Embed Size (px)
Citation preview

Morphologic Compensatory Mechanisms in the Heart
Peter B. Baker, M.D.

Cardiopulmonary Block Objectives
• Describe the pathologic changes in the cardiac chambers when subjected to a chronic pressure and/or volume load by various causes of heart disease
• Define compensated and decompensated heart disease by pathologic characteristics with particular attention to the ventricles

Specific Lecture Objectives
1. Describe the morphologic features of hypertrophy and dilation at the gross, histologic and ultrastructural levels
2. Define the term “remodel” as it relates to compensatory changes
3. Understand the concept of “compensated” heart disease
4. Describe the features of compensated and decompensated hypertensive heart disease.

Compensatory Changes inCongestive Heart Failure – Hypertrophy
Handout I.B
Remodeling General term that refers to changes in gross and/or
microscopic morphology of the heartHypertrophy
• Increased heart weight and size of myocardial cells in response to pressure or volume overload
• Myofibrils added in parallelPatterns of hypertrophy
Concentric – increased muscle mass with either no change, or small decrease in chamber volume Eccentric – increased muscle mass which develops along with chamber dilation, so there are 2 things going on hypertrophy and dilation

Changes Associated with Myocardial HypertrophyHandout I.B.6
• Altered protein synthesis• Synthesis of abnormal proteins• Fibrosis• Inadequate blood supply due to decreased capillary density • Altered handling of intracellular calciumThese alterations may eventually lead to reduced myocyte contractility
and CHF

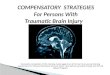
Normal Myocytes Hypertrophic Myocytes

NMy
Mi

Compensatory Changes inCongestive Heart Failure – Dilation
Handout I.C
Dilation• Increase chamber size in response to increase
volume or pressure/volume load• Sarcomeres added in seriesHypertrophy is always present with long-
standing dilationExcessive dilation results in decreased wall
thickness and increased wall tension

Compensated versus DecompensatedHeart Disease
Handout I.D
Compensated – hypertrophy, dilation and physiologic mechanisms are sufficient to maintain cardiac output
Decompensated – compensatory mechanisms no longer provide adequate cardiac output, CHF develops

Patterns of Compensatory Remodeling
Left Ventricle1. Pure pressure overload – concentric hypertrophyExamples - hypertensive heart disease - aortic stenosis2. Pressure and volume overload – eccentric
hypertrophyExamples - mitral / aortic valve insufficiency - ventricular septal defect
3. Regional loss of myocardium – eccentric hypertrophy
Example - healed myocardial infarction

Hypertensive Heart DiseaseHandout II.A
Compensated – left ventricular concentric hypertrophy maintains adequate cardiac output
Decompensated – hypertrophy no longer provides adequate cardiac output due to decreased myocardial contractility, resulting in LV dilation and gradual onset of CHF

LV


LV

Hypertensive Heart DiseaseHandout II.A.2
Compensated Decompensated
Congestive Heart Failure No YesLV Hypertrophy Yes YesLV Dilation No Yes*Increased Heart Weight Yes YesIncreased Heart Dimensions No YesIncrease LV Wall Thickness Yes Yes or NoRV Hypertrophy & Dilation No Yes
*In some patients, marked LV wall stiffness leads to CHF with little ventricular dilation

Key Points
• Morphologic compensatory changes – hypertrophy and dilation and the term “remodeling”
• “Compensated” heart disease• Pathologic features of compensated /
decompensated hypertensive heart disease