Embed Size (px)
Citation preview
Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
644
ORIGINAL ARTICLE
A DESCRIPTION OF THE SIZE AND DISTAL BRANCHING PATTERN OF THE DORSALIS PEDIS ARTERY: A CADAVERIC
STUDY Lané Prigge1,2, Nanette Briers2
1 Department of Anatomy, School of Pathology and Pre-Clinical Sciences, Faculty of Health Sciences, Sefako Makgatho Health Sciences University, Pretoria, South Africa. 2Department of Anatomy, Section of Clinical Anatomy, School of Medicine, Faculty of Health Sciences, University, Pretoria, South Africa.
Correspondence to: L Prigge Department of Anatomy, School of Pathology and Pre-Clinical Sciences, Faculty of Health Sciences, Sefako Makgatho Health Sciences University, PO Box 232 Medunsa 0204, Republic of South Africa. Email: [email protected].
ABSTRACT
Detailed knowledge of the dorsalis pedis artery (DPA) on the dorsum of the foot is required for reconstructive surgery, especially when a dorsalis pedis flap is utilised. The aim of this study was to determine the size and branching pattern of the DPA. Within the anterior tarsal tunnel of 40 cadaveric ankles, the size and branches of the DPA were measured, while the relationship of the branches of the DPA to the inferior extensor retinaculum (IER) was noted. The thickness and the locations of the DPA and its branches provided statistically significant data (p>0.05) that the DPA does not divide into equal diameter branches at the level of the ankle joint. The branching pattern of the DPA can be divided into three categories: 27.5% of the arteries arise proximal to the IER, 62.5% of the branches deep to the IER and 10% of the terminal branches distal to the IER. The measurements and locations of the branches noted should assist and inform surgeons of variations during vascular and reconstructive surgery. Key words: Neurovascular anatomy; reconstructive surgery; bifurcation; foot dorsum; inferior extensor retinaculum
INTRODUCTION
The anterior tibial artery extends distally as the dorsalis pedis artery (DPA), at the lower end of the tibia, midway between the malleoli (Sinnatamby, 2011). The DPA passes deep to the inferior extensor retinaculum (IER) and is responsible for the majority of arterial blood supply to the dorsum of the foot (Moore and Dalley, 2006). The DPA gives rise to a lateral tarsal artery and two- to three medial tarsal arteries. It then travels to the proximal end of the first intermetatarsal space, where it turns to the sole of the foot to form part the plantar arch (Standring, 2008). The pulse of the DPA can be palpated lateral to the tendon of the
extensor hallucis longus, where it is located next to the deep fibular nerve, between the tendons of the extensor hallucis longus and the tendons of the extensor digitorum longus (Sinnatamby, 2011).
In a case report by Kim and colleagues (2011), a first web space free flap was used to reconstruct both the upper and lower eyelid defects of a patient. The first dorsal metatarsal artery, a branch of the dorsalis pedis artery, was used to form an anastomosis with the frontal branch of the superficial temporal artery. Eo and co-workers
Submitted 29th August 2015, corrected 16th October 2015. Published online 18th February 2016. To cite: Prigge L, Briers N. 2016. A Description of the Size and Distal Branching Pattern of the Dorsalis Pedis Artery: A Cadaveric Study. Anatomy Journal of Africa. 5: 644 – 649.

Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
645
(2006) emphasize the importance of the knowledge and appreciation of the anatomy of the donor sites. They state that this will ensure accurate microsurgical reattachment of the severed blood vessels at the recipient site, which can be achieved by correctly resecting the free flap with the blood vessels.
Some authors describe the termination of the DPA more of a bifurcation rather than a vessel branching into branches (Pomposelli et al., 1995; Allen, 1997). According to Menin (2010), the term “bifurcation” describes an abrupt change in pattern. It then follows that in order for the distal termination of an artery to be considered a bifurcation, it must exhibit a drastic pattern change such as seen in the bifurcation of the common carotid artery, abdominal aorta and common iliac artery. Mooney (2009) describes a bifurcation as a division from a common origin into two equal parts, e.g. the division of a blood vessel into two equal-sized vessels. According to Douglas Harper (2013), the author of the online etymology dictionary, the term “bifid” (originating from the Latin bifidus) means to split into two equal parts. The confusing use of the term “bifurcation” associated with the
dorsalis pedis artery will impact on the knowledge of the anatomy of this area and the approach to surgical procedures on this structure.
During reconstructive flap surgery, the dorsalis pedis flap is widely used for reconstructions pertaining to the orbital area, intra-oral region and hand- and palm reconstructions (Chitra, 2009). The dorsalis pedis artery, as well as the deep fibular nerve, is contained within this flap, emphasizing the importance of both these anatomical structures (Strauch and Vasconez, 1990; Tang and Chen, 1990; Dong et al., 2003; Chitra, 2009).
The aims of this study were to quantitatively measure the size of the DPA and its branches, and to compare the results between the left and right, as well as between sexes. Furthermore, the branching patterns were evaluated in order to determine the correctness of the term “bifurcation” in the description of the branching pattern of the DPA and to shed more light on the varying patterns that may complicate microsurgical reattachment of blood vessels during reconstructive flap surgery.
MATERIALS AND METHODS
Ethical clearance was obtained from the Research Ethics Committee of the Faculty of Health Sciences at the University of Pretoria. According to the South African National Health Act, Act 61 of 2003, all cadavers used in this study were legally obtained and stowed in the Department of Anatomy for research and teaching purposes.
A total of 40 ankles were dissected, which involved the removal of the skin and the deep fascia of the leg, as well as the dorsal fascia of the foot being incised. An incision was made through the IER to expose the anterior tarsal tunnel containing the DPA and its branches on the dorsum of the foot. The branching pattern of the DPA in relation to the IER was noted and documented by making use of digital photographs. The diameter of the DPA and its branches were measured
externally at the level of the IER with a Vernier digital calliper (accuracy of 0.01mm), in order to determine the correctness of the term “bifurcation” in describing the distal termination of the DPA.
The statistics package, SPSS version 8, was used to calculate the frequencies and percentages. The Student t-test was used to quantify differences and to establish statistical significance in the difference in mean size of the DPA between the sexes.
Intra- and inter-observer error was tested using a random sample of 27 ankles. The first and second authors repeated the measurements on the size of the DPA. No significant differences were observed when comparing the intra- and inter-observer errors with the collected data.
Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
646
RESULTS
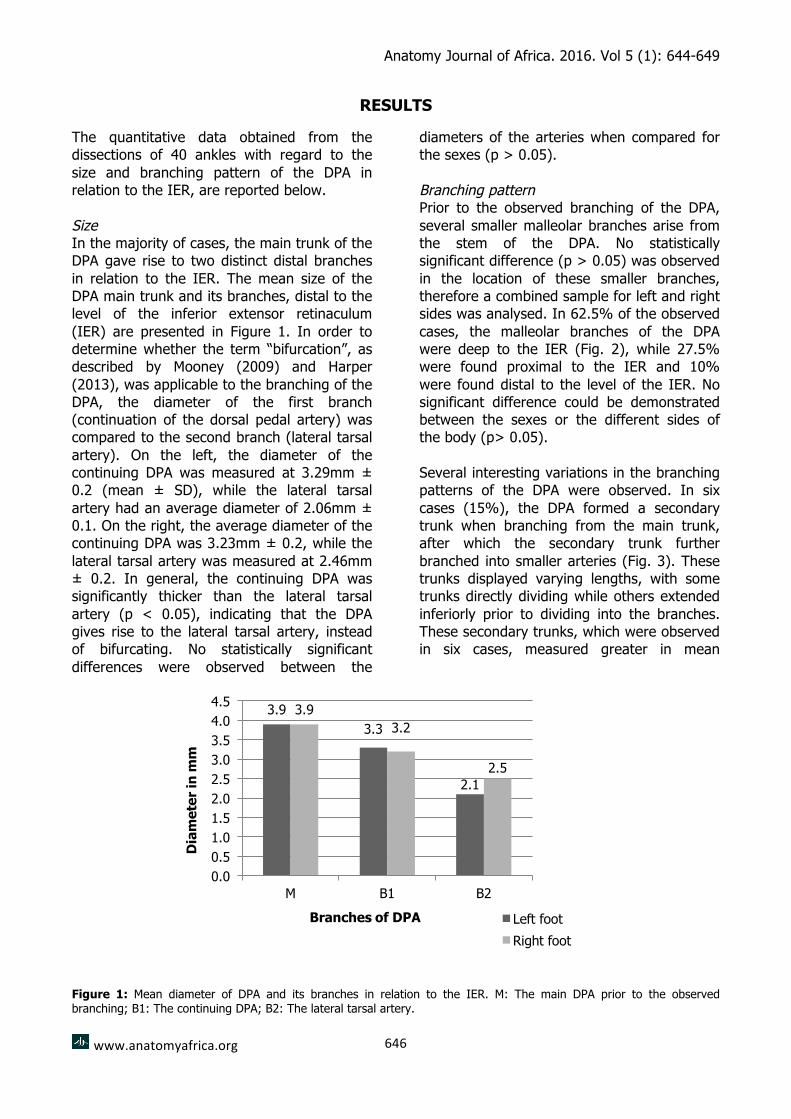
The quantitative data obtained from the dissections of 40 ankles with regard to the size and branching pattern of the DPA in relation to the IER, are reported below. Size In the majority of cases, the main trunk of the DPA gave rise to two distinct distal branches in relation to the IER. The mean size of the DPA main trunk and its branches, distal to the level of the inferior extensor retinaculum (IER) are presented in Figure 1. In order to determine whether the term “bifurcation”, as described by Mooney (2009) and Harper (2013), was applicable to the branching of the DPA, the diameter of the first branch (continuation of the dorsal pedal artery) was compared to the second branch (lateral tarsal artery). On the left, the diameter of the continuing DPA was measured at 3.29mm ± 0.2 (mean ± SD), while the lateral tarsal artery had an average diameter of 2.06mm ± 0.1. On the right, the average diameter of the continuing DPA was 3.23mm ± 0.2, while the lateral tarsal artery was measured at 2.46mm ± 0.2. In general, the continuing DPA was significantly thicker than the lateral tarsal artery (p < 0.05), indicating that the DPA gives rise to the lateral tarsal artery, instead of bifurcating. No statistically significant differences were observed between the
diameters of the arteries when compared for the sexes (p > 0.05). Branching pattern Prior to the observed branching of the DPA, several smaller malleolar branches arise from the stem of the DPA. No statistically significant difference (p > 0.05) was observed in the location of these smaller branches, therefore a combined sample for left and right sides was analysed. In 62.5% of the observed cases, the malleolar branches of the DPA were deep to the IER (Fig. 2), while 27.5% were found proximal to the IER and 10% were found distal to the level of the IER. No significant difference could be demonstrated between the sexes or the different sides of the body (p> 0.05). Several interesting variations in the branching patterns of the DPA were observed. In six cases (15%), the DPA formed a secondary trunk when branching from the main trunk, after which the secondary trunk further branched into smaller arteries (Fig. 3). These trunks displayed varying lengths, with some trunks directly dividing while others extended inferiorly prior to dividing into the branches. These secondary trunks, which were observed in six cases, measured greater in mean
Figure 1: Mean diameter of DPA and its branches in relation to the IER. M: The main DPA prior to the observed branching; B1: The continuing DPA; B2: The lateral tarsal artery.
3.93.3
2.1
3.93.2
2.5
0.00.51.01.52.02.53.03.54.04.5
M B1 B2
Dia
met
er in
mm
Branches of DPA Left footRight foot

Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
647
Figure 2: Branches (arrows) of the DPA, prior to its distal branching, are predominantly located deep to the IER (62.5%).
diameter than the main DPA. In two (5%) of the investigated cases, one of the secondary trunks divided into three dorsal branches (Fig.
4). These branches were identified as muscular, medial and lateral tarsal branches.
DPA
Figure 3: Variation in branching pattern: DPA trunks prior to the tarsal branching
Figure 4: Variation in branching pattern: formed Secondary trunk divides into three branches.
Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
648
DISCUSSION
The viability of the DPA is of special significance for a DPA-bypass that is often used for the treatment of ischemic foot complications (Pomposelli et al., 2003). The authors believe that the size of the DPA plays a vital role in its potential use as an outflow target artery, as explained by Pomposelli and co-workers (2003), as well as in the use of the DPA in arterial cannulation as indicated by Martin et al. (2001). Size For the term “bifurcation” to be used, the arterial diameter should be of equal value indicating that the artery divides into equal sized branches, as stated by Mooney (2009) and Harper (2013). In this study, the external diameter of the distal branches of the DPA did not branch into equal portions, and therefore the term “bifurcation” cannot be used to describe the branching pattern of the artery. This finding is important in the training of undergraduate and postgraduate students, as it is essential to use the proper terminology and to grasp the correct conceptual basis for applied surgical disciplines. Additionally, the terminology also impacts on the surgeon’s understanding of the anatomy underlying reconstructive flap surgery where a flap is usually harvested with its neurovascular supply intact, in order to provide a viable graft. The mean diameter of the branches, indicates that an average difference of 1.23mm was observed in the diameter of the branches on the left foot, while the right foot exhibited an arterial diameter difference of approximately 0.77mm between the respective branches. From these measurements it is evident that both the branches of the artery (the continuing DPA and the lateral tarsal artery) are not of the same diameter, therefore the term “bifurcation” cannot be used. This was further substantiated by a student t-test indicating that the difference in diameters is statistically significant (p < 0.05). Branching pattern
The dorsalis pedis artery is a continuation of the anterior tibial artery, and gives rise to the lateral and medial tarsal arteries, prior to travelling distally on the dorsum of the foot (Standring, 2008). The relation between the IER and malleolar branches, muscular branches, medial and lateral tarsal arteries were noted and categorised. These branches are commonly found in the vicinity of the IER, and may arise proximal (27.5%), deep to (62.5%), or distal (10%) to the IER. When reconstructive surgery of the leg and foot is performed, a free flap is harvested and the neurovascular supply is removed with the tissue flap to ensure adequate neurovascular supply at the recipient area (Strauch and Vasconez, 1990; Tang and Chen, 1990; Dong et al., 2003; Chitra, 2009). Detailed knowledge of these neurovascular structures will limit complications and lead to better results. In conclusion, the term “bifurcation” is an incorrect description for the branching pattern of the DPA in relation to the IER, as used in other research studies (Pomposelli et al., 1995; Allen, 1997). It was found that, based on the statistically significant differences in the arterial diameters, the branching of the lateral tarsal artery from the DPA cannot be considered as a bifurcation. The medial tarsal, malleolar and muscular branches arising from the main trunk of the DPA, are predominantly found underneath or deep to the IER. This research study will assist in future vascular reconstructive surgeries, based on the knowledge of the arterial branches of the DPA.
AUTHOR CONTRIBUTIONS
Both authors of this research paper have directly participated in the planning, conduction and final write-up of this paper. The authors have no conflict of interest to declare.

Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
649
The authors appreciate the valuable input and support of the staff members of the Department of Anatomy, University of
Pretoria, in the revision of the developing manuscript.

Anatomy Journal of Africa. 2016. Vol 5 (1): 644-649
www.anatomyafrica.org
650
REFERENCES 1. Allen BL. 1997. Plantar-advancement skin flap for central ray resections in the foot:
description of a technique. J Pediatr Orthop 17, 785–789. 2. Chitra R. 2009. The relationship between the deep fibular nerve and the dorsalis pedis artery
and its surgical importance. Indian J Plast Surg 42, 18–21. 3. Dong JS, Peng YP, Zhang YX, et al. 2003. Reverse anterior tibial artery flap for
reconstruction of foot donor site. Plast Reconstr Surg 112, 604. 4. Eo S, Kim Y, Kim JY, et al. 2008. The versatility of the dorsalis pedis compound free flap in
hand reconstruction. Ann Plast Surg 61, 157–163. 5. Harper D. 2013. Online etymology dictionary. Obtained on the 5 June 2013 from the website
http://www.etymonline.com/index.php?l=b&p=20. 6. Martin C, Saux P, Papazian L, et al. 2001. Long-term arterial cannulation in ICU patients
using the radial artery or dorsalis pedis artery. Chest 119, 901-906. 7. Menin S. 2010. Complexity and health professions education: a basic glossary. J Eval Clin
Prac 16, 838-840. 8. Mooney J. 2009. Illustrated dictionary of podiatry and foot science. Elsevier Health Sciences. 9. Moore LK, Dalley AF. 2006. Clinically Orientated Anatomy, 5th edition. Lippincott Williams
and Wilkins. pp 587; 642; 667-671. 10. Pomposelli F, Maecaccio E, Gibbons G, et al. 1995. Dorsalis pedis arterial bypass: Durable
limb salvage for foot ischemia in patients with diabetes mellitus. J Vasc Surg 21, 375. 11. Pomposelli FB, Kansal N, Hamdan AL, et al. 2003. A decade of experience with dorsalis pedis
artery bypass: Analysis of outcome in more than 1000 cases. J Vasc Surg 37, 307-315. 12. Sinnatamby CS. 2011. Last’s Anatomy. Regional and applied. 12th edition. Churchill
Livingstone, Elsevier. Chapter 3, Lower limb. pp 145 – 146. 13. Standring, S. 2008. Gray’s Anatomy. The anatomical basis of clinical practice. 40th edition.
Churchill Livingstone, Elsevier. Section 9, chapter 84. pp 1455 – 1456. 14. Strauch B, Vasconez LO. 1990. Grabb’s Encyclopedia of flaps. 1st ed. Boston: Little, Brown.
pp 1797 – 1800. 15. Tang YB, Chen HC. 1990. Dorsalis pedis flap with vascularized nerve graft for simultaneous
reconstruction of palm and digital nerves. Br J Plast Surg. 43:494.


![BRANCHING PROCESS - Cornell Universitypi.math.cornell.edu/~popovic/asymgen_final.pdf2122 L. POPOVIC allow for nonconstant population size [11], this unfortunately requires an a priori](https://img.dokumen.tips/doc/110x75/612595a5289e4b280d34ae75/branching-process-cornell-popovicasymgenfinalpdf-2122-l-popovic-allow-for.jpg)