Embed Size (px)
Citation preview


Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 270
Address for correspondence: Asst Prof. Somayyeh Dehghan, Department of Endodontic, Faculty of Dentistry, Qom University of Medical Sciences, Shahid Lavasani St, Qom, Iran. E-mail: [email protected]
A comparison of canal preparations by Mtwo and RaCe rotary files using full sequence versus one rotary file techniques; a cone-beam computed tomography analysis
Mohsen Aminsobhani1,3,4, Abdollah Ghorbanzadeh3,4, Somayyeh Dehghan3,5, Allahyar Nezadi Niasar2,6, Mohammad Javad Kharazifard7
1Department of Endodontics, 2Department of Radiology, Dental School, AJA University of Medical Sciences, 3Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, 4Department of Endodontics, Tehran University of Medical Sciences, Tehran, 5Qom University of Medical Sciences, Qom, 6Department of Radiology, 7Epidemiologic Department, Dental Research Center, Dental School, Tehran University of Medical Sciences, Tehran, Iran
INTRODUCTION
Cleaning and shaping are essential steps in root canal treatment procedures for removing
debris and microorganisms that are responsible for endodontic pathosis.[1,2] Since the introduction of nickel-titanium (NiTi) rotary instruments, it has
ABSTRACTObjectives: Using one rotary fi le can result in a faster canal preparation. This can be done with several fi le systems and endodontic motors. In the present study, a newly single fi le technique (one rotary fi le technique) with available rotary fi le systems is introduced. The aim of the present study was to evaluate centering ability and remaining dentin thickness of 2 rotary nickel-titanium systems (Mtwo versus RaCe) and instrumentation techniques (conventional versus one rotary fi le) by cone-beam computed tomography. Materials and Methods: A total of 76 mandibular molar teeth were selected and divided to 4 groups (n = 19 teeth with 57 canals). The teeth were mounted in resin and pre-instrumentation scans were prepared by Cone Beam Computed Tomography (CBCT). The canals instrumented with Mtwo and RaCe rotary fi les either in conventional or one rotary fi le technique (ORF). After cleaning and shaping of distal and mesial canals, post instrumentation scans were performed by CBCT in the same position as pre instrumentation scans. Centering ability and remaining dentin thickness were evaluated by Planmeca Romexis viewer. The data were analyzed with analysis of variance and post hoc t test (P < 0.05). Results: Mean centering ratios for Mtwo/conventional, Mtwo/ORF, RaCe/conventional and RaCe/ORF groups were assessed. At overall, there were no signifi cant differences between instrument types and instrumentation techniques (P > 0.05). However, in a few cross-sections, conventional technique and/or RaCe showed higher centering ability. One rotary fi le technique with either RaCe or Mtwo was signifi cantly faster than conventional technique (P = 0.02). There was no signifi cant difference among groups regarding fi le fracture. Mesiolingual canals showed more transportation compared with mesiobuccal and distal canals. Conclusions: Both of the instrumentation systems and techniques produced canal preparations with adequate centering ratio. One rotary fi le technique prepared canal signifi cantly faster than conventional technique.
Key words:
Centering ability, Cone beam computed tomography, Mtwo, one fi le technique, RaCe, root canal preparation
Access this article onlineQuick Response Code:
Website:
www.saudiendodj.com
DOI:
10.4103/1658-5984.132722
Ori
gina
lri
gina
l A
rtic
lert
icle

Aminsobhani, et al.: Centering ability of one rotary fi le technique
71Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
been shown that several NiTi fi le systems can maintain original canal shape, reduce procedural errors and prepare the canal faster.[3,4]
RaCe (FKG, La Chaux-de-Fonds, Switzerland) rotary endodontic instruments have triangular cross sections except for #15/.02 and #20/.02 instruments.[5] The fi le has alternating cutting edges; this design reduces fi le threading into the canal wall.[6] The instrument surface has been electro polished.[7]
Mtwo (VDW, Antaeus, Munich, Germany) instruments have an S-shaped cross-sectional design and a positive rake angle with 2 cutting edges.[8] Moreover, Mtwo instruments have an increasing pitch length from the tip to the shaft. This design has two advantages: 1- eliminates threading into canal walls 2- reduces debris extrusion beyond apex.[9] Mtwo preparations were well-centered in curved canals, even without a manual glide path before rotary instrumentation.[10]
According to the manufacturers, crown-down and standard preparation techniques are suggested for RaCe and Mtwo systems, respectively. The recently introduced NiTi fi les such as Reciproc and WaveOne are claimed to be able to completely prepare and clean root canals with only one instrument. These fi les are used in a reciprocal motion and need special devices and motors.[11,12] One Shape® is another new NiTi file with three different cross-sections along the file length. It works in continuous rotation motion with no need to special motors.[13] In the present study, one rotary fi le technique of instrumentation was suggested. Using a single file of available rotary file systems is proposed in this technique. Reduced working time, less cost, no need to new special motors and a previously experienced sense during canal preparation are some advantages of this technique.
Different methods such as serial sectioning, simulated canals and radiographic analysis have been used for evaluating centering ability of different systems. Since cone-beam computed tomography (CBCT) is more accessible and precise for three dimensional evaluation without destructing the teeth, we used CBCT for evaluating centering ability.[14] The aim of the present study was to evaluate centering ability and remaining dentin thickness in root canals prepared by two rotary nickel-titanium systems (Mtwo versus RaCe) and two canal preparation methods (conventional versus only one rotary fi le) by cone-beam computed tomography.
MATERIALS AND METHODS
Sample preparationSeventy six extracted human fi rst and second mandibular molars that were extracted because of periodontal problems were selected. Teeth were disinfected in sodium hypochlorite 5.25% for 30 min and then maintained in normal saline solution until use.[15] Straight radiographs in mesiodistal and buccolingual directions were taken to determine the root canal anatomy. The teeth with mature apices, no resorption, without restoration, no cracks and distinct mesial and distal roots with curvature within 15 to 45◦ limit were selected. Canal curvature was determined by using Schneider method.[16] Teeth with multiple, rapid apical curvature, or calcifi ed canals were excluded from the study. Specimens were coded and randomly divided into 4 groups (n = 19). The apical foramina were sealed with dental wax and all teeth were then mounted in acrylic resin blocks of 10 cm diameter (19 teeth in each resin block and collectively 76 teeth in four resin blocks). Pre instrumentation images were taken by CBCT machine Alphard VEGA, Asahi Roentgen Ind., Kyoto, Japan) with following settings: 80 kV, 4 mA, 51 × 51 mm fi eld of view and 0.1/voxel (mm) size. Access cavities were prepared by using diamond burs and apical patency was checked with stainless steel #10 K-fi le (Dentsply Maillefer, Ballaigues, Switzerland). Each resin block was divided to 4 rows by a dental saw so that we could determine working length by radiography. The working length was established with #15 K-fi le that was 1mm shorter than radiographic apex. The experimental groups were as following:
Group 1 (Mtwo, conventional): The canals were prepared by single-length technique as recommended by the manufacturer using Mtwo Ni-Ti rotary fi les in torque-limited electric motors (Dentaport ZX, Morita corp., USA) at 2 N/cm torque and 300 rpm. Four fi les were used in the following sequence: 10/.04, 15/.05, 20/.06 and 25/.06. Each fi le was removed when rotated freely at the end of the canal.
Group 2 (Mtwo, ORF): The canals were prepared with only one Mtwo #25/0.06 fi le. The values of torque and rpm were the same as in group 1. After preparation by #10 and #15 stainless steel K-fi les, the coronal and middle thirds of the canal were prepared by a #25/.06 Mtwo fi le with active lateral force in an anticurvature in-and-out motion until the file reached the working length. If the fi le did not reach the working length, the preparation was continued using #15 and #20 K-fi les

Aminsobhani, et al.: Centering ability of one rotary fi le technique
72 Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
in a watch winding movement and then #25/.06 Mtwo fi le was used until rotated freely at the apex.
Group 3 (RaCe, conventional): Distal and mesial canals were prepared by using RaCe NiTi rotary fi les. Instrumentation was carried out with a crown-down technique starting with the 40/.10 instrument at 600 rpm and 2 N/cm torque as suggested by the manufacturers, followed by 35/.08, 25/.06, 25/.04 and 25/.02 if necessary. Then canals were instrumented to working length with 25/.04 and 25/.06.
Group 4 (RaCe, ORF): For each tooth, instrumentation was carried out with only #25/.06 RaCe fi le at 600 rpm and 2 N/cm torque. Instrumentation technique was the same as in group 2.
In all experimental groups, as each instrument was changed, the canal was irrigated with 1 mL of 2.5% NaOCl by using a 30-gauge needle (Max-i-Probe; Dentsply, Rinn, Elgin, IL) and then recapitulated with a #15 K-fi le. After canal preparation, smear layer was removed by 3 ml of 17% EDTA. 1.3% NaOCl was used for final irrigation accompanying with Passive ultrasonic agitation. Preparation time was measured separately for distal and mesial canals to compare different systems and techniques. The preparation time included active instrumentation as well as the time required for changing instruments, cleaning the flutes of the instruments and irrigation. The number of fractured and permanently deformed instruments during preparation was also recorded. If there was any fi le fracture, another tooth was replaced for preparation. After canal shaping, post instrumentation CBCT scans were performed with similar values and position as pre instrumentation scans.
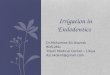
Evaluation of centering ability and remaining dentin thicknessCBCT images were analyzed by Planmeca Romexis viewer software (Version 2.3.1.R, Finland). Dentin thickness and centering ability was measured in 4 planes as shown in Figure 1: At furca, 3 mm apical to furca (coronal), 6 mm apical to furca (middle) and 3 mm coronal to the apex (apical). In each plane, dentin thickness of buccal, lingual, mesial and distal walls were measured in pre and post instrumentation CBCT scans [Figure 2]. The measurements were recorded for each canal (mesiobuccal, mesiolingual and distal) separately. The following formula was used
Figure 1: CBCT images were analyzed by Planmeca Romexis viewer software before and after instrumentation in 3 mm-thick sections: a- furcal, b- coronal, c- middle, d- apical
d
c
b
a
Figure 2: In each canal, dentin thickness of buccal, lingual, mesial and distal walls was measured in pre and post instrumentation CBCT scans

Aminsobhani, et al.: Centering ability of one rotary fi le technique
73Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
for the centering ability calculation in mesiodistal dimension: [(E1-E2)-(I1-I2)]/YMD. E1 and E2 represented the shortest distance from the external surface of each root to the periphery of the uninstrumented and instrumented canals, respectively. I1 and I2 represented the shortest distance from the internal surface of each root to the periphery of the uninstrumented and instrumented canals, respectively. YMD was the diameter of final canal preparation in mesiodistal direction. A result of zero indicated no canal transportation. A negative result indicated transportation toward the furcation region and a positive result indicated transportation away from the furcation region. The following formula was used for the centering ability calculation in buccolingual dimension: [(B1-B2)-(L1-L2)]/YBL. B1 and B2 represented the shortest distance from the buccal surface of each root to the periphery of the uninstrumented and instrumented canals, respectively. L1 and L2 represented the shortest distance from the lingual surface of each root to the periphery of the uninstrumented and instrumented canals, respectively. YBL was the diameter of final canal preparation in buccolingual direction. A result of zero indicated no canal transportation.
A negative result indicated transportation toward lingual and a positive result indicated transportation toward buccal.
The data for centering ability were statistically analyzed by using analysis of variance with a post hoc t test and the level of signifi cance was P < 0.05.
RESULTS
Centering ratio values of different sections in mesiodistal (MD) and buccolingual (BL) directions are listed in Tables 1 and 2. At overall, all instruments and techniques had low centering ratio with no signifi cant difference except in few sections.
In distal canal (only in MD direction), centering ratio values in RaCe system were signifi cantly lower than Mtwo in the apical thirds ( P = 0.03). Also, centering ratio values in the conventional technique were significantly lower than one rotary fi le technique (P < 0.001).
In mesiobuccal canal (only in MD direction), conventional technique showed significantly lower
Table 2: Mean centering ratio values of different sections of canals and SD in buccolingual directionGroups Mean centering ratio (SD)
MB canal ML canal Distal canalFurca Coronal Middle Apical Furca Coronal Middle Apical Furca Coronal Middle Apical
Mtwo/conv 0.250a
(0.171)−0.070b
(0.125)−0.028b
(0.166)−0.026b
(0.119)−0.188a
(0.156)0.061b
(0.107)0.067b
(0.141)0.068b
(0.133)0.021b
(0.100)0.002b
(0.050)0.024b
(0.118)0.004b
(0.094)Mtwo/ORF 0.197
(0.194)−0.039(0.182)
0.000(0.132)
0.036(0.106)
−0.250(0.196)
0.074(0.214)
0.004(0.137)
−0.042b
(0.083)0.023(0.111)
−0.017(0.055)
−0.003(0.047)
0.012(0.103)
RaCe/conv 0.232(0.185)
0.022(0.135)
0.009(0.138)
0.010(0.031)
−0.241(0.228)
−0.043(0.131)
0.043(0.122)
−0.010a*(0.031)
0.018(0.083)
0.008(0.067)
0.021(0.086)
0.016(0.060)
RaCe/ORF 0.219(0.247)
−0.013(0.121)
−0.004(0.115)
0.042(0.174)
−0.188(0.225)
0.043(0.112)
0.019(0.134)
−0.042b
(0.195)0.015
(0.060)0.011
(0.035)0.003
(0.047)0.016
(0.048)a, b: Signifi cant statistical difference between groups with different superscript letters and no signifi cant difference between groups with same superscript letters, a*: signifi cantly different from other groups in the cross-section, SD: Standard deviation, ORF: One rotary fi le technique, conv: full sequence technique, Race and Mtwo: rotary Ni-Ti systems, MB: Mesiobuccal canal, ML: Mesiolingual canal
Table 1: Mean centering ratio values of different sections of canals and SD in mesiodistal directionGroups Mean centering ratio (SD)
MB canal ML canal Distal canalFurca Coronal Middle Apical Furca Coronal Middle Apical Furca Coronal Middle Apical
Mtwo/conv 0.249a
(0.216)−0.083b
(0.146)−0.009c
(0.113)0.031d
(0.100)0.241a*(0.233)
−0.008b
(0.082)−0.033c
(0.129)0.057d
(0.096)0.207a
(0.151)−0.028b
(0.089)−0.048b
(0.100)0.052c
(0.107)Mtwo/ORF 0.469
(0.196)−0.140b
(0.204)−0.028(0.091)
0.005(0.117)
0.491b
(0.203)−0.184c
(0.167)−0.067(0.108)
−0.021d
(0.053)0.346
(0.185)−0.084(0.133)
−0.068(0.128)
−0.042c
(0.096)RaCe/conv 0.394
(0.151)−0.013a*(0.131)
−0.028(0.086)
0.021(0.041)
0.377b
(0.189)−0.065c
(0.086)−0.071(0.077)
0.010a*(0.080)
0.280(0.163)
−0.028(0.071)
−0.040(0.069)
0.000a*(0.047)
RaCe/ORF 0.298(0.182)
−0.127b
(0.119)−0.004(0.064)
0.042(0.101)
0.320b
(0.200)−0.135c
(0.131)−0.047(0.055)
0.036d
(0.089)0.315
(0.429)−0.035(0.078)
−0.052(0.068)
−0.015c
(0.076)a, b, c, d: Signifi cant statistical difference (2-way ANOVA with post hoc t test, P<0.05) between groups with different superscript letters and no signifi cant difference between groups with same superscript letters, a*: signifi cantly different from other groups in the cross-section, SD: Standard deviation, ORF: One rotary fi le technique, conv: full sequence technique, Race and Mtwo: rotary Ni-Ti systems, MB: Mesiobuccal canal, ML: Mesiolingual canal

Aminsobhani, et al.: Centering ability of one rotary fi le technique
74 Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
centering ratio values than one rotary fi le technique at the coronal third (P = 0.01).
In mesiolingual canal, conventional technique presented a significantly lower centering ratio values than one rotary file technique in the furcal (only in MD direction) ( P = 0.046) and coronal (only in MD direction) ( P < 0.001) thirds of the canal. Centering ratio values of RaCe system were significantly lower than Mtwo only at the apical third of the canal (in MD direction) ( P = 0.01). Also, conventional technique had a signifi cantly lower centering ratio values than one rotary fi le technique at the apical third of the canal (in BL direction) ( P = 0.01).
In distal canal (in MD direction), there was a significant difference between 4 sections regarding centering ratio except coronal with the middle section. In BL direction, there was no significant difference between 4 sections.
In mesiobuccal and mesiolingual canal (in MD direction), there was a significant difference between 4 sections regarding centering ratio. In BL direction, there was no signifi cant difference between 4 sections except furcal section with the other sections.
The highest centering ratio values were seen in furcal section. Despite higher values at furcal section, it was toward external surface of the root. At 3 and 6 mm apical to furca level (coronal and middle sections), there was lower centering ratio values but it often was toward inner surface of the root. There were more tendencies toward internal surface in Mtwo system with one rotary file technique although it was not signifi cantly different.
The mean time taken to prepare the canals with the different instruments is shown in Table 3. Instrumentation in one rotary file technique with either RaCe or Mtwo was significantly faster than
conventional technique in mesial ( P = 0.01) and distal canals (P = 0.02). There was no significant difference between Mtwo with RaCe and mesial with distal canals.
Three RaCe instruments (one fi le in the conventional technique and two files in one rotary file technique) were fractured during preparation. Only one Mtwo file was deformed permanently in one rotary file technique. The number of fractured instruments was not signifi cantly different between the fi le systems and or techniques.
DISCUSSION
The main purpose of instrumentation is to clean the canal while maintaining the anatomy and morphology of the canal.[3] Recently, different single file systems have been introduced. A recent study by Bürklein et al.[12] demonstrated that Reciproc and WaveOne with Mtwo and ProTaper rotary instruments could maintain the original canal curvature well with no signifi cant differences. Also, they found no signifi cant differences between Mtwo, Reciproc and WaveOne in coronal and middle thirds regarding debris removal. However, these fi les are used in a reciprocal motion and require specifi c automated devices.
Another new single NiTi file system, One Shape® that is introduced by Micro Mega Company[13] is an instrument that works in continuous rotation. It has three different cross-section zones along the blade.
In the present study, one rotary fi le technique using a Mtwo/RaCe #25/.06 fi le for each tooth was offered. The most notable benefits of this technique are no excess cost, no need to buy new instruments or specifi c motors. Reduced preparation time and a previously experienced sense during canal preparation are the other benefi ts.
Several methods have been used to evaluate the quality of root canal preparations, such as serial sectioning and microscopic evaluation, simulated canals, radiographic evaluation and cone beam computed tomography.[15,17-20] Serial sectioning[17] can result in loss of tooth structure. Another method is by using simulated root canals. It is reproducible and standard, but it cannot simulate complex anatomy of canals.[18] More complex simulated canals, True Tooth™ training replicas have been introduced recently.[19] These models have fi ve diffi culty
Table 3: Mean preparation time and SD (in seconds) with different instruments and techniquesGroups Mesial canals Distal canal
Time (s) SD Time (s) SDMtwo/conventional 530.4b 48 415.8b 54Mtwo/one fi le 356.4a 42 222a 75RaCe/conventional 548.4b 72 432b 96RaCe/one fi le 282a 72 156a 36(s): Seconds, SD: Standard deviation, Race and Mtwo: rotary Ni-Ti systems, a, b: Signifi cant statistical difference between groups with different superscript letters and no signifi cant difference between groups with same superscript letters

Aminsobhani, et al.: Centering ability of one rotary fi le technique
75Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
scales that many factors (i.e. pulp chamber size, canal curvature, apical branching, etc.) determine their diffi culty, but these models also have drawbacks such as different hardness with dentin. Radiographic evaluation is another method that is not destructive, but only allows two dimensional evaluations.[20] Cone beam volumetric tomography and micro computed tomography have been introduced to dentistry with good precision and resolution as well as no destruction of the specimen.[4,15] In the present study, cone beam computed tomography was used to compare centering ability of one rotary fi le technique with the established rotary Mtwo and RaCe instruments in curved root canals (round or oval shape) of extracted human mandibular molar teeth.
Preparation time is dependent on the technique and the numbers of instruments used.[21] In the present study, the preparation time included active instrumentation as well as the time required for changing instruments, cleaning the flutes of the instruments and irrigation. Therefore, preparation time significantly decreased in one rotary file technique because of no need to changing the files and more focus on canal preparation.
There were 3 RaCe fractured files versus 1 Mtwo deformed fi le in this study. Because of the S-shaped cross section, Mtwo instruments showed the higher torsional strength and higher resistance to torsional breakage compared with the triangular cross-sectional instruments.[22,23]
Mandibular molars, like most teeth, usually have significant curvature in both mesiodistal and buccolingual planes. Furthermore, they often have concavities on mesial and distal surfaces of the root.[24] These factors make the tooth susceptible to transportation and preparation errors such as perforations. There is limited information regarding transportation in buccolingual direction but in this study centering ability was evaluated in both directions.
As mentioned in Table 2, canal transportation at furcal level (In buccolingual direction) for mesiobuccal and mesiolingual canals was toward buccal and lingual sides respectively that is more valuable because they are safe zones with thicker dentin.
In mesiodistal direction, the highest centering ratio was seen at furcal section. Since transportation was toward
external side of the root (safety zone) with more dentin thickness, so it was favorable too. Higher incidence of canal transportation in mesiolingual canals may be due to more curvature in these canals.
According to the results of this study, centering ability in RaCe system was better than Mtwo system in a few sections. Although Alsudani et al.[25] reported significantly more canal transportation with RaCe fi les, other authors concluded that RaCe system create well-centered preparations.[17,26]
Mtwo instruments have good cutting efficiency, low cross-sectional area and relatively low number of spirals in each length unit. Therefore, it can resist deformation, but it is more rigid too.[9,27] This might explain the slightly higher incidence of canal aberrations observed in Mtwo system. Although the results of the present study were inconsistent with Bonaccorso et al.[28] and Celik et al.[3] researches, previous studies concluded the lowest transported canals in Mtwo groups.[29]
According to the results of the present study, only one rotary fi le technique showed relatively good centering ability and can be regarded suitable for cleaning and shaping of curved canals. Since preparation time was decreased significantly by using one rotary file technique; therefore, chemical debridement of the canal system was reduced. Larger volumes of irrigant and additionally activation of the irrigant should be used to improve disinfection. Further research is needed to evaluate this aspect.
CONCLUSIONS
Within the limitations of this study, both of the instrumentation systems and techniques produced canal preparations with adequate centering ratio. One rotary file technique prepared canal significantly faster than conventional techniques.
REFERENCES
1. Machado ME, Sapia LA, Cai S, Martins GH, Nabeshima CK. Comparison of two rotary systems in root canal preparation regarding disinfection. J Endod 2010;36:1238-40.
2. Lin J, Shen Y, Haapasalo M. A comparative study of biofilm removal with hand, rotary nickel-titanium , and self-adjusting file instrumentation using a novel in vitro biofilm model. J Endod 2013;39:658-63.
3. Celik D, Taşdemir T, Er K. Comparative study of 6 rotary nickel-titanium systems and hand instrumentation for root canal

Aminsobhani, et al.: Centering ability of one rotary fi le technique
76 Saudi Endodontic Journal • May-Aug 2014 • Vol 4 • Issue 2
preparation in severely curved root canals of extracted teeth. J Endod 2013;39:278-82.
4. Gekelman D, Ramamurthy R, Mirfarsi S, Paqué F, Peters OA. Rotary nickel-titanium GT and ProTaper files for root canal shaping by novice operators: A radiographic and micro-computed tomography evaluation. J Endod 2009;35:1584-8.
5. Aydin C, Inan U, Yasar S, Bulucu B, Tunca YM. Comparison of shaping ability of RaCe and Hero Shaper instruments in simulated curved canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e92-7.
6. Rangel S, Cremonese R, Bryant S, Dummer P. Shaping ability of RaCe rotary nickel-titanium instruments in simulated root canals. J Endod 2005;31:460-3.
7. Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 1. Shaping ability in simulated curved canals. Int Endod J 2004;37:229-38.
8. Yang G, Yuan G, Yun X, Zhou X, Liu B, Wu H. Effects of two nickel-titanium instrument systems, Mtwo versus ProTaper universal, on root canal geometry assessed by micro-computed tomography. J Endod 2011;37:1412-6.
9. Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 1.Shaping ability in simulated curved canals. Int Endod J 2006;39:196-202.
10. Uroz-Torres D, González-Rodríguez MP, Ferrer-Luque CM. Effectiveness of a manual glide path on the preparation of curved root canals by using Mtwo rotary instruments. J Endod 2009;35:699-702.
11. Dietrich MA, Kirkpatrick TC, Yaccino JM. In vitro canal and isthmus debris removal of the self-adjusting file, K3 ,and WaveOne files in the mesial root of human mandibular molars. J Endod 2012;38:1140-4.
12. Bürklein S, Hinschitza K, Dammaschke T, Schäfer E. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J 2012;45:449-61.
13. Micro-Mega [homepage on the internet]; Available from: http://www.Micro-Mega.com/One Shape® pdf. [Last accessed on 2013 Apr 24].
14. Sanfelice CM, da Costa FB, Reis Só MV, Vier-Pelisser F, Souza Bier CA, Grecca FS. Effects of four instruments on coronal pre-enlargement by using cone beam computed tomography. J Endod 2010;36:858-61.
15. Özer SY. Comparison of root canal transportation induced by three rotary systems with noncutting tips using computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:244-50.
16. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971;32:271-5.
17. Kfir A, Tsesis I, Yakirevich E, Matalon S, Abramovitz I. The efficacy of five techniques for removing root filling material:
Microscopic versus radiographic evaluation. Int Endod J 2012;45:35-41.
18. Yoshimine Y, Ono M, Akamine A. The shaping effects of three nickel-titanium rotary instruments in simulated S-shaped canals. J Endod 2005;31:373-5.
19. Dental Education Laboratories [homepage on the internet]; Available from: http://www.DELendo.com/TrueTooth™ training replicas. [Last accessed on 2013 June08].
20. Backman CA, Oswald RJ, Pitts DL. A radiographic comparison of two root canal instrumentation techniques. J Endod 1992;18:19-24.
21. Hülsmann M, Gressmann G, Schäfers F. A comparative study of root canal preparation using FlexMaster and HERO 642 rotary Ni-Ti instruments. Int Endod J 2003;36:358-66.
22. Yum J, Cheung GS, Park JK, Hur B, Kim HC. Torsional strength and toughness of nickel-titanium rotary files. J Endod 2011;37:382-6.
23. Zhang EW, Cheung GS, Zheng YF. Influence of cross-sectional design and dimension on mechanical behavior of nickel-titanium instruments under torsion and bending: A numerical analysis. J Endod 2010;36:1394-8.
24. Vertucci FJ, Haddix J. Tooth morphology and access cavity preparation. In: Hargreaves MK, Cohen S, editors. Pathways of the pulp. 10th ed. St. Louis: Mosby;2011.p208-12.
25. Al-Sudani D, Al-Shahrani S. A comparison of the canal centering ability of ProFile, K3, and RaCe Nickel Titanium rotary systems. J Endod 2006;32:1198-201.
26. Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J 2004;37:239-48.
27. Schäfer E, Oitzinger M. Cutting efficiency of five different types of rotary nickel-titanium instruments. J Endod 2008;34:198-200.
28. Bonaccorso A, Cantatore G, Condorelli GG, Schäfer E, Tripi TR. Shaping ability of four nickel-titanium rotary instruments in simulated S-shaped canals. J Endod 2009;35:883-6.
29. Schäfer E, Erler M, Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J 2006;39:203-12.
How to cite this article: Aminsobhani M, Ghorbanzadeh A, Dehghan S, Niasar AN, Kharazifard MJ. A comparison of canal preparations by Mtwo and RaCe rotary fi les using full sequence versus one rotary fi le techniques; a cone-beam computed tomography analysis. Saudi Endod J 2014;4:70-6.
Source of Support: This research was supported by a grant from Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran, Confl ict of Interest:The authors deny any confl icts of interest related to this study.