Embed Size (px)
Citation preview

AbbreviatioDeep tissue inj* CorrespondE-mail add
j.cathcart@uls1 Tel.: þ1 402 Tel.: þ44 (03 Tel.: þ44 (0
http://dx.doi.0965-206X/ª 2
Journal of Tissue Viability (2015) 24, 51e61
www.elsevier.com/locate/jtv
Basic research
3D anatomy and deformation of theseated buttocks
Sharon Eve Sonenblum a,*, Stephen H. Sprigle b,1,John McKay Cathcart c,2, Robert John Winder d,3
a School of Applied Physiology, Georgia Institute of Technology, 490 10th Street NW,Atlanta, GA 30318, USAb Schools of Applied Physiology and Industrial Design, Georgia Institute of Technology,490 10th Street NW, Atlanta, GA 30318, USAc School of Health Sciences, University of Ulster, Shore Road, Jordanstown,Newtownabbey, County Antrim BT38 0QB, Northern Ireland, United Kingdomd Institute of Nursing and Health Research, School of Health Sciences, University ofUlster, Shore Road, Newtownabbey BT37 0QB, United Kingdom
KEYWORDSMRI;Sitting;Anatomy;Tissue deformation;Pressure ulcer
ns: SCI, spinal cord injuury.ing author. Tel.: þ1 40resses: sharon.sonenbter.ac.uk (J.M. Cathc4 385 4302; fax: þ1 404) 2890368192.) 2890368440.
org/10.1016/j.jtv.2015.015 Tissue Viability Soc
Abstract Aim: To describe the 3D anatomy and deformation of the buttocks dur-ing sitting.Materials and methods: The buttocks of 4 able-bodied individuals and 3 individualswith spinal cord injury were scanned sitting in a FONAR Upright MRI. T1-weightedFast Spin Echo scans were collected with the individuals seated on a custom wheel-chair cushion to unload the ischial tuberosities (ITs) and seated on a 3 inch foamcushion. Multi-planar scans were analyzed, and the muscle, bone and adipose tissuewas manually segmented for 3D rendering and analysis of the quantity, geometry,and location of tissues.Results: The gluteus maximus was positioned lateral and posterior to the IT,covering the inferior portion of the IT for only 2 able-bodied participants. Adiposethickness directly under the IT did not differ by diagnosis, nor did it have a consis-tent response to loading. However, the envelopment of the IT by the surroundingadipose tissue was much greater in two of the participants with spinal cord injuries.These two subjects also had the most curved skin surface as the tissue wrapped
ry; IT, ischial tuberosity; FE, finite element; GM, gluteus maximus; ROI, region of interest; DTI,
4 385 0633; fax: þ1 404 894 [email protected] (S.E. Sonenblum), [email protected] (S.H. Sprigle),art), [email protected] (R.J. Winder).894 9320.
03.003iety. Published by Elsevier Ltd. All rights reserved.

52 S.E. Sonenblum et al.
around the IT. Tissue strains around the ischium were most visible in the adiposeand connective tissue. The gluteus maximus displaced and distorted upwards, pos-terior and lateral, away from the inferior IT.Conclusions: Multi-planar imaging is necessary to investigate anatomy and defor-mation of the buttocks. 5 out of 7 participants did not sit directly on muscle.The tissue beneath their ITs was predominantly composed of fat and connective tis-sue, suggesting that these tissues might be most vulnerable to injury.ª 2015 Tissue Viability Society. Published by Elsevier Ltd. All rights reserved.
1. Background
Sitting for extended periods is common acrossmany populations, with reports of healthy adultssitting for more than 6 h per day [1,2]. But forindividuals who use wheelchairs as their primarymobility device, sitting times have been measuredas upwards of 10e12 h per day [3e5]. These in-dividuals typically have reduced mobility andsensation, and therefore they are at increased riskof tissue breakdown and pressure ulcer develop-ment. In fact, more than 50% of individuals withspinal cord injury (SCI) experience skin breakdownat some point in their lives [6e8], adverselyimpacting their quality of life [9,10], andburdening the health care system with significanttreatment costs [11].
Pressure ulcers, by definition, result fromlocalized tissue loading that causes a series ofpathophysiological responses to deformation. Theprecise mechanisms by which internal loading andphysiological responses lead to pressure ulcers(PUs) are not known, however current evidencesuggests that damage can result directly from thedeformation [12,13], or from impairment to bloodflow caused by deforming tissue under load[14,15]. Individuals with SCI can exhibit muchgreater deformation during sitting due to changesto buttocks tissue mass and compliance [16e19].The range of tissue properties in persons with SCImay, in fact, reflect a spectrum of PU risk withinthis high-risk group.
In Sonenblum et al. [20], we introduced theconcept of Deformation Resistance. “DeformationResistance can be defined as the intrinsic charac-teristic of an individual’s soft tissues to withstandextrinsic applied forces.” In order to develop amethod for measuring Deformation Resistance,and later determining individualized risk, we firstneed to understand the loaded anatomy, as well asthe types of deformations experienced duringsitting.
An understanding of buttocks tissue deforma-tion during sitting is also important for supporting
Finite Element (FE) analyses of the buttocks. FEanalysis is a powerful computational tool that canfacilitate investigation of more conditions thanpossible with direct measurement. Furthermore, itis a tool that can assist in estimating tissue’s me-chanical properties and identifying the individualparameters that have the greatest influence on anindividual’s Deformation Resistance. FE has beenapplied to characterize sitting mechanics andevaluate wheelchair cushion designs [17,21e30].Unfortunately, FE models present in the literaturedo not reflect actual variations in buttocks anat-omy because that information is not available inthe literature, thereby limiting the external val-idity of existing FE models. Furthermore, valida-tion of existing FE models requires a complete 3Dassessment of deformation under load, which hasnot been studied.
Therefore, the overall objective of this paperwas to describe the 3D anatomy and deformationof the buttocks during sitting. The projectemployed 3D, seated Magnetic Resonance Imaging(MRI) and image segmentation and analysis of 7individuals’ buttocks to describe the 3D shape,size, location and distribution of tissue underneaththe pelvis, and to determine how these changedbetween an unloaded condition and seated onfoam.
2. Methods
2.1. Subjects
We sought to study a small but diverse subset ofindividuals. The 7 subjects, described in Table 1 (4able-bodied and 3 subjects with a spinal cordinjury) were recruited for their diversity, conve-nience, and availability. Only one of the partici-pants, Subject G, had a history of pelvic pressureulcers (contralateral to the imaged side). Institu-tional Review Board approval was received fromthe local institution and informed consent wasacquired from the recruited participants.

Table 1 Subject characteristics.
Subject ID Gender Age Weight (lbs) Diagnosis Unloading method
A F 32 115 a/b Contoured foam cutoutB M 52 209 a/b Contoured foam cutoutC M 53 185 a/b Contoured foam cutoutD F 23 117 a/b Thigh supportE M 18 105 SCI e C6/C7 Complete Thigh supportF M 43 190 SCI e T12 Incomplete Thigh supportG M 56 260 SCI e T12 Complete Contoured foam cutout
3D anatomy and deformation of the seated buttocks 53
2.2. Test environment
Participants were scanned in two seated condi-tions: an “IT Unloaded” posture and seated on flatfoam. In the “IT Unloaded” condition, all surfacecontact and normal loading were removed fromthe ischial tuberosities (ITs), but other parts of theneighboring tissue were loaded as necessary tomanage the subjects’ body weight in a seatedposture. Subjects A, B, C, and G were scanned on acontoured foam cutout, which unloaded the ITsbut supported the body weight on the greatertrochanters. Subjects D, E, and F were supportedby a stiff foam underneath the thighs, which off-loaded both the ITs and the trochanters.
For the loaded condition, participants werescanned while seated on a piece of 300 flat foam(high resilience 45 indentation load deflection(ILD) foam). This foam is commonly used in seatand wheelchair cushions and was selected to pro-vide a stable sitting surface during the loadedscan. Able-bodied subjects sat themselves on therelevant cushion. Participants with SCI transferredinto an MRI-compatible transfer chair (Fig. 1) fortransport into the scanner area and up the ramp,
Fig. 1 MRI compatible tools to assist with transfer into thplatform, and grab bar in the scanner. C) “IT Unloaded” custhat also unloads the greater trochanters.
and then transferred onto the cushion. Seatedstability was augmented from the lateral proximityof the MRI magnets as well as a horizontal supportbar positioned in front of the subject on whichthey could rest their arms.
2.3. Scan protocol
The scans were collected using a T1-weighted FastSpin Echo protocol previously described in Ref.[20]. Scans included 60 contiguous sagittal slices of3 mm thickness, and a 350 mm field of view.
2.4. Data processing
Raw DICOM scans were imported into Analyze AVWv11.0 for review and segmentation of the pelvis,gluteus maximus (GM), and subcutaneous fat.Semi-automated segmentation was performedunder the supervision of an experienced radiogra-pher (JC). Segmentation of tissue on scans of thisresolution does not allow for separate segmenta-tion of skin, so the skin is included within thesubcutaneous fat segmentation when visible. Pointclouds of the 3D segmented surfaces of the bones,
e Upright scanner. A) Elevating transfer chair. B) Ramp,hion with a contoured cutout. D) “IT Unloaded” cushion

54 S.E. Sonenblum et al.
muscles, and fat were exported for further anal-ysis in Matlab 14.0.
2.5. Data analysis
Analysis was completed in Analyze 11.0 (review,registration, and muscle properties) and MatlabR2014a (remaining measurements). In order todescribe the anatomy of the buttocks duringsitting, we performed multi-planar qualitative re-view of the scans. The “IT Unloaded” and foamscans were manually registered in 3D to align thepelvises for comparison. The volume and surfacearea of the segmented GM was exported fromAnalyze 11.0. Additionally, we identified the tissuewithin two regions of interest (ROI) underneath thepeak of the IT, defined as the lowest point of theischium (Fig. 2). The ROI were vertical cylinderswith diameters of 50 mm and 10 mm. The 50 mmROI was selected based upon the size (approxi-mately 50 mm long) and anterio-lateral orientationof the IT [31,32]. The percent of gluteus coverage(%GlutCoverage) was defined as the percent of the50 mm ROI covered by at least 2 mm of GM. Theradius of curvature of the superficial skin surfacewithin the 50 mm ROI was calculated in the sagittaland coronal planes. The best fit radius of curvatureof a contour was computed using a least squares fitto identify the center of the best fit circle, wherethe inverse of the radius was the radius of curva-ture [33]. The average tissue thickness underneaththe peak of the IT was measured in the 10 mmregion.
3. Results
Coronal and Sagittal MRI images for each of 7subjects seated on foam illustrate the wide varietyin seated buttocks anatomy (Fig. 3). The sagittal
Fig. 2 The 50 mm region of interest (ROI) includes the mosROI describes the region just beneath the peak of the IT.(inferior medial views) to describe what region of the pelvis
views show the ischium projecting inferior fromthe acetabulum. Slight differences in the ischialprojection may be attributed to slight differencesin pelvic tilt or anatomical variation. The sagittalviews highlight the anterior-posterior projection ofthe GM (highlighted in red) and the hamstrings andadductor magnus which originate from the anterioraspect of the ischium. Both views highlight dif-ferences in the location of the GM and differencesin the thickness of the skin and subcutaneous tis-sue underneath the IT.
3.1. Gluteus maximus
The GM varied considerably in volume across the 7subjects, with a mean (SD) of 677 cm3 (325 cm3)(Table 2). The able-bodied male subjects (B & C)had the greatest muscle volume. Respective vol-umes of two able-bodied women and two men withSCI (subjects D & F and subjects A & E) were alsosimilar. Subject G showed considerable atrophywith a muscle volume 60% less than other subjects.The surface areas of the GM were highly correlatedwith the volumes (correlation coefficient ¼ 0.958,p < 0.001), and averaged 751 cm2 (157 cm2).Muscle shape varied considerably, including athick, flat gluteus (e.g., Subject B), very thin,highly atrophied gluteus (Subject G), and somemore curved glutei that wrapped around the femur(Subjects E, F) (Fig. 3).
The GM was typically positioned lateral andposterior to the IT, although the location of theGM varied widely across the 7 subjects, and itsposition did not appear to be a function of themuscle volume. In both the “IT Unloaded” andloaded conditions, Subjects A and C presentedwith an appreciable amount of the IT covered bythe GM. In both subjects, sitting on foam dis-placed the GM away from the IT, reducing the GMcoverage from 97% to 48% for Subject A and 87% to
t heavily loaded tissue underneath the IT, and the 10 mmThe 50 mm ROI is also highlighted in red on the pelvisis included in the ROI.

Fig. 3 Coronal and sagittal views of the seated buttocks (on foam). Gluteus maximus is highlighted in red.L ¼ lateral, M ¼ medial, P ¼ posterior, A ¼ anterior.
3D anatomy and deformation of the seated buttocks 55
64% for Subject C. Subjects B, D, and E had min-imal IT coverage with none of the muscle wrap-ping underneath the ITs’ most inferior aspectwithin the 10 mm ROI (Table 2). Subject E was theonly subject with SCI who exhibited any ischialcoverage by the GM.
Fig. 4 displays a 3D rendering of the segmentedgluteus maximus and pelvis in order to illustratethe relationship between the GM and ischium forSubjects C and G seated on foam. In Subject C, anable-bodied male, the GM covers the body of theischium including the tuberosity and is largelypositioned posteriorly and lateral to that bonyprominence. The GM of Subject G, a male with SCI,rests entirely posterior and lateral to the ischium.It is not loaded by the ischium as he sits upon thefoam cushion.
3.2. Adipose tissue and skin
As with the GM, considerable variation wasobserved in the quantity and distribution of sub-cutaneous fat under load. Fat and skin thicknessdirectly under the peak of the IT averaged 13 mm
Table 2 Properties of the gluteus maximus (GM), and qu
Subject GM voume(cm3)
GM surfacearea (cm2)
% GluteusCoverage
IT unloaded Foa
A 466 656 97 48B 1116 940 4 3C 1119 969 87 64D 662 691 19 17E 452 612 5 7F 635 808 0 0G 292 578 0 0Mean 677 751 30 20StandardDeviation
325 157 43 26
(9 mm) (Table 2), but Subject B was the only per-son with a thickness greater than 15 mm. Theaverage loaded thickness was 10 mm for the othersix subjects. The shape of the skin under theischium in both seated conditions is described bythe radius of curvature (Fig. 5). When seated onfoam, the radii of curvature of Subjects A & Bincreased (i.e., became flatter). In distinction, theother subjects exhibited a decrease in the radii ofcurvature when the buttocks was loaded. That is,their tissue conformed around the ischium andformed a more curved shape compared to the ITunloaded condition. Subjects F and G, the two menwith T12 spinal cord injuries, had the smallestradius of curvature, or the sharpest curved skinwhen seated on foam.
The envelopment of the IT by the surroundingadipose tissue also varied across subjects. The 3Drenderings in Fig. 6 illustrate the differences inthree subjects. The adipose tissue is separatedfrom the bone by a variety of tissue types andquantities while seated (Fig. 3). For Subject B, theadipose tissue is separated from the bone bymuscle, connective tissues, and fat deposits in
antity of muscle and fat underneath the IT.
Avg fat thicknessin 10 mm ROI (mm)
Average GM thicknessin 10 mm ROI (mm)
m IT unloaded Foam IT unloaded Foam
14 13 17 059 32 0 08 7 21 8
18 10 0 015 15 0 06 11 0 0
30 6 0 021 14 6 118 9 9 3

Fig. 4 Positioning of the gluteus maximus (blue) rela-tive to the ischium (white) for Subjects C and G. Thefemur is also shown. Hidden bone is outlined in red,hidden muscle is outlined in blue.
56 S.E. Sonenblum et al.
between the sheaths of the muscle groups,resulting in a relatively flat layer of adipose tissue,while Subjects F and G have very little muscletissue between the bone and adipose. As a result,the adipose wraps closely around the ischium.
3.3. Deformation
Multi-planar comparisons of two males with similarlevels of spinal cord injury (Subjects F and G) offer
Fig. 5 Radius of curvature of
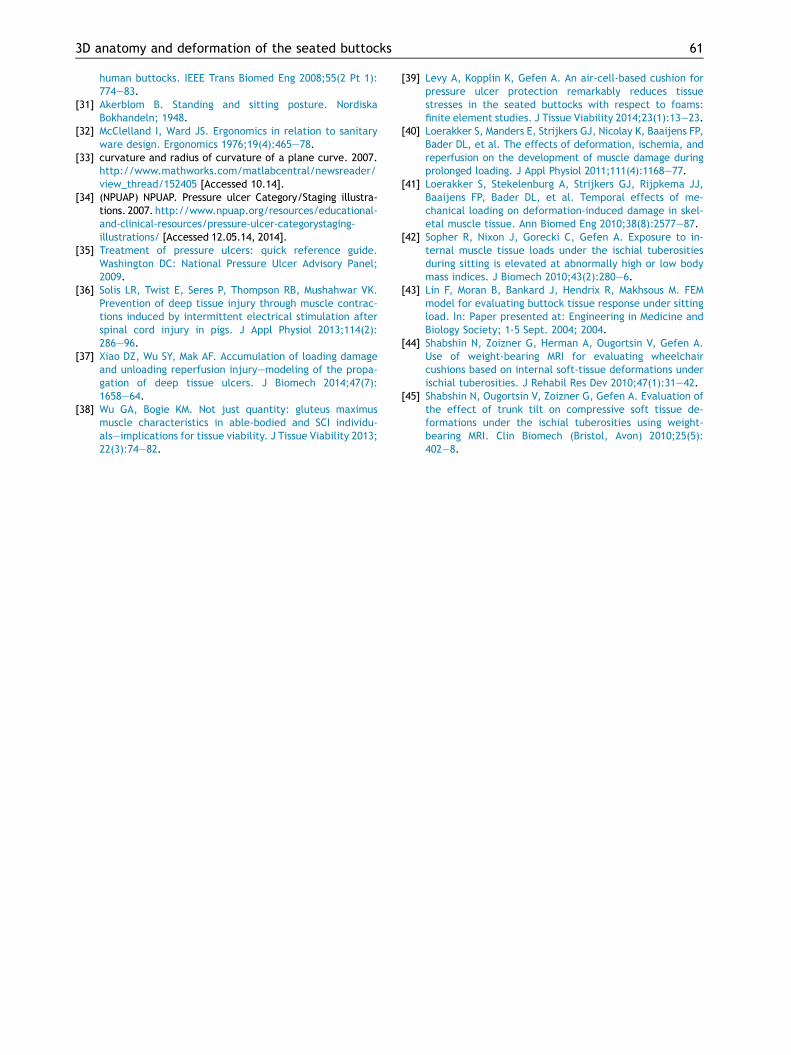
insight into the internal strains experienced by thebuttocks tissue while sitting (Figs. 7 and 8). Bothsubjects experienced a significant change in shapeof the tissue, especially the visceral fat and musclesurrounding the IT. Interestingly, the skin and fatdirectly beneath the IT of Subject F did notnoticeably change between the two loading con-ditions, whereas Subject G experienced consider-able vertical displacement underneath the IT. Yet,despite this lack of linear change in subcutaneousfat, Subject F experienced considerable deforma-tion in the tissue surrounding the IT, as visible bythe significant change in tissue shape in the coro-nal view (Fig. 7). The hip extensor and adductormuscles of Subject G are highly atrophied, andtheir space is filled with highly deformable adiposetissue anterior to the ischium (Fig. 8, Vfat). Thechange in projection of the common hamstringinsertion (Fig. 8, HST) to a slightly more superiorposition from the prominence of the IT, is consis-tent with strain of the tissue around the ischium.
As mentioned previously, the dark spacesbeneath the ischium are connective tissue andindicate these structures are directly loaded dur-ing sitting. These regions may experience defor-mation as well, but it is difficult to quantify at thisresolution.
With respect to the GM, deformation is charac-terized by both displacement and distortion of themuscle. Subjects’ muscles were displaced awayfrom the peak of the IT. Specifically, Subject F ex-hibits deformation to the inferior portion to of themuscle, which is displaced upwards. The inferior
the skin under the ischium.
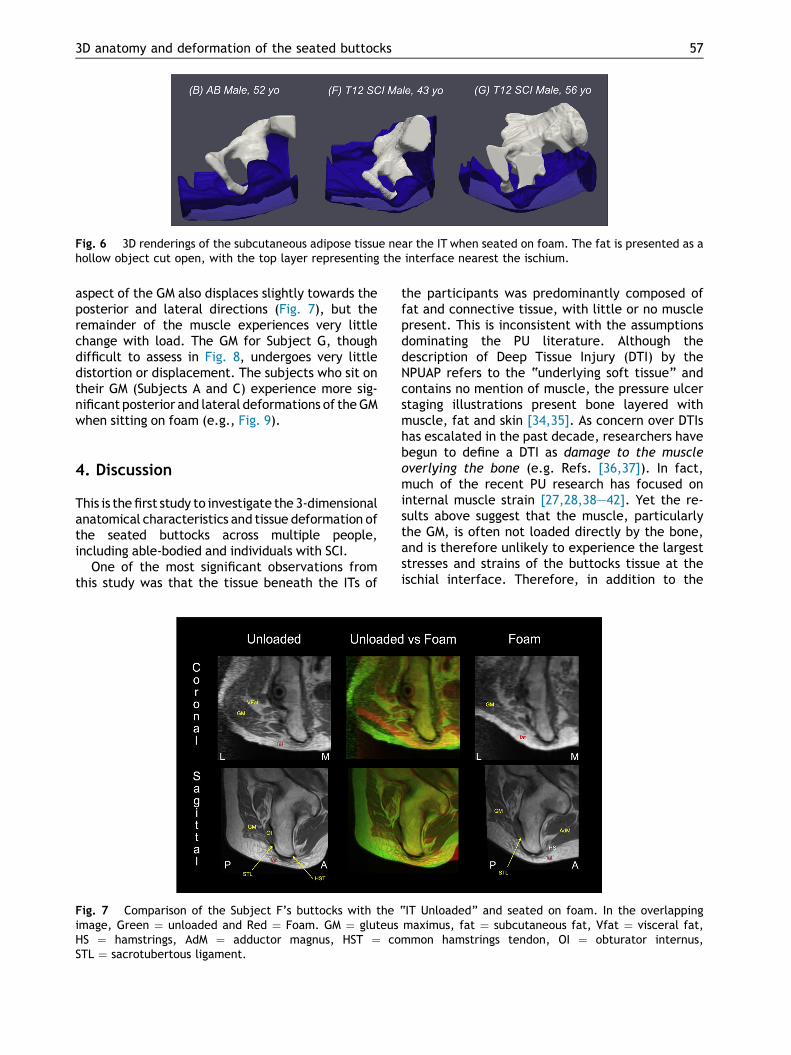
Fig. 6 3D renderings of the subcutaneous adipose tissue near the IT when seated on foam. The fat is presented as ahollow object cut open, with the top layer representing the interface nearest the ischium.
3D anatomy and deformation of the seated buttocks 57
aspect of the GM also displaces slightly towards theposterior and lateral directions (Fig. 7), but theremainder of the muscle experiences very littlechange with load. The GM for Subject G, thoughdifficult to assess in Fig. 8, undergoes very littledistortion or displacement. The subjects who sit ontheir GM (Subjects A and C) experience more sig-nificant posterior and lateral deformations of theGMwhen sitting on foam (e.g., Fig. 9).
4. Discussion
This is the first study to investigate the 3-dimensionalanatomical characteristics and tissue deformation ofthe seated buttocks across multiple people,including able-bodied and individuals with SCI.
One of the most significant observations fromthis study was that the tissue beneath the ITs of
Fig. 7 Comparison of the Subject F’s buttocks with theimage, Green ¼ unloaded and Red ¼ Foam. GM ¼ gluteusHS ¼ hamstrings, AdM ¼ adductor magnus, HST ¼ coSTL ¼ sacrotubertous ligament.
the participants was predominantly composed offat and connective tissue, with little or no musclepresent. This is inconsistent with the assumptionsdominating the PU literature. Although thedescription of Deep Tissue Injury (DTI) by theNPUAP refers to the “underlying soft tissue” andcontains no mention of muscle, the pressure ulcerstaging illustrations present bone layered withmuscle, fat and skin [34,35]. As concern over DTIshas escalated in the past decade, researchers havebegun to define a DTI as damage to the muscleoverlying the bone (e.g. Refs. [36,37]). In fact,much of the recent PU research has focused oninternal muscle strain [27,28,38e42]. Yet the re-sults above suggest that the muscle, particularlythe GM, is often not loaded directly by the bone,and is therefore unlikely to experience the largeststresses and strains of the buttocks tissue at theischial interface. Therefore, in addition to the
“IT Unloaded” and seated on foam. In the overlappingmaximus, fat ¼ subcutaneous fat, Vfat ¼ visceral fat,mmon hamstrings tendon, OI ¼ obturator internus,

Fig. 8 Comparison of the Subject G’s buttocks with the “IT Unloaded” and seated on foam. In the overlappingimage, Green ¼ unloaded and Red ¼ Foam. GM ¼ gluteus maximus, fat ¼ subcutaneous fat, Vfat ¼ visceral fat,HST ¼ common hamstrings tendon, STL ¼ sacrotubertous ligament.
58 S.E. Sonenblum et al.
current efforts to study muscle, PU researchshould address the loading on fat and connectivetissue as tissues that may herald necrosis duringDTI formation.
In addition to informing the future direction ofpressure ulcer research, these results indicate thatprevious studies of buttocks tissue strain, partic-ularly those utilizing finite element models of thebuttocks need to be interpreted with caution withrespect to generalizability. The published models
Fig. 9 Comparison of Subject C’s buttocks with the “IT UnGreen ¼ unloaded and Red ¼ Foam. GM ¼ gluteus maHS ¼ hamstrings, AbM ¼ abductor magnus, HST ¼ coSTL ¼ sacrotubertous ligament.
frequently reflect the anatomy of Subject C,whose GM is directly loaded by the ischial tuber-osity [21,25,39,42,43]. This anatomical presenta-tion was found to be in the minority and wasinconsistent with the anatomy of many of oursubjects. In the very least, the anatomical varia-tion identified in this study indicates that the tis-sues exposed to high stresses under the ischium donot involve significant muscle in 5 of the 7 subjectsscanned. Furthermore, the deformations observed
loaded” and seated on foam. In the overlapping image,ximus, fat ¼ subcutaneous fat, Vfat ¼ visceral fat,mmon hamstrings tendon, OI ¼ obturator internus,

3D anatomy and deformation of the seated buttocks 59
in fat indicate a wide range of stiffnesses acrossindividuals, and computational models mustreflect those differences.
As this is the first study to fully investigate the3D anatomy and deformation of the seated but-tocks, there are few studies available for com-parison of results. However, the results stronglysupport the need to use multi-planar analyses toinvestigate buttocks anatomy and deformation.Related studies investigated the tissue thicknessdirectly under the peak of the IT during sitting[44,45]. While fat thickness under the peak of theIT was similar to measurements in the presentstudy, the previous studies reported an average of8.2 mm of muscle under the peak of the IT. This isinconsistent with our findings, as 5 of 7 partici-pants had no gluteus muscle present directlybeneath the peak of the IT (in the 10 mm ROI)when unloaded (Table 2). Although the source ofthe discrepancy is unknown, our results did showthat analyzing a single slice of data hinders theability to identify tissues accurately. We relied onmulti-planar analysis to identify the anatomy.Furthermore, it is important to note thatmeasuring tissue thickness underneath the IT pro-vides an incomplete assessment of the buttocksanatomy in sitting. For example, Table 2 showsthat Subjects C and G have similar thicknesses offat directly under the peak of the IT when seatedon foam (7 and 6 mm, respectively), but the dis-tribution of that fat was very different for the twosubjects (Figs. 9 and 8, respectively). One addi-tional related study found GM volumes and dif-ferences in volume between able-bodiedindividuals and persons with SCI consistent withthe results presented above [38].
Although the present study was not designed toquantify Deformation Resistance, it illustrates thedifferences in Deformation Resistance across in-dividuals. The 3 subjects with SCI showed adisparate response to loading. Subject E demon-strated a Deformation Resistance that was similarto the 4 able-bodied subjects. On the other hand,the latter two participants with SCI appear to havemuch less Deformation Resistance than the able-bodied participants. Both Subjects F and G havevery highly curved tissue (i.e., low radius of cur-vature) while seated on flat foam. They also bothpresent with subcutaneous adipose tissue thatwraps around the ischium in response to loading,as compared with Subject B whose adipose tissueremains supported by internal structures andmaintains its shape. It can be inferred that theshear stresses and strains experienced by SubjectsF and G are considerably greater than thoseexperienced by other subjects, who experience
more uniform deformation of the adipose tissue.Clinically speaking, Subject B has a high Defor-mation Resistance, and appears as if he can sit on acushion support surface with limited risk to histissue. Subject G, who has a history of recurrentpressure ulcers (at the contralateral IT), experi-ences highly non-uniform tissue deformation,which is consistent with a high risk for tissuebreakdown. His cushion prescription and pressurerelief regimen need to reflect that increased risk.
4.1. Limitations
This study measured 7 seated individuals. Quanti-tative descriptions of complex tissue strains arenecessary to augment the results of this study, andare planned for future work. This study was limitedto only a single loaded surface (foam) and did notinvestigate the deformations experienced ondifferent cushions, nor did it investigate the in-fluence of varied postures. It is likely that pelvictilt (i.e., slouching versus sitting upright) will havea significant impact on the seated anatomy andtissue deformation because load will be trans-ferred from the bony skeleton to the soft tissuesdifferently. The influence of pelvic posture shouldbe investigated. Unfortunately, controlling posturein the FONAR upright scanner is challenging due tothe narrow space. Furthermore, complete off-loading of the buttocks while seated is problem-atic, because the body weight must be supportedsomehow. In this study we balanced the need forpostural stability throughout the scan with theneed to offload the tissue under the ischia andcoccyx. However, it is possible that tissue sur-rounding the IT experienced loading. Additionally,an expanded population including individuals whoare African-American and women with SCI is alsoneeded to improve our understanding of variationin seated buttocks anatomy and deformation. Withregards to the analysis method, manual segmen-tation is always subject to variation and user error.For this study, we addressed segmentation con-cerns by having all segmentations reviewed by anexpert, and by intentionally selecting measure-ments that were not highly sensitive to changes insegmentation. However, a more automated seg-mentation would be a valuable addition to theprocessing approach.
5. Conclusions
This study illustrated the importance of usingmulti-planar imaging to investigate anatomy anddeformation of the buttocks. Multi-planar imaging

60 S.E. Sonenblum et al.
provided the surprising result that only 2 out of 7participants had appreciable amounts of muscleunderneath their ischial tuberosities. The tissuebeneath their ITs was predominantly composed offat and connective tissue, suggesting that thesetissues might be most vulnerable to injury.
Conflicts of interest
None.
References
[1] Raijmakers BG, Nieuwenhuizen MG, Beckerman H, deGroot S. Differences in the course of daily activity levelbetween persons with and without chronic pain. Am J PhysMed Rehabil/Assoc Acad Physiatr 2015 Feb;94(2):101e9.
[2] Jancey J, Tye M, McGann S, Blackford K, Lee AH. Appli-cation of the occupational sitting and physical activityquestionnaire (OSPAQ) to office based workers. BMC publichealth 2014;14:762.
[3] Sonenblum SE, Sprigle S, Lopez RA. Manual wheelchair use:bouts of mobility in everyday life. Rehabil Res Pract 2012;2012:753165.
[4] Sonenblum SE, Sprigle S, Harris FH, Maurer CL. Charac-terization of power wheelchair use in the home and com-munity. Archives Phys Med Rehabil 2008;89(3):486e91.
[5] Sonenblum SE, Sprigle S. Distinct tilting behaviours withpower tilt-in-space systems. Disabil Rehabil Assist Technol2011;6(6):526e35.
[6] Salzberg CA, Byrne DW, Cayten CG, Kabir R,van Niewerburgh P, Viehbeck M, et al. Predicting andpreventing pressure ulcers in adults with paralysis. AdvWound Care 1998;11(5):237e46.
[7] Raghavan P, Raza WA, Ahmed YS, Chamberlain MA. Prev-alence of pressure sores in a community sample of spinalinjury patients. Clin Rehabil 2003;17(8):879e84.
[8] Krause JS, Broderick L. Patterns of recurrent pressure ul-cers after spinal cord injury: identification of risk andprotective factors 5 or more years after onset. Arch PhysMed Rehabil 2004;85(8):1257e64.
[9] Clark FA, Jackson JM, Scott MD, Carlson ME, Atkins MS,Uhles-Tanaka D, et al. Data-based models of how pressureulcers develop in daily-living contexts of adults with spinalcord injury. Arch Phys Med Rehabil 2006;87(11):1516e25.
[10] Langemo DK, Melland H, Hanson D, Olson B, Hunter S. Thelived experience of having a pressure ulcer: a qualitativeanalysis. Adv Skin Wound Care 2000;13(5):225e35.
[11] Chan BC, Nanwa N, Mittmann N, Bryant D, Coyte PC,Houghton PE. The average cost of pressure ulcer man-agement in a community dwelling spinal cord injury pop-ulation. Int Wound J 2013;10(4):431e40.
[12] Bouten CV, Breuls RG, Peeters EA, Oomens CW, Baaijens FP.In vitro models to study compressive strain-induced musclecell damage. Biorheology 2003;40(1e3):383e8.
[13] Gawlitta D, Li W, Oomens CW, Baaijens FP, Bader DL,Bouten CV. The relative contributions of compression andhypoxia to development of muscle tissue damage: anin vitro study. Ann Biomed Eng 2007;35(2):273e84.
[14] Sanada H, Nagakawa T, Yamamoto M, Higashidani K,Tsuru H, Sugama J. The role of skin blood flow in pressure
ulcer development during surgery. Adv Wound Care 1997;10(6):29e34.
[15] van Marum RJ, Meijer JH, Ribbe MW. The relationship be-tween pressure ulcers and skin blood flow response after alocal cold provocation. Arch Phys Med Rehabil 2002;83(1):40e3.
[16] Castro MJ, Apple Jr DF, Hillegass EA, Dudley GA. Influenceof complete spinal cord injury on skeletal muscle cross-sectional area within the first 6 months of injury. Eur JAppl Physiol Occup Physiol 1999;80(4):373e8.
[17] Linder-Ganz E, Shabshin N, Itzchak Y, Yizhar Z, Siev-Ner I,Gefen A. Strains and stresses in sub-dermal tissues of thebuttocks are greater in paraplegics than in healthy duringsitting. J Biomech 2008;41(3):567e80.
[18] Makhsous M, Venkatasubramanian G, Chawla A, Pathak Y,Priebe M, Rymer WZ, et al. Investigation of soft-tissuestiffness alteration in denervated human tissue using anultrasound indentation system. J Spinal Cord Med 2008;31(1):88e96.
[19] Sprigle S, Sonenblum S, Conner-Kerr T. mobilityRERC stateof the science conference: individualizing pressure ulcerrisk and prevention strategies. Disabil Rehabil AssistTechnol 2013;8(6):454e61.
[20] Sonenblum SE, Sprigle SH, Cathcart JM, Winder RJ.3-dimensional buttocks response to sitting: a case report.J Tissue Viability 2013 Feb;22(1):12e8. http://dx.doi.org/10.1016/j.jtv.2012.11.001 [Epub 2012 Dec 23].
[21] Linder-Ganz E, Shabshin N, Itzchak Y, Gefen A. Assessmentof mechanical conditions in sub-dermal tissues duringsitting: a combined experimental-MRI and finite elementapproach. J Biomech 2007;40(7):1443e54.
[22] Grujicic M, Pandurangan B, Arakere G, Bell WC, He T, Xie X.Seat-cushion and soft-tissue material modeling and a finiteelement investigation of the seating comfort for passenger-vehicle occupants. Mater Des 2009;30(10):4273e85.
[23] Linder-Ganz E, Gefen A. Stress analyses coupled withdamage laws to determine biomechanical risk factors fordeep tissue injury during sitting. J Biomech Eng 2009;131(1):011003.
[24] Then C, Menger J, Benderoth G, Alizadeh M, Vogl TJ,Hubner F, et al. Analysis of mechanical interaction be-tween human gluteal soft tissue and body supports.Technol Health Care 2008;16(1):61e76.
[25] Makhsous M, Lim D, Hendrix R, Bankard J, Rymer WZ, Lin F.Finite element analysis for evaluation of pressure ulcer onthe buttock: development and validation. IEEE TransNeural Syst Rehabil Eng 2007;15(4):517e25.
[26] Verver MM, van Hoof J, Oomens CW, Wismans JS,Baaijens FP. A finite element model of the human buttocksfor prediction of seat pressure distributions. ComputMethods Biomech Biomed Eng 2004;7(4):193e203.
[27] Loerakker S, Solis LR, Bader DL, Baaijens FP,Mushahwar VK, Oomens CW. How does muscle stiffnessaffect the internal deformations within the soft tissuelayers of the buttocks under constant loading? ComputMethods Biomech Biomed Eng 2013;16(5):520e9.
[28] Loerakker S, Bader DL, Baaijens FP, Oomens CW. Whichfactors influence the ability of a computational model topredict the invivodeformationbehaviourof skeletalmuscle?Comput Methods Biomech Biomed Eng 2013;16(3):338e45.
[29] Linder-Ganz E, Yarnitzky G, Yizhar Z, Siev-Ner I, Gefen A.Real-time finite element monitoring of sub-dermal tissuestresses in individuals with spinal cord injury: towardprevention of pressure ulcers. Ann Biomed Eng 2009;37(2):387e400.
[30] Wagnac EL, Aubin CE, Dansereau J. A new method togenerate a patient-specific finite element model of the
3D anatomy and deformation of the seated buttocks 61
human buttocks. IEEE Trans Biomed Eng 2008;55(2 Pt 1):774e83.
[31] Akerblom B. Standing and sitting posture. NordiskaBokhandeln; 1948.
[32] McClelland I, Ward JS. Ergonomics in relation to sanitaryware design. Ergonomics 1976;19(4):465e78.
[33] curvature and radius of curvature of a plane curve. 2007.http://www.mathworks.com/matlabcentral/newsreader/view_thread/152405 [Accessed 10.14].
[34] (NPUAP) NPUAP. Pressure ulcer Category/Staging illustra-tions. 2007. http://www.npuap.org/resources/educational-and-clinical-resources/pressure-ulcer-categorystaging-illustrations/ [Accessed 12.05.14, 2014].
[35] Treatment of pressure ulcers: quick reference guide.Washington DC: National Pressure Ulcer Advisory Panel;2009.
[36] Solis LR, Twist E, Seres P, Thompson RB, Mushahwar VK.Prevention of deep tissue injury through muscle contrac-tions induced by intermittent electrical stimulation afterspinal cord injury in pigs. J Appl Physiol 2013;114(2):286e96.
[37] Xiao DZ, Wu SY, Mak AF. Accumulation of loading damageand unloading reperfusion injuryemodeling of the propa-gation of deep tissue ulcers. J Biomech 2014;47(7):1658e64.
[38] Wu GA, Bogie KM. Not just quantity: gluteus maximusmuscle characteristics in able-bodied and SCI individu-alseimplications for tissue viability. J Tissue Viability 2013;22(3):74e82.
[39] Levy A, Kopplin K, Gefen A. An air-cell-based cushion forpressure ulcer protection remarkably reduces tissuestresses in the seated buttocks with respect to foams:finite element studies. J Tissue Viability 2014;23(1):13e23.
[40] Loerakker S, Manders E, Strijkers GJ, Nicolay K, Baaijens FP,Bader DL, et al. The effects of deformation, ischemia, andreperfusion on the development of muscle damage duringprolonged loading. J Appl Physiol 2011;111(4):1168e77.
[41] Loerakker S, Stekelenburg A, Strijkers GJ, Rijpkema JJ,Baaijens FP, Bader DL, et al. Temporal effects of me-chanical loading on deformation-induced damage in skel-etal muscle tissue. Ann Biomed Eng 2010;38(8):2577e87.
[42] Sopher R, Nixon J, Gorecki C, Gefen A. Exposure to in-ternal muscle tissue loads under the ischial tuberositiesduring sitting is elevated at abnormally high or low bodymass indices. J Biomech 2010;43(2):280e6.
[43] Lin F, Moran B, Bankard J, Hendrix R, Makhsous M. FEMmodel for evaluating buttock tissue response under sittingload. In: Paper presented at: Engineering in Medicine andBiology Society; 1-5 Sept. 2004; 2004.
[44] Shabshin N, Zoizner G, Herman A, Ougortsin V, Gefen A.Use of weight-bearing MRI for evaluating wheelchaircushions based on internal soft-tissue deformations underischial tuberosities. J Rehabil Res Dev 2010;47(1):31e42.
[45] Shabshin N, Ougortsin V, Zoizner G, Gefen A. Evaluation ofthe effect of trunk tilt on compressive soft tissue de-formations under the ischial tuberosities using weight-bearing MRI. Clin Biomech (Bristol, Avon) 2010;25(5):402e8.





























