Embed Size (px)
Citation preview

1
www.ncirs.usyd.edu.au
Maternal immunisation and infant
immunisation: core business for GPs
What’s new in 2016?
Peter McIntyre
Director, National Centre for Immunisation Research &
Surveillance
Senior Staff Specialist, Children’s Hospital at Westmead
Professor, University of Sydney
Recommended vaccines
- Free and user pays
Children:
• Free – National Immunisation Program (Commonwealth)
• 18 month pertussis
• Influenza for children with increased risk of severe disease
• User pays - Recommended in Handbook, not in NIP
• Meningococcal B
• Influenza for all children especially those < 5 years
• 2nd dose varicella
Maternal – in pregnancy
• Free - NIP (Commonwealth) – influenza
• Free - funded by State Governments – pertussis
2
Outline
Pertussis and Influenza
• Preventing death/severe disease in children
• Maternal immunisation
• Child immunisation
• Safety monitoring
Meningococcal B
• How much and how severe?
• Meningococcal B vaccine recommendations
3 www.ncirs.usyd.edu.au
Pertussis
4
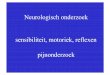
ICD-coded pertussis hospitalisations in infants aged <12
months, Australia, July 1998 - June 2012
0
10
20
30
40
50
60
70
80
90
100
0
50
100
150
200
250
300
350
400
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50
Cu
mu
lati
ve
pe
rce
nta
ge
of
ca
se
s
No
. o
f h
os
pit
alis
ed
ca
se
s
Age at onset (weeks)
First DTPa dose from 6 weeks
Source: AIHW National Hospital Morbidity Database
~30% of hospitalisations
before 6 weeks
Pertussis deaths
and
ICU with
ventilation:
80% < 6 weeks
Strategies to protect infants from severe
disease
Earlier vaccination of infant
• 6 weeks recommended from 2009
• Australian neonatal trial
Vaccination of contacts
• Vaccination of siblings: 18 month dose
• “Cocoon” vaccination of adult contacts
Maternal vaccination
6

2
Unexpected problem: rapid waning of
immunity with acellular pertussis vaccines
Without 18 month booster:
• From 2 years – Australian study (Quinn et al Pediatrics
2014)
With boosters at 18 months and 5-6 years:
• From 7-8 years – US study (Misegades et al JAMA 2013)
Australian study 2010 (NSW)
• Source: siblings 36%, parents 24%
• Most sibling sources aged 3-4 years and vaccinated
Australian study 2015 (WA)
• Source: siblings 51%, parents 32%
• Most sibling sources aged 3-4 years and vaccinated
US study 2015
• Source: siblings 51%, parents 32%
• Mother more important in youngest infants
• Average sibling age ~ 8 years and vaccinated
Source of infection for infants –
siblings and waning immunity
1. Jardine A, et al. CDI 2010; 34:116-21.2. Bertilone C, et al. CDI 2015;38:195-200
3. Skoff et al Pediatrics 2015; 136: 635-41.
www.ncirs.usyd.edu.au
The cocoon strategy
- incomplete cocoons
- incomplete coverage
- incomplete vaccine effectiveness
Deaths from whooping cough
in infants, England, 2001-2012
Sources: lab confirmed cases, certified deaths, Hospital episode statistics, GP registration details
Game changer : Maternal pertussis vaccine
12

3
Case control study – protection against pertussis in
infants under 8 weeks of age – UK
Vaccine effectiveness estimated at 91-93%
• Infants < 8 weeks old
13
California – infants born to vaccinated mothers can
still get pertussis but less severe than in unvaccinated
mothers
www.ncirs.usyd.edu.au
Safety of ante-natal pertussis
vaccination
Reassuring data – studies of 20,000
pregnancies (UK) and 120,000 (US)
dTpa vaccine is recommended as a single dose during the
third trimester of each pregnancy (see refer to 3.3 Groups
with special vaccination requirements). Vaccination during
pregnancy has been shown to be more effective in reducing
the risk of pertussis in young infants than vaccination of the
mother post partum.
Vaccination is recommended with each pregnancy to
provide maximal protection to every infant; this includes
pregnancies which are closely spaced (e.g. <2 years).
March 2015 Pertussis chapter update
Prepared for ATAGI # 57
Optimum timing in pregnancy
• Death in UK when dTpa given < 2 weeks pre-delivery
• Recent evidence that 2nd trimester (from 21 weeks) is
ok and may even be preferable1,2
• Co-administration with influenza vaccine?
• Should be fine, no data
1. AbuRaya Vaccine 2014 2 Eberhardt et al Clin Inf Diseases 2016
UK pertussis deaths post program – no “herd”
protection for infants of non-immunised mothers

4
Coverage, coverage – it’s all about the baby……
www.ncirs.usyd.edu.au
18 m dose
Recommended in Handbook since 2010
Funded from April 2016 (and required for no jab,
no pay)
• Reduce sibling infections
• Should eliminate any concern about lower infant
antibodies post maternal immunisation
AusVaxSafety
National active SMS-based
surveillance
2016 – 2019: Pertussis vaccines
• Children 12 months – 7 years
• Monthly reporting
• AESI: extensive limb swelling
www.ncirs.usyd.edu.au
Influenza
22
0
20
40
60
80
100
120
140
160
180
200
0-5m 6-23m 2-4y 5-11y 12-17y 18-64y ≥65y
Incidence(per 100,000)
Age group
Hospitalisation ICU
Influenza vaccine
not indicated
ICD-coded hospitalisation for influenza 2002–2013
Influenza vaccine fundedonly with risk factors
Vaccine funded for all > 65 years
Children <18y + significant comorbidities x 2 chance of admission to ICU
Deaths per year vs. Years of Life Lost per death 2006-13
24
0.6 1.0 1.7 0.9 0.6
22.4
60.4
81 83 7976
68
37
8
0
10
20
30
40
50
60
70
80
90
0–5m 6–23m 2–4y 5–11y 12–17y 18–64y ≥65y
Nu
mb
er
of
de
ath
s p
er
year
, o
r n
um
be
r o
f Y
LL p
er
case
Average number of deaths per year
Annual number of YLL per case of death
* based on ABS Cause of Death data (influenza being any cause of death)

5
+ = ?
Influenza in pregnancy
2009 Pandemic = 42 ICU admissions and
3 deaths in pregnant women in Australia
Influenza immunisation in pregnancy-it’s all about the baby!
Influenza and pertussis vaccines in pregnancy
– important findings from WA1-4
Safety
• N=2885 women
• 14% self-reported AEFI
• 1.4% medically attended1
• More local reactions with dTpa than influenza
Uptake4
• 35% private O&G; 20% GP; 44% antenatal; 2% private midwife
• Most important reasons not to have flu vaccine:
- not recommended + concern re side effects
• Most important reason to have flu vaccine: “for baby”
1. Regan et al ANZJOG 2014; 2. Regan et al BMC Preg and Childbirth 2015;
3. Regan et al Women and Birth 2016; 4. Regan et al Vaccine 2016
Influenza immunisation for children
Free on NIP for children from 6 months with pre-
disposing illness
• In these children, especially important for all
household members to also receive vaccine
High hospitalisations < 2 years
• < 6 months only preventable by maternal vaccination
• Need 2 doses in first year
• Vaccine effectiveness higher in children
29
RCH Melbourne
Dr Margie Danchin:
Influenza vaccine for kids
April 2016
> 300,000 views
Facebook responses
from parents

6
www.ncirs.usyd.edu.au
Meningococcal B
Uncommon but…..
High severity
31
Significant mortality despite appropriate
treatment
• ~5-10% of cases are fatal2,3
Significant morbidity despite appropriate
treatment
• ~10% of MenB child survivors experience major
sequelae, including limb amputations, seizures
and hearing loss4
• More than 30% of MenB child survivors
experience other deficits such as psychological
disorders, digit amputations and unilateral
hearing loss4
Top image: Courtesy of Centers for Disease Control and Prevention and Dr. Gust. Bottom image: Courtesy of Meningitis Research Foundation UK. Available
at www.meningitis.org.
1. Thompson MJ, et al. Lancet. 2006;367:397-403; 2. Meningococcal meningitis factsheet No 141. World Health Organization website.
http://www.who.int/mediacentre/factsheets/fs141/en/index.html; 3. Rosenstein NE, et al. N Engl J Med. 2001;344:1378-1388; 4. Viner RM, et al. Lancet
Neurol. 2012;11:774-783.
Meningococcal B and C disease compared
33
MenB disease <2 years
10.1
17.218.6
16.8
11.0
6.4 6.2
0.0
5.0
10.0
15.0
20.0
25.0
0-2 3-4 5-6 7-8 9-11 12-17 18-23
Me
an a
nn
ual
no
tifi
cati
on
s p
er
10
0,0
00
pe
rso
n-y
ear
s
Age (months)
Meningococcal vaccines
Serogroup-specific
Registered/ in use in Australia:
• Serogroup C: Meningococcal C (MenC) conjugate vaccine
• Serogroups A/C/W/Y: 4-valent conjugate vaccine
• Serogroups A/C/W/Y: 4-valent polysaccharide vaccine
• Serogroup B: multi-component recombinant MenB vaccine
» NOT capsular polysaccharide
Meningococcal B
– a number of surface proteins associated with
immunity
36
http://f1000.com/prime/reports/m/3/16/fig-002

7
Recombinant multicomponent Meningococcal B vaccine:
4CMenB
37 Source:
McIntosh D. Presented at: 2013 Vaccine Preventable Diseases Conference; April 2013; Dublin, Ireland. Available at:
www.immunisation.ie/en/Conferences/2013VPDConference/PDFFile_17228_en.pdf (accessed Mar 2014)
Registered in
Australia
August 2013
Available on
private
market since
March 2014
4CMenB schedule
Multiple doses
• 4 doses starting @ 2 months
• 3 doses starting @ 6 months
• 2 doses starting > 12 months
38
Age in months
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 …. x x+1 x+2
Young infants
Older infants
Toddlers
Others
3 instead of 4 doses
in infants
Early results of use in
UK look promising for
2 or more doses
4CMenB: Reactogenicity – infants
Systemic reactions in an phase 2 study in infants given 4CMenB at
age 2, 4, 6, and 12 months (concurrent with ‘routine’ vaccines):
40Source of figure: Borrow R. Public Health England. Issues in evaluating the impact of a new meningococcal B vaccine
http://www.slideshare.net/meningitis/issues-in-evaluating-the-impact-of-a-new-meningococcal-b-vaccine
Source of study: Findlow et al. Clin Infect Dis 2010;51:1127-37
Paracetomol recommended
( 3 doses)
Early reactogenicity data
from UK do not suggest
any major problems
Varicella Breakthrough
varicella
2 doses of varicella vaccine are recommended
only one dose is “free”
Breakthrough varicella is usually mild
• can be severe occasionally
• ? increases risk of zoster
• school absence
Second dose is VV alone
• MMR+V at 18 months
• Can give VV @ 12 months with MMR separate
42

8
Summary
Maternal immunisation
Exciting potential to prevent severe disease in infants
less than 6 months of age
High coverage is key
• Partnership with other antenatal care providers
Main motivators for high coverage
• Dr recommendation + baby welfare
Child immunisation
User pays but recommended (influenza, Men B, 2nd
varicella)
• “ask and it shall be given” ….including influenza
• Take opportunities to inform parents 43
Acknowledgements
44
Helen Quinn Kevin Yin
Nick Wood Sanjay Jayasinghe
Frank Beard Cyra Patel
Kristine Macartney Clayton Chiu
Sami Carlson
NCIRS is supported by the Australian Government
Department of Health, the NSW Ministry of Health and the
Sydney Children’s Hospitals Network.