Embed Size (px)
Citation preview

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 1/45
Anal Canal carcinoma
Academic Radiotherapy Department
Centre Oscar Lambret
Lille, France

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 2/45
ACC : 2 populations• « classical » 65 years
• Rare < 40 years
• Sex ratio F/M (3/1)
• Young : HPV (HPV 16)
• Sexually linked
• Incidence
– Male Homosexuel
• rare incidence 2/100000 – Male homosexuel HIV +60/100000

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 3/45
• Squamous carcinoma 2/3
• Sphincter extension
• anal margin, lower rectum > 50 %
• Lymph nodes ++
• Metastases rare
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 4/45
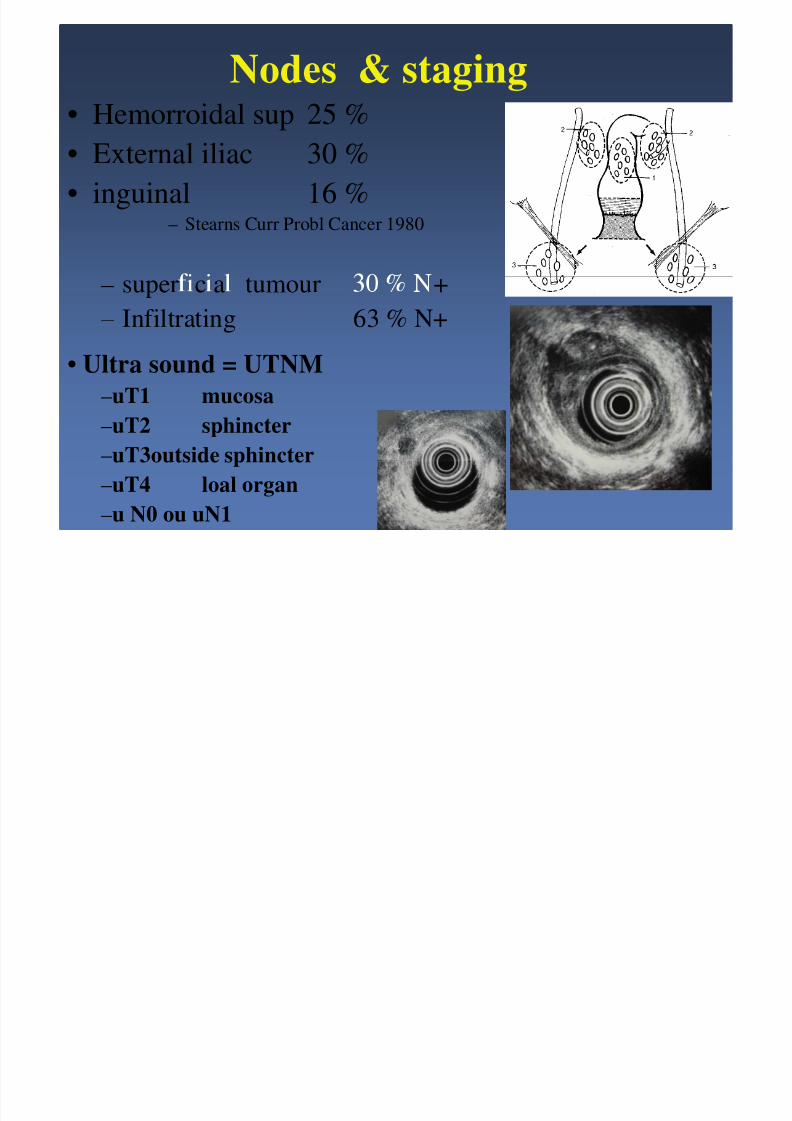
Nodes & staging• Hemorroidal sup 25 %
• External iliac 30 %
• inguinal 16 %– Stearns Curr Probl Cancer 1980
– super c a tumour +– Infiltrating 63 % N+
• Ultra sound = UTNM
–uT1 mucosa
–uT2 sphincter
–uT3outside sphincter
–uT4 loal organ–u N0 ou uN1

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 5/45
CT, MRI & Inguinal nodes
clinical US
sensibility 10-25 % 82-92 % p < 0.01
specificity 85-100 % 82-87 %
– ,
– Moslovic, Br J Obstet Gynaecol 1999
– Rossi, Eur J Cancer 1997

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 6/45
TNM (UICC 1987)
T1 < 2 cmT2 2-5 cm
T 5 m
T4 local extension(vagina, bladder)
N1 perirectal
N2 inguinal, iliac
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 7/45
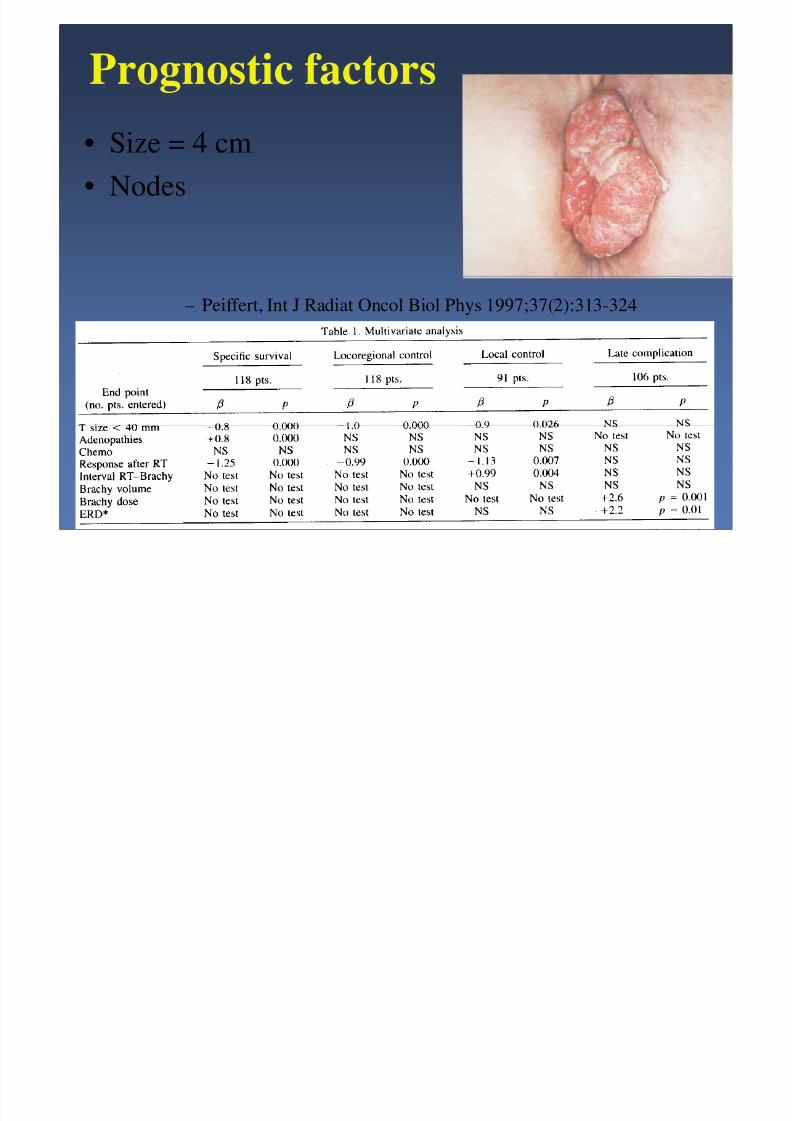
Prognostic factors
• Size = 4 cm
• Nodes
– Peiffert, Int J Radiat Oncol Biol Phys 1997;37(2):313-324

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 8/45
Exclusive surgery
• amputation• Survival at 5 years 60 %
•
• Local recurrences 30-40 %
– Boman, Cancer 1984– Clark ; Lancet Oncol 2004
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 9/45
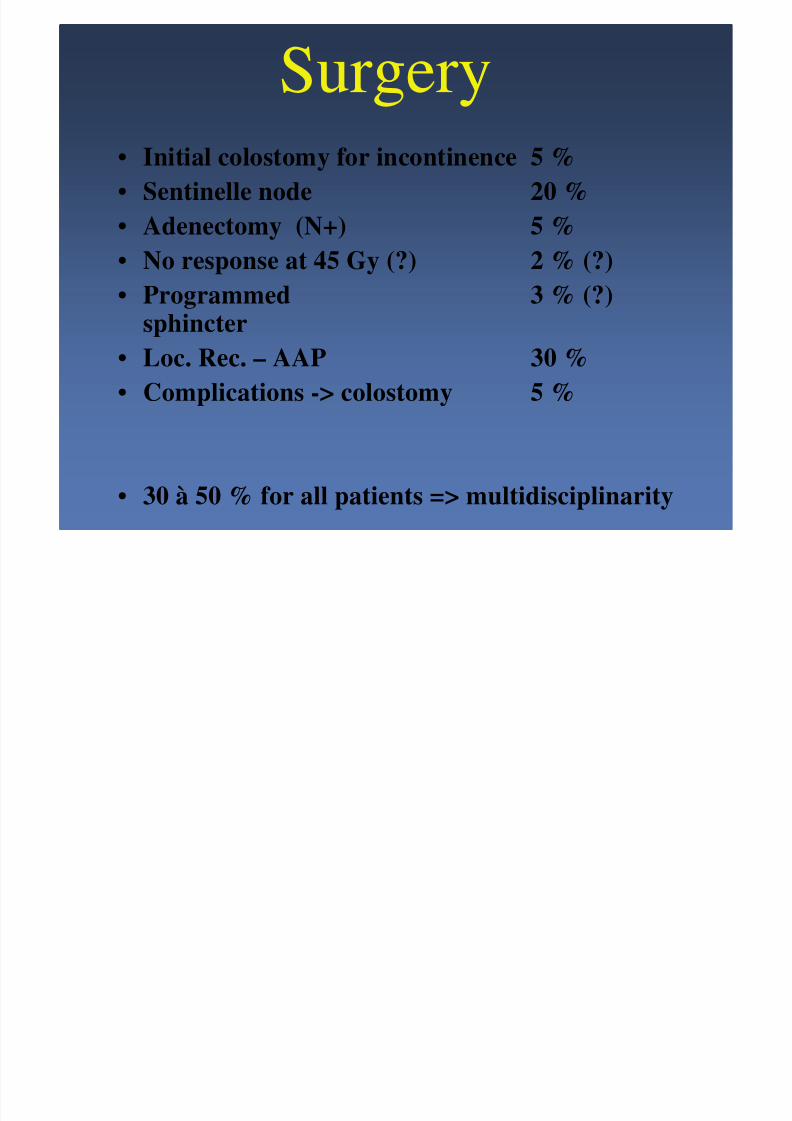
Surgery• Initial colostomy for incontinence 5 %
• Sentinelle node 20 %• Adenectomy (N+) 5 %
• No response at 45 Gy (?) 2 % (?)
• Programmed 3 % (?)sphincter
• Loc. Rec. – AAP 30 %
• Complications -> colostomy 5 %
• 30 à 50 % for all patients => multidisciplinarity
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 10/45
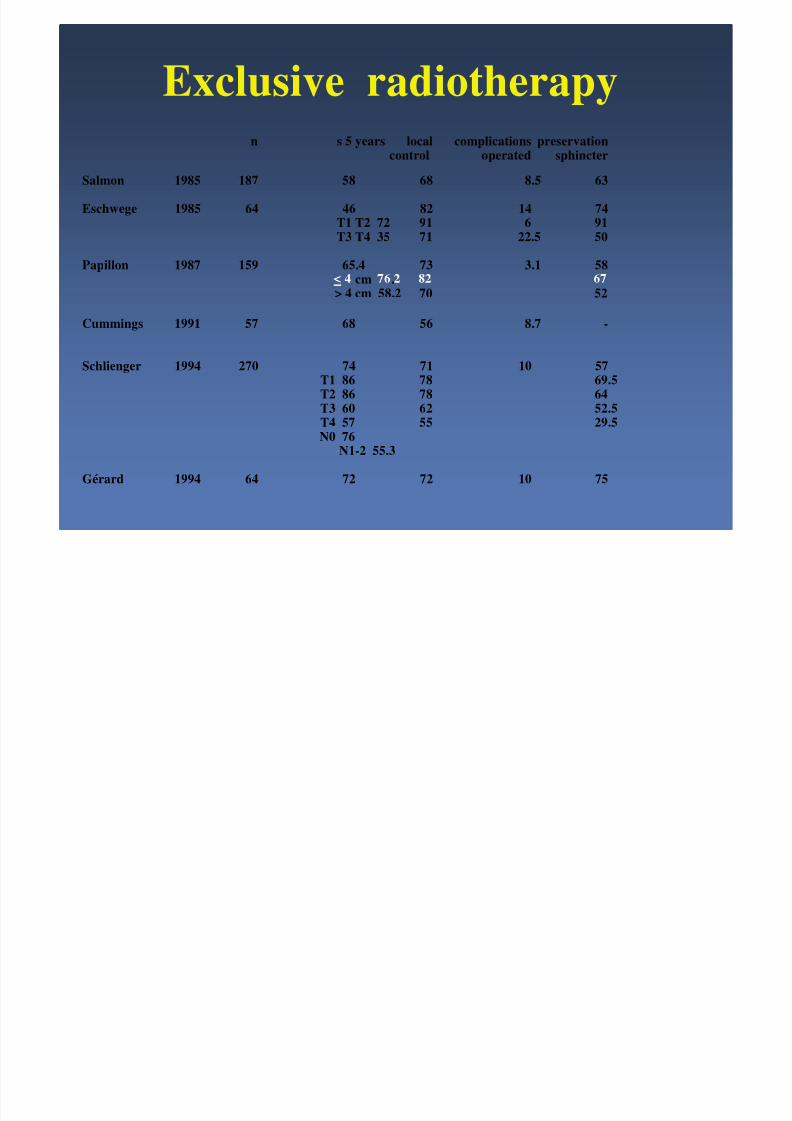
Exclusive radiotherapyn s 5 years local complications preservation
control operated sphincter
Salmon 1985 187 58 68 8.5 63
Eschwege 1985 64 46 82 14 74T1 T2 72 91 6 91T3 T4 35 71 22.5 50
Papillon 1987 159 65.4 73 3.1 58cm .
> 4 cm 58.2 70 52
Cummings 1991 57 68 56 8.7 -
Schlienger 1994 270 74 71 10 57T1 86 78 69.5
T2 86 78 64T3 60 62 52.5T4 57 55 29.5N0 76
N1-2 55.3
Gérard 1994 64 72 72 10 75

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 11/45
exclusive radiotherapy ?
5 years
w colostomy survival
Touboul T < 4 cm N0 90 % 83 %Papillon T < 4 cm N0 82 % 76 %

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 12/45
Radio-chemotherapy ?
• USA pre-operative– 30 Gy + 5 FU + MMC
–
– Nigro, Dis Colon Rectum 1974;17:354-356

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 13/45
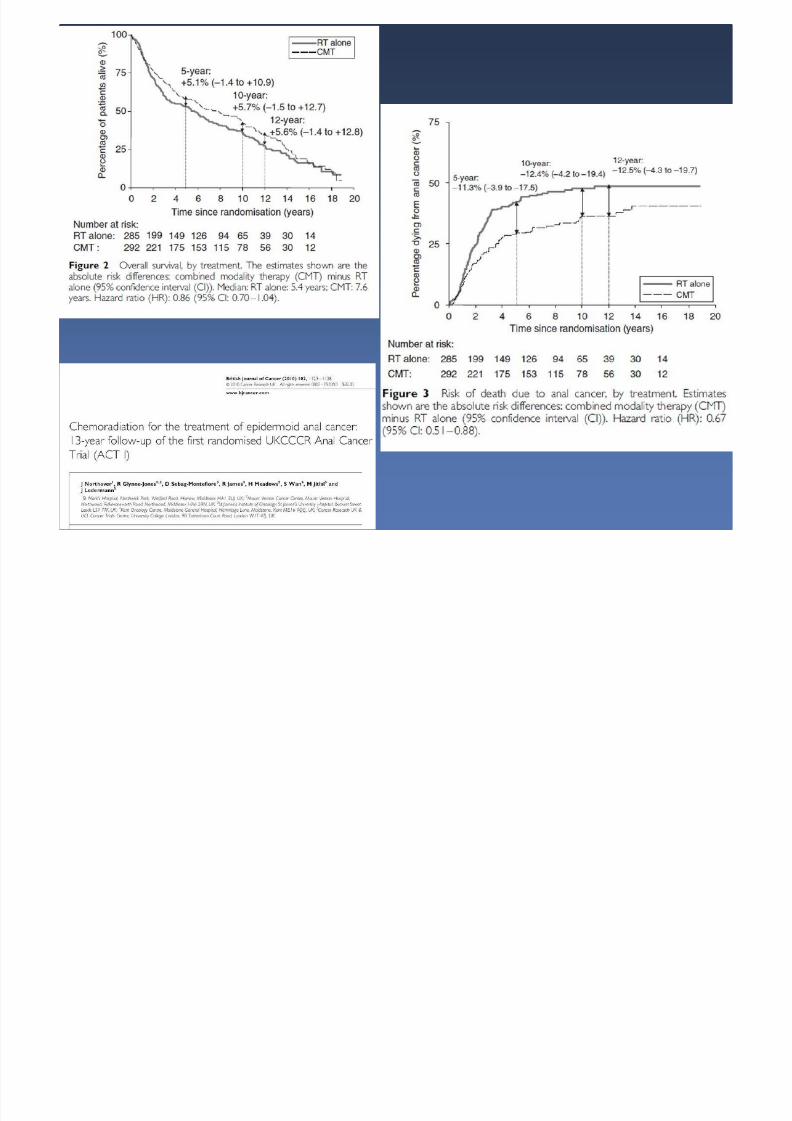
UKCCCR• n = 577
• 45 Gy 1.8/f + boost 15 Gy
+
• MMC12 mg/m2 j1
• mg m - -
at 3 years RT RT-CT
CR 30 % 39 %Local failure 59 % 36 % p<0.001
mortality 39 % 28 % p=0.02
– UKCCCR, Lancet 1996 ; 345 : 1049-54

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 14/45
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 15/45
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 16/45
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 17/45
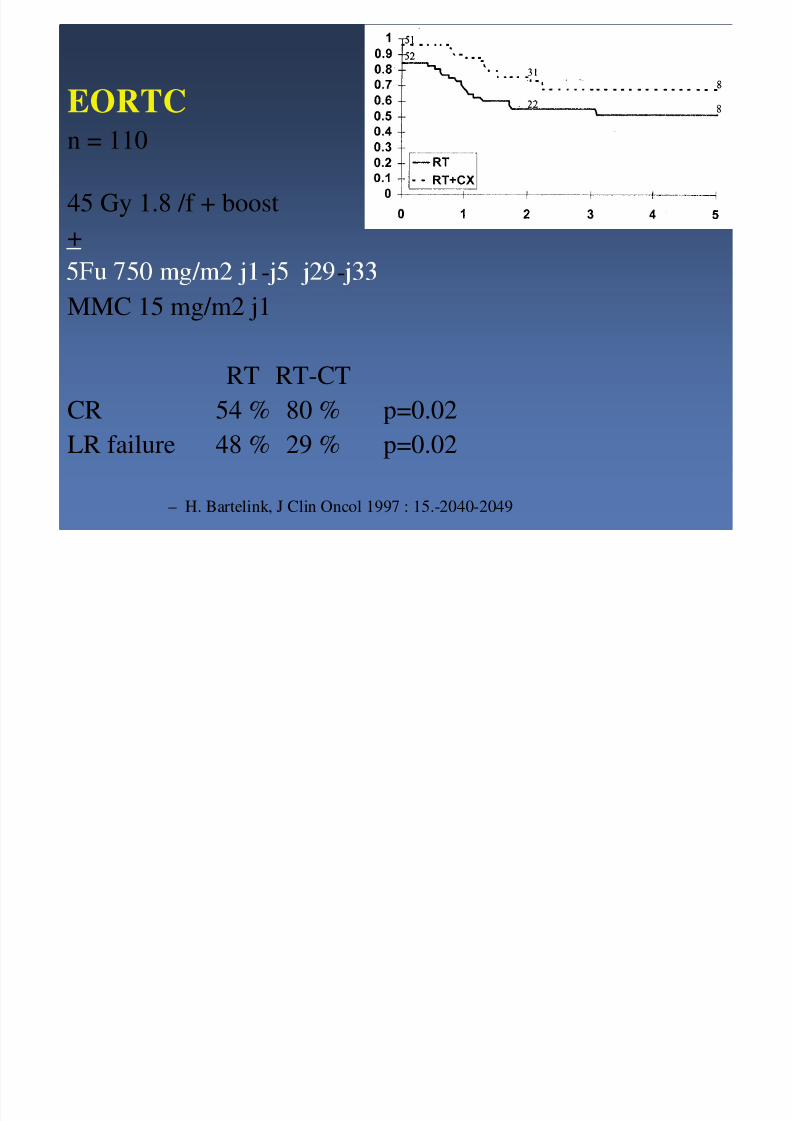
EORTCn = 110
45 Gy 1.8 /f + boost+
- -
MMC 15 mg/m2 j1
RT RT-CT
CR 54 % 80 % p=0.02
LR failure 48 % 29 % p=0.02
– H. Bartelink, J Clin Oncol 1997 : 15.-2040-2049
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 18/45
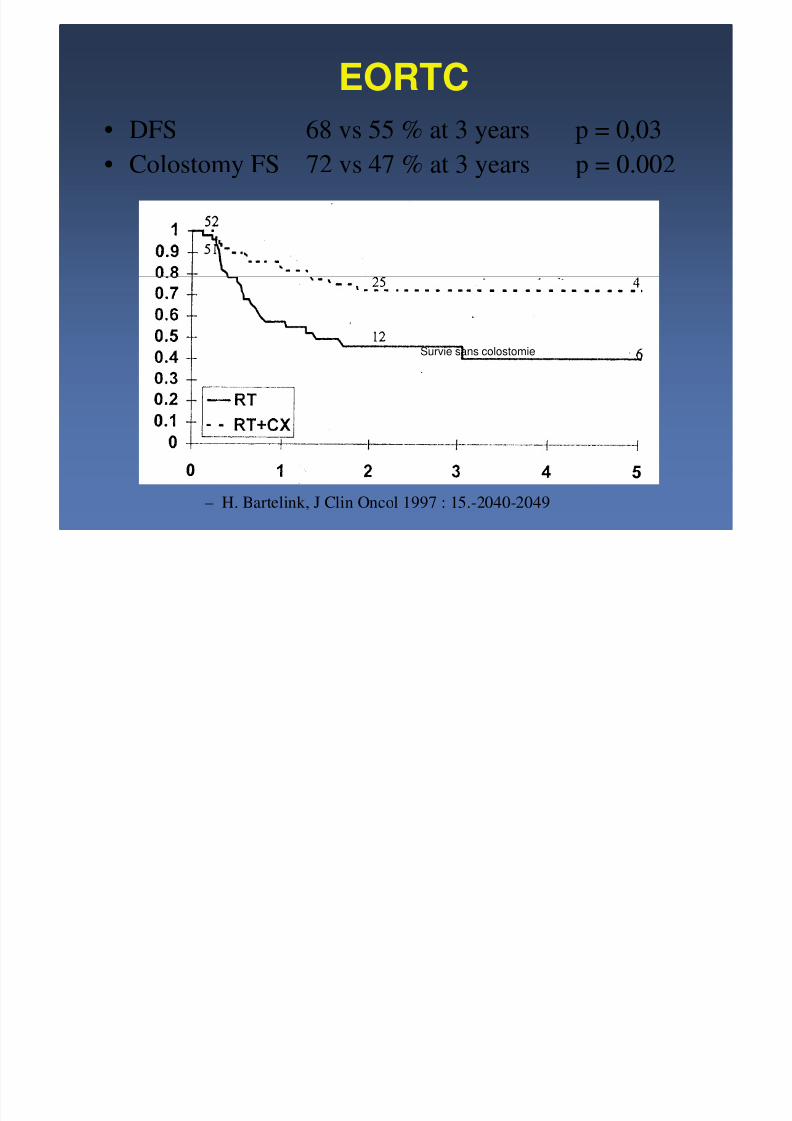
• DFS 68 vs 55 % at 3 years p = 0,03
• Colostomy FS 72 vs 47 % at 3 years p = 0.002
EORTC
– H. Bartelink, J Clin Oncol 1997 : 15.-2040-2049
Survie sans colostomie

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 19/45
RT/CT > RT for local control
• Same overall survival
• c ra o erapy
• Which chemotherapy ?

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 20/45
Mitomycin C ???
• n = 310 RTOG
• 45 Gy + 5FU 1g/m2/j j1-j4 j29-j32vs
• 45 Gy + 5FU + MMC 10mg/m2 j1 j29
5FU FU MMC
colostomy free 4 years 59 % 71 % p=0.014
DFS 51 % 73 % p=0.0003
toxicity GIII-IV 7 % 20 % p<0.001
– Flam, Pajak, Petrelli et al JCO 1996; 9 : 2527-2539
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 21/45
Mitomycin C versus CDDP ???
• 5FU-Cisplatine efficient in metastatic conditions
• 2 cycles 5FU-Platine neoadj -> 72 % RR– Peiffert, Seitz, Rougier, Annals of Oncology 8:575-581, 1997
• phase I, II : decreased toxicity
• 5FU-CDDP after 5FU-Mitomycine failure
– 25 non responding at 45 Gy + CT
– 9 Gy + 5FU 1g/m2/j j1-j4 + CDDP 100mg/m2 j2
– 50 % DFS at 4 years
– Flam, Pajak, Petrelli et al JCO 1996; 9 : 2527-2539

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 22/45
Phase III Trial ACCORD 03
• Locally advanced anal canal carcinoma
– Induction chemotherapy
– High dose radiotherapy
• First endpoint : colostomy free survival
• Secondary endpoint : QoL

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 23/45
FNCLCC ACCORD 03
CT
CDDP 5FU 2 cycl
CT
CDDP 5FU 2 cycl
No CT No CT
R
low boost
15 Gy
45 Gy
CDDP 5 FU 2 cyc
high boos
20-25 Gy
45 Gy
CDDP 5 FU 2 cycl
low boost
15 Gy
45 Gy
CDDP 5 FU 2 cycl
high boos
20-25 Gy
45 Gy
CDDP 5 FU 2 cycl

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 24/45
QoL Questionnaires
• Questionnaires– General: EORTC QLQ-C30
– pec c: - ana sp ncter conservat ve trt
• Filled out by the patients
– At the inclusion (INCL)
– Two months after the treatment (2M)
– (Every year: Y1-Y5)

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 25/45
Patients cohort
306 patients enrolled in ACCORD 03
119 patients2 QoL Q (INCL-2M)
187 patients(0 or) 1 QOL (INCL or 2M)
No difference for clinical data

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 26/45
Functional QOL scores / Time
60
70
80
90
+ 5.9 + 8.4
010
20
30
40
50
global health physical role emotional cognitive social
inclusion 2 months after ttt
* p<0.01
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 27/45
Conclusion ACCORD 03
• First study with baseline pretreatment QOLscores
• The 2 treatment intensification classes– high dose RT
– and induction chemotherapy
are not deleterious on QOL
EORTC t l 22011 40014

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 28/45
EORTC protocol 22011 - 40014Continuous fluorouracil plus mitomycin C
versus mitomycin C plus Cisplatin
as chemotherapy combination in combined radiochemotherapyfor locally advanced anal cancer.
A phase II-III study.
Trial StatusClosed
Date of activation: 29/07/2003Closed on : 19/11/2007
Targeted Sample size: 678
boost23.4 Gy 2.5 semaines
5FU 200 mg/m2/j j1-17MMC 10 mg/m2/j
36 Gy 4 sem5FU 200 mg/m2/j j1-j26
MMC 10 mg/m2/j j1
boost23.4 Gy 2.5 semaines
CDDP 25 mg/m2/j j1-8-15MMC 10 mg/m2 j1
36 Gy 4semCDDP 25 mg/m2/j j1-8-15-22
MMC 10 mg/m2 j1
R

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 29/45
Patients with measurable disease >4 cmN0 or N+ received RT (36Gy+2 week gap+23.4Gy) with either MMC/CDDP or MMC/5-FU(MMC 10mg/m(2) d1 of each sequence; 5-FU 200mg/m(2)/day c.i.v. daily; CDDP 25mg/m(2) weekly). Forty patients/arm wereneeded to exclude a RECIST objective response rate (ORR), 8 weeks after treatment, of <75% (Fleming 1, alpha=10%,beta=10%).
RESULTS:
The ORR was 79.5% (31/39) (lower bound confidence interval [CI]: 68.8%) with MMC/5-FUversus 91.9% (34/ 37) (lower bound CI: 82.8%) with MMC/CDDP.
In the MMC/5-FU group, two patients (5.1%) discontinued treatment due to toxicity versus 1129.7% in the MMC/CDDP rou .
EORTC protocol 22011 - 40014
Nine grade 3 haematological events occurred with MMC/CDDP versus none with 5-FU/MMC.
Thirty-one patients in the MMC/5-FU arm (79.5%) and 18 in the MMC/CDDP arm (48.6%) werefully compliant with the protocol treatment (p=0.005).
CONCLUSIONS:Radio-chemotherapy with MMC/CDDP seems promising as only MMC/CDDP demonstratedenough activity (RECIST ORR >75%) to be tested further in phase III trials; MMC/5-FU did not.
MMC/CDDP also had an overall acceptable toxicity profile.
Eur J Cancer. 2009 Nov;45(16):2782-91
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 30/45
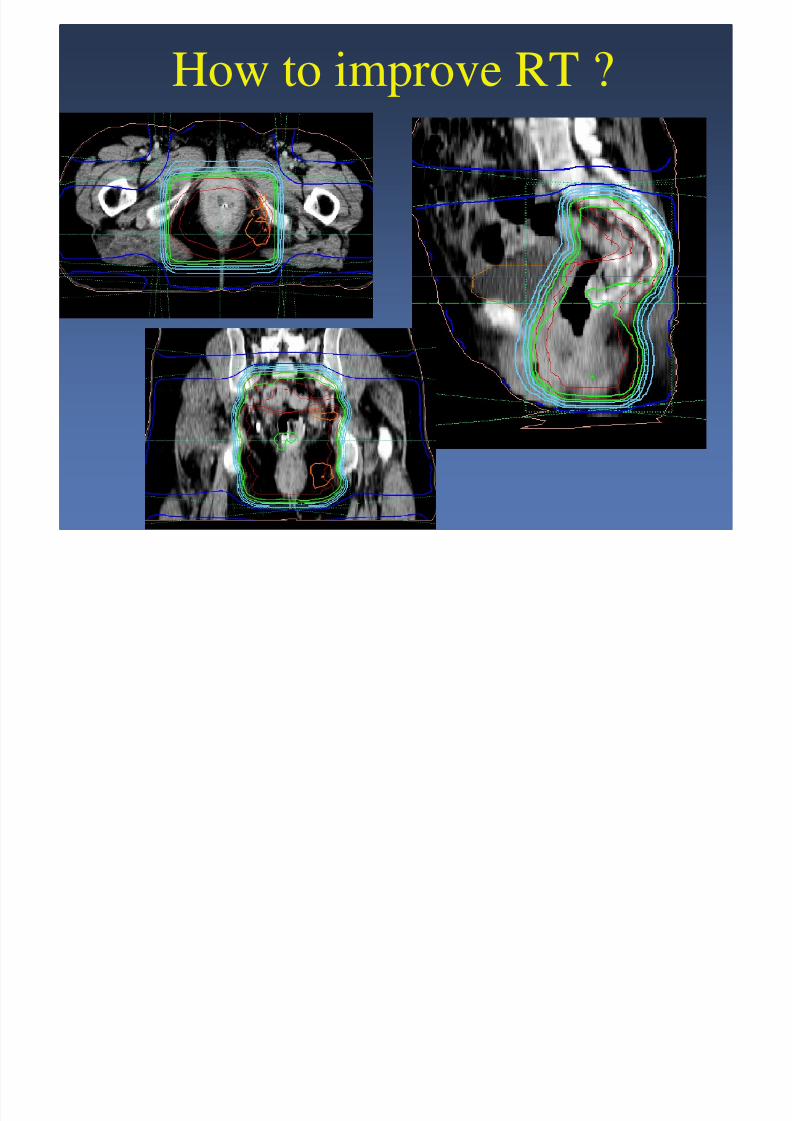
How to improve RT ?

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 31/45
Radiotherapy : short gap ?
• n = 137
• Overall treatment time
– Allal, Cancer 1997

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 32/45
BOOST• brachytherapy
• electrons
• 4 fields box
– Peiffert, Int J Radiat Oncol Biol Phys 1997;37(2):313-324
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 33/45
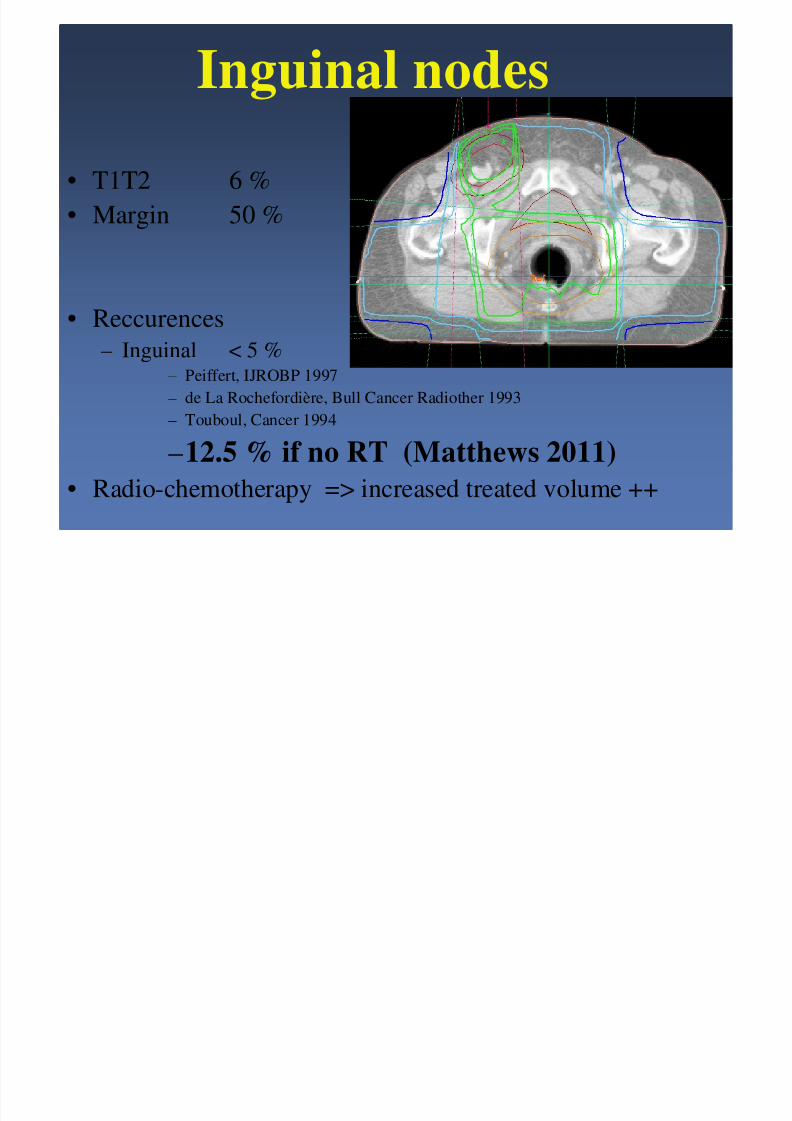
Inguinal nodes
• T1T2 6 %
• Margin 50 %
• Reccurences
– Inguinal < 5 %– Peiffert, IJROBP 1997
– de La Rochefordière, Bull Cancer Radiother 1993– Touboul, Cancer 1994
–12.5 % if no RT (Matthews 2011)
• Radio-chemotherapy => increased treated volume ++

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 34/45
N+ clinical
++
U.S.+ cytology
-
-High risk inguinal
< ligne pectinéemargin uT3
+
-radio-chemotherapy
+ sent ne e no e
Follow up
-

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 35/45
Comparison RT3D / Tomotherapy
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 36/45
Sphincter function
• Colostomy for complication
Papillon 159 2.2 %Wagner 108 9 %
Allal 125 6 %
Peiffert 118 5 %
– Peiffert, Int J Radiat Oncol Biol Phys 1997;37:313-324• Médian : 7 months
• Non stomy– Incontinence 6 %
– Some lost 19 %
– Vordermark, Radiotherapy and Oncology 1999; 239-243

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 37/45
RECURRENCES
• CHEMOTHERAPY
– 5FU, CDDP, Mitomycine C, Gemcitabine
• urgery• Reirradiation
• Poor prognosis
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 38/45
SPECIFIC CASES
• Small T1
• HIV+
• Old patients
• Rare histology– Adenocarcinoma
– Verrucus cracinoma
– melanoma

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 39/45
Small T1 : Exclusive surgery ?
survival 5 years loc. Rec .
Klotz 1967 33 61 33
Stearns & Quan 1970 30 66 63
Beahrs 1979 21 85 45Frost 1984 20 66 60
Boman 1984 18 100 22
Follow up +++++
Patients HIV+ : incidence X 60
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 40/45
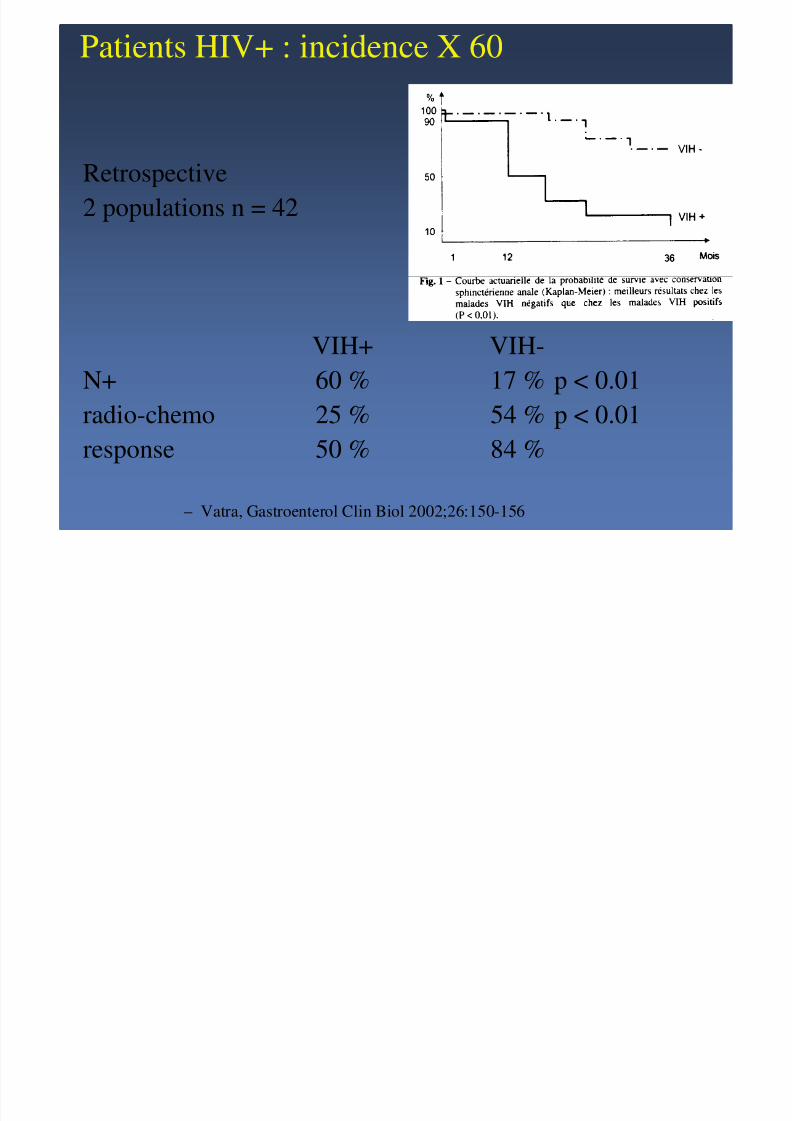
Patients HIV+ : incidence X 60
Retrospective
2 populations n = 42
VIH+ VIH-
N+ 60 % 17 % p < 0.01
radio-chemo 25 % 54 % p < 0.01
response 50 % 84 %
– Vatra, Gastroenterol Clin Biol 2002;26:150-156
P i HIV

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 41/45
Patients HIV+
• CD4 < 200/ µµµµl
– Toxicity ↑↑↑↑, 50 % colostomy
– rt-ct difficult• CD4 > 200/ µµµµl
– Standard tt
– same toxicity
– pronostic ⊥⊥⊥⊥– Hoffman, Int J Radiat Oncol Biol Phys 1999;44:127-131
• Tritherapy before radiochemotherayPlace, Dis Colon Rectum 2001;44:506-512
• HIV + = HIV - : Fraunholz 2011
8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 42/45
Old Patients
• n = 58 age > 75 ans• RT 39.6 Gy + boost 20 Gy
• CT 5FU 600 mg/m2/j j1-j4 MMC 9.5 mg/m2 j1
RT RTCTtt 95 % 95 %
toxicity G3 32 % 68 %
Survival at 5 years 49 % 59 %late G 3-4 0 5
– Allal, Cancer 1999;85:26-31
• Verrucous carcinoma

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 43/45
– Slow growing
– aggressive– Surgery
– Chu, Dis Colon Rectum 1994
• Melanoma– =
– radiosensitive– Malaguarnera, Bull Cancer 1997
– Brady, Dis Colon Rectum 1995
• Adenocarci• noma
– treatment = squamous
– Joon, Int J Radiat Oncol Biol Phys 1999
St d d t t t

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 44/45
Standard treatment
• T < 4 cm N0 (T1N0)
– Radiotherapy– 45 Gygap 3 weeks boost 15 - 20 Gy
• T > 4 cm and/or N+
– concomitant Radiochemotherapy
– 45 Gy gap 3 weeks boost 15 - 20 Gy
– 5Fu MMC or 5Fu CDDP

8/6/2019 6 Lartigau Anal Canal
http://slidepdf.com/reader/full/6-lartigau-anal-canal 45/45
CONCLUSION
• Rare
• Conservative treatment
• Combined chemo radiothear
• Thanks to X. Mirabel, Lille & D Peiffert, Nancy





























