-
8/4/2019 4.01 Page Summary - Anaemia
1/11
4.01 Iron Deficiency Anaemia
Any condition in which the number of red blood cells/mm3,
theamount of Hb in 100mL of blood, and/or the volume ofpacked red
blood cells/100 mL of blood are than normalCLINICALLY DEFINED AS:
Concentration of oxygen-transporting material in a designated
volume of blood (incontrast to total quantities as in
oligocythemia,oligochromemia, and oligemia)
EPIDEMIOLOGY
30% of the total world population is anaemic
have Iron Deficienc 600 million eo le
RISK FACTORS & AETIOLOGY OF IRON DEFICIENCY:
1. Dietary lack2. Impaired Absorption3. Increased Requirement4.
Chronic Blood Loss
5.Dietary lack: Infants, Children, Impoverished, Elderly
6.Impaired Absorption - Due to Absorptive disorders,
Steathorrhea,Chronic Diarrhoea, Gastrectomy ( hydrochloric acid and
transittime in duodenum)
7.Increased requirement.
Growing infants and children, adolescents, and premenopausal
(especially pregnant)
Risk: socioeconomic females with multiple, frequent
pregnancies
8.Chronic Blood Loss
Most common cause of iron deficiency in the Western world.
If bleeding occurs into tissues or cavities of the body, the
hemeiron can be totally recovered and recycled.
However, external hemorrhage, as can occur from the GIT, the
urinary tract, or the genital tract, depletes iron reserves
t men and postmenopausal women in the Western world must
beattributed to GIT blood loss until proven otherwise
(important
PATHOPHYSIOLOGY
Iron Deficiency produces a Hypochromic Microcytic
Anaemia.Simultaneously, depletion of essential iron-containing
enzymes in cellsthroughout the body can cause other changes,
including koilonychia,alopecia, atrophic changes in the tongue and
gastric mucosa, andintestinal malabsorption.
- Reserves in the form ofFerritin andHemosiderin may be adequate
to maintainnormal hemoglobin and hematocrit levels aswell as normal
serum iron and Transferrinsaturation.
- Progressive depletion of these reserves firstlowers serum iron
and transferrin saturationlevels, without producing anemia.
- In this early stage, there is increased erythroidactivity in
the bone marrow.
- Anemia only appears when iron stores arecompletely depleted,
accompanied by lowserum iron, serum ferritin, and
transferrinsaturation.
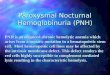
Hypochromic microcytic anemia of iron deficiency (peripheral
bloodsmear). Note the small red cells containing a narrow rim of
peripheralhemoglobin. Scattered fully hemoglobinized cells, present
due to recentblood transfusion, stand in contrast.Patients may be
asymptomatic due to:
Slow Hb Haemodynamic Compensation & enhancement of O2-
carrying capacity of blood
2,3-DPG (aka: BPG) Right shift of O2 dissociation curve so
that
CLINICAL FEATURES
General Symptoms (very non-specific)
Angina Dyspnea
Palpitations Intermittent
Claudication
Fatigue Headaches
Faintness
General Signs
Systolic Flow Murmur Cardiac failure
Tachycardia Pallor
Rarely: papilloedema & retinal haemorrhages after acute
bleed (can be accompanied by blindness).
SIGNS IN SPECIFIC ANAEMIAS
MICROCYTIC:
Iron Deficiency Anaemia
Tongue Papillae atrophy
Brittle Hair and Nails
Angular stomatitis
Koilonychia (spoon nails)
Epithelial changes
Dysphagia & Glossitis
(Plummer-Vinson/Paterson-Brown-Kelly
syndrome)
NORMOCYTIC
Haemolytic Anaemia: Destroyed Cells Journey to the Spleen
Dark urine
Chills
Jaundice
Splenomegaly
Aplastic Anaemia: Bleeding, Infection & Bruising
MACROCYTIC
Megaloblastic Anaemias
Symptoms Malaise (90%) Dyspnea (50%)
Paraesthesiae (80%) Mouth soreness (20%)
Weight Skin pig. change
Grey hair Impotence
Memory Depression
Personality change Hallucinations
Visual disturbance
Signs
Pyrexia
Angular Stomatitis (Cheilosis)
Skin pigmentation change andVitiligo
Tongue Smooth
Heart failure
B12 Deficiency Additional Neuro Signs
Neurological disease in up to 40% of cases.
Focal demyelination affecting:
Ferritin: Iron-protein complex, containing ~23% iron; Ferric
Ions + Apoferritin;
Found in intestinal mucosa, spleen, BM, reticulocytes &
liver; Regulates ironstorage & transport from intestinal lumen
to plasmaHemosiderin: Golden yellow or yellow-brown insoluble
protein produced by
phagocytic digestion of hematin; found in most tissues,
especially liver, spleen, andBM; In the form of granules much
larger than ferritin molecules (of which they arebelieved to be
aggregates); Higher content ~37% of iron; stains blue with
PerlPrussian blue stain.Transferrin: Iron-transporting protein;
Non-heme Beta -1 Globulin of the plasma,capable of associating
reversibly with up to 1.25mcg iron/g. EXTRA
-
8/4/2019 4.01 Page Summary - Anaemia
2/11
DIAGNOSISBased on Hx & Examination (see clinical
features)
FBCAnaemia indicated by Hb on FBC +/- Clinical features
Furtherinvestigation based on MCV
RDW (Red cell distribution width; variation in the size of
yourRBCs; demonstrates anisocytosis) may also assist in Normal
MCV(normocytic anaemia), Low MCV (microcytic anaemia) and HighMCV
(macrocytic anaemia)
Blood Film: Elicits hallmarks of cells indicating diagnosis or
furtherinvestigation
FURTHER INVESTIGATION
MICROCYTICIron Deficiency Anaemia (IDA)
Hx Diet, meds (NSAIDs), bleeding (esp menstrual)
Blood Film
o Microcytic RBCs (MCV < 80 fL)
o Hypochromic (MCH < 27 pg)
o Poikilocytosis (variation in shape)
o Anisocytosis (variation in size)
o Target cells present
Iron Studies
o Plasma Ferritin - Best single test to confirm IDA
(Measures iron stores; very sensitive (other measuresaffected by
many factors)
o Transferrin saturation of 120 fl
RCC for degree of anaemia
Blood Film Oval Macrocytosis, Poikilocytosis, RBCFragmentation,
Hypersegmented Neutrophils
Retic count for degree of anaemia
Leuc count or N
Platelet count or N
Bone Marrow Cellularity, Megaloblastic changes in
erythroidseries, giant metamyelocytes, dysplasticmegakaryocytes,
increased iron in stores,pathological non-ring sideroblasts
Serum Ferritin
Plasma LDH often
Serum Bilirubin May be from ineffective erythropoiesis
Serum Vit B12 Schilling Test: usually
-
8/4/2019 4.01 Page Summary - Anaemia
3/11
NORMAL BONE MARROW FUNCTION
Bone marrow array of cells, specialized functions- Host defence
(granulocytes, monocytes, lymphocytes ie white cells)- Oxygen
transport (erythrocytes ie red cells)- Haemostasis (platelets
released by megakaryocytes)
Haemopoiesis takes place in the bone marrow after7 months
gestation,& priorto this in the fetal liver & spleen.
The haemopoietic stem cell:- is capable ofself renewal- is
capable ofdifferentiation ("multipotent or pluripotent") to
erythroid, lymphoid ormyeloid (granulocytic, monocytic,
erythroid,
or megakaryocyte) progenitors.- has no unique morphological
characteristics & is morphologicallyidentical to a small to
intermediate sized lymphocyte.
Exposure to haemopoietic growth factors stem cell
becomescommitted (differentiation). Commitment to a lineage is
irreversible &the capacity for self-renewal is lost as
maturation progresses. Growthfactors continue to influence cell
maturation & subsequently function.
Haemopoietic growth factors are produced by an array of
haemopoietic& stromal cells which reside in the marrow.
EPO is an exception in that its main source is the kidneyGrowth
factors are in general stimulatory although inhibitory factors
alsoexist. Growth factors act in synergy with each other especially
in lowconcentrations.
Bone marrow microenvironment provides a suitable structural,
nutritional &hormonal environment for haemopoiesis. The
microenvironment includes:
Stromal cells (macrophages, fibroblasts, reticulum cells, fat
cells &endothelial cells). Stromal cells are one important
source ofhaemopoietic growth factors & othercytokines. They
have animportant role in haemopoietic cell adhesion, through cell
adhesionmolecules, & hence determine the localisation of
haemopoiesis.
Extra-cellular matrix (ECM including components such
as:fibronectin, laminin, collagen & proteoglycans)
Microvascular network of thin walled venous sinusoids
allowingcommunication with the rest of the body through the
systemiccirculation
Some haemopoietic growth factors have established roles in cl
inicalpractice eg EPO (erythropoietin), G-CSF (Granulocyte - Colony
Stimulatingfactor) & GM-CSF (Granulocyte/Monocyte - Colony
Stimulating Factor).Most common nutritional deficiency that lead to
alterations inhaemopoiesis are deficiencies ofVitamin B 12, Folate
& Iron
Other Factors Required for Normal Haemopoiesis
(EspeciallyErythropoiesis):- Metals - iron, manganese, cobalt-
Vitamins - vitamin B 12 , folic acid, vitamin C, E, B 6 ,
thiamine,
riboflavin & pantothenic acid- Amino acids
LIFE HISTORY OF RED CELL:GENERATION, LOSS & DESTRUCTION
Red cells - formed in the red marrow from Erythroid
StemCells
Mature under influence of erythropoietin (EPO) through anumber
of divisions leading from Erythroblasts Erythrocytes/RBCs
120 day life span. Normally balance
b/wproduction/destruction
Production can be accelerated up to 7X fold if demand (Achieved
by expansion of the volumeof red marrow andby shortening of the
transit time for red cell maturation(skipped divisions).
Destruction after their 120 day life span may involvecontinual
loss of membrane components, theaccumulation ofproductsofoxidated
damage and/ordecreased deformability of the RBC Unable to
squeezethroughtheminute (1-2 um) fenestrations in the
splenicmicrovasculature Effete RBC finally phagocytosed
bymacrophages of the Reticuloendothelial System, mainly inthe
spleen but also in the Liver and BM. Phagocytosis ofRBCs becomes
more prominent when red cell survivalis shortened (hemolysis).
Blood Loss Anaemia
Clinical signs are very different in anaemia:
Acute: Secondary to blood loss (following trauma or surgery)
Acute blood loss anaemia, there are changes in the pulseand BP
and the patient may present in a state of shock(Very low BP, Rapid
pulse, cold & discoloured extremities,sweating, dilated pupils
etc)
"Reactive " thrombocytosis (raised platelet count) and areactive
increase in white blood cells (leucocytosis) mayoccur.
Chronic (intermittent or slow bleeding from eg peptic ulcer
orheavy menstrual loss - menorrhagia).
Compensating mechanisms which allow the patient tofunction in
their day to day activities with relative ease.(Alteration in Hb
function allowing oxygen release to thetissues more readily)
Chronic blood lossresults in iron deficiencyIt is clear that for
a proper assessment of a person with bloodloss anaemia there are
three critical processes:
- Careful history (abnormal bleeding, menstrualhistory in women,
symptoms of peptic ulcer, alteredbowel habit etc.)- Physical
examination - signs of acute bleeding, iron
CONSEQUENCES OF DEFICIENCIES OF ESSENTIAL HAEMATINICS
Deficiency of one or more of these elements involved in
haemopoiesis AnaemiaDiagnosis relies on history, physical
examination and laboratory tests, commencing with a blood count and
examination of the blood film.Iron deficiency is the commonest
cause of anaemia throughout the world. In underdeveloped countries
this is due to gastrointestinal blood lossfrom hookworm
infestation.In our society, the commonest cause of iron deficiency
is menstrual blood loss in fertile women. This is so common as to
be consideredalmost "normal for age". In older women and men, the
diagnosis of iron deficiency which cannot be explained by obvious
blood loss must be
followed by a search for a source ofoccult bleeding, possibly
from a carcinoma of the gastrointestinal tract or from peptic
ulceration of thestomach.Iron deficiency anaemia is also common in
infants and young children due to poor iron intake.48711500 Dr
Hambury Ronald Cooper chlormycetin eye drops -
patientMICROCYTOSIS:The laboratory hallmark of iron deficiency is
the presence of small red blood cells. This can be best appreciated
from the electronically derivedmean corpuscular volume (MCV).
Normal MCV is 80-100fl but in iron deficiency the MCV falls to
under 80fl.Specific studies: serum iron level, serum transferrin
and serum ferri tin (the best measurement of overall iron stored in
the body).
MACROCYTOSIS:Reductions in the amount of folic acid orvitamin B
12in the body result in anaemia characterised by an increase in red
cell size and specificappearances within the bone marrow
(megaloblastosis).
- The MCV is over 100fl and the blood film shows large red cells
and variations in size and shape.- There may also be changes in the
neutrophils which can show marked nuclear hypersegmentation.- Not
all causes of macrocytosis induce megaloblastosis of the bone
marrow Excess alcohol consumption for example is the
commonest cause of macrocytosis in our community but is not
associated with megaloblastic anaemia.Unlike iron deficiency, the
lack of folic acid or vitamin B 12 is rather uncommon.Deficiency of
vitamin B 12Can cause profound neurological damage. Lack of vitamin
B 12 is most commonly caused by poor absorption from the bowel.
- Autoimmune disease known as pernicious anaemia Ab produced by
the patient's own immune system destroys gastric cells
whichnormally secrete a substance known as intrinsic factor.
- Intrinsic factor must bind to vitamin B 12 in the stomach for
vitamin B 12 to be absorbed in the terminal ileum. When intrinsic
factor is nolonger secreted vitamin B 12 absorption ceases.
- Other non-immune causes for vitamin B 12 deficiency also exist
including surgical removal of stomach or terminal ileum.Folic acid
absorption occurs in the jejunum and does not require intrinsic
factor. Diseases affecting the small bowel (eg coeliac disease)
orsurgical removal of large segments of small intestine can
therefore impair its absorption. Some groups of patients with poor
diets eg the elderly,severely depressed individuals and adolescents
can also become deficient from inadequate folic acid intake.
Hemolytic Anemia - any anemia resulting from an increased rate
of erythrocyte destruction
-
8/4/2019 4.01 Page Summary - Anaemia
4/11
HAEMOLYSIS - Premature Destruction of RBCs
RBC survives 120 days; shortening in time = haemolysis
Survival measurement: radiolabel RBC with Chromium-51 and
re-inject, sample at intervals of several days to measure
removal(rarely used)
Haemolytic Amaemia Lab Tests:
Hb Rapidly reduced due to either Haemolysis of Blood Loss.
If
Haemolysis, confirm with clinical presentation of Scleral
jaundice& splenomegaly (from RBC destruction)
Reticulocytes
Bilirubin (from haem breakdown from Hb)
Lactic DeH (LDH; found in RBCs)
Haptoglobulin Absent (haptoglobin binds haem and prevents
renal excretion)
Blood Film Examination look for morphological changes
Bone marrow examination (rarely performed) - May show
erythroid hyperplasis ( RBC precursors)
Coombs Test: Looks for Abs on the cell surface (direct
antiglobulin tests) if immune mediated hemolysis
suspectedMechanisms of Haemolysis:
- Abnormalities of RBC membrane and underlying
cytoskeletalproteins loss of surface lipid and spherocyte formation
(eghereditary spherocytosis)
- Enzyme deficiencies in RBC: Commonest is G6P DeH (RBC cantmake
NADPH antioxidant; Excessive oxidant stress denatures Hb
Haemolysis)
- Abnormalities of the Hb structure or synthesis (inherited)
(e.g. SickleCell and Thalassaemia)
- Autoimmune destruction in spleen and liver (due to production
of
VITAMIN B12 AND THE NERVOUS SYSTEM
B12 involved myelin (and other protein) synthesis by glial
cells
Deficiency fatty deposits in the myelin and coalesce
(largestfibres most affected)
Slower AP conduction cant sustain high frequency information
blocked transmission
May affect: (1) Peripheral Nerves, (2) Spinal Cord, (3)
Brain
1. Peripheral Nerves - Peripheral Neuropathy of:Sensory
Neurons:
Numbness and Parasthesias ("pins and needles") in hands andfeet,
often symmetrically (glove and stocking distribution).
Due to slowing and asynchrony of APs in sensory neuronesMotor
Neurons
Motor weakness due to wasting of peripheral muscles may
occur
Stretch reflexes are diminished in affected regions2. Spinal
Cord - Two major pathways affected in the white matter ofthe spinal
cord (combined degeneration)
I. Dorsal Or Posterior Columns (will cause SensoryDifficulties,
Proprioception loss (particularly in the dark), Loss ofthe sense of
Vibration)
II. Lateral Corticospinal Tract (will cause Stretch
reflexes are exaggerated, Motor tone is increased, Babinski
signis present)
3. Brain - Demyelination results in Confusion,
Depression,Moodiness, Memory Losses, Overt Psychosis
Prognosis:
Symptoms rapidly resolve with B12 treatment
Recovery from demyelination and associated axonal damage
-
8/4/2019 4.01 Page Summary - Anaemia
5/11
OTHER MICROCYTIC HYPOCHROMIC ANAEMIAS
Anaemia of Chronic Disease- Normocytic, can be normochromic-
Mild Hb rarely 95fl, as high as 120-140gl)- Macrocytes typically
oval in shape- Reticulocyte count low,
- May be moderately reduced platelet and WCC- Hypersegmented
neutrophils (6 or more lobes)- serum bilirubin, hydroxybuturate and
lactate dehydrogenase as
result of marrow cell breakdown- Marrow hypercellular, large
erythroblasts, giant and abnormally
shaped metamyelocytesPathogenesis:
Folate causes anaemia by inhibiting thymidylate synthesis, a
ratelimiting step in DNA synthesis. Folate is delivered to cells as
MethylTHF, which is a coenzyme for this reaction.B12 is also
involved in this step as is demethylates methyl THF to THFto be
used in synthesis of folate. the proximate cause of anaemia inB12
deficiency is folate deficiency see appendix 1 for more infoB12 and
Pernicious anaemia: - due to autoimmune attack atrophyof stomach.
Wall of stomachbecomes thin, plasma cell and lymphoidinfiltrate
oflamina propria. There is achlorhydria and absent secretionof
Intrisic Factor (IF) which is necessary for absorption of B12
Causes of microcytic anemia = TAILS: T- Thalassemia,A - Anemiaof
chronic disease, I- Iron deficiency anemia, L - Lead
toxicityassociated anemia, S- Sideroblastic anemia.
-
8/4/2019 4.01 Page Summary - Anaemia
6/11
Appendix 2
Intravascular haemolysisCaused by:
- mechanical injury: caused by defective cardiac valves, thrombi
withinthe microcirculation, or repetitive physical trauma (marathon
running,bongo drum beating) can physically lyse red cells.
- complement fixation: can occur on antibody-coated cells
duringtransfusion of mismatched blood.
- infection by intracellular parasites such as falciparum
malaria, orexogenous toxic factors: Toxic injury is exemplified by
clostridialsepsis, which releases toxins that attack the red cell
membrane.
Intravascular hemolysis is manifested by
hemoglobinemia and hemoglobinuria
jaundice
hemosiderinuria
Methalbuminaemia.
Decreased serum haptoglobin
Free hemoglobin in plasma is promptly bound by an 2-globulin
(haptoglobin), producing a complex that is rapidly cleared by
themononuclear phagocyte system, thus preventing excretion into
theurine.
When haptoglobin is depleted free hemoglobin prone to oxidation
tomethemoglobin, which is brown in color. The renal proximal
tubular
cells reabsorb and catabolize much of the fil tered hemoglobin
andmethemoglobin, but some passes out with the urine, imparting a
red-brown color. Iron released from hemoglobin can accumulate
withintubular cells, giving rise to renal hemosiderosis.
Concomitantly, hemegroups derived from the complexes are
catabolized to bilirubin withinthe mononuclear phagocyte system,
leading to jaundice. In hemolyticanemias, the serum bilirubin is
unconjugated and the level ofhyperbilirubinemia depends on the
functional capacity of the liver andthe rate of hemolysis. When the
liver is normal, jaundice is rarelysevere. Excessive bilirubin
excreted by the liver into the gastrointestinaltract leads to
increased formation and fecal excretion of urobilin
Extravascular hemolysis
extreme alterations in shape are required for red cells to
navigate thesplenic sinusoids successfully, reduced deformability
makes thepassage difficult and leads to sequestration within the
cords, followed
by phagocytosis. This is an important pathogenetic mechanism
ofextravascular hemolysis in a variety of hemolytic anemias.
Withextravascular hemolysis, hemoglobinemia and hemoglobinuria are
notobserved, and its principal features are anemia and jaundice.
However,some hemoglobin inevitably escapes from phagocytes, leading
todecreases in plasma haptoglobin. The morphologic changes
areidentical to those in intravascular hemolysis, except that
"work"hyperplasia of the mononuclear phagocyte system often leads
tosplenomegaly.
Appendix 1
Two reactions in humans are known to require vitamin B12.
1) Methylcobalamin is an essential cofactor for
methioninesynthase, an enzyme involved in the conversion
ofhomocysteine to methionine. In the process,methylcobalamin yields
a methyl group and is regeneratedfrom N5-methyltetrahydrofolic acid
(N5-methyl FH4), theprincipal form of folic acid in plasma.
2) In the same reaction, N5-methyl FH4 is converted
totetrahydrofolic acid (FH4). FH4 is crucial, since it is
required(through its derivative N5,10-methylene FH4) for conversion
ofdeoxyuridine monophosphate to deoxythymidinemonophosphate, an
immediate precursor of DNA
It has been postulated that the fundamental cause of impaired
DNAsynthesis in vitamin B12 deficiency is the reduced availability
of FH4,most of which is "trapped" as N5-methyl FH4.34In addition,
the deficit inFH4 can be exacerbated by an "internal" folate
deficiency caused by afailure to synthesize metabolically active
polyglutamylated forms.35Thismay stem from a requirement for
vitamin B12 in synthesis ofmethionine, which contributes a carbon
group needed in the metabolicreactions that create folate
polyglutamates. Whatever the mechanism of internal folate
deficiency, lack of folate isthe proximate cause of anemia in
vitamin B12 deficiency, as the anemia
inevitably improves with administration of folic acid.
WARM ANTIBODY IMMUNOHEMOLYTICANEMIA. - MOST COMMON FORM (48% TO
70%)OF IMMUNE HEMOLYTIC ANEMIA.- Mostly IgG but sometimes IgA-
Mostly extravascular destruction- IgG-coated red cells bind Fc
receptors onmonocytes and splenic macrophages, which resultsin loss
of red cell membrane during "partial"phagocytosis.As in hereditary
spherocytosis, the loss of cellmembrane converts the red cells to
spherocytes,which are sequestered and removed in the spleen,the
major site of red cell destruction in this disorder.
Thus, moderate splenomegaly is characteristic ofthis form of
anemia.
Cold Agglutinin Immunohemolytic Anemia. -caused by so-called
cold agglutinins, IgM antibodiesthat bind and agglutinate red cells
avidly at lowtemperatures (0 to 4C).- accounts for 16% to 32% of
cases- Antibodies appearacutelyafter mycoplasmapneumonia and
infectious mononucleosis selflimited, clinical features rare.-
Other infectious agents assoc. with this form ofinclude CMV,
influenza virus, HIV.- Chronicanemias occur in association with
certainlymphoid neoplasms or as an idiopathic condition.- Clinical
symptoms binding of IgM to red cells at
sites such as exposed fingers, toes, and ears wheretemp
-
8/4/2019 4.01 Page Summary - Anaemia
7/11
Past Exams MEQs
2003 MEQ paper 1: Brian Murphy is a 77 year old man who presents
toyour surgery complaining of tiredness and dyspnoea. You note that
he ispale and has signs of heart failure. His haemoglobin measures
87g/L(normal range 125-165 g/L).1. Name 3 laboratory test results
that would suggest the anaemia is due tohaemolysis rather than
reduced red cell production.Model Answerraised reticulocyte
count
positive direct antiglobulin (Coombs) testraised bilirubin
levelabsent haptoglobin in serumraised serum LDH
presence of methaemalbumin in serum
2. a) Which components of the red cell are responsible for blood
groups?b) The direct antiglobulin (Coombs) test is requested and is
positive. Whatdoes the direct antiglobulin test detect?Model
Answer
a) Surface glycoproteins and/or glycolipidsCellular carbohydrate
transferasesb) The presence of immunoglobulin and/or complement on
the surface ofred blood cells
3. Describe two possible mechanisms of destruction of
circulating red cellswhich become coated with
immunoglobulin/antibody.Model Answer(i) antibody fixes complement
and red cells lyse in the circulation(ii) antibody fails to fix
complement and red cells are removed fromcirculation in the liver
or spleen via Fc receptors of reticulo-endothelial
cellmacrophages)
4. The patient is treated with oral prednisone. Name two short
term andtwo long term complications of oral corticosteroid
administration.Model Answer
Short term: mood change, insomnia, hyperglycaemia,
hypertension,Long term: obesity, skin thinning, bruising,
cataracts, adrenalsuppression, osteoporosis, infection
2001 MEQ paper 1: Sarah Weiss is a 15 year-old girl who comes to
theGP with her mother who is concerned that Sarah has lost weight,
seemstired all the time and appears pale. Up until 10 months ago,
Sarah was agood eater and was a normal and active girl. Her weight
is now 58 kg(was previously 68 kg) and her height is 165 cm.The GP
orders a full blood count (FBC) and blood film which show:
FBC Sarahsresults
Referencerange
Blood film
WCC 8.1 x 109/L 4.513.0 x109/L
Hypochromia +
Platelets 598 x109/L
150600 x109/L
Microcytosis +
Haemoglobin *81 g/L 120160 g/L Poikilocytes +
MCV *71 fl 7895 fl Pencil cells occasional(thin elongated
cells)
MCHC *295 g/L 320360 g/L
1. RegardingSarahs blood filmand red cell indices,which 2
features aremost helpful insuggesting thecause of heranaemia is
irondeficiency?Model AnswerHypochromia (asshown by lowMCHC)
andmicrocytosis (asshown by low MCV)are characteristicfindings of
irondeficiency anaemia.Other red cellchanges such as
pencil cells are less reliable indicators of iron deficiency.
The plateletcount at the upper end of the normal range (borderline
thrombocytosis)suggests that blood loss may be a factor.
2. You plan to do additional tests to confirm the diagnosis.
List 3 additionalblood parameters you would test which would
confirm a diagnosis of irondeficiency. Specify whether you would
expect each to be high, low ornormal.Model AnswerConfirm the
diagnosis of iron deficiency with appropriate iron studies (eg,low
serum iron, high serum transferrin and total iron binding capacity,
lowiron saturation, low serum ferritin)
For the past year Sarah has not eaten meat, fish, chicken, eggs,
ormilk products. She changed to a vegan diet consisting of
greenvegetables, legumes and cereals because of concerns about
killing
animals and eating animal products.
3. a) Give 2 foods or food types which would have been the major
sourcesof iron in her diet during the past year.b) How might the
bioavailability of iron be increased in her diet?Model Answera)
Cereals and legumesb) By taking in more foods containing vitamin C,
eg, citrus, tomatoes.
2005 RFA 2: Cynthia Salakas is a 78-year old widow who presents
withdyspnoea, palpitations on exertion and "pounding in the ears".
She alsodescribes unsteadiness on standing with occasional falls.
Mrs Salakaslives alone with no family support and prepares her own
meals. Onexamination, she is pale and anxious, with a tachycardia
of 100 beats/minand BP of 130/80. The spleen is just palpable but
there is nolymphadenopathy.
A full blood count shows the following:
Indices Mrs Salakas' Results Normal Range
Hb 68 g/L 115 - 165 g/L
MCV 124 fl 76 - 96 fl
WBC 3.5 x 109/L 4.0 - 11.0 x 109/L
-
8/4/2019 4.01 Page Summary - Anaemia
8/11
Platelets 89 x 109/L 150 - 500 x 109/L
1. List at least THREE common causes of a macrocytic
anaemia.Model AnswerLiver disease, Vitamin B12 deficiency, Folate
deficiency, Alcohol excess,Myelodysplastic syndromes, Drug effect
(drugs interfering with DNAsynthesis cytotoxics and
immunosuppressive agents), Haemolysis orhaemorrhage
(reticulocytosis)
She has had difficulty preparing her own meals over the past
fewmonths as she feels very unsteady and has resorted to
toastedcheese or tomato sandwiches several evenings per week as
hermain meal. She often consumes only half to three-quarters of
her
usual intake and she has noticed some weight loss which she
isbecoming concerned about.2. What nutritional assessment methods
could you use to decide if MrsSalakas is malnourished? (Give
THREE)Model Answer1) Diet history and food frequency: ask the
patient for all foods and fluidsconsumed over a typical week and
how this may have changed over thepast few months-compare previous
to now. Also do a food frequency ofmajor food items consumed over 1
week. Compare intake torecommendations for her age and gender.
Consider the patients barriersto be able to obtain a normal
intake.2) Anthropometry: ask the patient for a weight history over
the past 6-12months.3) Laboratory results: consider the current
results obtained and determineif further studies are required to
determine if anaemia is likely due to poordiet and if the patient
also has overall malnutrition.
Further testing shows a serum B12 level of 60 pmol/L (normal
range130-600 pmol/L) with normal red cell folate level.3. Describe
the typical blood film of B12/folate deficiency.Model
AnswerVariable anaemia, red cells are macrocytic, with increased
oval forms anda marked variation in size (anisocytosis) and shape
(poikilocytosis),Variable leukopenia. Neutrophils show
hypersegmentation (greater than 6lobes) with occasionalgiant forms
(macropolycytes), Variable thrombocytopenia, with
giantplatelets
You perform a neurological examination on Mrs Salakas.
Herperception of position, sense and vibration is impaired in the
feetand hands. Tendon reflexes are generally brisk with upgoing
plantars. Her gait is abnormal, with unsteadiness on
walking.
4 a) Describe the location and nature of the pathological
effects of B12deficiency on the nervous system.b) Describe at least
TWO of the main neurological signs associated withB12
deficiency.
Model Answera) Primarily affects white matter of the dorsal and
lateral columns of thespinal cord, and cerebral cortex Myelin
degeneration and loss of nervefibres in dorsal and lateral tracts,
nerve degeneration in dorsal root gangliaand peripheral nerves
(subacute combined degeneration)b) Confusion, impaired memory,
Sensory changes dominate symmetricaltered sensation, paraesthesiae
in glove-stocking, distribution. Laterchanges include ataxia, gait
problems, reduced vibration and positionsense, Upper motor neurone
signs weakness, increased tendon reflexesand Babinskis sign, late
in disease (lateral column disease).
Mrs Salakas is transfused initially and commenced on a course
ofparenteral B12 replacement. After two weeks in hospital she
feelsmuch improved and is anxious to return home.5. You are about
to discuss handing over her care with her local GP. Listat least
TWO community services or agencies that could provide
supportfollowing her assessment as fit to go home. Give a brief
explanation ofeach agency's role and why she might require their
involvement.Model AnswerAgencies RoleHome/community nursing
Supervision of medications, wound dressings,review of function at
home, sometimes showering/personal hygieneHome care Assistance with
cleaning home, showering/personal hygieneMeals on wheels MealsOT
home assessment Minimise risk of falls from instabilityOutpatient
physiotherapy and transportation Continued improvement
ofneuromuscular function
2004 RFA 2: Soraya Mahfouz is a 73 year old woman, widowed one
yearago. She has been brought to you, her GP, by her son who is
concernedthat she is not coping. Mrs Mahfouz reports that she
doesnt feel up tomuch, and while insisting that she is managing at
home, is clearlyavoiding activity due to fatigue and breathlessness
on exertion that hasbecome more of a problem in the last three
months. She has lost 4-5 kg inthe last year but has no specific
symptoms on system review other than
features of moderate depression. On examination she has pallor
ofmucous membranes and nailbeds and you suspect that she is
significantlyanaemic. She has no evidence of bruising or
splenomegaly, but her liveredge is palpable 2 cm below the costal
margin.
1. Identify two features from this womans history and/or
examinationsuggestive of anaemia. For each of these features state
why they aresuggestive.Model Answer* Fatigue and breathlessness
with physical activity may reflect a rise incardiac output
incompensation for a decreased erythrocyte mass* Pallor of mucous
membranes and nailbeds these are sites which allowreliable
detection ofpallor, from which one can infer a decrease in the
oxygen-carryingcapacity of the blood
Her haemoglobin is 93 g/L, (normal range 115 - 165 g/L),
meancorpuscular volume is 72 fL (normal range 80 - 100 fL) and
meancorpuscular haemoglobin concentration is 295 g/L (normal range
310- 350 g/L). Platelet and white cell measures are normal, as is
theblood film.2. Describe the physiology of red blood cell
production. Pay particularattention to key nutritional components
and any other relevant stimulatoryfactors.Model AnswerRed blood
cells are produced in the bone marrow. They require
numerousmicronutrients including iron for haem and vitamin B12 and
folate whichare essential for maturation. The hormone
erythropoietin stimulates theirproduction and is secreted in
response to hypoxic conditions in the kidney,
such as after haemorrhage or in high altitude living.
3. What is the most likely micronutrient deficiency underlying
this womansanaemia and why?Model AnswerThe most likely deficient
micronutrient is iron, because the MCV and theMCHC are both reduced
(microcytic, hypochromic anaemia). B12 andfolate deficiencies
produce a megaloblastic anaemia.
4. List 3 additional blood parameters you would test which would
confirm adiagnosis of iron deficiency. Specify whether you would
expect each to behigh, low or normal.Model AnswerConfirm the
diagnosis of iron deficiency with appropriate iron studies (eg,low
serum iron, high serum transferrin and total iron binding capacity,
lowiron saturation, low serum ferritin)
5. Describe the mechanisms by which the biochemical environment
in thetissues mediates oxygen delivery to active cells from
haemoglobin in redcells.Model AnswerIn active tissues, higher
temperature, acid pH, high concentrations of CO2and 2,3-
diphosphoglycerate (product of anaerobic glycolysis) all shift
thehaemoglobin dissociation curve to the right, decreasing the
affinity ofhaemoglobin for oxygen.
You confirm that she has a significant iron deficiency, with
depletediron stores.6. a) What is the most likely cause of iron
deficiency anaemia in a womanof this age?b) What tests would you
recommend to confirm the most likely cause?Model Answer
a) In post-menopausal females, the commonest cause of iron
deficiency isgastrointestinal blood loss.b) Gastroscopy and
colonoscopy or other imaging of the gastrointestinaltract
7. Soraya is likely to need some services to help her live in
thecommunity. A referral is made to the Aged Care Assessment
Team(ACAT).a) Write a short paragraph describing, for Soraya and
her son, the role ofthe ACAT team.b) Write another short paragraph
explaining what they should know aboutCommunity Aged Care Packages
(CACPs).Model Answera)* ACATs help older people and their carers
work out what kind of care willbest meet their needs when they are
no longer able to manage at home
without assistance* ACATs provide information on suitable care
options and can helparramge access or referral to appropriate
community or residential care*They are usually attached to
hospitals or community centres* They provide thorough assessments
of care needs* The team usually consists of doctors, nurses, social
workers and alliedhealth professionals (including occupational
therapists, physiotherapistsand speech therapists)
-
8/4/2019 4.01 Page Summary - Anaemia
9/11
* They are usually accessed via the local doctor or sometimes
duringhospital admissionb)* Community Aged Care Packages (CACPs)
are planned and coordinatedpackages of care to help older people
remain living in their own homes* They may include help with
bathing, showering or personal hygiene,social support, transport,
laundry, meal preparation and gardening* The Australian Government
provides a subsidy to local service providersand clients pay a
portion of the fee (depending on their own income andability to
pay)* For people on a basic pension, fees must not exceed 17.5% 0f
thatpension.* People on higher incomes may be asked to pay
additional fees (limitedto 50% of any income above the maximum
pension rate)* Access to CACPs is only possible following an
assessment and referralby the ACAT team
Past Exams SBAs
Case 6Mrs Mehar Singh is a 45 year old woman who complained of
increasinglethargy over the past month and was found to have pale
mucosa onexamination. Her blood count shows a haemoglobin of 90 g/L
(115-165g/L) with mean cell volume of 60 fL (75-100 fL), white cell
count of 6 x109/L (4-11 x 109/L) and platelets of 510 x 109/L
(150-400 x 109/L). Her GPnotes that a previous haemoglobin result
at the time of her hysterectomytwelve months ago was normal.
Investigations demonstrate that she isiron deficient.
25. Further investigations should include:
1 A) Isotope tests of vitamin B12 absorption2 B) Bone marrow
examination3 C) Upper endoscopy and colonoscopy4 D) Duodenal biopsy
for adult coel iac disease
Answer C
26. The best immediate marker of a response to iron therapy
would be:1 A) Normalisation of the platelet count2 B) Increasing
reticulocyte count3 C) Increase in haemoglobin4 D) Reduction in
pallor
Answer B
27. Which of the following is most correct regarding dietary
ironabsorption?1 A) The major site of absorption is the lower small
intestine2 B) Iron in eggs and vegetables is as well absorbed as
iron inmeat3 C) Ferrous iron is more readily absorbed than ferric
iron4 D) Increased body iron stores result in increased dietary
ironabsorption
Answer C
28. Which one of the following proteins is the major carrier of
iron inblood?1 A) Albumin2 B) Ferritin3 C) Transcobalamin
4 D) Transferrin
Answer D
29. Iron plays a key functional role for all of the following
proteinsEXCEPT:1 A) Cytochrome oxidase2 B) Hemoglobin3 C) Insulin
receptor 4 D) Myoglobin5Answer C
Case 4Ron Porter is a 53 year old solicitor who presents to his
GP in Mosmanwith mild dyspnoea on exertion and a history suggestive
of angina. There
is no history of blood loss. Results of a full blood count are
given in thetable below. An occult blood test was performed on a
stool specimen andreported to be negative. He is considered for a
blood transfusion.
Indices Mr Porters Results Normal Range
Haemoglobin 75 g/L 130 180 g/L
MCV 65.3 fL 80 100 fL
MCHC 317 g/L 300 350 g/L
White Cell Count 4.7 x 109/L 4.0 11.0 x 109/L
Platelets 426 x 109/L 150 400 x 109/L
19. Which of the following disorders may manifest as
hypochromicmicrocytic anaemia?1 A) Haemolytic anaemia2 B)
Thalassaemia trait
3 C) Liver disease4 D) Acute blood loss
Answer B
20. Which one of the following series of results would be
consistent withiron deficiency?1 A) Increased iron saturation,
elevated serum ferritin, and normalserum transferrin2 B) Normal
serum ferritin, reduced serum iron, and reduced totaliron binding
capacity3 C) Reduced serum ferritin, reduced iron saturation,
andincreased total iron binding capacity4 D) Reduced serum
transferrin and reduced serum transferrinreceptor
Answer CExplanation:A-False: This pattern suggests
haemochromatosis. B-False:This pattern suggests anaemia of chronic
disease.C-True: Thiscombination is typical of iron deficiency.
D-False: Serum transferrin andtransferrin receptor levels are
typically elevated in iron deficiency.
21. Which of the following is correct about iron?1 A) Iron is
more readily absorbed in the ferric (Fe3+) form2 B) Iron absorption
is enhanced in the presence of ascorbate3 C) Transferrin is the
main reservoir of iron in the liver4 D) Ferritin represents the
major circulating form of iron
Answer BExplanation: The ferrous form of iron is more readily
absorbed and iron isstored as ferritin, not transferrin.
Transferrin is the major circulating ironbinding protein .
22. The transfer of oxygen from haemoglobin to the tissues is:1
A) Decreased by 2,3-diphosphoglycerate (2,3-DPG)2 B) Increased at
low pH3 C) Not af fected by the storage of red cel ls at 4oC4 D)
Enhanced by fetal haemoglobin
Answer BExplanation: 2,3-DPG lowers the affinity of haemoglobin
for oxygen,thereby facilitating oxygen delivery to the tissues.
Acidosis (lower pH)lowers the affinity of haemoglobin for oxygen,
resulting in a shift to theright of the haemoglobin oxygen
dissociation curve. The affinity foroxygen is greater in foetal
than in adult haemoglobin.PBL Reference: 4.01, Lecture 1: Role of
haemoglobin in oxygen deliveryto tissues
23. Which one of the following is the most likely cause of
anaemia in MrPorter?1 A) Dietary iron deficiency2 B) Malabsorption3
C) Diverticulitis4 D) Gastrointestinal malignancy
Answer D
24. Which of the following red cell concentrate transfusions
would beincompatible and cause a serious haemolytic transfusion
reaction?1 A) Donor Group O RhD Negative to Patient Group A
RhDPositive2 B) Donor Group A RhD Positive to Patient Group A
RhDNegative3 C) Donor Group AB RhD Positive to Patient Group B
RhDPositive4 D) Donor Group O RhD Positive to Patient Group AB
RhDPositive
Answer C
Most examined material in SBAs
4.01Lec 3 Introduction to anaemia4.01 Lec 4 Iron deficiency4.04
LT1 Microcytosis4.01 LT3 Consequences of deficiency4.05 LT6 Iron
metabolism,4.05 LT7 Tests of iron status in anaemia
-
8/4/2019 4.01 Page Summary - Anaemia
10/11
-
8/4/2019 4.01 Page Summary - Anaemia
11/11