Embed Size (px)
Citation preview

2222ndnd Annual IHCA Conference Annual IHCA Conference20102010
‘‘The Medical Team of the Future’The Medical Team of the Future’Medical Education & Training Unit, HSEMedical Education & Training Unit, HSE
Dr. Gerard BuryDr. Gerard BuryDirectorDirector

Lifelong learning
UG Education PG Training CME / CA
Properly planned and carefully conducted medical education is the foundation of a comprehensive health service.
Lifelong learning
UG Education PG Training CME / CA
Properly planned and carefully conducted medical education is the foundation of a comprehensive health service.
Report of the Inter-Departmental Committee on Medical SchoolsThe Goodenough Report 1944
Which way?Which way?

Health Act 2004Health Act 2004
‘The object of the Executive is to use the resources available to it ‘The object of the Executive is to use the resources available to it in the most beneficial, effective and efficient manner to improve, in the most beneficial, effective and efficient manner to improve,
promote and protect the health and welfare of the public’promote and protect the health and welfare of the public’

Medical Education & Training 2010Medical Education & Training 2010
Health Act 2004Health Act 2004
Fottrell Report 2006Fottrell Report 2006
Buttimer Report 2006Buttimer Report 2006
MPA 2007MPA 2007
Medical Education & Training 2010Medical Education & Training 2010
Fit for purpose, in the Irish health serviceFit for purpose, in the Irish health service


Future TeamsFuture Teams
DriversDrivers
• Change in medicine: demographics, science, evidenceChange in medicine: demographics, science, evidence• Complexity of careComplexity of care• Economics, limited and expensive resources Economics, limited and expensive resources • Transparency: for members, health organisations and patientsTransparency: for members, health organisations and patients• LeadershipLeadership
• Professionalism and trust: value systems in medicineProfessionalism and trust: value systems in medicine

Future TeamsFuture Teams
Barriers?Barriers?
• Change in medicine: demographics, science, evidenceChange in medicine: demographics, science, evidence• Complexity of careComplexity of care• Economics, limited and expensive resources Economics, limited and expensive resources • Transparency: for members, health organisations and patientsTransparency: for members, health organisations and patients• LeadershipLeadership
• Professionalism and trust: value systems in medicineProfessionalism and trust: value systems in medicine
Future TeamsFuture Teams
Barriers?Barriers?
• Poor trainingPoor training• Inadequate focus on how to form and run teamsInadequate focus on how to form and run teams
• Teams of doctors: flat or hierarchical?Teams of doctors: flat or hierarchical?• Interdisciplinary clinical teamsInterdisciplinary clinical teams• Interprofessional clinical teamsInterprofessional clinical teams• Care teams --- Organisational teamsCare teams --- Organisational teams
Future TeamsFuture Teams
High performance teamsHigh performance teams11
• Structure: who and what?Structure: who and what?• Context: why?Context: why?• Process: how?Process: how?• Productivity: outcomes?Productivity: outcomes?
1. Heinemann, Zeiss. 20021. Heinemann, Zeiss. 2002

Problem Teams?Problem Teams?
• Doctor orders, nurse (phyio, SLT, OT…) does?Doctor orders, nurse (phyio, SLT, OT…) does?• I decide, you do…I decide, you do…• We each have a go and then see what works…We each have a go and then see what works…• I’ll do my job and hope the rest do theirsI’ll do my job and hope the rest do theirs• I’ll do it all, because no-one else can do it properlyI’ll do it all, because no-one else can do it properly• Delegation works bestDelegation works best• What team?What team?• What do they do anyway?What do they do anyway?
5. ACGME Competencies 5. ACGME Competencies The program must integrate the following ACGME The program must integrate the following ACGME
competencies into the curriculum: competencies into the curriculum: f. Systems-based Practicef. Systems-based Practice
Residents must demonstrate an awareness of and responsiveness to the larger Residents must demonstrate an awareness of and responsiveness to the larger
context and system of health care, as well as the ability to call effectively context and system of health care, as well as the ability to call effectively on other resources in the system to provide optimal health care. Residents on other resources in the system to provide optimal health care. Residents are expected to: are expected to:
(5) work in interprofessional teams to enhance patient safety and improve (5) work in interprofessional teams to enhance patient safety and improve patient patient
Teamwork skills are important to demonstrating competence in SBP. Teamwork skills are important to demonstrating competence in SBP. Participation as members and leaders of interdisciplinary teams will allow Participation as members and leaders of interdisciplinary teams will allow residents opportunities to develop and demonstrate abilities in using a residents opportunities to develop and demonstrate abilities in using a variety of tools and teamwork skills to identify, analyze, implement, variety of tools and teamwork skills to identify, analyze, implement, evaluate and report improvement initiatives as well as identifying evaluate and report improvement initiatives as well as identifying system system errorserrors. .

5. ACGME Competencies 5. ACGME Competencies The program must integrate the following ACGME The program must integrate the following ACGME
competencies into the curriculum: competencies into the curriculum: f. Systems-based Practicef. Systems-based Practice
a.a. Describe the learning activity(ies) through which residents Describe the learning activity(ies) through which residents achieve competence in the elements of systems-based achieve competence in the elements of systems-based practice: work effectively in various health care delivery practice: work effectively in various health care delivery settings and systems, coordinate patient care within the health settings and systems, coordinate patient care within the health care system; incorporate considerations of cost-containment care system; incorporate considerations of cost-containment and risk-benefit analysis in patient care; advocate for quality and risk-benefit analysis in patient care; advocate for quality patient care and optimal patient care systems; and work in patient care and optimal patient care systems; and work in interprofessional teams to enhance patient safety and care interprofessional teams to enhance patient safety and care quality. quality.

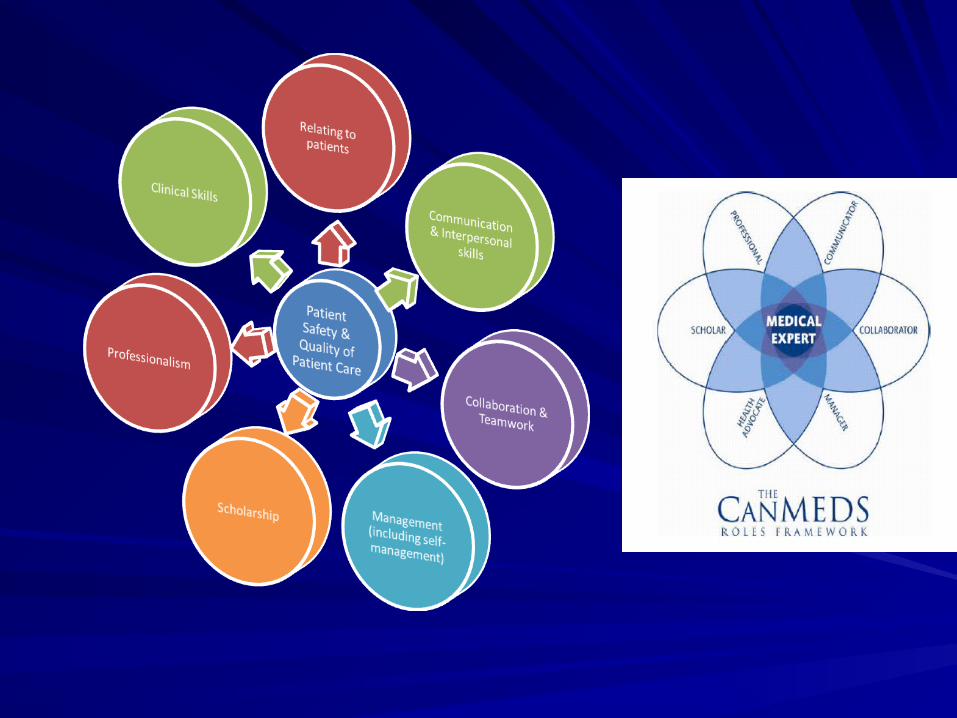
Future Teams Future Teams Members need:Members need:
Knowledge Knowledge • Roles of other healthcare professionals Roles of other healthcare professionals
SkillsSkills• Communication Communication • ReflectionReflection• Conflict resolutionConflict resolution
Attitudes Attitudes • Mutual respect Mutual respect • Open to trust Open to trust • Willing to collaborateWilling to collaborate
Future Teams Future Teams Teams need:need:
• Shared decision-making by:Shared decision-making by:
consensusconsensus
expert opinionexpert opinion
majority viewsmajority views• Balanced responsibilities, values, knowledge, skills, and goalsBalanced responsibilities, values, knowledge, skills, and goals• Mechanisms to input all expertiseMechanisms to input all expertise• Mechanisms to handle disagreementsMechanisms to handle disagreements

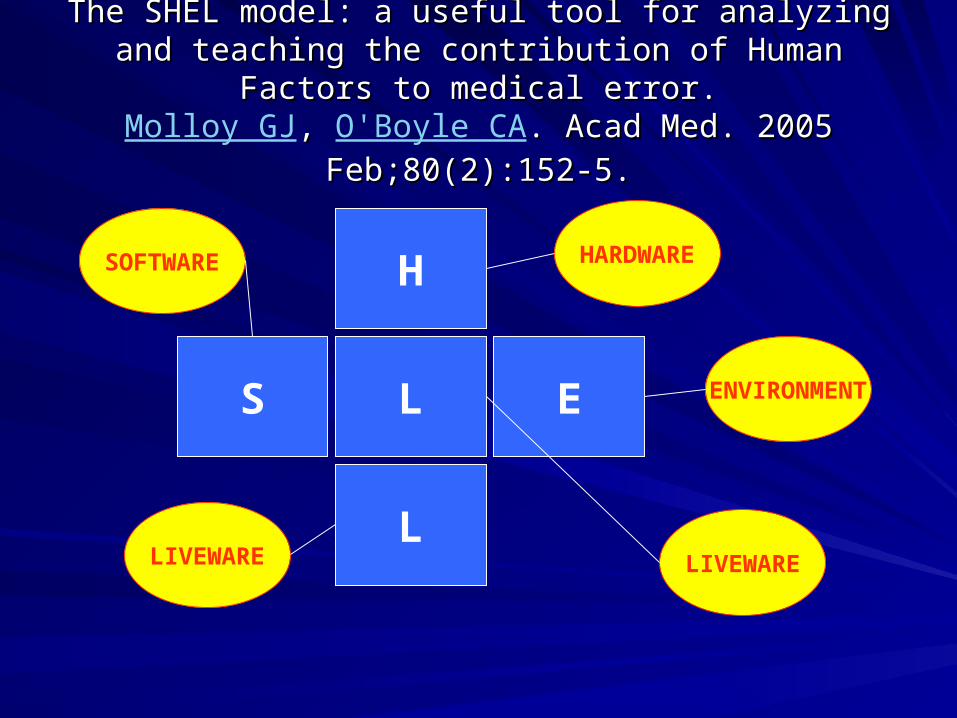
The SHEL model: a useful tool for analyzing and teaching the The SHEL model: a useful tool for analyzing and teaching the contribution of Human Factors to medical error.contribution of Human Factors to medical error.
Molloy GJ, , O'Boyle CA. Acad Med. 2005 Feb;80(2):152-5.. Acad Med. 2005 Feb;80(2):152-5.
S
H
EL
L
The SHEL model: a useful tool for analyzing and teaching the The SHEL model: a useful tool for analyzing and teaching the contribution of Human Factors to medical error.contribution of Human Factors to medical error.
Molloy GJ, , O'Boyle CA. Acad Med. 2005 Feb;80(2):152-5.. Acad Med. 2005 Feb;80(2):152-5.
S
H
EL
L
HARDWARE
ENVIRONMENT
LIVEWARE
SOFTWARE
LIVEWARE

A surgical safety checklist to reduce mortality and morbidity A surgical safety checklist to reduce mortality and morbidity in a global populationin a global population
Haynes AB et al. NEJM 2009; 360:491-9.Haynes AB et al. NEJM 2009; 360:491-9.
• Safe Surgery Checklist implemented by teamsSafe Surgery Checklist implemented by teams• 8 hospitals, 8 cities worldwide 8 hospitals, 8 cities worldwide • 3373 / 3955 patients before / after3373 / 3955 patients before / after• Deaths: 1.5% - 0.8% (p=0.003)Deaths: 1.5% - 0.8% (p=0.003)• Complications: 11% - 7% (p<0.001)Complications: 11% - 7% (p<0.001)• Better team care works…Better team care works…
Simulation-based mock codesSimulation-based mock codes significantly correlate with significantly correlate with improved pediatric patient cardiopulmonary arrest survival improved pediatric patient cardiopulmonary arrest survival
rates.rates.Andreatta P et al. Pediatr Crit Care Med. 2010 Jun 24. et al. Pediatr Crit Care Med. 2010 Jun 24.
• Paediatric cardiac arrestsPaediatric cardiac arrests• Initial training of team members Initial training of team members • 48 months - teams called to mock / training codes48 months - teams called to mock / training codes• Survival in real cardiac arrests rose to 50% (r=0.87)Survival in real cardiac arrests rose to 50% (r=0.87)• Well above national average, steady x 3 yearsWell above national average, steady x 3 years

Medical Education & Training Unit Medical Education & Training Unit
HSEHSE
• Medical CouncilMedical Council• Inter-Departmental Steering Group on MET (Health, Inter-Departmental Steering Group on MET (Health,
Education & Finance)Education & Finance)• National Committee on Medical Education & TrainingNational Committee on Medical Education & Training• Postgraduate training bodiesPostgraduate training bodies• Medical schoolsMedical schools• HSE METHSE MET• Forum of Postgraduate Medical Training BodiesForum of Postgraduate Medical Training Bodies
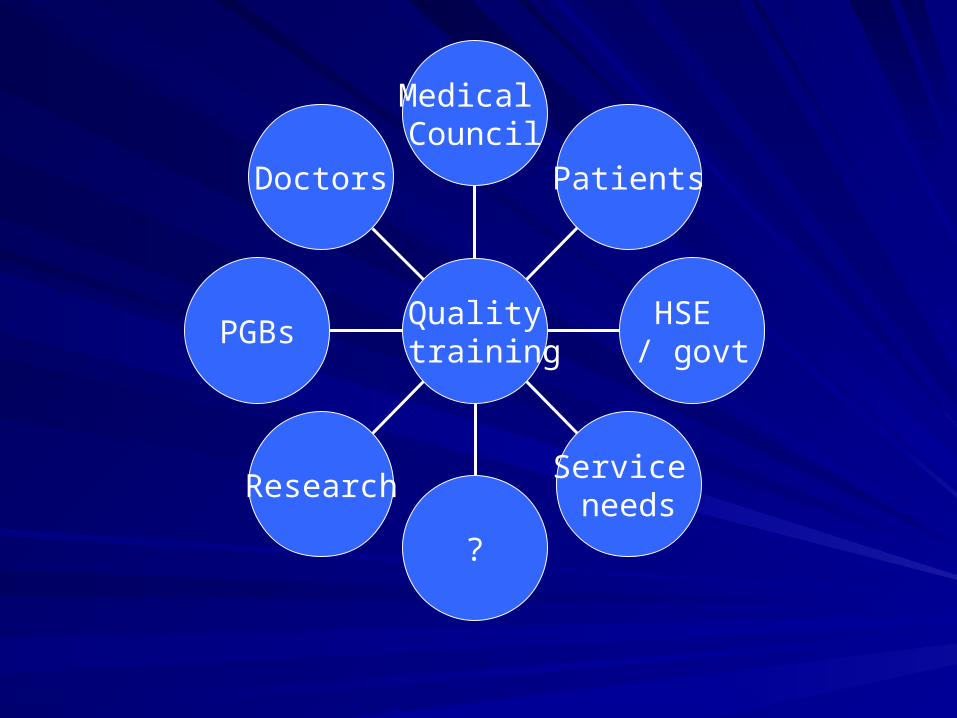
Doctors
PGBs
Research
?
Service needs
HSE / govt
Patients
Medical Council
Quality training

Major rolesMajor roles
• Basic medical educationBasic medical education• InternshipInternship• Specialist medical trainingSpecialist medical training• Competence assuranceCompetence assurance


BMEBME InternIntern
divisiondivision
Spec trainingSpec training
divisiondivision
6 medical schools6 medical schools 35 hospitals35 hospitals 13 approved bodies13 approved bodies
10: 615 EU10: 615 EU
? Non-EU? Non-EU
10: 521 posts10: 521 posts 10: 4,800 NCHDs10: 4,800 NCHDs
3,700 trainees3,700 trainees
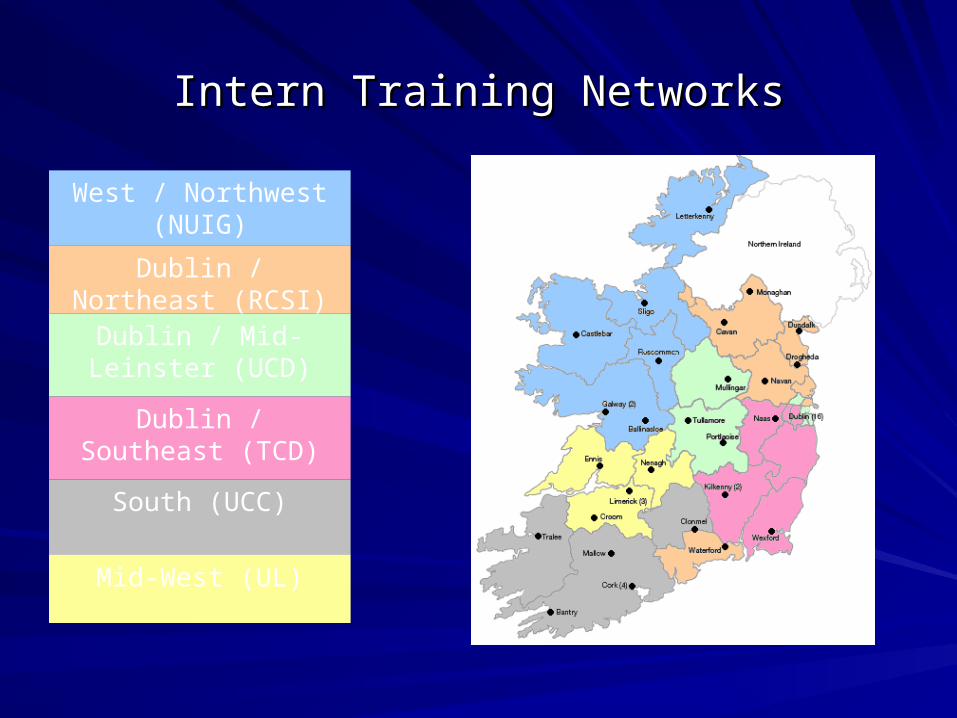
Intern Training NetworksIntern Training Networks
Dublin / Northeast (RCSI)
West / Northwest (NUIG)
Dublin / Mid-Leinster (UCD)
Dublin / Southeast (TCD)
South (UCC)
Mid-West (UL)


TeamworkTeamwork

Thank you