Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
A Combination of SAHA and Quinacrine IsEffective in Inducing Cancer Cell Death inUpper Gastrointestinal CancersShoumin Zhu1, Zheng Chen1, Lihong Wang2, Dunfa Peng1, Abbes Belkhiri2,A. Craig Lockhart3, and Wael El-Rifai1,4,5
Abstract
Purpose: We aimed to investigate the therapeutic efficacy ofsingle agent and the combination of quinacrine and suberoyla-nilide hydroxamic acid (SAHA) in wt- and mut-p53 upper gas-trointestinal cancer (UGC) cell models.
Experimental Design: ATP-Glo, clonogenic cell survival,Annexin V, comet, DNA double-strand breaks (DSBs), qPCR, andWestern blot analysis assays were utilized.
Results: Using clonogenic cell survival, ATP-Glo cell viabil-ity, Annexin V, and sub-G0 population analysis, we demon-strated that a combination of quinacrine and SAHA signifi-cantly decreased colony formation and increased cancer celldeath (range, 4–20 fold) in six UGC cell models, as comparedwith single-agent treatments, irrespective of the p53 status (P< 0.01). The combination of quinacrine and SAHA inducedhigh levels of DSB DNA damage (>20-fold, P < 0.01). Western
blot analysis showed activation of caspases-3, 9, and g-H2AXin all cell models. Of note, although quinacrine treatmentinduced expression of wt-p53 protein, the combination ofquinacrine and SAHA substantially decreased the levels ofboth wt-P53 and mut-P53. Furthermore, cell models that wereresistant to cisplatin (CDDP) or gefitinib treatments weresensitive to this combination. Tumor xenograft data con-firmed that a combination of quinacrine and SAHA is moreeffective than a single-agent treatment in abrogating tumorgrowth in vivo (P < 0.01).
Conclusions: Our novel findings show that the combinationof quinacrine and SAHA promotes DNA damage and is effectivein inducing cancer cell death, irrespective of p53 status andresistance to CDDP or gefitinib in UGC models. Clin Cancer Res;24(8); 1905–16. �2018 AACR.
IntroductionGastric and esophageal cancers cause over 1,000,000 deaths
each year worldwide (1). Although the incidence of most cancersis declining, esophageal adenocarcinoma is rising fast in theWesternworld (2). At the timeof diagnosis, upper gastrointestinalcancers (UGCs) are often advanced or metastatic with anincreasedmorbidity andmortality (3, 4). Themajority of patientswith UGCs have poor response to current therapeutic modalitieswith frequent tumor recurrence (5, 6). Despite significantimprovements in surgical outcome, radiation techniques, andchemotherapy, the 5-year survival rarely exceeds 20% (7, 8). Drugresistance remains a challenging problem in UGC therapy as wellas in the treatment of many other types of cancer. Developingnovel therapeutic approaches to overcome drug resistance is
desperately needed to improve the current therapeutic responseand clinical outcome.
Quinacrine, an antimalarial drug, has been shown to possessanticancer effects both in vitro (9) and in vivo (10). In the cancercells, quinacrine can simultaneously suppress NF-kB and activatep53 signaling with limited genotoxicity (9). Quinacrine can alsosuppress cellular inhibitors of apoptosis, independent of p53 (8).Suberoylanilide hydroxamic acid (SAHA), the first histone dea-cetylase inhibitor (HDACi) approved for cancer therapy (11), wasfound to inhibit class I HDACs and class II HDACs. SAHA inhibitsHDACs' activity and has multiple cellular effects. These includeinduction of cell-cycle arrest, reactive oxygen species (ROS),apoptosis, and autophagy (12–15). However, its efficacy as asingle agent in cancer treatment is considered moderate (16).Several preclinical studies and early clinical trials show evidencethat SAHA can be combined with other anticancer drugs (17). Ofnote, SAHA is well tolerated in patients and has limited toxicity,which is rapidly reversible upon discontinuation of the drug (18).
Chemotherapy remains the bedrock for the fight against cancer.Several chemotherapeutics induce DNA damage that is sensed byp53, which, depending on the level, either arrests the cell cycle toallow DNA damage repair or induces apoptosis (19). The P53mutation is one of themost prevalent genetic alterations in gastriccancer (20). Over 50% of human esophageal cancers harbormutant p53 (mut-p53; ref. 21). Mutant p53 is considered atumorigenic protein that acquires gain of oncogenic propertiesthat promote transformation, tumor growth, and increased resis-tance to anticancer treatments (13, 22). The high mutation rateand hyperstability ofmut-p53 protein in cancer can lead to failure
1Department of Surgery, University of Miami, Miami, Florida. 2Department ofSurgery, Vanderbilt University Medical Center, Nashville, Tennessee. 3Division ofMedical Oncology, University of Miami, Miami, Florida. 4Sylvester Comprehen-sive Cancer Center, University ofMiami, Miami, Florida. 5Department of VeteransAffairs, Miami Healthcare System, Miami, Florida.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Wael El-Rifai, University of Miami, Rosenstiel MedScience Bldg., 1600 NW 10th Ave., Rm 4007, Miami, FL 33136. Phone: 305-243-9648; Fax: 305-243-1053; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-17-1716
�2018 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 1905
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

of response to chemotherapeutics (23). Of note, there are datathat indicate wt-p53, in some instances, can be a poor predictor ofchemotherapy response (24, 25). Similar to mut-p53, patientswith wt-p53 may be resistant to a variety of antitumor agents,including cisplatin, doxorubicin, and 5-FU (22, 26, 27). Thepresence of wt-p53 in advanced cancers, such as breast cancer,chronic lymphocytic leukemia, ovarian, and renal cell carcinoma,results in a significantly lower response and/or curative rates (24,25, 28, 29).Wild-type p53 canmediate cell-cycle arrest and inhibitdrug response, even in the context of heterozygous p53 pointmutations or in the absence of p21 (25).
In this study, we investigated effects of combination ofquinacrine and SAHA against wt- and mut-p53 UGC models.Our findings indicate that quinacrine and SAHA combination ismore effective than a single-agent treatment in inducing cancercell death. The results indicate that this combination augmentstherapeutic response by increasing DNA damage levels, pro-moting degradation of both wt- and mut-p53 protein levels,and suppressing oncogenic signaling pathways, such as AKTand NF-kB pathways. Additional investigations are needed totest quinacrine and SAHA combination in additional preclin-ical and/or clinical settings to determine the therapeutic efficacyof this combination.
Materials and MethodsCell culture and reagents
Gastric (AGS, SNU1, MKN28, and MKN45) and esophageal(FLO1, OE33, and OE19) adenocarcinoma cells lines were usedin the study. AGS, SNU1, and MKN45 are p53 wild-typecells, whereas MKN28, FLO1, OE19, and OE33 are mutantp53 cell models (http://p53.free.fr/Database/Cancer_cell_lines/p53_cell_lines.html; Supplementary Table 1). Immortalizednonneoplastic normal esophageal cell line EPC2, kindly provided
byDr. Anil Rustgi (University of Pennsylvania, Philadelphia, PA),was included as a control. AGS and SNU1 cells were purchasedfrom ATCC. MKN28 and MKN45 cells were obtained from theRiken Cell Bank. The human esophageal adenocarcinoma celllines (OE33 and FLO1) were kindly provided by Dr. David Beer(University of Michigan, Ann Arbor, MI). OE19 cells wereobtained from Sigma-Aldrich. AGS and MKN28 cells were cul-tured in F12 media (GIBCO) supplemented with 5% FBS (Invi-trogen Life Technologies) and 1% penicillin/streptomycin(GIBCO). SNU1, MKN45, and FLO1 were cultured in DMEM(GIBCO) supplemented with 10% FBS and 1% penicillin/strep-tomycin.OE33 andOE19 cellsweremaintained inRPMImedium(GIBCO) supplemented with 10% FBS and 1% penicillin/strep-tomycin. All cell lines were ascertained to conform to the originalin vitromorphologic characteristics and were authenticated usingshort tandem repeat profiling (Genetica DNA Laboratories). Allcell lines reported here have been tested and shown to be free ofmycoplasma (R&D Systems). Horseradish peroxidase–conjugat-ed anti-mouse (7074P2) and anti-rabbit (7062P2) secondaryantibodies, p-STAT3 (Y705), STAT3, p-AKT (S473), AKT, p-NF-kB (S536), NF-kB, p-H2AX, H2AX, and Apoptosis AntibodySampler Kit (9915) and b-actin (4970) antibodies were obtainedfrom Cell Signaling Technology.
Clonogenic survival and ATP-Glo cell viability assayCells were rinsedwith PBS, trypsinized, andharvested in single-
cell suspension. Cells (1,000 cells/well) were seeded in 6-wellplates. The next day, cells were treated overnight with quinacrine(1 or 2 mmol/L) and SAHA (1 or 2 mmol/L) or vehicle, followed byreplacement with a regular drug-free culture media. After incu-bation for 10 days, colonies were fixed with 4% paraformalde-hyde and stained with 0.05% crystal violet. The plates wereimaged and stained colonies were counted. In addition, weutilized the cell Titer ATP-Glo Cell Viability Assay (Promega) forquantitative estimation of cell growth and survival (IC50). Cellswere plated in 96-well microplates at 1,000 cells per well, andvehicle (DMSO) or various concentrations of quinacrine (0–20mmol/L) or SAHA (0–20 mmol/L) were administered for 96 hours.Measurements using a Luminometer (BMG LABTECH) wereconducted following the manufacturer's protocol.
Cell-cycle analysisThe DNA content and cell-cycle distribution of gastric cancer
cells treated with the quinacrine and SAHA were determined byflow cytometry. Cells were plated in 6-well plates at a seedingdensity of 1�105 cells perwell. Twenty-four hours later, cellsweretreated with quinacrine (2 mmol/L) and SAHA (2 mmol/L) over-night. The cells were then harvested and collected by centrifuga-tion, washed twice in PBS (pH 7.2), and fixed with 70% coldethanol. Cells were stained with 200 mL of propidium iodide (PI)solution [200 mg/mL RNase (Sigma), 20 mg/mL PI, and 0.1%Triton X-100 (Sigma) in PBS] and incubated at 37�C for 30minutes. A total of 104 events were acquired in a flow cytometer(BD Biosciences), and data were analyzed using CellQuest soft-ware (BD Biosciences).
Apoptosis analysisCells were treated with vehicle or quinacrine and SAHA (2
mmol/L) overnight. Cells were then collected and stained withAnnexin V-FITC and PI (BioVision). The cells were washedwith PBS and resuspended in a binding buffer for subsequent
Translational Relevance
Upper gastrointestinal cancers (UGCs), adenocarcinomasof the stomach and esophagus, are characterized by frequentresistance to standard chemotherapeutics and poor clinicaloutcome. Although targeted therapy approaches have beensuccessful in several cancer types, UGCs response to severaltreatments has been discouraging and lower than expected.The response to SAHA and other HDAC inhibitors in gastro-intestinal cancers has not been encouraging either. Althoughantimalarial drugs have shown some anticancer activity, thereis a need to identify drug combinations that enhance thera-peutic efficacy. In this study, we demonstrate that a combina-tion of quinacrine and SAHA is potent in inducing cancer celldeath and abrogating tumor growth. In fact, we have shownthat this combination leads to degradation of both wild-typeand mutant p53 with significant increases in reactive oxygenspecies and DNA damage levels. The use of this combinationovercame resistance to gefitinib or cisplatin. In vivo studiesusing tumor xenograft models demonstrated significantregression of tumor volumes. Our findings not only uncovera novelmechanistic direction, but also provide data that couldsupport future clinical trials that test HDAC inhibitors alongwith quinacrine in patients with cancer.
Zhu et al.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1906
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

FACS analysis by a flow cytometer (Becton Dickinson). Apo-ptotic cell death was assessed by counting the numbers ofcells that stained positive for Annexin V-FITC and negativefor PI.
DNA double-strand break stainingCells were seeded on 6-well plates at a density of 2 � 105 cells
per well. Cells were treated with quinacrine (2 mmol/L) and SAHA(2 mmol/L) overnight, and then fixed by 3.7% formaldehyde/PBSfor 10 minutes and washed once with 1� PBS. The cells wereblocked for 30 minutes at room temperature with normal goatserum (10%; Thermo Fisher Scientific). Next, the cells were addedto 1� anti–phospho-histone antibody solution and incubatedovernight at 4�C. The cells were then washed five times with PBSTand were incubated in 1� secondary antibody–FITC conjugatesolution and washed five times with PBST. Coverslips weremounted with VECTASHIELD Mounting Medium containingDAPI to counterstain cellular nuclei. g-H2AX foci were scoredmanually throughout the cell nuclei using an Olympus fluores-cence microscope. The average number of foci per cell wascalculated from a minimum of 250 cells per dose/time point.Experimental data represent the average of three independentexperiments.
Comet assayDNA single- and double-strand break (DSB) levels were eval-
uated using a Comet Assay Kit (Trevigen) under alkaline condi-tions following themanufacturer's instructions. Briefly, cells werenontreated or treated with quinacrine (2 mmol/L) and SAHA (2mmol/L) overnight. Cells were suspended in PBS at 105 cells/mLand mixed with Comet Agarose at 1:10 ratio (v/v). The cellmixture (75 mL) was immediately layered onto a comet slide.The slide was maintained at 4�C for 15 minutes for gelling andthen immersed in lysis buffer at 4�C for 30minutes. The slide wasthen placed in alkaline solution for 30 minutes in the dark, andelectrophoresis was performed at 1 V/cm and 300 mA. Afterelectrophoresis, the slide was rinsed with H2O, immersed in70% ethanol for 5 minutes, and allowed to air dry. The slide wasthen stained with Vista Green DNA Dye, and comet "tails" werevisualized with an Olympus fluorescence microscope. Extent tailmoment values of comet assay were quantitated using the Open-Comet software (30).
qPCR analysisTotal RNAwas isolated fromcell lines by using the RNeasyMini
Kit (Qiagen). Total RNA (1 mg) was reverse transcribed by aniScript cDNA synthesis kit (Bio-Rad). qPCRwasperformedusing aBio-RadCFXConnect Real-timePCRDetection System (Bio-Rad),with the threshold cycle number determined by Bio-Rad CFXmanager software version 3.0. The primers for human HPRT1were forward: 50-TTGGAAAGGGTGTTTATTCCTCA-30; reverse: 50-TCCAGCAGGTCAGCAAAGAA-30. The primers for human P53were forward: 50-AGAGACCGGCGCACAGAG-30; reverse: 50-GGTGAAATATTCTCCATCCAGTG-30. Reactions were performedin duplicate, and results of three independent experiments weresubjected to statistical analysis. Fold change was calculated usingthe DDCt method (31). The results of the target genes werenormalized to HPRT1.
Western blottingCells were plated at a density of 2� 105 cells per well in 6-well
plates and treatedwith vehicle or drugs. After the indicated time of
treatment, cells were lysed by brief sonication in the RIPA LysisBuffer (Santa Cruz Biotechnology), and cellular proteins werecollected in the supernatant fraction after centrifugation at13,000 rpm for 10 minutes. Proteins were separated on12.5% SDS-PAGE and transferred to Immobilon PVDF mem-branes (Millipore). Membranes were probed with specific anti-bodies, and proteins were visualized by using horseradishperoxidase (HRP)–conjugated secondary antibodies andImmobilon Western Chemiluminescent HRP Substrate detec-tion reagent (Millipore). Gel loading was normalized for equalb-actin. All immunoblots were imaged using the Bio-Rad Che-miDoc XRSþ System (Bio-Rad).
Luciferase assayThe PG13 luciferase reporter, which contains 13 copies of the
wt-p53 binding-consensus sequence, was used as ameasure of thetranscription activity of p53 (Addgene plasmid #16442; ref. 32).Cells were seeded in 12-well plates and transfected with the PG13luciferase reporter by using the DNAfectin transfection reagent(Applied Biological Materials). The cells were harvested for lucif-erase assays 48 hours later using a Luciferase Assay Kit (Promega)according to themanufacturer's protocol. b-Galactosidase expres-sion plasmid was used as a control for normalization. Eachtransfection was performed in triplicate. Measurements using aLuminometer (BMG LABTECH) were conducted following themanufacturer's protocol.
Synergism analysesSynergy was quantified using the Chou–Talalay method as
described previously using the CalcuSyn software to calculate thevalues of the combination index (http://www.biosoft.com/w/calcusyn.htm, Biosoft; refs. 33, 34). The dose–effect curve foreach drug alone is determined on the basis of experimentalobservations using the median-effect principle and is comparedwith the effect achieved with a combination of the two drugs toderive a combination index (CI) value. The CI indicates the levelof synergism or antagonism: <0.9 indicates synergism (0.3–0.7strong; 0.7–0.85 moderate; 0.85–0.9 slight), 0.9–1.1 nearly addi-tive effect, and >1.1 antagonism (34).
In vivo experimentsFive-week-old female NIH-III nude mice were purchased from
Charles River Laboratories, Inc. and maintained under specificpathogen-free conditions. UGC cells were injected subcutaneous-ly (2 � 106 cells/site) into the flanks. When the tumor volumereached approximately 150 mm3, the mice were randomly divid-ed into four groups and treated with quinacrine (200 mg/kg, oralgavage), SAHA (50 mg/kg, i.p.), or a combination of quinacrineand SAHA three times per week for 3 weeks. Tumor growth wasdetermined by measuring the width and length of the tumorswith a caliper twice weekly, and body weight was measured tomonitor drug toxicity. The tumor volume was calculated usingthe following formula: tumor volume (mm3) ¼ 1/2 (W)2 � (L).The Institutional Animal Care and Use Committee approved allanimal work.
Statistical analysesValues were expressed as mean � SD of three independent
experiments. With the GraphPad Prism 5 software, a one-wayANOVA Newman–Keuls multiple comparisons test was per-formed to compare the differences among three groups or more,
A Combination of QC and SAHA Induces Cancer Cell Death
www.aacrjournals.org Clin Cancer Res; 24(8) April 15, 2018 1907
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

and a two-tailed Student t test was used to compare the statisticaldifference between two groups. Differences with P values �0.05are considered statistically significant.
ResultsQuinacrine sensitizes UGC cells to SAHA treatment
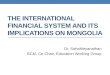
Using the ATP-Glo cell viability assay, we found that thecombination of quinacrine and SAHA significantly decreasedcell viability in all tested UGC models (AGS, SNU1, MKN45,OE33, FLO1, OE19, and MKN28), as compared with single-agent treatments; these results were confirmed by determiningthe IC50 in response to single agent or a combination ofquinacrine and SAHA (Fig. 1A–G). The IC50s of quinacrine,SAHA, and quinacrine and SAHA of all the tested UGC models
were summarized in Fig. 1H. We did not detect significantchanges in viability of immortalized normal esophageal cells(EPC2, Supplementary Fig. S1A and S1B). We tried to discerncell response to quinacrine and SAHA treatment. ATP-Glo assaywas performed in AGS, SNU1, MKN45, MKN28, and OE33 cellsfollowing drug treatment. The cell survival ratio was decreasedby 90% in AGS cells, 95% in SNU1 cells, 85% in MKN45 cells,and 90% in both MKN28 cells and OE33 cells followingcoadministration of 2 mmol/L quinacrine and 2 mmol/L SAHAcompared with vehicle treatment cells (P < 0.01, Supplemen-tary Fig. S2A–S2E). For increased stringency, we used quina-crine (1 mmol/L) and SAHA (1 mmol/L) for overnight treatmentand long-term (10 days) clonogenic survival assay. The resultsindicated that quinacrine and SAHA cotreatment induced 70%cell death in both AGS and MKN28 cells and induced 60% cell
Figure 1.
Quinacrine (QC) sensitized upper gastrointestinal cancer cells to SAHA treatment. A–G, ATP-Glo assay for the quinacrine and SAHA combination and single-agenttreatment in cancer cells (AGS, SNU1, MKN45, OE33, FLO1, OE19, and MKN28). H, The summary of IC50 of quinacrine, SAHA, or quinacrine þ SAHA treatmentof all the tested UGC cell models is shown with combination index (CI) values of synergistic activity in UGC cell lines. Count (n) refers to the number ofreplicate experiments.
Zhu et al.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1908
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

death in FLO1 cells as compared with vehicle treatment cells(Supplementary Fig. S3A–S3C, P < 0.001). Furthermore, thecombination index values were calculated using the Chou–Talalay isobologram equation (34). We combined the ratio of 1with quinacrine and SAHA with twofold serial dilutions (startfrom 20 mmol/L). The results indicated synergistic activitybetween quinacrine and SAHA for almost all UGC cell linestested, as indicated by combination index values of <0.7 (Fig.1H). Taken together, these findings indicated that quinacrineand SAHA have a synergistic effect in induction of UGC cellsdeath, which raised a question of how quinacrine sensitizedUGC cells to SAHA treatment.
Quinacrine and SAHA combination induces cell deathDisturbance of the cancer cell cycle is one of the therapeutic
targets for development of new anticancer drugs (35). The cell-cycle distribution of each phase was examined by flow cytometry.As shown in Fig. 2, significant G0–G1 arrest was induced bycombination treatment in AGS, SNU1, MKN28, and FLO1 cellsin comparison with individual treatments and vehicle treatmentcells (Fig. 2A–D, P < 0.01).
Consistent with these results, the Annexin V-FITC apoptosisassay showed that quinacrine and SAHA cotreatment inducedapoptosis by approximately 10-fold in AGS cells, 20-fold inMKN45 cells, 16-fold in MKN28 cells, and 50-fold in FLO1 cellsrelative to control cells (Fig. 3A–D).
Quinacrine and SAHA combination increases levels of DNAdamage
Furthermore, we analyzed the extent of DNA damage byexamining the level of g-H2AX. H2AX is considered a marker ofDNA DSBs and activation of DNA damage response (36). Ourresults demonstrated that the combination of quinacrine andSAHA significantly increased the DSB levels as compared withindividual treatments and vehicle treatment in AGS, SNU1,MKN28, and FLO1 cells (Fig. 4A–D, P < 0.01), as indicated bythe increased number of g-H2AX foci in these cells comparedwith vehicle treatment cells (Fig. 4A–D, P < 0.01). Next, weevaluated the DNA damage induced by quinacrine and SAHAtreatment by performing comet assay in AGS and MKN28 cells;the results indicated that cotreatment of quinacrine couldsignificantly enhance the DNA damages caused by SAHA inAGS and MKN28 cells compared with individual treatmentsand vehicle treatment cells (eightfold, P < 0.01; SupplementaryFig. S4A and S4B).
These results provide compelling evidence that DNA damageplays a causal role in the anti-UGC cytotoxic efficacy of combinedquinacrine and SAHA.
Quinacrine and SAHA combination induces apoptosis andblocks cell survival signaling pathways
Antimalarial drugs, such as quinacrine and chloroquine, havebeen previously shown to inhibit autophagy (37). Therefore, we
Figure 2.
Quinacrine (QC) and SAHA combination increases cancer cell death.A–D, The distribution of each phase of cell cycle was examined by flow cytometry in AGS, SNU1,MKN28, and FLO1 cells. One-way ANOVA test was performed to compare the differences among four groups, and a two-tailed Student t test was used tocompare the statistical difference between two groups. Each bar in the graph to the right represents themean of the sub-G0� SD of three independent experiments.�� , P < 0.01.
A Combination of QC and SAHA Induces Cancer Cell Death
www.aacrjournals.org Clin Cancer Res; 24(8) April 15, 2018 1909
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

tested the effects of quinacrine alone and in combination withSAHA. As expected, we observed induction of LC3B-II levelsfollowing treatment with quinacrine. These levels were furtherincreased following combination treatment (Supplementary Fig.S5A and S5B).
We then investigated the levels of cell death following single-agent and combined treatments. We investigated the effects oftreatment with quinacrine and SAHA alone or in combination onthe endogenous levels of p53, g-H2AX, and caspases-3 and 9;including wt-p53 (AGS, SNU1, and MKN45) and mut-p53(MKN28, FLO1, and OE33) UGC cells. When treated with quin-acrine alone, we observed induction of wt-p53 as shown in (AGS,SNU1, and MKN45; Fig. 5A; Supplementary Fig. S6A), with noeffect on mut-p53 (MKN28, FLO1, and OE33; Fig. 5B; Supple-mentary Fig. S6B). However, SAHA alone and the combination ofquinacrine and SAHA demonstrated a notable reduction in thelevels of wt-p53 and mut-p53 (Fig. 5A and B; Supplementary
Fig. S6). Western blot analysis also indicated that AGS, SNU1,MKN45, MKN28, OE33, and FLO1, following quinacrine andSAHA combination treatment, have increased activation ofg-H2AX and caspases-3 and 9 (Fig. 5A and B; Supplementary Fig.S6). Moreover, we found that there was no significant differencefor p53 mRNA levels in mut-P53 cell lines after quinacrinecotreatment with SAHA as compared with control cells, butquinacrine treatment alone increased p53 mRNA expression inwt-P53 cell lines (Supplementary Fig. S7A–S7F). Luciferase assayshowed that the quinacrine/SAHA treatment decreased P53 activ-ity, as comparedwith controls (Supplementary Fig. S8,P<0.01). Itwould be interesting to find out more about the mechanisms ofP53 degradation induced by quinacrine and SAHA treatment inthe future.
SAHA decreased the activation of AKT (38). Quinacrineinhibited AKT and the NF-kB pathway (8, 9). Here, we showedthat when quinacrine was combined with SAHA, there was a
Figure 3.
The combination of quinacrine (QC) and SAHA treatment induces high levels of apoptosis. A–D, The Annexin V-FITC and propidium iodide (PI) stainingwas performed following quinacrine and SAHA or vehicle treatment in AGS, MKN45, MKN28, and FLO1 cells. One-way ANOVA test was performed tocompare the differences among four groups, and a two-tailed Student t testwas used to compare the statistical difference between twogroups. Each bar in the graphto the right represents the mean of the Q2 � SD of three independent experiments. All measurements were compared with control (Ctrl). � , P < 0.05;�� , P < 0.01.
Zhu et al.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1910
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

remarkable decrease of AKT, STAT3, and NF-kB activitiesin AGS, FLO1, SNU1, and MKN28 cells (Fig. 5C and E; Sup-plementary Fig. S9). The luciferase reporter assay showedsimilar results; quinacrine/SAHA treatment caused significantdecrease in NF-kB and STAT3 activities in AGS, FLO1, SNU1,and MKN28 cells (Fig. 5D and F, P < 0.01, SupplementaryFig. S10, P < 0.01). These findings suggest that concurrentinterruption of cell survival signaling pathways warrants furtherinvestigation in cancer therapy.
CDDP or gefitinib-resistant cells maintain sensitivity toquinacrine and SAHA treatment in vitro
Cisplatin (CDDP) is a first-line chemotherapeutic drug forgastric cancer, however, cancer cells often develop multiplemechanisms to overcome cisplatin-induced DNA damage andapoptosis, leading to cisplatin resistance (39). Targeted therapieshave emerged as a new hope in cancer management during recentyears. The vast majority of gastric cancer patients receiving gefi-tinib develop resistance (40). Chemotherapeutic resistance is amajor challenge in our approaches to treat UGCs. There are twomajor forms of drug resistance: primary resistance and acquiredresistance. To address this problem, we developed in vitro cell
models of acquired resistance to CDDP (CDDP-R) using an AGScancer cell line following continuous treatment with dose esca-lation for 6 months. We also tested our cell lines and found thatOE19 cells have intrinsic resistance to CDDP (IC50 > 10 mmol/Lfor OE19). Using AGS CDDP-R and OE19 cell models, the resultsindicated that these cells remain sensitive to the combined quin-acrine and SAHA treatment (Supplementary Fig. S11A–S11D).Of note, AGS parental and AGS CDDP-R cell lines achievedsimilar IC50 (around 0.80 mmol/L) for quinacrine and SAHAtreatment (Supplementary Fig. S11B). The results also showedthat OE19 cells are sensitive to the quinacrine and SAHA com-bination treatment (IC50 ¼ 0.55 mmol/L; Supplementary Fig.S11D). Next, we tested our cell lines and found that MKN45 cellshave intrinsic resistance to gefitinib (IC50 ¼ 34.121 mmol/L),using MKN45 cell model. We found that these cells remainsensitive to the combined quinacrine and SAHA treatment (IC50
¼ 0.56 mmol/L, Supplementary Fig. S11E and S11F).We includedthe IC50 of gefitinib and CDDP for all the cell lines we used(Supplementary Fig. S11G). In the future, we will perform in vivoapproaches to investigate the therapeutic efficacy of quinacrineand SAHA combination in preclinical models of resistance toCDDP and gefitinib.
Figure 4.
Quinacrine (QC) and SAHA treatment leads to high levels of DNA damage. A–D, g-H2AX (green) staining in AGS, SNU1, MKN28, and FLO1 cells following treatments(left) and relative percentage of foci positive cells (right). One-way ANOVA test was performed to compare the differences among four groups, anda two-tailed Student t test was used to compare the statistical difference between two groups. Each bar in the graph to the right represents the mean of thecells with DSB � SD of three independent experiments. �� , P < 0.01.
A Combination of QC and SAHA Induces Cancer Cell Death
www.aacrjournals.org Clin Cancer Res; 24(8) April 15, 2018 1911
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

Combination of quinacrine and SAHA treatment is effective inUGC tumor xenograft mouse model
We evaluated the effects of quinacrine and SAHA combinationtreatment in OE33 cells. Treatment with quinacrine or SAHAalone significantly inhibited tumor growth as compared withcontrol tumors (P < 0.05, Fig. 6A), and treatment with quinacrine
and SAHA combination significantly inhibited tumor growth ascompared with individual treatments and control tumors (P <0.01, Fig. 6A). The results demonstrated that tumors derived fromOE33 cells combined quinacrine and SAHA treatment grewsubstantially slower than the individual treated tumor and controltumors (Fig. 6B and C). Immunostaining with the anti–cleaved
Figure 5.
Quinacrine (QC) and SAHA treatment induces apoptosis and blocks cell survival signaling pathways.A andB,Western blot analyses for p53, g-H2AX, and caspases-3and 9, and actin following treatment of quinacrine and SAHA in wt-p53 (AGS and SNU1) and mut-p53 (MKN28 and FLO1) UGC cells. C, Western blotanalyses were performed in AGS cells for AKT, STAT3, and NF-kB activities following treatment of quinacrine and SAHA.D, Luciferase reporter assay for STAT3 andNF-kB was performed in AGS cells following quinacrine and SAHA treatment. E, Western blot analyses were performed in FLO1 cells for AKT, STAT3,and NF-kB activities following treatment of quinacrine and SAHA. F, Luciferase reporter assays for STAT3 and NF-kB were performed in FLO1 cells followingquinacrine and SAHA treatment. One-way ANOVA test was performed to compare the differences among four groups, and a two-tailed Student t test was used tocompare the statistical difference between two groups. Each bar in the graph to the right represents the mean of relative luciferase activity � SD of threeindependent experiments. � , P < 0.05; ��, P < 0.01.
Zhu et al.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1912
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

caspase-3 and anti–Ki-67 antibodies indicated that the reducedtumor growth is likely due to a lower proliferation rate and higherapoptosis caused by quinacrine þ SAHA treatment, as cleaved
caspase-3 staining was much stronger in quinacrine þ SAHAtreatment tumors than individual treatments and vehicle treat-ment tumors (P < 0.01, Fig. 6D). Ki-67 staining was much weaker
Figure 6.
Quinacrine (QC) and SAHA combination abrogates tumor growth in tumor xenograft mouse models. A, Tumor volume was measured at the indicated times; eachdata point represents the mean �SD for 10 tumor xenografts. B and C, Representative xenograft tumors of sacrificed mice (left) and quantification of tumorweight at the end of experiment (right).D and E, IHC stainingwas performed for caspase-3 and Ki-67 proteins. One-way ANOVA test was performed to compare thedifferences among four groups, and a two-tailed Student t test was used to compare the statistical difference between two groups. Each bar in the graphto the right represents the mean � SD of three independent experiments. �, P < 0.05; �� , P < 0.01.
A Combination of QC and SAHA Induces Cancer Cell Death
www.aacrjournals.org Clin Cancer Res; 24(8) April 15, 2018 1913
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

in quinacrine and SAHA treatment tumors than individual treat-ments and vehicle treatment tumors (P < 0.01, Fig. 6E).
DiscussionUpper gastrointestinal cancers are characterized by resistance
to chemotherapeutics and poor clinical outcome. Of note, thesecancers are characterized by massive changes in DNA copy num-bers showing chromosomal instability in the form of frequentgains and losses that affect large regions and subregions ofthe chromosomes (41–44). Although mutations and/or amplifi-cation of RTK genes have been reported, targeted therapyapproaches have shown limited therapeutic efficacy (45–47). Therecent next-generation sequencing and TCGA data reports indi-cate that mutations of p53 occur in more than half of thesetumors, whereas mutations in other genes occur at low frequen-cies (43, 44). Given the complexity of UGCs, the use of combi-natorial therapy couldbe an essential step toovercome the limitedclinical efficacy of the current therapeutic strategies. In this study,we have investigated, for the first time, the effects of quinacrine incombination with SAHA on wt- and mut-p53 UGC cells. Ourresults demonstrate that a combination of quinacrine and SAHAis potent in inducing cancer cell death in preclinical models ofUGCs.We further demonstrate that this combination targets bothwt- and mut-p53 leading to their degradation, which could be anessential step in the observed significant response to this combi-nation, as compared with single-agent treatments.
Quinacrine is an antimalarial drug that has been effectivelyused for several decades (48). The side effects and general toxicityof quinacrine are usually well tolerated (49). Over the past fewyears, there has been an interest in repurposing quinacrine for thetreatment of cancer. In fact, earlier reports have shown thatquinacrine treatment can suppress oncogenic pathways such asERK, PI3K/AKT/mTOR, and NF-kB pathways (50, 51). However,quinacrine alone has not shown promising results in the treat-ment of cancer (52). SAHA is an HDAC inhibitor approved forcancer therapy (11). Unfortunately, its efficacy as a single agent incancer treatment is only moderate (16). Some preclinical studiesand early-phase clinical trials showed evidence that SAHA can becombined with other anticancer drugs (17). We have investigatedthe combination of quinacrine with SAHA. We found that quin-acrine can induce LC3B-II protein expression, whereas combinedquinacrine/SAHA treatment induced higher levels of LC3B-II thanquinacrine treatment alone. Of note, quinacrine is a potentinhibitor of autophagy that has 60-fold higher potency of autop-hagy inhibition than chloroquine (53). Although, we have notspecifically investigated the details of autophagy in our study, ourfindings suggest that the quinacrine and SAHA combination canpromote cancer cell death.
P53 is a major pathway in regulating apoptosis and DNAdamage repair. P53 is a double-sword protein that can induceapoptosis in response to high levels of DNA damage or DNAdamage repair and cell survival in response to low and moderatelevels of DNA damage (54). The DNA damage repair capacity ofp53 canmediate resistance to chemotherapeutics. Indeed, a recentreport has shown that wt-p53 can mediate therapeutic resistanceby initiating and promoting the process of DNA damage repair(25). We found that treatment with quinacrine alone leads toinduction of wt-p53, whereas the combination of quinacrine andSAHA demonstrated low levels of p53 protein, suggesting thepresence of SAHA-mediated rapid degradation of quinacrine-
induced p53 with abrogation of DNA damage repair. It has beenshown that SAHA treatment can induce ROS and DNA damage(55, 56). In addition, quinacrine can also induce ROS and DNAdamage (54). Our results demonstrate that with the suppressionof wt-p53 levels, the combined treatment with quinacrine andSAHA led to accumulation of lethal levels of DNA damage. Arecent study suggested that induction of p53 by quinacrine ismainly mediated by suppression of NF-kB activity (9). On theother hand, NF-kB activation by SAHA can lead to hyperacetyla-tion, nuclear translocation, and activation of RelA/p65 (57).Therefore, it is possible that by using the quinacrine and SAHAcombination, SAHA is antagonizing the quinacrine-mediatedinduction of p53. We conclude that the combination of quina-crine and SAHA augments the anticancer therapeutic efficacy notonly by inhibition of autophagy, but also via suppression of p53protein levels, inhibition of DNA damage repair, and accumula-tion of lethal levels of DNA damage.
Several studies have shown thatmutant p53acquires oncogenicfunctions and is an important factor in drug resistance in responseto DNA damage and chemotherapeutics. In the current study, weshow that the quinacrine treatment alone had no effect on mut-p53, whereas the quinacrine and SAHA combination promoteddegradation of oncogenic mut-p53 and increased DNA damagelevels higher than single-agent treatments. This was associatedwith a significant increase in cell death in vitro and reduction oftumor volume in in vivo preclinical models. Previous studies inother cancer types have shown that SAHA's inhibition onHDAC6and HDAC8 decreases the mut-p53 protein level (58, 59). How-ever, we acknowledge that the exact mechanism by which thecombination of quinacrine and SAHA mediates degradation ofmut-p53 in UGCs requires additional investigations.
Anticancer drugs upregulate the NF-kB pathway, which resultsin the development of drug resistance (60). Akt plays an impor-tant role in the signaling pathways in response to growth factorsand other extracellular stimuli to regulate several cellular func-tions, including cell growth, apoptosis, and survival (61). Block-ing signaling to STAT3 inhibits cancer cell growth, showing thatSTAT3 is crucial to the survival and growth of tumor cells and is anattractive therapeutic target for cancer (62). Here, we showed thatwhen cells were treated with quinacrine and SAHA, there was asignificant decrease of AKT, STAT3, and NF-kB activity in UGCcells. These findings suggest that concurrent interruption of cellsurvival signaling pathways warrants further investigation incancer therapy.
Chemotherapeutic resistance is a major challenge in the treat-ment of upper gastrointestinal cancers. By testing gastric cancercells with acquired resistance to cisplatin, as compared with theirparental ones, we found that resistant and parental cells are highlysensitive to quinacrine and SAHA combination. A similar findingwas noted in OE19 cells that has intrinsic resistance to cisplatin.Furthermore, the MKN45 cell model, resistant to gefitinib treat-ment, was also sensitive to this combination. Together, theseresults suggest that the quinacrine and SAHA combined treatmentapproach may be tested in clinical trials of UGCs.
In conclusion, our novel findings show that the quinacrine andSAHA combination is more effective than a single-agent treat-ment.Our results provide evidence thatDNAdamagemayplay anadditional role in cytotoxic efficacy of combined quinacrine andSAHA. Our results demonstrate that this combination leads toabrogation of both wt and mut-p53 protein levels and augmentsthe therapeutic response. Additional investigations are needed to
Zhu et al.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1914
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

fully explain themolecular and signaling effects of quinacrine andSAHA combination. Our findings may support clinical trials thattest the activity of this combination in UGC patients.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
DisclaimerThe contents of this work are solely the responsibility of the authors and do
not necessarily represent the official views of theDepartment of Veterans Affairs,NIH, or University of Miami.
Authors' ContributionsConception and design: S. Zhu, W. El-RifaiDevelopment of methodology: S. Zhu, Z. ChenAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): S. Zhu, Z. Chen, D. PengAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): S. Zhu, Z. Chen, L. Wang, D. Peng, A. Belkhiri,A.C. Lockhart
Writing, review, and/or revision of the manuscript: S. Zhu, A.C. Lockhart,W. El-RifaiAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): W. El-RifaiStudy supervision: W. El-Rifai
AcknowledgmentsThis study was supported by the NIH (R01CA93999 and
R01CA131225), Research Career Scientist award (1IK6BX003787), and amerit award (I01BX001179) from the U.S. Department of Veterans affairs(to W. El-Rifai).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received June 16, 2017; revisedOctober 27, 2017; accepted January 25, 2018;published OnlineFirst January 31, 2018.
References1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer
statistics, 2012. CA Cancer J Clin 2015;65:87–108.2. Edwards BK,Ward E, Kohler BA, EhemanC, Zauber AG, AndersonRN, et al.
Annual report to the nation on the status of cancer, 1975–2006, featuringcolorectal cancer trends and impact of interventions (risk factors, screening,and treatment) to reduce future rates. Cancer 2010;116:544–73.
3. Chiu WT, Lee HT, Huang FJ, Aldape KD, Yao J, Steeg PS, et al. Caveolin-1upregulation mediates suppression of primary breast tumor growth andbrain metastases by stat3 inhibition. Cancer Res 2011;71:4932–43.
4. Bhoopathi P,ChettyC,DontulaR,GujratiM,DinhDH,Rao JS, et al. SPARCstimulates neuronal differentiation of medulloblastoma cells via theNotch1/STAT3 pathway. Cancer Res 2011;71:4908–19.
5. Carew JS, Giles FJ, Nawrocki ST. Histone deacetylase inhibitors: mechan-isms of cell death and promise in combination cancer therapy. Cancer Lett2008;269:7–17.
6. Miyata H, Yamasaki M, Kurokawa Y, Takiguchi S, Nakajima K, Fujiwara Y,et al. Survival factors in patients with recurrence after curative resection ofesophageal squamous cell carcinomas. Ann Surg Oncol 2011;18:3353–61.
7. Jani TS, DeVecchio J,Mazumdar T, Agyeman A,Houghton JA. Inhibition ofNF-kappaB signaling by quinacrine is cytotoxic to human colon carcinomacell lines and is synergistic in combination with tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) or oxaliplatin. J Biol Chem2010;285:19162–72.
8. Wang Y, Bi Q, Dong L, Li X, Ge X, Zhang X, et al. Quinacrine enhancescisplatin-induced cytotoxicity in four cancer cell lines. Chemotherapy2010;56:127–34.
9. Gurova KV, Hill JE, Guo C, Prokvolit A, Burdelya LG, Samoylova E, et al.Small molecules that reactivate p53 in renal cell carcinoma reveal a NF-kappaB-dependent mechanism of p53 suppression in tumors. Proc NatlAcad Sci U S A 2005;102:17448–53.
10. Gallant JN, Allen JE, Smith CD, Dicker DT, Wang W, Dolloff NG, et al.Quinacrine synergizes with 5-fluorouracil and other therapies in colorectalcancer. Cancer Biol Ther 2011;12:239–51.
11. Marks PA, Breslow R. Dimethyl sulfoxide to vorinostat: development ofthis histone deacetylase inhibitor as an anticancer drug. Nat Biotechnol2007;25:84–90.
12. Ungerstedt JS, Sowa Y, XuWS, Shao Y, Dokmanovic M, Perez G, et al. Roleof thioredoxin in the response of normal and transformed cells to histonedeacetylase inhibitors. Proc Natl Acad Sci U S A 2005;102:673–8.
13. Xu XD, Yang L, Zheng LY, Pan YY, Cao ZF, Zhang ZQ, et al. Suberoylanilidehydroxamic acid, an inhibitor of histone deacetylase, suppresses vasculo-genic mimicry and proliferation of highly aggressive pancreatic cancerPaTu8988 cells. BMC Cancer 2014;14:373.
14. Chen X, Radany EH, Wong P, Ma S, Wu K, Wang B, et al. Suberoylanilidehydroxamic acid induces hypersensitivity to radiation therapy in acute
myelogenous leukemia cells expressing constitutively active FLT3mutants.PLoS One 2013;8:e84515.
15. Shao Y, Gao Z, Marks PA, Jiang X. Apoptotic and autophagic cell deathinduced by histone deacetylase inhibitors. Proc Natl Acad Sci U S A2004;101:18030–5.
16. Schaefer EW, Loaiza-Bonilla A, JuckettM, DiPersio JF, Roy V, Slack J, et al. Aphase 2 study of vorinostat in acute myeloid leukemia. Haematologica2009;94:1375–82.
17. Nolan L, Johnson PW, Ganesan A, Packham G, Crabb SJ. Will histonedeacetylase inhibitors require combination with other agents to fulfil theirtherapeutic potential? Br J Cancer 2008;99:689–94.
18. Mann BS, Johnson JR, He K, Sridhara R, Abraham S, Booth BP, et al.Vorinostat for treatment of cutaneousmanifestations of advanced primarycutaneous T-cell lymphoma. Clin Cancer Res 2007;13:2318–22.
19. Breen L, Heenan M, Amberger-Murphy V, Clynes M. Investigation of therole of p53 in chemotherapy resistance of lung cancer cell lines. AnticancerRes 2007;27:1361–4.
20. Fenoglio-Preiser CM, Wang J, Stemmermann GN, Noffsinger A. TP53 andgastric carcinoma: a review. Hum Mutat 2003;21:258–70.
21. IrelandAP, ShibataDK, ChandrasomaP, Lord RV, Peters JH,DeMeester TR.Clinical significance of p53 mutations in adenocarcinoma of the esoph-agus and cardia. Ann Surg 2000;231:179–87.
22. Scuto A, Kujawski M, Kowolik C, Krymskaya L, Wang L, Weiss LM, et al.STAT3 inhibition is a therapeutic strategy for ABC-like diffuse large B-celllymphoma. Cancer Res 2011;71:3182–8.
23. Maslon MM, Hupp TR. Drug discovery and mutant p53. Trends Cell Biol2010;20:542–55.
24. WongKK, Izaguirre DI, Kwan SY, King ER,DeaversMT, SoodAK, et al. Poorsurvival with wild-type TP53 ovarian cancer? Gynecol Oncol 2013;130:565–9.
25. Jackson JG, Pant V, Li Q, Chang LL, Quintas-Cardama A, Garza D, et al.p53-mediated senescence impairs the apoptotic response to chemo-therapy and clinical outcome in breast cancer. Cancer Cell 2012;21:793–806.
26. Corcoran RB, Contino G, Deshpande V, Tzatsos A, Conrad C, Benes CH,et al. STAT3 plays a critical role in KRAS-induced pancreatic tumorigenesis.Cancer Res 2011;71:5020–9.
27. Manuel ER, Blache CA, Paquette R, Kaltcheva TI, Ishizaki H, Ellen-horn JD, et al. Enhancement of cancer vaccine therapy by systemicdelivery of a tumor-targeting Salmonella-based STAT3 shRNA sup-presses the growth of established melanoma tumors. Cancer Res2011;71:4183–91.
28. Bertheau P, Lehmann-Che J, Varna M, Dumay A, Poirot B, Porcher R, et al.p53 in breast cancer subtypes and new insights into response to chemo-therapy. Breast 2013;22 Suppl 2:S27–9.
A Combination of QC and SAHA Induces Cancer Cell Death
www.aacrjournals.org Clin Cancer Res; 24(8) April 15, 2018 1915
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

29. Noon AP, Vlatkovic N, Polanski R, Maguire M, Shawki H, Parsons K, et al.p53 andMDM2 in renal cell carcinoma: biomarkers for disease progressionand future therapeutic targets? Cancer 2010;116:780–90.
30. Gyori BM, Venkatachalam G, Thiagarajan PS, Hsu D, Clement MV. Open-Comet: an automated tool for comet assay image analysis. Redox Biol2014;2:457–65.
31. Pfaffl MW. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res 2001;29:e45.
32. el-Deiry WS, Tokino T, Velculescu VE, Levy DB, Parsons R, Trent JM,et al. WAF1, a potential mediator of p53 tumor suppression. Cell1993;75:817–25.
33. Chou TC. Preclinical versus clinical drug combination studies. Leuk Lym-phoma 2008;49:2059–80.
34. Chou TC.Drug combination studies and their synergy quantification usingthe Chou-Talalay method. Cancer Res 2010;70:440–6.
35. Schwartz GK, Shah MA. Targeting the cell cycle: a new approach to cancertherapy. J Clin Oncol 2005;23:9408–21.
36. Tanaka T, Halicka D, Traganos F, Darzynkiewicz Z. Cytometric anal-ysis of DNA damage: phosphorylation of histone H2AX as a marker ofDNA double-strand breaks (DSBs). Methods Mol Biol 2009;523:161–8.
37. Goodall ML, Wang T, Martin KR, Kortus MG, Kauffman AL, Trent JM, et al.Development of potent autophagy inhibitors that sensitize oncogenicBRAF V600E mutant melanoma tumor cells to vemurafenib. Autophagy2014;10:1120–36.
38. Yang B, Yu D, Liu J, Yang K, Wu G, Liu H. Antitumor activity of SAHA, anovel histone deacetylase inhibitor, against murine B cell lymphoma A20cells in vitro and in vivo. Tumour Biol 2015;36:5051–61.
39. HuangD,DuanH,HuangH, TongX,HanY, RuG, et al. Cisplatin resistancein gastric cancer cells is associated with HER2 upregulation-inducedepithelial-mesenchymal transition. Sci Rep 2016;6:20502.
40. Greulich H, Chen TH, Feng W, Janne PA, Alvarez JV, Zappaterra M, et al.Oncogenic transformation by inhibitor-sensitive and -resistant EGFRmutants. PLoS Med 2005;2:e313.
41. El-Rifai W, Smith MF Jr, Li G, Beckler A, Carl VS, Montgomery E, et al.Gastric cancers overexpress DARPP-32 and a novel isoform, t-DARPP.Cancer Res 2002;62:4061–4.
42. Tan P, Yeoh KG. Genetics and molecular pathogenesis of gastric adeno-carcinoma. Gastroenterology 2015;149:1153–62e3.
43. Cancer Genome Atlas Research N, Analysis Working Group: Asan Univer-sity; BC Cancer Agency; Brigham and Women's Hospital; Broad Institute;Brown University, et al. Integrated genomic characterization of oesopha-geal carcinoma. Nature 2017;541:169–75.
44. Cancer Genome Atlas Research N. Comprehensive molecular characteri-zation of gastric adenocarcinoma. Nature 2014;513:202–9.
45. Samson P, Lockhart AC. Biologic therapy in esophageal and gastric malig-nancies: current therapies and future directions. J Gastrointest Oncol2017;8:418–29.
46. Katsha A, Belkhiri A, Goff L, El-Rifai W. Aurora kinase A in gastrointestinalcancers: time to target. Mol Cancer 2015;14:106.
47. Lordick F, Janjigian YY. Clinical impact of tumour biology in the man-agement of gastroesophageal cancer. Nat Rev ClinOncol 2016;13:348–60.
48. Taggart JV, Earle DP, Berliner RW, Welch WJ, Zubrod CG, Jailer JW, et al.Studies on the Chemotherapy of the HumanMalarias. V. The AntimalarialActivity of Quinacrine. J Clin Invest 1948;27(3 Pt 2):93–7.
49. Sokal DC, Hieu do T, Loan ND, Hubacher D, Nanda K, Weiner DH, et al.Safety of quinacrine contraceptive pellets: results from10-year follow-up inVietnam. Contraception 2008;78:66–72.
50. Changchien JJ, Chen YJ, Huang CH, Cheng TL, Lin SR, Chang LS. Quin-acrine induces apoptosis in human leukemia K562 cells via p38 MAPK-elicited BCL2 down-regulation and suppression of ERK/c-Jun-mediatedBCL2L1 expression. Toxicol Appl Pharmacol 2015;284:33–41.
51. Guo C, Gasparian AV, Zhuang Z, Bosykh DA, Komar AA, Gudkov AV, et al.9-Aminoacridine-based anticancer drugs target the PI3K/AKT/mTOR, NF-kappaB and p53 pathways. Oncogene 2009;28:1151–61.
52. Wang W, Gallant JN, Katz SI, Dolloff NG, Smith CD, Abdulghani J, et al.Quinacrine sensitizes hepatocellular carcinoma cells to TRAIL and che-motherapeutic agents. Cancer Biol Ther 2011;12:229–38.
53. Bouamar H, Jiang D,Wang L, Lin AP, Ortega M, Aguiar RC. MicroRNA 155control of p53 activity is context dependent and mediated by Aicda andSocs1. Mol Cell Biol 2015;35:1329–40.
54. Bunz F, Hwang PM, Torrance C, Waldman T, Zhang Y, Dillehay L, et al.Disruption of p53 in human cancer cells alters the responses to therapeuticagents. J Clin Invest 1999;104:263–9.
55. Campanella C, D'Anneo A, Marino Gammazza A, Caruso Bavisotto C,Barone R, Emanuele S, et al. The histone deacetylase inhibitor SAHAinduces HSP60 nitration and its extracellular release by exosomal vesiclesin human lung-derived carcinoma cells. Oncotarget 2016;7:28849–67.
56. Schroer N, Pahne J, Walch B, Wickenhauser C, Smola S. Molecular patho-biology of human cervical high-grade lesions: paracrine STAT3 activationin tumor-instructed myeloid cells drives local MMP-9 expression. CancerRes 2011;71:87–97.
57. Liu Y, Denlinger CE, Rundall BK, Smith PW, Jones DR. Suberoylanilidehydroxamic acid induces Akt-mediated phosphorylation of p300, whichpromotes acetylation and transcriptional activation of RelA/p65. J BiolChem 2006;281:31359–68.
58. Li D, Marchenko ND, Moll UM. SAHA shows preferential cytotoxicity inmutant p53 cancer cells by destabilizingmutant p53 through inhibition ofthe HDAC6-Hsp90 chaperone axis. Cell Death Differ 2011;18:1904–13.
59. Lee H, Deng J, Xin H, Liu Y, Pardoll D, Yu H. A requirement of STAT3 DNAbinding precludes Th-1 immunostimulatory gene expression by NF-kap-paB in tumors. Cancer Res 2011;71:3772–80.
60. Godwin P, Baird AM, Heavey S, Barr MP, O'Byrne KJ, Gately K. Targetingnuclear factor-kappa B to overcome resistance to chemotherapy. FrontOncol 2013;3:120.
61. SongG,OuyangG, Bao S. The activationof Akt/PKB signaling pathway andcell survival. J Cell Mol Med 2005;9:59–71.
62. Lin L, Liu A, Peng Z, Lin HJ, Li PK, Li C, et al. STAT3 is necessary forproliferation and survival in colon cancer-initiating cells. Cancer Res2011;71:7226–37.
Clin Cancer Res; 24(8) April 15, 2018 Clinical Cancer Research1916
Zhu et al.
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716

2018;24:1905-1916. Published OnlineFirst January 31, 2018.Clin Cancer Res Shoumin Zhu, Zheng Chen, Lihong Wang, et al. Cancer Cell Death in Upper Gastrointestinal CancersA Combination of SAHA and Quinacrine Is Effective in Inducing
Updated version
10.1158/1078-0432.CCR-17-1716doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2018/01/31/1078-0432.CCR-17-1716.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/24/8/1905.full#ref-list-1
This article cites 62 articles, 19 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/24/8/1905To request permission to re-use all or part of this article, use this link
on January 9, 2021. © 2018 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 31, 2018; DOI: 10.1158/1078-0432.CCR-17-1716