-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
1/49
NOSOCOMIAL INFECTION
Hari Kusnanto
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
2/49
"It may seem a strange principle toenunciate as the very first
requirementin a hospital that it should do the sick
no harm"
Florence Nightingale
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
3/49
Nosocomial infection =
Any infection that is not present orincubating at the time the
patient isadmitted to the hospital
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
4/49
Nos oc om ial in fec t ion :
It is an infection acquired in a medicalsetting in the course of
medical care. Itmeets the following criteria:
Not found on admissionTemporally associated with admission or
aprocedure at a health-care facilityWas incubating at admission but
related to aprevious procedure or admission to same orother
health-care facility.
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
5/49
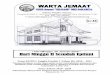
How hazardous is healthcare?Dr. Lucien Leape Harvard Medical
School. USA
Dangerous Regulated Ultrasafe
(>1/1000 ) (< 1/100,000 Total lives
lost peryear
1
10
100
1000
10,000
100,000
1 10 100 1000 10,000 100,000 1M 10M
Bungee jumping
Mountainclimbing
Healthcare
Driving
Chemicalmanufacturing
Chartered
flights
Scheduled airlines European
railroads
Nuclear power
Number of encounters for each fatality
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
6/49
At any time, over 1.4 million people worldwide are sufferingfrom
infections acquired in hospital.Between 5% and 10% of patients
admitted to modern
hospitals in the developed world acquire one or
moreinfections.The risk of health care-associated infection in
developingcountries is 2 to 20 times higher than in developed
countries.In some developing countries, the proportion of
patientsaffected by a health care acquired infection can exceed
25%.
In the United States, 1 out of every 136 hospital
patientsbecomes seriously ill as a result of acquiring an infection
inhospital; this is equivalent to 2 million cases and about 80000
deaths a year.In England, more than 100 000 cases of health
care-associated infection lead to over 5000 deaths
directlyattributed to infection each year.A NZ study of
hospital-acquired infectionestimated prevalence rate of 9.5%
(Graves 2003)
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
7/49
History of infection control and hospital epidemiology
Pre 1800: Early efforts at wound prophylaxis
1800-1940: Nightingale, Semmelweis, Lister, Pasteur1940-1960:
Antibiotic era begins, Staph. aureus nurseryoutbreaks, hygiene
focus1960- 1970s: Documenting need for infection control
programs, surveillance begins1980s: focus on patient care
practices, intensive careunits, resistant organisms, HIV1990s:
Hospital Epidemiology = Infection control, quality
improvement and economics2000s: ??Healthcare system
epidemiology
modified from McGowan, SHEA/CDC/AHA training course
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
8/49
Opportunities and Problems
Hospitals are complex institutions wherepatients go to have the
i r heal th pro blemdiagno sed and t reated
But,
hospitals and medical/surgicalinterventions in t rodu ce r i sks
that mayharm a patients health
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
9/49
Additional morbidityProlonged hospitalizationLong-term physical,
developmentaland neurological sequelaeIncreased cost of
hospitalizationDeath
Consequences of Nosocomial Infections
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
10/49
Challenges
Make a hospital safe Prevent harm to the patient and
employees initial focus on infectious diseases increasingly all
adverse (harmful) events
are targets
Improve hospital efficiency Eliminate unnecessary costs
Eliminate wasteful practices
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
11/49
Responsibilities of the Infection Control Program
Surveillance of nosocomialinfectionsOutbreak
investigationDevelop written policies forisolation of patients
Develop written policies toreduce risk from patientcare
practicesCooperation with
occupational healthCooperation with qualityimprovement
program
Education of hospitalstaff on infection controlOngoing review of
allaseptic, isolation andsanitation techniques
Monitoring of antibioticutilizationMonitoring of
antibioticresistant organisms
Eliminate wasteful orunnecessary practices
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
12/49
Monthly incidence of febrile episodes and associated BSI rates
per1000 discharges in the pediatric inpatient units from January
to
December 1999
0
100
200
300400
500
600
700
800
J a n
F e b
M a
r c h
A p r i l
M a
y
J u n e
J u l y
A u g u s t
S e p t .
O c t .
N o v .
D e
c .
Month
R a
t e / 1 0 0 0
d i s c
h a r g e
Febrile episodesBSI
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
13/49
Staphylococcus aureus
Common Many sites esp blood, wounds
Bacteraemia
50% hospital onset 1/3 of community onset are health care
related
High mortality in bacteraemia
Pre-antibiotics 82% MSSA median 25% MRSA median 35%
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
14/49
Blood stream infections: seriousmorbidity
Blood stream infections Renal failure, osteomyelitis, prolonged
antibiotic
therapy etc
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
15/49
Many primary sites for BSI;but IV catheters main site at all
major hospitals
Body system(TCH data) 1998 1999 2000 2001 2002 2003 2004
Total
IV Device 109 72 81 54 39 45 42 442
Respiratory 50 36 54 31 41 49 47 308
GIT 47 38 46 43 40 41 59 314
Genito-urinary 43 38 38 43 45 54 70 331
Skin 24 22 22 19 18 27 35 167
Unknown 19 39 32 37 32 28 27 214
Cardiovascular 13 9 10 12 8 19 14 85
Musculo-skeletal 10 14 5 13 12 20 19 93
Haematology 9 17 10 15 16 15 20 102
Maternal 9 4 5 5 6 3 2 34
Neurology 4 13 8 7 6 5 5 48
Other 0 0 2 1 1 1 0 5
Prim Bacteraemia 0 5 7 8 7 9 14 50
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
16/49
IV catheter infections can be reduced
Too many used
In for too longPoor selection of most appropriate cathetersPoor
selection of sites
Almost every doctor inserts them
including CVCs - even if little trainingCVCs used instead of
peripheral catheters
for convenience BUT much higher per day risk
W h i t ll t
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
17/49
We can have an impact on all typesof infections
Surgical site Infection rates can be decreased
Blood stream infections
Especially IV catheterUrinary tractPneumonia
All types If you recognize there is a problem
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
18/49
QI versus Regulatory Strategies inInfection Control
Regulatory approachExternal organizationsestablish rules
andregulations
Data collection forcomparison with outsidestandardsInspections
forcompliancePenalties for non-compliance
TQM/QI approachInternal organization ofhospital staff to
developgoals and methods
Data collection for internalreviewContinuous efforts
toimproveFailure belongs to theentire system, not anindividual
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
19/49
Organizing for Infection Control
Requires cooperation, understanding andsupport of hospital
administration andmedical/surgical/nursing leadership
There is no simple formula: Every hospital is different Every
hospitals problems are different Every hospitals personnel are
different The hospital must develop its own uniqueprogram
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
20/49
Changes in Nosocomial Infection Rates inHospitals with or
without Effective Programs
Infection site andpatient risk
Hospitals with veryeffective programs
Hospitals withineffective programs
Surgical Wound % %High risk -48.0 +13.8Low risk -23.6 +21.3
Urinary TractHigh risk -35.8 +18.5Low risk -41.6 +30.7
PneumoniaSurgical patients -7.3 +9.3Medical patients -7.7
+10.0
Bloodstream All patients -27.6 +25.5
SENIC Study, CDC
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
21/49
Essential Components of an EffectiveInfection Control Program
(after SENIC)
One full time infection control practitionerper 250 beds optimal
ratio may be different
A physician with training and expertise ininfection
controlSurveillance and feedback of rates toclinicians
Control activities (interventions, policies,training)
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
22/49
Personnel Hospital Epidemiologist MD with clinical training
Usually part time salaried by the hospital for
infection control duties and part time asinfectious diseases
clinician
Training in infection control
Infection Control Practitioner Usually a nurse but can be a
microbiologist Has clinical experience before entering
infection
control
Full time in infection control, no other clinical
oradministrative duties Training in infection control
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
23/49
Organizing for Infection Control
Main elements Develop an effective surveillance system Establish
policies and regulations to
reduce risks Develop with clinicians (physicians and
nurses) Develop and maintain a program of
continuing education for hospitalpersonnel
Use scientific (epidemiologic) method tostudy problems and test
hypotheses
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
24/49
Organizing for Infection Control
Additional elements of an effectiveprogram Antibiotic monitoring
and control Microbiologic laboratory liaison Antibiotic
susceptibility data
dissemination Occupational health
Provide resource to other departmentsfor quality improvement
study designand data analysis
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
25/49
Key elements of surveillance
Defining as precisely as possible theevent to be surveyed (case
definition)Collecting the relevant data in asystematic, valid
way
Consolidating the data into meaningfularrangementsAnalyzing and
interpreting the dataUsing the information to bring aboutchange
adapted from R. Haley
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
26/49
Infection Control Committee Purpose Advisory
Review ideas from infection control team Review surveillance
data
Expert resource Help understand hospital systems and
policies
Decision making Review and approve policies and surveillance
plans Policies binding throughout hospital
Education Help disseminate information and influence
others
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
27/49
Infection Control Committee
Committee Representatives
Hospital Epidemiologist Infection Control Practitioners
Administrator
Ward, ICU and Operating room Nurses
Medicine/Surgery/Obstetrics/Pediatrics Central Sterilization
Hospital Engineer Microbiologist Pharmacist
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
28/49
Infection Control Committee
Qualifications to be on the committee Interest Represent group
in hospital
Experts in their field Diplomatic Good communicators
Resources : Where to get more information or help
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
29/49
Resources : Where to get more information or help Training
Courses Society of Hospital Epidemiologists of America (SHEA)
Association of Professionals in Infection Control
(APIC) National courses and congressesBooks Textbooks: Bennett
and Brachman - Wenzel - Mayhall APIC Curriculum and Guidelines CDC
GuidelinesJournals Infection Control and Hospital Epidemiology
Journal of Hospital Infections American Journal of Infection
ControlConsulting services National: CDC, Ministry of Health
Colleagues
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
30/49
Risk factors for surgical wound infection
AgeObesityMalnutrition (low albumin)
DiabetesSteroids/immunosuppressionProlonged
pre-ophospitalization
Infection at anothersiteProlonged procedure
DrainsUrgency of surgeryForeign bodySkill of surgeon
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
31/49
Strategies to develop effectivepatient care practices
Team collaborationStaff educationCommunication
Identify problems with polices and procedures
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
32/49
Identify problems with polices and proceduresExample: Pre- and
Post-Operative Care
Skin shaved the nightbefore surgeryInappropriate peri-op
antibiotic prophylaxisInstruments used fordressing
changessubmerged disinfectantLarge containers ofantiseptics, no
routinefor cleaning and refilling
Eliminate shaving of skinthe night before surgerySingle dose
peri-opantibiotic prophylaxisguidelinesUse individual sterile
packsof wound care instrumentsUse small containers ofantiseptics;
clean and drycontainers before refilling
RecommendationProblem Area
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
33/49
Methods to reduce cost ofnosocomial infections
Reduce incidenceReduce morbidityShorten hospital stayReduce
costs of treating infectionsReduce costs of preventative
measuresStop ineffective control measures
Eli i t t
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
34/49
Eliminate wasteExample: Unnecessary nursing techniques
Dressing change of aseptic woundsDaily dressing change of venous
catheterdressingsDaily change of intravenous infusion sets
Preoperative shavingRoutine changing of urinary cathetersTwice
daily urinary catheter careProtective gowns except for care of
infectedpatients
Daschner, F. J Hosp Infect (1991) 18, 73-78)
Eliminate waste:
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
35/49
Eliminate waste:Unnecessary microbiologic monitoring
Routine environmental cultures of walls,floors, air, sinks, or
other hospital surfacesRoutine cultures of healthcare workers
noseand hands
Clinical cultures which are not available toclinicians in time
to help with decisionmaking
Also: Failure to generate annual summary ofculture data to
provide clinicians with datafor empirical selection of
antibiotics
Cultures of Walls Floors and Other Smooth
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
36/49
Cultures of Walls, Floors and Other SmoothSurfaces: Not
Necessary
All hospitals have some bacterial colonization ofenvironmentWhat
is the evidence that the environmentdirectly infects the
patient?
Hospitalized patients infect the environment Poor technique,
poor handwashing, poordisinfection have all been shown to infect
thepatients but these are all related to poor practicenot the
environment directly
Floors, Walls, Tables, Beds etc. should becleaned properly but
not cultured
Prolongation of Hospital Stay due to
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
37/49
Prolongation of Hospital Stay due toNosocomial Infections in the
USA
Infection Site Excess Days
Surgical Wound 6.0
Urinary tract 1.2
Pneumonia 4.0
Bacteremia 7.0
Other sites 4.2 Adapted from Dixon, Ann Int Med 89:749, 1978
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
38/49
Annual Costs and Benefits of Infection ControlProgram in a
Hypothetical 250-bed Hospital
Estimated reduction of directcosts from infectionsprevented
$246,700
Estimated infection controlprogram expenses
$60,000
Hospital savings $186,700
Each $1000 invested in infection controlwill return $3000 in net
direct cost savings
Annual Nosocomial Infection Cost Savings by Introducing
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
39/49
Annual Nosocomial Infection Cost Savings by IntroducingEffective
Infection Control Program to a 250-bed Hospital
Infection site Infectionswithout
anyprogram
Infectionswith
effectiveprogram
Infectionsprevented
Averagecost per infection
$
Totalsavings
$
Surgical wound 186 120 66 1944 128,3Urinary tract 283 195 88 318
29,5Respiratory 74 58 16 1540 24,64Bacteremia 34 22 12 2268
15,2Other sites 136 92 44 1113 48,97
TOTAL 713 487 226 $246
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
40/49
Antibiotic Prophylaxis in Surgery
Potentially an important part of surgical woundinfection
preventionMay also be a significant expense for the hospitalWhat is
the cost-benefit of prophylactic antibiotics? What is cost of wound
infection? In money? In
suffering? How effective is prophylaxis? How much can we spend
to prevent a case of wound
infection ?
Cost of Surgical Prophylaxis with Cefonocid
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
41/49
Cost of Surgical Prophylaxis with Cefonocidin a Boston Teaching
Hospital
Assuming $10 per course: $178 to prevent one breast infection
$539 to prevent one herniorrhaphy infection
$1,515 to prevent one readmission for breastinfection $622 to
prevent one readmission for
herniorrhaphy
From: Platt et al. NEJM 322:153, 1990.
Impact of Cefonocid Prophylaxis
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
42/49
p p y(per 1,000 patients)
Routine use for breast surgery wouldprevent 56 infections 23
definite wound infections
16 UTIsRoutine use for herniorrhaphy wouldprevent: 19 infections
13 definite wound infections
from: Platt et al. NEJM. 322:153,1990.
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
43/49
Organization and support
A. Institutional support Infection control as a department
Placement in the organization
Authority Personnel Other resources
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
44/49
Organization and support
B. Infection control committee membership support by the medical
staff
participation by other disciplines annual planning
Organization and support
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
45/49
Organization and support
C. Infection Control Program
quality assessment information for clinicians
educational/informational resource surveillance data
outbreak investigation assurance of appropriate asepsis,
sterilization,
disinfection minimize risk from invasive procedures/devices
use of isolation occupational health
Therapy
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
46/49
Therapy
Ideally directed toward organisms detected byculturesEmpiric
therapy may have to be given know your hospitals antibiogram
choose drugs that should be -cidal Beta-lactam drugs
Cephalosporins Glycopeptides Aminoglycosides
Therapy
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
47/49
Therapy
Ideally directed toward organisms detected byculturesEmpiric
therapy may have to be given know your hospitals antibiogram
choose drugs that should be -cidal Beta-lactam drugs
Cephalosporins Glycopeptides Aminoglycosides
h d
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
48/49
Drugs that treat Pseudomonas
CiprofloxacinCeftazidimeCefepimeTimentinPiperacillin/Tazobactam
(Zosyn)Imipenem
Fi l P i
-
8/12/2019 6. Nosocomial_Prof. Hari Kusnanto
49/49
Final Point
Three day rule: You can treat a patient with broad spectrum
antibiotics
for three days, but need to narrow spectrum of
antibioticcoverage at three days when culture and
susceptibilityresults come back!