-
8/8/2019 A Framework for Discovering KM Forces
1/8Electronic copy available at:
http://ssrn.com/abstract=983309
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
A Framework for Discovering KM Forces: The Fifth Element
Khalid SamaraLondon South Bank University
Business, Computing and Information Management
Abstract
This paper is an ongoing research in the area of knowledge
management (KM) and evidence-based practice (EBP).
This study reveals that when health care organisations in the UK
initiate a KM initiative, their success has been
limited by undervaluing the importance of tacit clinical
knowledge (non-codified) in practice to use them in
theirdecision-making. This research advocates that one of the key
failures of evidence-based health care has been
instigated by clinicians who usually work not with explicit
codified knowledge (such as guidelines) but directly with
knowledge in practice (tacit-knowledge). This paper focuses on
research evidence, drawing on the work of Nonaka
knowledge creation framework that tacit into explicit knowledge
contributes, as a matter of social interaction.
However, the respective model has not granted high flexibility
to adjust to changing conditions and has not placed
enough clarity neither on evidence based policies or the
requirements to lever the barriers and risks during the
configuration of knowledge creation, which heavily impacts on
knowledge transformation. By helping to explain the
reasoning behind this, I would add that a fifth element is
required onto the SECI model as a force to clarify the
importance of those context, social, cultural and technological
barriers. The extension supports the illumination andstructure
clustering of heterogeneous knowledge sources by determining the
probable forces and barriers that may
influence a KM gap in the organisation.
Keywords: KM, Evidence Based Practice, SECI model, Tacit and
Explicit Knowledge
1. Introduction
Knowledge has both tacit and explicit dimensions such that the
integration of knowledge has an
important social component. Knowledge management (KM) is
commonly associated with knowledge
engineering, which in itself is a field within artificial
intelligence concerned in the advancement of
knowledge-based systems as decision support or expert systems
(Jianqiang et al., 2005 and Olszak M C,
et al., 2006) Most notable problems that current KM systems
contain is the need to improve in handling
heterogeneity and dispersion of knowledge sources, rich and
complex information in facilitating better
knowledge acquisition, codification, generation and transfer of
knowledge (Jianqiang et al., 2005,
Wakefield, 2005, Celina 2006 ) This is also highlighted within
clinical practice as a significant challenge
in how to fuse collective knowledge and experiences into a KM
system on an ongoing basis. This
perspective builds upon and extends the evidence based
decision-making view, as the integration of KM
systems and evidence based has always been inseparable and
directly inclusive to manage clinical
knowledge. The term evidence based is now used widely (Gabbay
and May 2004; Gali N, et al. 2004;
Russel J, et al. 2004; Kawamoto et al., 2005; Gilgun, 2005;
Heneghan 2005) Knowledge creation is
often theory driven conceptual diagrams such as the widely
accepted model of Knowledge transfer based
on the empirical work of Nonakas SECI matrix (1994, 1995) of
knowledge creation. This paper presents
a critic of key empirical aspects of Nonakas SECI model of
knowledge creation. The research advocates
that one of the fundamental achievements of Knowledge creation
is the assimilation and distribution of
EBP. However, the paper argues that the SECI model does not
elaborate the richness required for EBP
nor does it contain the requirements to oversee the barriers and
risks of the formation of knowledge.
-
8/8/2019 A Framework for Discovering KM Forces
2/8Electronic copy available at:
http://ssrn.com/abstract=983309
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
This research advocates that the SECI model should be treated as
a meta-model in the sense that other
models have and can been built from the SECI model. Nonakas
theory of knowledge capturing and
creation is an extension of Michael Polanyi. In Polanyis (1966)
theory of knowledge creation tacit
knowledge remains personalised deep rooted in the individual
even after knowledge develops into
explicit forms (i.e. guidelines) Once again, this may seem to be
a problematic notion and raises the
question of how organisations determine best practice once
knowledge is transformed.
2. Know ledge Management and Evidence Based Health Care
The dynamics of knowledge transfer (KT) and of evidence-based
policy analysis needs to be re-
examined with the current thinking of health care organisations.
Hospitals are large organisations and as
they become larger and more multifaceted what is being studied
also becomes more complex internally
as well as externally, hence the need to examine all segments as
a whole relationship becomes a critical
process. Furthermore, the health care is continually working
towards refining and managing information
overload, and has been extensively examined in various areas of
health; dermatology (Grindlay et al.,
2006), neonatal hearing (Moorjani and Fortnum, 2004), and
nursing (Hsia T L et al., 2006) The
dissemination of information into knowledge (clinical notes,
guidelines) underpins the evaluation of
health needs, together with the development of health strategy
and monitoring of progress. Knowledge
management combines and investigates data for forecasting and
decision-making. Data is no longer
viewed as a collection of names and amounts; value is placed
upon the innovative use and application of
the data as information to become an integral part of a
knowledge domain. KM in the healthcare
generally provides two types of support: diagnoses support and
management support.
KM provides suggestions on how to manage patients condition.
Some of the suggestions may involve
tests that have to be carried out, what medication or treatment
should be considered. However,information is complex, there are
ambiguities, organisational culture, conflicting interest and
uncertainty. For this reason, knowledge creation lies in a
holistic approach bounded by concealed
barriers and as a consequence it becomes necessary to identify
those barriers, which has unequivocally
limited health care organisations to translate their core
knowledge needs into a long term strategic
decision-making process. There are concerns that information
overload is one of the major obstacles
that clinicians have to overcome (Hsia T L et al., 2006) The
resulting information overload and joint with
insufficient information management capabilities appear to be
among the prime causes of important
information being either overlooked or misinterpreted. These
factors; could be contributed by cliniciansthat rely on implicit
information as apposed to EBP where knowledge is codified into
accurate data
through rigorous testing. It is those rigorous guidelines that
lay down the ground rules and disseminates
the fuzzy unstructured sources, in turn providing knowledge that
are requisites for the sharing and
collective knowledge of both the practitioner and patient with
unique preferences, concerns and
expectations. Gabbay and Le May (2004) stresses that the current
core knowledge culture in the health
care is the collectively reinforced, internalised, tacit
guidelines practiced between practitioners within
their domain. This form of knowledge transfer has ultimately
created barriers in clinical knowledge and
increasing heterogeneity and knowledge deficiencies.
-
8/8/2019 A Framework for Discovering KM Forces
3/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
3. Defining Heterogeneous Know ledge Sources
Heterogeneous knowledge sources are the diverse unconnected
knowledge domains that are highly tacit
and virtually inaccessible to other domains dispersed internally
(i.e. secondary, primary care) or
externally (i.e. suppliers), of highly specific nature and
remains virtually inaccessible to users
representing other sections of the same field. The
transformation of tacit knowledge into evidence base
or making evidence base a tacit context is an essential
condition for the creation of new knowledge. It is
essential for the accessibility of newly codified knowledge as
it makes reusability for further knowledge
and increases the likelihood of knowledge durability, for
instance best practice.
4. Nonakas theory of Know ledge Creation
The SECI process and ba together form the dynamic environment
where knowledge can be created and
converted (Nonaka, 1994 and Nonaka; Toyama; Konno 2000)
Knowledge creation consists of three
elements. (1) A knowledge conversion process, SECI (2) Context
knowledge ba (3) Knowledge assets.
All three are needed for knowledge creation. However, knowledge
cannot be created from nothing. A ba
environment forms part of the SECI as a stimulus for the
concentration of the organisation knowledge
and of the individuals who own and create such knowledge
(Nonaka, 2000).
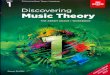
Figure 1. Adapted by Nonaka (1994-1995) SECI model
The following SECI elements in figure 1 are the processes of
knowledge creation.
Socialisation is the world where individuals share feelings,
emotions, experiences and mental model. Externalisation requires
the expression of tacit knowledge and its translation into
comprehensible
forms that can be understood by others. Internalisation of newly
created knowledge is the conversion of explicit knowledge into
the
organisation's tacit knowledge. Combination involves the
conversion of explicit knowledge into more complex sets of
explicit
knowledge. In this stage, the key issues are communication and
diffusion processes and the
systemisation of knowledge.
As one cannot be free from context, social, cultural,
technological forces it would seem plausible at this
stage to identify were the forces that determine the output and
accuracy of that knowledge source.
More importantly the objective of knowledge codification,
generation and transfer is the creation of
evidence based and best practice, which necessitates precision
during codification. In the SECI model
there seems to be no theory about emerging forces that
unequivocally predicts the development of new
knowledge sources.
Socialisation Externalisation
Combination Internalisation
-
8/8/2019 A Framework for Discovering KM Forces
4/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
In the compound of Nonaka (2000) essential assumption of
knowledge creation is the dynamics of
individual and group communication processes. However, the lever
for new and codified knowledge is
fused only when those forces and barriers are constantly sieved
within the knowledge creation process.
As newly created knowledge sources become operational and part
of the knowledge domain there are
existing forces impinging on the evolutionary process of tacit
into explicit sources. Therefore, care
should be taken not to underestimate or underemphasize the
importance of barriers and the internal or
external forces that may intrude on the process of knowledge
creation within an organisation.
Nonakas SECI model describes the requirements of knowledge
creation, but overlooks what may impose
that creation itself. Nonaka attempts to describe the individual
inside a dynamic process when
transforming tacit into explicit knowledge as individuals become
amplified and part of the knowledge
network (Nonaka, 1994,1995) Except the SECI model fails to
represent the fundamental and fluid nature
of forces (risks, barriers) that may interrupt the knowledge
creation process. Such as in the context of
health care were majority of failures with KM systems to a
certain extent has been due to strategic and
organisational structures; those failures have not been
theoretically or empirically examined within the
framework of knowledge management. In the health care knowledge
is mostly ambiguous and messy
hence, a mechanism, for exemplifying the internal and external
forces in knowledge creation is essential.
5. SECI Fifth Element
In figure 2, is an extension of Nonakas SECI model of knowledge
creation. In between the elements I
have added forces as a fifth and primary element as part of the
knowledge creation process. The
extension allows and easily facilitates the fusion of
heterogeneous knowledge sources given that the
forces determine the flow and synthesis of those diverse
knowledge sources. Then ultimately the diverse
and unconnected knowledge domains that are highly tacit become
accessible to other domains withinthe organisation. As forces are
normally constant to return knowledge creation should be viewed as
an
iterative process. The fifth element will determine the
following forces:
Barriers between the individual and the KM systems (i.e.
portals, collaboration tools, ontologys)
Barriers between diverse specialist domains (increasing
accessibility to users representing other
sections of the same field)
Evidence-based health care knowledge must stem from both tacit
knowledge and codified explicit
knowledge Barriers between the individual and learning enabling
environment
-
8/8/2019 A Framework for Discovering KM Forces
5/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
Secondly cluster structure and the diversity of highly complex
knowledge sources must be tamed in
order to support the fusion of heterogeneous knowledge sources
to (1) enable a stable knowledge
learning environment, (2) identify a KM representation or
allocating a KM repository, (3)
increase accessibility between other sections in the
organisation and (4) identify the forces
and obstacles for tacit knowledge.
Wicked/Tame
Figure 2.SECI Fifth Element
5. Knowledge Management Framework
The health care unlike other industries is not prone to indulge
in high competition or forming strategic
alliances or even prone to indulge into high tech innovative
technologies. Unlike the health care majority
of firms are more open to meet the opportunities and threats in
the organisations external and internal
environment and have included KM as part of the firms asset
therefore utilised and nurtured for further
tactical solutions.
It is extensively reported that the health care in the UK are
yet challenging to find ways to improve its
KM strategy as a fundamental part of its clinical manoeuvre
especially when this should be exploited
further to improve the implementation of EBP and to decrease the
heterogeneity among practitioners
(Andre et al., 2002; Gabbay and Le May 2004; McCaughan 2005;
Heneghan 2005) A significant part of
the knowledge exists inside the human mind and the tacit
knowledge plays a large role in the health
care processes and can be made explicit only under particular
conditions. These conditions must be
applied within certain rules and once these rules are functional
we can explore possibilities for KM and
the forces that may impinge upon them.
Socialisation Externalisation
Forces
Internalisation Combination
-
8/8/2019 A Framework for Discovering KM Forces
6/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
It is inevitable as forces and barriers increase the knowledge
gap within the health care also increases.
This is due to a number of reasons one which could be
encountered by dynamic changes and nature of
the industry itself. In figure 3, the KM framework is a generic
conceptualisation of the proposed fifth
element that represents the probable forces and barriers that
may influence a KM gap in the
organisation. The strategic health executive seeking to develop
an edge to enhance KM can use this
model to better understand the context in which the organisation
operates. The framework is meant to
raise questions and facilitate discussion concerning the
strategising facets that may or may not be in
place within an organisation.
Figure 3. Knowledge Management Framework (Fifth Element)
6. KM Representation
The forces of technologies and innovation that determine the
direction of a firm are the same forces that
direct and govern the health care industry because technologies
are rapidly changing forces influencing
the functioning of individual and in turn the organisation.
Information technologies enhance efficiency of
decision-making and has the requisites necessary to identify and
analyse aspects concerning the
leveraging and codification of knowledge as it heavily directs
its focus on the relational aspects of the
user in the product and knowledge development cycle (Williams,
2006) Purposeful information and
knowledge are likely to be tacit sources, and so, the
integration of information technology (IT) becomesalso a pivotal
enabler to the success of KM to turn highly unstructured research
information into
clinical knowledge.
KNOW-HOW
Knowledge domain competence
Expertise, knowledge, skill of KM
Human capital, asset Identify key knowledge
Support towards knowledge communities
KM representation: technologies,knowledge groupware,
ontology,knowledge model technologies
KNOWLEDGE TRANSFER
Data management
Information management
Comprehension of tacit/explicitknowledge
LEARNING & MEMORY
Organisational memory
Individuals memory
Learning organisation
Individual learning
CHANGE
Embrace change
Change to knowledge intensiveorganisation
Change to risk knowledge monitoringorganisation
Change towards a robust evidence basedpractice
-
8/8/2019 A Framework for Discovering KM Forces
7/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
Whilst IT has recreated the concept of KM and plays a major part
in the heightening and alleviation in
the management of heterogeneous knowledge sources, the key KM
challenges facing organisations are
determining what robust KM systems to implement, which user
friendly processes and practices to
institute that are not cumbersome (Chinho Lin et al., 2005) It
is also understandable that the role of IT
in supporting KM initiatives varies for different categories of
organisations (Gosh and Scott, 2005) This
may imply that the knowledge enablers for health care need to
support the KM culture, while capturing
best practices and knowledge from clinical work. Collaborative
technologies structuring through virtual
systems and purposful action make collabrative technologies
particularly appropriate for the context of
KM.
For this reason when developing a system in this area of KM it
maybe necessary to rely on systems for
groupware, which provide generic functions. However, knowledge
groupware, ontology and web based
DSS may not carry much weight if the KM culture as whole does
not maintain the dynamic forces which
shape the direction of the organisation.
7. Conclusion
This paper presented the relationships between the individual
action and KM structure, which needs to
be studied as a shared relationship. Moreover, the ability to
deliver reliable EBP requires the integration
of both explicit research evidence and non-research knowledge
and to determine the forces that impinge
on knowledge creation. The proposed framework helped to identify
an extension yet critical element
adapted from Nonakas SECI model. The extension promotes
awareness of forces and barriers that may
impinge during the knowledge creation process as key performers
within a KMS infrastructure. Also, to
allow the capturing of knowledge without impairing the autonomy
of each domain and heterogeneity
involved a high level unified KM framework to support awareness
for structure clustering and
sustainability of heterogeneous knowledge sources is needed.
This paper advocates that organisations need to constantly
identify KM forces and barriers, as forces are
normally constant to return. These improvements would guide
individuals to transform their knowledge
using technologies and to identify key knowledge to create a
synthesis, integration and collection of
ideas, to discover and relate them to relevant information by
identifying different knowledge sources.
The framework encourages individuals to go through a process of
self-learning and develop an
organisation wide interest in KMS. Furthermore, this research is
an ongoing study in the context of KM
centred on the UK health care. The initial conceptual model
presented in this paper is a generic model
and still in development to be examined specifically surrounding
health care organisations.
-
8/8/2019 A Framework for Discovering KM Forces
8/8
Journal of Knowledge Management Practice, Vol. 8, No. 1, March
2007
References
Andre, M., Borgquist, L., Foldevi, M. & Mlstad, S., 2002,
Asking for rules of thumb: A Way to Discover TacitKnowledge in
General Practice, Family Practice, vol.19, pp.617622
Chinho, L., Jong, M.Y. & Shu, M.T., 2005, Case Study on
Knowledge Management Gaps, Journal of KnowledgeManagement, vol.9
(3), pp.36-50
Ghosh, B. & Scott, J.E., 2005, Comparing Knowledge
Management in Health Care and Technical SupportOrganisations: IEEE
Transactions on Information Technology in Biomedicine, vol.9 (2)
pp.162 - 168
Grindlay, D., Boulos, M.N.K & Williams, H.C., 2006,
Introducing the National Library for Health Skin
ConditionsSpecialist Library, BMC Dermatology, vol.5 (4)
pp.3-11
Gilgun, J.F., 2005, The Four Cornerstones of Evidence Based
Practice in Social Work, Research on Social WorkPractice, vol.15
(1) pp.3-9
Gali, N., Seeger, W., Naeije, R., Simonneau, G. & Rubin,
L.J., 2004, Comparative Analysis of Clinical Trials
andEvidence-Based Treatment Algorithm in Pulmonary Arterial
Hypertension, Journal Of The American College ofCardiology, vol.43
(12), pp.82-88
Gabbay, J., & Le May, A., 2004, Evidence Based Guidelines or
Collectively Constructed Mind Lines: EthnographicStudy of Knowledge
Management in Primary Care, British Medical Journal, vol.329,
pp.1-5
Heneghan, C., 2005, The Doctors Advice and Sleepless Nights:
what can you find in 5 minutes, British Medical
Journal, Evidence-Based Medicine, vol.10, pp.37-38
Hsia, T.L., Lin, L.M., Wu, J.H. & Tsai, H.T., 2006, A
Framework for Designing a Nursing Knowledge ManagementSystem:
Interdisciplinary Journal of Information, Knowledge and Management,
vol.1, pp.14-22
Jianqiang, L., ORiain, S., OSullivan, D. & Wang Q., 2005, A
Framework of Context Aware Knowledge Management,Digital Enterprise
Research Unit, National Institute of Ireland, Science Foundation
Ireland, pp.1-15
Kawamoto, K., Houlihan, C.A., Balas, E.A. & Lobach, D F.,
2005, Improving Clinical Practice Using Clinical DecisionSupport
Systems, British Medical Journal BMJ, vol.330, pp.1-8
McCaughan, D., 2005, Primary Care Practitioners Based Everyday
Practice on Internalised Tacit Guidelines DerivedThrough Social
Interactions with Trusted Colleagues, British Medical Journal,
vol.8 (3), p.94
Moorjani, P. & Fortnum, H., 2004, Dissemination of
Information to General Practitioners: A Questionnaire Survey,BMC
Family Practice, vol.5 (27) pp.1-3
Nonaka, I., 1994, A Dynamic Theory of Organisational Knowledge
Creation, Organisation Science, vol.5 (1) pp.14-37
Nonaka, I. & Takeuchi, H., 1995, The Knowledge-Creating
Company How Japanese Companies Create theDynamics of Innovation;
Oxford University Press, New York, pp.70-75, 1st Edn
Nonaka, I., Toyama, R. & Nagata, A., 2000, A firm as a
Knowledge Creating Entity: A New Perspective on TheTheory of The
Firm, Industrial and Corporate Change, Oxford University Press,
vol.9 (1) pp.2-20
Nonaka, I., Toyama, R. & Noboru, K., 2000, SECI Ba
Leadership: A Unified Model of Dynamic Knowledge Creation,Elsevier
Science, Long Range Planning, vol.33, (5) pp.6-34
Olszak, M.C. & Ewa, Z., 2006, Business Intelligence Systems
in the Holistic Infrastructure Development
SupportingDecision-Making in Organisations, Interdisciplinary
Journal of Information, Knowledge, and Management, vol.1 pp.1-3
Polanyi, M., 1966, The Tacit Dimension; Garden City, Doubleday
& Company, New York, p.13, 1st Edn
Russell, J., Greenhalgh, T., Boynton, P. & Rigby, M., 2004,
Soft Networks for Bridging the Gap Between Researchand Practice:
Illuminative Evaluation of CHAIN British Medical Journal, vol.328,
pp.2-7
Williams, R., 2006, Narratives of Knowledge and Intelligence:
Beyond the Tacit and Explicit, Journal of knowledgemanagement,
vol.10 (4) pp.81-99
Wakefield, R.L., 2005, Identifying Knowledge Agents in a KM
strategy: The Use of The Structural Influence Index,Information
& Management, vol.42 (7) pp.936-945