-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
1/17
This article was downloaded by: [University of Veracruzana]On:
20 August 2015, At: 11:11Publisher: RoutledgeInforma Ltd Registered
in England and Wales Registered Number: 1072954 Registered office:
5 Howick Place,London, SW1P 1WG
Journal of HIV/AIDS & Social ServicesPublication details,
including instructions for authors and subscription
information:
http://www.tandfonline.com/loi/whiv20
A Comparison of Grief Reactions in Cancer, HIV/AIDS,
and Suicide BereavementJames A. Houck PhD
a
a Pastoral Counseling Studies at the Department of Pastoral
and Theological Studies ,
Neumann College , USA
Published online: 04 Oct 2008.
To cite this article: James A. Houck PhD (2007) A
Comparison of Grief Reactions in Cancer, HIV/AIDS, and
SuicideBereavement, Journal of HIV/AIDS & Social Services, 6:3,
97-112, DOI: 10.1300/J187v06n03_07
To link to this article:
http://dx.doi.org/10.1300/J187v06n03_07
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy
of all the information (the “Content”) containedin the publications
on our platform. However, Taylor & Francis, our agents, and our
licensors make norepresentations or warranties whatsoever as to the
accuracy, completeness, or suitability for any purpose of t
Content. Any opinions and views expressed in this publication
are the opinions and views of the authors, andare not the views of
or endorsed by Taylor & Francis. The accuracy of the Content
should not be relied upon ashould be independently verified
with primary sources of information. Taylor and Francis shall not
be liable forany losses, actions, claims, proceedings, demands,
costs, expenses, damages, and other liabilities whatsoeveor
howsoever caused arising directly or indirectly in connection with,
in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private
study purposes. Any substantial or systematicreproduction,
redistribution, reselling, loan, sub-licensing, systematic supply,
or distribution in anyform to anyone is expressly forbidden. Terms
& Conditions of access and use can be found at
http://www.tandfonline.com/page/terms-and-conditions
http://dx.doi.org/10.1300/J187v06n03_07http://www.tandfonline.com/action/showCitFormats?doi=10.1300/J187v06n03_07http://www.tandfonline.com/page/terms-and-conditionshttp://www.tandfonline.com/page/terms-and-conditionshttp://dx.doi.org/10.1300/J187v06n03_07http://www.tandfonline.com/action/showCitFormats?doi=10.1300/J187v06n03_07http://www.tandfonline.com/loi/whiv20
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
2/17
A Comparison of Grief Reactionsin Cancer, HIV/AIDS,
and Suicide Bereavement
James A. Houck, PhD
ABSTRACT. This study compared the grief reactions of people
whomourned three different types of death: Cancer, HIV/AIDS, and
suicide,and addressed the question whether these bereavement groups
can be dif-ferentiated on the basis of their grief, as measured by
the Grief Experi-ence Questionnaire (GEQ; Barrett & Scott,
1989). The results indicatethat these groups (cancer: N = 50,
AIDS-related: N = 50, and suicide:N = 50) had different grief
reactions, specifically, in the areas of stigma-tization andunique
reactions to suicide. The implications of these resultsafford grief
counselors, health-care providers, and pastoral
professionals,intervention strategies that enfranchise people, who
may experience oneof these types of deaths, to work through their
grief. Furthermore, thisunderstanding of specific grief
characteristics can also be assimilated intoa therapist’s preferred
bereavement paradigm, for example, stages of grief
(Kübler-Ross, 1969), phases of
bereavement (Parkes, 1972), or tasks
of mourning (Worden, 2004).
doi:10.1300/J187v06n03_07 [Article copies avail-able for a fee
from The Haworth Document Delivery Service: 1-800-HAWORTH.
E-mail address: Website: © 2007 by The Haworth Press, Inc.
All rights reserved.]
James A. Houck, PhD, is Assistant Professor of Pastoral
Counseling Studies at theDepartment of Pastoral and Theological
Studies, Neumann College.
Address correspondence to: James A. Houck, PhD, Assistant
Professor, Depart-ment of Pastoral and Theological Studies, Neumann
College, One Neumann Drive,Aston, PA 19014 (E-mail:
[email protected]).
The author wishes to express special thanks to his mentors and
colleagues: SharonE. Cheston, EdD, Sr., Suzanne Mayer, PhD, IHM,
and J. Sheppard Jeffreys, EdD.
Journal of HIV/AIDS & Social Services, Vol. 6(3)
2007Available online at http://jhaso.haworthpress.com© 2007 by
Τhe Haworth Press, Inc. All rights reserved.
doi:10.1300/J187v06n03_07 97
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
3/17
KEYWORDS. Cancer, AIDS, suicide, bereavement,
disenfranchisedgrief, Grief Experience Questionnaire, counseling,
and mental health
INTRODUCTION
A common misconception about grief is that it is
one-dimensional, thatis, experienced solelyas an emotional turmoil.
Instead,grief is a multifac-eted experience, causing a disruption
in a person’s physical, emotional,spiritual, social, and
philosophical well-being. Worden (2004) proposesthat the grief
reaction can be categorized into four areas:
1. Feelings: sadness, anger, guilt, anxiety, etc.2.
Physical Sensations: tightness in the chest and throat, lack
of en-ergy, dry mouth, etc.
3. Cognitions: disbelief, confusion, preoccupation, sense
of pres-ence, etc.
4. Behaviors: sleep andappetite disturbances,
socialwithdrawal, etc.
These experiences are considered normal reactions of grief,
whichusually diminish in intensity over time ( Sadock & Sadock,
2003).
Review of Grief Reactions: Normal and
Complicated
Although it is affirmedby many in the field ofmentalhealth
thatgrief
is considered a “normal” reaction to any type of loss, and can
be experi-enced on many different levels, there is, however, a
point when grief isconsidered abnormal.This phenomenon occurswhen
grief andmourningbecome complicated as the level of impairment
escalates to the point of severely limiting the day-to-day
functioning of one who mourns a loss.From a cognitive perspective,
Neimeyer, Prigerson, and Davies (2002)suggest that complicated
grief occurs when a person is unable to assimi-late the loss into
his/her personal life narrative; in other words, “recon-structa
meaningful personal reality” (p.236) by relearning assumptionsabout
the world, roles in the family, etc., challenged by the loss.
Lazare (1979) suggests that abnormal, or pathological, grief
occurswhen one or more of the following symptoms are evident: (1)
when aperson is not able to talk about the deceased without
experiencing a
fresh grief reaction; (2) when minor events trigger an intense
emotionalresponse; (3) when the death of the loved-one is often the
topic of con-versation; (4) when there is a reluctance to remove
the loved one’s
98 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
4/17
possessions; (5) when the survivor reports physical symptoms
similarto those of the deceased; (6) when a survivor has made
radical and sud-den lifestyle changes following the loss; or (7)
when the survivor be-comes preoccupied with the presence of the
deceased.
Catalan (1995) affirms that pathological grief can be
categorized un-der several headings. Absence or delayed
grief is an absence or delay of the manifestations
of numbness and disbelief, separation distress, andsubsequent
features associated with normal grief. Chronic
grief occurswhen the most distressing features of
mourning persist over time, andthe intensity of emotions escalates
as well. For example, although anni-versary reactions to the death
of a loved-one are considered normal,even after many years, a
person still may feel unable to move on with
their lives,or complain about being “stuck” in their grief
(Worden, 2004). Inhibited or distorted grief is
seen in people with an erratic pattern of emotional responses
and thoughts. Complaints of somatic symptoms,anxiety, depression,
or behavioral manifestations such as hostility, dis-placed anger,
and overidentification with the deceased may becomemore prominent
than the usual features of grief.
METHODOLOGY
Grief is universal: A normal, human reaction when a person
experi-ences a loss. Much in the sameway every human being has a
thumbprint,grief is the common denominator in all societies.
However, just as no
two thumbprints are alike,no two people grieve in the same
manner, norshould they be treated the same by grief workers,
therapists, clergy, andother health-care providers. Therefore, I
designed a study to identifyspecific characteristics of grief that
are unique to cancer, HIV/AIDS,and suicide bereavement.
Social workers, grief counselors, and clinical directors
recruited par-ticipants for this study from various hospice and
HIV/AIDS facilities,and suicide support groups. Participants
included members from adultbereavement groups, who have lost a
loved-one most recently to one of three causes of death:
Cancer (N = 50), AIDS-related (N = 50), or sui-cide (N = 50).
Theabove agencies distributedtake-home packets, whichincluded a
letterof appreciationfor their willingness to participate in
thestudy, an informed consent form, a brief demographic
questionnaire,
and the GriefExperience Questionnaire (GEQ; Barrett & Scott,
1989). Inorder to maintain confidentiality, the researcher did not
have any contactwith the participants, but instructed them in the
consent form to mail the
James A. Houck 99
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
5/17
completed packets in a separate addressed and stamped envelope
to theagency that recruited them for the study. The packets were
then col-lected after 1 month of being distributed.
The purpose of this study was twofold. The first purpose was to
deter-mine whether characteristics of group membership could be
determinedbased on grief reactions, as measured by the GEQ (Barrett
& Scott,1989). Although the participants were previously
grouped by the type of loss they had experienced, a
discriminant function analysis (DFA) wasused to identify whether
the cut off scores were appropriate to distinguishgrief reactions
between cancer, HIV/AIDS, and suicide bereavement.The null
hypothesis was that there are nodifferences ingrief reactions
be-tween the groups. Once the null had been rejected, a second
purpose was
to identify which grief variables contributed most to
discriminating be-tween the groups. Permission for this study was
granted by the Institu-tional Review Board of Loyola College in
Baltimore, Maryland.
Instruments
The Grief Experience Questionnaire. The GEQ (Barrett &
Scott,1989) was designed to compare the differences in bereavement
experi-ences of persons who have had a spouse commit suicide versus
personswho had a spouse die anaccidental ornatural death.The
measure consistsof55 items concerning the frequency ofvarious grief
reactions, eachwitha 5-point Likert-response scale of
(1) Never , (2) Rarely, (3) Sometimes,(4)
Often, and (5) Almost always. The wording was changed
from
“spouse” to “loved-one” to include a broader sample of other
types of re-lationships to the deceased. Grief reaction subscales
included multidi-mensional aspects of grief, somatic
reactions, general grief, search for explanation, loss of
social support, stigmatization, sense of guilt, senseof
responsibility, sense of shame, sense of rejection,
self-destructive be-haviors, and unique reactions to suicide,
and have a Cronbach’s Alpharanging from .68 to .97. A copy of the
GEQ can be obtained throughthe Journal of Suicide and
Life-Threatening Behavior (1989) 19, pp.201-215.
RESULTS
Socioeconomic Status
To ensure an equal number in each group, 150 completed
packets(50 per group) were needed for the study. Initially, 350
total packets
100 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
6/17
were distributed which provided a 43% return rate. The
participants in-cluded 105 women (67.9%) and 45 men (32.1%).
Ethnicity in the sam-ple was 10% Hispanic, 43% Caucasian, and 47%
African-American.The range of ages was from 19 to 79 years with a
mean age of 44.65years. Income ranged from $20,000 to $60,000, with
a mean income of $36,000. The education levels for the total
sample were 30.9% com-pleted high school, 51.2% attended college,
and 17.9% attended gradu-ateschool. When comparinganyof
thesocioeconomic demographics tothe grief reactions, no
significance correlation (.30), which could dis-tinguish one
bereavement group from another, was found.
Specific Grief-Related Demographics
Participants were asked to indicate their relationship to the
deceased,how much time had passed since the death of their
loved-one, whetherthey attended support groupsfor their grief,
andtheir current HIVstatus.
Participants’ relationship to the deceased included the
following:24% lost a parent, 21% lost a spouse, 15.4% lost a
sibling, 13.6% lostchildren, 10.5% lost a close friend, 7.4% lost a
life-partner. Another 9%lost an extended family member such as an
uncle or grandparent. At thetime of completing the testing packet,
participants were asked howmuch time had passed since their loved
one’s death. The range for thisquestionwas 3 months to over 5 years
witha meanof24.3 months. Thesespecific grief-related demographics
were evenly distributed throughoutthe three bereavement groups.
A stepwise discriminant analysis identified overall significance
forthe GEQ variables, p < .001 for each of the group
means. This signifi-cance indicates that despite the type of the
death, these groups have sim-ilar grief reactions albeit varying
degrees. For example, out of the 11variables, 2 were identified as
contributing to the discrimination be-tween each of the bereavement
groups, namely unique reactions to
sui-cide and stigmatization, accounting for 88.6 and
11.4% of the variance,respectively. In addition, these
characteristicswere calculated with a com-bined Chi-square=
217.03, p < .000. Even after removal of the
strongestcharacteristic, unique reactions to suicide, there
was still strong associ-ation between the groups and the
predictors, Chi-square = 39.097, p <
.000. Therefore, based on the analysis that the grief reactions
differeddepending on which type of grief participants were
experiencing, thenull hypothesis of no differences between thethree
groupswas rejected.
James A. Houck 101
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
7/17
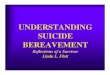
In order to determine to what degree the bereavement groups are
sim-ilar or different, the most significant functions (Unique
Reactions toSuicide and Stigmatization) were analyzed at
the group means for eachtype of death (Table 1). For example, the
variable Unique Reactions toSuicide (Function1)
separatedtheresponses of thesuicide bereavementgroup (1.911) from
those of the cancer (1.829) and AIDS-related(.082) bereavement
groups. Barrett and Scott (1989) assert that a de-fining
characteristic for unique reactions to suicide is attributed to a
sur-vivor concealing the circumstances surrounding the death in
order toavoid the sensitivity of perhaps having the cause of death
broadcast inthe media. The expectation was that the suicide group
would scorehigher in this particular category. In addition,
HIV/AIDS bereavement
may have only slight characteristics similar to suicide
bereavement.Stigmatization (Function 2) separates the responses of
the AIDS-
related bereavement group (.775) from the cancer (.413) and
suicidebereavement (.362) groups. Again, Barrett and Scott (1989)
define stig-matization in bereavement as society having a negative
perception of the survivor as a result of the death of his/her
loved-one. It is not surpris-ing that the HIV/AIDS group scored
highest in this category, becausethe literature spoke of HIV/AIDS
as being a highly stigmatized disease(Burkett, 1995; Shilts, 1988;
Snyder, Omato,& Crain, 1999). Yet, whatis noteworthy is how
similar cancer and suicide bereavement are interms of
stigmatization. Unlike HIV/AIDS bereavement, where it ap-pears that
the stigma is transferred to surviving loved-ones, suicide
andcancer bereavement did not demonstrate this characteristic as
strongly.Perhaps one reason why stigma appears in the cancer group
may berelated to how the person developed the disease (e.g.,
excessive smok-ing, not taking care of oneself, etc.). At one time
society viewed suicideas a highly stigmatized death, however, that
trend seems to be chang-ing. What may be attributing to this lack
of stigmatization currently isthe way society has become more
sympathetic in their understanding
102 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
TABLE 1. Function of Significant Grief Reactions for Each
Group
Type of Death Function 1Unique Reactions
to Suicide
Function 2Stigmatization
Cancer 1.829 .413AIDS .082 .775
Suicide 1.911 .362
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
8/17
regarding the causes of suicide, for example, mental illness,
despair,etc. (Corr, Nabe, & Corr, 2005). In addition, the
growing number of resources and support groups available for
surviving loved-ones of both cancer and suicide bereavement
may further indicate why survi-vors experience less stigmatization
than do survivors in HIV/AIDSbereavement.
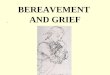
A classification table tests the effectiveness of the
discriminant anal-ysis in distinguishing three bereavement groups
(Table 2). As a statisti-cal tool, the primary purpose of the
discriminant analysis is to classify aset of scores into predefined
groups versus randomly assigning partici-pants. Since this study
started with participants from three self-identi-fied bereavement
groups, the discriminant analysis was used to test
whether their grief reaction scores were indicative of the
characteristicsfor each type of death they were grieving. Prior to
the study, if partici-pants were randomly assigned to one of the
three bereavement groups,there would be a 33.3% chance of
predicting them correctly. However,based on the actual grief
reaction scores, the discriminant analysismatched 82.0% according
to the type of death participants reportedexperiencing. For
example, the cancer bereavement group had a 94%classification rate
with 47/50 cases being classified correctly. The sui-cide
bereavementgroup hadan 86% classification rate with 43/50
casesclassified correctly, whereas the HIV/AIDS group had the
lowest clas-sification rate (66%) with 33/50 cases classified
correctly. This lowerclassification rate for the HIV/AIDS group may
indicate that survivorsshare bereavement characteristics of the
other two groups. As a result,
20% of the HIV/AIDS group may have more in common with
cancerbereavement, that is, traits of a disease model which include
antici-patory grief issues (Rando, 2000). Still, the HIV/AIDS group
(14%)
James A. Houck 103
TABLE 2. Classification Results
Actual Group Membership Based on Scores
Cancern (%)
HIV/AIDSn (%)
Suiciden (%)
Self-identified group membership
Cancer (N = 50) 47 (94) 3 (6) 0 (0)
AIDS (N = 50) 10 (20) 33 (66) 7 (14)
Suicide (N = 50) 3 (6) 4 (8) 43 (86)
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
9/17
may also have some characteristics unique to suicide
bereavement(e.g., concealing the true nature of the death, feeling
the death wassenseless and a waste of life, etc.).
Additional Data
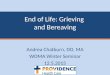
Comparison of Means. When comparing the 11 GEQ variables
meanscores between the three bereavement groups, an obvious
separationbetween the groups occurred (Table 3). For the most part,
the lowestmean scores occurred in the cancer group, with the
HIV/AIDS groupscoring much higher. The highest mean scores of the
three occurredin the suicide group and may be indicative of a more
intensified grief re-action resulting from a sudden and unexpected
death of a loved-one.Furthermore, although cancer and HIV/AIDS are
classified as life-threatening diseases, the level of
stigmatization is significantly lowerin the cancer group than in
the HIV/AIDS group. Yet despite this con-trast, the
variable search for explanation is slightly higher in the
cancergroup mean scores (2.432) than the HIV/AIDS group mean
scores(2.396). Perhaps the higher score in the cancer group may
indicate how,despite research and awareness, many bereft loved-ones
still strugglewith not only the mysteries of the origins of cancer,
but also perhaps therapid spread of this disease within the
body.
104 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
TABLE 3. Comparison of Group Means
Variables Cancer (N = 50) AIDS (N = 50) Suicide (N = 50)
Somatic reactions 2.176 2.442 2.552
General grief reactions 2.056 2.386 2.720
Search for explanation 2.432 2.396 3.412
Loss of support 1.572 2.322 2.932
Stigmatization 1.172 2.305 2.822
Sense of guilt 1.928 2.517 3.116
Sense of responsibility 1.320 1.890 2.560
Sense of shame 1.316 2.241 2.496
Sense of rejection 1.172 2.212 2.816
Self-destructive behavior 1.348 1.940 2.360Unique reactions to
suicide 1.292 1.992 2.828
5-point response scale: (1) Never ,
(2) Rarely , (3) Sometimes ,
(4) Often , and (5) Almost always.
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
10/17
DISCUSSION
Major Contributions
This study examined whether three separate bereavement
groups,cancer, HIV/AIDS, and suicide have their own distinct grief
reactions.Although the discriminant analysis supports three
distinct bereavementgroups, one major contribution of this study
reveals that stigmatizationis significantly higher in HIV/AIDS
bereavement than canceror suicidebereavement, accounting for 11.4%
of the variance.
According to the GEQ (Barrett & Scott,
1989), stigmatization is de-fined as how society looks
upon people and is measured by the follow-
ing questions:
1. Think that people were gossiping about you or the
(deceased)person.
2. Feel like people were probably wondering about what kind of
per-sonal problems you and the (deceased) person had
experienced.
3. Feel like others blamed you for the death.4. Feel like the
death somehow reflected negatively on you or your
family.5. Feel somehow stigmatized by the death.
The role stigmatization plays in discriminating the HIV/AIDS
be-reavement group from the other two groups may be attributed to
society’s
continued discomfort, fear, and intolerance surrounding the
disease. Forexample, in addition to the deceased, the surviving
loved-one also feelssomehow morally depraved and flawed because of
his/her association tothe deceased (e.g., spouse, life-partner,
parent, sibling, caregiver, etc.).
A second contribution of this study involves the differences
betweenthe HIV/AIDS and suicide bereavement groups. Previously
classifiedby Doka (2002), as types of death that result in
disenfranchised grief,the HIV/AIDS and suicide groups were further
differentiated in thisstudy by the GEQ category
of unique reactions to suicide. This “unique-ness”
accounts for 88.6% of the variance and is measured by the
follow-ing questions:
1. Wonderabout your loved-one’s motivation fornot
livinglonger?2. Feel like your loved-one was somehow getting even
with you by
dying?3. Feel that you should have somehow prevented the
death?
James A. Houck 105
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
11/17
4. Tell someone that the cause of death was something different
thanwhat it really was?
5. Feel like the death was a senseless and wasteful loss of
life?
In the past, society may have placed someof the blame for the
suicideon the family members, thus offering less social support
than it wouldfor survivors of a natural death. As a result,
survivors may have feltalienated from their friends and
acquaintances, because of the blame,rejection, and lack of
understanding on the part of society. Calhoun andAllen (1991)
discovered that surviving family members tended to bemore
psychologically disturbed, less trusting, and more blameworthythan
family members grieving nonsuicidal deaths. Therefore, to cope
with the sudden and unexpectedness of the suicide, family
membersmay have refused to discuss the death with friends or
coworkers, or mayhave attempted to recreate events mentally leading
up to the death. Yet,a unique feature this study demonstrated by
the discriminant analysiswas that those who grieve a loved-one’s
death from suicide, may not beexperiencing the same level of
stigma, versus cancer, or HIV/AIDSgrief, as survivors once did
throughout history (Berman & Jobes, 1997;Rubel, 2003). This
change in society’s perception toward those whoseloved-one died
from suicide, may be attributed to a growing under-standing of the
complexities surrounding why people commit suicide,for example,
mental illness, inability to cope with overwhelming cir-cumstances,
etc.
Implications for Mental Health and Health-Care
Providers
Disenfranchised grief poses significant problems for people
whenfaced with the death of a loved-one, but are not afforded the
right, role,or capacity to openly grieve as other members of
society. For mentalhealth and health-care providers, being aware
that such stigma still ex-ists within society is vital to helping
people work through their grief. Infact, this understanding can
also be assimilated into a therapist’s pre-ferred bereavement
paradigm (e.g., stages of grief : Kübler-Ross,
1969; phases of bereavement : Parkes, 1972; or tasks
of mourning: Worden,2004), in order to educate survivors on issues
that might inhibit the pro-cess of mourning.
For example, people who grieve the loss of a loved-one’s death
tocancer, HIV/AIDS, or suicide may often feel neglected and
forgotten.Yet they have specific bereavement needs. One need, in
particular, is tobecome “enfranchised” by the therapist (Corr,
1998). Giving people
106 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
12/17
permission to grieveopenly legitimizes their statusas mourners.
In fact,therapists need to communicate to the surviving loved-one
that soci-ety’s perception of thedeath may notnecessarily reflect
theirownexpe-rience (Rando, 2000).
Quite often bereaved loved-ones are forced to wrestle with
unan-swered questions, withhold their feelings from family members
andfriends, etc., and cover up the nature of the death to avoid
further judg-ment and emotional isolation. In the early years of
HIV/AIDS, the pop-ular phrase “Silence = Death” was used to protest
society’s denial of theepidemic natureof a disease that was
immediately stigmatized (Burkett,1995). In some instances, suicide
maybe particularly troubling to revealin social settings,
especially if thesurviving loved-one is in a position of
public authority (Rubel, 2003). Today, silencing the
disenfranchisedgrievers only further wounds them into possible
social isolation, andplacing them at a far greater risk for
bereavement complications.
Active listening, normalizing feelings, expressing empathy,
educat-ing people on the process of mourning, and providing a safe
environ-ment where thoughts, emotions, feelings, and personal
stories can beshared is a crucial step toward healing one’s grief.
Many clients maybe apprehensive about sharing their stories and
feelings because theymay have never been given permission to talk
about the death before.Although therapists may assume this kind of
permission-giving will beattractive to many, disenfranchised
grievers may be skeptical abouttherapists’ intentions. Too familiar
with “guilt by association” judgments
rendered by society, they may have difficulty accessing the
therapist’sempathy. Therefore, disenfranchised grievers need to be
reassured thatthey not only are viewed by therapists as person’s of
value and worth,but they need to know their loved-one’s memory will
be afforded thesame courtesy.
Intervention Strategies
Rando (2000) states that in working with disenfranchised
grievers,different types of support may be needed not only to
facilitate grief, butalso may be required at different times. Such
resources include:
• Identify the type of support the mourner requires and what
supportis desired, for example, individual verses support
group.
• Work with the mourner to identify unmet needs as
secondarylosses, for example, loss of income, role, etc.
James A. Houck 107
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
13/17
• Deal with the mourner’s feelings about not getting needs for
sup-port and why those needs are not getting met.
• Review the mourner’s expectations for support to determine
whetherthey are appropriate, and help them readjust these if
inappropriate,for example, self-medicating through drugs or
alcohol.
• Assess the lack of support to determine whether it is owing to
alack of assertiveness or other psychological issues.
• Educate the mourner that support for disenfranchised grief
oftencanbe found in support groups and/orprinted material.Refer
themto these sources.
• Educate themourner on unrealistic expectationsor incorrect
infor-mation about the mourner’s needs.
Religious/Spiritual Needs and Support
Pargament, Koenig, and Perez (2000) notes that a grieving
person’sreligion and spirituality have become important issues to
address incounseling. Whether it is existential issues related to
God or the Divine,relationships with others, or finding peace, many
pastoral professionalshelp bereft people understand the
significance of religious/spiritualcoping in their grief. As in any
bereavement setting, listening to a survi-vor’s story, especially
one’s religious/spiritual story is a critical part of the
process of mourning. To this end, Paragament et al. states that
reli-gion/spirituality can function in the following ways:
Preservation: To use religion/spirituality not necessarily to
changebut to survive, or to provide stability in everyday life.
Reconstruction: To use religion/spirituality to rebuild
prior beliefsabout God and the world that may have been challenged
by thedeath of a loved-one.
Re-Valuation: Using religion/spirituality to help people
discovernew sources of significance, e.g., letting go of old
attachments tothe loved-one and discovering new ways to invest
themselves inother people or endeavors.
Re-Creation: Using religion/spirituality as a means of
transform-ing a person’s core significance and his/her approach to
life, e.g.,giving up of avoidant strategies in search for a
closeness with Godand others.
108 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
14/17
By focusing on the grieving person’s specific
religious/spiritual cop-ingmethods, pastoral professionals may be
able to identify the differentways religion/spirituality enhances
or hinders the mourning process. Infact, this awareness will make
it possible to integrate religion/spiritualitymore fully and
effectively in counseling.
Limitations and Future Area of Research
As this study examined the grief reactions, among cancer,
HIV/ AIDS, and suicide bereavement groups, there are several
limitations tothe study, which lends itself to future areas of
research.
Cultural Limitations
This study focused primarily on the grief reactions from a
westerncultural perspective. A future area of research would be to
compare andcontrast the three bereavement groups in other cultures,
for example,African, Asian, Latino, European, Scandinavian, Pacific
Islands, etc.This research would address specific cultural issues
related to bereave-ment that may or may not be similar to the
western culture. In addition,this type of research would be
beneficial particularly in Asia and Africawhere HIV/AIDS is at
epidemic proportions (Stine, 2005). Nonetheless,there are specific
cultural groups within the United States, for example,Asian,
African, etc., that would warrant future research in this area.
Specific Groups within Each Group
The study specifically targeted three types of death (cancer,
HIV/ AIDS, and suicide). However, there are certainly
subgroups within themain groups. For example, it would be worth
studying different types of grief reactions and
religious/spiritual coping between different types
of cancerdeaths. Another example would be to differentiate
between HIV/ AIDS deaths resulting from different modes of
contraction. In otherwords, would the level of stigmatization be
the same or different forloved-ones who contracted HIV/AIDS via an
accidental stick with aninfected needle, sexual contact,
breast-feeding, or sharing needles fromillegal intravenous drug
use, from thegroup at large?Subgroups (differ-
ent methods of suicide) within the larger suicide bereavement
groupmight be another area for future research to measure unique
reactionsto suicide, for example, how survivors react to loved-ones
committing
James A. Houck 109
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
15/17
suicide by gunshot, hanging, pills, setting themselves on fire,
asphyxia-tion, etc.
Other Types of Death
This study was limited to examining grief reactions from three
spe-cific bereavement groups. There are other types of deaths not
includedin this study. Therefore, a future area of research would
be to compareand contrast different types of death including other
disenfranchisedgroups, for example, accidental, drunk driving,
murder, etc. Also, in lightof the recent research on trauma,
comparing specific types of death thatresult in traumatizing
bereaved survivors as defined by Jacobs(1999)or
Rando (2000) would be beneficial to the field.
Longitudinal Studies
This study examined grief reactions among three bereavement
groupswithin the parameters of 3 months to5 years. A future area of
researchwould be to design a longitudinal study among the three
bereavementgroups to measure the differences in intensity of grief
reactions, levelsof resiliency, use of religious/spiritual coping
skills, and sense of disen-franchisement over a 1, 3, 5, and
10-year period of time.
Religious and Spiritual Coping
In recent years, there has been an increasing amount of
attentiongiven to the effects religious and spiritual coping have
on mental health(Pargament et al., 2000; Shafranske, 1997). In
times of grief, manypeople turn to religion and spirituality to
find stability, hope, and mean-ing (Doka & Morgan, 1993).
Therefore, it would be beneficial to thefield of research on
disenfranchised grief to study how these groupscope in terms of
religious/spiritual beliefs and practices.
SUMMARY
This study compared thegrief reactionsof peoplewho mourned
threedifferent types of death:Cancer, HIV/AIDS, and suicide,
andaddressedthequestion whether thethree bereavement groupscanbe
differentiatedon the basis of their grief, as measured by the GEQ
(Barrett & Scott,1989). The results indicated that these groups
had different reactions,
110 JOURNAL OF HIV/AIDS & SOCIAL SERVICES
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
16/17
specifically, in the areas of stigmatization and unique
reactions to sui-cide. Despite over 20 years of HIV/AIDS education
and awareness,stigma still surrounds this disease. In fact, stigma
appears to be trans-ferred to surviving loved-ones in bereavement,
to a greater extent thanin cancerandsuicide. However, survivors of
a loved-one’s suicide morethan likely will purposefully conceal the
circumstances of the deathfrom the media in order to avoid
society’s judgment as distinguishedfrom cancer and HIV/AIDS deaths.
The result is that both the suicideand HIV/AIDS groups may be
forced into a silence regarding grievingtheir losses openly.
Nonetheless, for those who offer grief counseling,providing a safe
and accepting, nonjudgmental environment where thesesurvivors can
tell their story helps facilitate the steps toward healing.
To this end, the field of research within disenfranchised grief
is vastand limitless. Cultural nuances and societal attitudes may
change fre-quently. In fact, what is considered taboo in one
society may be consid-ered normal behavior in the other culture.
However, what does notchange is an ongoing commitment to study of
disenfranchised grief inthe context of social, political,
religious, and economic arenas. Al-though tremendous strides have
been made in the area of education, re-search, and awareness, fear
and public opinion can combine for anoverwhelming way in which
stigma and isolation is fed. Nevertheless,there is hope for
grieving people to be empowered to rise above suchshunning behavior
when practitioners, researchers, policymakers, andclergy become
more aware of the grief and stigma factors these personsface, and
when thought is given to the types of supports those
grievingpersons need at that time.
REFERENCES
Barret, T. W. & Scott, T. B. (1989). Development of thegrief
experience questionnaire(GEQ). The Journal of Suicide and
Life-Threatening Behavior, 19, 201-215.
Berman, A. & Jobes, D. (1997). Adolescent suicide
assessment and intervention.Washington, DC: American Psychological
Association.
Burkett, E. (1995). The gravest show on earth: America in
the age of AIDS . Boston,MA: Houghton Mifflin.
Calhoun, L. G. & Allen, B. G. (1991). Social reactions to
the survivors of suicide in the
family: A review of the literature. Omega, 23(2),
95-97.Catalan, J. (1995). Psychiatric problems associated with
grief. In L. Sherr (Ed.), Grief and AIDS .
Chichester, UK: Wiley Press.
Corr, C. (1998). Enhancing the concept of disenfranchised
grief. Omega, 38, 1-20.
James A. Houck 111
-
8/19/2019 A Comparisson of Grief Reactions in Cancer HIV and
Suicide Bereavement
17/17
Corr, C., Nabe, C., & Corr, D. (2005). Death and dying, life
and living (5th ed.).Belmont, CA: Wadsworth Publishing.
Doka, K. (Ed.). (2002). Disenfranchised grief: New
directions, challenges, and strate-gies for practice. Champaign,
IL: Research Press.
Doka,K. & Morgan,J. (Eds.). (1993). Death and
spirituality. Amityville, NY:BaywoodPublishing Company, Inc.
Jacobs, S. (1999). Traumatic grief: Diagnosis, treatment,
and prevention. Philadelphia,PA: Taylor and Francis.
Sadock, B. J. & Sadock, V. A. (2003). Kaplan and Sadock’s
synopsis of psychiatry:Behavioral sciences/clinical psychiatry, 9th
edition. Baltimore, MD: LippincottWilliams & Wilkins.
Kübler-Ross, E. (1969). On death and dying. New York:
Macmillan.Lazare, A. (1979). Unresolved grief. In A. Lazare
(Ed.), Outpatient psychiatry: Diag-
nosis and treatment (pp. 498-512). Baltimore, MD:
Williams and Wilkins.
Paragament, K. I., Koenig, H. G., & Perez, L. (2000). The
many methods of religiouscoping: Development and initial validation
of the RCOPE. Journal of Clinical Psy-chology, 56 ,
519-543.
Parkes, C. M. (1972). Bereavement: Studies of grief in
adult life. New York: Interna-tional Universities Press,
Inc.
Rando, T. (2000). Clinical dimensions of anticipatory
mourning: Theory and practicein working with the dying, their loved
ones, and their caregivers. Champaign, IL:Research Press.
Rubel,B. (2003). Thegrief response experienced by thesurvivorsof
suicide. Retrievedon November 6, 2002, from
www.griefworkcenter.com.
Shafranske, E. P. (1997). Religion and the clinical
practice of psychology. Washington,DC: American Psychological
Association.
Shilts, R. (1988). And the band played on. New York:
Penguin Books.Snyder, M.,Omoto, A. M., & Crain, A. (1999).
Punished for their good deeds:Stigma-
tization of AIDS volunteers. American Behavioral Scientist,
42, 1175-1192.Worden, J. W. (2004). Grief counseling and grief
therapy: A handbook for the mental
health practitioner (3rd ed.). New York: Springer
Publishing Company.
doi:10.1300/J187v06n03_07
112 JOURNAL OF HIV/AIDS & SOCIAL SERVICES