Embed Size (px)
Citation preview

� 3/24
� 3/26
� Urine output improved è D/C IV LR
� 3/27
� Residual <100ml è NGT clamped � Loose stools è check for C-diff è Negative � New meds: aztreonan, morphine, percocet

� 3/28
� Pt vomits 3 times � Gastroparesis � New meds: zofran � Ambulated
� 3/29
� Pt slightly dehydrated è ½ NS @ 25cc/hr � New med: erythromycin
� 3/30
� Calorie count posted � Psych consulted for anxiety � New meds: ativan

GOALS PLANS
1. Advance to post-gastrectomy diet as tolerated by pt to avoid gastroparesis 2. Increase po intake to >50% within 3 days
-Change to nocturnal TF to increase appetite and optimize intake during the day -Small frequent feeds appropriate -Drink beverages in between meals -Order a calorie count to document exact po intake -Educate pt and family on post-gastrectomy diet guidelines -Continue to provide pt with preferred food and beverages.

� 3/31
� N/V occur è
� Blake drain inserted è straw-colored fluid suctioned from J-tube site
� 4/1
� Calorie count not completed
� 4/2 � Poor po, pt not hungry
� New calorie count posted
� 4/3 � Pt extremely thirsty � New meds: amlodipine, atenolol

Date Wt Na+ K+ BUN Creat Glu Ca Hgb Hct MCV Palb
/Alb A1C
3/09 140 3.7 18 0.6 90 9.3 Alb 3.8
3/23 132# 141 3.8 20 0.5 115 7.6 ê
10.6ê
32 ê
99.7 Palb 7.6 Alb 2.7 ê
4.9%
3/27 139# 139 4.1 17 0.4 148 7.1 ê
11.2ê
33.9ê
96.9
3/30 140# 138 4.2 17 0.4 124 11.7 ê
35.4 96.5
4/01 134 ê
4.6 15 0.4 123 7.5 ê
4/03 133 ê
4.8 14 0.6 113 7.6 ê
96.9

� Sodium (Na+): ê (hyponatremia) with edema, severe diarrhea/vomiting, hyperglycemia, malabsorption
� Calcium (Ca+): ê(hypocalcaemia) with hypoalbuminemia, diarrhea, malabsorptions, diarrhea, acute pancreatitis
� Hemoglobin (Hgb): ê with anemia, cirrhosis
� Hematocrit (Hct): êwith anemia, blood loss, hemolysis, cirrhosis
� Prealbumin (Palb): ê with acute catabolic states, stress, surgery, malnutrition, low protein intake

Drug Name Classification Side Effects
Heparin Anitcoagulant N/V, ab pain, GI bleed, black tarry stools, éK, êTG, êchol
Metoprolol Antihypertensive N/V, dyspepsia, diarrhea, éK, éTG
Protonix Antiulcer/Antigerd êgastric acid secretions, égastric pH, nausea, ab pain, diarrhea, égastrin, êvitB12, échol, églu, écreat
Narcan Opioid antagonist N/V, diarrhea, HTN, edema
Aztreonan Antibiotic Altered taste, N/V, diarrhea, écreat
Morphine Analgesic/Narcotic êwt, éthirst, dehydration, dyspepsia, dysphagia, êgastric motility, N/V, diarrhea
Percocet Analgesic/Narcotic Anorexia, dry mouth, dyspepsia, gastritis, N/V, diarrhea, êNa
KCl Electrolyte GI irritation, N/V, ab pain, diarrhea, éK, éCl

Drug Name Classification Side Effects
Zofran Antiemetic/Antinauseant Ab pain, diarrhea, êK
Erythromycin Antibiotic égastric motility, epigastric distress, N/V, diarrhea, pancreatitis
Ativan Antianxiety êwt, éappetite, éwt, éthirst, N/V, diarrhea
Discharge Medications
Amlodipine Antihypertensive Dysphagia, nausea, edema
Atenolol Antihypertensive éTG, êHDL, éK, éuric acid, éBUN
MVI Multivitamin
Ferrous Sulfate Hematinic/Antianemic Anorexia, êZn, N/V, dyspepsia, diarrhea, dark stools, éH/H, éfe, false êCa
Ascorbic Acid Vitamin C N/V, dyspepsia, gastric cramps, diarrhea, edema, éCa excretion, êNa excretion

� 4/2 � NPO � Jevity 1.5 @ 50cc/hr via J-tube
� 4/3 � Breakfast: ½ cup farina, 8oz 1% milk, Ensure Plus � Lunch: Nothing � Dinner: 3 oz. fish (tilapia), 1/3 cup mashed potatoes � Nocturnal TF: Jevity 1.5 @ 50cc/hr x 8 hours (10pm-6am)

Nutrient Requirements
(average)
Total Average Intake
Total Average Intake
(w/out TF)
Total Kcal 1,650 1,652 450
Protein (gm) 81 77 26
Fat (gm) 50 48 9
Carbohydrate (gm)
219 239 67

0
300
600
900
1,200
1,500
1,800
Kcals Protein (cal)
Fat (cal) CHO (cal)
Calo
ries
Nutrient Requirements
Total intake
Intake w/out TF

NCP
Assessment
Diagnosis
Intervention
Monitoring/Evaluation

� SFH Dietitians (and Dietetic Intern) remained an integral part of the Interdisciplinary Plan of Care for E.W. throughout her stay
� E.W. was marked as a “HIGH RISK” patient, so she was seen every 1-3 days by a dietitian for close monitoring
� Nursing staff administered appropriate tube feeding orders and documented rates hourly
� Diet orders were promptly modified as patient toleration shifted
� Calorie counts were posted to evaluate po intake
� Labs were drawn daily and as requested

� Transferred to rehab at Our Lady of Consolation (Medicare would only cover 14 days at the hospital)
� Dr.- “Pt overall doing well and continues to improve”
� Pt referred to DeMatteis Outpatient Center
� Diet order � Post-gastrectomy diet
� Small meals and snacks (5-6x/day) � NCS � Drink between meals � No carbonated beverages � Protein at each meal
� Ensure supplements
� Medications � Amlodipine � Ferrous Sulfate � Atenolol � Vitamin C � Protonix � MVI

Postoperative Nutritional Effects of Early Enteral Feeding Compared with Total Parental Nutrition in
Pancreaticoduodenectomy Patients
� Purpose: Assess the nutritional status and clinical outcomes of patients s/p Whipple according to nutritional method between EEN and TPN
� Methods/Materials:
� Randomized, single center, parallel group trial
� 40 patients over age 18 (mean age of 61) who received PD with malignant periampullary pathology at Gangnam Severance Hospital between May 2007-December 2008

� Assessment of nutrition � Weight � Laboratory parameters � Patient Generated Subjective Global Assessment
� POD # 7, 14, 21, and 90
� Post-Op Nutrition Support: Pt’s were divided into 2 groups � Enteral feeding- starting w/in 24hr post-op at a rate of 20mL/hr
(increasing by 20mL/day unit reaching 25kcal/kg) � Total Parenteral- starting on POD#1 w/ solution of 25kcal/kg � Patients were given sips of water POD#4-5, and then transitioned
to a regular diet within 7 days, or as tolerated

� RESULTS � Transition to an oral diet was quicker in the EEN group � Hospital stay was shorter in the EEN group � 1st BM took ~ ½ the time in the EEN group than TPN group � 34% of patients had post-op complications, similar rates in both
groups Park JS, et al. ח Early Enetral Nutrition in Pancreaticoduoencetomy
KWWS���MNPV�RUJ 265http://dx.doi.org/10.3346/jkms.2012.27.3.261
alteration of the gut system, and less expensive than TPN (15-17). Pancreatic leakage is one of the leading postoperative com-plications after PD, and it can lead to prolonged hospital stay, increased costs and mortality. Consequently, pancreatic sur-geons often prefer postoperative TPN because of the greater risk of pancreatic leakage. However, several reports have suggested that there is no marked di!erence in pancreatic leakage between EEN and TPN groups (11, 18). Our study is consistent with pre-vious reports that EEN is not a signi"cant factor for pancreatic leakage. In contrast to the report of Martignoni et al. (11), there were no signi"cant di!erences in the occurrence of delayed gastric emptying between the EEN and TPN groups. #e main di!er-ence between the report of Martignoni et al and the present study was the cyclic infusion of enteral nutrition. Certainly, the cyclic enteral nutrition has advantages for patients over continuous enteral nutrition because it is closer to the natural form of en-teral nutrition (19). Our results demonstrate that EEN does not increase the incidence of delayed gastric emptying after PD. Moreover, EEN promotes faster recovery of bowel peristalsis by reducing time to recanalize for passing gas and feces. Our results are not consistent with the "ndings of Brennan et al. (9), who suggested that TPN was associated with increased infectious complications. #e main di!erence between the re-port of Brennan et al. and this study was caloric load. #ey pro-vided high calories at a rate of 30-35 kcal/day, which is consid-ered relative overfeeding today, and this overfeeding may in-crease postoperative complications when compared with per-missive underfeeding (20). However, a routine use of TPN does not seem to provide any bene"t because the high rate of glucose intolerance observed in TPN patients. #ere are several methods to deliver enteral nutrition after PD. Nasojejunal tube provides a cost e!ective and desirable method of enteral nutrition without the morbidity from an additional enterotomy (21). However, the frequency of nasojejunal tube dislodgement and occlusion was as high as 35% to 100% (22, 23).
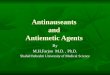
Fig. 3. Mean prealbumin and transferring levels on preoperative day and on days 7, 14, 21, and 90 postoperatively *. Error bars: 95% confidence interval. *There was signifi-cant difference between the EEN and TPN Group at any time point of postoperative days.
Mea
n pr
ealbu
min
(mg/
L)
Mea
n tra
nsfe
rrin
(g/L
)
Pre OP POD 7 POD 14 POD 21 POD 90 Pre OP POD 7 POD 14 POD 21 POD 90
400
350
300
250
200
150
100
50
0
3.5
3
2.5
2
1.5
1
0.5
0
In the present study, nasojejunal feeding tube was used for all EEN patients, and jejunostomy tube was not used according to our department policy. #at is because any unnecessary enter-otomy was a potential source of complications. #ere were no catheter related major complications in the EEN group except for accidentally dislodged nasojejunal tube. In our experience, tube occlusion can be prevented by irrigating it with 20 mL water every 8 hr and after giving medications. The accidentally dis-lodgement of nasojejunal tube was the most common phenom-enon, and special education and attention must be paid to "rm nasal "xation. We think that a nasojejunal tube is an e!ective tool for providing enteral feeding after PD. In our study, EEN related adverse effect occurred in 22.2% and were resolved by reduction or temporary interruption of infusion. All patients in EEN group reached the nutritional goal without having di$culty by following the infusion protocol. #is may be attributed to the fact that our protocol started at a slow flow rate with careful and progressive increase in the feeding volume. Also, this can prevent abdominal distension caused by reaching the nutritional goal too aggressively and early (24). In usual practice, the parenteral nutrition begins at goal rates, whereas the enteral feedings advance to goal rate over several days. Although the level of rapid turnover proteins such as pre-albumin and transferrin dropped in all the patients after the op-eration, it was recovered signi"cantly fast in the EEN group in the early postoperative period. #ese results indicate that EEN modulates a metabolic response, favoring the synthesis of pro-teins. It has been shown that patients can maintain a normal body weight after surgery, but it is frequently less than their preoper-ative body weight (25-27). Kozuscheck et al. (28) reported that 85% of patients who had undergone PPPD reached the preop-erative body weight one year after surgery. However, in the pres-ent study, preoperative body weight restored in 3 weeks in the EEN group, and recovery of weight 3 weeks after the operation was signi"cantly better in the EEN patients than in the TPN pa-
EEN Group EEN GroupTPN Group TPN Group
Prealbumin Results

� RESULTS (cont.) � No significant difference in the rate of serum albumin
change � No significant difference in the rate of pancreatic
leakage (one of the leading post-op complications) � Weight change:
� EEN group- wt gradually decreased until POD# 14, and rapidly recovered on POD #21
� TPN group- wt gradually decreased until POD# 90

� CONCLUSION � Early Enteral Nutrition in gastrointestinal surgery
should be recommended whenever possible.
� “The benefits of EEN have been demonstrated to be more physiological, better preventative in morphologic and functional alteration of the gut system, and less expensive.”

� American Dietetic Association. (2011). Pocket Guide for International Dietetics & Nutrition Terminology (IDNT) Reference Manual: Standardized Language for the Nutrition Care Process. Chicago: American Dietetic Association.
� Beers, M. H., Porter, R. S., Jones, T. V., J. L., & Berkwits, M. (Eds.). (2006). The Merck Manual of Diagnosis and Therapy (18th ed). White house Station, NJ: Merck Research Laboratories.
� DeVita, V. T., Rosenberg, S. A., & Lawrence, T. S. (2008). Cancer: Principles and Practice of Oncology. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.
� Facing Pancreatic Cancer. (2012). Retrieved March 24, 2012, from Pancreatic Cancer Action Network: http://www.pancan.org section_facing_pancreatic_cancer/learn_ about_pan_cancer
� Gottschlich, M. M, (2007). The A.S.P.E.N Nutrition Support Core Curriculum. Silver Spring: American Society for Parenteral and Enteral Nutrition.
� Langhorne, M. E., Fulton, J. S., & Otto, S. E. (2007). Oncology Nursing. St. Louis: Mosby/Elsevier.
� Martin, J. A., & Moser, J. (2010, January 18). Ampullary Carcinoma: Epidemiology, Clinical Manifestations, Diagnosis, and Staging. Retrieved March 24, 2012, from UpToDate: http://www.uptodate.com/contents/ampullary-carcinoma-epidemiology-clinical-manifestations-diagnosis-and-staging
� Pancreatic Cancer: Integrative Treatment Program. (n.d.). Retrieved March 27, 2012, from Cancer Treatment Centers of America: http://www.cancercenter.com/ pancreatic-cancer/pancreatic-cancer-information.cfm
� Park, J. S., Chung, H.-K., Hwang, H. K., Kim, J. K., & Yoon, D. S. (2011). Postoperative Nutrition Effects on Early Enteral Feeding Compared to Total Parental Nutrition in Pancreaticoduodenectomy Patients. Journal of Korean Medical Society , 27, 261-267.
� Pronsky, Z. M., & Crowe, S. J. (2010). Food Medication Interactions. Birchrunville: Food-Medication Interactions.
� Reber, H. A. (2011, October 11). Pancreaticoduodenectomy (Whipple Procedure): Techniques. Retrieved March 24, 2012, from UpToDate: http://www.uptodate. com/ contents/pancreaticoduodenectomy-whipple-procedure-techniques