Embed Size (px)
Citation preview

Revista de
Osteoporosis y Metabolismo Mineral
ISSN 1889-836XVolume 2
Supplement 4October 2010
www.revistadeosteoporosisymetabolismomineral.com
Epidemiology of osteoporotic fractures. Mortality anb morbidityJódar Gimeno E
Adherence to the treatment of osteoporosisGómez de Tejada Romero MJ
Osteoporosis: Concept and importance. Clinical pictureDel Pino Montes J
Zoledronic acid in the treatment of osteoporosisSosa Henríquez M, Groba Marco M, Díaz González JM
55
1100
1155
2211
S u p p l e m e n t

Revista de
Osteoporosis y Metabolismo Mineral
Pilar Aguado AcínJavier Alegre LópezMaría José Amérigo GarcíaAbdón Arbelo RodríguezMiguel Arias PacienciaEmilia Aznar VillacampaChesús Beltrán AuderaPere Benito RuizSantiago Benito UrbinaMiguel Bernard PinedaPedro Betancor LeónJosep Blanch i RubióJosé Antonio Blázquez CabreraJavier Calvo CataláMª Jesús Cancelo HidalgoJorge Cannata AndíaAntonio Cano SánchezCristina Carbonell AbellaJordi Carbonell AbellóPedro Carpintero BenítezEnrique Casado BurgosSantos Castañeda SanzFidencio Cons MolinaSonia Dapia RobledaManuel Díaz CurielBernardino Díaz López
Adolfo Díez PérezCasimira Domínguez CabreraAnna Enjuanes GuardiolaPedro Esbrit ArgüellesFernando Escobar JiménezJordi Farrerons MinguellaJosé Filgueira RubioJordi Fiter AresteJuan José García BorrásSergio García PérezJuan Alberto García VadilloEduardo Girona QuesadaCarlos Gómez AlonsoMª Jesús Gómez de Tejada RomeroJesús González MacíasEmilio González ReimersJenaro Graña GilSilvana di GregorioDaniel Grinberg VaismanNuria Guañabens GayFederico Hawkins CarranzaDiego Hernández HernándezJosé Luis Hernández HernándezGabriel Herrero-Beaumont CuencaEsteban Jódar GimenoFernando Lecanda Cordero
Pau Lluch MezquidaJosé Andrés López-Herce CidCarlos Lozano TonkinMª Luisa Mariñoso BarbaGuillermo Martínez Díaz-GuerraJulio Medina LuezasLeonardo Mellivobsky SaldierManuel Mesa RamosPedro Mezquita RayaAna Monegal BrancosJosefa Montoya GarcíaMaría Jesús Moro ÁlvarezManuel Muñoz TorresLaura Navarro CasadoManuel Naves GarcíaJosé Luis Neyro BilbaoXavier Nogués i SolánJoan Miquel Nolla SoléJosé Antonio Olmos MartínezNorberto Ortego CentenoSantiago Palacios Gil-AntuñanoEsteban Pérez AlonsoRamón Pérez CanoJosé Luis Pérez CastrillónLuis Pérez EdoPilar Peris Bernal
Concepción de la Piedra GordoJavier del Pino MontesJosé Manuel Quesada GómezEnrique Raya ÁlvarezRebeca Reyes GarcíaJosé Antonio Riancho MoralLuis de Rio BarqueroLuis Rodríguez ArboleyaMinerva Rodríguez GarcíaAntonia Rodríguez HernándezManuel Rodríguez PérezMontaña Román GarcíaInmaculada Ros VillamajóRafael Sánchez BorregoArmando Torres RamírezAntonio Torrijos EslavaCarmen Valdés y LlorcaCarmen Valero Díaz de LamadridAna Weruaga ReyJaime Zubieta Tabernero
METHODOLOGY AND DESIGN OF DATA
Pedro Saavedra SantanaJosé María Limiñana Cañal
Sociedad Española de Investigación Ósea y del Metabolismo Mineral (SEIOMM)
PresidentManuel Sosa Henríquez
Vice-presidentJavier del Pino Montes
TreasurerEsteban Jódar Gimeno
SecretariatMª Jesús Gómez de Tejada Romero
Avda. Capitán Haya, 60 (1ª planta)28020 Madrid (Spain)
Telf: +34-917499512Fax: +34-915708911
e-mail: [email protected]
http://www.seiomm.org
Editing
Avda. Reina Victoria, 47 (6º D)28003 Madrid
Telf./Fax 915 537 462e-mail: [email protected]
http://www.ibanezyplaza.com
Graphic designConcha García García
English translationAndrew Stephens
ImpresionImprenta Narcea
SVP32/09-R-CM
Legal depositAS-4777-09
ISSN 1889-836X
® Copyright SEIOMMAll rights reserved. The contents of the Journal may not bereproduced or transmitted by any process without the writ-ten authorisation of the holder of the rights to exploit thesaid contents.
Committee of experts
DirectorManuel Sosa Henríquez
Editor HeadMª Jesús Gómez de Tejada Romero
ED ITORIAL T ÉCNICA Y COMUNICAC IÓN
Ibáñez & Plaza Asociados, S. L.
E-mail: [email protected] version: http://www.revistadeosteoporosisymetabolismomineral.com

-This supplement has been sponsored by Gebro Pharma.-The publication reflects the views and findings of the authors signatories.-The active and listed medicines must comply with the instructions the technical data approved in Spain.

Revista de
Osteoporosis y Metabolismo Mineral
Epidemiology of osteoporotic fractures. Mortality anb morbidityJódar Gimeno E
Adherence to the treatment of osteoporosisGómez de Tejada Romero MJ
Osteoporosis: Concept and importance. Clinical pictureDel Pino Montes J
Zoledronic acid in the treatment of osteoporosisSosa Henríquez M, Groba Marco M, Díaz González JM
55
1100
1155
2211
ISSN 1889-836XVolume 2
Supplement 4October 2010


Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S5-S95
Jódar Gimeno EServicio de Endocrinología y Nutrición Clínica - Hospital Universitario Quirón Madrid - Facultad de Medicina - Universidad Europea de Madrid
Epidemiology of osteoporoticfractures. Mortality and morbidity
Correspondence: Esteban Jódar Gimeno - Servicio de Endocrinología y Nutrición Clínica - Hospital UniversitarioQuirón Madrid - Facultad de Medicina - Universidad Europea de Madrid - C/Diego de Velázquez, 2 - Pozuelo deAlarcón - Madrid (Spain)e-mail: [email protected]
IntroductionThe osteoporotic fracture has an enormous econo-mic impact, in addition to its effects on health. Inthe year 2000, it was estimated that there were 4million new fractures in Europe – some 8 fractu-res per minute, or one fracture every 8 seconds1.Of these, 0.89 million were hip fractures. Thedirect costs have been estimated at nearly 32billion euros, which it is expected will increase to77 billion euros by 2050 as a function of demogra-phic changes expected in Europe2.
The combined risk of suffering hip, forearmand clinical vertebral fractures is approximately40%, similar to that of developing cardiovasculardisease3. In Caucasian women, the risk of hip frac-ture over their lifetime is 1/6, higher than that ofsuffering breast cancer -1/9-4.
In our country it is calculated that 2 millionwomen have osteoporosis, putting its prevalenceat 26.1% of women over 50 years of age5. Morethan 25,000 fractures appear annually, from whichoriginate direct costs of more than 126 millioneuros, with indirect costs reaching 420 millioneuros annually6.
Incidence and prevalenceThe incidence of fractures is bimodal, with peaksin young people and in older people. In youngpeople the predominant fractures are of the largebones, normally after intense trauma, and withgreater frequency in males. Although in this groupbone resistance is not usually in question, theavailable data show that this factor may play somerole in its pathogeny7. From 35 years of age, theincidence of fractures in women ascends gradually
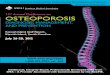
until it is double that of males. Before the availa-bility of studies which assessed radiographic ver-tebral fractures in place of clinical fractures, it wasthought that this peak was due to fractures of thehip and forearm. These studies have proved thatvertebral fractures contribute significantly to thisincidence (Figure1).
Fracture of the hipIn most populations the incidence of hip fractureincreases exponentially with age (Figure 1). Fromthe age of 50, the women to man ratio approxima-tes to 2 to 18. In conjunction with this, 98% of hipfractures appear in people over the age of 35years and 80% in women (given that women pre-dominate in later years). Most occur after a fallfrom a height equal to or less than their own.
Recent studies of the database of the GeneralPractitioners of the United Kingdom (GeneralPractice Research Database, GPRD), which inclu-des 6% of the population, has characterised theincidence of fractures adjusted for age and sex8.The global risk of hip fracture from 50 year of agein the United Kingdom is 11.4% and 3.1% forwomen and men, respectively. The greater part ofthis risk accumulates in the more advances ages insuch a way that the risk of suffering a hip fractu-re in the following 10 years at 50 is 0.3% while at80 years the risk is 8.7% - in the case of males0.2% and 2.9% respectively.
Hip fractures have a seasonal influence, with ahigher incidence in the winter, even though theyoccur principally in people’s homes, which seemsto suggest that this is due to worse conditions ofillumination or a slowing of neuromuscular refle-

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S5-S96
xes in colder periods. The direction and way offalling is significant, with a lateral fall directly onthe hip more likely to cause a fracture than a fron-tal forward fall9.
The incidence varies substantially from onepopulation to another and is usually higher inCaucasians than in other races. Across Europe, theproportion of hip fractures varies up to 7 timesbetween different countries, with our countrybeing among those with a low incidence10, andNorway, Sweden, Iceland, Denmark and the USAconsidered to have a high incidence11. Thus, envi-ronmental factors have an important role in theaetiology of hip fractures, although those studiedto date – smoking, alcohol consumption, physicalactivity, ethnic origin and/or migratory status –have not completely explained these differences.
In our country, a retrospective study whichassessed 13,195 hip fractures found a clear domi-nance of the female sex (74%) with an averageage of 80.7 ± 8.4 years. The average incidence was6.94 ± 0.44 fractures of the hip for each 1,000 inha-bitants per year. The prospective study from thissame work found a monthly prevalence of 0.60 ±0.04 fractures per 1,000 inhabitants with 74%being women and an average age of 81.4 ± 8.1years. The authors conclude that the average pre-valence in 2003 was 7.20 fractures per 1,000 inha-bitants, of whom a third had suffered a previouship fracture and only 18% having previously recei-ved medical treatment for osteoporosis12.
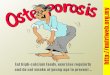
Vertebral fractureThe data from the European Vertebral OsteoporosisStudy (EVOS) have shown over recent years that thestandardised prevalence by age for vertebral fracturein Europe is 12.2% for men and 12.0% for womenbetween 50 and 79 years of age13. The prevalence offractures by age and sex in this population areshown in Figure 2. Although classically, it had been
thought that vertebral fractureswere more common in menthan in women, the data fromthe EVOS study show that this isnot so at younger ages; the pre-valence of deformities at betwe-en 60 and 75 years is similar, oreven higher in men, possiblydue to a higher incidence oftraumas. The majority of verte-bral fractures in older womenhappen in daily activities suchas picking up or lifting objectsmore than because of falls.Many vertebral fractures areasymptomatic and, what ismore, there is no unanimousagreement regarding the radio-graphic definition of vertebraldeformities. In studies whichuse radiographic screening, theincidence of vertebral deformi-ties has been estimated as beingthree times those of the hip,
although only a third of those result in a medicalconsultation14. The data from the EVOS study haveallowed a more precise assessment of radiographicvertebral fractures in a broad population. Betweenthe years of 75 and 89, the incidence of vertebralfractures is 13.6 per 1,000 inhabitant years in menand 29.3 per 1,000 person years for women13, whichis clearly higher than the 0.2 per 1,000 person yearsin men and 9.8 per 1,000 person years assessed inpeople between 75 to 85 years defined through cli-nical presentation in an earlier study in the US15. Thestandardised global incidence from the EVOS studywas 10.7 per 1,000 person years in women and 5.7per 1,000 person years in men.
From the comparison of the population dataavailable, it is evident that the heterogeneity of theprevalence of vertebral fractures is much lowerthan that found in fractures of the hip. This con-trasts with the much lower variability betweenpopulations of vertebral fractures identified by cli-nics or through hospitalisation.
Distal forearm fractureThe Colles fracture has a presentation profile dif-ferent from that of the hip and the vertebrae.There is an increase in the incidence in Caucasianwomen between 45 and 60 years of age followedby a plateau16, which has been related to a chan-ge in neuromuscular reflexes caused by aging, andby a tendency to suffer lateral or backward fallswhose impact they are attempted to avoid or cus-hion with the arms extended. The majority ofthese wrist fractures appear in women and morethan 50% appear in women over 65 years of age.The GPRD database shows a risk of vital fracturein women of 50 years of age of 16.6%, whilst at 70years this risk falls to 10.4%. The incidence inmales is significantly lower and does not changeexcessively with age (rest of life risk of 2.9% at 50years and 1.4% at 7017.
Figure 1. Incidence of fractures of the hip, radiographic vertebral andforearm, according to age and sex (adapted from refs 17 and 15)
��
� ��
�
�
��
�
�
��� Male
Female
Age (years)
Pre
vale
nce
(%
)
50
25
20
15
10
5
055 60 65 70 75

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S5-S97
Temporal projectionsThe progressive aging of the population, espe-cially in the western world, but also in developingcountries, will produce a spectacular increase inthe number of osteoporotic fractures. In fact, bet-ween 1990 and 2000, a worldwide increase in hipfractures of 25% was reported. The peak for thepresentation of hip fractures appears at 75-79years of age in both sexes; for the other fracturesthe peak appears at 50-59 years and reduces withage1. For 2050, the projection of the incidence ofvertebral fractures is predicted to increase by310% in males and 240% in women18.
However, recent European studies have shownthat the incidence, adjusted for age and sex, of hipfractures has been reducing over the last deca-de19,20. The steady growth in weight in the Westand better screening and treatment for osteoporo-sis have been suggested as reasons for this reduc-tion, which could counteract the progressive agingof the population of Europe.
Tendency to the aggregation of fractures inindividualsIn different epidemiological studies it has been sug-gest that patients with fragility fractures have anincreased risk of developing other types of fractures.Thus, for example, a previous vertebral deformityincreases from 7 to 10 times the risk of developinglater vertebral deformities21. The risk of suffering asecond hip fracture is also increased by a similarmagnitude. North American data show an increasedrisk of hip fracture of 1.4 times in women and of 2.7times in men after suffering a Colles fracture22. Theincreased risk of a later vertebral fracture in thesame cohort is 5.2 and 10.7 times. The EVOS study23,has shown that existing vertebral deformities predictan increased risk of hip fractures occurring of bet-
ween 2.8 and 4.5 times, which increase with thenumber of deformities and their intensity. The inci-dence of new vertebral fractures in the year after theappearance of a vertebral fracture is 19.2%, and theaccumulated incidence over 10 years of any type offracture after an earlier fracture is 70%24. All thesedata, taken together, show the importance of takingappropriate therapeutic measures after the diagnosisof an osteoporotic fracture.
Risk factors for fracturesThere are many factors associated with the risk ofdeveloping osteoporotic fractures. Some of these,notable among which is bone mineral density asthe most predictive, directly influence bone resis-tance, while others are related to falls and theircharacteristics. All these factors interact in eachindividual in a complex way. Although a detailedreview of these factors is outside the scope of thischapter, Table 1 lists the principal factors accor-ding to SEIOMM’s clinical practice guide25.
Mortality after osteoporotic fractureThe patterns of mortality after the most frequenttypes of fractures have been studied. In theRochester, USA cohort the rate of survival 5 yearsafter suffering a hip or vertebral fracture was 80%of that expected in men and women without frac-ture of a similar age14. In our country, 13% ofpatients who have suffered a fracture die in thefollowing 3 months. In the two years after the frac-ture, mortality reaches 38%6.
Mortality of hip fractureThe mortality associated with fractures of the hipis higher in men than in women and increaseswith age, as well as in those subjects with majorco-morbidities and a worse functional state pre-
Table 1. Risk factors for osteoporotic fracture
High risk Moderate risk
Mixed (Associatedwith BMD +independentcomponent)
Advanced AgePersonal History of Osteoporotic Fractures Maternal History of Hip FracturesLow weight* Glucocorticoids**High remodelled bone
Diabetes Mellitus Smoking
Associated withlow BMD
Hypogonadism in males Primary HyperPTHPrimary HyperPTHAnorexia Nervosa Prolonged immobilisation AnticomicialsMalabsoprtion
Feminine sex Early menopause***AmenorrheaRheumatoid ArthritisHyperthyroidismVitamin D deficitLow intake of calcium****
High risk: relative risk > 2. Moderate risk: relative risk > 1 y < 2. *Body mass index: < 20 kg/m2. **Period supe-rior to 3 months and but of 7,5 mg prednisone/day. ***Before 45 years. ****Inferior to 500-850 mg/day. The fac-tors related to the falls tendency and associated with the production of fractures are condidered independentfactors. BMD: bone mineral density.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S5-S9
fracture14. Around 8% of men and 3% of women ofmore than 50 years of age die while hospitaliseddue to fractures. In the United Kingdom, survivalafter suffering a fracture of the hip is 63.6% in menas against an expected 90.0%, and in women74.9% as against the 91.1% expected17. The risk ofdeath is maximum immediately after the fractureand reduces gradually with time. The cause ofdeath is not usually attributed to the fracturedirectly, but to other co-morbidities present.
Mortality after vertebral fractureIn contrast to what occurs with hip fractures, ver-tebral fractures are associated with an increasedrisk of death later in the year after the fracture14.Again, the excess risk appears to be due to co-morbidities present, but differently from the casewith hip fractures, it worsens over time. In theGPRD study the survival observed a year after suf-fering a vertebral fracture was 86.5% against 93.6%expected. At five years, the survival observed was56.5% against the 69.9% expected17.
Morbidity after osteoporotic fractureIn the USA, 7% of the survivors of any type of frac-ture have some kind of permanent limitation and8% require chronic hospital care. On average, awhite north American woman of 50 years has a13% probability of suffering a functional deteriora-tion after any kind of fracture26. In our country45% of patients who have suffered a vertebral frac-ture are left with functional damage and up to 50%can develop total or partial disability6.
Morbidity after hip fractureAs in relation to mortality, hip fractures are themain cause of later morbidity. Patients with hipfracture have a propensity to develop of acutecomplications such as ulcers due to decubitus,broncho-pneumonia and infections of the urinarytract. Perhaps the most significant complication inthe long term is difficulty in deambulation whichappears in 50% of cases. Age is a key determinantof what happens after the fracture: while only 14%of subjects receiving a fracture between 50 and 55years of age are sent to hospital for chronic care,up to 55% of those over 90 years of age need tocontinue to receive chronic care26.
Morbidity after vertebral fractureIn spite of the scarce or zero symptomology of themajority of vertebral fractures, their high fre-quency makes them responsible for a great num-ber of hospitalisations: almost 2,200 a year inEngland and Wales in patients older than 45 yearsof age. The principal consequences of a vertebralfracture are back pain, kyphosis and loss ofheight. The scores of the specific quality of life test(QUALEFFO) diminish in line with an increase inthe number of vertebral fractures27.
Morbidity after distal forearm fracturesFractures of the distal forearm do not appear toincrease mortality (morbidity?)17. While fractures ofthe wrist can impact adversely on daily activitiessuch as writing or cooking, few patients are leftcompletely incapacitated. However, up to 50% of
8
�
� � ��
�
�
�
�� � � � ��
�
�
Prevalence10,000/year
Prevalence10,000/year
Male
Age Age
Female
Figure 2. Prevalence of vertebral deformities by sex (adapted from ref. 13)
�
� �� � �
��
�
� � � � � � ��
�
�
� ��
��
�
�
�
�
�
�
400
300
200
100
0
400
300
200
100
0
50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+ 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
85+
Hip
X-ray vertebral
Wrist

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S5-S99
those subjects who suffer such a fracture state thatthey have a poor functional state 6 months onfrom the fracture26.
ConclusionsOsteoporosis is a disease which has an enormousimpact on public health, both from the point ofview of the individual, and collectively for healthsystems, economies and populations. The epide-miological characterisation and better knowledgeof the risk factors for osteoporotic fractures, com-bined with the development of drugs of provenefficacy, puts us in an excellent position for thedevelopment of preventative and therapeutic mea-sures, both populational, as well as for those indi-viduals at high risk.
Bibliography
1. Johnell O, Kanis JA. An estimate of the worldwide pre-valence and disability associated with osteoporoticfractures. Osteoporos Int 2006;17:1726-30.
2. Kanis JA, Johnell O. Requirements for DXA for themanagement of osteoporosis in Europe. OsteoporosInt 2005,16:229-32.
3. Kanis JA. Diagnosis of osteoporosis and assessment offracture risk. Lancet 2002;359:1929-33.
4. Cummings SR and Melton LJ. Epidemiology and outco-mes of osteoporotic fractures. Lancet 2002;359:1761-6.
5. Díaz Curiel M, García JJ, Carrasco JL, Honorato J, PérezCano R, Rapado A, et al. Prevalencia de osteoporosisdeterminada por densitometría en la población feme-nina española. Med Clin (Barc) 2001;116:86.
6. Gimeno A, Guanabens N, Monegal A, Peris P. 2005Consulta de... osteoporosis. Prous Science, Barcelona.
7. Goulding A, Jones IE, Taylor RW, Manning PJ, WilliamsSM. More broken bones: A 4-year double cohort studyof young girls with and without distal forearm fractu-res. J Bone Miner Res 2000;15:2011-8.
8. Melton LJ. Epidemiolory of fractures. In: Riggs BL,Melton LJ (eds.) Osteoporosis: Etiology, Diagnosisan&-Management. Raven Press, New York, NY, USA,1988;133-54.
9. Nevitt MC, Cummings SR. Type of fall and risk of hipand wrist fractures: The study of osteoporotic fractu-res. The Study of Osteoporotic Fractures ResearchGroup. J Am Geriatr Soc 1993;41:1226-34.
10. Johnell 0, Gullberg B, Allander E, Kanis JA. The appa-rent incidence of hip fracture in Europe: A study ofnational register sources. MEDOS Study Group.Osteoporos Int 1992;2:298-302.
11. Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A,Ogelsby P, et al. International variations in hip fractu-re probabilities: implications for risk assessment. JBone Miner Res 2002;17:1237-42.
12. Herrera A, Martínez AA, Ferrández L, Gil E, Moreno A.Epidemiology of osteoporotic hip fractures in Spain.Int Orthop 2006;30:11-4.
13. O’Neill TW, Felsenberg D, Varlow J, Cooper C, KanisJA, Silman AJ. The prevalence of vertebral deformity inEuropean men and women: The European VertebralOsteoporosis Study. J Bone Miner Res 1996;11:1010-8.
14. Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ.Incidence of clinically diagnosed vertebral fractures: Apopulation-based study in Rochester, Minnesota, 1985-1989. J Bone Miner Res 1992;7:221-227.
15. The European Prospective Osteoporosis Study (EPOS)Group. Incidence of vertebral fracture in Europe:Results from the European Prospective OsteoporosisStudy (EPOS). J Bone Miner Res 2002;17:716-24.
16. Melton LJ, Cooper C. Magnitude and impact of osteo-porosis and fractures. In: Marcus R, Feldman D, KelseyJ (eds.) Osteoporosis, 2nd ed. Academic Press, SanDiego, CA, USA, 2001;pp.557-67.
17. van Staa TP, Dennison EM, Leufkens HG, Cooper C.Epidemiology of fractures in England and Wales. Bone2001;29:517-22.
18. Gullberg B, Johnell O, Kanis JA. World-wide projec-tions for hip fracture. Osteoporos Int 1997;7:407-10.
19. Chevalley T, Guilley E, Herrmann FR, Hoffmeyer P,Rapin CH, Rizzoli R. Incidence of hip fracture over a10-year period (1991-2000): Reversal of a seculartrend. Bone 2007;40:1284-9.
20. Kannus P. Niemi S, Parkkari J, Palvanen M, Vuori I,Jarvinen M. Nationwide decline in incidence of hipfracture. J Bone Miner Res 2006;21:1836-8.
21. Ross PD, Davis JW, Epstein RS, Wasnich RD. Pre-exis-ting fractures and bone mass predict vertebral fractureincidence in women. Ann Intern Med 1991;114:919-23.
22. Cuddihy MT, Gabriel SE, Crowson CS, O’Fallon WM,Melton LJ. Forearm fractures as predictors of subse-quent osteoporotic fractures. Osteoporos Int1999;9:469-75.
23. Ismail AA, Cockerill W, Cooper C, Finn JD, AbendrothK, Parisi G, et al. Prevalent vertebral deformity predictsincident hip though not distal forearm fracture: Resultsfrom the European Prospective Osteoporosis Study.Osteoporos Int 2001;12:535-9.
24. Lindsay R, Silverman SL, Cooper C, Hanley DA, BartonI, Broy SB, et al. Risk of new vertebral fracture in theyear following a fracture. JAMA 2001;285:320-3.
25. González Macías J Guañabens Gay N, Gómez AlonsoC, del Río L, Barquero M, Muñoz Torres M, et al.(2008) Guías de práctica clínica en la osteoporosisposmenopáusica, glucocorticoidea y del varón.Sociedad Española de Investigación Ósea Y delMetabolismo Mineral, Rev Clin Esp 2008;208(Suppl1):1-24.
26. Chrischilles EA, Butler CD, Davis CS, Wallace RB. Amodel of lifetime osteoporosis impact. Arch InternMed 1991;151:2026-32.
27. Oleksik A, Lips P, Dawson A, Minshall ME, Shen W,Cooper C, et al. Health-related quality of life in pos-tmenopausal women with low BMD with or withoutprevalent vertebral fractures. J Bone Miner Res2000;15:1384-92.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S10-S1410
Gómez de Tejada Romero MJDepartamento de Medicina - Facultad de Ciencias de la Salud - Universidad de Sevilla (Spain)
Adherence in the treatment ofosteoporosis
e-mail: [email protected]
SummaryTherapeutic compliance is of great importance ifthe demonstrable efficacy of drugs is to be repro-duced in clinical practice. It has been sufficientlydemonstrated that there is a lack of adherence inthe pharmacological treatment of osteoporosis.The factors which influence this are highly diver-se and complex, with some dependent on the tre-atment itself, whether in the drug (efficacy, secon-dary effects) or in its administration regime (fre-quency, mode of administration). The appearanceof every day more efficacious drugs, with morespaced out administration periods and modes ofadministration which reduce undesirable secon-dary effects, diminish considerably the rate ofabandonment of treatment for osteoporosis.However, these improved drugs should be com-plemented with an appropriate doctor-patientrelationship, aimed at instructing and educatingthe latter and at maintaining their interest, toachieve a proper adherence to treatment, andthus, the maximum efficacy of the drugs.
Introduction. The size of the problemThe importance of osteoporosis lies in the fact thatit predisposes the appearance of fractures, whichmeans that it constitutes a major health problem1,2.The fractures most commonly associated withosteoporosis are vertebral, hip and the distalradius, or Colles, fractures3. It has been estimatedthat the risk of a patient with osteoporosis of suf-fering any fracture during the rest of their lifevaries between 40-50% in women and between13% and 22% in men, and, in the specific case ofhip fracture, the risk for a white woman is 17.5%,while for a man it is 6% 1,2,4.
All these fractures have a high level of morbi-dity and result in a high social-health cost4,5: for
example, approximately 25% of vertebral fracturesand practically all fractures of the hip require hos-pitalisation2. But, in addition, osteoporotic fractu-res, especially of the hip, have a considerablemortality. Indeed, studies carried out in thiscountry show that at the end of one year after ahip fracture approximately 30% of patients havedied, increasing to 40% when the follow up isextended to two years6-10. Other studies have des-cribed a reduction in survival at 5 years of 15%after a hip fracture, observing that the greater partof the deaths occur in the first six months after it2.
Osteoporosis is a chronic process, usuallyasymptomatic, which deteriorates the bone,making it susceptible to fracture. The ultimateobjective in the treatment of osteoporosis is tominimise the risk of suffering new fractures11-14.There is no drug which reduces this risk to zero:most of the drugs available nowadays for the tre-atment of osteoporosis obtain reductions of bet-ween 40% and 65%11-14, even when the medicationis taken continuously during a period of timewhich varies between 3 and 5 years. These cir-cumstances (lack of symptoms, necessity for pro-longed treatment) means that, as happens withother similar diseases (arterial hypertension,hypercholesterolemia, diabetes mellitus), theabandonment by the patient of their medication iscommon, and for many diverse reasons.Institutions such as the World Health Organisationand the American Heart Association recognise thatone of the main problems in the treatment ofchronic diseases in developed countries is non-compliance on the part of patients in the correcttaking of their medicines15,16.
With reference specifically to osteoporosis,multiple studies have demonstrated deficiencies inadherence to treatment by patients, and this has

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S10-S1411
been studied with all drugs used: calcitonin, oes-trogen therapy, raloxifen, teriparatide and biphos-phonates17-22, and some have even compared theabandonment of osteoporosis treatment depen-ding on which drug is being used. The existingworks are highly varied, and often have contradic-tory results23-28. The disparity in the populationsstudied and the methodologies applied explainthe difficulties in comparing results. However, allthese studies agree on the fact that adherence toosteoporosis treatment is, in general, low, and thatin the first year the percentage abandonment isfound to be between 30% and 50% in most cases.
The success of treatment for osteoporosisdepends to a great extent on adherenceIt is evident that those patients who take theirmedicine for osteoporosis regularly have betterresults, both in reference to changes in bonemineral density29, and, more importantly, in thereduction of the rate of fractures and a decrease inmortality30,31. A study carried out by Siris et al. in abroad population of postmenopausal women ofover 45 years of age, for whom had been indica-ted a biphosphonate as a treatment for osteoporo-sis, showed that, after 2 years of follow up, thosewomen who took the treatment correctly (43%)had a reduction of risk of fracture, both vertebraland non-vertebral, 21% higher than those patientswho did not correctly follow the treatment32.Earlier, Caro et al. had obtained similar results, fin-ding a reduction in the appearance of new fractu-res higher (16%) among those patients who werecompliant, as opposed to those who were not. Inthis study the period of follow up was also 2years, and the drugs evaluated were calcitonin,hormone replacement therapy and biphosphona-tes33. The same authors repeated the study, usinga broader database, with a cohort of more than38,000 women affected by osteoporosis, andobtained similar figures: poor adherence to treat-ment was associated with an increase in the riskof fracture of 17% after a follow up of 1.7 years34.These results are corroborated by those obtainedin other studies35,37.
The appropriate adherence to treatment is notonly beneficial for the health of the patients, butalso results in improved cost-effectiveness for thedrug therapy for osteoporosis38.
The importance of the frequency of admi-nistration in the adherence to treatment forosteoporosisPoor adherence to treatment for osteoporosis isdependent on many factors39,40. We have alreadyindicated at the start that low or zero symptomo-logy of the disease, and its being chronic, are twoof the most important. Other factors which havean influence on adherence are patient-dependent:age, state of health, socio-cultural position. Othersare dependent on the medical action taken (moti-vation, follow up, carrying out of tests which iden-tify the state of the disease). And finally, there arefactors dependent on the type of drug used in the
treatment: secondary effects, efficacy, mode andfrequency of administration. Therefore, adherenceis complex and difficult to quantify41. The modifi-cation of the factors which negatively influencetreatment compliance is one of the objectives allprofessionals should have when antiosteoporotictherapy is prescribed.
Up until now, the main interest in improvingadherence has been centred on drug-dependentfactors. In general, the drug treatments for osteo-porosis have few secondary effects, and only afew infrequent effects could be considered to beserious. On the other hand, over time ever moreefficacious and powerful drugs have been develo-ped, varying the modes of administration andlengthening the frequency of dosage, all intended,ultimately, to improve adherence42,43.
The biphosphonates and adherence in thetreatment of osteoporosisThe biphosphonates constitute the group of drugsmost used in the treatment of osteoporosis44,45, andare considered to be the first choice for the treat-ment of osteoporosis in our ambit46. The gastroin-testinal secondary effects of the biphosphonates,the motive for abandonment of treatment in a highpercentage of cases47, necessitated the finding ofpreparations whose administration was more spa-ced out, and whose mode of administration wasdifferent from oral: what were initially daily dosesbecame weekly administration in the case of alen-dronate48 and risedronate49, and monthly oraladministration became quarterly intravenous inthe case of ibandronate50,51. The last biphosphona-te to be marketed for the treatment of osteoporo-sis, zoledronate, is for annual, intravenous admi-nistration52, which ensures, at least, complianceand therapeutic efficacy over a year, which is veryimportant in view of the high number of abandon-ments of treatment which happen over thisperiod53-55.
So, all these changes in the administration regi-mes of the biphosphonates can improve adheren-ce in the long term drug treatment of osteoporoticpatients56,57. The beneficial results of this have beendemonstrated in different studies. Penning vanBest et al. used a database in the Netherlands ofthe dispensation of drugs over a year, and foundthat, of 2,124 women who started therapy withbiphosphonates, 51.9% of those to whom thedrugs were administered weekly continued treat-ment, but only 42% of those taking a daily dosecontinued treatment, with different types ofbiphosphonates used (etidronate, alendronate orrisedronate)58. Cramer et al. studied 2,741 womenin treatment with biphosphonates and observedthat, at the end of a year, persistence was 44.2% inthose who had taken the biphosphonates weekly,as against 31.7% among those who took themdaily59.
In another study carried out in the UnitedStates, Ettinger et al. analysed the sale of prescrip-tions of alendronate and risedronate in more than211,000 women. They found that, at the end of a

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S10-S1412
year, 56.7% of those patients who had takenbiphosphonates weekly continued to receive thedrug, as against 39% of those who had taken itdaily. However, the authors noted that more than40% of patients did not continue with treatmentwith weekly biphosphonates, and suggested thatformulations which allowed a more spaced outadministration could improve therapeutic com-pliance60. Cramer et al. in a work carried out in atotal of 15,640 women in the United Kingdom,France and the United States, found that after ayear, the persistence of patients with biphospho-nates was higher in those who received the medi-cation weekly, compared to those who received itdaily: 44% vs 32% respectively in the UntiedStates; 52% vs 40% in the United Kingdom; and51% vs 44% in France; in all cases the value of p< 0.00161.
In the study known as PERSIST, adherence totreatment at 6 months in a group of women whoreceived ibandronate monthly was compared withanother group which took alendronate weekly,and it was found that 56.6% of those who took themonthly treatment continued with treatment asopposed to 38.6% of those who took alendronateweekly62. We have not found a study which com-pares the adherence to treatment between biphos-phonates with an annual dose and those adminis-tered more frequently.
On the other hand, there are studies whoseobjective was to record the preferences of patientswith osteoporosis in respect to the pharmacologi-cal preparations for their treatment, in which itwas observed that, as a general rule, patients pre-fer a more spaced out administration of treat-ment63-65. A multicentric, randomised, double blindstudy carried out by McLung et al. to assess thesafety and efficacy of a single intravenous dose of5 mg of zoledronic acid vs 70 mg of alendronatetaken orally, weekly, carried out in 225 womenwith postmenopausal osteoporosis who had pre-viously received weekly treatment with alendrona-te, found that 78.7% of patients expressed theirpreference for an annual intravenous treatment asopposed to a weekly oral treatment66, equal to thatstated by the majority of patients participating in asimilar study carried out by Saag et al.67.
However, although a higher adherence to tre-atment is seen with doses at longer intervals, it isnotable that almost all the studies also concludethat the percentage of patients receiving thecorrect medication is sub-optimal, and this is thecase whatever the mode of administration. Thisindicates that, as we have suggested earlier, thera-peutic compliance in osteoporosis is complex, anddependent on diverse factors not only related tothe drug, but also to the patient and their surroun-dings, as well as to the medical action taken. Areview by Cochrane, Hayes et al.68 indicates thatpatients take approximately half the medicationprescribed. Analysing a series of interventionstaken to increase adherence to treatment, theyfound that those that were sure to be efficaciousin the long term were complex to implement.
Included amongst these interventions were provi-sion of detailed information, self-monitoring bypatients, advice, telephone reminders, family sup-port and psychological treatment. But they conclu-ded that, taken as a whole, the results were ratherpoor, recommending that new studies dealingwith the improvement of adherence to treatmentbe carried out.
In view of these results, it is evident that theinclusion in the therapeutic arsenal for osteoporo-sis of more powerful drugs, which can be admi-nistered at greater intervals of time and in wayswhich cause fewer secondary effects, increaseconsiderably adherence to treatment. But weshould not forget that in conjunction with theseimproved drugs we should address other adheren-ce factors related to the patients themselves, aswell as proceeding with medical/health interven-tions which support and promote therapeuticcompliance.
Bibliography
1. Dennison E, Cooper C. Epidemiology of osteoporoticfractures. Horm Res 2000;54(Suppl 1):S58-S63.
2. Johnell O, Kanis J. Epidemiology of osteoporotic frac-tures. Osteoporos Int 2005;16(Suppl 2):S3-S7.
3. Dennison E, Mohamed MA, Cooper C. Epidemiologyof osteoporosis. Rheum Dis Clin North Am2006;32:617-29.
4. Cummings SR, Melton LJ III. Epidemiology and outco-mes of osteoporotic fractures. Lancet 2002;359:1761-7.
5. Burge R, Dawson-Hughes B, Solomon DH, Wong JB,King A, Tosteson A. Incidence and economic burdenof osteoporosis-related fractures in the United States,2005-2025. J Bone Miner Res 2007;22:465-75.
6. Sosa M, Segarra MC, Hernández D, González A,Limiñana JM, Betancor P. Epidemiology of proximalfemoral fracture in Gran Canaria (Canary Islands). AgeAgeing 1993;22:285-8.
7. Sosa Henríquez M, Segarra Sánchez MC, LimiñanaCañal JM, Priego López M, Betancor León P. Fracturaosteoporótica de la extremidad proximal del fémur.Relación con el hábitat y diferencias hospitalarias. RevEsp Enf Metab Oseas 1993;2:26-9.
8. Sosa Henríquez M, Segarra Sánchez MC, Limiñana CañalJM, Hernández Hernández D, González Pacheco A,Betancor León P. Morbilidad y mortalidad de la fracturaosteoporótica de la extremidad proximal del fémur trasun año de seguimiento. Med Clin (Barc) 1993;101:481-3.
9. Díez A, Puig J, Martínez MT, Díez JL, Aubia J, VivancosJ. Epidemiology of fractures of the proximal femurassociated with osteoporosis in Barcelona, Spain.Calcif Tissue Int 1989;44:382-6.
10. Sosa Henríquez M. La fractura osteoporótica de cade-ra en España. Rev Esp Enf Metab Oseas 1993;2:41-4.
11. Sambrook P, Cooper C. Osteoporosis. Lancet 2006;367:2010-8.
12. Sosa Henríquez M, Hernández Hernández D.Tratamiento de la osteoporosis. En: Sosa Henríquez M,editor. Medicine. Número extraordinario: Osteoporosis.Madrid: Ed. Doyma; 2006.p.35-9.
13. Rosen CJ. Postmenopausal osteoporosis. N Engl J Med2005;353:595-603.
14. Seeman E, Eisman JA. Treatment of osteoporosis: why,whom, when and how to treat. Med J Austral2004;180:298-303.
15. World Health Organization. Adherence to Long-termTherapies: Evidence for Action. WHO/MNC/03.01World Health Organization; 2003.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S10-S1413
16. American Heart Association. 2003. Report availablefrom: http://strokeconference.americanheart.org/inclu-des/pdfs/Sessions WednesdayNewspaper.pdf (acces-sed on 17 May 2006).
17. Tosteson AN, Grove MR, Hammond CS, Moncur MM,Ray GT, Hebert GM, et al. Early discontinuation of tre-atment for osteoporosis. Am J Med 2003;115:209-16.
18. Carnevale V, Nieddu L, Romagnoli E, Bona E,Piemonte S, Scillitani A, et al. Osteoporosis interven-tion in ambulatory patients with previous hip fracture:a multicentric, nationwide Italian survey. OsteoporosInt 2006;17:478-83.
19. Curtis JR, Westfall AO, Allison JJ, Freeman A, Saag KG.Channeling and adherence with alendronate and rise-dronate among glucocorticoid users. Osteoporos Int2006;17:1268-74.
20. Weycker D, Macarios D, Edelsberg J, Ester G.Compliance with drug therapy for postmenopausalosteoporosis. Osteoporos Int 2006:17:1645-52.
21. Papaioannou A, Ioannidis G, Adachi JD, Sebaldt RJ,Ferko N, Puglia M, et al. Adherence to bisphosphona-tes and hormona replacement therapy in a tertiary caresetting of patients in the CANDOO database.Osteoporos Int 2003:14:808-13.
22. Foster SA, Foley KA, Meadows ES, Johnston JA, WangSS, Pohl GM, et al. Adherence and persistence withteriparatide among patients with commercial,Medicare, and Medicaid insurance. Osteoporos Int2010; Aug 27. [Epub ahead of print].
23. Turbí C, Herrero-Beaumont G, Acebes JC, Torrijos A,Graña J, Miguélez R, et al. Compliance and satisfactionwith raloxifene versus alendronate for the treatment ofpostmenopausal osteoporosis in clinical practice: Anopen-label, prospective, nonrandomized, observatio-nal study. Clin Ther 2004;26:245-56.
24. Rossini M, Bianchi G, Di Munno O, Giannini S,Minisola S, Sinigaglia L, et al. Treatment ofOsteoporosis in clinical Practice (TOP) Study Group.Determinants of adherence to osteoporosis treatmentin clinical practice. Osteoporos Int 2006;17:914-21.
25. Papaioannou A, Kennedy CC, Dolovich L, Lau E,Adachi JD. Patient adherence to osteoporosis medica-tions: problems, consequences and management stra-tegies. Drugs Aging 2007;24:37-55.
26. McCombs JS, Thiebaud P, McLaughlin-Miley C, Shi J.Compliance with drug therapy for the treatment andprevention of osteoporosis. Maturitas 2004;48:271-8.
27. Pasion EG, Sivananthan SK, Kung AW, Chen SH, ChenYJ, Mirasol R, et al. Comparison of raloxifene and bis-phosphonates based on adherence and treatmentsatisfaction in postmenopausal Asian women. J BoneMiner Metab 2007;25:105-13.
28. Ringe JD, Christodoulakos GE, Mellström D, Petto H,Nickelsen T, Marín F, et al. Patient compliance withalendronate, risedronate and raloxifene for the treat-ment of osteoporosis in postmenopausal women. CurrMed Res Opin 2007;23:2677-87.
29. Yood RA, Emani S, Reed JI, Edelman Lewis B,Charpentier M, Lydick E. Compliance with pharmaco-logic therapy for osteoporosis. Osteoporos Int2003;14:965-8.
30. Patrick AR, Brookhart MA, Losina E, Schousboe JT,Cadarette SM, Mogun H, et al. The complex relationbetween bisphosphonate adherence and fracturereduction. J Clin Endocrinol Metab 2010;95:3251-9.
31. Lekkerkerker F, Kanis JA, Alsayed N, Bouvenot G,Burlet N, Cahall D, et al. Adherence to treatment ofosteoporosis: a need for study. Osteoporos Int2007;18:1311-7.
32. Siris ES, Harris ST, Rosen CJ, Barr CE, Arvesen JN,Abbott TA, et al. Adherence to bisphosphonate the-rapy and fracture rates in osteoporotic women: rela-tionship to vertebral and nonvertebral fractures from 2US claims databases. Mayo Clin Proc 2006;81:1013-22.
33. Caro JJ, Ishak KJ, Huybrechts KF, Raggio G, Naujoks C.The impact of compliance with osteoporosis therapyon fracture rates in actual practice. Osteoporos Int2004;15:1003-8.
34. Huybrechts KF, Ishak KJ, Caro JJ. Assessment of com-pliance with osteoporosis treatment and its consequen-ces in a managed care population. Bone 2006;38:922-8.
35. McCombs JS, Thiebaud P, McLaughlin-Miley C, Shi J.Compliance with drug therapies for the treatment andprevention of osteoporosis. Maturitas 2004;48:271-87.
36. Adachi J, Lynch N, Middelhoven H, Hunjan M, CowellW. The association between compliance and persisten-ce with bisphosphonate therapy and fracture risk: Areview. BMC Musculoskelet Disord 2007;8:97. doi:10.1186/1471-2474-8-97.
37. Van den Boogaard CHA, Breekveldt-Postman NS,Borggreve SE, Goettsch WG, Herings RMC. Persistentbisphosphonate use and the risk of osteoporotic frac-ture in clinical practice: a database analysis study. CurrMed Res Opin 2006;22:1757-64.
38. Hiligsmann M, Rabenda V, Gathon HJ, Ethgen O,Reginster JY. Potential clinical and economic impact ofnonadherence with osteoporosis medications. CalcifTissue Int 2010;83:202-10.
39. Zafran N, Liss Z, Peled R, Sherf, Reuveni H. Incidenceand causes for failure of treatment of women with pro-ven osteoporosis. Osteoporos Int 2005;16:1375-83.
40. Carr AJ, Thompson PW, Cooper. Factors associatedwith adherence and persistence to bisphosphonatetherapy in osteoporosis: a cross-sectional survey.Osteoporos Int 2006;17:1638-44.
41. Lee S, Glendenning P, Inderjeeth CA. Efficacy, sideeffects and route of administration are more importantthan frequency of doping of anti-osteoporotic treat-ments in determining patient adherence: a criticalreview of published articles from 1970 to 2009.Osteoporos Int 2010; Jun 30. [Epub ahead of print].
42. Register JY. Adherence and persistence: impact on out-comes and health care resources. Bone 2006;38:18-21.
43. Martens MG, Shaw H. Maximizing effectiveness of bis-phosphonate therapy for osteoporosis. South Med J2008;101:824-30
44. Sosa Henríquez M, Filgueira Rubio J. López-Herce CidJA. Díaz Curiel M, Lozano Tonkin C. del Castillo RuedaA, et al. ¿Qué opinan los internista españoles de laosteoporosis? Rev Clin Esp 2005;205:379-82.
45. Sociedad Española de Medicina Interna (SEMI).Protocolos. Osteoporosis. Madrid: Sociedad Españolade Medicina Interna y Scientific CommunicationManagement; 2004.
46. Sociedad Española de investigaciones óseas y metabo-lismo mineral (SEIOMM). Osteoporosis postmenopáu-sica. Guía de práctica clínica. Rev Clin Esp2003;203:496-506.
47. M. Sosa Henríquez, E. Jódar Gimeno. Bifosfonatos: prin-cipios básicos, farmacocinética y tolerancia gastrointes-tinal. En: J. Calaf i Alsina, editor. Bifosfonatos y osteo-porosis postmenopáusica. Barcelona: Ed. ScientificComunication Management SL; 2003;p.113-121.
48. Schnitzer T, Bone HG, Crepaldi G, Adami S, McClungM, Kiel D, et al. Therapeutic equivalence of alendro-nate 70 mg once-weekly and alendronate 10 mg dailyin the treatment of osteoporosis. Alendronate Once-Weekly Study Group. Aging (Milano) 2000;12:1-12.
49. Ilter E, Karalok H, Tufekci EC, Batur O. Efficacy andacceptability of risedronate 5 mg daily compared with35 mg once weekly for the treatment of postmenopau-sal osteoporosis. Climacteric 2006;9:129-34.
50. Reginster JY, Adami S, Lakatos P, Greenwald M, StepanJJ, Silverman SL et al. Efficacy and tolerability of once-monthly oral ibandronate in postmenopausal osteopo-rosis: 2 year results from the MOBILE study. AnnRheum Dis 2006;65:654-61.
51. Eisman JA, Civitelli R, Adami S, Czerwinski E, RecknorC, Prince R, et al. Efficacy and tolerability of intrave-nous ibandronate injections in postmenopausal osteo-porosis: 2-years results from DIVA study. J Rheum2008;35:488-97.
52. Black DM, Delmas PD, Eastell R, Reid IR, Boonen S,Cauley JA, et al. Once-yearly zoledronic acid for treat-ment of postmenopausal osteoporosis. N Engl J Med2007;356:1809-22.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S10-S1414
53. Lewiecki EM. Intravenous zoledronic acid for the treat-ment of osteoporosis. Curr Osteoporos Rep 2008;6:17-23.
54. Maricic M. The role of zoledronic acid in the manege-ment of osteoporosis. Clin Rheumatol 2010;29:1079-84.
55. Ringe JD. Development of clinical utility of zoledronicacid and patient considerations in the treatment ofosteoporosis. Patient Prefer Adherence 2010;4:231-45.
56. Boonen S, Vandershueren D, Venken K, Milisen K,Delforge M, Haentjens P. Recent developments in themanegement of postmenopausal osteoporosis withbisphosphonates: enhanced efficacy by enhancedcompliance. J Intern Med 2008;264:315-32.
57. Cosman F. Treatment of osteoporosis and preventionof new fractures: role of intravenously administeredbisphosphonates. Endocr Pract 2009;15:483-93.
58. Penning-van Beest FJ, Goettsch WG, Erkens JA,Herings RM. Determinants of persistence with bisphos-phonates: a study in women with postmenopausalosteoporosis. Clin Ther 2006;28:236-42.
59. Cramer JA, Amonkar MM, Hebborn A, Altman R.Compliance and persistence with bisphosphonatedosing regimens among women with postmenopausalosteoporosis. Curr Med Res Opin 2005;21:1453-60.
60. Ettinger MP, Gallagher R, MacCosbe PE. Medication per-sistence with weekly versus daily doses of orally admi-nistered bisphosphonates. Endocr Pract 2006;12:522-8.
61. Cramer JA, Lynch NO, Gaudin AF, Walker M, Cowell W.The effect of dosing frequency on compliance and per-sistence with bisphosphonate therapy in postmenopausalwomen: a comparison of studies in the United States, theUnited Kingdom, and France. Clin Ther 2006;28:1686-94.
62. Cooper A, Drake J, Brankin E; the PERSISTInvestigators. Treatment persistence with once-monthly ibandronate and patient support vs. once-weekly alendronate: results from the PERSIST study.Int J Clin Pract 2006;60:896-905.
63. Fraenkel L, Gulanski B, Wittink D. Patient treatmentpreferances for osteoporosis. Arthritis Rheum2006;55:729-35.
64. Emkey R, Koltun W, Beusterien K, Seidman L, Kivitz A,Devas V, et al. Patient preference for once-monthlyibandronate versus once-weekly alendronate in a ran-domized, open-label, cross-over trial: the BonivaAlendronate Trial in Osteoporosis (BALTO). Curr MedRes Opin 2005;21:1895-903.
65. Payer J, Killinger Z, Sulková I, Celec P. Preferences ofpatients receiving bisphosphonates - How to influencethe therapeutic adherence. Biomed Pharmacother 2007Aug 9; [Epub ahead of print].
66. McClung M, Recker R, Miller P, Fiske D, Minkoff J,Kriegman A, et al. Intravenous zoledronic acid 5 mg inthe treatment of postmenopausal women with lowbone density previously treated with alendronate.Bone 2007;41:122-8.
67. Saag K, Lindsay R, Kriegman A, Beamer E, Zhou W. Asingle zoledronic acid infusion reduces bone resorp-tion markers more rapidly than weekly oral alendrona-te in postmenopausal women with low bone mineraldensity. Bone 2007;40:1238-43.
68. Haynes RB, Yao X, Degani A, Kripalani S, Garg A,McDonald HP. Interventions to enhance medication adhe-rence. Cochrane Database Syst Rev 2005;4:CD000011.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2015
Del Pino Montes JProfesor Titular de Medicina - Universidad de Salamanca - Servicio de Reumatología - Hospital Universitario de Salamanca
Osteoporosis: Concept andimportance. Clinical picture
Correspondence: Javier del Pino Montes - Servicio de Reumatología - Hospital Universitario de Salamanca -Paseo San Vicente, 48-183 - 37007 Salamanca (Spain)e-mail: [email protected]
IntroductionOsteoporosis is a common disease, responsible ingreat part for the fractures which occur in peopleover 50 years of age. Due to diverse pathogenicmechanisms a reduction in bone mass is produ-ced, which is accompanied by an increase in bonefragility. Osteoporotic fractures are a health pro-blem of great magnitude due to their repercus-sions not only in the health and quality of life ofthe patient, but also for the economic and socialcosts which its treatments and their side effectsbrings.
Definition of osteoporosisOsteoporosis has probably accompanied huma-nity since its existence, but the current conceptand definition are very recent. The definition wasdecided in two key meetings of experts, the firstin 19931 and the more recent one, organised bythe NIH in March 20002, from which resulted twoseparate consensus documents. In the first ofthese, osteoporosis was defined as “a systematicskeletal disorder characterised by the reduction inbone mass and alterations in the microarchitectu-re of bone tissue, with the consequent increase inthe fragility of bone and its susceptibility to fractu-re”1. In the consensus of the year 2000, the defini-tion was simplified to indicate that it consisted ofa disease “in which bone resistance is deteriora-ted, which predisposes it to fracture”. In addition,it was specified that “ bone resistance is the resultof the integration of the density and quality ofbone”2. Viewed in this way, it is considered that acompromise of biomechanical function (resistan-ce) happens not only due to the loss of quantity,but also due to the deterioration of other ele-ments, such as the microarchitecture, on which
the quality of bone depends. No mention wasmade of aetiopathogenic causes or mechanisms,given that they could influence more than onecausal factor, and there are various pathogenicmechanisms from which could result in a reduc-tion in bone resistance. It is very interesting thatfrom the clinical point of view only the fracture ismentioned, which could reflect the poor clinicalexpression of the disease during its developmentbefore the fracture.
Much time has passed in achieving a consen-sus on this concept since the first observation in1830, when Jean Lobstein confirmed some largerthan usual holes in some human bones, which hedescribed as porous, giving birth to the term oste-oporosis. Its recognition as a clinical entity is dueto Fullen Allbright, who described postmenopau-sal osteoporosis in 1940 and related it to a reduc-tion in oestrogen3. The concept remained for along time as the equivalent of loss of bone mass.The continuation of this error has, without adoubt, been contributed to by the definition ofdensitometric osteoporosis proposed by the wor-king group of the World Health Organisation(WHO) which met in 19924.
It is important to distinguish between the twodefinitions which coexists at the moment. Theyrepresent two different approaches to the sameproblem, the diagnosis and assessment of risk offracture on the one hand, and the conceptual defi-nition on the other. Densitometric classification isan operational proposal for the assessment of riskof fracture using bone mineral density (BMD) cut-off points to diagnostic ends. It is worth remem-bering that a densitometric diagnosis of osteopo-rosis does not mean an absolute indication for tre-atment. And, on the contrary, some patients with

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2016
low bone mass, but not low enough to be diagno-sed with osteoporosis, may have fractures. It isalready indicated in the WHO technical reportcited, that other parameters such as age, speed ofbone loss or frequency of falls should be taken into account4. This approach towards the assessmentof risk of fracture is preferable. The existence ofosteoporosis, or diminished bone mineral density,is one more piece of data to be included in theassessment of the patient. Recently, the WHOstudy group has proposed a tool for the calcula-tion of risk of fracture called FRAX, which inclu-des a series of clinical parameters in addition toBMD for the evaluation of the risk of fractures5.From the practical and therapeutic points of viewthe approach which centres on the patient accor-ding their risk of fracture is more useful, than themore simplistic approach which sees osteoporosisonly in densitometric terms.
Some bone parametersIn the definition some concepts are introducedsuch as the mass, microarchitecture, resistance,density and quality of bone.
Bone mass and bone mineral density are rela-ted to the quantity of bone. Bone mass increasesduring the first decades of life until it reaches itsmaximum called “peak bone mass”, at between 20and 30 years of age6. It is possible to measurebone mass “in vivo” by calculating the BMD,which is expressed in g/cm2. Low bone mass is theconsequence of two variables: the peak bonemass achieved in youth and bone loss at later sta-ges. Osteoporosis is usually the consequence ofbone loss in adults, however, an individual whodoes not reach their optimum bone mass duringyouth may develop osteoporosis without therebeing great bone loss. So, insufficient bonegrowth in childhood and adolescence is as impor-tant as later bone loss in the development of oste-oporosis2. The WHO has established an operatio-nal definition based on levels or cut-off points ofBMD for white postmenopausal women. Thus,normal values of BMD are considered to be thoseabove -1 (SD) in relation the average for youngadults (T-score > -1); osteopenia entails values ofBMD between -1 and -2.5 SD (T-score between -1and -2.5); osteoporosis entails BMD values lowerthan -2.5 DE (T-score lower than -2.5) and esta-blished osteoporosis is when along with the aboveconditions are associated one or more osteoporo-tic fractures4. However, this classification shouldbe used for epidemiological studies, but it shouldnot be used in individuals as the sole criterion forthe assessment of the patient. BMD only explains70% of bone fragility7. For this reason, in the con-sensus of the year 2000, another element of boneresistance was introduced, which is bone quality.
Microarchitecture is one of the components notdirectly related to bone mass which was alreadyintroduced into the definition of osteoporosis in1993. Loss of bone affects bone mass and itsmicroarchitecture, and is especially important forthe resistance of trabecular bone. The increase in
the fragility of bone, when the number and thick-ness of trabeculae are reduced, has been confir-med in numerous biomechanical studies8.Techniques currently possible allow knowledge ofbone microarchitecture and its resistance “in vivo”by means of methods such as the micro-TC, and,although at the moment only used by researchers,may become useful for the clinical evaluation ofpatients in the not too distant future9.
Bone quality is one component of resistance,along with bone density10. It is a broad term, butintegrated into bone quality are considered to besome parameters such as microarchitecture, turno-ver, damage accumulation and bone mineralisa-tion. In a more generic way one may think of qua-lity all those elements related to bone resistance,as distinct from bone mass.
Risk of fractureA fracture occurs when a force, such as a trauma,is applied to an osteoporotic bone. In this sense,osteoporosis is a risk factor for fragility fractures.From the data of numerous epidemiological stu-dies diverse risk factors for low bone mass andfractures have been identified. It is useful to dis-tinguish between two types of risk factor, sincesome are related to the BMD, and therefore withsuffering osteoporosis, while the rest are associa-ted with osteoporotic fracture, whose preventionshould be the principle objective of therapeuticinterventions. Some of the risk factors for lowbone mass can be seen in Table 1. Greater consi-deration should be given to risk factors for fractu-re, such as low BMD itself, and others, indepen-dent of BMD, among which are found previoushistory of fragility fractures, family history of oste-oporotic fractures, thinness, active smoking, con-sumption of alcohol and an increase in bone tur-nover11. Not all these factors have the same predic-tive force for fractures and notable for their clini-cal importance are personal or family history offractures12-15.
Some extraskeletal circumstances may influen-ce the mechanism of production of fractures.Hence, it is useful to remember that fracturesdepend on the concurrence in an individual of afragile bone and a fall. It is not surprising that thefrequency of falls is also associated with a higherrisk of fractures16.
When the development of a cohort is observedit is possible to check how a group with negligi-ble fragility fractures occurs in subjects with BMDabove the level of osteoporosis17. Therefore, stra-tegies directed at the detection of those indivi-duals with osteoporosis are insufficient to preventfractures. It would seem to be more profitable todirect that effort to the identification of individualswith a high risk of fractures. Hence, the estimationof absolute risk at 10 years allows the approxima-tion of reality with greater objectivity. The WHOhas proposed a software tool FRAX, available on-line, which allows the evaluation of the absoluterisk of fracture at 10 years5. The calculation ismade using an algorithm which includes BMD and

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2017
a series of independent clinical factors which areincluded in Table 2. The strongest clinical factors,in addition to the BMD, are age, personal historyof fracture, family history, consumption of corti-coids and the existence of rheumatoid arthritis.
AetiopathologyIn the last decade we have seen a revolution inthe understanding of bone biology. Part of theintricate network of cytokines, growth factors andthe cell’s participation in the regulation of bonemetabolism and how to modify these cellular sig-nals in different situations are now understood.Osteoporosis is the consequence of an alterationin bone remodelling which consists of an imba-lance which favours resorption over formation.The result is low bone mass, and changes in themicroarchitecture18. There are various types ofosteoporosis which can be classified into twogroups, primary and secondary19.
The most common type of osteoporosis is pos-tmenopausal, which is linked to two conditions,the menopause and aging. In women the ceasingof ovary function, and the consequent reductionin oestrogens, is accompanied by a phase of acce-lerated bone loss. Treatment by substituting theoestrogens reverses, to a great degree, this situa-tion. The oestrogens reduce osteoclastogenesis bymeans of a complex, and not yet completelyunderstood, interaction of cellular signals andbone cells20. Their deficiency increases resorptionand the loss of bone mass and structure, whichtranslates into bone fragility.
Another type of primary osteoporosis is invo-lutive osteoporosis, which affects both men andwomen, and which is more associated with aging.The existence of a negative calcium balance anda certain degree of secondary hyperparathyroi-dism have been the pathogenic mechanisms lin-ked to this bone loss. However, recent studiessuggest that oestrogen deficiency may play a sig-nificant role in later stages of life, regulating thehomeostasis of extraskeletal calcium. The oestro-gens may modulate the cacium balance, favouringits intestinal absorption and limiting its renal elimi-nation. In addition, an active influence of the oes-trogens in the metabolism of vitamin D and itscapacity to reduce the secretory reserve of para-thormone (PTH), has been described. These cir-cumstances have allowed the development of aunitary model of involutive osteoporosis, in whichthe deficiency of oestrogens plays a central role21.
Male osteoporosis is less frequent than postme-nopausal osteoporosis. From the point of view ofusing the BMD, recommended as cut-off points foran indication of postmenopausal osteoporosis area T-score below -2.5 of the average for the youngpopulation22. The occurrence of primary osteopo-rosis in males appears to be lower than that forwomen. In the first situation the productionmechanism is principally of an involutive type.
The causes of secondary osteoporosis are thosewhich are produced as a consequence of a disea-se, or from taking pharmaceutical drugs. The most
common is osteoporosis due to glucocorticoids.The risk of fracture is independent of BMD and isboth related to the daily dose and the accumulateddose. Yet, even doses lower than 7.5 mg/day ofprednisone, or equivalent, increase the risk of ver-tebral fracture when the accumulated dose is lowerthan 1g23. When the treatment with glucocorticoidsis withdrawn the risk of fracture goes down, butremains higher in relation to patients who have nottaken them24. In general, we may consider that halfthose patients treated for 6 months with glucocor-ticoids will have osteoporosis. The greatest boneloss is produced during the first 3 months of treat-ment due to its effect in inhibiting the apoptosis ofthe osteoclasts25. This action is by empowered byan increase in the apoptosis of the osteoblasts witha reduction in bone formation. The adverse effectsof treatment also reach the muscle, which is atro-phied, in turn, losing force and resistance, whichpresents a risk of falls.
Importance of osteoporosisOsteoporosis has a great impact on the generalpopulation. Osteoporotic fractures impose a loadof great magnitude from a socioeconomic point of
Table 1. Some risk factors for low bone mass
Not modifiable Modifiable
Age Little physical exercise(sendentarism)
Sex (female) Diet poor in calcium
Genetic Hyperproteic diet
Menopause Smoking
Hypogonadism Alcohol abuse
Endocrinal diseases:Cushing, primaryhyperparathyroidism,hyperthyroidism
Thinness (BMI < 19kg/m2)
Rheumatologicaldiseases: Rheumatoidarthritis
Glucocorticoids
Nutritional diseases:malnutrition anorexianervosa
Immunosuppressors
Disease of the digestivesystem: celiac disease,severe hepatopathies
Anticoagulants
Neoplasias: multiplemyeloma Heparin
Proton pump inhibitors

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2018
view. It is a very common disease which affects150-200 million people in the world.Approximately half of these patients come fromthe developed countries of North America, Europeand Japan. In general terms, it is estimated thataround 33% of women over the age of 50 yearswill suffer from osteoporosis. Although measureshave been proposed to reduce the problem, oste-oporosis continues to be under-diagnosed andmany patients, even with fractures recognisable asosteoporotic, remain without treatment. The socialand political measures are not yet sufficient toaddress the prevention of this serious socio-healthproblem.
In addition to the personal repercussions dueits high morbi/mortality, osteoporosis generatesconsiderable socioeconomic costs. The analysis ofthese costs carry a high degree of uncertainty. Thecalculation is difficult and unreliable, since theavailable information is incomplete26.
The costs, as is logical, are not limited to thepharmacological or surgical interventions. Theyare divided into direct and indirect costs. Amongthe first are those due to hospitalisation, outpatientcare and drugs. These may be related to immedia-te assistive, social and hospital care, both shortand long term, and to drugs. The costs of hospi-talisation can be seen to be influenced by its dura-tion. Within the outpatient care are included visitsto the traumatologist, visits to other doctors, inclu-ding the general practitioner, nurse visits, physio-therapy, occupational therapy and telephoneassistance. Counted in the direct non-medicalcosts are social care and informal care. Services tobe taken into account within social care, amongothers, are adaptations to the home, home health
care, general home help and transport. Finally,among indirect costs, should be considered as keythe loss of production of the patient, or of thefamily who looks after them27. On the other hand,the reduction in quality of life related to health hasa significant social and individual cost.
Clinical manifestationsOsteoporosis is an asymptomatic disease. For thisreason it has been called the “silent epidemic”4. It isa mistake to consider that bone loss is accompaniedby musculoskeletal pain, and it is relatively commonthat patients are referred for this reason with thesuspicion of osteoporosis, especially women in theperi- or first years of the menopause.
The principle clinical manifestations are due toits complications, fractures. The most frequent fra-gility fractures are located in the spinal column,the wrist and the hip. They are usually classifiedin a more general way as vertebral or non-verte-bral. Among the non-vertebral fractures are alsoincluded those of the humerus, pelvis, ribs andother less frequent types. Not usually included asosteoporotic fractures are those of the finger, andcranium, but there are some doubts about fractu-re of the ankle21.
They are produced by a minor trauma, such asa simple fall from a standing position. For this rea-son also, they are known as fragility fractures.They appear principally after the age of 50 years,and that differentiates them from the traumaticfractures which predominate in youth. The clinicalmanifestations of these fractures are the same asother fractures in the same location, and areaccompanied with pain, loss of functional powerand deformity29.
The vertebral fracture is the most prevalent. Itstypical clinical presentation form is acute pain,although not infrequently it can be asymptomatic.It can be the consequence of a mechanical effortin carrying or lifting weight, but also can have noapparent cause. The most typical manifestation isacute, intense pain located in the spine, which isexacerbated with movement and reduces withrest. This becomes very incapacitating, impedingsleep. The intensity of the pain usually reducesafter the first 2-3 weeks, before disappearing after2-3 months. The pain may radiate towards the ribsor the legs, according to whether it proceeds fromthe dorsal or lumbar spine. However, almost twothirds of vertebral fractures are asymptomatic andcan only be confirmed by means of radiographyof the lumbar or dorsal spine. For this reasonthese are classified as clinical or morphometricfractures, the latter only evident through imagingtechniques30,31. In some patients, as a consequenceof structural changes in the spine there may deve-lop an instability of the spine, with paraspinalmuscular contraction, ligamentous tension andincongruity in the articular facets which may bethe cause of chronic axial pain32.
Thoracic vertebral fractures usually have a“cradle” compression from which originates thecharacteristic kyphosis of these patients (“the
Table 2. Variables included in the FRAX tool
- Age
- Sex
- Weight
- Stature
- Previous fracture
- Parents with hip fracture
- Active smoker
- Taking glucocorticoids
- Rheumatoid arthritis
- Secondary osteoporosis
- Excessive consumption of alcohol
- BMD in femoral neck, which nuances the overall
result of the other variables

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2019
widow’s hump”). In lumbar fractures the vertebraeare usually squashed in height the centre (devil’svertebrae). The loss of height of the vertebralbodies reduces the distance between the ribcageand the pelvis, which in some patients evenresults in the establishment of painful contact bet-ween the ribs and pelvis (costo-pelvic syndrome).The accumulation of vertebral crushing is transla-ted into a loss of height. Some authors considerthat a reduction of more than 3 cm in two yearsmay be a sign of vertebral fractures. It has beenproposed that the span of the higher extremities,a measure equal to the body height in youth, becompared with the height of the patient to detectreductions in height. It is of considerable interestthat rarely in osteoporotic vertebral fractures areobserved the neurological complications whichaccompany vertebral fractures of a different ori-gin33. The appearance of medullary or radicularneurological manifestations should make us thinkof a non-osteoporotic origin for a fracture32. Thesemodifications in the spine may cause difficulties inthoracic movement and affect breathing. Theabdomen loses capacity , and becomes prominent,with consequent modification the intestinal tract.The most serious fracture is that of the hip, gene-rally triggered by a fall. Although there are no datawhich support it, it has become common beliefthat in the presence of significant osteoporosis,the patient fractures their hip standing up, afterwhich they fall. The highest rate of mortality asso-ciated with osteoporosis is related to hip fractureand represents one of its most significant socialcosts. The causes of death are diverse and in manycases are not directly related to the fracture34. Themortality is 20-30% in the first year, which meansthat the risk of death increases by 2 to 10 timesthat expected in a population with similar charac-teristics35. Most cases require surgical intervention.But the repercussions of a hip fracture are notlimited to its hospital treatment, but also to thedeterioration of the quality of life. The majority ofpatients have residual disability and a percentageof cases lose the capacity to live an independentlife. For example, only a fifth of those patientswho walked unaided before the fracture can do so6 months after it27.
The Colles fracture has fewer repercussionsthan the two earlier ones. Some patients can expe-rience persistent local pain, functional incapacity,neuropathy and posttraumatic arthritis; in addi-tion, it is a significant risk factor for future presen-tation of vertebral or hip fractures27. Finally, thepsychological and social impact should be takeninto account, which may result in osteoporoticfractures. The development of depression is thepsychological disorder most frequently cited. Theappearance of anxiety, fear of new fractures, andother emotional reactions are also important, andinfluence the recuperation of those patients36. Therepercussions on families of patients with hip frac-ture and often with a great physical and psycholo-gical dependency, cannot sensibly be calculateddue to their complexity.
Bibliography
1. Consensus development conference: diagnosis,prophylaxis, and treatment of osteoporosis. Am J Med1993;94:646-50.
2. NIH Consensus Development Panel on OsteoporosisPrevention D, and Therapy. Osteoporosis prevention,diagnosis, and therapy. JAMA 2001;285:785-95.
3. Patlak M. Bone builders: the discoveries behind pre-venting and treating osteoporosis. FASEB J2001;15:1677E-E.
4. WHO. Assessment of fracture risk and its applicationto screening for postmenopausal osteoporosis. Reportof a WHO Study Group. World Health Organ Tech RepSer 1994;843:1-129.
5. Kanis JA, Johnell O, Oden A, Johansson H, McCloskeyE. FRAX and the assessment of fracture probability inmen and women from the UK. Osteoporos Int2008;19:385-97.
6. Mora S, Gilsanz V. Establishment of peak bone mass.Endocrinol Metab Clin North Am 2003;32:39-63.
7. Johnell O, O'Neill T, Felsenberg D, Kanis J, Cooper C,Silman AJ. Anthropometric measurements and verte-bral deformities. European Vertebral OsteoporosisStudy (EVOS) Group. Am J Epidemiol 1997;146:287-93.
8. Brandi ML. Microarchitecture, the key to bone quality.Rheumatology (Oxford) 2009;48(Suppl 4):iv3-8.
9. Genant HK, Engelke K, Prevrhal S. Advanced CT boneimaging in osteoporosis. Rheumatology (Oxford)2008;47(Suppl 4):iv9-16.
10. Recker RR, Barger-Lux MJ. The elusive concept ofbone quality. Curr Osteoporos Rep. 2004;2(3):97-100.
11. National Osteoporosis Foundation (NOF). Risk assess-ment. Physician´s Guide for the prevention and treat-ment of osteoporosis 2003.
12. Barrett-Connor E, Sajjan SG, Siris ES, Miller PD, ChenYT, Markson LE. Wrist fracture as a predictor of futurefractures in younger versus older postmenopausalwomen: results from the National Osteoporosis RiskAssessment (NORA). Osteoporos Int 2007.
13. Kanis JA, Borgstrom F, De Laet C, et al. Assessment offracture risk. Osteoporos Int 2005;16:581-9.
14. Kanis JA, Johansson H, Oden A, et al. A family historyof fracture and fracture risk: a meta-analysis. Bone2004;35:1029-37.
15. Roux C, Fechtenbaum J, Kolta S, Briot K, Girard M. Mildprevalent and incident vertebral fractures are risk factorsfor new fractures. Osteoporos Int 2007;18:1617-24.
16. Barrett-Connor E, Weiss TW, McHorney CA, Miller PD,Siris ES. Predictors of falls among postmenopausalwomen: results from the National Osteoporosis RiskAssessment (NORA). Osteoporos Int 2008.
17. Sornay-Rendu E, Munoz F, Garnero P, Duboeuf F,Delmas PD. Identification of osteopenic women athigh risk of fracture: the OFELY study. J Bone MinerRes 2005;20:1813-9.
18. Lane NE, Yao W. Developments in the scientificunderstanding of osteoporosis. Arthritis Res Ther2009;11:228.
19. Kok C, Sambrook PN. Secondary osteoporosis inpatients with an osteoporotic fracture. Best Pract ResClin Rheumatol 2009;23:769-79.
20. Raisz LG. Pathogenesis of osteoporosis: concepts, con-flicts, and prospects. J Clin Invest. 2005;115(12):3318-25.
21. Seeman E. Pathogenesis of bone fragility in womenand men. Lancet 2002;359:1841-50.
22. Kanis JA, McCloskey EV, Johansson H, Oden A, MeltonLJ, 3rd, Khaltaev N. A reference standard for the des-cription of osteoporosis. Bone 2008;42:467-75.
23. De Vries F, Bracke M, Leufkens HG, Lammers JW,Cooper C, Van Staa TP. Fracture risk with intermittenthigh-dose oral glucocorticoid therapy. Arthritis Rheum2007;56:208-14.
24. van Staa TP, Leufkens HG, Cooper C. The epidemio-logy of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int 2002;13:777-87.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S15-S2020
25. Natsui K, Tanaka K, Suda M, et al. High-dose glucocor-ticoid treatment induces rapid loss of trabecular bonemineral density and lean body mass. Osteoporos Int2006;17:105-8.
26. Stevenson M, Jones ML, De Nigris E, Brewer N, DavisS, Oakley J. A systematic review and economic evalua-tion of alendronate, etidronate, risedronate, raloxifeneand teriparatide for the prevention and treatment ofpostmenopausal osteoporosis. Health Technol Assess2005;9:1-160.
27. Johnell O, Kanis JA. An estimate of the worldwide pre-valence and disability associated with osteoporoticfractures. Osteoporos Int 2006;17:1726-33.
28. Adachi JD, Ioannidis G, Olszynski WP, et al. Theimpact of incident vertebral and non-vertebral fractu-res on health related quality of life in postmenopausalwomen. BMC Musculoskelet Disord 2002;3:11.
29. Compston J. Clinical and therapeutic aspects of osteo-porosis. Eur J Radiol 2009;71:388-91.
30. Cooper C, O'Neill T, Silman A. The epidemiology of
vertebral fractures. European Vertebral OsteoporosisStudy Group. Bone 1993;14(Suppl 1):S89-S97.
31. Gehlbach SH, Bigelow C, Heimisdottir M, May S,Walker M, Kirkwood JR. Recognition of vertebral frac-ture in a clinical setting. Osteoporos Int 2000;11:577-82.
32. Francis RM, Aspray TJ, Hide G, Sutcliffe AM, WilkinsonP. Back pain in osteoporotic vertebral fractures.Osteoporos Int 2007.
33. Green AD, Colon-Emeric CS, Bastian L, Drake MT,Lyles KW. Does this woman have osteoporosis? Jama2004;292:2890-900.
34. Parker MJ, Anand JK. What is the true mortality of hipfractures? Public Health 1991;105:443-6.
35. Johnell O, Kanis J. Epidemiology of osteoporotic frac-tures. Osteoporos Int 2005;16(Suppl 2):S3-S7.
36. Papaioannou A, Kennedy CC, Ioannidis G, et al. Theimpact of incident fractures on health-related quality oflife: 5 years of data from the Canadian MulticentreOsteoporosis Study. Osteoporos Int 2009;20:703-14.

Sosa Henríquez M, Groba Marco M, Díaz González JM1
1 Farmacéutico. Las Palmas de Gran CanariaUniversidad de La Palmas de Gran Canaria - Grupo de Investigación en Osteoporosis y Metabolismo Mineral - Hospital Universitario Insular -Servicio de Medicina Interna - Unidad Metabólica Ósea
Zoledronic acid in the treatmentof osteoporosis
Correspondence: Manuel Sosa Henríquez - C/Espronceda, 2 - 35005 Las Palmas de Gran Canaria (Spain)e-mail: [email protected]
IntroductionNowadays we have available a highly varied thera-peutic arsenal for the treatment of osteoporosis1.The biphosphonates constitute the group of drugsmost commonly used for the treatment of this dise-ase and are the first choice according to theSEIOMM guides2. Among the biphosphonates, zole-dronic acid is the most potent third generation nitro-genated biphosphonate currently on the market3,4.Its action mechanism means that it has a great affi-nity with the hydroxyapatite crystals of bone, aboveall in those areas of high bone turnover, reducingthe speed of bone remodelling. In turn it is releasedduring bone resorption and internalised by the oste-oclasts, which interfere in the metabolism and func-tion of these cells, and favour their apoptosis5.Zoledronic acid has an affinity for bonding withhydroxyapatite higher than other biphosphonates6
and is the most powerful inhibitor of farnesyl-diphosphate-synthase and of bone resorption7.
Zoledronic acid is the first drug which allowsannual treatment in postmenopausal patientsaffected by osteoporosis, or at high risk of fractu-re. The administration of 5 mg of zoledronic acidonce a year has been shown to be efficacious inthe reduction in risk of vertebral fractures inpatients with postmenopausal osteoporosis or hipfracture due to a recent light trauma8. In turn itproduces an increase in bone mineral density anda reduction in markers for bone turnover9. Beinggenerally well tolerated, its annual administrationmakes it a comfortable and efficacious treatmentoption, in such a way that the patient’s adherenceto treatment is not a problem, thus maintaining theprotection of bone over a whole year.
Therapeutic efficacya) In patients with postmenopausalosteoporosisThe reference study for the therapeutic efficacy ofzoledronic acid in the treatment of postmenopau-sal osteoporosis is called Health Outcomes andReduced Incidence with Zoledronic Acid Once-Yearly (HORIZON-PFT)8. It consists of a multicen-tre, randomised, double blind, placebo-controlledtrial of three years duration, which compared theefficacy of a single intravenous perfusion of 5 mgof zoledronic acid lasting 15 minutes, against aplacebo.
In order to carry out this study a total of 7,765patients were selected, between 65 and 89 yearsof age, with a T-Score ≤ -2.5 in the femoral neck,with or without data indicative of existing verte-bral fracture, or patients with a T-Score of ≤ -2.5and radiological proof of at least two light verte-bral fractures or one moderate vertebral fracture.Those patients previously treated with antiresorp-tive drugs were permitted to participate, with thepatients being classified into two groups as a func-tion of whether or not they had previously takendrugs against osteoporosis. The patients to whoma cleansing period could be applied, were ran-domly allocated to one of the groups. The firstgroup included patients who had not taken anypermitted drugs (calcitonin, raloxifen, tibolone,hormonal therapy, tamoxifen, ipriflavone,medroxyprogesterone), whilst in the secondgroup were classed patients who had taken per-mitted antiosteoporotic drugs. This excludedpatients who had taken, at any time, parathryroidhormone, sodium and strontium fluoride, anabo-
Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3021

lics or somatropin in the 6 months, or systemiccorticosteroids, orally or intravenously, in the 12months, prior to their incorporation into the trial.Blood concentrations of calcium higher than 2.75mmol/l or lower than 2.00 mmol/l, or a creatinineclearance of lower than 30.0 ml/minute in eitherof the two baseline visits, were also exclusion cri-teria. 3,889 patients were randomly assigned toreceive a single perfusion of 5 mg zoledronic acidover 15 minutes, and 3,876 to receive a placebo atthe baseline, at 12 months and at 24 months. Allthe patients received between 1,000 and 1,500 mgof calcium and between 400 and 1,200 UI of vita-min D orally.
The principal evaluation criteria were: theappearance of a new vertebral fracture (in thosepatients not treated with concomitant medicationagainst osteoporosis) and/or the hip fracture (inall patients). The secondary evaluation criteriawere bone mineral density, markers for bone tur-nover and results in terms of safety.
I. Effect on incidence of fractureThe objective of any antiosteoporotic treatment isthe prevention of fractures, wherever they arelocated. After three years of study, the incidenceof morphometric vertebral fractures in the grouptreated with a placebo was 10.9% as against 3.3%in the group treated with 5 mg of zoledronic acidadministered intravenously over 15 minutes. Thismeans a significant reduction (p<0.001) in the riskof morphometric fractures of 70% (relative risk:0.30; CI 95%: 0.24 to 0.38). Significant reductionswere also observed in the relative risk (RR) ofthese fractures in the group benefiting from zole-dronic acid after one year (1.5% against 3.7% inthe placebo group), and after two years (2.2%against 7.7%: RR 0.29), of treatment (Table 1).
The treatment with zoledronic acid resulted ina reduction of 41% in the risk of hip fracture.During these three years, the incidence of hip frac-ture was 2.5% in the group treated with a placeboand 1.4% in that treated with zoledronic acid(razón de riesgo instantáneo) hazard ratio: 0.59; CI95%: 0.42 to 0.83). In comparison with the inci-dence in the placebo group, the incidence of non-vertebral, clinical and clinical vertebral fractureswas reduced significantly in the group treated withzoledronic acid. These reductions were 25%, 33%and 77% respectively (p<0.001 for all the compa-risons) (Table 1).
II. Effect on bone mineral density and bioche-mical markersThe HORIZON-PFT study also associated zoledro-nic acid with a significant improvement in bonemineral density and markers for bone metabo-lism9. The changes in BMD in the hip after threeyears of study were +4.1% in the group treatedwith zoledronic acid, as against -1.9% in the grouptreated with the placebo; +6.9% as against +0.2%respectively in the BMD in the lumbar spine; and+3.9% as against -1.2% in the BMD in the femoralneck. This means a statistically significant increase
(p<0.001 for all comparisons) in BMD in the grouptreated with zoledronic acid of 6.02% in the totalhip (CI 95%: 5.77 to 6.28), of 6.71% in the lumbarspine (CI 95%: 5.69 to 7.74) and 5.06% in thefemoral neck (CI 95%: 4.75 to 5.36), in comparisonwith the placebo group.
In principle, these changes do not only reflectan increase in the density of the lumbar vertebralbodies, but also any change in the calcification ofthe aorta or the density of the posterior processes,none of which would contribute to the resistanceof the vertebral body.
The evaluation of the spinal BMD by DEXAintegrates the cortical and trabecular bone com-partments with the limitation of including in theanteposterior projection the image of the posteriorprocesses of the spine, or aortic calcifications ifthey exist. For this reason a sub-analysis of HORI-ZON-PFT was carried out in which, by means ofquantitative computerised tomography (whichdefines with greater clarity the cortical and trabe-cular compartments) which found that zoledronicacid caused both an increase in total bone and anincrease in spongy bone in the hip. The changesafter three years of treatment were +2.9% against -3.2% for the placebo. However, the difference inchanges in the cortical bone were not statisticallysignificant (-0.4% as against -1.4% in the placebogroup)10. The same was observed in the spinalcolumn, where the results obtained by bone den-sitometry in HORIZON-PFT and by quantitativecomputerised tomography in this sub-study, weresimilar11.
Another phase II clinical trial, randomised,double blind, placebo controlled, studied theeffect of zoledronic acid at doses of 0.25, 0.5, and1 mg as against a placebo in 351 postmenopausalwomen with low BMD12. After a year of the clini-cal trial it was observed that the increases in BMDin the spinal column in all the groups which hadtaken zoledronic acid (even at different doses)were similar. These were between 4.3% and 5.1%of the average BMD in the placebo group(p<0.001), and remained stable. The BMD in thefemoral neck also increased progressively duringthe whole period of the study. While the BMD inthe femoral neck of the placebo group decreasedby 0.4%, if we compared this with the groupswhich took zoledronic acid, these groups had asignificantly higher difference of between 3.1%and 5.1% with respect to the placebo group10.
With regard to the markers for remodelledbone, in the clinical trial HORIZON-PFT it wasalso observed that the three biochemical markersdiminished significantly in patients treated withzoledronic acid in comparison with those in theplacebo group. At 12 months the blood concentra-tions of carboxy-terminal telopeptide of type 1collagen, of bone-specific alkaline phosphataseand of amino-terminal propeptide of type 1 colla-gen had reduced by 59% (95% CI: 55 to 63), 30%(95% CI: 27 to 32) and 58% (95% CI: 55 to 60), res-pectively in the group treated with zoledronic acid(p< 0.001 for all the comparisons)9.
Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3022

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3023
III. Effects on histology and bone resistanceLong term treatment with zoledronic acid does notappear to affect bone quality in postmenopausalpatients with osteoporosis. At the end of theHORIZON-PFT clinical trial no qualitative altera-tions were detected in bone tissue, in fibrosis ofthe medulla or in cellular toxicity in bone biopsiestaken in patients participating in this study. Inaddition, quantitative histology revealed the pre-servation of trabecular bone architecture in biop-sies taken from patients treated over three yearswith zoledronic acid.
Quantitative computerised tomographic datafrom patients in the HORIZON-PFT11 study sho-wed that zoledronic acid also improved somestrength indices. After three years of treatment, theresistance to bone compression improved signifi-cantly (p≤ 0.001) in those patients who had takenzoledronic acid in relation to patients treated witha placebo13. The analysis carried out of the quan-titative computerised tomographies showed anaverage change from the initiation of treatmentwith zoledronic acid and with a placebo of +4.9%as against -3.7% in the femoral neck, and of +9.8%as against -4.3% in the trochanter, respectively11.There was also an improvement in the volume ofcortical bone with treatment with this biphospho-nate. The average of the total variations in the hipfrom the point of initiation was 7.20%, as opposedto -0.02% with the placebo (p= 0.003).
b) In patients with hip fracture due to lighttraumaThe therapeutic efficacy of zoledronic acid inpatients who have suffered a hip fracture due tolight trauma has also been demonstrated in a mul-ticentric, double blind, randomised trial of threeyears duration, known as the HORIZON-Recurrent
Fracture Trial (HORIZON-RFT)14. 2,127 patientswere studied over an average follow up period of1.9 years.
This study included men and women over 50years of age who had suffered a hip fracture as aconsequence of a light trauma, and whose fractu-re had been treated surgically in the 90 days follo-wing the trauma. These patients had these charac-teristics in common: they had both legs, they hadbeen tracked in the outpatient clinic before thefracture, and they did not want, or were unable, toreceive treatment with oral biphosphonates.Excluded from the study were those patients trea-ted with strontium or sodium fluoride, those whohad a bone disease other than osteoporosis, thosewho suffered from cancer, and those who had acreatinine clearance lower than 30 mL/min (<1.8L/h), blood calcium > 2.8 or < 2.0mmol/L or a lifeexpectancy of less than six months. As in HORI-ZON-PFT8, those patients who had been treatedearlier with biphosphonates or PTH were subjectto a cleansing period. Simultaneous treatmentswith modulators selective for oestrogen receptor,calcitonin, tibolon or hormonal therapy, and exter-nal hip protectors were permitted.
1,065 patients were randomly allocated toreceive an intravenous infusion of 5 mg of zole-dronic acid over 15 minutes and 1,062 to receivea placebo, annually. In this clinical trial all patientswere also administered calcium and vitamin D.
The principle measure of efficacy in the studywas the appearance of new fractures. Secondarymeasures of efficacy included new hip fracture, ver-tebral or non-vertebral fractures, and the change inBMD in the hip not fractured during the study.
After two years of treatment, the treatment withzoledronic acid reduced clinically the risk of newfractures by 35% compared with the placebo. While
Table 1. Relative risks of incidence of fracture in the two groups of the study. Horizon-PFT study8
Type of fracture PlaceboNº of patients (%)
Zoledronic AcidNº of patients (%)
Relative risk(IC del 95%) P value
Morphometricvertebral fracture(stratum I)
310 (10.9) 92 (3.3) 0.30 (0.24-0.38) p< 0.001
Hip fracture 88 (2.5) 52 (1.4) 0.59 (0.42-0.83) p< 0.002
Non-vertebralfracture 388 (10.7) 292 (8.0) 0.75 (0.64-0.87) p< 0.001
Any clinical fracture 456 (12.8) 308 (8.4) 0.67 (0.58-0.77) p< 0.001
Clinical vertebralfracture 84 (2.6) 19 (0.5) 0.23 (0.14-0.37) p< 0.001
Multiple (≥ 2) mor-phometric vertebralfractures (stratum I)
66 (2.3) 7 (0.2) 0.11 (0.05-0.23) p< 0.001

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3024
13.9% of the patients who took the placebo suffe-red a clinical fracture during the two years of followup, only 8.6% of those patients receiving zoledro-nic acid had a new fracture. The drug reduced sig-nificantly the risk of suffering a new non-vertebralfracture (7.6% of the beneficiaries of zoledronicacid as opposed to 10.6% of those taking the place-bo) and vertebral fractures (1.7% as opposed to3.8%, respectively) by 27% and 46% respectivelycompared with the placebo, p< 0.05 in all cases. Intheir turn, the BMD in total hip and in the femoralneck improved significantly (p< 0.001) with zole-dronic acid compared with the placebo. After 12months, the changes since the start of treatmentwere +2.6% in total hip and +0.8% in the femoralneck compared with -1.0% and -1.7% respectivelyfor the placebo. After 24 months of follow up thefigures were +4.7% and +2.2% compared with -0.7% and -2.1%, respectively. And finally, after 36months of observation, +5.5% and +3.6% as compa-red with -0.9% and -0.7% respectively.
The conclusions of the study were that anintravenous infusion of 5 mg of zoledronic acidover 15 minutes significantly reduces the risk ofsuffering new fractures and results in an improve-ment in BMD, in men and women who have suf-fered a hip fracture after a light trauma. A surpri-sing, but highly practical, finding is a reduction inmortality of 28% observed in the group of patientswho received zoledronic acid.
A doubt has been raised as to what is the bestmoment for the administration of zoledronic acidafter a hip fracture, since it has been suggestedthat this drug might interfere with physiologicalrepair mechanisms, but this has not been demons-trated. Eriksen et al.15 observed in a post-hocanalysis of the HORIZON-PFT study that themedian period of time of the first infusion aftersurgical intervention was 46 days (range= 1 to 123days) and found that the first infusion of 5 mg ofzoledronic acid administered after the first twoweeks from the surgical intervention was moreefficacious in the reduction of risk of new fractu-res. The current trend in some services in Spain isto administer the infusion of zoledronic acid attwo months from the surgical intervention. This isa subject which merits further debate.
Zoledronic acid compared with otherdrugs for the treatment of osteoporosisa) Zoledronic acid against alendronateThe association between a low bone mineral den-sity and the appearance of fractures is widelyknown16. However, only one in five patients whohave suffered a fracture will follow on with a tre-atment for osteoporosis17, and it is estimated that20% of women who have suffered a vertebral frac-ture will present with another fracture within ayear18. From this comes the importance that boneturnover is normalised rapidly in patients withhigh risk of fracture.
A multicentric trial of 24 weeks, randomised,double blind and with double placebo, showedthat a single infusion of 5 mg of zoledronic acid
took effect more rapidly than 70 mg of aledronatetaken orally weekly in postmenopausal patientswith low BMD19. This was found by comparing therelative change with respect to the baseline situa-tion of the marker for bone resorption urinary N-telopeptide of type 1 collagen (NTX) after the firstweek in both groups, and by observing that thetreatment with zoledronic acid produced a reduc-tion significantly greater than that of oral alendro-nate. In addition, during the 24 weeks which thestudy lasted, the reductions in NTX were higher atall moments of post-baseline evaluation in thegroup treated with zoledronic acid, with concen-trations of NTX which stayed at premenopausalvalues from week 12 to the end of the study. It isimportant to point out that significant reductionsin NTX are not solely associated with a reductionin bone resorption, but also, in postmenopausalwomen with osteopenia or without osteoporosis,reductions in NTX at three months are closelyassociated with increases in BMD in the lumbarspine at one year20. The concentrations of bone-specific alkaline phosphatase (BSAP), marker forbone formation, showed a more gradual reductionin both the group which received 5 mg of zoledro-nic acid, and in that which received 70 mg weeklyof alendronate orally, reaching the margin of pre-menopausal values at week 12.
In a co-operative, multicentric, randomiseddouble blind non-inferiority study, Orwoll et al.21
evaluated in 302 men affected by osteoporosis theeffect of 5 mg i.v. annually of zoledronic acid asagainst 70 mg weekly of aledronate. Bone mineraldensity and biochemical markers for bone remo-delling were studied and it was observed that after24 months the results were equivalent in all theparameters analysed, but that the men preferredthe annual i.v. administration of zoledronic acid.
A controversial aspect of treatment for postme-nopausal osteoporosis is the excessive suppres-sion of bone turnover. However, data from thisstudy show that a rapid reduction in the markersfor bone resorption are followed by a slow butcontinous increase in concentrations over thefollowing six months. On the other hand, histolo-gical studies 13 have allowed the rejection of theexistence of “frozen bone”, a syndrome widelyfeared in patients taking biphosphonates with ahypothetical excess of suppression of remodelling.
Adverse effects were more frequent in thegroup which took zoledronic acid than in thosetaking alendronate (91% for the group on 5 mg ofzoledronic acid intravenously compared with86.4% for 70 mg of alendronate orally). Howeverthese symptoms were mostly flu-like and disappe-ared after the first three days from the administra-tion of the drug.
Finally, when patients were asked for their pre-ferred treatment, most of them went for the annualintravenous treatment due to its greater ease ofuse, higher satisfaction and wider availability as atreatment to be taken over a prolonged period.This point will be commented on at greater lengthbelow.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3025
b) Comparison with other drugsJansen et al.22 conducted a study to compare theefficacy of the biphosphonates in the reduction ofrisk of vertebral fracture in women affected bypostmenopausal osteoporosis. To achieve this,after a systematic literature search, they analysedthe baseline results in patients included in diffe-rent studies. The results of this work suggest thatthere is a 98% probability that, among the 4biphosphonates studied, zoledronic acid shows agreater reduction in the risk of vertebral fractures.
Zoledronic acid in patients with osteoporo-sis induced by glucocorticoids.Due to their anti-inflammatory and immunosup-pressive effects, the use of glucocorticoids in clini-cal practice is very extensive, and their effective-ness undisputed. However, their chronic usecarries the risk of producing many adverse effects,of which osteoporosis is one of the most frequentand concerning23,24. Treatment with glucocorticoidsare associated with a higher loss of bone massand, therefore, a higher risk of suffering a fracturein the future.
An annual induction of 5 mg of zoledronic acidhas been authorised in the European Union totreat men and women with osteoporosis causedby the chronic and continual use in low doses ofglucocorticoids (usually known as steroids). In arandomised, double blind study of a year’s dura-tion, conducted in 54 centres in 12 Europeancountries, Australia, Hong Kong, Israel and the US,it was observed that the efficacy of an infusion of5 mg of zoledronic acid was greater than 5 mg ofrisedronate orally, daily, for the prevention andtreatment of osteoporosis induced by glucocorti-coids25. 833 patients were randomly allocated toreceive either zoledronic acid (n=416) or risedro-nate (n=417). The patients were grouped by sex,and assigned to treatment or prevention sub-groups, depending on the duration of their use ofglucocorticoids which they had been taking befo-re the study. The treatment sub-group consisted ofpatients treated for more than 3 months (272patients receiving zoledronic acid and 273 risedro-nate), and the prevention sub-group consisted ofpatients treated for less than 3 months (144patients for each biphosphonate). The results ofthis clinical trial were that, after 12 months, theincreases in bone mineral density in the lumbarspine were significantly higher for those on zole-dronic acid than for those on risedronate, in boththe prevention and treatment sub-groups. In turn,after 6 months of the study, the zoledronic acidproduced a significantly higher, and earlier, incre-ase in BMD than risedronate, indicating a morerapid start to its efficacy. Although once again theadverse effects were more frequent in thosepatients who received zoledronic acid, again, theywere light, occurring during the first three daysafter the infusion and were quickly controlled.The more serious adverse events were a worse-ning of rheumatoid arthritis in the treatment sub-group, and fever in the prevention sub-group.
In conclusion, therapy with zoledronic acid ismore effective, and with a quicker action, than thecurrent established therapy for the treatment ofosteoporosis induced by glucocorticoids, havingalso the advantage of proper annual complianceand of providing sustained osteo-protection25.
Zoledronic acid in male osteoporosisIt is estimated that one in five men over 50 yearsof age will suffer a fracture due to osteoporosis.Zoledronic acid has recently been approved bythe European Union for the treatment of osteopo-rosis in men who have a high risk of fracture, soimproving the quality of life of this section of thepopulation. These conclusions have been reachedas a result of the HORIZON-Recurrent FractureTrial which was commented on in more detail inthe section on the benefits of zoledronic acid inpatients who have suffered a hip fracture due tolight trauma26. In fact, zoledronic acid is one of thefew drugs accepted in Spain for the treatment ofosteoporosis in males.
Preferences for treatmentAs we have already mentioned, the oral biphos-phonates increase bone mineral density and redu-ce the frequency of vertebral fractures, but theyhave had, as limitations, poor absorption, adverseeffects on the digestive tract, and difficulties intaking the treatment. In addition, they are associa-ted with poor compliance and low therapeuticadherence. Many patients to whom these antioste-oporotic drugs are prescribed abandon the treat-ment and, after 12 months, the majority take lessthan 80% of the pills prescribed27-30. This pooradherence to oral biphosphonates compromisestheir efficacy in reducing fractures and increasesmedical costs31,32, above all in older disabledadults, who often cannot follow the administrationregime properly and strictly33.
Weekly treatments provide a better adherencethan daily treatments, but even so, a sufficientadherence is only reached in around 50% ofpatients27,30. For this reason, a regime of adminis-tration of an annual perfusion guarantees topatients a full therapeutic effect for at least 12months. This has been observed in a study whichcompared the efficacy of a single annual infusionof zoledronic acid, as against that of alendronate,taken orally weekly, in postmenopausal patientswith low bone mineral density19. In this study, allpatients who had taken medication or placebointravenously, or orally weekly, were asked if theypreferred the annual intravenous infusion, weeklyoral treatment, or both equally. Of the 221 patientsof all categories evaluated who had responded tothe questionnaire, 73.8% expressed a general pre-ference for annual intravenous infusions, 9% pre-ferred weekly oral administration, while 11.8%considered both dosage regimes as equal34.
A regime of administration once a year is anattractive option for the treatment of osteoporosissince it will provide assured bone protection overthe whole year. In addition, as has already been

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3026
mentioned, the intravenous administration resultsin a quicker initiation of activity than that obtainedwith oral biphosphonates19.
TolerabilityIn general, if we compare the tolerability ofpatients to zoledronic acid as against a placebo,this has been good23,24. Although it is true that thenumber of adverse effects in the group which tookzoledronic acid was higher than that of the place-bo, these effects were mostly light and transitory.While in the HORIZON-PTF study the incidence ofadverse effects was 95.5% and 93.9% respectively,with a p-value significantly equal at 0.002, inHORIZON-RFT no statistically significant differen-ce was found between the two groups. However,in HORIZON-PTF there were no significant diffe-rences in terms of the incidence of serious adver-se effects or the abandonment of the study bypatients (29.2% as against 31.1% and 38.3% asagainst 41.2%, respectively).
The most frequent symptoms were reported inthe three days following the perfusion of the medi-cine. These were pyrexia, flu-like symptoms, myal-gia, headache and arthralgia. In general thesesymptoms were classified as light or moderate anddissipated over a period of 3 days. The proportionof patients who received zoledronic acid and whoin turn had some post-administration symptomwas significantly higher compared with the place-bo group after the first day (31.6% as against 6.2%),the second day (6.6% as against 2.1%), and afterthe third day (2.8% as against 1.1%). It is importantto note that in patients from the HORIZON-RFTstudy who received paracetamol at the time of, andafter, the perfusion of the treatment, only the myla-gia and pyrexia were significantly higher in thegroup which received the zoledronic acid14.
An annual therapy with zoledronic acid is notassociated with renal toxicity in the long term.Although between days 9 and 11 after the perfu-sion 1.3% of the patients in the group treated withzoledronic acid presented an increase of morethan 0.5 mg/dl in the blood concentration of cre-atinine, as opposed to 0.4% of patients in the pla-cebo group, these changes were transitory; by theend of 30 days, in more than 85% of patients, theconcentrations had returned to being within amargin of 0.5 mg/dl with respect to the valuesbefore the perfusion and in the remainder, theyhad returned to these levels by the followingannual review. After three years of treatment nosignificant differences were observed between thetaking of the placebo or the zoledronic acid interms of the concentrations of blood creatinine orin creatinine clearance13,14.
In addition, although after 9-11 days from thefirst perfusion, 49 patients from the group treatedwith zoledronic acid had blood calcium lowerthan 2,075 mmol/l, compared with 1 patient in theplacebo group, all these events were transitoryand asymptomatic.
Generally, the cardiovascular tolerability wassimilar in the patients of both groups. However,
6.9% of those patients treated with zoledronic acidpresented with arrhythmia, and this was signifi-cantly higher (p=0.003) than in the placebo groupin which 5.3% of patients developed it. While inHORIZON-RFT no notable difference was foundin the incidence of serious arrhythmia (1.1% asagainst 1.3% in patients in the zoledronic acidgroup and in the placebo group, respectively), itis important to note that the incidence of auricularfibrillation in HORIZON-PFT was indeed signifi-cantly higher in the group treated with the biphos-phonate compared to that with the placebo (1.3%as against 0.5% respectively, with a p-value of<0.001). However, after the evaluation, the num-ber of patients whose auricular fibrillation wasreported as a serious event hardly varied (50 in thegroup treated with zoledronic acid and 17 in theplacebo group). Subsequently, various meta-analyses have confirmed that there is no associa-tion between the use of biphosphonates and auri-cular fibrillation35-39.
It is well known that most of the cases of maxi-llary osteonecrosis have been observed in patientswith cancer treated with frequent and high dosesof intravenous biphosphonates40-42. However, inthe HORIZON-PFT reference study there were nospontaneous notifications of mandibular osteone-crosis. By means of a search of a database ofadverse events in the trial, which was followed byan evaluation by experts, two possible cases ofmaxillary osteonecrosis were identified (one in theplacebo group and one in the group treated withzoledronic acid). In both patients, this resulted ina delay in healing after surgery, and the two caseswere resolved later with antibiotic and debride-ment treatment8,14. Four patients who receivedzoledronic acid developed osteonecrosis in theknee or hip, compared with three patients in theplacebo group8. Hence, a SEIOMM position docu-ment produced in conjunction with all the natio-nal societies dedicated to osteoporosis and all theodontological and/or maxillofacial societies, esta-blished that zoledronic acid utilised at doseswhich are used in the treatment of osteoporosisdoes not increase the risk of maxillary osteonecro-sis43.
Finally, a slight increase in the risk of adverseinflammatory opthalmological events in the 15days following the perfusion was confirmed 8, ashas been noted in relation to other biphosphona-tes. However, these events were treated and resol-ved with outpatient treatment in all cases.
Recommendations on dose and method ofadministrationZoledronic acid received the approval of the regu-latory authorities of the US (FDA) and theEuropean Union (EMEA) as the first and onlyonce-yearly treatment for women with postmeno-pausal osteoporosis.
In the European Union and in the UnitedStates, the use of zoledronic acid has been appro-ved as a treatment for osteoporosis in postmeno-pausal women at risk of fracture. It has also been

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3027
approved for patients who have suffered a hipfracture through trauma, and in Europe, in menwho suffer from osteoporosis and who have ahigh risk of suffering a fracture. 5 mg of intrave-nous zoledronic acid annual is recommended,administered in a single infusion of 100 ml over aminimum period of 15 minutes. Before the infu-sion, it is recommended that the blood levels ofcalcium are established and that a calculation ofcreatinine clearance be carried out by determiningthe levels of blood creatinine. Also, it is necessaryto confirm the prior state hydration of the patientand advise them to drink at least two glasses ofwater before the infusion, and continue after itwith normal hydration. A supplement of calciumand vitamin D is also recommended.
In patients older than 65 years of age, or withlight to moderate renal deficiency, it is not neces-sary to adjust the dose of zoledronic acid. In theEuropean Union, neither is such an adjustment indosage recommended in patients who suffer liverinsufficiency, but this is not the case in the UnitedStates. Finally, treatment with this third generationbiphosphonate is not recommended in patientssuffering from serious renal insufficiency (creatini-ne clearance < 35 mL/min).
The Spanish Society for Bone and MineralMetabolism Research (SEIOMM), in the update ofits guides for the treatment of postmenopausal,steroidal and male osteoporosis, recommends theconsideration of zoledronic acid as a drug with agrade of recommendation A for the reduction ofosteoporotic vertebral, non-vertebral and hip frac-tures2.
Zoledronic acid as a preventativetreatmentEvery day more articles are being published whichdemonstrate the efficacy of zoledronic acid in theprevention of bone loss in patients.
A study published recently demonstrated thattreatment every three months with zoledronic acidover a year, was efficacious against the loss ofbone mass during the first year of chemotherapyin premenopausal women with breast cancer44. Itis important to mention that adjuvant chemothe-rapy is associated with a significant reduction inbone mineral density in premenopausal womenwith breast cancer, hence the importance of a tre-atment efficacious in combating this.
In this study, 101 women were randomly assig-ned, 85 completed 12 months and 62 completedevaluations over the following 24 months. In theplacebo group the blood C-telopeptide (CTX)increased progressively during the first 12months, regressed towards the baseline, but sta-yed significantly above the line after 24 months. Inthe lumbar spine, the BMD diminished from thebaseline value by 5.5% at 12 months, and by 6.3%at 24 months. Similarly, after 24 months, the BMDin the total hip and the femoral neck diminishedby 2.6% and 2.4% respectively. However, in thosepatients who took zoledronate, the BMD remainedstable (p< 0.0001 in comparison with the place-
bo). Although the blood CTX reduced significantlyat 6 months, these levels returned to baselinelevels at 12 months, remaining stable during thefollowing 24 months.
There are also studies which try to establish therole of zoledronic acid in the prevention of loss ofBMD in postmenopausal women. One example isthe study carried out by McLung et al. whoseobjective was to evaluate the efficacy of zoledro-nic acid for the prevention of bone loss in postme-nopausal women with low bone mass45. This clini-cal trial of two year duration, randomised, multi-centric, double blind and placebo controlled, pos-tmenopausal women with low bone mass wererandomly selected to receive 5 mg of zoledronicacid intravenously at the time of their selectionand at month 12 (two doses of 5 mg of zoledronicacid intravenously each year), 5 mg of zoledronicacid intravenously only at the time of selectionand a placebo at month 12, or placebo at the timeof random selection and at month 12.
The trial’s results show that both in the groupwhich received two doses of zoledronic acidannually, and that which received one dose, a sta-tistically significant higher increase in BMD in thelumbar spine was produced in comparison withthe group which received the placebo (5.58% and4.42% in comparison with 1.32%, respectively, P<0.001). Similarly, a statistically significantly greaterincrease in the BMD of the hip, femoral neck andtrocanter was obtained in month 12 and month 24(all with a p value < 0.001). Finally, in thosepatients who received zoledronic acid a statisti-cally significant increase in markers for bone tur-nover was produced, although the changes in thegroup which received two one doses annuallywere greater. The total incidence of adverseevents and of serious adverse effects were similarin all the treatment groups.
Cost-benefitOsteoporosis places considerable economicdemands on health resources46-48. It is for this rea-son that pharmaco-economic considerations areimportant factors in the selection of antiosteoporo-tic treatment. At present, the price of zoledronicacid is not high in comparison with other drugs.One infusion of zoledronic acid costs 422,65 €(Price plus VAT) in Spain. In Table 2 we can seethe annual cost of zoledronic acid in comparisonwith other drugs used in the treatment of osteopo-rosis.
ConclusionThe intravenous administration of 5 mg of zole-dronic acid once a year has been shown to be effi-cacious in the reduction of risk of vertebral fractu-res in patients with postmenopausal osteoporosisor hip fractures due to light trauma. It also produ-ces an increase in bone mineral density andreductions in the markers for bone turnover, andis generally well tolerated. All this makes zoledro-nic acid a drug of first choice in the treatment ofosteoporosis.

Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3028
Table 2. Annual cost of different drugs used in the treatment of osteoporosis. Own development from the data-base of the General Council of the Official College of Pharmacologists. Version 198, (7-9-2010)
Active principal Commercialname
Dose. Period.Method of
administrationPresentation
Packet cost28 days
(Euros withoutVAT)
Annual cost(Euros without
VAT)*
Zoledronic acid Aclasta 5 mg. Annuali.v. Bottle 100 ml 406.39 406.39**
Alendronate Fosamax 70 mg.Weekly. Oral
Tablets. Packageswith 4 21.19 275.47
Alendronate Severalgenerics
70 mg.Weekly. Oral
Tablets. Packageswith 4 15.42 200.46
Alendronate +Vitamin D Fosavance 70 mg.
Weekly. OralTablets. Packages
with 4 27.47 357.11
Risedronateweekly
Acrel.Actonel
35 mg.Weekly. Oral
Tablets. Packageswith 4 33.34 433.42
Risedronateweekly Generics 35 mg.
Weekly. OralTablets. Packages
with 4 22.93 298.09
Risedronatemonthly
Acrel.Actonel
75 mg.Monthly 2 day.
Oral
Tablets. Packageswith 2 33.32 399.84
Ibandronate Bonviva.Bondenza
150 mg.Monthly. Oral
Tablets. Packageswith 1 33.32 399.84
Strontium ranelate Protelos.Osseor
2 g. Diaily.Oral
Envelopes.Packages with 28 47.49 617.37
PTH 1-34 Forsteo 20 μg. Daily.Sub-cutaneous
Preloaded pen.Packages with
28 dose384.79 5,002.87
PTH 1-84 Preotact 100 μg. Diaria.Sub-cutaneous
2 cartridges14 dose c/u 380,95 4,952.35
Raloxifen Evista.Optruma
60 mg. Diaily.Oral
Tablets.Packages with
2833.08 430.04
Nasal calcitonin Miacalcic.Several
200 UI. Daily.Nasal
NebulizerPackages with
28 dose72.13 937.69
*Calculated on the basis of 13 packets per year, since it should be taken into account that the tablets in packets of28 provide 28*12 months=336 tablets per year. More than one additional packet is necessary (29 tablets) to comple-te 365 days of the year, with the exception of ibandronate.**In the case of zoledronic acid the cost of 1 syringe, needle and 100ml saline solutions should be added, plus thecost of staff of day hospital or place where it is administered, which varies from one hospital centre to another.

Bibliography
1. Licata AA. Update on therapy for osteoporosis. OrthopNurs 2007;26:162-6; quiz 67-8.
2. Comité de expertos de la SEIOMM. Guías de prácticaclínica en la osteoporosis postmenopáusica, glucocor-ticoidea y del varón. Rev Osteoporos Metab Miner2009;1:53-60.
3. Russell RG, Croucher PI, Rogers MJ. Bisphosphonates:pharmacology, mechanisms of action and clinical uses.Osteoporos Int 1999;9(Suppl 2):S66-S80.
4. Rogers MJ, Gordon S, Benford HL, Coxon FP, LuckmanSP, Monkkonen J, et al. Cellular and molecular mecha-nisms of action of bisphosphonates. Cancer 2000;88(12Suppl):2961-78.
5. Fleisch H. Bisphosphonates: mechanisms of action andclinical use in osteoporosis--an update. Horm MetabRes 1997;29:145-50.
6. Shinoda H, Adamek G, Felix R, Fleisch H, Schenk R,Hagan P. Structure-activity relationships of various bis-phosphonates. Calcif Tissue Int 1983;35:87-99.
7. Nancollas GH, Tang R, Phipps RJ, Henneman Z, GuldeS, Wu W, et al. Novel insights into actions of bisphos-phonates on bone: differences in interactions withhydroxyapatite. Bone 2006;38:617-27.
8. Black DM, Delmas PD, Eastell R, Reid IR, Boonen S,Cauley JA, et al. Once-yearly zoledronic acid for treat-ment of postmenopausal osteoporosis. N Engl J Med2007;356:1809-22.
9. Delmas PD, Munoz F, Black DM, Cosman F, Boonen S,Watts NB, et al. Effects of yearly zoledronic acid 5 mgon bone turnover markers and relation of PINP withfracture reduction in postmenopausal women withosteoporosis. J Bone Miner Res 2009;24:1544-51.
10. Eastell R, Black DM, Boonen S, Adami S, Felsenberg D,Lippuner K, et al. Effect of once-yearly zoledronic acidfive milligrams on fracture risk and change in femoralneck bone mineral density. J Clin Endocrinol Metab2009;94:3215-25.
11. Eastell R, Lang T, Boonen S, Cummings S, Delmas PD,Cauley JA, et al. Effect of once-yearly zoledronic acidon the spine and hip as measured by quantitative com-puted tomography: results of the HORIZON PivotalFracture Trial. Osteoporos Int 2010;21:1277-85.
12. Reid IR, Brown JP, Burckhardt P, Horowitz Z,Richardson P, Trechsel U, et al. Intravenous zoledronicacid in postmenopausal women with low bone mine-ral density. N Engl J Med 2002;346:653-61.
13. Recker RR, Delmas PD, Halse J, Reid IR, Boonen S,Garcia-Hernandez PA, et al. Effects of intravenouszoledronic acid once yearly on bone remodeling andbone structure. J Bone Miner Res 2008;23:6-16.
14. Lyles KW, Colon-Emeric CS, Magaziner JS, Adachi JD,Pieper CF, Mautalen C, et al. Zoledronic Acid inReducing Clinical Fracture and Mortality after HipFracture. N Engl J Med 2007;357:nihpa40967.
15. Eriksen EF, Lyles KW, Colon-Emeric CS, Pieper CF,Magaziner JS, Adachi JD, et al. Antifracture efficacyand reduction of mortality in relation to timing of thefirst dose of zoledronic acid after hip fracture. J BoneMiner Res 2009;24:1308-13.
16. Siris ES, Miller PD, Barrett-Connor E, Faulkner KG,Wehren LE, Abbott TA, et al. Identification and fractu-re outcomes of undiagnosed low bone mineral densityin postmenopausal women: results from the NationalOsteoporosis Risk Assessment. Jama 2001;286:2815-22.
17. Hajcsar EE, Hawker G, Bogoch ER. Investigation andtreatment of osteoporosis in patients with fragility frac-tures. Cmaj 2000;163:819-22.
18. Lindsay R, Silverman SL, Cooper C, Hanley DA, BartonI, Broy SB, et al. Risk of new vertebral fracture in theyear following a fracture. Jama 2001;285:320-3.
19. Saag K, Lindsay R, Kriegman A, Beamer E, Zhou W. Asingle zoledronic acid infusion reduces bone resorp-tion markers more rapidly than weekly oral alendrona-te in postmenopausal women with low bone mineraldensity. Bone 2007;40:1238-43.
20. Kim SW, Park DJ, Park KS, Kim SY, Cho BY, Lee HK,et al. Early changes in biochemical markers of boneturnover predict bone mineral density response toantiresorptive therapy in Korean postmenopausalwomen with osteoporosis. Endocr J 2005;52:667-74.
21. Orwoll E, Miller PD, Adachi JD, Brown J, Adler RA,Kendler D, et al. Efficacy and safety of a once-yearlyi.v. infusion of zoledronic acid 5 mg versus a once-weekly 70 mg oral alendronate in the treatment ofmale osteoporosis: A randomized, multicenter, double-blind, active-controlled study. J Bone Miner Res.
22. Jansen JP, Bergman GJ, Huels J, Olson M. Preventionof vertebral fractures in osteoporosis: mixed treatmentcomparison of bisphosphonate therapies. Curr MedRes Opin 2009;25:1861-8.
23. Heffernan MP, Saag KG, Robinson JK, Callen JP.Prevention of osteoporosis associated with chronicglucocorticoid therapy. Jama 2006;295:1300-3.
24. Hoes JN, Jacobs JW, Boers M, Boumpas D, ButtgereitF, Caeyers N, et al. EULAR evidence-based recommen-dations on the management of systemic glucocorticoidtherapy in rheumatic diseases. Ann Rheum Dis2007;66:1560-7.
25. Reid DM, Devogelaer JP, Saag K, Roux C, Lau CS,Reginster JY, et al. Zoledronic acid and risedronate inthe prevention and treatment of glucocorticoid-indu-ced osteoporosis (HORIZON): a multicentre, double-blind, double-dummy, randomised controlled trial.Lancet 2009;373:1253-63.
26. Orwoll E, Miller PD, Adachi JD, Brown J, Adler RA,Kendler D, et al. Efficacy and safety of a once-yearlyi.v. infusion of zoledronic acid 5 mg versus a once-weekly 70 mg oral alendronate in the treatment ofmale osteoporosis: A randomized, multicenter, double-blind, active-controlled study. J Bone Miner Res 2010.
27. Cramer JA, Amonkar MM, Hebborn A, Altman R.Compliance and persistence with bisphosphonatedosing regimens among women with postmenopausalosteoporosis. Curr Med Res Opin 2005;21:1453-60.
28. Siris ES, Harris ST, Rosen CJ, Barr CE, Arvesen JN,Abbott TA, et al. Adherence to bisphosphonate the-rapy and fracture rates in osteoporotic women: rela-tionship to vertebral and nonvertebral fractures from 2US claims databases. Mayo Clin Proc 2006;81:1013-22.
29. Downey TW, Foltz SH, Boccuzzi SJ, Omar MA, KahlerKH. Adherence and persistence associated with thepharmacologic treatment of osteoporosis in a managedcare setting. South Med J 2006;99:570-5.
30. Recker RR, Gallagher R, MacCosbe PE. Effect of dosingfrequency on bisphosphonate medication adherencein a large longitudinal cohort of women. Mayo ClinProc 2005;80:856-61.
31. Huybrechts KF, Ishak KJ, Caro JJ. Assessment of com-pliance with osteoporosis treatment and its consequen-ces in a managed care population. Bone 2006;38:922-8.
32. Silverman SL, Gold DT, Cramer JA. Reduced fracturerates observed only in patients with proper persisten-ce and compliance with bisphosphonate therapies.South Med J 2007;100:1214-8.
33. van Eijken M, Tsang S, Wensing M, de Smet PA, GrolRP. Interventions to improve medication compliance inolder patients living in the community: a systematicreview of the literature. Drugs Aging 2003;20:229-40.
34. McClung M, Recker R, Miller P, Fiske D, Minkoff J,Kriegman A, et al. Intravenous zoledronic acid 5 mg inthe treatment of postmenopausal women with lowbone density previously treated with alendronate.Bone 2007;41:122-8.
35. Vestergaard P, Schwartz K, Pinholt EM, Rejnmark L,Mosekilde L. Risk of atrial fibrillation associated withuse of bisphosphonates and other drugs against osteo-porosis: a cohort study. Calcif Tissue Int 2010;86:335-42.
36. Kim SY, Kim MJ, Cadarette SM, Solomon DH.Bisphosphonates and risk of atrial fibrillation: a meta-analysis. Arthritis Res Ther 2010;12:R30.
37. Arslan C, Aksoy S, Dizdar O, D SD, Harputluoglu H,Altundag K. Zoledronic acid and atrial fibrillation incancer patients. Support Care Cancer 2010.
Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3029

38. Mak A, Cheung MW, Ho RC, Cheak AA, Lau CS.Bisphosphonates and atrial fibrillation: Bayesian meta-analyses of randomized controlled trials and observa-tional studies. BMC Musculoskelet Disord 2009;10:113.
39. Loke YK, Jeevanantham V, Singh S. Bisphosphonatesand atrial fibrillation: systematic review and meta-analysis. Drug Saf 2009;32:219-28.
40. Khan A. Osteonecrosis of the jaw and bisphosphona-tes. BMJ 2010;340:c246.
41. Gebara SN, Moubayed H. Risk of osteonecrosis of thejaw in cancer patients taking bisphosphonates. Am JHealth Syst Pharm 2009;66:1541-7.
42. Mauri D, Valachis A, Polyzos IP, Polyzos NP,Kamposioras K, Pesce LL. Osteonecrosis of the jawand use of bisphosphonates in adjuvant breast cancertreatment: a meta-analysis. Breast Cancer Res Treat2009;116:433-9.
43. Sosa Henríquez M, Gómez de Tejada Romero MJ,Bagán Sebastián JV, Díaz Curiel M, Díez Pérez A, E JG,
et al. Osteonecrosis de los maxilares. Documento deconsenso. Rev Osteoporos Metab Miner 2009;1:41-52.
44. Hershman DL, McMahon DJ, Crew KD, Shao T,Cremers S, Brafman L, et al. Prevention of bone lossby zoledronic acid in premenopausal women under-going adjuvant chemotherapy persist up to one yearfollowing discontinuing treatment. J Clin EndocrinolMetab 2010;95:559-66.
45. McClung M, Miller P, Recknor C, Mesenbrink P, Bucci-Rechtweg C, Benhamou CL. Zoledronic acid for theprevention of bone loss in postmenopausal womenwith low bone mass: a randomized controlled trial.Obstet Gynecol 2009;114:999-1007.
46. Becker DJ, Kilgore ML, Morrisey MA. The societal burdenof osteoporosis. Curr Rheumatol Rep 2010;12:186-91.
47. Keen RW. Burden of osteoporosis and fractures. CurrOsteoporos Rep 2003;1:66-70.
48. Kanis JA, Johnell O. The burden of osteoporosis. JEndocrinol Invest 1999;22:583-8.
Rev Osteoporos Metab Miner 2010; 2 (Supl 4): S21-S3030