familia y se cambib en la visita siguiente. Despuis de un maxim0 de 29 visitas, 10s nifios habian realizado unas ganancias significativas de un prome- dio de 13 puntos en el CI, en comparacion con niiios de un grupo control homogtneo. Mejoraron tambitn 10s conocimientos de las madres sobre como cuidar a sus niiios. Se concluy6 que unos propramas de intervencibn siniilares podrian ser iitiles en una escala mhs grande y no necesitaban ser caros si la ayuda de la madre se utilizaba por compIeto.
REFERENCES Alderman, M. H., Levy, B., Husted, J., Searle, R. (1973) ‘A young-child nutrition programme in rural
Jamaica.’ Lancet, i , 1166. Back, E., Grantham-McGregor, S. M., Hawke, W. A,, Milbourn, P., Robinson. A., Williams, B. (1972) ‘A
four year developmental survey of Jamaican children.’ (Preliminary report) Wesf Indian Medical Journal, 21,50.
Caldwell, B. M. (1965) Pre-school Inventory. Syracuse, N.Y.: Children’s Center, State University of New York.
Coard, B. (1971) ‘How the West Indian child is made educationally subnormal in the British school system. The scandal of the black child in schools in Britain.’ London: New Beacon Books.
Dunn, L. M. (1965) Peabody Picture Vocabulary Test. Nashville, Tenn.: American Guidance Service. Geisy, R. (Ed.) (1970) A Guide for Home Visitors. Nashville, Tenn.: Peabody College. Gilmer, B., Miller, J., Gray, S. (1970) ‘Intervention with mothers and young children. A study of intra-
family effects.’ Nashville, Tenn. : Demonstration and Research Centre for Early Education. Papers and Reports, vol. 4, no. 1 1 .
Crantham-McGregor, S. M., Hawke, W. A. (I97 I ) ‘Developmental assessment of Jamaican infants.’ Developmental Medicine and Child Neurologv, 13, 582. - Desai, P., Back, E. H. (1972) ‘A longitudinal study of infant growth in Kingston, Jamaica.’ Human Biology, 44, 549.
Gray, S. (1971) ‘Home visiting programs for parents of young children.’ Nashville, Tenn.: Demonstration and Research Center for Early Education, Peabody College. Papers and Reports, vol. 5, no. 4. - Klaus, R. A. (1970) ‘The early training project: a seventh-year report.’ Child Development, 41,909.
Griffiths, R. (1970) ‘The abilities of young children.’ London: Child Development Research Centre. Heber, R., Garber, H., Harrington, S., Hoffman, C., Fallender, C. (1972) ‘Rehabilitation of families at risk
Jensen, A. R. (1969) ‘How much can we boost IQ and scholastic achievement?’ Harvard Educational Review,
Kennedy, W. A. (1969) ‘A follow-up normative study of Negro intelligence and achievement.’ Monographs of the Society for Research in Child Development, 34, 40.
Lancet, (1973) ‘Biological differences and social justice.’ Lancet, i , 414. Levenstein, P. (1974) ‘A message from home: a home based intervention method for low-income preschool-
ers.’ Paper presented at a Conference on The Mentally Retarded and Society: a Social Science Perspective,
for mental retardation.’ 1972 Progress Report. University of Wisconsin.
39, 1.
at Niles, Michigan, 1974. Miall, W. E., Desai, P., Standard, K. L. (1970) ‘Malnutrition, infection and child growth in Jamaica.’
Journal of Biosocial Science, 2, 3 I . Palmer, F. ( 1 970) ‘Socio-economic status and intellective performance among Negro preschool boys.’
Developmental Psychology, 3, 1. - (1971) Concept Training Curriculumfiv Children Ages Two to Five, Vol. I-V. Stonybrook: State Univer- sity of New York.
Pollack, M. ( I 972) Today’s Three Year Olds in London. London: S.I.M.P./Heinemann Medical. Richardson, S. A. (1972) ‘Ecology of malnutrition: nonnutritional factors influencing intellectual and be-
havioral development.’ In Picou, D., Birch, H. G., Richardson, S. A., (Eds.) Nutrition, the Nervous System and Behaviour. P.A.H.O. Publication no. 251, p. 101.
Stuart, H. C., Stevenson, S. S. (1959) ‘Physical growth and development.’ In Nelson, W. E. (Ed.) Textbook of Pediatrics, 7th Ed. Philadelphia: W. B. Saunders, p. 48.
Tizard, J. (1970) ‘New trends in developmental psychology.’ British Journal of Educational Psychology, 40,1. Weikart, D. (1971) ‘Early childhood special education for intellectually subnormal and/or culturally different
children.’ Paper prepared for the National Leadership Institute in Early Childhood Development, Wash- ington, D.C.
Wein, N. (1971~) ‘Analysis of the four subtests of the Caldwell pre-school inventory revised for Jamaican children.’ Report from Bernard van Leer Foundation of Jamaica, Ltd. Project for Early Childhood Education. - (1971b) ‘Validation study of the Caldwell and Peabody Picture Vocabulary Test.’ Report from Bernard van Leer Foundation of Jamaica, Ltd. Project for Early Childhood Education.
Wilson, A. B. (1967) ‘Educational consequences of segregation in a Californian community.’ In Racial Isolafion in Public Schools, Vo/. 2. Washington, D C.: U.S. Government Printing Office.
Yule, W., Berger, M., Rutter, M., Yule, B. (1975) ‘Children of West Indian immigrants-XI. Intellectuaf performance and reading attainment.’ Jouvnnl of Child Psychology and Psychiatry, 16, 1.
Zimiles, H. (1953) ‘An analysis of current issues in the evaluation of educational programs.’ In Hellmuth, J. (Ed.) Disadvnntaged Child. Vol. 2. New York: Brunner/Mazel.
613