Embed Size (px)
Citation preview

5/5/2010
1
NINAD KARANDIKAR, MD
ASSISTANT PROFESSOR
DEPT OF PM&R
UNIVERSITY OF KY
Understand the normal anatomy and bio-mechanics of the shoulder
Perform a good history and physical exam in a patient with c/o shoulder pain
Formulate a differential diagnosis
Obtain appropriate work-up to confirm diagnosis
Discuss treatment algorithms for appropriate management
An estimated 20 percent of the population will
suffer shoulder pain during their lifetime1
Shoulder pain is second only to low back pain
in patients seeking care for musculoskeletal
ailments in the primary care setting2
Shoulder pain is defined as “chronic” when
it has been present for longer than six
th dl f h th th ti tmonths, regardless of whether the patient
has previously sought treatment
WHAT IS THE INVOLVED
STRUCTURE ?STRUCTURE ?
WHAT IS THE MECHANISM ?
ANATOMY OF THE SHOULDER COMPLEX

5/5/2010
2
Anatomy of the Shoulder Joint “Shoulder” Joint: 4 different articulations
Gleno-humeral
Acromio-clavicular
Sterno-clavicular
Scapulo-thoracic
SPACE: Sub-acromial
BURSA: Sub-acromial (and sub-deltoid)
“Shoulder” Joint Articulations
aaaaaaaaaaaaa
Sacrifices stability to improve mobility
Stability:
Bony (Intrinsic): glenoid fossa articulating with the
humeral head & negative intra-articular pressureg p
Soft tissue (extrinsic):
○ Capsule with ligaments (Primary STATIC stabilizer)
○ Labrum
ROTATOR CUFF (Primary DYNAMIC
stabilizer)
ANTERIOR VIEW POSTERIOR VIEW
LATERAL VIEWLATERAL VIEW

5/5/2010
3
1. Serves as a base for muscle attachment The musculature controls scapular motion mainly
through synergistic co-contractions and force couples
M i f d i bili i h2. Maintenance of dynamic stability with controlled mobility at the glenohumeraljoint The scapula moves in a coordinated fashion with
the moving humerus, so that the humeral head is constrained within the glenoid fossa throughout the full range of shoulder motion
The maintenance of proper alignment of the glenoid fossa
○ Allows for optimal bony constraint
○ Facilitates muscular constraint by maintaining proper length tension relationships of the rotator c ff m scleslength-tension relationships of the rotator cuff muscles
○ This in turn allows efficient contraction of the rotator cuff muscles, thereby compressing the humeral head into the fossa
○ The scapula rotates upward with overhead activities to clear the acromion from the rotator cuff decreasing the likelihood of “physiologic” impingement
3 The third role of the scapula is best3. The third role of the scapula is best represented as the link in the proximal-to-distal transfer of energy that allows the most appropriate shoulder positioning for optimal function of the arm
The scapula is pivotal in transferring the large forces and high energy from the major sources for force and energy—the legs and trunk—to the actual delivery mechanism of the energy and force the arms andmechanism of the energy and force—the arms and hands
These actions can be accomplished most effectively through the stable and controlled platform of the scapula, so that the entire arm rotates as a unit around the stable base provided by the scapulothoracic and the glenohumeral joints
The muscles primarily responsible for scapular stability and motion are: Trapezius
Serratus anterior
Rhomboids
Levator scapulae
Weakness of these muscles predisposes to scapular malposition, malfunction and consequently impingement syndrome

5/5/2010
4
COMMON CAUSES OF SHOULDER PAINSHOULDER PAIN
INTRINSIC CAUSES3
Rotator cuff disorders
Acromio-clavicular joint disorders
Gleno-humeral disordersAdhesive capsulitisAdhesive capsulitis
Osteoarthritis
Instability
Other chronic pain: including less common, non-shoulder problems
Extrinsic Causes Neurologic
Cervical nerve root compression (C5, C6)
Brachial plexus lesions
Herpes zoster
Cardiovascular Myocardial ischemia
Axillary vein thrombosis
Thoracic outlet syndrome
Thoracic Spinal cord lesion
Cervical spine disease
Abdominal Hepatobiliary disease
Diaphragmatic irritation (eg, splenic injury, ruptured ectopic pregnancy, perforated viscus)
Thoracic Upper lobe pneumonia
Apical lung tumor
Pulmonary embolus
MOST COMMON CAUSES Impingement Syndrome
Adhesive Capsulitis These 2 causes account for the majority j y
of primary care office visits for “Shoulder Pain”
“Impingement syndrome” is the term used to
describe symptoms and signs that result from
compression of the rotator cuff tendons and the
s bacromial b rsa bet een the greater t bercle ofsubacromial bursa between the greater tubercle of
the humeral head and the lateral edge of the
acromion process
Overhead repetitive activity is important in
pathophysiology

5/5/2010
5
Repetitive Impingement
Rotator cuff tendon inflammation (tendinitis)
Rotator Cuff degeneration (also called tendinosis / tendinopathy)
Rotator cuff tears (partial or complete)
Adhesive capsulitis refers to a stiffened glenohumeral joint that has lost significant range of motion (abduction and rotation)
Pathology: Pathology: It is a reversible contraction of the joint capsule in
almost all cases
Most common causes: Rotator cuff problems
Stroke
DM / Thyroid problems
Patients with adhesive capsulitis complain primarily of stiffness, although they may have
pain
l d t t di i i h d i f ti always demonstrate diminished passive range of motion
Patients with rotator cuff tendinopathy typically complain of pain with active motion
passive motion remains normal (in the absence of guarding)
HISTORY TAKING
Detailed History of “Pain” Location / Character / radiation
Onset / duration / progress
Participation in sports
H/O trauma / infection / CA / Sz disorder
H/O DM / thyroid disorders
Associated loss in ROM & weakness
Night pain +/- fever and constitutional symptoms
Any unexplained significant sensory or motor deficit
Occupational & recreational history
PHYSICAL EXAMINATION

5/5/2010
6
Look: Atrophy / erythema Feel: TTP / warmth / swelling / trigger points Move
Active + Passive Resisted Resisted
Special (Provocative)Tests Impingement Labral Tear Instability Thoracic outlet
Neurological exam, if necessary
Movement Muscles
Fwd Flex Deltoid, Pec major, Long head of Biceps
Extension Deltoid, Teres major, Lat dorsi, Pecmajor, Triceps (Long Head)j , p ( g )
Abduction Deltoid, Supraspinatus
Adduction Pec major, Lat dorsi, Teres major
Int rotation Pec major, Deltoid, Lat dorsi, Teresmajor, Subscapularis
Ext Rotation Infraspinatus, Deltoid, Teres minor
Apley’s scratch test
EXAMINE SCAPULO-THORACIC RHYTHM Stand behind the patient
Place a thumb on or to hold the inferior tip of each scapula
Have the patient abduct and / or forward flex the arm
Assess for scapular asymmetry
Always perform an exam in a gown to assess for scapular rhythm
1 deg of movement at the scapula for every 2 degrees of gleno-humeral abduction
PROVOCATIVE TESTSTESTS
5/5/2010
7
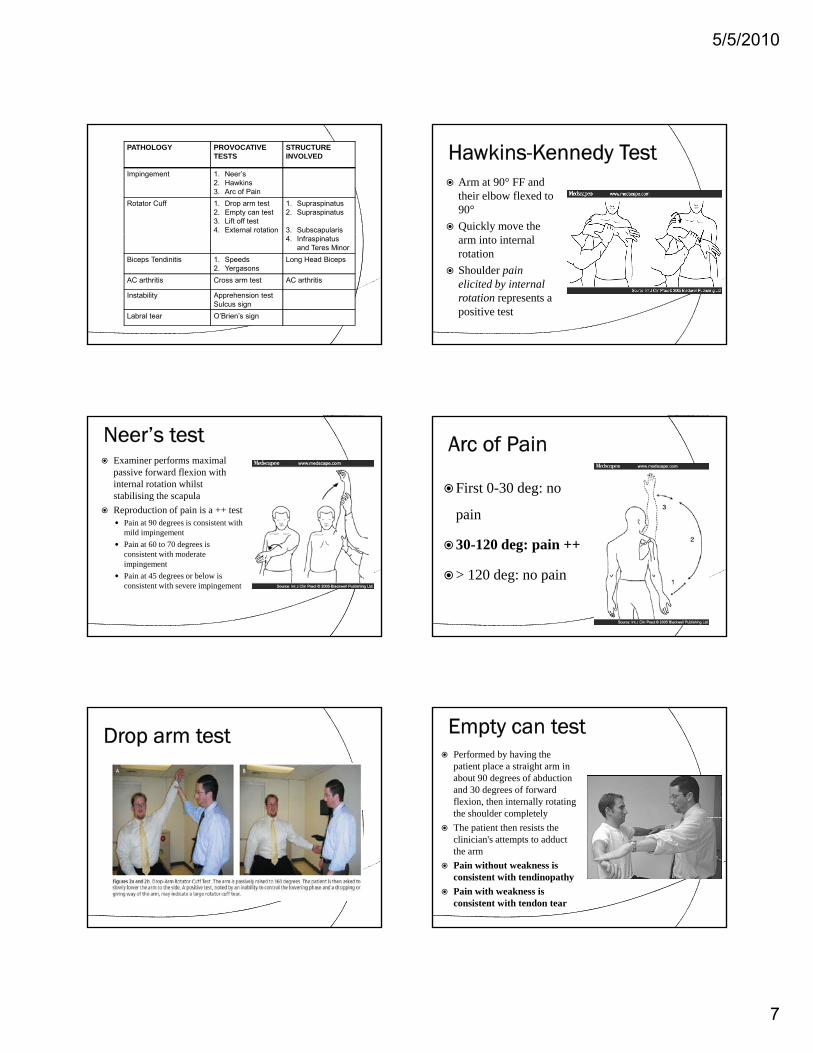
PATHOLOGY PROVOCATIVETESTS
STRUCTUREINVOLVED
Impingement 1. Neer’s2. Hawkins3. Arc of Pain
Rotator Cuff 1. Drop arm test2. Empty can test3. Lift off test4. External rotation
1. Supraspinatus2. Supraspinatus
3. Subscapularis4. Infraspinatus
and Teres Minor
Biceps Tendinitis 1. Speeds2. Yergasons
Long Head Biceps
AC arthritis Cross arm test AC arthritis
Instability Apprehension testSulcus sign
Labral tear O’Brien’s sign
Arm at 90° FF and their elbow flexed to 90°
Quickly move the arm into internal rotation
Shoulder pain elicited by internal rotation represents a positive test
Examiner performs maximal passive forward flexion with internal rotation whilst stabilising the scapula
Reproduction of pain is a ++ test Pain at 90 degrees is consistent with g
mild impingement
Pain at 60 to 70 degrees is consistent with moderate impingement
Pain at 45 degrees or below is consistent with severe impingement
First 0-30 deg: no
pain
30-120 deg: pain ++
> 120 deg: no pain
Performed by having the patient place a straight arm in about 90 degrees of abduction and 30 degrees of forward flexion, then internally rotating the shoulder completelyp y
The patient then resists the clinician's attempts to adduct the arm
Pain without weakness is consistent with tendinopathy
Pain with weakness is consistent with tendon tear

5/5/2010
8
Lift off test
The patient attempts to externally rotate the arms against resistance while the arms are at the sides and the elbows are flexed to 90 degrees
Speed’s and Yergason’s Test The patient
elevates the affected arm to 90 degrees, then actively adducts it
Reproduction of pain: ++ test
Apprehension Test The patient is instructed to flex their
arm to 90° with the elbow fully extended and then adduct the arm 10-15°medial to sagittal plane
The arm is then maximally internally rotated and the patient resists the pexaminer's downward force
The procedure is repeated in supination
+ test: Pain elicited by the fIrst manoeuvre (pronation) is reduced or eliminated by the second maneuvre (supination)

5/5/2010
9
3,4,5 Clinical Rules regarding tests for Shoulder Pain
1. A prospective analysis of 400 patients found that
the triad of weakness found with the empty-can
supraspinatus and external rotation tests, along
with a positive impingement test (e.g., Hawkins'
impingement test), had a 98 percent probability
of being a rotator cuff tear (partial or complete)4
Clinical Rules regarding tests for Shoulder Pain2. A retrospective analysis of 191 persons found that the
combination of being older than 65 years, having weakness on
external rotation testing and experiencing night pain resultedexternal rotation testing, and experiencing night pain resulted
in a 91 percent probability of having a rotator cuff tear
(partial or complete)5
3. However, 54 percent of asymptomatic persons older than 60
years have been shown to have a partial or full thickness
rotator cuff tear by MRI6
DIAGNOSING S OSHOULDER PAIN
Chronic Shoulder Pain: Part I. Evaluation and Diagnosis AAFP Vol. 77 / No. 4. February 2008
Clinical review of Shoulder pain: diagnosis and management in primary care. Mitchell, C. et al. BMJ 2005;331:1124-1128

5/5/2010
10
1. Xrays
2. Ultrasound
3 MRI scan3. MRI scan
4. Arthrogram
5. MR arthrogram
6. Labs: rarely required
Xrays
AP view
Axillary view
S l i
Fracture
Dislocation
Sh f i
Views Demonstrate
Scapular Y view Shape of acromion
Acromio-humeral interval
Hill-Sach lesion
Bankart lesion
DJD
Calcific tendinitis
Used in assessing rotator cuff tears (specially full thickness tears), labral tears, and biceps tendon tears
Less expensive than MRI
Accuracy with operator experience is close to that of MRI scan: 86 % vs 93 %*
*Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. Iannotti JP. J Bone Joint Surg Am. 2005 Jun;87(6):1305-11.
Dinnes J, Loveman E, McIntyre L, Waugh N. The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review. Health Technol Assess. 2003;7(29):iii, 1-166
Best modality for imaging the soft tissues of the shoulder
Preferred modality for imaging rotator cuff tears, both full-thickness and partial with a sensitivity of 92% and specificity of 88 100%7of 92% and specificity of 88-100%7
Also used to evaluate labral lesions and so may be helpful in the diagnosis of instability
MR Arthrogram is the test of choice for diagnosing labral tears

5/5/2010
11
1. Activity Modification
2. Medications (NSAIDs, topicals, judicious
use of opioids)p )
3. Physical therapy (including modalities)
4. Injections
5. Surgery
Reduction or avoidance of overhead activity is the mainstay of treatment for impingement and rotator cuff pathology
Avoiding heavy loading / lifting on the Avoiding heavy loading / lifting on the affected shoulder
Avoid Cross-body shoulder adduction activities (e.g. golf swing, weight lifting)
Vocational Counseling
Pain control is imperative to allow for the progression of treatment
Use of nonsteroidal anti-inflammatory drugs (NSAIDs) nonsteroidal anti inflammatory drugs (NSAIDs)
Acetaminophen
Judicious short-term opiate medication
may help achieve this goal
Risks and benefits of each class should be considered before use
Mainstay of therapy: Scapular stabilization
Stretching / strengthening / ROM
Modalities
A recent Cochrane review showed that A recent Cochrane review showed that stretching and strengthening provide improved short-term recovery and long-term function in patients with rotator cuff disease*
*Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev. 2003;(2):CD004258
Steroid Injections Indicated if poor response to activity
modification, medication and physical therapy
Directed towards the affected area
Subacromial Subacromial
AC joint
Gleno-humeral
Efficacy and accuracy of injection is extremely controversial
Accuracy of Steroid Injections done without guidance Sethi et al (Arthroscopy January 2005)
Based on our cadaveric study, we believe that without some form of radiologic guidance, it is unlikely that an anteriorly placed intra-articular glenohumeral injection will be accurately placed in awake patients, and we do not recommend this technique. Level IV.
Manchester Rheumatology Service (BMJ 1993) inaccurate placement of medication in 65% of the 108 joints
injected
Eustace's (1997) study 68% of shoulder injections performed by specialist physicians
without radiological guidance failed to hit their targets

5/5/2010
12
Steroid Injections: AAOS recommendations (OKU) Rotator cuff disease:
Subacromial injections are a treatment option currently supported by the American Academy of Orthopedic Surgeons (AAOS), although this may change with further review
Acromioclavicular joint for osteoarthritis: Subacromial injections are endorsed by the AAOS, despite
few studies demonstrating its effectiveness
Adhesive capsulitis: respond to intra-articular injections with decreased pain and
increased function, particularly in combination with physical therapy for stretching
Steroid Injections: AAOS recommendations Glenohumeral osteoarthritis:
Intra-articular steroid injections are not recommended by the AAOS
Intra articular hyaluronic acid injections have shown Intra-articular hyaluronic acid injections have shown promise in several studies, but the AAOS has no recommendation for this treatment to date
Self EB. Clinical guidelines for shoulder pain. In: Norris TR, ed. Orthopaedic Knowledge Update. Shoulder and Elbow 2. 2nd ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons, 2002:443-467
CLINICAL RECOMMENDATIONS
Clinical recommendation Evidence rating ReferencesMost patients with chronic shoulder pain
improve with nonoperative treatment. Worse outcomes are associated with severe pain,
prolonged symptoms, or gradual onset.
B 4, 5
There is little evidence for or against the use of medication for chronic shoulder pain.
B 10
Physical therapy can provide improved short-term recovery and long-term function
for rotator cuff disorders.
B 11
Although subacromial corticosteroid injections for rotator cuff disorders are very
B 12-16injections for rotator cuff disorders are very common in clinical practice, there is little
evidence to support or refute its use.
Glenohumeral joint injection has been shown to hasten the resolution of symptoms
in patients with adhesive capsulitis, but most patients resolve without intervention, and interventions have not been shown to
improve long-term outcomes.
B 16, 19
Chronic Shoulder Pain: Part II. Evaluation and Diagnosis AAFP Vol. 77 / No. 4. February 2008
Most patients with a chronic shoulder disorder can initially be treated conservatively with some combination ofA ti it difi tiActivity modification
Physical therapy
Medications and
Corticosteroid injections, if necessary, with no improvement after trying the above
Chronic Shoulder Pain: Part II. Evaluation and Diagnosis AAFP Vol. 77 / No. 4. February 2008

5/5/2010
13
1. No relief of pain and improvement in function, with an adequate trial of conservative therapy for 6 weeks to 3 months
2. Gleno-humeral instability (early referral)
3 Uncertainty of diagnosis (early referral)3. Uncertainty of diagnosis (early referral)
4. DJD of AC joint or GH joint
5. First dislocation – occupation/sport/active
6. Individualize on age, co-morbidities and activity level Labral tear or a rotator cuff tear in an active individual
Surgical Options Arthroscopic and open, based on indication
Impingement: Subacromial decompression
Excision of distal end of clavicle
Rotator cuff tears: Repair +/- decompression
Instability +/- labral tear: Repair +/- soft tissue tightening
Adhesive capsulitis: Adhesiolysis:
DJD Partial or complete joint replacement
MY ALGORITHMGO
Algorithm for chronic shoulder pain
Diagnosis and treatment of chronic painful shoulder: review of nonsurgical interventions. Andrews JR Arthroscopy. 2005 Mar;21(3):333-47
“The role of the Physician is to entertain the Patient whilst his disease runs itswhilst his disease runs its usual course."Molière 17th century
1. Pope DP, Croft PR, Pritchard CM, Silman AJ. Prevalence of shoulder pain in the community: the influence of case definition. Ann Rheum Dis. 1997;56(5):308-312.
2. Steinfeld R, Valente RM, Stuart MJ. A common sense approach to shoulder problems. Mayo Clin Proc. 1999;74(8):785-794.
3. Self EB. Clinical guidelines for shoulder pain. In: Norris TR, ed. Orthopaedic Knowledge Update: Shoulder and Elbow 2. 2nd ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons, 2002:443-467
4. Murrell GA, Walton JR. Diagnosis of rotator cuff tears Lancet. 2001; 357(9258):769-770
5. Litaker D, Pioro M, El Bilbeisi H, Brems J. Returning to the bedside:using the history and physical exam to identify rotator cuff tears. J Am Geriatr Soc. 2000;48(12):1633-1637
6 Sher JS Uribe JW Posada A Murphy BJ Zlatkin MB Abnormal findings on magnetic resonance images6. Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995;77(1):10-15
7. Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value Iannotti JP J Bone Joint Surg Am 1991 Jan;73(1):17-29





























