Embed Size (px)
Citation preview
I. INTRODUCTION
Pneumonia is an inflammatory illness of the lung. Frequently, it is described
as lung parenchyma/alveolar (microscopic air-filled sacs of the lung responsible for
absorbing oxygen from the atmosphere) inflammation and (abnormal) alveolar
filling. Pneumonia can result from a variety of causes, including infection with
bacteria, viruses, fungi, or parasites, and chemical or physical injury to the lungs. Its
cause may also be officially described as idiopathic, that is unknown, when
infectious causes have been excluded.
Bronchopneumonia (Lobular pneumonia) is one of two types of bacterial
pneumonia as classified by gross anatomic distribution of consolidation
(solidification). In bacterial pneumonia, invasion of the lung parenchyma by bacteria
produces an inflammatory immune response. This response leads to a filling of the
alveolar sacs with exudate. The loss of air space and its replacement with fluid is
called consolidation. In bronchopneumonia, or lobular pneumonia, there are
multiple foci of isolated, acute consolidation, affecting one or more pulmonary
lobes.
Pneumonia is a common illness in all parts of the world. It is a major cause of
death among all age groups. In children, the majority of deaths occur in the
newborn period, with over two million deaths a year worldwide. The World Health
Organization estimates that one in three newborn infant deaths are due to
pneumonia and WHO also estimates that up to 1 million of these (vaccine
preventable) deaths are caused by the bacteria Streptococcus pneumoniae, and
90% of these deaths take place in developing countries. Mortality from pneumonia
generally decreases with age until late adulthood. Elderly individuals, however, are
at particular risk for pneumonia and associated mortality.
New Research Spares Children the Pain of the Needle
ScienceDaily (Jun. 27, 2007)
http://www.sciencedaily.com/releases/2007/06/070626123930.htm

Children suffering from pneumonia could be spared the pain of the doctor's
needle, thanks to new research funded by the British Lung Foundation.
The study, a world-first carried out by researchers at The University of
Nottingham, discovered that children given oral treatment recovered as quickly,
suffered less pain, required less oxygen therapy in hospital and were able to go
home sooner than those given injections.
Two-and-a-half million children are affected by pneumonia each year in Europe.
Until now, most children have been admitted to hospital and treated with injected
antibiotics.
The findings suggest that these injections — endured by generations of children
— may be unnecessary and could be replaced with oral doses of the medicine in the
majority of cases. The study has been published online in the medical journal
Thorax.
The research involved 243 children in hospitals throughout the UK. It was led by
Terence Stephenson, Professor of Child Health, and Dr Maria Atkinson, both of The
University of Nottingham's Medical School.
The study is the first in the developed world to compare oral treatment versus
intravenous (IV) treatment for children with community-acquired pneumonia, who
are unwell enough to need admission to hospital.
Professor Stephenson said: “This is good news for children who hate injections;
good news for parents whose children will spend less time in hospital; good news for
paediatricians who hate sticking needles in children and good news for the NHS, as
fewer beds will be occupied and the treatment is cheaper.”
Dame Helena Shovelton, Chief Executive of the British Lung Foundation, said:
“Treating childhood pneumonia will be less painful and distressing for parents, for
children and for the health professionals caring for them, thanks to this research.
We are very proud to have made this breakthrough possible.”

The research project involved 243 children, enrolled over a 21-month period at
eight UK hospitals. Half were randomly assigned to receive a week of oral antibiotic
treatment and half to receive antibiotics intravenously.
Follow-up over subsequent weeks showed that both types of treatment are
effective in tackling the illness — and the former actually had a number of
advantages over the latter. Oral antibiotics are also cheaper than those given via
the IV route.
The researchers concluded: “We suggest that in countries like the UK, all but the
sickest children with community-acquired pneumonia should be treated with oral
amoxicillin initially.
http://www.sciencedaily.com/releases/2007/06/070626123930.htm
The group chose Pneumonia as their case for presentation because they want
to expand their knowledge gained in classroom lectures. This case is chosen
because it seems for them that it is just simple but when they conducted a study
about it they learned that there are so many factors that could be cause for
Pneumonia. The group would like to gain more information about the disease
condition. Other than the fact that the case is very common and it is the usual case
used by the student nurses for their case presentations the group still took part in
conducting a case study about Pneumonia because they have considered the fact
that Pneumonia according to DOH is one of the leading caused of infant mortality in
the Philippines. Interest leads the group to come up with such study as they make
every effort to expand their knowledge about pneumonia.
1. PERSONAL DATA

Baby Nicole is a 1 year and 2 months old baby girl who was born last
September 09, 2006 in Quezon City General Hospital. Because of her age, the group
decided to interview the mother of the patient. Her parents are Peyton Scott and
Lucas Scott. They are currently living in Dolores, Magalang, Pampanga. They are all
having Filipino nationality and are all followers of Born Again religion.
Baby Nicole was admitted last November 22, 2007, at around 12 noon in
Balitucan District Hospital complaining for on and off fever. And was discharge last
November 24 2007.
2. PERTINENT FAMILY HISTORY
Nathan ScottBD: Nov-10-1955
Chris DavisDD: April-22-1992
Cancer
Peyton ScottBD: Jan.-4-1977Asthma
Lucas ScottBD: April-09-1979
Jake ScottBD: Dec.-04-2000Cerebral Palsy
Nicole ScottBD; Sept.-09-2006BPN
Brooke DavisDD: Dec.26-2003birth complication
Haley ScottBD: july-5-1954Asthma

Birth Date: BD
Death Date: DD
Male:
Female:
Diseased:
With existing illness:
The diagram shows that Lucas Scott and Peyton Scott are the parents
of Baby Nicole. At the paternal side, Lucas’s parents or the grandparents of
Baby Nicole are both still alive. Haley Scott the grandmother of Baby Nicole is
diagnosed with asthma. At the maternal side, Peyton’s parents or Baby
Nicole’s grandparents on mother side are both already dead. Chris Davis the
grandfather of Baby Nicole died because of cancer, while Brooke Davis died
because of birth complications. The mother of Baby Nicole which is Peyton
Scott is diagnosed with asthma. Baby Nicole has one brother which is Jake
Scott. He is diagnosed with cerebral palsy.
Scott family is composed of 4 members. Peyton Scott gave birth to 2
children. Her first child is Jake Scott he was born last December 04 2000, at
East Avenue Medical Center via normal spontaneous delivery. After about 6
years she gave birth to her 2nd child which is Baby Nicole at Quezon City
General Hospital via normal spontaneous delivery also. She said that during
her pregnancy she’s a little bit irritable with her husband. But she has
positive attitudes with her pregnancies.
The Scott family is currently residing at Brgy. Dolores, Magalang,
Pampanga. They live in a wooden house owned by their boss. Mr. Lucas the
father of Baby Nicole works as a hollow block maker. He earns 1800/week
and works from 6am-6pm. He is a smoker; he usually smokes 5 sticks/day. He
also drinks alcoholic beverages; he usually drinks 2 bottles/week. Peyton
Scott is a house wife, she stays at home to take care of their children. She
stated that the house is in good condition but the surrounding is very dusty
because it’s near the hollow block making site.

Mrs. Scott believes to herbolarios, she usually consults herbolarios to
have hilot and tawas. She also uses herbal medicines when they caught
simple illnesses like cough or cold. The usual herbal medicines that they use
are oregano, ampalaya leaves, guava, and sambong. Mrs. Scott said that
whenever she has an emergency financial problem they usually come to their
boss to borrow some money.
3. PERSONAL HISTORY
Mrs. Scott told the group that she’s having a monthly check up during
her pregnancy. She delivered her 1st baby for 6 hours. And she delivered her
2nd baby which is baby Nicole for 2 hours. They are both delivered in the
hospital and they are all 9 months when they were delivered. Mrs. Scott said
that she only breastfed her children for 2 weeks after that she begins to
bottle feed them. She also stated that her children were all fully immunized.
Growth and Development
Erik Erickson’s Psychosocial Development
Trust Vs. Mistrust (birth to 1 year)
Characterized by taking in through all the senses, loving care of
a mothering person is essential to develop trust, must have basic needs met,
and having an attachment to primary care taker
Baby Nicole manifested this by crying when she woke up and
her mom is not around. She gained trust because her mother responded to
her eagerly whenever she’s crying and give her food whenever she’s hungry.
Sigmund Freud’s Psychosexual Development
Oral Stage (birth to 1 year)

Characterized by infant-seeking pleasure via oral activities such
as biting, sucking, chewing, and vocalizing.
Baby Nicole manifested this by putting everything that she
reaches in her mouth like IV tube, and she’s stop crying whenever she sucks
her pacifier.
Jean Piaget’s Cognitive Development
Sensorimotor (birth to 2 years)
Characterized y progression from reflex activity through simple
repetitive behaviors to imitative behaviors, information is gained through the
senses and developing motor abilities, develop a sense of cause and effect,
problem-solving is by trial and error, high level of curiosity, experimentation,
and enjoinment in novelty, begin to separate self from others, develop sense
of object permanence, begin language development.
Baby Nicole manifested this because when the group is
assessing her. She wants to get the penlight from one of the member, and
when the group member hides it, Nicole is still looking for it.
4. HISTORY OF PAST ILLNESSES
Mrs. Scott stated that baby Nicole had mumps last September and got
tigdas hangin when she’s just about 7 months. She also had sore eyes last
October. Other than that she also had some cough and colds.
5. HISTORY OF PRESENT ILLNESSES
Baby Nicole was hospitalized twice already. She was first hospitalized
last November 10 2006 at Quezon City General Hospital with complain of
difficulty of breathing, cough and colds. During that hospitalization she was

diagnosed to have Pneumonia. She stayed in the hospital for 1 week. Her 2nd
hospitalization was in Balitukan District hospital last November 22 2007. She
was admitted with complains of on and off fever for 7 days and cough for 3
days.
6. PHYSICAL EXAMINATION
Initial Assessment upon Admission (November 22 2007)
Vital signs:
T= 38 °C
P= 143 bpm
R= 49 cpm
Complain of 7 days on and off fever accompanied by cough and colds.
Fairly nourished
Fairly developed
Weight: 14 kg
(+) Rales on both lung fields
(-) Wheezes
November 23 2007
General Condition
The patient is seen lying on bed with her mother, awake and conscious
She’s wearing comfortable and loose sando and short. The patient is slightly
irritable and looks untidy because of uncombed hair and slightly wet back.
Vital Signs:
T= 37.5°C
P= 148 bpm
R= 61 cpm
Skin and Hair

With dark brown complexion all throughout the body. Hair evenly
distributed.
Head
Hair is evenly distributed, smooth and shiny. No dandruff. Symmetrical
contours of the head. No abnormal depressions, masses, and nodules upon
palpation.
Eyes
Symmetrical eyebrow movement and evenly distributed hair.
Symmetrical eyelid movement and evenly distributed eye lashes.
Symmetrical eye movement.
No abnormal discharges. With pinkish palebral conjunctiva. With round and
black iris. With white sclera. No abnormal masses and nodules. Pupils dilate
upon introduction of light. With (+) blink reflex.
Ears
Symmetrical ear shape, non-tender, and firm. Ears line the outer
cantus of the eye. Presence of serumen in minimal amount. Intact tympanic
membrane. No abnormal masses and nodules upon palpation. Pinna recoils
after it is folded. Good sense of hearing evident by head turning upon
mentioning her name.
Nose
Presence of little amount of nasal secretion because of colds. No
abnormal masses, nodules and lesions. With good sense of smell evident by
removing the cotton ball with alcohol introduce by the student nurse.
Mouth
Symmetrical pale, lips. Presence of 8 teeth. Tongue located at the
middle. Able to move tongue. With (+) gag reflex. With good sucking reflex.
No abnormal lesion and sores.
Neck

Located on the midline. No abnormal masses, nodules and lesions.
Trachea is located at the center
Chest
Symmetrical lung expansion. With evenly distributed hair. No masses
and lesions. With abnormal breath sound (rales) on both lung fields. With
shallow, short breaths.
Heart
No unusual heart sound upon auscultation.
Abdomen
Uniform in color. Round shape of abdomen. No lesions and masses. No
tenderness upon palpation. Presence of normal bowel sound. (gurgle)
(16/min)
Upper Extremities
Able to move hands freely. Symmetrical in shape. With dirty
fingernails. No abnormal lesions and masses. Pale nailbeds.
Lower Extremities
Able to move feet freely. Symmetrical in shape. With dirty toe nails. No
masses and lesions.

7. DIAGNOSTIC AND LABORATORY PROCEDURES
Diagnosti
c/
Laborator
y
procedur
es
Date ordered,
Date
performed,
Date results in
Indication(s)
or Purpose(s)
Results Normal
Values (units
used in the
hospital)
Analysis and
Interpretation of
results

Chest X-
ray
DO: 1i1-22-07
DP: 11-23-07
DRI: 11-23-07
To visualize
possible
enlargement of
the heart and
assess
presence of
congestion in
the lungs.
Chest
roentgenograms
reveal minimal hazy
infiltrates on both
lower lung fields.
Heart and great
vessels are of
normal size and
configuration.
Hemidiaphragms
sulci and other
visualized included
chest structures are
unremarkable.
The results were
interpreted by the
physician, the results
revealed pneumonitis
on both lung fields.
Nursing Responsibilities:
Preprocedural care:
Orient the client about the procedure.
Inform the client that the procedure is pain free.

If the client is pregnant, inform her that radiation can be harmful to the fetus. If an x-ray is necessary,
precautions will be taken to minimize radiation exposure to the baby.
Ask the client to remove some or all of their clothes and ask them to wear a gown.
Ask them to remove jewelry, eye glasses and any metal objects or clothing that might interfere with the x-ray
images.
During the procedure:
Assist the client and will position the patient with hands on hips and chest pressed the image plate. For the
second view, the patient's side is against the image plate with arms elevated.
The patient who can’t stand may be positioned lying down on a table for chest x-rays.
Ask the patient to hold very still and may be asked to keep from breathing for a few seconds while the x-ray
picture is taken to reduce the possibility of a blurred image.
Postprocedural care:
Ask the client to wait until the technologist determines that the images are of high enough
quality for the radiologist to read.
Diagnostic/
Laboratory
procedures
Date ordered,
Date
performed,
Date results in
Indication(s) or
Purpose(s)
Results Normal
Values (units
used in the
hospital)
Analysis and
Interpretation of
results

Hematology
Hemoglobin
DO: 1i1-22-07
DP: 11-22-07
DRI: 11-23-07
To monitor levels of
blood components
that could be
indicative of infection
or other disease or
health conditions
It measures the total
amount of
hemoglobin in the
blood to determine
the oxygen carrying
capacity of the blood.
Hemoglobin in
vertebrates
transports oxygen
from the lungs to the
rest of the body, such
as to the muscles,
where it releases the
oxygen load. Due to
11.2 mg % 12-16 mg %
The results are slightly
below normal, which
may indicate that the
patient is at risk of
having ineffective
tissue perfusion and
lack of adequate
oxygen.

Hematocrit
vaginal bleeding of
the patient, there is
loss of blood and
should be monitored
if she needs blood
transfusion to
maintain the normal
circulation of oxygen
in blood to
supplement the body
and organs.
It measures the
percentage of RBCs in
the total blood
volume. It may also
provide idea on
patient’s fluid status.
The hematocrit is the
percent of whole
blood that is
composed of red
37 vol.% 37-47 vol.%
The results are with in
normal range that may
indicate normal RBCs in
the blood.

WBC
Lymphocytes
blood cells. The
hematocrit is a
measure of both the
number of red blood
cells and the size of
red blood cells
The total white blood
cell count is the
absolute number of
leukocytes circulating
in a cubic millimeter
of blood. It is used to
determine factor of
inflammation and also
to determine and
evaluate body’s
physiologic capacity
to resists and
overcome infection.
A variety of WBC
7,700/cu.mm
64%
10-25x10
25-40
The results are below
normal that can
indicate that the WBCs
are already worn out by
the microorganism.
The results were
elevated which may

Platelet Count
(leucocyte), present
also in the lymph
nodes, spleen,
thymus gland, gut
wall and bone
marrow. They are
involve in immunity
and can be
subdivided into B-
cells which produce
circulating antibodes
and T-cell which are
primarily responsible
for cell-mediated
immunity
A disc –shaped cell
structure, 1-2 um in
diameter, which is
present in the blood.
Assess for any risk of
bleeding and for
252/cu. Mm. 150-450/cu mm
indicate that the body
is trying to fight the
infection by producing
lymphocytes that
produces
T-cells and B-cells
which produces
antibodies and
responsible for cell
mediated immunity.
The results are within
normal range that may
indicate normal clotting
time and is safe from
bleeding.

clotting time.
Nursing Responsibilities:
Before:
Check the doctor’s order.
Determine the prescribed test and other restrictions prior to the test.
Get the laboratory requisition slip.
Explain to the patient what the procedure to be done is.
Inform the patient that this requires a blood sample.
Inform the patient how the procedure is performed, the equipment to be used.
During:
Explain to the patient what test should be done.
Prepare all the equipments to be used.
Tell the patient when to insert the needle for her to be prepared.
Encourage the patient to remain calm during the test.
Assist the patient if necessary.

Ensure a sterile blood sample from the patient.
After:
Send the blood sample to the laboratory immediately.
Proper documentation

III. ANATOMY AND PHYSIOLOGY
Respiration is necessary because all living cells of the body require
oxygen and produce carbon dioxide. The respiration system assists in gas
exchange and performs other formation as well our body needs a constant
supply of oxygen to support metabolism. The respiratory system brings
oxygen through the airways of lungs into the alveoli, where it diffuses into
the blood for transport to the tissue, this process is so vital that difficult in
breathing is expected as a threat to life in self. The respiratory system allows
oxygen from the air to enter the blood and carbon dioxide to leave the blood
and enter the air. The cardiovascular system transport oxygen from the lungs
to the cells of the body and carbon dioxide. Without healthy respiratory and
cardiovascular system, the capacity to carry out normal activity is reduced,
and without adequate respiratory and cardiovascular system friction, life
itself is possible.
Nose- The term nose refers to the visible structure that forms a prominent
feature of the face. Most of the nose is composed of cartilage, although the
bridge of the nose consists of bone the bone and cartilage and covered by
connective tissue and shin.
Nasal cavity- The nasal extends from the noses to the choane the nares or
nostrils are the external opening of the nose and the choane are the
openings to the pharynx. The nose is formed from both bone and cartilage.
The nasal bone forms the bridge and the remainder of the nose is composed
of cartilage and connective tissue. Each opening of the nose to the face leads
to the cavity. The vestibule is lined anteriorly to the skin and hair that filter
foreign objects and prevent from being inhaled. The posterior vestibule is
lined with a mucous membrane, composed of columnar epithelial cells and,
goblets cells that secrete mucous. The mucous membrane extends
throughout the airways and cilia propel mucous to the pharynx for
elimination by swallowing or coughing. The portion of mucous membrane that
is located at the top of the nasal cavity, just beneath the cribriform plate of
the ethmoid bone, is specialized epithelium; witch provides the sense of
smell.

Along the side of the vestibule are turbinate, mucous membrane covered
projections that contain a rich blood supply from the internal and external
carotid arteries. They warm and humidify inspired air.
Paranasal sinuses- open areas within the skull are named for the bones in
witch they lie: frontal, ethmoid, sphenoid and maxillary. Passageway from
paranasal sinuses drain into the nasal cavity. The nasolacrimal duct, witch
drain tears from the surface of the eyes, also drains the nasal cavity.
Pharynx- it is a funnel-shaped tube that extends from the nose to the larynx.
It is the common passageway of both the respiratory and digestive system. It
can be divided into three regions:
a. Nasopharynx- is located above the margin of the soft palate and
receives air from the nasal cavity. From the ear, the Eustachian
tubes open into the nasopharynx. The pharyngeal tonsils are
located on the posterior wall of the nasopharynx.
b. Oropharynx- serves both respiration and digestion. It receives
air from the nasopharynx and food from the oral cavity. Palatine
tonsils are located along the sides of the posterior mouth, and
the lingual tonsils are located at the base of the tongue.

c. Laryngopharynx- located below the base of the tongue, is the
most inferior portion of the pharynx. It connects to the larynx
and serves both the respiration and digestion.
Larynx- is commonly called the voice box. It connects the upper and
lower airway. It lies just anterior to the upper esophagus. Nine cartilages
form the larynx: epiglottis, thyroid, cricoid, arythenoid, corniculate,
cuneiform. The cartilage are attach to the hyoid bone above and below
the trachea by muscles and ligaments. The slit the vocal cords forms the
glottis. The epiglottis, a leaf shaped structure immediately posterior to the
base of the tongue. The thyroid cartilage protrudes in front of the larynx
forming the Adam’s apple.
Trachea- extends from the larynx to the level of the seventh thoracic
vertebrae, where it divides into two main bronchi. The point at witch the
trachea divides is called carina. The trachea is a flexible, muscular, 12cm
long air passage with C-shaped cartilaginous ring.
Lungs- it lie within the thoracic cavity on either side of the heart. They
are cone-shaped, with the apex above the first rib and the base resting on
the diaphragm. Each lung is divided into superior and inferior lobes by an
oblique fissure. The right lung is further divide by a horizontal fissure,
witch bounds a middle lobe. The right lung therefore has three lobes. The
lung contains gas, blood, and thin alveolar wall and support structure. The
alveolar walls contain elastic and collagen fibers. These fibers are capable
of stretching when the pulling force is exerted on then from outside of the
body or whey they are inflated from within.
Alveoli- the lungs parenchyma, consists of millions of alveolar units, is
the working area of the lung tissue it birth a person has approximately 24
million alveoli, by the age 8 yrs a person 300 million. The total working
alveolar surface are is the approximately 750 to 860 square feet. Oxygen
and CO2 are exchange through the respiratory membrane about 0.2 mm
thick (The average diameter of the pulmonary capillary only about 5
mins).
Thorax- provides protection for the lungs, heart and great vessels. The
outer shell of the thorax is made up of 12 pairs of ribs. The ribs connects
posterior to the transverse processes of the thoracic vertebrae of the

spine. Anteriorly, the first seven pairs of ribs are attached to the sternum
by cartilage. The 8th, 9th and 10th ribs are attached to each other by costal
cartilage. The 11th and12th ribs allow full chest expansion because they
are not attached in any way to the sternum.
Diaphragm- it is the primary muscle of breathing and serves as the lower
boundary of the thorax. The diaphragm is dome- shaped in the relaxed
position, with central muscular attachments to the xiphoid process of the
sternum and the lower rib.
IV. PATIENT AND HIS ILLNESS
A. PATHOPHYSIOLOGY

a. Schematic Diagram
(book base)
yema
(Patient Centered)
Viral infection
Inflammation of pulmonary parenchyma
Fungal infection
Engorgement with effusion of blood and serum into the alveoli
in 1 or more lobes;(stage I) lobe airless and alveoli contain fibrin, serum, RBC,
neutrophils,(stage II) lobe larger with fibrin in alveoli
and decreased cellular elements and bacteria
(stage III) Usually pneumococcal
Bronchopneumonia Interstitial pneumonia
Bacterial infection
Lobar pneumonia
Mucopurulent exudate in terminal
bronchioles. Clogging of bronchioles. Necrosis and
sloughing of bronchial mucous membranes.
Formation of peribronchial
abscesses and pneumatoceles.
Usually staphylococcal
Resolution with treatment (stage IV)
Inflammation of walls of alveoli, bronchi and bronchioles. Usually
viral and staphylococcal
Risk Factors
-second-hand
smoker
-age
-environment
-nutrition
-pleural effusion-pleurisy
-empyema
-pleural effusion-empyemaResolution
with treatment
-pneumothorax-empyema
Resolution with
treatment

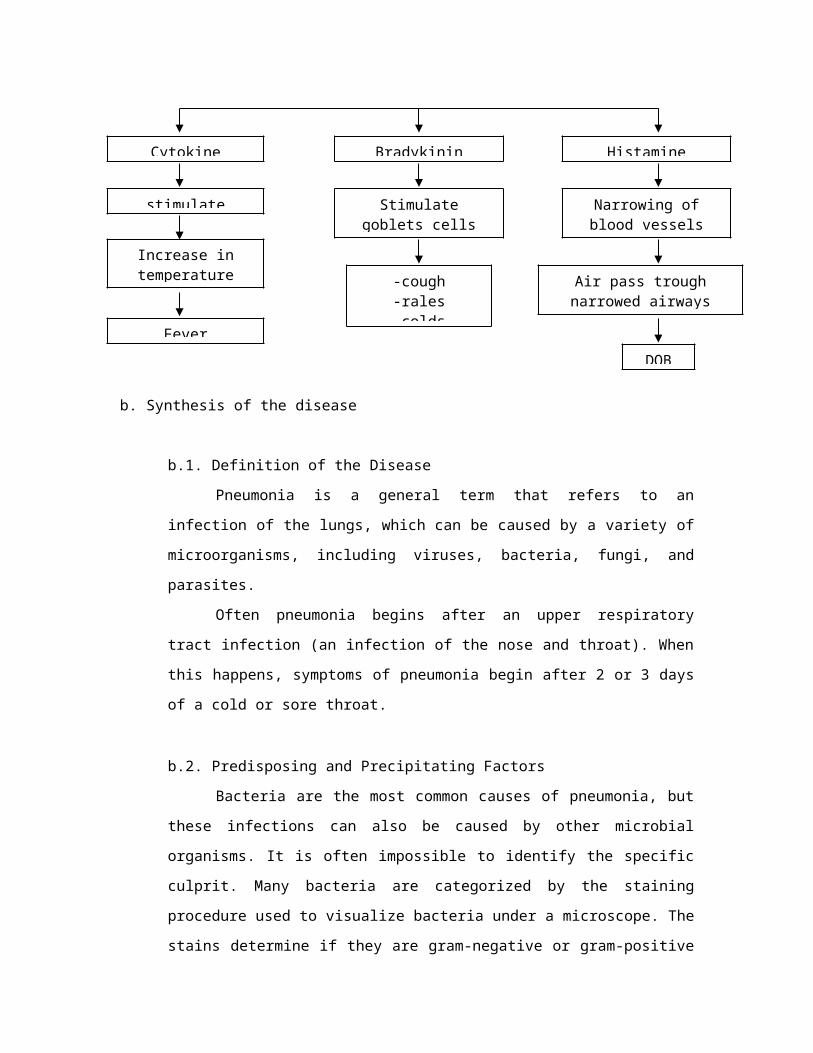
b. Synthesis of the disease
b.1. Definition of the Disease
Pneumonia is a general term that refers to an infection of the
lungs, which can be caused by a variety of microorganisms, including
viruses, bacteria, fungi, and parasites.
Invasion of microorganism
Enter lower respiratory tract
Stimulate respiratory response
-cough-rales-colds
Accumulation of exudates and
bacteria
Cytokine
Release of chemical mediators
Parenchymal and Alveolar sacs tend to consolidate
stimulate
Fever
Stimulate goblets cells
Increase in temperature
Bradykinin
Narrowing of blood vessels
Histamine
Air pass trough narrowed airways
DOB
Often pneumonia begins after an upper respiratory tract
infection (an infection of the nose and throat). When this happens,
symptoms of pneumonia begin after 2 or 3 days of a cold or sore
throat.
b.2. Predisposing and Precipitating Factors
Bacteria are the most common causes of pneumonia, but these
infections can also be caused by other microbial organisms. It is often
impossible to identify the specific culprit. Many bacteria are
categorized by the staining procedure used to visualize bacteria under
a microscope. The stains determine if they are gram-negative or gram-
positive bacteria. This gives the physician an idea of the severity of the
pneumonia and how to treat it.
Gram-Positive Bacteria. These bacteria appear blue on the stain. The
following are common gram-positive bacteria:
The most common cause of pneumonia is the gram-positive bacterium
Streptococcus pneumoniae (also called S. pneumoniae or
pneumococcal pneumonia ). It was thought to cause 95% of
community-acquired bacterial infection, but research now indicates it
is far less, accounting for about half of all cases. (Some studies suggest
it may account for even fewer, 10% to 30% of cases.)
Staphylococcus aureus , the other major gram-positive bacterium
responsible for pneumonia, accounts for about 10% of bacterial cases.
It is one of the main causes of pneumonia that occurs in the hospital
(nosocomial pneumonia). It is uncommon in healthy adults but can
develop about five days after viral influenza, usually in susceptible
individuals, such as people with weakened immune systems, very
young children, hospitalized patients, and drug abusers who use
needles.
Streptococcus pyogenes or Group A Streptococcus.

Gram-Negative Bacteria. These bacteria stain pink . Gram negative bacteria
are common infectious agents in hospitalized or nursing home patients,
children with cystic fibrosis, and people with chronic lung conditions.
The most common gram-negative species causing pneumonia is
Haemophilus influenzae (generally occurring in patients with chronic
lung disease, older patients, and alcoholics).
Klebsiella pneumoniae may be responsible for pneumonia in alcoholics
and in other people who are physically debilitated.
Pseudomonas aeruginosa is a major cause of pneumonia that occurs in
the hospital (nosocomial pneumonia). It is common in pneumonia
patients with chronic or severe lung disease.
Moraxella catarrhalis is found in everyone's nasal and oral passages.
Experts have identified this bacteria as a cause of certain pneumonias,
particularly in people with lung problems, such as asthma or
emphysema.
Neisseria meningitidis is one of the most common causes of meningitis
(central nervous system infection), but the organism has been
reported in pneumonia, particularly in epidemics of military recruits.
Other gram-negative bacteria that cause pneumonia include E. coli (a
cause in newborns), Proteus (found in several damaged lung tissue),
and Enterobacter.
Bacterial pneumonias tend to be the most serious and, in adults, the
most common cause of pneumonia. The most common pneumonia-causing
bacterium in adults is Streptococcus pneumoniae (pneumococcus).
Respiratory viruses are the most common causes of pneumonia in young
children, peaking between the ages of 2 and 3. By school age, the bacterium
Mycoplasma pneumoniae becomes more common.
In some people, particularly the elderly and those who are debilitated,
bacterial pneumonia may follow influenza or even a common cold.
Many people contract pneumonia while staying in a hospital for other
conditions. This tends to be more serious because the patient's immune
system is often impaired due to the condition that initially required

treatment. In addition, there is a greater possibility of infection with bacteria
that are resistant to antibiotics.
b.3. Signs and Symptoms
Symptoms of pneumonia vary, depending on the age of the child and the
cause of the pneumonia. Some common symptoms include:
Fever- A fever occurs when the thermostat resets at a higher
temperature, primarily in response to an infection.
Chills- The "chills" that often accompany a fever are caused by the
movement of blood to the body's core, leaving the surface and
extremities cold.
Cough- this is the body’s way to expel foreign objects in our body
Unusually rapid breathing- the small blood vessels in the lungs
(capillaries) become leaky, and protein-rich fluid seeps into the alveoli.
This results in less functional area for oxygen-carbon dioxide
exchange. The patient becomes relatively oxygen deprived, while
retaining potentially damaging carbon dioxide. The patient breathes
faster and faster, in an effort to bring in more oxygen and blow off
more carbon dioxide.
Breathing with grunting or wheezing sounds-this is because of the
secretions that are present in the lungs.
Labored breathing that makes a child's rib muscles retract (when
muscles under the rib cage or between ribs draw inward with each
breath)
Vomiting –because the respiratory center and the vomiting center are
the same which is the medulla oblongata, when there is an
abnormality in breathing this may also trigger the patient to vomit.
Chest pain
Abdominal pain
Decreased activity
Loss of appetite (in older children) or poor feeding (in infants)
In extreme cases, bluish or gray color of the lips and fingernails
Health Promotion and Preventive Aspects of the Disease

There are vaccines to prevent infections by viruses or bacteria that
cause some types of pneumonia.
Children usually receive routine immunizations against Haemophilus
influenzae and pertussis (whooping cough) beginning at 2 months of
age. (The pertussis immunization is the "P" part of the routine DTaP
injection.) Vaccines are now also given against the pneumococcus organism
(PCV), a common cause of bacterial pneumonia.
Children with chronic illnesses, who are at special risk for other types
of pneumonia, may receive additional vaccines or protective immune
medication. The flu vaccine is strongly recommended for children with
chronic illnesses such as chronic heart or lung disorders or asthma, as well as
otherwise healthy children.
Because they are at higher risk for serious complications, infants who
were born prematurely may be given treatments that temporarily protect
against RSV, which can lead to pneumonia in younger children.
Doctors may give prophylactic (disease-preventing) antibiotics to
prevent pneumonia in children who have been exposed to someone with
certain types of pneumonia, such as pertussis. Children with HIV infection
may also receive prophylactic antibiotics to prevent pneumonia caused by
Pneumocystis carinii.
Antiviral medication is now available, too, and can be used to prevent some
types of viral pneumonia or to make symptoms less severe In addition;
regular tuberculosis screening is performed yearly in some high-risk areas
because early detection will prevent active tuberculosis infection including
pneumonia.
In general, pneumonia is not contagious, but the upper respiratory viruses
that lead to it are, so it is best to keep your child away from anyone
who has an upper respiratory tract infection. If someone in your home has a
respiratory infection or throat infection, keep his or her drinking glass and
eating utensils separate from those of other family members, and wash your
hands frequently, especially if you are handling used tissues or dirty
handkerchiefs.

V. THE PATIENT AND HIS CARE
A. MEDICAL MANAGEMENT
a. IVF’s, BT, NGT fee ding, Nebulization, TPN, Oxygen Therapy, etc.
Medical management/
treatment
Date ordered,Date performed,
Date changed
General Description
Indication(s) or Purpose(s)
Client response to the treatment
D5IMB 500cc DO: 11-22-07
DP: 11-22-07
DC: ------------
Sterile, nonpyrogenic
solution for fluid and
electrolyte
replenishment and
caloric supply in
single dose
containers for IV
administration
Indicated as a source
of water, electrolytes
and calories, or as an
alkalinizing agent.
The patient showed
no signs of fluid
overload,
dehydration and
phlebitis along the
intravenous site.
Nursing Responsibilities:

Before:
Identify the purpose of IV therapy and to the client’s significant others.
Before starting the IV therapy, consider duration of therapy, type of infusion, condition of veins and medical
conditions of patient to assist in choosing the IV site.
Make sure that the equipments are sterile.
During:
Secure the IV site with a board to prevent it from dislocation.
After:
Regulate the IV fluid as ordered by the physician.
After the IV therapy, identify local complications at or near the IV needle site.
Check for signs of infiltration, phlebitis and signs of fluid overload or dehydration.
Routinely check for the IV level to change it immediately to prevent air from entering the veins.
b. Drugs

Name of Drugs: Generic Name
Brand Name
Date orderedDate
performedDate
changed/D/C
Route or admin
dosage and frequency of admin
Gen. action Function
ClassificationMechanism of ax
Indications or purposes
Client response to the
medication w/ actual side
effects
Generic Name:
Cefuroxime
Sodium
Brand name:
Cefuroxime
DO: 11-22-07
DP: 11-22-07
DC:-----------
450 mg IV
every 8 hours
Anti-inffectives,
second generation
cephalosporin, bind
to bacterial cell wall
membrane, causing
cell death.
Treatment of
respiratory tract
infections.
There’s a
decrease of
microorganisms
causing the
infection evident
by not having
fever.
Nursing Responsibilities:

Before:
Obtain skin test before the start of the treatment.
Determine previous hypersensitivity to the medication.
Explain the reason for prescribing the medication, the effects and side effects of the drug to the client’s s.o.
During:
Administer slowly over 3-5 minutes.
Monitor site frequently for thrombophlebitis (pain, redness and swelling).
Check the IV patency before administering the medication.
After:
Instruct S.O. to report signs of superinfection (furry overgrowth on tongue, loose or foul- smelling stools) and
allergy.
Instruct client’s S.O. to notify any health carte professional if fever and diarrhea develop, especially if stool
contains pus, blood or mucus
Name of Drugs: Generic Name
Date orderedDate
performedDate
Route or admin
dosage and frequency
Gen. action Function
ClassificationMechanism of ax
Indications or purposes
Client response to the
medication w/ actual side

Brand Name changed/D/C of admin effects
Generic Name:
Acetaminophe
n
Brand name:
Paracetamol
DO: 11-22-07
DP: 11-22-07
DC:-----------
140 mg IV
every 4 hours
PRN
Antipyretic, nonopioid
analgesics. Inhibits
the synthesis of
prostaglandins that
may serve as
mediators of pain and
fever, primarily in the
CNS.
Treatment for
fever.
The patient’s
temperature was
maintained within
normal range.
Nursing Responsibilities:
Before:
Obtain culture and sensitivity test before the treatment starts.
Obtain history of hypersensitivity to analgesics.
Get the patients temperature before administering the medication

During:
Check the patency of the IV.
Administer slowly.
After:
Obtain patients temperature.
Instruct S.O. to report signs of superinfection (furry overgrowth on tongue, loose or foul- smelling stools) and
allergy.
Instruct client’s S.O. to notify any health carte professional if fever and diarrhea develop, especially if stool
contains pus, blood or mucus
Name of Drugs: Generic Name
Brand Name
Date orderedDate
performedDate
changed/D/C
Route or admin
dosage and frequency of admin
Gen. action Function
ClassificationMechanism of ax
Indications or purposes
Client response to the
medication w/ actual side
effects
Generic Name:
Albuterol
DO: 11-22-07
DP: 11-22-07
1 neb. TID Bronchodilators;
binds to beta 2-
Used as
bronchodilator to
The patient
maintained

Brand name:
Salbutamol
DC:11-23-07
DO: 11-23-07
DP: 11-23-07
DC:-------------
1 neb every 4
hours.
adrenergic re ceptors
in airway smooth
muscle, leading to
activation of adenyl
cyclase and
increased levels of
cyclic-3’, 5’-
adenosine
monophosphate
(cAMP). Increases in
cAMP activate
kinases, which inhibit
the phosphorylation
of myosin and
decrease intracellular
calcium that leads to
relaxation of smooth
muscle airways.
control and
prevent reversible
airway obstruction
caused by
respiratory
conditions.
patent airway.
Nursing Responsibilities:
Before:
Assess lung sounds before administration and during peak of medication. Note characteristics of sputum.

Make sure that the equipments are clean before using them.
During:
Shake inhaler well.
Maintain a fowler’s position.
Keep the inhaler close to the patient to make sure she inhales the medication.
After:
Provide mouth care because nebulization can cause bad taste.
Advise patient to rinse with water, to minimize drying of mouth.
c. Diet
Type of Diet Date orderedDate startedDate changed
General Description
Indication(s) or Purpose(s)
Specific foods taken
Client’s Response
and/or reaction to diet

Diet For Age DO: 11-22-07
DP: 11-22-07
DC: ------------
Diet for age
means that the
patient can eat
anything that
he/she can
tolerate at
his/her age.
It will help
prevent
aspiration.
The patient eats
crackers, and
drink water.
The patient’s so
didn’t give the
patient food that
he/she can’t
tolerate.
Nursing Responsibilities:
Before:
Explain the purpose of the diet order, the consequences of not following such diet and how it will be implemented.
Emphasize the food that the patient can take.
During
Make sure that the client is taking the specified diet.
After:
Emphasize the new preferred diet.
d. Activity/Exercise
Type of exercise
Date ordered, Date started, Date changed
General Description Indications or
PurposesClient’s response to the
treatment

Activity as
tolerated.
DO: 11-22-07
DP: 11-22-07
DC: ------------
The patient is allowed
to do activities as
long as he/she can
tolerate them.
To provide sense of well
being. And to have some
exercise in other ways,
The patient walks with her mom
in the hospital.
Nursing Responsibilities:
Educate patient’s SO about what activities is the patient allowed to do.
Make sure that the patient is doing the desired exercise or activity.
Have the patient rest after doing an activity.
Emphasize the importance of following the activity.

B. SURGICAL MANAGEMENT
The group found no surgical treatment for pneumonia. While
searching the group have open sites that indicate that there are no surgical
treatments available for pneumonia since that this disease is curable.

C. NURSING MANAGEMENT1. Nursing Care plan
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives Nursing Interventions
Rationale Expected Outcome
S =
O= pt manifested:>DOB
>(+) rales
>with nasal flaring
>with non productive cough
>skin warm to touch
>with shallow respiration
=pt may manifest:>changes in respiratory rate and rhythm
Ineffective airway clearance r/t retained pulmonary secretions AEB non-productive cough secondary to BPN
Pneumonia is an inflammation of the lung parenchyma caused by various microorganisms. An inflammatory reaction that occurs in the alveoli produces exudates. And as part of inflammatory reaction WBC migrate to the alveoli and fill the normally air containing spaces. The exudates together with the migration of WBC produces thick secretions that blocks the airways does leading to ineffective airway clearance.
Short term:After 4 hours of NI, pt will be able to improvement of airways patency AEB reduction of cough and noiseless breathing
Long term:After 3 days of NI, the patient will be able to maintain patent airway AEB absence of pt’s abnormal respiratory manifestations that has been observed and assessed
Establish rapport
Assess gen. condition of the pt.
monitor and record VS
auscultate breath sounds and assess air movement
elevate pt.’s HOB
reposition pt. periodically
Instruct pt.’s SO to increase fluid intake of pt.
perform CPT
administer medications as order
To gain trust and cooperation of the pt.
to provide appropriate assessment and management
to obtain base line data
to ascertain status and to note progress
to maximize oxygen consumption
prevents accumulation and pooling of secretions
to liquefy secretion for easy expectoration
to loosen the secretions
to provide appropriate treatment and to help facilitate airway patency
Short term:After 4 hours of NI, pt shall have demonstrate improvement of airway patency AEB reduction of cough and noiseless breathing.
Long term:After 3 days of NI, the patient should be able to maintain patent airway AEB absence of pt’s abnormal respiratory manifestations that has been observed and assessed
Problem # 1: Ineffective Airway Clearance

Problem #2: Ineffective Breathing Pattern
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives Nursing Interventions
Rationale Expected Outcome
S =
O= pt manifested:> (+) rales
>non-productive cough
> abnormal respiratory depth and rate
>shallow breaths
=pt may manifest:>increased a/p diameter
>altered chest excursion
Ineffective breathing pattern r/t retained pulmonary secretions AEB abnormal respiratory rate and depth.
An inflammatory reaction can occur in the alveoli, producing an exudates. White blood cells, mostly neutrophils, also migrate into the alveoli and fill the normally air-containing spaces. Bronchospasm may also occur in patients with reactive airway disease. The secretions and bronchospasm makes the patient to have ineffective breathing pattern.
Short term:After 4 hours of NI, pt will be able to have an improvement of breathing pattern AEB normalization of respiratory rate and depth.
Long term:After 3 days of NI, the patient will be free from respiratory distress and other s/sx of hypoxia.
Establish rapport
Assess gen. condition of the pt.
monitor and record VS
elevate pt.’s HOB
provide adequate rest and sleep
suction secretions when necessary
administer medications as order
To gain trust and cooperation of the pt.
to provide appropriate assessment and management
to obtain base line data
to promote maximum lung expansion and oxygen consumption
to reduce potential dyspnea and fatigue.
to facilitate and promote effective breathing pattern
to promote well ness through pharmacologic means.
Short term:After 4 hours of NI, shall have demonstrate improvement of breathing pattern AEB normalization or respiratory rate and depth.
Long term:After 3 days of NI, the patient should be able to maintain patent airway AEB absence of pt’s abnormal respiratory manifestations that has been observed and assessed
Problem #3: Impaired Gas Exchange

Assessment
Nursing Diagnosis
Scientific Explanation
Objectives Nursing Interventions
Rationale Expected Outcome
S=
O= pt manifested:> irritability
> nasal flaring
>DOB
>pale lips and nail beds
> increase respiratory distress
>non-productive cough
>(+) rales
=pt may manifest: >cyanosis
impaired gas exchange r/t altered oxygen supply DOB
Due to retained mucus secretions in the bronchi, there will be an alteration in the normal perfusion of gases in the alveoli, resulting in oxygen deficit and carbon dioxide that will therefore develop to an impairment in gas exchange.
Short term:After 4 hours of NI, pt will have an improvement of gas exchange AEB pinkish lips and nailbeds.
Long term:After 3 days of NI, pt will be able to demonstrate improvement in ventilation and presence of adequate oxygenation AEB absence of DOB.
Establish rapport
Assess gen. condition of the pt.
monitor and record VS
elevate pt.’s HOB
reposition pt. periodically
Instruct pt.’s SO to increase fluid intake of pt.
Provide adequate rest and sleep
administer oxygen inhalation as order
administer due medications
To gain trust and cooperation of the pt.
to provide appropriate
assessment and management
to obtain base line data
to maximize oxygen consumption
prevents accumulation and pooling of secretions
to liquefy secretion for easy expectoration
to lessen oxygen demand of the pt.
to provide oxygen supply
to promote wellness through pharmacologic means.
Short term:After 4 hours of NI, pt shall have demonstrate improvement in gas exchange AEB pinks lips and nailbeds.
Long term:After 3 days of NI, pt should be able to demonstrate improvement in ventilation and presence of adequate oxygenation AEB absence of DOB.
Problem #4: Hyperthermia
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives Nursing Interventions
Rationale Expected Outcome

S=
O= pt manifested:>elevated temp. 38
>skin warm to touch
>irritable
> (+)rales
>Restless
Hyperthermia The set point of the hypothalamic thermostat changes suddenly from the normal level to increasing than the normal value as a result respiratory infection related to bronchopneumonia and as the body’s defense mechanism against infection
Short term:After 3hours of nursing intervention, the client will have a decrease temperature from 38C to 37C
Long Term;After 2 days of nursing intervention, the client will maintain peripheral temperature within normal range.
Establish rapport
Assess gen. condition of the pt.
monitor and record VS
Provide TSB
Provide adequate rest periods
Encouraged client SO to provide for adequate ventilation
Instruct client’s SO to loosen the client’s clothing and wear loose clothing
Emphasized to client’s So the need for well balanced diet
Administer medications as order
To gain trust and cooperation of the pt.
to provide appropriate assessment and management
to obtain base line data
To promote heat loss by evaporation and conduction
To reduce metabolic demands
To have adequate oxygen exchange
To provide comfort
To increase body resistance and meet metabolic needs
To lower body temperature
trough pharmacologic means.
Short term:After 3 hours of nursing intervention the client shall have a decrease temperature from 38C to 37C
Long Term:After 2 days of nursing intervention, the client shall maintain peripheral temperature within normal range.
Problem #5: Sleep Pattern Disturbance
Assessment
Nursing Diagnosis
Scientific Explanation
Objectives Nursing Interventions
Rationale Expected Outcome

S=
O= pt manifested:>DOB
>restless
>frequent crying
>non-productive cough
Sleep pattern disturbance r/t external stimuli and DOB AEB restlessness
Pt’s suffering from pneumonia requires a comfortable position during sleeping which includes the high fowler’s position and an elevated head. Lying on flat on bed makes the pt uncomfortable and the occurrence of having DOB usually follows. However, if the pt is an infant, it would be more difficult for them to fall asleep not just because of shortness of breath but also of the pain they are experiencing. Another contributing factor is the unfamiliar environment which eventually affects the sleeping routine of the pt.
Short term: After 4 hours of NI, pt’s SO will be able to verbalize understanding o0f different sleep disturbance and will be able to demonstrate techniques to implement sleeping for the infant
Long term:After 3 days of NI, pt’s SO will be able to report improvement in pt’s sleep/rest pattern
Establish rapport
Assess gen. condition of the pt.
monitor and record VS
obtain feedback from the SO regarding usual bedtime routine and hours of sleep of the pt
observe parent-infant interactions provisions of emotional support
promote relaxation by providing calm and quite environment
elevate head by several degrees conducive for sleeping
To gain trust and cooperation of the pt.
to provide appropriate assessment and management
to obtain base line data
to determione usual sleep pattern and comparative baseline data
lack of knowledge of infant cues and problems relationship may create tension interfering with sleep routines based on adult schedules may not meet child’s needs
hospital environment can interfere to the sleep and relaxation of the child’s mind and body
upright position facilitates adequate ventilation and provides comfort
Short term: After 4 hours of NI, pt’s SO should be to verbalize understanding o0f different sleep disturbance and will be able to demonstrate techniques to implement sleeping for the infant
Long term:After 3 days of NI, pt’s SO should be able to report improvement in pt’s sleep/rest pattern

2. Actual SOAPIE’s
S=”sinisinat pa sya” as verbalized by the mother
O= Received patient sitting on bed, awake. With an ongoing IVF # 2 D5 IMB
>skin warm to touch
>with non-productive cough
>with abnormal breath sounds(rales)
>with shallow respirations
>DOB
>SOB
Vital signs taken as follows:
T= 37.5C
P=148 bpm
R=61 cpm
A= Ineffective airway clearance r/t retained pulmonary secretions AEB non-
productive cough secondary to BPN.
P= after 2-4 hours of N.I. pt. will have an improvement of airways patency
AEB minimal cough and normalized respiratory depth and rate.
I = Established rapport
= assessed gen. condition of the pt.
=monitored and recorded vital signs
=provided AM care
=auscultated chest and back for breath sounds
=kept pt.’s back dryo
=repositioned pt. periodically
=instructed pt.’s SO to increase fluid intake of the pt.
=Instructed pt.’s SO to elevate pt.’s HOB
=instructed pt.’s SO to perform CPT
=provides restful environment
E= Goal met AEB reduction of cough and normalization of RR
VI. CLIENTS DALY PROGRESS CHART’
1. Clients Daily Progress Chart
DAYS ADMISSION11-22-07
DAY 211-23-07
DISCHARGE11-24-07
Nursing Problems
1. Ineffective Airway Clearance * * *2. Ineffective Breathing Pattern * * *3. Impaired gas Exchange *4. Hyperthermia *5.Sleep pattern disturbance * * *
Vital Signs
Temperature 38°c 37.5°c 36.2°cPulse Rate 143 bpm 148 bpm 126 bpmRespiratory Rate 49 cpm 61 cpm 42 cpm
Laboratory Procedures
HematologyHemoglobinHematocritWBC LymphocytesPlatelet count
X-rayMedical Management
IVFD5IMB 500cc * * *
Nebulization

Salbutamol Neb * * N/ADrugs
Cefuroxime * * *Paracetamol * * AF
Diet
Diet for Age * * *
Activity/exercise
Activity as Tolerated * * *

2. Discharge Planning
The patient is actively playing with her mom. Still have cough and
slight difficulty of breathing.
S= 0
O=received pt. lying on bed on supine position, awake, with an ongoing IVF
#3 D5IMB 500cc at 450 cc level regulated at 29-30 mgtts/min infusing well
on the left arm.
>active
>Afebrile
>with normal breath sounds
>with good skin turgor
>slight DOB
>non-productive cough
Vital signs taken as follows:
T= 36.2C
P=126 bpm
R=42 cpm
A= for health maintenance and home management
P= after 30 mins. To 1 hour of N.I. pt. will verbalize understanding about
health teachings given.
I = established rapport
= assessed gen. condition of pt.
= monitored and recorded vital signs
= auscultated lung for breath sounds
= provided comfort measures
=IVF out at 12:40 pm
M= Cefixime 100mg/5ml susp. ¾ tsp BID
= SCMC syrup 1 tsp TID
= Multivitamins syrup 1 tsp OD
E= Activity as tolerated

T= To comply to treatment regimen
H= instructed pt.’s SO to increase fluid intake of the pt.
= instructed pt.’s SO to keep pt.’s back dry
= Instructed pt.’s SO to increase pt.’s intake of food rich in vit. C
= instructed pt.’s SO to perform chest and back tapping
O= Instructed pt.’s So to go back to the scheduled follow up check up
(Dec. 1 2007)
D=Diet for age
E= Goal met AEB SO’s verbalization of understanding about health teachings
given.
VII. CONCLUSION AND RECOMMENDATION
Pneumonia is an acute infection of lung parenchyma including alveolar
spaces and interstitial tissue. Pneumonia is a common illness in all parts of

the world. It is a major cause of death among all age groups. In children, the
majority of deaths occur in the newborn period, with over two million deaths
a year worldwide. The World Health Organization estimates that one in three
newborn infant deaths is due to pneumonia.] Mortality from pneumonia
generally decreases with age until late adulthood. Elderly individuals,
however, are at particular risk for pneumonia and associated mortality.
Pneumonia and its management still pose a challenge not only to the
health care team involve but also the person diagnosed with this condition.
However, recent advances in our understanding of the pathophysiology,
diagnosis, and monitoring of the different kinds of pneumonia can help
physicians optimize treatment strategies. Contemporarily treatment
guidelines emphasize an aggressive approach, with the prompt and liberal
use of antibiotic medications to the microorganism producing the disease to
control the spread to other parts of the body aside from its origin. It is
increasingly recognized that successful pneumonia treatment requires a
commitment from both patient and physician. Patient education can
empower persons with pneumonia top begin guided self management and
awareness of their disease condition. Such shared responsibility will help to
ensure a favorable outcome and an enhanced quality of life.
Often pneumonia begins after an upper respiratory tract infection (an
infection of the nose and throat). When this happens, symptoms of
pneumonia begin after 2 or 3 days of a cold or sore throat. Since pneumonia
often follows ordinary respiratory infections, the most important preventive
measure is to be alert to any symptoms of respiratory trouble that linger
more than a few days. Good health habits, proper diet and hygiene, rest,
regular exercise, etc., increase resistance to all respiratory illnesses. They
also help promote fast recovery when illness does occur. Proper consultation
can aid on the early diagnosis of the disease and treatment plan for decrease
duration of having the disease.
Because pneumonia is a common complication of influenza (flu),
getting a flu shot every fall is good pneumonia prevention. Vaccines to
prevent certain types of pneumonia are available. The prognosis for an
individual depends on the type of pneumonia, the appropriate treatment, any
complications, and the person's underlying health.

Learning Derive:
In doing this case study, I have learned new things about pneumonia. I
have learned that there are different factors that can lead you to acquiring
pneumonia. And that pneumonia usually occurs to pediatric pt. because their
immune system is not yet fully developed and that they have less body
defense against bacteria that causes pneumonia. The living condition or
situation can also contribute to the occurrence of the disease. There are also
vaccines, wherein before I never thought that there are such vaccines, that
we can get to prevent pneumonia from occurring. This case study makes me
realize a lot of things. One is that, before my perception about Pneumonia is
just “sipon and ubo”, I didn’t even know then what could be the cause of
Pneumonia, but with this study I’ve learned that different microorganisms
could cause the disease. And I’ve also learned the different types of
Pneumonia. The most important thing that I’ve learned from this study is not
on the disease proper but on how to come up with a good case study. If you
want to have a good case study you should get all the needed information
you need for your case, and don’t skip any information because this could
greatly affect your study. It is also important on how you establish rapport to
your client so that they will not be hesitant to give you information about
their family. -Emilyn Serrano
As we go along with our case study about BPN, I have learned so many
things about it on how to deal with it and how to handle this kind of case. It is
important to include not only the patient in the study but also the family of
the patient. Because a case study will not be completed unless the family is
not included. Bronchopneumonia is defined as a type of pneumonia that is
localized, often to the bronchioles and surrounding alveoli. It means that this
kind of disease may show any symptoms of coughing, chest pains, fever,
blood-streaked sputum, chills, and difficulty in breathing. This type of disease

may be nosocomial or community acquired. Patients who are immobile
develop retention of secretions; thus, most commonly involves the lower
lobes. If treated, recovery usually involves focal organisation of lung by
fibrosis. This type of diseases includes infants and the elderly people. BPN is
a disease that spreads from bronchioles to nearby alveoli. Now I’ve learned
the how painful the suffering of the people who are infected with this kind of
diseases. In treating this kind of disease we should always competent on
what we do especially on what we give to our patients because a single
mistake can put danger to the life of our patient. Giving medicines to our
patient can help them to recover fast and to be able to help them fight for
their disease. And also giving them nebulization can help them relieve chest
pain because too much secretion is blocking on their airway. And also we
should not always forget to put our shoes to our patients because through
this we would be able to understand them and also to gain their trust. We
should always remember that they are also humans like us, with a heart that
also needs nourishment and care from other people. Through giving
medicines regularly and also through treating them humanely our patient will
be able to recover fast and also to have a greater chance for improvement.
That’s why as a student nurse we should always practice to treat our patients
humanely no matter what race, looks and kind of person they are. So that in
the coming future hopefully if we would become a registered nurse we would
be able to remember and practice all the things that we have learned from
the past. And through this I’m sure that we would also be a successful nurse
because if you treat your patient humanely you will not only make them
happy but also God will be very proud of you.
-Adrian Guarin
VIII. BIBLIOGRAPHY
Deglin, Judith Hopfer & Vallerand, April Hazard. Davis’s Drug Guide for
Nurses(10th edition). Philadelphia, Pannsylvania. 2007
Smeltzer, Suzanne et al. Brunner & Suddarth’s Textbook of Medical-
Surgical Nursing(11th edition).

Doenges, Marilynn E. Nurse’s Pocket Guide: Diagnoses,
Interventions and Rationales. (9th Edition). F.A. Davis Co., 2004.
Delmars’s Pediatric Nursing Care Plans.(third edition)., Karla L.
Luxner
http://www.sciencedaily.com/releases/2007/06/070626123930.htm
http://www.netdoctor.co.uk/diseases/facts/pneumonia.htm
http://encarta.msn.com/encyclopedia_761577180/Respiratory_System.html
Angeles University Foundation
Angeles City
College of Nursing

A Case Study
Bronchopneumonia
Submitted by:
Dumas, Joycee
Guarin, Adrian
Serrano, Emilyn
Group 3
Submitted to:
Mr. Ercel Gamboa
Research Paper helphttps://www.homeworkping.com/





























