Embed Size (px)
Citation preview

A Case Control Study on Physical
Health Components and
Cardiometabolic Risk Markers among
Elderly
Muhammad Kamil Che Hasan 9/21/2014 1

Outline
• Problem Statement
• Significant of Study
• General Objective
• Specific Objective
• Literature Review
• Study Flowchart
• Methodology
• Inclusion & Exclusion Criteria
• Data Analysis
• Discussion
• Conclusion
9/21/2014 2

Problem Statement
• Rising in trend of non-communicable diseases (e.g. diabetes mellitus, obesity, cardiovascular diseases) has become significant over the years
• Cardiometabolic diseases remain the leading cause of death and disabilities in the Malaysian population
• Abnormalities in physical (musculoskeletal) health were found associated with various health conditions.
9/21/2014 3
Significant of Study
• Relevance between physical health components and physiological profile among elderly is still lacking.
• The relationship between physical health status and cardiometabolic profile is not explored much.
• This study will add new knowledge in the relationship of alterations in physical health and changes in cardiometabolic risk markers.
• It may help identifying physical health disturbance and cardiometabolic disease target group for prevention and rehabilitation.
9/21/2014 4

General Objective
• To explore the relationship between physical health components and cardiometabolic risk markers among elderly with cardiometabolic disease.
9/21/2014 5

To measure physical health components in elderly with cardiometabolic diseases as follows: a.Cardiorespiratory endurance (6-Minutes Walk Test) b.Muscular strength (Arm Curl Test & Chair Stand Test) c.Agility (Timed-up-and Go Test) d.Flexibility (Back Scratch Test & Sit and Reach Test)
To compare physical health components and cardiometabolic risk markers between control and cardiometabolic group.
To investigate the relationship between physical health components and cardiometabolic risk markers among elderly with cardiometabolic diseases.
To determine cardiometabolic risk markers which are waist circumference, BMI, high-sensitivity C-reactive protein (hsCRP), serum adiponectin, fasting blood lipids (e.g. cholesterol, triglycerides, HDL, LDL), fasting glucose, fasting insulin and fasting insulin sensitivity (HOMAIR) in elderly with cardiometabolic diseases.
1
2
3
4
Specific Objective
9/21/2014 6

• Cardiometabolic disease is a condition with the presence of at least 3 of the 5 following metabolic abnormalities including central obesity, hypertension, insulin resistance, elevated level of triglycerides and low concentration of high-density lipoprotein
(Kelly 2012; Salvi et al. 2012; Gluba et al. 2012; Chang et al. 2009)
• Cardiometabolic risk factors are closely related to diabetes and cardiovascular disease which are fasting hyperglycemia, overweight/obesity, elevated systolic and diastolic blood pressure, and dyslipidemia.
(Vanuzzo et al. 2008)
• In geriatric populations, the speeds of walking and gait pattern are widely investigated in order to predict various health conditions such as dementia, muscle strength and stroke
(Newman et al. 2011; Ben et al. 2008; Inzitari 2007)
9/21/2014 7
Literature Review

• Normal gait profiles also can be applied as the reference for disability assessment, intervention and treatment planning
(Chiu & Wang 2007)
• Physical activity declines with increasing age (Purath et al. 2007)
• The increase of aging population may increase the number of individuals who are at risk of chronic disease.
(Christensen et al. 2009)
• Increased risk for sedentary lifestyle, declines in physical activities.
(Centers for Disease Control 2006)
9/21/2014 8
Literature Review

Study Flowchart
9/21/2014 9
Selection of subjects from UKM Medical Centre
Consent form and Sociodemographic Information Collection
Having at least 3 or more cardiometabolic diseases such as diabetes, obesity, hypertension, dyslipidemia, and cardiovascular diseases
CARDIOMETABOLIC GROUP CONTROL GROUP
Physical health components data will be obtained*: i. Cardiorepiratory fitness (6-minutes walk test)
ii. Body composition (Waist Circumference, Body-Mass Index)
iii. Muscular strength (Arm Curl Test, Chair Stand Test)
vi. Agility (Timed-up-and Go)
v. Flexibility (Back Scratch Test, Sit and Reach Test)
(*if the patient feel tired, the test will be done in two different times) &
International Physical Health Questionnaire
YES NO
9/21/2014 10
Blood Pressure Measurement &
Blood Sampling (10ml) for cardiometabolic markers:
i. Human Sensitivity C-Reactive Protein (hsCRP)
ii. Serum Adiponectin
iii. Fasting Glucose and Insulin
iv. Fasting Lipid Profile
Analysis & Results
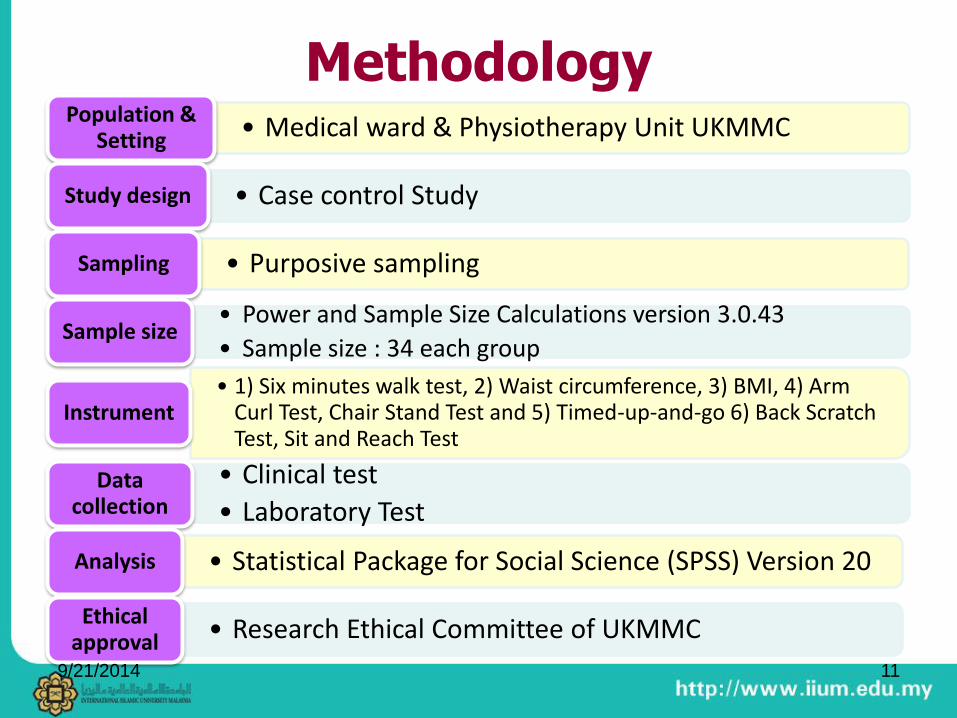
Methodology • Medical ward & Physiotherapy Unit UKMMC Population &
Setting
• Case control Study Study design
• Purposive sampling Sampling
• Power and Sample Size Calculations version 3.0.43
• Sample size : 34 each group Sample size
• 1) Six minutes walk test, 2) Waist circumference, 3) BMI, 4) Arm Curl Test, Chair Stand Test and 5) Timed-up-and-go 6) Back Scratch Test, Sit and Reach Test
Instrument
• Clinical test
• Laboratory Test Data
collection
• Statistical Package for Social Science (SPSS) Version 20 Analysis
• Research Ethical Committee of UKMMC Ethical approval
9/21/2014 11

• Aged between 60-75 years
• Physically independent
• Having at least three
cardiometabolic disease such as
diabetes, obesity, hypertension,
dyslipidemia, and cardiovascular
diseases (for cardiometabolic
group).
• Healthy or having not more than
two cardiometabolic disease (for
control group)
• Registered blindness
• Severe hearing impairment
• Uncontrolled epilepsy
• Progressive neurological disease
• Chronic disabling arthritis
• Use of walking aids
• Any neurological, skeletal muscle,
or joint disturbance that precluded
participation in testing.
• Have been advised by their
physician to refrain from exercise
for health reasons.
Inclusion Criteria
Exclusion Criteria
9/21/2014 12

Data Analysis
• Sociodemographic data – descriptive statistics
• Physical health components –independent t-test
• Cardiometabolic risk markers (Glucose, insulin, HOMA-IR, HDL, TG, LDL, Adiponectin, hsCRP) – Mann-Whitney U test.
• Cardiometabolic risk markers (Cholesterol, WC, BMI, SBP, DBP) – independent t-test
• Correlation between physical health components and cardiometabolic risk markers - Spearman rho correlation test.
9/21/2014 13

Sociodemographic Data
Control (n=34) Cardiometabolic (n=34)
Age (Mean ± SD) 65.79 ± 4.88 64.71 ± 4.01
Frequency Percentage (%) Frequency Percentage (%)
Gender
Male
Female
20
14
58.8
41.2
24
10
70.6
29.4
Race
Malay
Chinese
Indian
Others
22
9
3
0
64.7
26.5
8.8
0
23
5
3
3
67.7
14.7
8.8
8.8
Educational Level
Primary Level
Secondary Level
Tertiary Level
10
17
7
29.4
50.0
20.6
11
19
4
32.4
55.9
11.8
Smoking Status
Yes
No
6
28
17.6
82.4
0
34
0
100
Marital Status
Single
Married
0
34
0
100
1
33
2.9
97.1
Occupation
Own Business
Retired
11
23
32.4
67.6
7
27
20.6
79.4 9/21/2014 14

Physical Health Components
Physical Health Components Mean ± SD
Independent t-test
Control
(n=34)
Cardiometabolic
(n=34)
t-value
p-value
Chair Stand Test
(frequency in 30s) 11± 3 10 ± 3
1.022
0.311
Arm Curl Test
(frequency in 30s) 15 ± 3 14 ± 4
0.679
0.500
Chair Sit and Reach Test(cm) 0.89 ± 3.21 -0.49 ± 4.75
1.405
0.165
Time Up and Go (s) 6.94 ± 1.41 8.02 ± 3.38
-1.732
0.090
Six Minutes Walk Test (m) 409.52 ± 85.14 404.50 ± 87.20
0.241
0.811
Back Scratch Test (cm) -13.97 ± 2.99 -12.24 ± 2.12
-0.542
0.590
9/21/2014 15

Cardiometabolic Risk Markers
Cardiometabolic risk markers
Mean ± SD
t-value/
z-value
p-value
Control (n=34)
Cardiometabolic (n= 34)
Glucose (mmol/L) 5.10 ± 0.12 6.62 ± 0.42
-3.202b
0.001*
Insulin (mU/L) 3.37 ± 0.75 10.29 ± 2.68
-2.600 b
0.009*
HOMA-IR 0.79 ± 0.183 3.49 ± 1.09
-2.846 b
0.004*
Cholesterol (mmol/L) 4.24 ± 0.14 3.85 ± 0.15
1.873 a
0.065
High Density Lipoprotein (mmol/L) 1.04 ± 0.05 0.94 ± 0.05
-2.600 b
0.009
Triglycerides (mmol/L) 1.12 ± 0.11 1.49 ± 0.13
-2.846 b
0.004*
Low Density Lipoprotein (mmol/L) 2.97 ± 0.12 2.62 ± 0.13
-1.908 b
0.056*
Adiponectine (ug/ml) 3.87 ± 0.15 3.42 ± 0.19
-2.668 b
0.008
High Sensitivity C-Reactive Protein (mg/L) 0.31 ± 0.04 0.36 ± 0.05
-2.085 b
0.037
Waist Circumference (cm) 91.02 ± 1.92 97.18 ± 1.78
-1.717 a
0.086*
Body Mass Index (kg/m2) 26.19 ± 0.79 28.97 ± 0.92
-0.760 a
0.447*
Systolic (mmHg) 138.74 ± 17.95 144.03 ± 19.69
-1.159 a
0.251
Diastolic (mmHg) 84.15 ± 11.54 84.24 ± 7.90
-0.037a
0.971 9/21/2014 16

Correlation
• physical health components and cardiometabolic risk markers in plasma
Cardiometabolic Risks Markers in Plasma
Glucose Insulin HOMA-IR Cholesterol HDL TG LDL Adiponectin hsCRP
CST 0.265*
(0.029)
0.146
(0.235)
0.163
(0.185)
-0.050
(0.684)
-0.121
(0.326)
0.159
(0.195)
-0.040
(0.745)
0.062
(0.615)
-0.054
(0.664)
ACT 0.161
(0.191)
0.110
(0.371)
0.125
(0.308)
-0.114
(0.354)
-0.110
(0.372)
0.074
(0.549)
-0.094
(0.447)
-0.074
(0.546)
-0.058
(0.638)
CSRT -0.137
(0.264)
-0.276*
(0.023)
-0.291*
(0.016)
0.022
(0.860)
0.137
(0.265)
0.024
(0.846)
-0.070
(0.568)
0.205
(0.094)
-0.236
(0.052)
TUG 0.011
(0.927)
-0.087
(0.479)
-0.078
(0.526)
-0.109
(0.378)
0.011
(0.929)
-0.141
(0.253)
-0.139
(0.260)
0.060
(0.626)
0.128
(0.297)
SMWT 0.104
(0.398)
0.073
(0.555)
0.064
(0.603)
-0.020
(0.874)
-0.142
(0.274)
0.197
(0.107)
0.016
(0.897)
0.029
(0.815)
-0.159
(0.196)
BST -0.090
(0.467)
0.027
(0.830)
0.000
(0.998)
-0.189
(0.898)
0.066
(0.595)
-0.136
(0.269)
-0.203
(0.097)
0.036
(0.772)
-0.115
(0.351)
9/21/2014 17

Correlation • physical health component and other cardiometabolic risk
markers Cardiometabolic Risks Markers in Health Status
WC BMI Systolic Diastolic
CST -0.041
(0.738)
0.022
(0.857)
0.182
(0.138)
0.318**
(0.008)
ACT 0.027
(0.825)
0.020
(0.870)
0.036
(0.774)
0.172
(0.161)
CSRT -0.147
(0.233)
-0.119
(0.332)
0.043
(0.727)
-0.067
(0.588)
TUG -0.158
(0.199)
-0.100
(0.415)
-0.078
(0.529)
-0.116
(0.345)
SMWT -0.118
(0.338)
-0.022
(0.860)
-0.032
(0.794)
0.103
(0.402)
BST -0.276*
(0.022)
-0.289*
(0.017)
-0.022
(0.856)
-0.073
(0.553)
*Correlation is significant at the 0.05 level
**Correlation is significant at the 0.01 level
9/21/2014 18

Correlation
• waist circumference (WC) and BMI with other cardiometabolic risk markers
Blood Profile
Glucose Insulin HOMA-IR HDL TRIGL LDL Adipo. hsCRP
WC 0.139
(0.258)
0.399**
(0.001)
0.379**
(0.001)
-0.207
(0.090)
0.280**
(0.021)
0.097
(0.433)
-0.202
(0.099)
0.427**
(<0.001)
BMI 0.247*
(0.042)
0.485**
(<0.001)
0.488**
(<0.001)
-0.297*
(0.014)
0.272**
(0.025)
-0.016
(0.897)
-0.341**
(0.004)
0.550**
(<0.001)
**Correlation is significant at the 0.01 level
*Correlation is significant at the 0.05 level
9/21/2014 19

Discussion
• Cardiorespiratory endurance among two groups or elderly is comparable to each other.
(Mador et al. 2012)
• Lower and upper muscular strength has similar finding between the two groups.
(Forte et al. 2013; Goble et al. 2009)
• Flexibility and agility among control and cardiometabolic groups was found to have similar effect on elderly
(Hunter et al. 2013; Hong et al. 1999)
9/21/2014 20

Discussion - 2
• cardiometabolic group have combination of higher level in glucose, insulin and HOMA-IR as compared to the control group
(Tobisch et al. 2011; Hsieh et al. 2008; Doehner et al. 2005; Shepherd & Khan 1999)
• high density lipoprotein, triglycerides and high sensitivity
CRP has higher level in cardiometabolic group (Wang et al. 2013; Tofan et al. 2012; Hadaegh et al. 2006; Hsiao et al. 2013)
9/21/2014 21
Discussion - 3
• waist circumference has relationship with insulin, HOMA-IR, triglycerides, hsCRP.
• BMI was found significant having positive relationship with glucose, insulin, HOMA-IR , TG, and hsCRP.
• BMI was observed negative relationship with HDL and adiponectin.
(Cnop et al. 2003; Gavrila et al. 2003; Yang et al. 2002)
9/21/2014 22

Strength & Limitation
Strength
• test protocol and the use of instruments were practical for elderly
• latest cardiometabolic risk markers were used – hsCRP and adiponectin
Limitation
• could not represent a whole population because sample was recruited among volunteers in UKMMC
• there was a gap between day 1 and day 2, therefore large number of participants who could not attend day 2
9/21/2014 23
Nursing
• Orthopedic nurses particularly should highly emphasis the community to promote physical well-being in order to prevent further complications
• Platform for future nurse practitioner to include physical health test as part of their initial assessment
• Involvement in multi-disiplinary collaboration to strengthen the finding
9/21/2014 24

Conclusion
• Physical health components are not associated with cardiometabolic risk markers among elderly
• Waist circumference and body mass index has association in cardiometabolic risk markers. It is suggested that the higher BMI in a person, the higher risk to get cardiometabolic disease
• Elderly with good muscular strength and flexibility components in physical health leads the potential of preventing the cardiometabolic diseases by reducing the cardiometabolic risk markers
• Therefore, effective muscular strength and flexibility promotion strategies for physical health are urgently needed in preventing cardiometabolic diseases
9/21/2014 25

References • Ben Salem D, Walker PM, Aho S, Tavernier B, Giroud M, Tzourio C, Ricolfi F, Brunotte F. 2008. Brain flexibility and
balance and gait performances mark morphological and metabolic abnormalities in the elderly. J ClinNeurosci. 15(12):1360-5.
• Centers for Disease Control and Prevention. National Health and Nutrition Survey III 2009. Available at: http://www.cdc.gov/nchs/nhanes/nh3data. htm. Accessed August 07, 2012.
• Chang I.H., Han J.H., Myung S.C., et al. (2009); Association Between Metabolic Syndrome And Chronic Kidney Disease In The Korean Population. Nephrology; 14:321–6.
• Chiu, M.C. & Wang, M.J. 2007.The effect of gait speed and gender on perceived exertion, muscle activity, joint motion of lower extremity, ground reaction force and heart rate during normal walking. Gait & Posture. 25 (3): 385-392.
• Christensen K., Doblhammer G., Rau R., Vaupel J.W. (2009); Ageing Populations: The Challenges Ahead, Lancet; 374:1196-1208.
• Gluba A., Dimitri P.M., Gregory Y.H. Lip, Simon Hannam, Jacek Rysz, Maciej Banach (2012); Metabolic Syndrome And Renal Disease; International Journal Of Cardiology.
• Inzitari M, Newman AB, Yaffe K, Boudreau R, de Rekeneire N, Shorr R, Harris TB, Rosano C. 2007. Gait speed predicts decline in attention and psychomotor speed in older adults: the health aging and body composition study.Neuroepidemiology.29(3-4):156-62.
• Inzitari M, Pozzi C, Rinaldi LA, Masotti G, Marchionni N, Di Bari M. 2007. Cognitive and functional impairment in hypertensive brain microangiopathy.JNeurol Sci. 15;257(1-2):166-73
• Kelly Bosak, APRN (2012), Managing Metabolic Syndrome: Focus on Physical Activity; The Journal for Nurse Practitioners; Volume 8, Issue 3, 206-211.
• Korniloff K., Häkkinen A., Kautiainen H. (2010), Leisure-Time Physical Activity and Metabolic Syndrome Plus Depressive Symptoms in the FIN-D2D Survey; Preventive Medicine; 51, 466–470.
9/21/2014 26

References • Loprinzi P.D., Cardinal B. J. (2012), Interrelationships Among Physical Activity, Depression, Homocysteine, And
Metabolic Syndrome With Special Considerations By Sex; Preventive Medicine; 54; 388–392.
• National Academy Of Sciences; Does The Built Environment Influence Physical Activity? Examining The Evidence. Retrieved June 8, 2012, From, Http://www.Nap.Edu/Catalog/11203.Html, 2005.
• Newman AB, Simonsick EM, Naydeck BL, Boudreau RM, Kritchevsky SB, Nevitt MC, Pahor M, Satterfield S, Brach JS, Studenski SA, Harris TB. 2006. Association of long-distance corridor walk performance with mortality, cardiovascular disease, mobility limitation, and disability.JAMA. 3;295(17):2018-26.
• Purath J, Susan W. Buchholz, & Deborah L. Kark (2009); Physical Fitness Assessment of Older Adults In The Primary Care Setting; Journal of the American Academy of Nurse Practitioners; 21; 101–107.
• Rabieyah Mat & Hajar Md. Taha; Socio-Economic Characteristics Of the Elderly In Malaysia (2003), 21st Population Census Conference 19 – 21 November 2003 Kyoto, Japan; 1-20.
• Said Q., Marx C.M, Schwartz J.S., Ben-Joseph R., Brixner D.I. 2010. Impact of Body Mass Index on the Incidence of Cardiometabolic Risk Factors in Ambulatory Care Settings over 5 Years or More. Value in Health. 13(2).
• Salvi V., Virginia D'Ambrosio, Filippo Bogetto, Giuseppe Maina (2012), Metabolic Syndrome In Italian Patients With Bipolar Disorder: A 2-Year Follow-Up Study; Journal Of Affective Disorders; 136:599–603.
• Vanuzzo D, Pilotto L, Mirolo R, Pirelli S. 2008. Cardiovascular risk and cardiometabolic risk: an epidemiological evaluation. G ItalCardiol (Rome).9(4 Suppl 1):6S-17S.
• Wilkin L.D. and Haddock B.L. (2010), Health-Related Variables and Functional Fitness among Older Adults; Int’l. J. Aging and Human Development; Vol. 70(2); 107-118.
9/21/2014 27

Acknowledgements
• Associate Prof. Ho Siew Eng
• Dr. Nor Farah Mohamad Fauzi
• Mr. Leonard H. Joseph
• Dr. Muhammad Lokman Md Isa
• Ms. Quzaimah Zulkifle
• Ms. Farrah Ilyani Che Jamaludin
• Dr. Hanita Othman
• Pathology Laboratory staff
• Participants
9/21/2014 28

9/21/2014 29

Sample Size
9/21/2014 30
HOMA-IR
9/21/2014 31





























