Embed Size (px)
Citation preview

Acta Biomaterialia xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /actabiomat
Brief communication
A histological and mechanical analysis of the cardiac lead–tissueinterface: implications for lead extraction
1742-7061/$ - see front matter � 2014 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.actbio.2014.01.008
⇑ Corresponding author. Tel.: +1 650 724 6672; fax: +1 650 724 9501.E-mail address: [email protected] (G.C. Gurtner).
1 These authors contributed equally to this work.
Please cite this article in press as: Rennert RC et al. A histological and mechanical analysis of the cardiac lead–tissue interface: implications for leadtion. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
Robert C. Rennert a,1, Kristine Rustad a,1, Kemal Levi a, Mark Harwood b, Michael Sorkin a,Victor W. Wong a, Amin Al-Ahmad b, Paul Zei b, Henry Hsia c, Ramin E. Beygui d, Linda Norton b,Paul Wang b, Geoffrey C. Gurtner a,⇑a Department of Surgery, Stanford University Medical Center, Stanford, CA, USAb Division of Cardiovascular Medicine, Department of Internal Medicine, Stanford University Medical Center, Stanford, CA, USAc Division of Cardiology, Department of Internal Medicine, UCSF, San Francisco, CA, USAd Department of Cardiothoracic Surgery, Stanford University Medical Center, Stanford, CA, USA
a r t i c l e i n f o
Article history:Received 12 September 2013Received in revised form 19 November 2013Accepted 7 January 2014Available online xxxx
Keywords:FibrosisPacemakerTensile testStress analysis
a b s t r a c t
The major risks of pacemaker and implantable cardioverter defibrillator extraction are attributable to thefibrotic tissue that encases them in situ, yet little is known about the cellular and functional properties ofthis response. In the present research, we performed a histological and mechanical analysis of human tis-sue collected from the lead–tissue interface to better understand this process and provide insights for theimprovement of lead design and extraction. The lead–tissue interface consisted of a thin cellular layerunderlying a smooth, acellular surface, followed by a circumferentially organized collagen-rich matrix.51.8 ± 4.9% of cells were myofibroblasts via immunohistochemistry, with these cells displaying a similarcircumferential organization. Upon mechanical testing, samples exhibited a triphasic force–displacementresponse consisting of a toe region during initial tensioning, a linear elastic region and a yield and failureregion. Mean fracture load was 5.6 ± 2.1 N, and mean circumferential stress at failure was 9.5 ± 4.1 MPa.While the low cellularity and fibrotic composition of tissue observed herein is consistent with a foreignbody reaction to an implanted material, the significant myofibroblast response provides a mechanicalexplanation for the contractile forces complicating extractions. Moreover, the tensile properties of thistissue suggest the feasibility of circumferential mechanical tissue disruption, similar to balloon angio-plasty devices, as a novel approach to assist with lead extraction.
� 2014 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
The number of pacemakers and implantable cardioverter defi-brillators (ICDs) that are implanted each year continues to increase[1,2]. However, device-related complication rates are also rising[3], portending an increase in the rate of endovascular lead extrac-tion procedures. While the indications for extraction have beenestablished, and include systemic infections, pocket infectionsand lead malfunction [4], the potential for major cardiovascular in-jury or death with this procedure remains [5], despite the in-creased efficacy of laser-assisted techniques [6]. In fact, therecent multi-center Lead Extraction in the Contemporary Setting(LExICon) Study, which looked only at laser-assisted lead extrac-tion, reported a procedural major adverse event rate of 1.4%, andan overall in-hospital mortality rate of 1.86% [7].
Interestingly, the major risks associated with lead extraction,including cardiac avulsions and vascular tears [7], can be directlylinked to an imperfect separation of the lead from the fibrous tis-sue that binds it to the myocardium and venous endothelium.Moreover, this fibrotic response appears to be dynamic, as leadimplantation time has been linked to an increase in complexityand overall failure of lead removal procedures [7,8], likely stem-ming from an increase in fibrosis along the lead body and electrodetip over time.
Unfortunately, studies examining the in situ response toimplantable pacemaker and ICD leads are rare [9,10], with rela-tively little known about the histological and mechanical featuresof the resulting tissue. A better understanding of this process couldhelp improve the design of leads and extraction techniques, andfurther decrease the morbidity and mortality associated with thisprocedure. As such, this study aims to characterize the cellularand mechanical properties of human tissue collected from the leadsurface upon removal of implantable devices, using stains, imaging
extrac-

2 R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx
and mechanical analyses that have been established for thedescription of scarring and fibrosis in other organs.
2. Materials and methods
2.1. Extraction and collection of tissue
All patients were consented as per the IRB protocol prior to theirextraction procedure (IRB #19053). Procedures were performed inthe operating room with electrophysiology and cardiac surgeryphysicians present. Pacemaker and/or ICD leads were extractedeither by manual traction alone, or with a combination of Excimerlaser sheaths (Spectranetics, Colorado Springs, CO) and manualtraction. Upon completion of the procedure, all attached tissuewas kept on the lead, and the lead and tissue were placed into50 ml conical polypropylene tubes (BD Falcon, San Jose, CA) andput on ice. After collection, leads were promptly sent to the labora-tory for analysis.
2.2. Histological analysis
Tissue surrounding freshly extracted cardiac leads was carefullyremoved using microsurgical instruments, fixed in 4% paraformal-dehyde and embedded in paraffin blocks, before being cut into10 lm thick sections. After deparaffinization and rehydration, sec-tions were stained with hematoxylin and eosin (H&E, Sigma–Al-drich, St Louis, MO), Masson’s trichrome (Sigma–Aldrich) ordirect red 80 (picrosirius red, Sigma–Aldrich). Sections were alsoimmunostained for type I and III collagens (primary 1:100, Abcam,Cambridge, MA; secondary 1:400 Alexa-Fluor 594 & 488, Invitro-gen, Grand Island, NY), with nuclei stained with 40,6-diamidino-2-phenylindole (DAPI; Vector Laboratories, Burlingame, CA).Immunolabeling using a directly conjugated antibody against a-smooth muscle actin (a-SMA) (Cy3, 1:250, Sigma–Aldrich, St Louis,MO), and for the intermediate filaments vimentin and desmin (pri-mary 1:100, Abcam; secondary 1:400 Alexa-Fluor 594, Invitrogen)was similarly performed.
2.3. Myofibroblast quantification
To quantify myofibroblasts, four high-power images (400�)were taken (at the 12, 3, 6 and 9 o’clock positions) of a single tissuesection per patient for both alpha-smooth muscle actin (a-SMA)and DAPI using an Axioplan 2 Imaging microscope (Carl Zeiss,Inc., Oberkochen, Germany), and overlayed in Photoshop CS5(Adobe, San Jose, CA). Only patients with intact, circular tissue sec-tions and positive staining were analyzed. Double positive and to-tal cells were then counted for each picture by three independentinvestigators. Total a-SMA positive cell counts were averaged, nor-malized to total nuclei and reported as the mean percentage of a-SMA positive nuclei per total cells.
To ensure that vascular smooth muscle and endothelial cells(also stained by a-SMA) were excluded from this analysis, tissueblood vessel frequency and morphology were characterized onseparate sections stained with H&E and directly conjugated anti-isolectin (Alexa-Fluor 488, Griffonia simplicifolia, 1:200, Invitrogen).Cells exhibiting blood vessel morphology were found to be discreteand rare, and were excluded from myofibroblast cell counts.Expression levels of the intermediate filaments vimentin and des-min were also determined to confirm the myofibroblastphenotype.
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
2.4. Tissue thickness quantification
To quantify tissue thickness, four high-power images (400�)were taken (at the 12, 3, 6 and 9 o’clock positions) of a singleH&E stained tissue section per patient. Images were opened in Axi-oVision 4.8 software (Carl Zeiss, Inc, Oberkochen, Germany), andtissue thickness was measured once at each position (excludingirregular tissue appendages). Only patients with intact, circular tis-sue sections were included in average tissue thickness calculations.
2.5. Scanning electron microscopy (SEM) imaging
For high-resolution SEM characterization of tissue, fresh tissuesections were cut to expose the tissue–lead interface and fixed in4% paraformaldehyde, 2% gluteraldehyde and 0.1 M cacodylatebuffer overnight. The tissue was then serially dehydrated in gradedethanol/water solutions, critically dried using a Tousimis Autosam-dri-814 critical point dryer (Tousimis Research Corporation, Rock-ville, MD) and sputter-coated with a conductive layer of gold–palladium (AuPd). The samples were imaged using a Hitachi3400 N VP scanning electron microscope (Hitachi High Technolo-gies America, Inc., Schaumburg, Illinois) at the Stanford Cell Sci-ences Imaging Facility.
2.6. Mechanical testing
Following technical refinements, selected tissue samples wereimmediately placed in phosphate-buffered saline upon collection,and stored at either –20 �C or 4 �C for mechanical testing. Tissueplaced at –20 �C was analyzed within weeks of freezing, while tis-sue stored at 4 �C was analyzed within 72 h. The circumferentialforce–length relationships of samples were determined utilizingan adapted tensile ring methodology [11]. Briefly, circumferentialsamples were cut to create tissue rings with an approximate widthof 1.5 mm. The rings were then loaded onto hooks of a uniaxial ten-sile testing apparatus (Bionix 200, MTS Systems Corporation, EdenPrairie, MN) equipped with a 44.48 N load cell and stretched untilfailure using a strain rate of 1% s�1. The circumferential stress (rC)was calculated by dividing the load (L) at a given time point by twotimes the cross-sectional area (2⁄A) of the specimens at that giventime point:
rC ¼L
2A
Initial cross-sectional areas were calculated from baseline tis-sue width and thickness measurements, with cross-sectional areasat various levels of stretch determined as previously describedbased upon an assumption of isovolumic tissue deformation [11].Circumferential strain (eC) was defined as the change in circumfer-ence/original circumference, and was determined to be the same asthe diametric strain (strain based on diameter) as shown in the fol-lowing equation (D = inner tissue ring diameter):
eC ¼pðDþ DDÞ � DD
pD¼ DD
D:
The circumferential tissue modulus was determined by plottingcircumferential stress vs. circumferential strain, and calculatingthe slope of the line from the strain frame 1.5 to 2, as this initiallinear portion of the curve was present in all samples.
2.7. Statistical analysis
Quantitative data are expressed as mean ± standard error of themean. Statistical significance across two groups was determinedusing a Student’s t-test, and across multiple groups using a one-
l analysis of the cardiac lead–tissue interface: implications for lead extrac-

R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx 3
way ANOVA (SPSS Statistics v20.0, IBM, Armonk, NY). For all tests,a p-value � 0.05 was considered statistically significant.
3. Results
3.1. Patient characteristics and tissue properties
Over a 2 year period, 43 total leads were collected from 20 pa-tients, with 28 leads (65%) having attached tissue. The average pa-tient age at time of lead removal was 60.4 years, with the averagetime from lead implant being 5.2 years (Table 1). 15 of the 20 pa-tients (75%) underwent lead removal as a result of infection, withnine pacemaker pocket infections (45%), four lead vegetations(20%) and two cases of bacteremia (10%). Outside of infectiouscomplications, two patients underwent implant removal due to de-vice erosion through tissue (10%) and one patient experienced alead fracture (5%). The two remaining patients underwent lead re-moval as a result of patient pain or for lead management followingfactory recall.
3.2. Tissue histology and cellular composition
The amount and thickness of tissue obtained from the leads var-ied across patients, with scar tissue often being found not only onthe coiled surfaces and the lead tips, but also on the intravascularlylocated lead body (Fig. 1a and b). Leads without adherent tissuewere excluded from further analysis. The average thickness of cir-cumferential tissue samples was 458.6 ± 117.4 lm (n = 7 patients),with this variation likely stemming from the use of multipleextraction techniques (i.e. traction alone or laser-assisted). H&E,Masson’s trichrome and picrosirius red staining of tissue (n = 8 pa-tients) showed a collagen-rich matrix with a low cellularity, anddensely spaced collagen fibers demonstrating a circumferentialorganizational pattern (Fig. 1c and d, Supplemental Fig. 1a).
Collagen organization and temporal dynamics were furthercharacterized through picrosirius red staining, wherein thinner,less densely packed fibers tend to be yellowish-green, while thick-er, more closely packed fibers are more likely to be orange-red[12,13]. Interestingly, this analysis revealed a trend toward smallerdiameter fibers near the lead interface in the initial 7–8 monthsafter implantation (Fig. 1d, left panels), suggestive of a predomi-
Table 1Patient and lead characteristics.
Patient Age (yrs) Gender Reason for Removal Number of Le
1 57 F Pocket infection 22 65 M Pocket infection 13 53 F Lead vegetation 44 60 M Pocket infection 25 75 M Lead vegetation 16 67 F Pocket infection 47 91 M Bacteremia 18 48 F Lead fracture 19 67 F Patient pain 310 63 M Pocket infection 211 67 M Pocket infection 212 54 M Lead vegetation 313 65 M Pocket infection 214 68 F Lead vegetation 215 78 M Device erosion 216 18 F Device recall 217 45 F Device erosion 218 78 M Pocket infection 219 47 M Bacteremia 220 41 M Pocket infection 3
Patients with multiple time from implant dates reflect unique implantation procedures.
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
nant deposition of immature type III collagen known to occur inthe early stages of wound healing [14,15]. Conversely, more uni-form, thicker diameter collagen fibers were frequently observedin tissue samples obtained from leads that had been in place longer(Fig. 1d, right panels), consistent with normal scar remodeling anda transition to more organized and mature type I fibers. Collagenimmunolabeling confirmed the predominance of type I collagenin more mature post-implantation fibrotic tissues (Fig. 1e); how-ever, the persistence of lower levels of type III fibers in these sam-ples is suggestive of an ongoing remodeling process.
Immunohistochemical staining (n = 5 patients) revealed that51.8 ± 4.9% of total cells expressed the myofibroblast marker a-SMA, with many of these cells displaying a spindle-like morphol-ogy characteristic of myofibroblasts (Fig. 2a). Vimentin immuno-histochemistry demonstrated a similar staining pattern as a-SMA, while desmin staining was largely negative (Fig. 2b and c),with this a-SMA(+)/vimentin(+)/desmin(�) cell profile matchingprevious descriptions of myofibroblasts in pathologic fibrovascularand myocardial tissues [16,17]. These findings are consistent witha significant, sustained myofibroblast response on the level ofother pathologic fibroses, such as hypertrophic scars [18], liverfibrosis [19] and idiopathic pulmonary fibrosis [20]. Additionally,a-SMA positive myofibroblasts displayed cytoplasmic extensionsorganized along the circumferential axis of the lead, suggestive ofa potential role in the generation of contractile forces upon theimplant.
3.3. SEM analysis
SEM analysis (n = 3 patients) revealed that the lead–tissueinterface was composed of a narrow layer of cells (likely monocyticbased on morphology and presence of a foreign body) underlying asmooth, acellular surface, followed by a deeper, more fibrous layerwith a primarily circumferential organization (Fig. 3a–c). Addition-ally, tissue ingrowth into the ICD coils was readily visualized(Fig. 3d), and found to occur as early as 6 months afterimplantation.
3.4. Mechanical properties
Mechanical analysis of fibrotic tissue (n = 3 patients, 7 samples)generated force–displacement curves with three discrete regions:
ads Lead Location Implant Type Time from Implant (months)
RA, RV P. D 84RV D 85RA (2), RV, LV P. D 78,7RA, RV D 76RV D 85RA, RV(2), LV RD 137, 88RV P 6RA, RV D 10RA, RV, LV P. D 11RA, RV P, D 106RA, RV P. D 43RA, RV, LV P, D 67RA, RV P 224RA, RV RD 84RA, RV P 44, 92RA, RV P.D 68RA, RV P. 0 56RA, RV P 1.2RA, RV P.D 38RA, RV(2) P. D 18
RA, right atrium; RV, right ventricle; LV, left ventricle; P, pacer; D, defibrillator.
l analysis of the cardiac lead–tissue interface: implications for lead extrac-
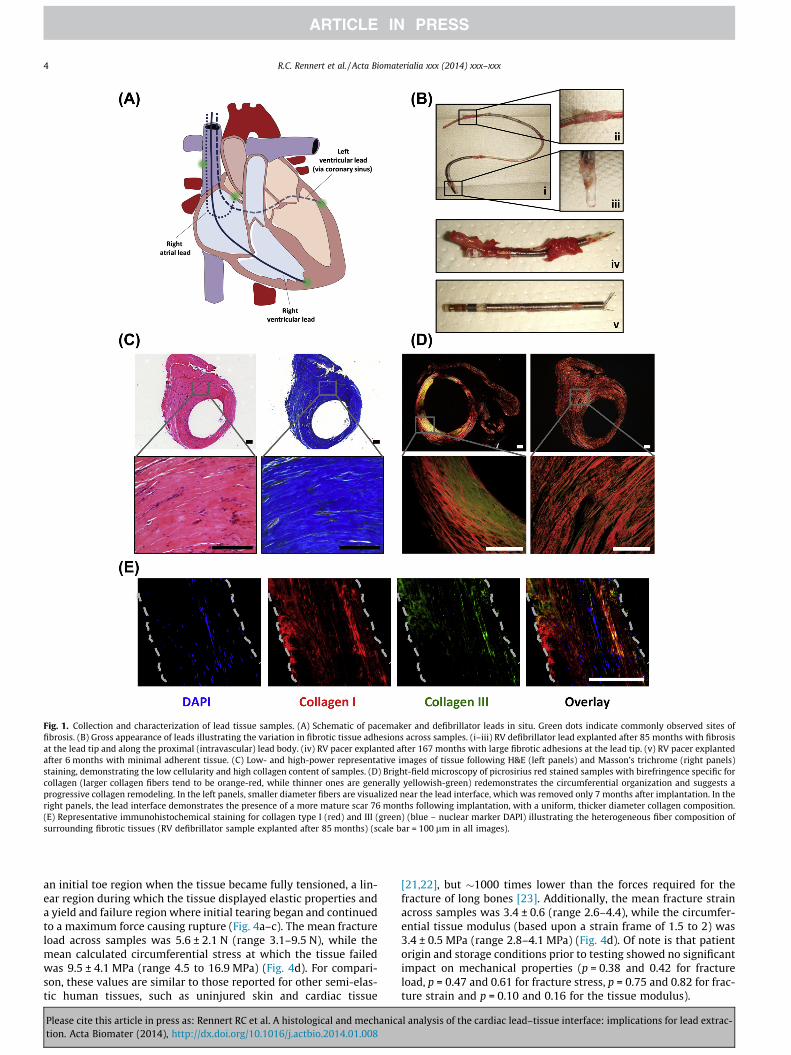
Fig. 1. Collection and characterization of lead tissue samples. (A) Schematic of pacemaker and defibrillator leads in situ. Green dots indicate commonly observed sites offibrosis. (B) Gross appearance of leads illustrating the variation in fibrotic tissue adhesions across samples. (i–iii) RV defibrillator lead explanted after 85 months with fibrosisat the lead tip and along the proximal (intravascular) lead body. (iv) RV pacer explanted after 167 months with large fibrotic adhesions at the lead tip. (v) RV pacer explantedafter 6 months with minimal adherent tissue. (C) Low- and high-power representative images of tissue following H&E (left panels) and Masson’s trichrome (right panels)staining, demonstrating the low cellularity and high collagen content of samples. (D) Bright-field microscopy of picrosirius red stained samples with birefringence specific forcollagen (larger collagen fibers tend to be orange-red, while thinner ones are generally yellowish-green) redemonstrates the circumferential organization and suggests aprogressive collagen remodeling. In the left panels, smaller diameter fibers are visualized near the lead interface, which was removed only 7 months after implantation. In theright panels, the lead interface demonstrates the presence of a more mature scar 76 months following implantation, with a uniform, thicker diameter collagen composition.(E) Representative immunohistochemical staining for collagen type I (red) and III (green) (blue – nuclear marker DAPI) illustrating the heterogeneous fiber composition ofsurrounding fibrotic tissues (RV defibrillator sample explanted after 85 months) (scale bar = 100 lm in all images).
4 R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx
an initial toe region when the tissue became fully tensioned, a lin-ear region during which the tissue displayed elastic properties anda yield and failure region where initial tearing began and continuedto a maximum force causing rupture (Fig. 4a–c). The mean fractureload across samples was 5.6 ± 2.1 N (range 3.1–9.5 N), while themean calculated circumferential stress at which the tissue failedwas 9.5 ± 4.1 MPa (range 4.5 to 16.9 MPa) (Fig. 4d). For compari-son, these values are similar to those reported for other semi-elas-tic human tissues, such as uninjured skin and cardiac tissue
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
[21,22], but �1000 times lower than the forces required for thefracture of long bones [23]. Additionally, the mean fracture strainacross samples was 3.4 ± 0.6 (range 2.6–4.4), while the circumfer-ential tissue modulus (based upon a strain frame of 1.5 to 2) was3.4 ± 0.5 MPa (range 2.8–4.1 MPa) (Fig. 4d). Of note is that patientorigin and storage conditions prior to testing showed no significantimpact on mechanical properties (p = 0.38 and 0.42 for fractureload, p = 0.47 and 0.61 for fracture stress, p = 0.75 and 0.82 for frac-ture strain and p = 0.10 and 0.16 for the tissue modulus).
l analysis of the cardiac lead–tissue interface: implications for lead extrac-

Fig. 2. Myofibroblasts are a large component of the fibrotic response to implanted leads. (A) Immunohistochemical staining and quantification of the myofibroblast markeraSMA (red; blue – nuclear stain DAPI). Approximately 50% of total cells are aSMA (+), with many displaying a spindle cell morphology characteristic of myofibroblasts (whitearrowheads). (B, C) Fibrotic tissues were also positive for the intermediate filament vimentin, and largely negative for desmin, consistent with a myofibroblast phenotype(scale bar = 100 lm in all images).
Fig. 3. SEM visualization of scar tissue. (A, B) Low, medium and high magnification SEM images of collected tissue illustrating a narrow layer of cells (black arrowheads)underlying a smooth lead–tissue interface (white arrowheads), followed by a deeper, circumferentially organized fibrous layer (brown arrowheads). (C) High magnificationSEM visualization of the smooth lead–tissue interface. (D) SEM visualization of tissue ingrowth into lead coils (white arrowheads).
R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx 5
Please cite this article in press as: Rennert RC et al. A histological and mechanical analysis of the cardiac lead–tissue interface: implications for lead extrac-tion. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008

Fig. 4. Analysis of mechanical properties of scar tissue. (A) Depiction of experimental setup for determination of the circumferential mechanical properties of tissue. Thecircumferential stress (rC) was calculated by dividing the load (L) at a given time point by two times the cross-sectional area (2 * A) of the specimens at that given time pointrC ¼ L
2A
� �. Circumferential strain (eC) was defined as the change in circumference/original circumference, and was determined to be the same as the diametric strain
eC ¼ pðDþDDÞ�DDpD ¼ DD
D
� �, where D = the inner tissue ring diameter. (B) Representative images from mechanical analysis depicting a sample pre-load (left image) and beginning
to fail (right image). Failure occurred at approximately the midpoint of all tissue samples (white arrow). (C) Force–displacement curves of samples, illustrating the toe, linearand yield/failure regions. Average circumferential stress is shown in red. (D) Sample cross-sectional areas, fracture loads and calculated circumferential fracture stress/strainand circumferential tissue modulus values. The circumferential tissue modulus was defined as the slope of the circumferential stress vs. circumferential strain curve from thestrain frame of 1.5 to 2, as this initial linear portion was present in all samples.
6 R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx
4. Discussion
In designing this study, we hypothesized that a better charac-terization of the fibrotic response to lead implants could be usedto improve both the design of leads and extraction techniques.The discussion of our findings is therefore focused around thishypothesis.
Overall, the fibrosis-dominated response to lead implants char-acterized herein is consistent with a foreign body reaction to animplanted material. This response is an attempt by the body to iso-late the implant from the local environment, and is typically char-acterized by an acute inflammatory cell infiltrate that progresses toa macrophage-dominated chronic inflammatory phase, and ulti-mately results in fibrotic capsule formation following fibroblastrecruitment and proliferation [24,25].
The foreign body response is not fixed, however, as the relativelevel of fibrosis and inflammation within reactive tissue can beinfluenced by both surface characteristics of the implant, as wellas the cellular composition of affected tissue [25]. For example, im-plants with high surface-to-volume exteriors can promote an in-creased macrophage response characterized by the formation offoreign body giant cells at the implant surface, which can ulti-mately contribute to device failure from persistent oxidative stress[24,25]. Exerting a similar modulatory influence, permanent andstable cell types (e.g. cardiomyocytes and endothelial cells) arethought to have an increased propensity for fibrosis following
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
foreign body insult, compared to the more regenerative responseof cell populations with a higher replicative capacity (e.g. epithelialcells) [25]. Interestingly, mechanotransduction pathways can alsoaffect both inflammation and fibrosis [26,27], and are likely con-tributors to the foreign body response in this scenario as the intro-duction of a static implant to the dynamic environment of thecardiovascular system undoubtedly creates mechanical force per-turbations. While the presence of an infection (the reason for re-moval in the majority of leads) may also influence the fibroticresponse, the long-term asymptomatic period of lead functionalityprior to removal, as well as the presence of a similar fibrotic re-sponse in non-infected leads, suggests this is not a main contribu-tor to the formation of fibrosis.
Interpreted in this light, the low cellularity and high collagencontent of the fibrotic tissue in this study is most likely due to boththe low regenerative capacity of the cell types in contact with thecardiac implants and advancements in implantable material designspecifically made to limit their resulting macrophage response[24,25,28]. While these findings are largely consistent with theevolving definition of biocompatibility as it relates to long termimplantable devices, namely the ability to perform a desired func-tion without eliciting an undesired local or systemic effect [29], thepotential for fibrosis-related mitigation of electrical impulses atthe lead tip, a focal point for adhesions in this study, remains a con-cern. In fact, the dynamic nature of this response is illustrated bythe eventual formation of a smooth surfaced capsule at the
l analysis of the cardiac lead–tissue interface: implications for lead extrac-

R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx 7
implant–tissue interface seen with SEM, as well as the remodelingof collagen fibers suggested by immunohistochemical and picrosi-rius red staining, which is similar to that observed in injured skinand myocardium [12].
Some level of fibrosis is nonetheless desirable to maintain leadstability following implantation. However, given the strikinglyhigh coefficients of friction encountered during specimen collec-tion, we hypothesized that either tissue ingrowth occurred alongthe length of the lead, or contractile forces must be present, suchas those known to occur in injured skin and cardiac tissue as a re-sult of myofibroblast infiltration and organization [16,30,31]. Inlight of the absence of macro- or microscopic tissue ingrowth alongthe lead bodies, we reasoned that the main force resisting extrac-tion was generated as part of the normal fibrotic response to an im-plant, potentially exacerbated by the robust mechanicalstimulation of the intravascular environment.
It was therefore not surprising that approximately half of allnucleated cells in the lead–tissue samples were positive for themyofibroblast marker a-SMA, with many of these cells displayingcytoplasmic extensions consistent with the exertion of circumfer-ential contractile forces. Although myofibroblasts display variabil-ity in cytoskeletal patterning that make their definitiveimmunohistochemical identification challenging [32], theobserved a-SMA(+)/vimentin(+)/desmin(�) profile is consistentwith previous descriptions of myofibroblasts within pathologicfibrovascular and myocardial tissues [16,17]. Moreover, the colla-gen-rich and relatively acellular nature of the tissue samples (ascharacterized by histology and electron microscopy) makes thepresence of other potentially similarly staining cell types, such asvascular smooth muscle and mature cardiomyocytes, unlikely.
While typically absent in normal tissues [33], myofibroblastsare known to rapidly populate sites of injury in response to pro-inflammatory cytokines [34]. These cells likely originate from res-ident fibroblasts, as well as non-resident cells, such as monocytesand endothelial precursor cells, and following recruitment, providemechanical tension to the remodeling matrix by anchoring andcontracting [34]. Upon completion of normal repair processes,myofibroblasts typically undergo apoptosis [30]; however, theycan persist under certain pathological conditions. Specifically,myofibroblasts have been shown to account for up to 65% of thefibroblast-like cells within hypertrophic scars [18], and more than50% of all cells within the scar tissue of advanced stage fibrotic liv-ers [19]. While not quantified, similarly high levels of myofibro-blasts are also seen within the fibroproliferative clusters ofidiopathic pulmonary fibrosis [20], as well as in the capsular re-sponse to foreign body implants [35]. Interestingly, cardiac tissuealso displays a strong, sustained myofibroblast response followinginjury, with high levels of myofibroblasts organized along stresslines seen decades after ischemic events [16].
The prolonged myofibroblast response observed in this study istherefore not unique, but almost certainly contributes to the highlead–tissue coefficient of friction through the generation of cir-cumferential forces. Most importantly, the identification of a largemyofibroblast response in this setting suggests that a more con-trolled regulation of contractile forces on the implant is possible,especially given recent advancements in our ability to modulatemyofibroblast differentiation [36].
The mechanical analyses performed in this study were designedto provide another dimension to the characterization of collectedtissues. In planning these studies, the most clinically relevantmechanical aspect was determined to be circumferential tensilestrength and failure load, as these properties dictate the ease of ra-dial tissue disruption and ability to separate the surrounding fibro-sis from the implant surface. We therefore calculatedthe circumferential mechanical properties of this tissue utilizingthe experimental setup described in Fig. 4a, ignoring the likely
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
variable elastic properties when stressed in other directions[22,37,38].
Not surprisingly, the collected tissue displayed mechanicalproperties consistent with other biomaterials. The toe, linearand failure regions observed on our stress–strain curves havebeen previously described for other tissue types, including skinand normal cardiac tissue [21,22,37,39]. This triphasic behaviorhas been ascribed largely to the collagen fibers within a giventissue, and corresponds to the sequential progression of collagenuncrimpring, stretching of collagen triple helices or cross-linksbetween helices and ultimately disruption of the fibril structurethat occurs with an increasing load [37,40–43]. While directcomparisons of the failure load and circumferential stress re-ported herein to other tissue types is difficult due to variationsin experimental technique across studies, the validity of ourfindings is supported by reports of comparable failure loads of�4.9 N for normal cardiac tissue [21]. Similarly, our data arewithin the wide range (1–32 MPa) of previously reported tensilestrength values for intact skin [22]. The narrow range of the cir-cumferential tissue modulus is also supportive of the reproduc-ibility of the experimental system, as well as a similarity instiffness across individual samples.
Extrapolating this mechanical data to the complicating natureof lead–tissue adhesions upon extraction, the development ofleads with an expandable exterior, similar to balloon angioplastydevices, could theoretically be used to disrupt the surroundingfibrotic tissue and facilitate safe lead removal. Supporting thefeasibility of this approach, the stress–displacement curves gen-erated herein are likely representative of the maximum tensileproperties of this fibrotic response, as these mechanical analyseswere performed on tissue collected from leads with relativelylong implantation times. Moreover, the forces necessary to pro-duce sub-failure expansile stress within our samples, the deliv-ery of which in situ would allow lead removal with minimialassociated risk of vessel rupture, are achievable with currentangioplasty balloon technology [44]. For rapid clinical transla-tion, this methodology could even be combined with existingextraction techniques to accelerate the lead removal process,as the simultaneous or segmental expansion of a coating balloonon the non-conductive portions of implanted leads would likelybe faster than the progressive tissue disruption of cuttingsheaths along the entire lead length, with this more time-inten-sive process reserved exclusively for conductive portions of thelead that would not be amenable to an exterior coating.
Throughout this study, quantitative correlation of sample prop-erties to clinical data was dictated by the variable amount of tissuecollected per lead. For example, while we believe that maturationof the fibrotic response suggested by the immunohistochemicaland picrosirius red staining is almost certainly associated with anincrease in tensile strength due to the known influence of collagenfibril diameter on the strain response to loading [45], the limitednumber of samples and patient implant times available formechanical testing made a definitive analysis of the effect of timeon fibrotic tissue strength outside the scope of this study. Nonethe-less, the histological and mechanical data presented herein providea novel, clinically relevant characterization of the tissue responseto implants within the cardiovascular system, as well as feasibilitydata for researchers seeking to use mechanical scar disruption forthe improvement of lead extraction techniques.
5. Conclusions
Characterization of the tissue surrounding implanted cardiacpacemaker and ICD leads reveals a mostly low cellularity fibroticresponse, with densely packed collagen fibers organized in a
l analysis of the cardiac lead–tissue interface: implications for lead extrac-

8 R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx
circumferential pattern around the implant. A sustained myofibro-blast response is also present and similarly organized along the cir-cumferential axis, likely providing circumferential contractileforces complicating lead removal. The mechanical properties ofthis tissue are similar to those reported for skin and uninjuredmyocardium, suggesting the possibility of novel, mechanicallybased extraction techniques.
Financial disclosure
The authors have no potential conflicts of interest, affiliations orfinancial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or mate-rials discussed herein.
Acknowledgements
The authors would like to thank Yujin Park for her assistancewith tissue processing and staining, as well as Lydia-Marie Joubertat the Stanford Cell Imaging Facility for her assistance with elec-tron microscopy.
Appendix A. Supplementary data
Supplementary data associated with this article can be found,in the online version, at http://dx.doi.org/10.1016/j.actbio.2014.01.008.
Appendix B. Figures with essential color discrimination
Certain figures in this article, particularly Figures 1, 2, and 4, aredifficult to interpret in black and white. The full color images canbe found in the on-line version, at http://dx.doi.org/10.1016/j.actbio.2014.01.008
References
[1] Kurtz SM, Ochoa JA, Lau E, Shkolnikov Y, Pavri BB, Frisch D, et al. Implantationtrends and patient profiles for pacemakers and implantable cardioverterdefibrillators in the United States: 1993–2006. Pacing Clin Electrophysiol2010;33(6):705–11.
[2] Uslan DZ, Tleyjeh IM, Baddour LM, Friedman PA, Jenkins SM, St Sauver JL, et al.Temporal trends in permanent pacemaker implantation: a population-basedstudy. Am Heart J 2008;155(5):896–903.
[3] Voigt A, Shalaby A, Saba S. Rising rates of cardiac rhythm management deviceinfections in the United States: 1996 through 2003. J Am Coll Cardiol2006;48(3):590–1.
[4] Wilkoff BL, Love CJ, Byrd CL, Bongiorni MG, Carrillo RG, Crossley 3rd GH, et al.Transvenous lead extraction: heart rhythm society expert consensus onfacilities, training, indications, and patient management. Heart Rhythm2009;6(7):1085–104.
[5] Gaca JG, Lima B, Milano CA, Lin SS, Davis RD, Lowe JE, et al. Laser-assistedextraction of pacemaker and defibrillator leads: the role of the cardiac surgeon.Ann Thorac Surg 2009;87(5):1446–50. discussion 1450–1441.
[6] Wilkoff BL, Byrd CL, Love CJ, Hayes DL, Sellers TD, Schaerf R, et al. Pacemakerlead extraction with the laser sheath: results of the pacing lead extraction withthe excimer sheath (PLEXES) trial. J Am Coll Cardiol 1999;33(6):1671–6.
[7] Wazni O, Epstein LM, Carrillo RG, Love C, Adler SW, Riggio DW, et al. Leadextraction in the contemporary setting: the LExICon study: an observationalretrospective study of consecutive laser lead extractions. J Am Coll Cardiol2010;55(6):579–86.
[8] Bracke F, Meijer A, Van Gelder B. Extraction of pacemaker and implantablecardioverter defibrillator leads: patient and lead characteristics in relation tothe requirement of extraction tools. Pacing Clin Electrophysiol2002;25(7):1037–40.
[9] Epstein AE, Kay GN, Plumb VJ, Dailey SM, Anderson PG. Gross and microscopicpathological changes associated with nonthoracotomy implantabledefibrillator leads. Circulation 1998;98(15):1517–24.
[10] Candinas R, Duru F, Schneider J, Luscher TF, Stokes K. Postmortem analysis ofencapsulation around long-term ventricular endocardial pacing leads. MayoClin Proc 1999;74(2):120–5.
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
[11] Biancani P, Hausman M, Weiss RM. Effect of obstruction on ureteralcircumferential force-length relations. Am J Physiol 1982;243(2):F204–210.
[12] Rich L, Whittaker P. Collagen and picrosirius red staining: a polarized lightassesment of fibrillar hue and spatial distribution. Braz J Morphol Sci2005;22(2):97–104.
[13] Dayan D, Hiss Y, Hirshberg A, Bubis JJ, Wolman M. Are the polarization colorsof picrosirius red-stained collagen determined only by the diameter of thefibers? Histochemistry 1989;93(1):27–9.
[14] Williams IF, McCullagh KG, Silver IA. The distribution of types I and III collagenand fibronectin in the healing equine tendon. Connect Tissue Res 1984;12(3–4):211–27.
[15] Sussman C, Bates-Jensen BM. Wound healing physiology: acute and chronic.In: Sussman C, Bates-Jensen BM, editors. Wound care: a collaborative practicemanual. Philadelphia, PA: Lippincott Williams & Wilkins; 2007. p. 21–51.
[16] Willems IE, Havenith MG, De Mey JG, Daemen MJ. The alpha-smooth muscleactin-positive cells in healing human myocardial scars. Am J Pathol1994;145(4):868–75.
[17] Touhami A, Di Pascuale MA, Kawatika T, Del Valle M, Rosa Jr RH, Dubovy S,et al. Characterisation of myofibroblasts in fibrovascular tissues of primary andrecurrent pterygia. Br J Ophthalmol 2005;89(3):269–74.
[18] Nedelec B, Shankowsky H, Scott PG, Ghahary A, Tredget EE. Myofibroblasts andapoptosis in human hypertrophic scars: the effect of interferon-alpha2b.Surgery 2001;130(5):798–808.
[19] Knittel T, Kobold D, Piscaglia F, Saile B, Neubauer K, Mehde M, et al.Localization of liver myofibroblasts and hepatic stellate cells in normal anddiseased rat livers: distinct roles of (myo-)fibroblast subpopulations in hepatictissue repair. Histochem Cell Biol 1999;112(5):387–401.
[20] Kuhn C, McDonald JA. The roles of the myofibroblast in idiopathic pulmonaryfibrosis. Ultrastructural and immunohistochemical features of sites of activeextracellular matrix synthesis. Am J Pathol 1991;138(5):1257–65.
[21] Edwards MB, Draper ER, Hand JW, Taylor KM, Young IR. Mechanical testing ofhuman cardiac tissue: some implications for MRI safety. J Cardiovasc MagnReson 2005;7(5):835–40.
[22] Ni Annaidh A, Bruyere K, Destrade M, Gilchrist MD, Ottenio M.Characterization of the anisotropic mechanical properties of excised humanskin. J Mech Behav Biomed Mater 2012;5(1):139–48.
[23] Augat P, Reeb H, Claes LE. Prediction of fracture load at different skeletal sitesby geometric properties of the cortical shell. J Bone Miner Res1996;11(9):1356–63.
[24] Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials.Semin Immunol 2008;20(2):86–100.
[25] Anderson J. Mechanisms of inflammation and infection with implanteddevices. Semin Immunol 1993;2(3):33S–41S.
[26] Wong VW, Rustad KC, Akaishi S, Sorkin M, Glotzbach JP, Januszyk M, et al.Focal adhesion kinase links mechanical force to skin fibrosis via inflammatorysignaling. Nat Med 2012;18(1):148–52.
[27] Wong VW, Paterno J, Sorkin M, Glotzbach JP, Levi K, Januszyk M, et al.Mechanical force prolongs acute inflammation via T-cell-dependent pathwaysduring scar formation. FASEB J 2011;25(12):4498–510.
[28] Kao WJ, Zhao QH, Hiltner A, Anderson JM. Theoretical analysis of in vivomacrophage adhesion and foreign body giant cell formation onpolydimethylsiloxane, low density polyethylene, and polyetherurethanes. JBiomed Mater Res 1994;28(1):73–9.
[29] Williams DF. On the mechanisms of biocompatibility. Biomaterials2008;29(20):2941–53.
[30] Darby I, Skalli O, Gabbiani G. Alpha-smooth muscle actin is transientlyexpressed by myofibroblasts during experimental wound healing. Lab Invest1990;63(1):21–9.
[31] Kapoor M, Liu S, Huh K, Parapuram S, Kennedy L, Leask A. Connective tissuegrowth factor promoter activity in normal and wounded skin. Fibrogen TissueRepair 2008;1(1):3.
[32] Skalli O, Schurch W, Seemayer T, Lagace R, Montandon D, Pittet B, et al.Myofibroblasts from diverse pathologic settings are heterogeneous in theircontent of actin isoforms and intermediate filament proteins. Lab Invest1989;60(2):275–85.
[33] Eyden B. The myofibroblast: a study of normal, reactive and neoplastic tissues,with an emphasis on ultrastructure. Part 1. Normal and reactive cells. JSubmicrosc Cytol Pathol 2005;37(2):109–204.
[34] Porter KE, Turner NA. Cardiac fibroblasts: at the heart of myocardialremodeling. Pharmacol Ther 2009;123(2):255–78.
[35] Hwang K, Sim HB, Huan F, Kim DJ. Myofibroblasts and capsular tissue tensionin breast capsular contracture. Aesthetic Plast Surg 2010;34(6):716–21.
[36] Webber J, Jenkins RH, Meran S, Phillips A, Steadman R. Modulation ofTGFbeta1-dependent myofibroblast differentiation by hyaluronan. Am J Pathol2009;175(1):148–60.
[37] Lanir Y, Fung YC. Two-dimensional mechanical properties of rabbit skin II.Experimental results. J Biomech 1974;7(2):171–82.
[38] Gibson T, Stark H, Evans JH. Directional variation in extensibility of humanskin in vivo. J Biomech 1969;2(2):201–4.
[39] Tong P, Fung YC. The stress–strain relationship for the skin. J Biomech1976;9(10):649–57.
[40] Roeder BA, Kokini K, Sturgis JE, Robinson JP, Voytik-Harbin SL. Tensilemechanical properties of three-dimensional type I collagen extracellularmatrices with varied microstructure. J Biomech Eng 2002;124(2):214–22.
l analysis of the cardiac lead–tissue interface: implications for lead extrac-

R.C. Rennert et al. / Acta Biomaterialia xxx (2014) xxx–xxx 9
[41] Diamant J, Keller A, Baer E, Litt M, Arridge RG. Collagen; ultrastructure and itsrelation to mechanical properties as a function of ageing. Proc R Soc Lond BBiol Sci 1972;180(60):293–315.
[42] Folkhard WE, Mosler E, Geerken E, Knorzer E, Nemetschek-Gonsler H,Nemetschek T, et al. Quantitative analysis of the molecular slidingmechanism in native tendon collagen—time-resolved dynamic studies usingsynchrotron radiation. Int J Biol Macromol. 1986;9:169–75.
[43] White WL, Brody GS, Glaser AA, Marangoni RD, Beckwith TG, Must JS, et al.Tensiometric studies of unwounded and wounded skin: results using astandardized testing method. Ann Surg 1971;173(1):19–25.
Please cite this article in press as: Rennert RC et al. A histological and mechanication. Acta Biomater (2014), http://dx.doi.org/10.1016/j.actbio.2014.01.008
[44] Capelli C, Nordmeyer J, Schievano S, Lurz P, Khambadkone S, Lattanzio S, et al.How do angioplasty balloons work: a computational study on balloonexpansion forces. EuroIntervention 2010;6(5):638–42.
[45] Roeder BA, Kokini K, Voytik-Harbin SL. Fibril microstructure affects straintransmission within collagen extracellular matrices. J Biomech Eng2009;131(3):031004.
l analysis of the cardiac lead–tissue interface: implications for lead extrac-





























