Embed Size (px)
Citation preview

ECHOCARDIOGRAM DIAGNOSIS OF PULMONARY HYPERTENSION MAY BE INACCURATE IN ESRD PTS Ifeanyi Isaiah, Jesse Goldman, Sung-Ji Schmidt, Sheila Weaver, Jean Lee, Temple University Divisions of Nephrology and Pulmonary
Previous studies of PPH in hemodialysis (HD) patients suggest an increased prevalence of 26.7%-39.7%. However, these studies rely exclusively upon echocardiography to define PH and echocardiography often overestimates pulmonary arterial pressures (PAP). We applied current American College of Chest Physician (ACCP) guidelines, using right heart catheterization (RHC) to establish the true prevalence of PH We conducted a retrospective, observational, analysis of all echocardiographic and RHC studies in prevalent HD patients from our outpt dialysis units. We used a peak systolic PAP ≥ 40 mmHg by 2-D echocardiogram initially to screen for PH and later a mean PAP ≥ 25 mmHg (with pulmonary capillary wedge pressure (PCWP) < 15 mm Hg) to confirm PPH. In subjects with PCWP >15, a trans-pulmonary gradient (TPG) > 15 suggested a mixed disease process. Patients with valvular abnormalities or Left Ventricular (LV) ejection fraction < 40% were excluded. Medical records of 502 patients (56% female; mean age 59.4 ± 14.037 years) were reviewed. 439 patients had undergone echocardiography. 127 (28.9%) patients had an elevated PAP suggesting PH (mean PAP was 43.098 ± 11.404 mmHg). Of these patients, 22 (17.32%) also had RHC data. 11/22 (50%) of these patients had RHC confirming elevated mean PAP. PCWP exceeded 15 mm Hg in all 11 patients. 46 additional patients had RHC obtained for a variety of reasons without echo. Of these patients, 40 patients had mean PAP ≥25 mmHg. 14 of these patients had PCWP ≤ 15 suggesting primary disease. 26 of these patients had PCWP > 15. 16 patients had TPG ≤ 15 (suggesting heart failure as etiology) and 10 patients had TPG > 15 (suggesting mixed disease process therefore 10/439 or 2.3%). Our study shows a higher prevalence of PH in ESRD pts receiving HD than the general population. However, based on RHC data, the true prevalence of primary pulmonary hypertension in these patients is overestimated by echocardiography. Therefore, we recommend that all hemodialysis patients with echocardiographic evidence for PH have subsequent RHC to determine whether PPH is actually present.
97
COMPUTERIZED ANEMIA MANAGEMENT PROGRAM (CAMP©)DOSING OF ONCE MONTHLY DE NOVO DARBEPOETIN ALFAVERSUS BODYWEIGHT-BASED DOSING. Khaled Ismail, Elias Chalhoub, Ramy Fayad, Mark D. Faber, Stanley Frinak, Jerry Yee. Henry Ford Hospital, Detroit, MI, USA. Monthly (QM) Darbepoetin alfa (DA) has been shown to be effective for the treatment of anemia of CKD. (Ling et al. Clin Nephrol, 2005). Recent studies, however, have shown that normalization of hemoglobin with erythropoietin stimulating agents (ESA) may increase cardiovascular and ESRD risk in CKD (Singh et al. NEJM, 2006 and Drüeke et al, NEJM 2006). This study was to determine the efficacy of QM DA delivered using CAMP©. Also, this study would elucidate whether there were differences between conventional weight-based DA dosing and the CAMP© dosing regimen. CAMP© was deployed to facilitate treatment of ESA-naïve CKD stage 3–5 patients with i.v. or oral iron and QM DA. Dosing was determined by entry hemoglobin (Hb) rather than bodyweight, according to a computerized algorithm. The therapeutic goal was to maintain Hb in the specified range of 11–13 g/dL. Individual serum iron, transferrin saturation (TSAT), ferritin, Hb and DA dose were obtained QM. Age (y), bodyweight (kg), presence/absence of proteinuria and diabetes were also recorded. Exclusion criteria included receipt of an organ allograft, active immunosuppression and ESRD status. Data were reported as means±SD. Data analysis was by ANOVA and paired 2-tail t-test. Mean followup of (n=68) patients was 301±74 d and the mean number of DA doses was 9.2±2.6. Hb goal was achieved in 60.3% of patients. Hb>13 g/dL occurred in only 1.5%. The mean initiation doses by bodyweight versus CAMP© were 157.6 mcg and 97.8 mcg, respectively (difference 59.8 mcg p<.0001). The mean maintenance dose by CAMP© was 23.7 mcg less than the suggested weight-based dose (p=.015). Multivariate analysis showed no interaction between the last maintenance Hb and diabetes, proteinuria, weight, or any combination of the three. We conclude that CAMP© effectively managed the anemia of CKD in non-ESRD patients with a low probability of overshooting the Hb goal. This approach may abrogate the increased cardiovascular, renal and mortality risks that may be associated with normalization of Hb in CKD. Moreover, the mean Hb-based QM DA algorithmic dose Hb was significantly less than that calculated by weight-based dosing. Presence of diabetes and/or proteinuria and weight had no impact on the last maintenance hemoglobin. The use of weight-based dosing for initiation of DA would likely increase the mean Hb of our trial population, but possibly at the expense of exceeding the target Hb range.
98
A CASE OF COLLAPSING FSGS ASSOCIATED WITH STILL’S DISEASE. Gaurav Jain, Peter Hart, Rahul Pandey, Rubin Bahuva. Cook County Hospital,Chicago,Illinois Collapsing FSGS is commonly described in HIV patients, though many cases have been reported in non-HIV related diseases in the recent years. We present a rare case of collapsing FSGS in a patient with Still's disease. Case Presentation: A 43 y/o hispanic female with no significant past medical history presented with fevers and joint pains for 5 months. P/E revealed a temperature of 103.2 F, diffuse macular skin rash, axillary lymphadenopathy, hepatosplenomegaly, synovitis at the wrists and pedal edema. Labs revealed: WBC 18,000, 88% neutrophils, BUN/Creat 47/6.8, Ferritin 1650, reactive hyperplasia on lymph node biopsy, nephrotic range proteinuria of 8 gm/day, negative ANA and RF and negative viral, bacterial and fungal blood cultures. A detailed work up was negative for infection, malignancy, rheumatologic or autoimmune diseases. She was diagnosed with Adult Still's disease as per the Yamaguchi criteria. Renal biopsy results were consistent with the collapsing FSGS. She was started on Prednisone and all her systemic symptoms resolved with regression of her proteinuria from 8gm/day to 3 gm/day. Her renal function has remained stable for the past 18 months with a BUN/Creat of 42/4.0 with no dialysis requirements. Discussion: Non HIV related FSGS has been described in patients with Parvovirus B19 infection, autoimmune disorders, Hepatitis C viral infection and rarely in patients using Pamidronate; our patient had a negative workup for all of the above. In recent years, patients with Still's disease have been described to have proteinuria and hematuria, though very little has been elucidated in terms of histologic diagnosis. Collapsing FSGS is typically described as an aggressive variant of FSGS with rapid progression to end stage renal disease and poor response to treatment. Notably in our patient, the renal disease regressed parallel to the symptoms of Still's disease, which might point to a better prognosis, and hope of resolution in such cases. Also it suggests a common pathophysiology, possibly immune complex mediated, of the two conditions. Early recognition and intervention for glomerular involvement in Still’s disease may thus help us better understand the disease mechanisms and the association between the two disease entities.
99
FACTORS RESPONSIBLE FOR REDUCTION IN EFFECTIVE IONIC DIALYSANCE (EID) DURING HEMODIALYSIS (HD). Manasvi Jaitly, Sumit Mohan, Muhammad Mujtaba, Herman Anderson, Jen-Tse Cheng, Velvie Pogue. Harlem Hospital, NY.
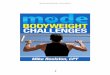
Correlation of EID and Qbw
End of Dialysisy = 0.66x + 22, r = 0.85, p<0.01
Start of Dialysisy = 0.58x + 58,r = 0.85, p<0.01
150
225
300
225 300 375Qbw (ml/min)
EID
(m
l/min
)
Effective Ionic Dialysance calculated using changes in dialysate Na+
conductivity is an online measure of HD adequacy. EID is measured at regular intervals by the Gambro® Phoenix dialysis system during treatment. Access recirculation (AR) and cardiopulmonary recirculation (CPR) are thought to affect EID during dialysis. We observed a ? in EID during HD and attempted to explain this ?. Data were collected for 9 pts in the first and last 30 mins of treatment. We measured AR, access blood flow (Qa), cardiac output (CO), actual blood flow (Tb) using ultrasound dilution. Compensated blood flow (Qb) was recorded from the dialysis system. Blood and dialysate samples were obtained to calculate dialyzer clearance for urea (KdUN) and creatinine (KdCr). Plasma protein and hematocrit were measured to calculate the total blood water flow (Qbw) and plasma water flow (Qpw).A significant ? in the EID (247 v 221, p<0.01), KdUN (280 v 228, p<0.02) and KdCr (215 v 171, p<0.01) was noted at the end of treatment in the absence of a significant ? in Qb (398 v 396, p=ns). However, a significant ? in Tb (374 v 355, p<0.01), Qbw (319 v 299, p<0.01) and Qpw (215 v 192, p<0.01) was seen. The Qa (903 v 879, p=ns) and AR (0 v 0) did not change but the ?CO (5.4 v 4.3, p<0.01) at the end produced a significant ?CPR (16% v 19%, p<0.02). A significant (p<0.01) linear relationship was seen between (Tb, Qbw,Qpw) and (EID, KdUN, KdCr). We propose that ?Qbw during dialysis
because of continuing UF leads to?EID. Other causes of ?EID may include ?CPR and ?dialyzer surface area (reflected by ?EID for the same Qbw towards the end of HD). The ?Qbw and ?Qpw without a significant ?in Qb, underscores the importance of using Tb to assess Kd. In conclusion
this study shows the contribution of ?Qbw and ?dialyzer surface area to ?EID during treatment.
100
NKF 2007 Spring Clinical Meetings Abstracts A49





![Erythropoietin or Darbepoetin for patients with cancer - meta … · 2015. 6. 23. · [Intervention Review] Erythropoietin or Darbepoetin for patients with cancer - meta-analysis](https://img.dokumen.tips/doc/110x75/5ff17f74f9f4533f6a3db127/erythropoietin-or-darbepoetin-for-patients-with-cancer-meta-2015-6-23-intervention.jpg)