Embed Size (px)
Citation preview

9/15/2011
1
Managing
Tips and Techniques for keeping treatment on course
invisalign® Aligner Tracking Issues
• Dr. Karol Miranda
● DDS Universidad Latino Americana de Ciencia y Tecnología, (ULACIT), Costa Rica.
● Private Practice for 6 years
● Actively treating Invisalign patients
● Associated professor at the ULACIT, College of Dentistry
● Presently working with Align Technology, and involved in clinical education at the Treat Facility in Costa Rica
The statements, views and opinions expressed in this program and related course materials are those of
the speaker.
Align Technology, Inc. may not endorse such statements, views or opinions.
Attendees are responsible for legal and regulatory compliance of any marketing and referral programs.
Unplanned reaction
Not on course
Probable Root causes
1. Lack of inter-proximal space
2. Attachment disengaged
3. Moving to quickly
Possible Reactions
1. Buttons and elastics
2. Go back to the best seating aligner
3. Mid course correction
Regardless of which decision you
make… it’s inconvenient and costly

9/15/2011
2
Research indicates that 90% of the time clinicians after trying the other two methods* still need a
Mid-Course Correction for the same issue
90%
*Buttons/elastics and/or back to best seating aligner
Being efficient… time management
GROWTH
Planning to avoid and/or lessen the impact of the bumps along the road Today’s lecture will focus on being proactive
instead of reactive to Invisalign® aligner fitting
issues. For more information on individual
situations in which the aligners stop tracking;
please refer to the attached PDF file.
Please note!!!
Built into the ClinCheck® Treatment Plan
Planned reaction (Class II elastics)

9/15/2011
3
Built into the ClinCheck® Treatment Plan
Planned reaction (IPR and attachments)
To be proactive you need to understand these tooth movement
principles of invisalign® aligners
1. Apply a pushing force on unlimited tooth surfaces… as required
2. Multiple tooth movements can be performed at one time… torque + rotation + leveling
3. Force levels are calculated and adjusted as needed for each tooth and/or multiple teeth within optimal biological levels
1. Apply a pushing force on the available tooth surface(s) … as required
2. Multiple tooth movements can be performed at one time… torque + rotation + leveling
3. Force levels are calculated and adjusted as needed for each tooth and/or multiple teeth within optimal biological levels
Bench tested with the Force Measurement
Apparatus (FMA)
Let’s look at a situation where these principles were programmed
and implemented clinically
Courtesy of Dr. Janice Grossman

9/15/2011
4
Initial records Initial records
Recent history of fixed orthodontics
Initial ClinCheck®Beginning Initial periapical radiographs
Initial ClinCheck®Projected End
A dynamic representation of the right cuspid root movement
Simulated roots for demonstration purposes… not real

9/15/2011
5
A dynamic representation of the central incisor root movements
Simulated roots for demonstration purposes… not real Simulated roots for demonstration purposes… not real
A dynamic representation of the left cuspid root movement
Goal was parallel roots, crowns and equal implant spaces
ClinCheck® treatment model was based on the tooth movement principles of Invisalign® aligners
1. Creating surface(s) to push on… Smaller pontics and large attachments
Creating surface(s) to push on…

9/15/2011
6
2. Multiple tooth movements can be performed at one time… torque + rotation + leveling
Staging
3. Force levels are calculated and adjusted as needed for each tooth and/or multiple teeth within optimal biological levels
Six months progress (½ the way)Initial
Six months progress
Total treatment time 11 months
Before
After
Final position
The root parallelism is very remarkable… no refinements or auxiliary treatment

9/15/2011
7
Using your best diagnostic and treatment planning tool(s) to help you stay on course
Top 6 things you need to review in your ClinCheck® model to stay on track
Interincisal angleInterproximal space
Attachments
Tooth size discrepancy
Root MovementsInitial Bite Set
Bitesetting
TIPSUse articulating paper
90 degree buccal shots
TIP Compare photos with ClinCheck model The diagnosis and treatment approach is based on what you see!! 45 degrees
60 degrees
90 degrees
Class I or Class II?

9/15/2011
8
Anterior overjet view helps determine the most anterior
contact(s)
TIP TIPCan send photos of study models with
occlusal marks and scribe lines… if needed to verify the bite
Patient appears to be
biting with the
mandible forward?
Photos with articulated marks verified the patient had
postured forward in the initial photos… bite was reset
There is more inter-occlusal contacts
There are anterior
inter- occlusal stops
Bite set… based on inaccurate photos
Bite set… based on accurate photos
Inaccurate Bite Set
1.Initial bite set
Unnecessary Movements
Occlusal problems
Unnecessary IPR Midline Shift
Possible Clinical Consequences

9/15/2011
9
Root movement
Understand where and type!!!
Relative movements are more
Predictable
and stable
Relative extrusion Pure extrusion
Use these tools to obtain information on root movements
Which teeth will have
significant root
movement?

9/15/2011
10
Superimpose Superimpose
Where are the roots moving?
White is the final stage
To help identify root movementDraw imaginary lines
Does the right central need an attachment?
Buccal view is great to evaluate the amount and type of incisor retraction
Can you see that the maxillary
incisors had bodily retraction? For Lingual root
torque the software will add Power Ridges
Using the ClinCheck® to identify root movement
You can see them in the Treatment
Overview

9/15/2011
11
Do the lower incisors need attachments?
With the long clinical crowns and black triangles… this amount of
incisor root movement shouldn’t need any attachments
The Grid It provides linear measurements
2mm of mesial root uprighting… needs an
attachment
Before After
Tooth Movement Assessment TMA
Another great tool to help identify some significant root movements
TMA helps quantify what you see
… and plan ahead to take care of any challenging tooth movements
challenging tooth
movements
Buttons and elastics for rotation and A-P… a
planned reaction in the Invisalign®aligner
treatment

9/15/2011
12
CC: Maxillary midline
diastema
History of maxillary first
molar extractions
What you may expect if
the principles of
Invisalign aligner tooth
movement aren’t
followed
Watch the maxillary central incisors!!Progress records… since the maxillary central
incisor crowns were starting to tip mesial
Root cause(s)
Crowns moving mesial from the
beginning
Timing of attachments
Lack of pushing surfaces
Proactive
Different staging
Place attachments from the start
Create space around the teeth
Reactive
Refinement
Auxiliary techniques

9/15/2011
13
Mandibularexcess 3-3
Mandibular excess 6-6
0.88mm 3.88mm
Teeth 6-7 9-10
Space 0.7mm 0.5mm
Teeth 27-28 28-29 29-30 19-20 20-21
IPR 0.3mm 0.3mm 0.3mm 0.2mm 0.2mm
Auxiliary treatment required to achieve root parallelism
Buttons and C-Chain to tip the roots mesial
An example of before and after with the use of auxiliaries
BEFORE AFTER
We are not going to let
the same result take
place a second time.
Attachments as well as mesial and distal tooth surfaces to push on……
9/15/2011
14
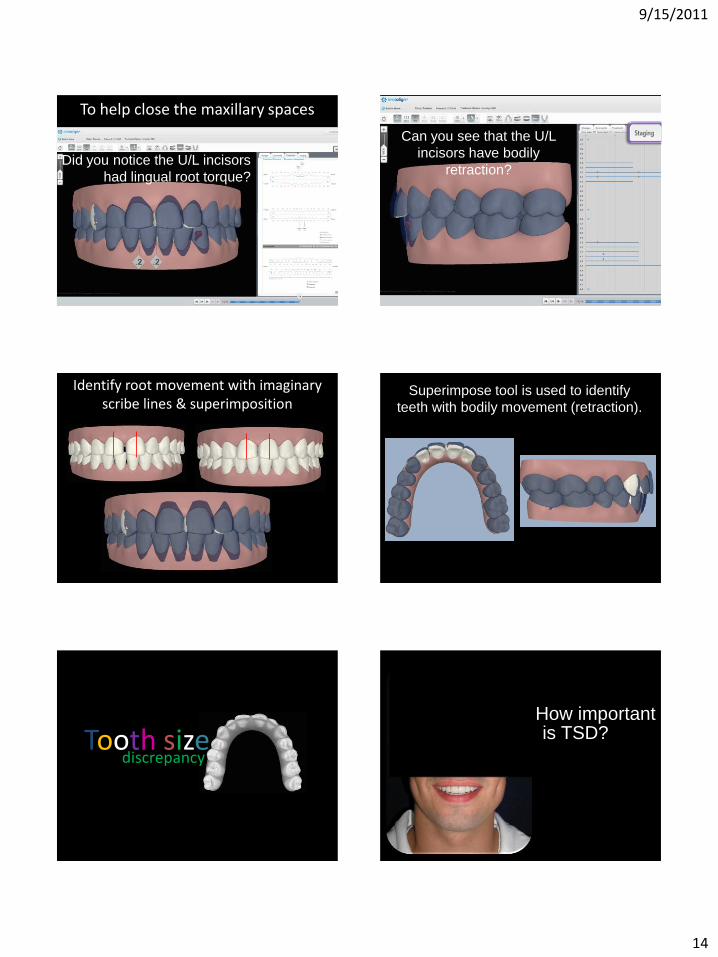
To help close the maxillary spaces
Did you notice the U/L incisors
had lingual root torque?
Can you see that the U/L
incisors have bodily
retraction?
Identify root movement with imaginary scribe lines & superimposition
Superimpose tool is used to identify
teeth with bodily movement (retraction).
Tooth sizediscrepancy
How important is TSD?

9/15/2011
15
Where would you say the TSD is? Maxillary lateral incisors are smaller than ideal
Post Splint
Centric Relation Occlusion(CRO)Treatment for 6 months
with the invisalign® System
TSD resolved by creating space around the
undersized maxillary laterals
Harmony established with a combination of
Invisalign and restorations

9/15/2011
16
What if… Tooth Size Discrepancy is not
considered?
Could result in :
1. Overretraction of the anterior teeth… posterior
openbite.
2. Compromised esthetics
3. Less than ideal occlusion… poor stability
AttachmentsGo Optimized
Add attachments to improve the engagement between the tooth
and the aligner to make root movements more predictable

9/15/2011
17
If you want to add or remove attachments use the Attachment Interface
The Future is even brighter in the world of attachments
SPACEInteproximal
Create spaces in the direction the teeth are moving this will improve the engagement
between the tooth and the aligner, making the movement more predictable
Stage 0: No space to move the lateral
Stage 3: Space is being created for the lateral
IPR before aligner 15IPR is prescribed when there is adequate clinical
access
ANGLEInterincisal

9/15/2011
18
Why the inter-incisal angle is so important?
1. There is a close relationship between the inter-incisal angle and the angle of the condylar eminence… affecting the functional occlusion
2. Esthetics
3. Long term stability… retention
Reviewing the ClinCheck® Treatment Plan
Inter-Incisal Angle
The Inter-incisal angle is patient specific
There is no standard Inter-incisal angle it is based on the occlusion
Being proactive at the ClinCheck® treatment planning stage can help keep you and the patient on track
Providing excellent results
It was a Pleasure!!! QUESTIONS?

9/15/2011
19
To obtain your CE certificate for this program please complete a brief survey at:
www.AligntechInstitute.com/asksurvey
Upon completion of your survey* you will have immediate access to your CE certificate.
*This survey is only available to the participants who attend the “live” presentation via the webinar/phone. Participants who complete the archived program on AligntechInstitute.com need to complete a CE test to obtain their CE certificate.

















