Embed Size (px)
Citation preview

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
1 of 99
Abstral Adcirca Adempas Afinitor Alecensa
Alunbrig Amitiza Amitriptyline Ampyra Androgel Androderm
Aralast NP Aranesp Arcalyst Armodafinil Aubagio
Avonex Bavencio Beleodaq
Berinert Betaseron
Bexarotene Bosulif Briviact Bydureon Byetta
Cabometyx
Cayston
Cholbam
Chorionic Gonadotropin Cimzia Cinryze Clomipramine
Cometriq
Copaxone
Cotellic
Crinone Cyramza Daklinza
Daliresp
Darzalex Doxepin Duopa Dysport Empliciti Epclusa Epogen
Erivedge Esbriet Estradiol
Extavia Farydak
Fentanyl Oral Fentora
Firazyr Forteo Gattex Genotropin
Gilenya Giltorif Glassia Harvoni Hetlioz Humatrope Ibrance Iclusig Idhifa
Ilaris
Imbruvica Imfinzi
Imipramine
Increlex Inflectra Inlyta Jakafi Juxtapid Kalydeco
Kanuma Kineret Kisqali Korlym Kuvan Kynamro Kyprolis Lartruvo
Lazanda
Lenvima Letairis Lidocaine Transdermal Linzess Lonsurf Lynparza Mavyret Mekinist Menest Methamphetamine
Modafinil Movantik
Mozobil Myalept Natapara
Nexavar
Nerlynx
Ninlaro Norditropin Novarel Nuplazid Nutropin Nutropin Aq Odomzo Ofev
Olysio Omnitrope Opsumit Orencia, Orencia Clickject Orenitram
Orkambi Otezla Oxandrolone
Oxymetholone Pegasys Peg-Intron Phenergan/Phenado Plegridy
Pomalyst Procrit Procysbi Prolastin C Prolia Promacta
Promethazine Promethegan Radicava
Ravicti Rebif
Relistor Remicade
Remodulin
Repatha Revatio
Revlimid Rubraca Rydapt
Saizen Samsca Serostim Sildenafil Simponi Sirturo Somavert Sovaldi Sprycel Stelara
Strensiq
Subsys Surmontil Sutent Sylatron Sylvant Symlin Tabloid
Tafinlar Tagrisso Tarceva Targretin Tasigna Tecentriq Tecfidera
Technivie
Testim Testosterone
Tetrabenazine
Thalomid
Thioridazine Topiramate Tracleer Treanda
Trimipramine Uptravi Vecamyl Vectibix
Venclexta Victoza
Viekira
Votrient Xalkori Xeljanz
Xgeva
Xolair Xtandi Xyrem Yondelis
Yervoy
Zaleplon
Zelboraf Zemaira Zejula Zepatier Zolinza Zonisamide
Zorbtive Zurampic Zydelig Zykadia
Zytiga
H5883_Ph_Nov17PAlist_NM 10262017
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
2 of 99
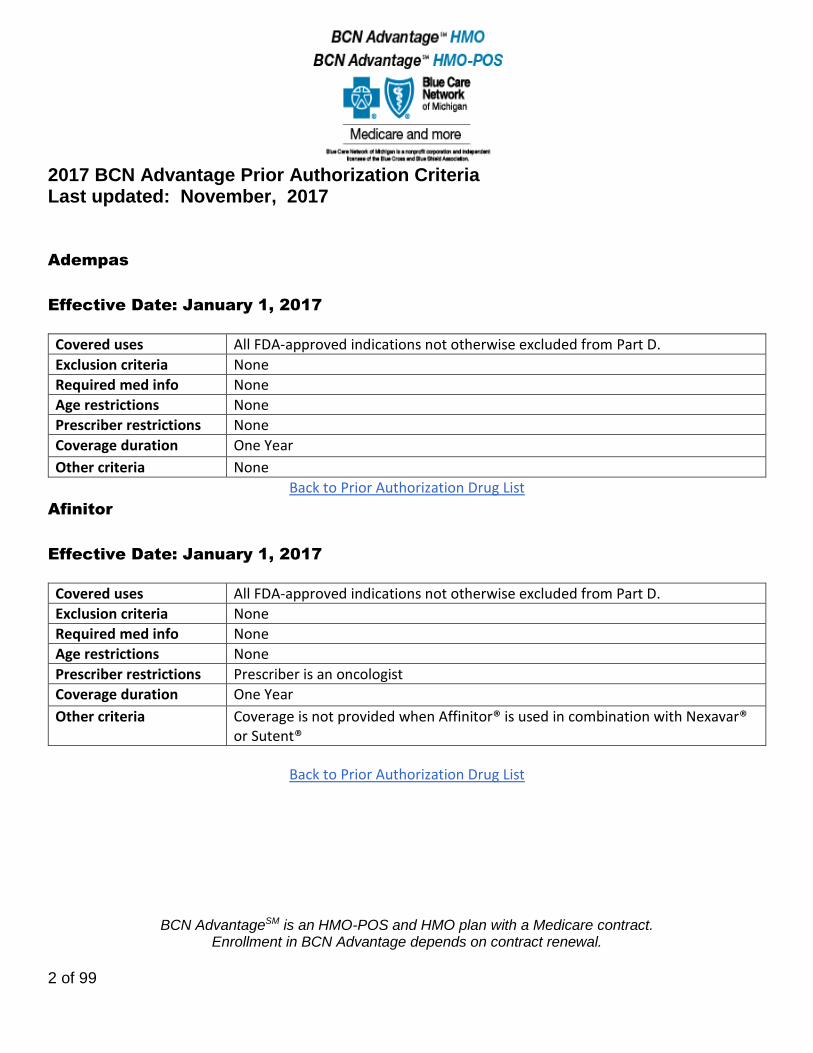
Adempas
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Afinitor
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescriber is an oncologist
Coverage duration One Year
Other criteria Coverage is not provided when Affinitor® is used in combination with Nexavar® or Sutent®
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
3 of 99
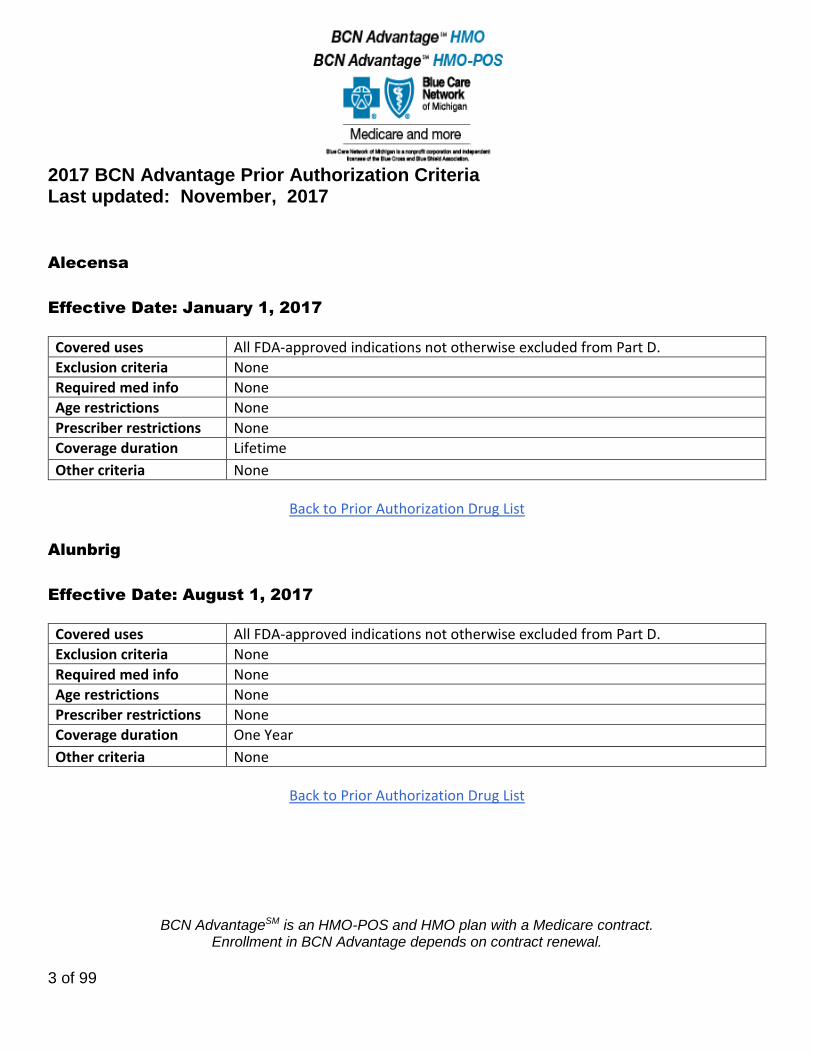
Alecensa
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Alunbrig
Effective Date: August 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
4 of 99
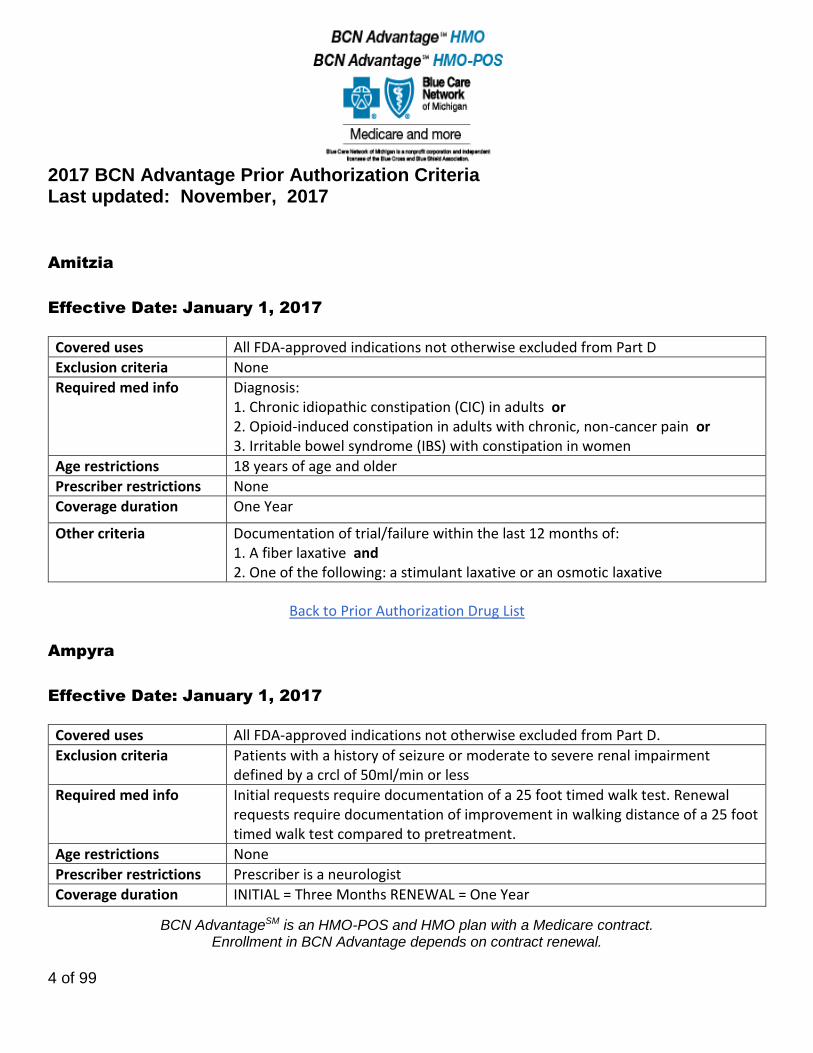
Amitzia
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis: 1. Chronic idiopathic constipation (CIC) in adults or 2. Opioid-induced constipation in adults with chronic, non-cancer pain or 3. Irritable bowel syndrome (IBS) with constipation in women
Age restrictions 18 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Documentation of trial/failure within the last 12 months of: 1. A fiber laxative and 2. One of the following: a stimulant laxative or an osmotic laxative
Back to Prior Authorization Drug List
Ampyra
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria Patients with a history of seizure or moderate to severe renal impairment defined by a crcl of 50ml/min or less
Required med info Initial requests require documentation of a 25 foot timed walk test. Renewal requests require documentation of improvement in walking distance of a 25 foot timed walk test compared to pretreatment.
Age restrictions None
Prescriber restrictions Prescriber is a neurologist
Coverage duration INITIAL = Three Months RENEWAL = One Year
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
5 of 99
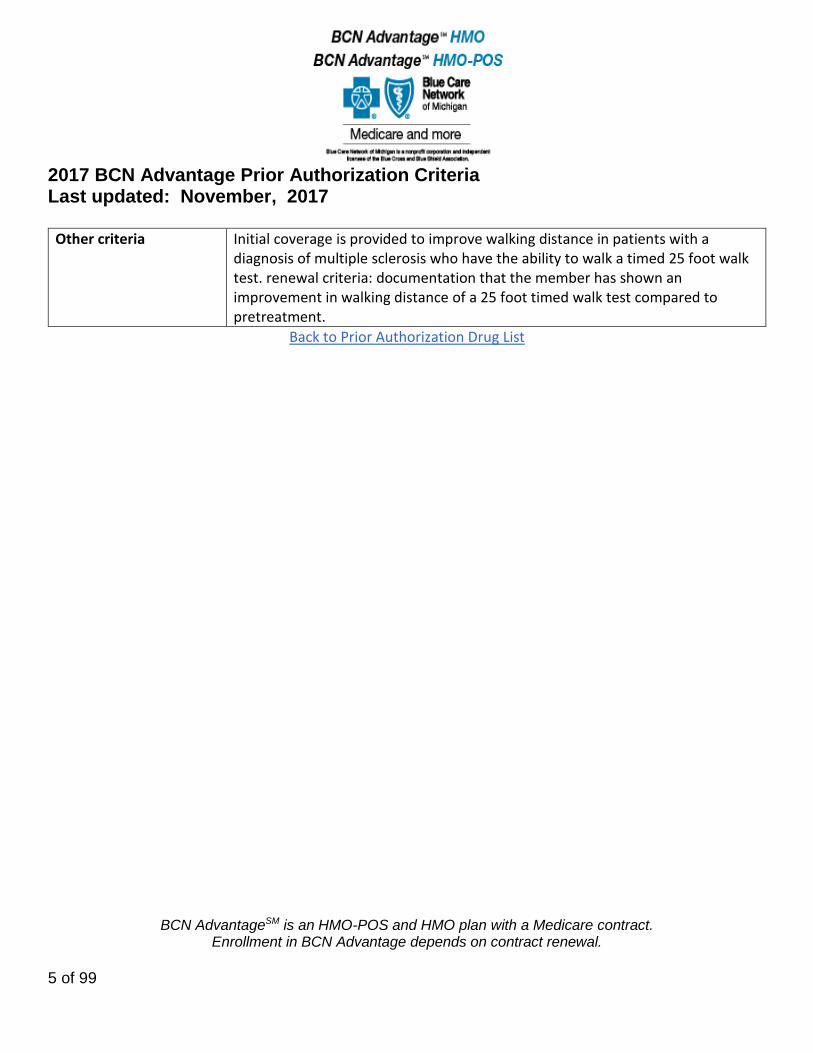
Other criteria Initial coverage is provided to improve walking distance in patients with a diagnosis of multiple sclerosis who have the ability to walk a timed 25 foot walk test. renewal criteria: documentation that the member has shown an improvement in walking distance of a 25 foot timed walk test compared to pretreatment.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
6 of 99
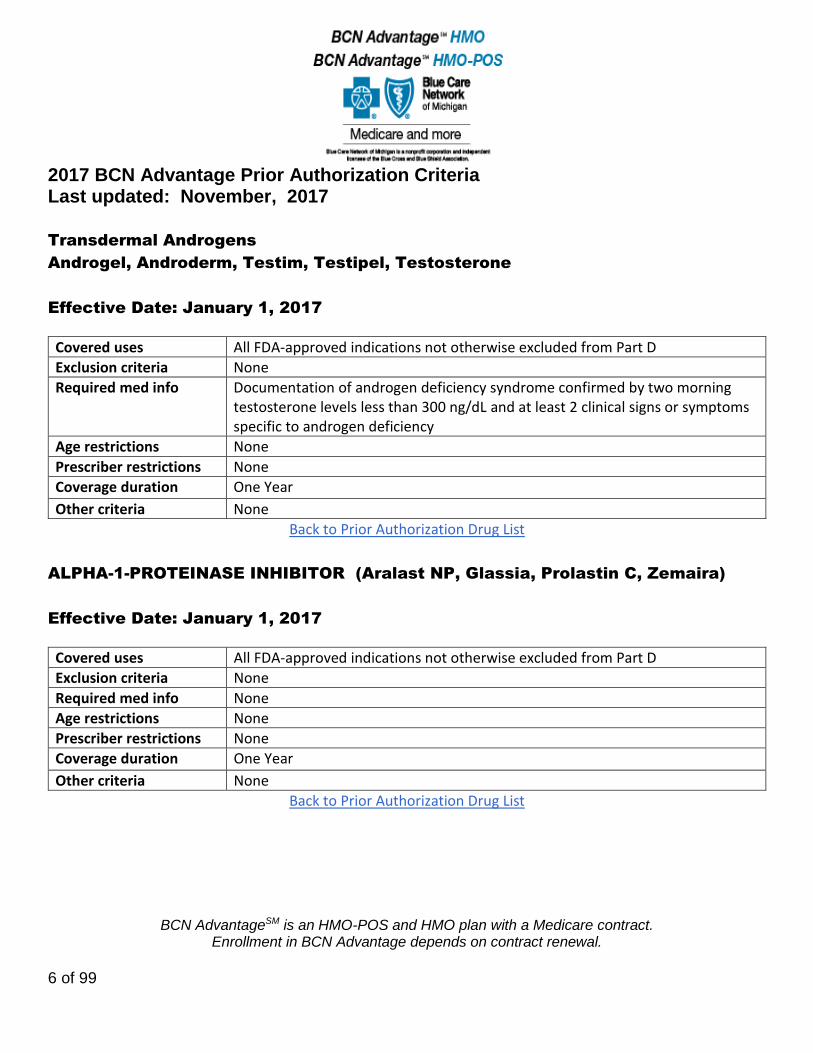
Transdermal Androgens
Androgel, Androderm, Testim, Testipel, Testosterone
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Documentation of androgen deficiency syndrome confirmed by two morning testosterone levels less than 300 ng/dL and at least 2 clinical signs or symptoms specific to androgen deficiency
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
ALPHA-1-PROTEINASE INHIBITOR (Aralast NP, Glassia, Prolastin C, Zemaira)
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
7 of 99
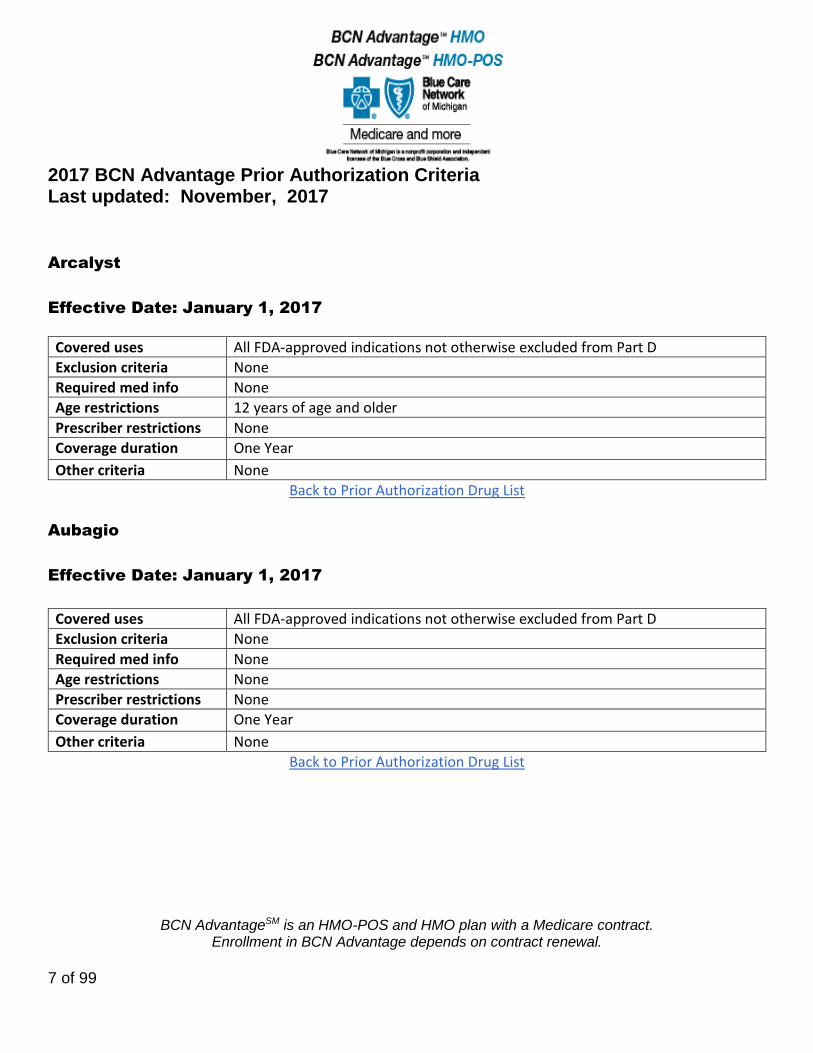
Arcalyst
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions 12 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Aubagio
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
8 of 99
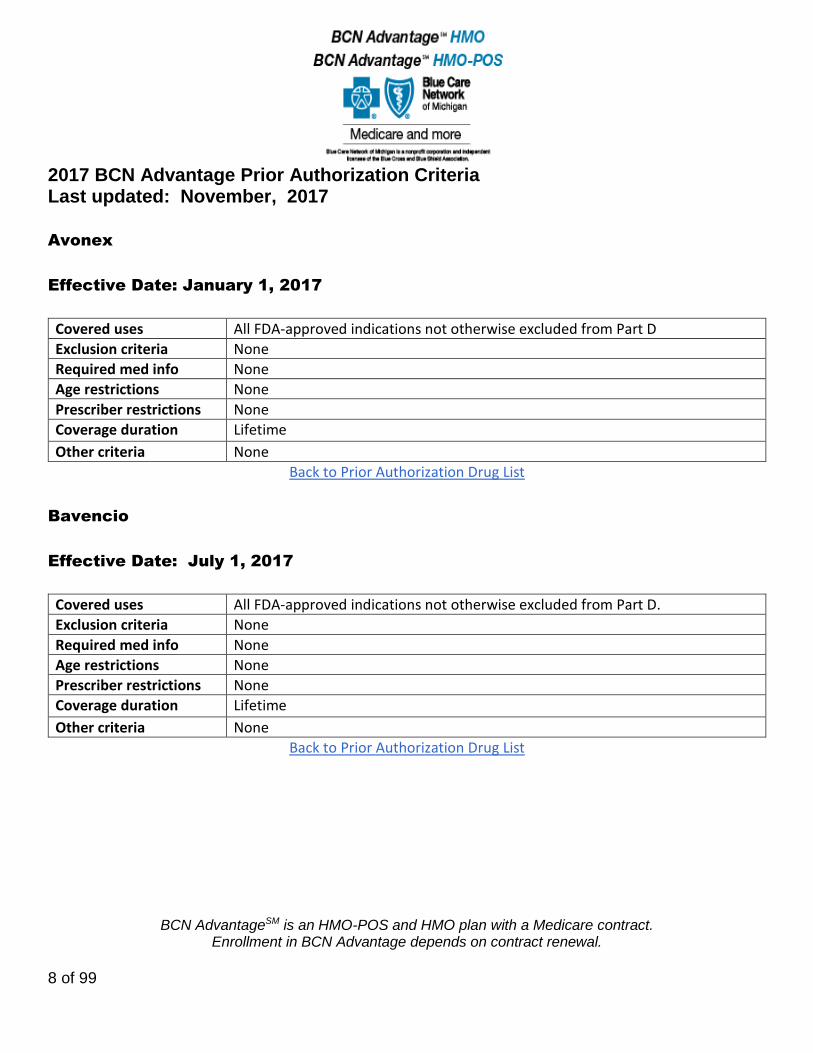
Avonex
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Bavencio
Effective Date: July 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
9 of 99
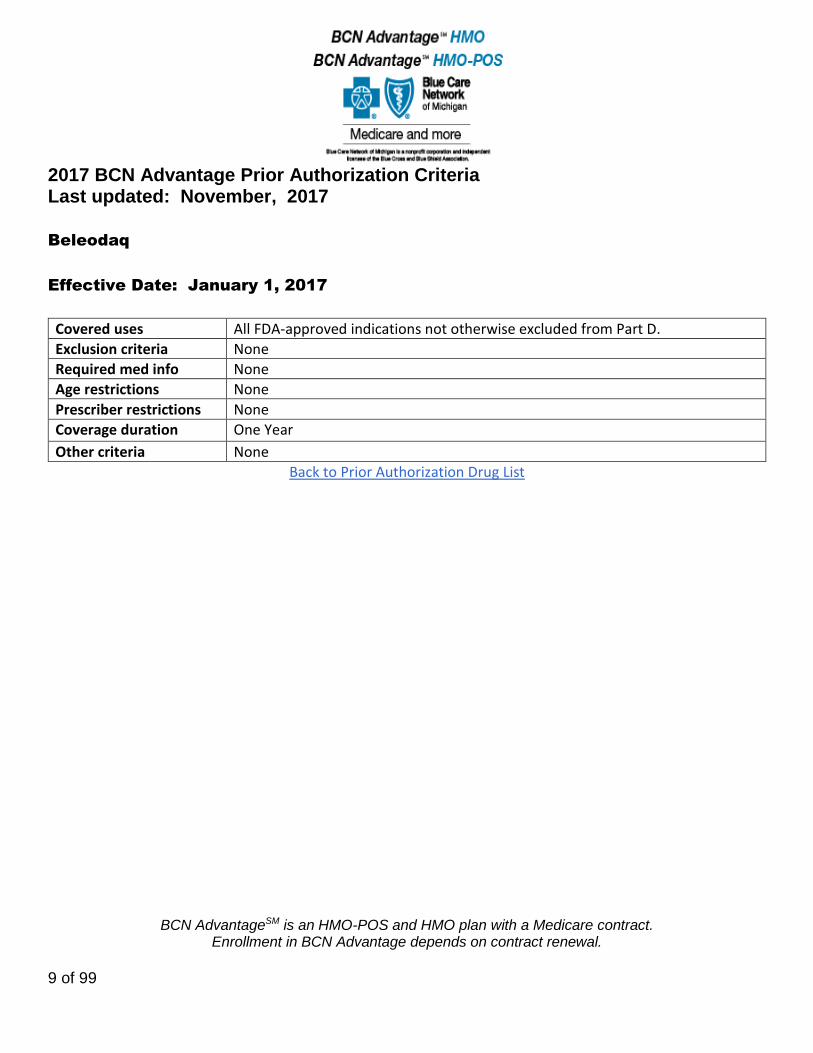
Beleodaq
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
10 of 99
Berinert
Effective Date: January 1, 2017
Covered uses For acute attacks of hereditary angioedema (HAE). All FDAapproved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions 13 years or older.
Prescriber restrictions None
Coverage duration One Year
Other criteria Diagnosis of hereditary angioedema (HAE) established by an immunologist or hematologist
Back to Prior Authorization Drug List
Betaseron
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
11 of 99
Bosulif
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Briviact
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
12 of 99
Cabometyx
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Cayston
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Cayston is subject to Part B versus Part D coverage review
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
13 of 99
Cholbam
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Chorionic Gonadotropin
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
14 of 99
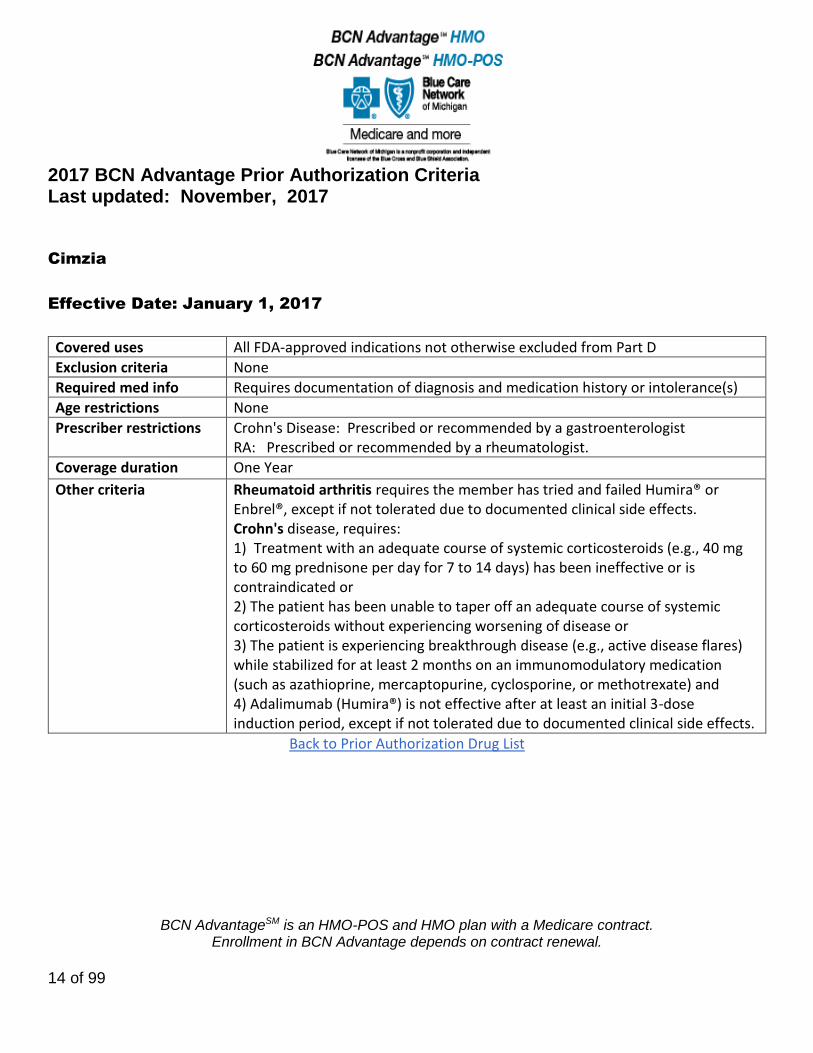
Cimzia
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Requires documentation of diagnosis and medication history or intolerance(s)
Age restrictions None
Prescriber restrictions Crohn's Disease: Prescribed or recommended by a gastroenterologist RA: Prescribed or recommended by a rheumatologist.
Coverage duration One Year
Other criteria Rheumatoid arthritis requires the member has tried and failed Humira® or Enbrel®, except if not tolerated due to documented clinical side effects. Crohn's disease, requires: 1) Treatment with an adequate course of systemic corticosteroids (e.g., 40 mg to 60 mg prednisone per day for 7 to 14 days) has been ineffective or is contraindicated or 2) The patient has been unable to taper off an adequate course of systemic corticosteroids without experiencing worsening of disease or 3) The patient is experiencing breakthrough disease (e.g., active disease flares) while stabilized for at least 2 months on an immunomodulatory medication (such as azathioprine, mercaptopurine, cyclosporine, or methotrexate) and 4) Adalimumab (Humira®) is not effective after at least an initial 3-dose induction period, except if not tolerated due to documented clinical side effects.
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
15 of 99
Cinryze
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by an immunologist, allergist, or rheumatologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Cometriq
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
16 of 99
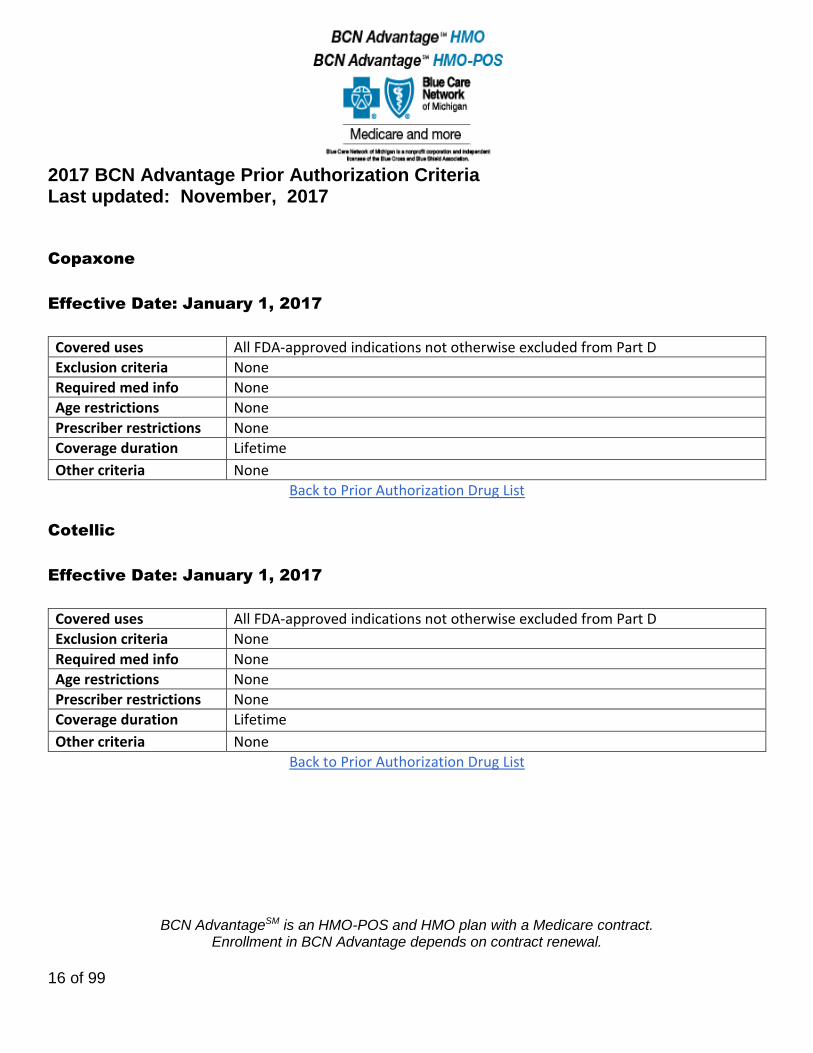
Copaxone
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Cotellic
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
17 of 99
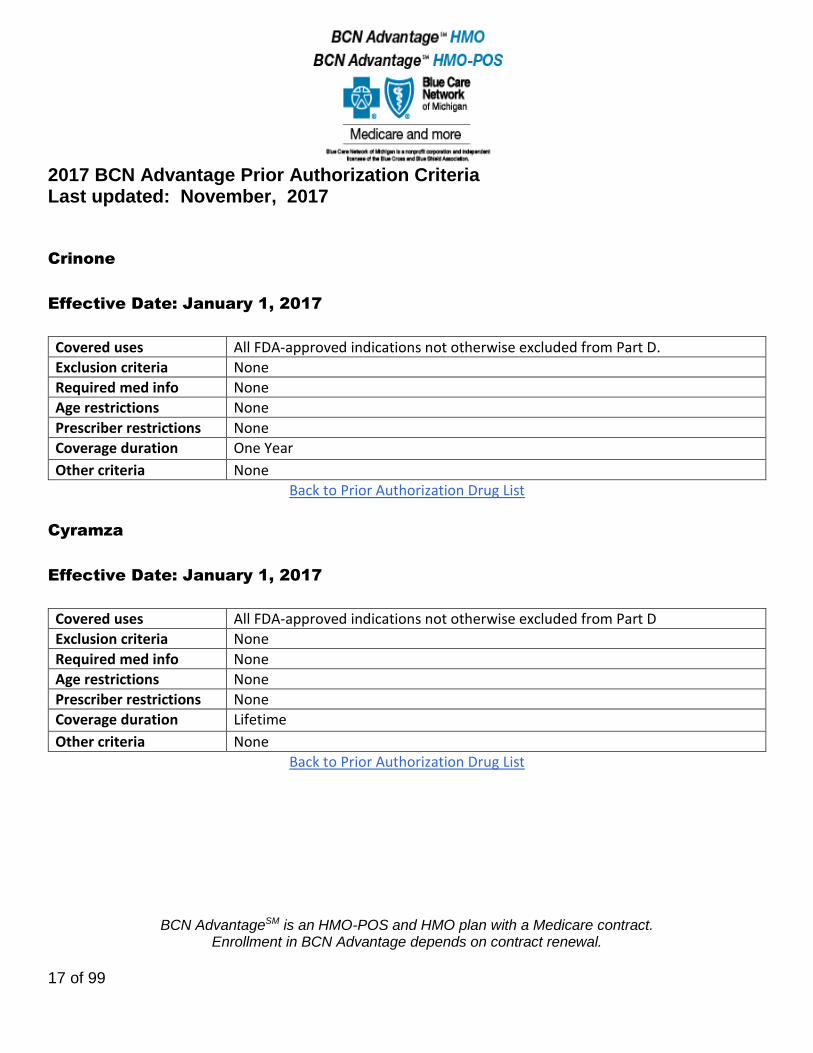
Crinone
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Cyramza
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
18 of 99
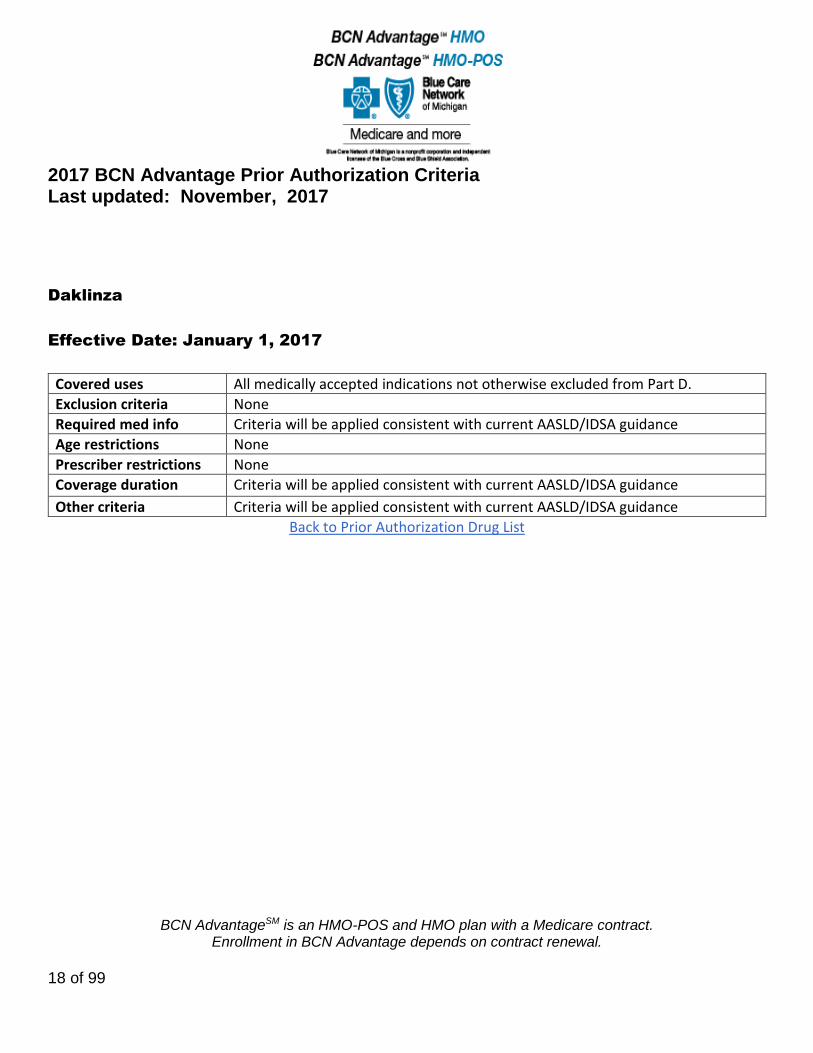
Daklinza
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Criteria will be applied consistent with current AASLD/IDSA guidance
Age restrictions None
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
19 of 99
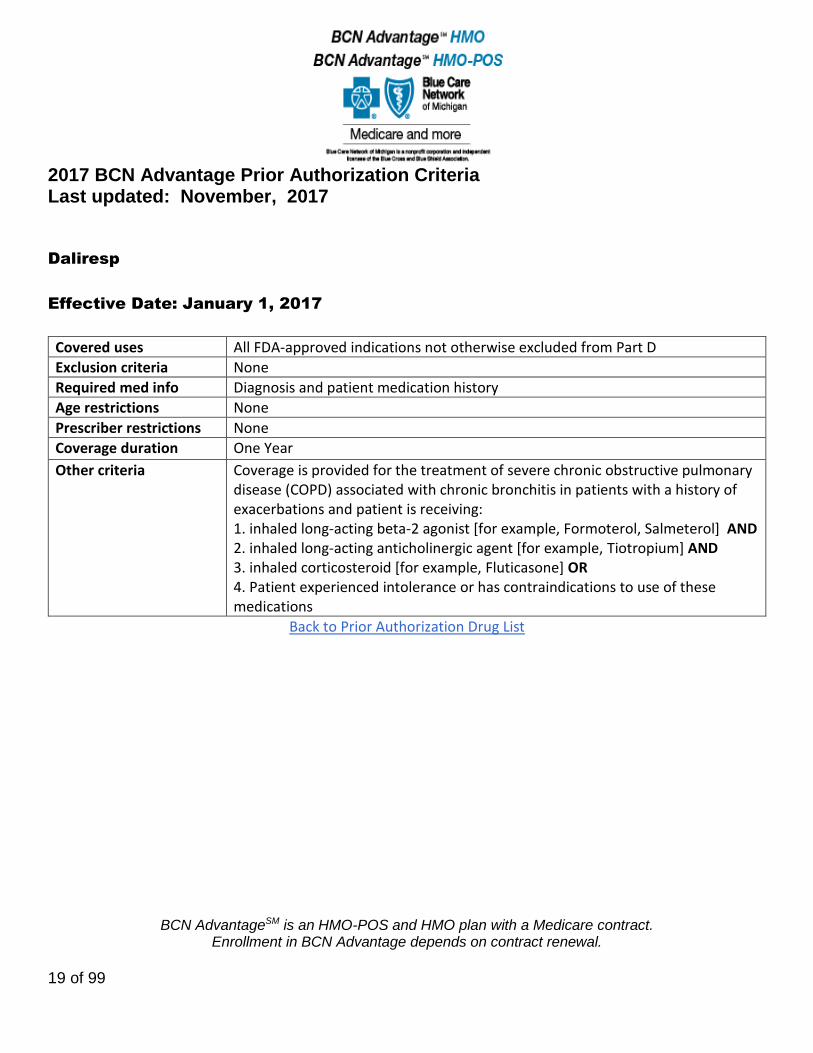
Daliresp
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis and patient medication history
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Coverage is provided for the treatment of severe chronic obstructive pulmonary disease (COPD) associated with chronic bronchitis in patients with a history of exacerbations and patient is receiving: 1. inhaled long-acting beta-2 agonist [for example, Formoterol, Salmeterol] AND 2. inhaled long-acting anticholinergic agent [for example, Tiotropium] AND 3. inhaled corticosteroid [for example, Fluticasone] OR 4. Patient experienced intolerance or has contraindications to use of these medications
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
20 of 99
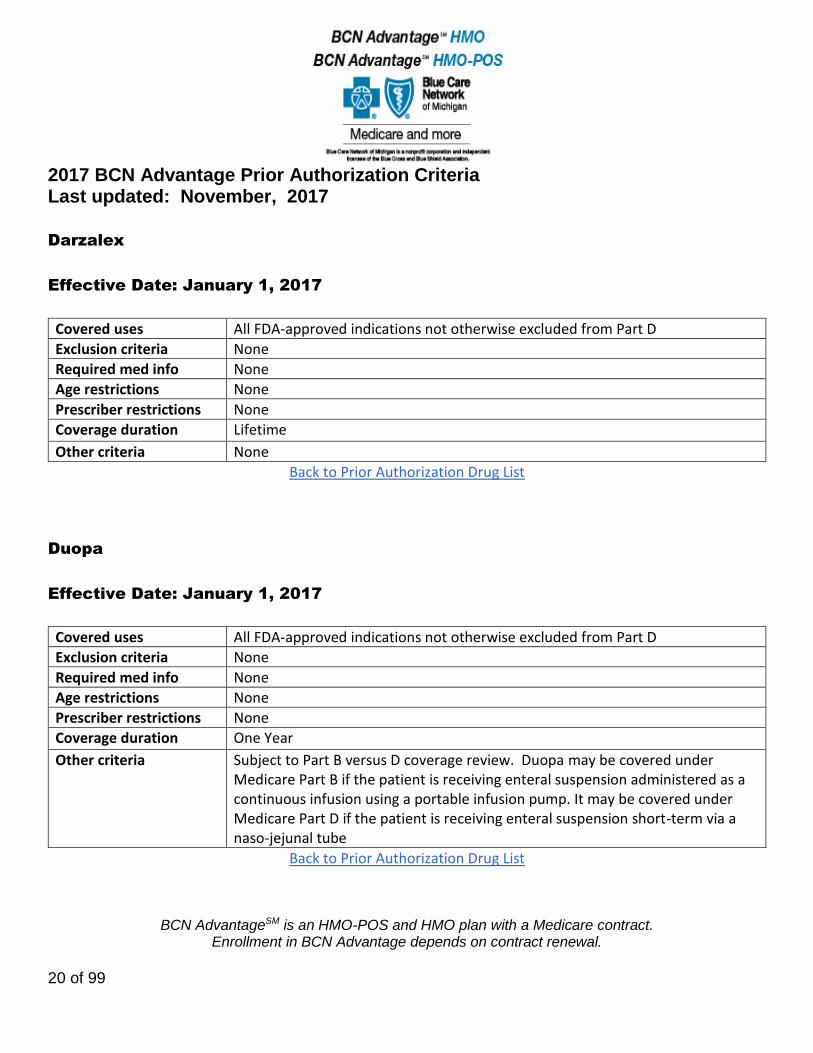
Darzalex
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Duopa
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Subject to Part B versus D coverage review. Duopa may be covered under Medicare Part B if the patient is receiving enteral suspension administered as a continuous infusion using a portable infusion pump. It may be covered under Medicare Part D if the patient is receiving enteral suspension short-term via a naso-jejunal tube
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
21 of 99
Dysport
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Will not be covered for cosmetic purposes
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Empliciti
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
22 of 99
Epclusa
Effective Date: March 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info CRITERIA WILL BE APPLIED CONSISTENT WITH CURRENT AASLD/IDSA GUIDANCE
Age restrictions None
Prescriber restrictions None
Coverage duration CRITERIA WILL BE APPLIED CONSISTENT WITH CURRENT AASLD/IDSA GUIDANCE
Other criteria CRITERIA WILL BE APPLIED CONSISTENT WITH CURRENT AASLD/IDSA GUIDANCE
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
23 of 99
Erythropoesis Stimulating Agents:
Arnesp, Epogen, Procrit
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria Anemia due to folate, vitamin b12, iron deficiencies, hemolysis, bleeding, or bone marrow fibrosis. Anemia associated with treatment of acute and chronic myelogenous leukemias or erythroid cancers. Anemia due to cancer treatment in patients with uncontrolled hypertension. Anemia not associated with cancer treatment or renal disease under inclusions. Anemia associated only with radiotherapy. Prophylactic use to prevent chemotherapy induced anemia. Prophylactic use to reduce tumor hypoxia. Erythropoietin-type resistance due to neutralizing antibodies.
Required med info
Age restrictions
Prescriber restrictions
Coverage duration 3 months
Other criteria Erythropoesis stimulating agents are subject to Part B vs Part D review.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
24 of 99
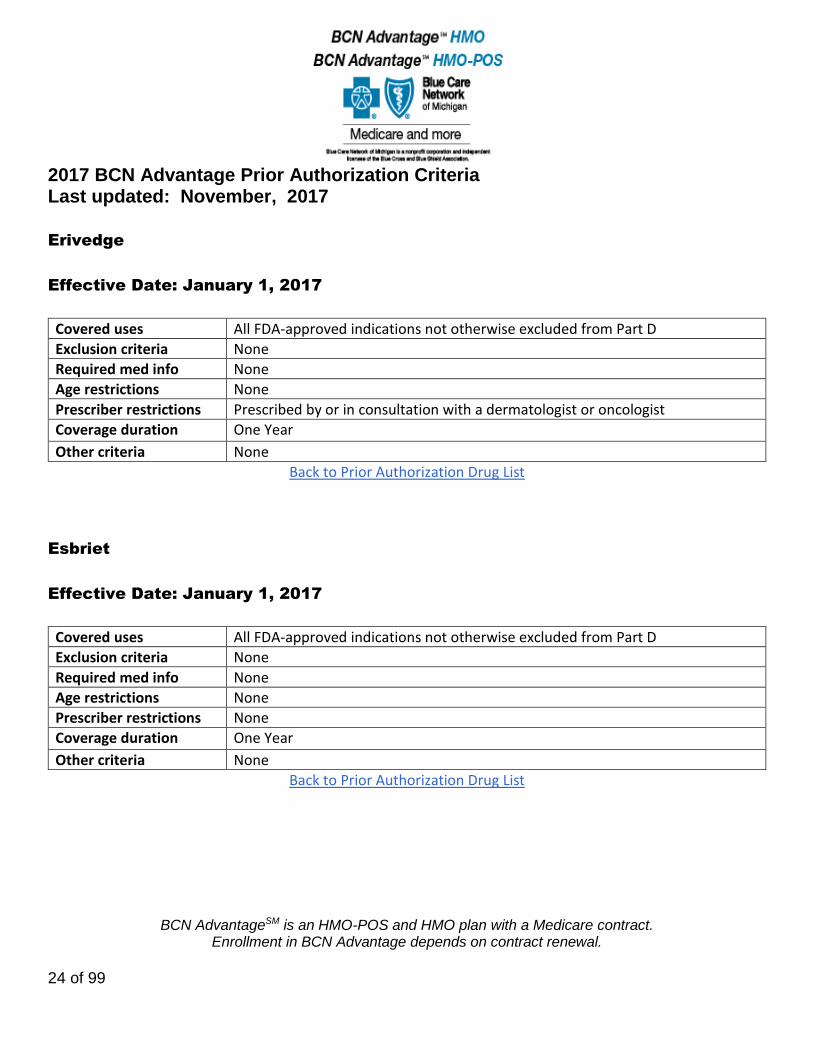
Erivedge
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by or in consultation with a dermatologist or oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Esbriet
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
25 of 99
Estrogens (Estradiol, Menest)
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions Authorization is required for members 65 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Oral Estrogen (Menest) will be approved when used as part of a cancer treatment regimen. For all other uses, Menest will be approved if two of the following safer alternatives as been tried and failed or are not appropriate or contraindicated. Safer alternatives include: e.g., SSRIs, venlafaxine ER, Premarin vaginal cream, Estrace vaginal creams, Estring or Femring Vaginal Rings, Vagifem vaginal tablets
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
26 of 99
Extavia
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Farydak
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
27 of 99
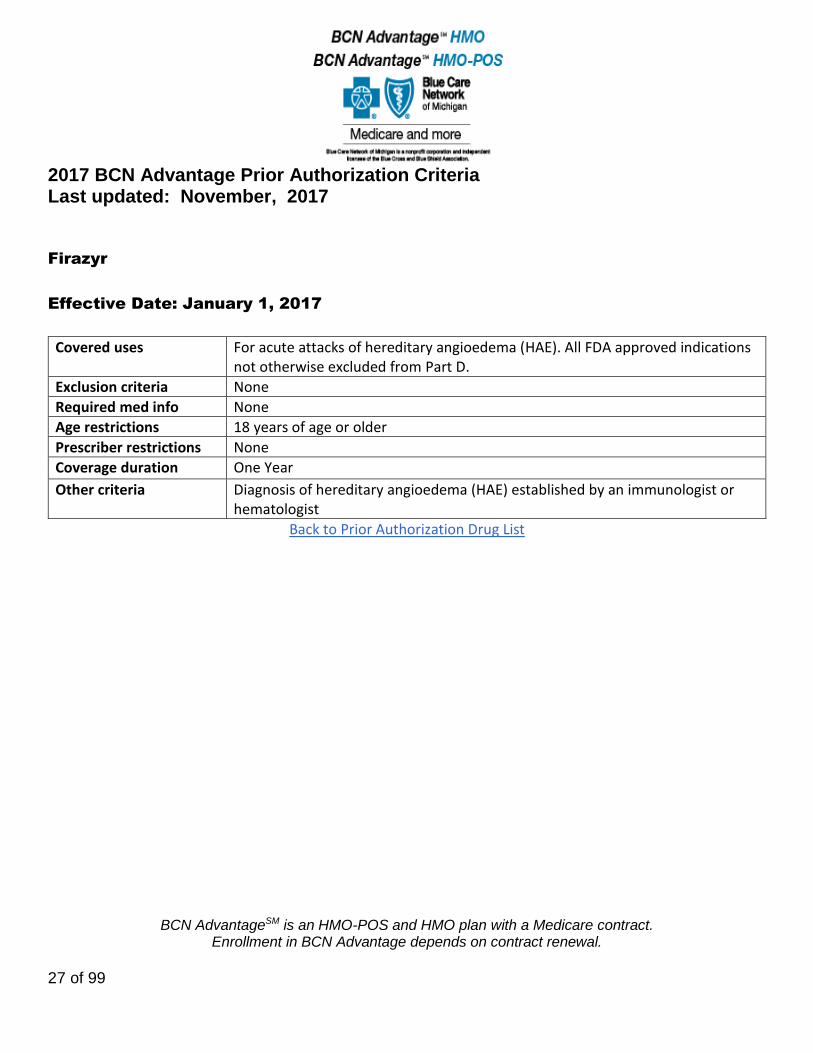
Firazyr
Effective Date: January 1, 2017
Covered uses For acute attacks of hereditary angioedema (HAE). All FDA approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions 18 years of age or older
Prescriber restrictions None
Coverage duration One Year
Other criteria Diagnosis of hereditary angioedema (HAE) established by an immunologist or hematologist
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
28 of 99
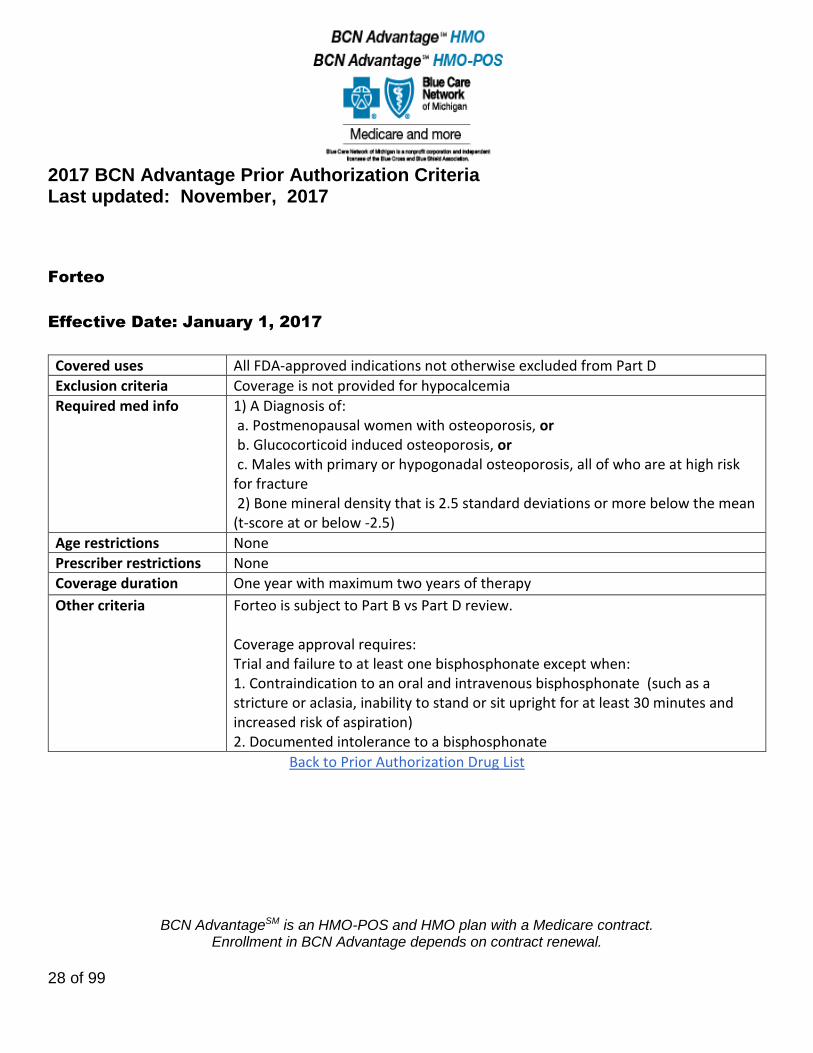
Forteo
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Coverage is not provided for hypocalcemia
Required med info 1) A Diagnosis of: a. Postmenopausal women with osteoporosis, or b. Glucocorticoid induced osteoporosis, or c. Males with primary or hypogonadal osteoporosis, all of who are at high risk for fracture 2) Bone mineral density that is 2.5 standard deviations or more below the mean (t-score at or below -2.5)
Age restrictions None
Prescriber restrictions None
Coverage duration One year with maximum two years of therapy
Other criteria Forteo is subject to Part B vs Part D review. Coverage approval requires: Trial and failure to at least one bisphosphonate except when: 1. Contraindication to an oral and intravenous bisphosphonate (such as a stricture or aclasia, inability to stand or sit upright for at least 30 minutes and increased risk of aspiration) 2. Documented intolerance to a bisphosphonate
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
29 of 99
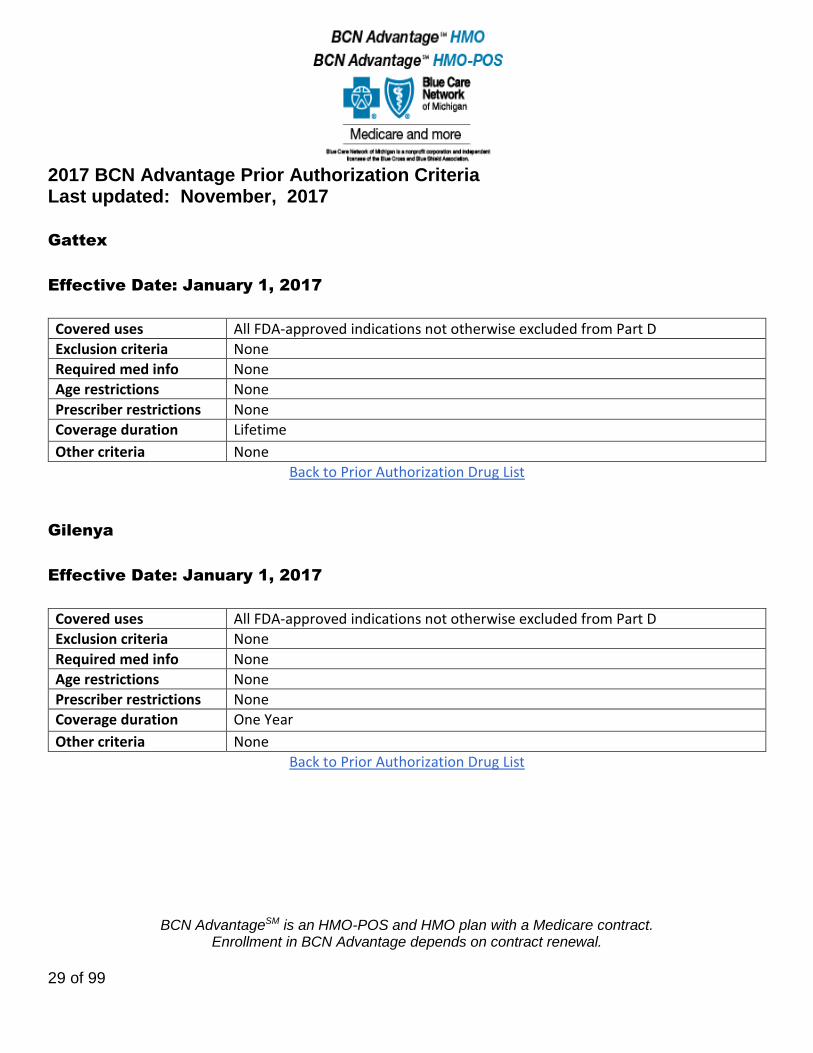
Gattex
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Gilenya
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
30 of 99
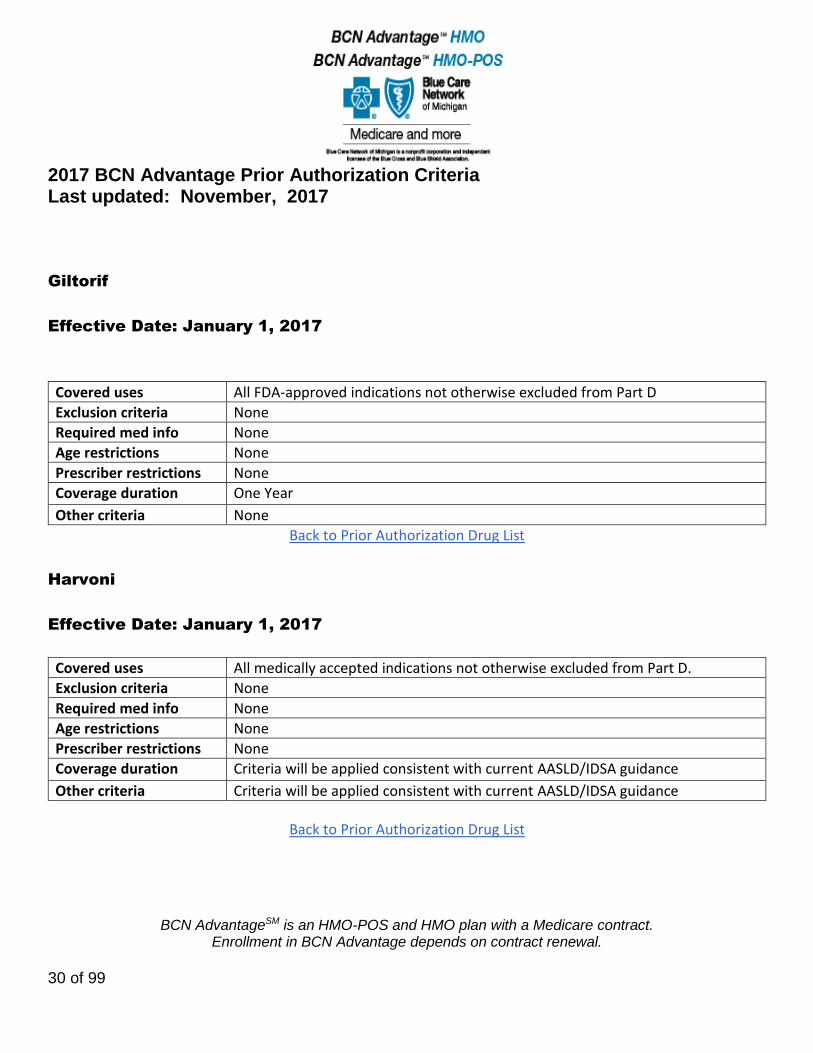
Giltorif
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Harvoni
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
31 of 99
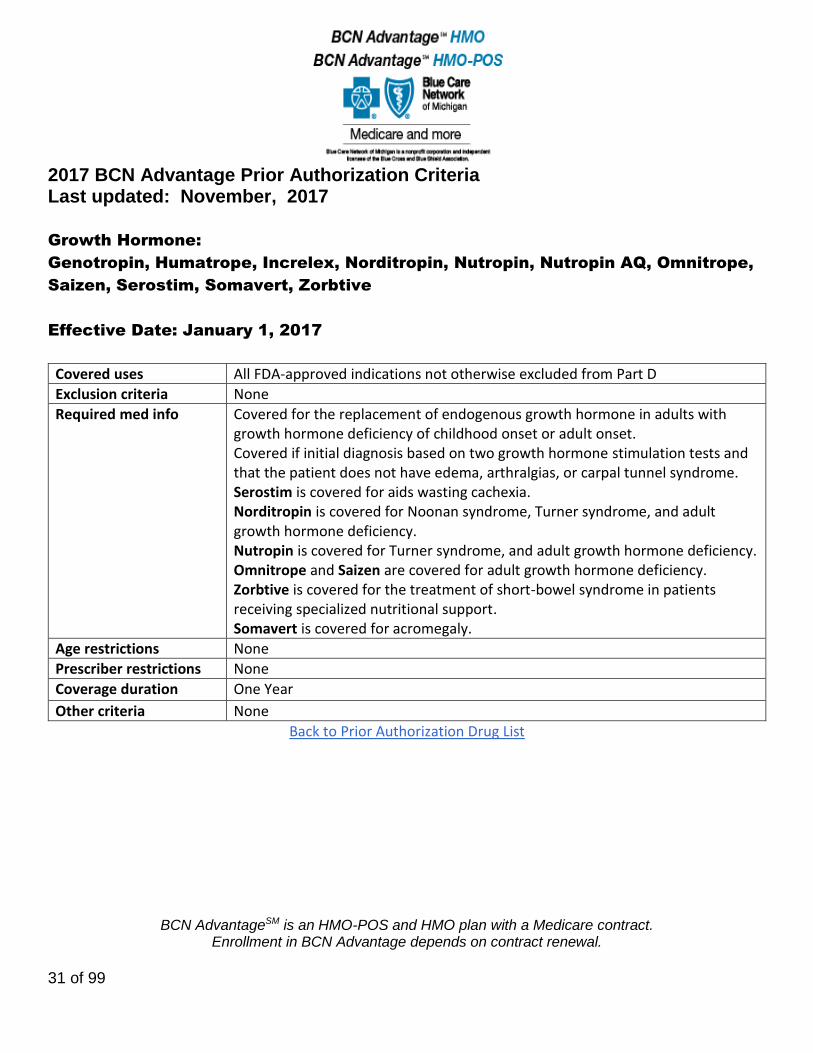
Growth Hormone:
Genotropin, Humatrope, Increlex, Norditropin, Nutropin, Nutropin AQ, Omnitrope,
Saizen, Serostim, Somavert, Zorbtive
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Covered for the replacement of endogenous growth hormone in adults with growth hormone deficiency of childhood onset or adult onset. Covered if initial diagnosis based on two growth hormone stimulation tests and that the patient does not have edema, arthralgias, or carpal tunnel syndrome. Serostim is covered for aids wasting cachexia. Norditropin is covered for Noonan syndrome, Turner syndrome, and adult growth hormone deficiency. Nutropin is covered for Turner syndrome, and adult growth hormone deficiency. Omnitrope and Saizen are covered for adult growth hormone deficiency. Zorbtive is covered for the treatment of short-bowel syndrome in patients receiving specialized nutritional support. Somavert is covered for acromegaly.
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
32 of 99
Hetlioz
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Documentation of patient visual capabilities
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
33 of 99
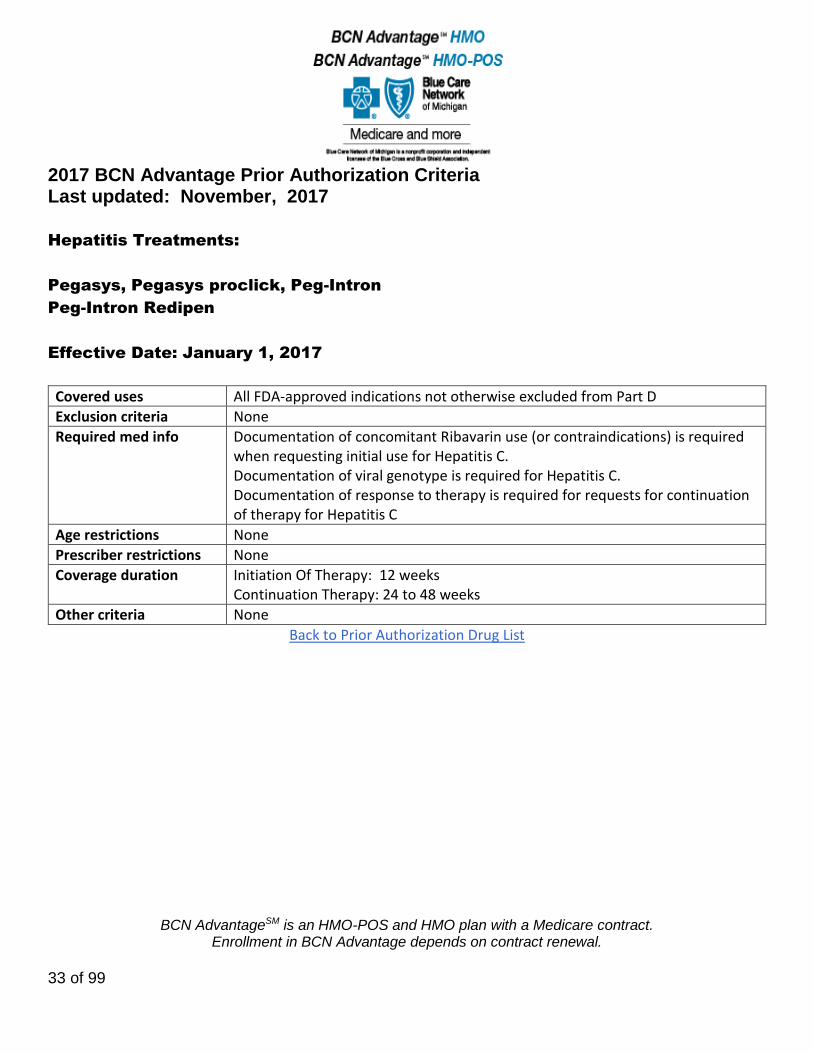
Hepatitis Treatments:
Pegasys, Pegasys proclick, Peg-Intron
Peg-Intron Redipen
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Documentation of concomitant Ribavarin use (or contraindications) is required when requesting initial use for Hepatitis C. Documentation of viral genotype is required for Hepatitis C. Documentation of response to therapy is required for requests for continuation of therapy for Hepatitis C
Age restrictions None
Prescriber restrictions None
Coverage duration Initiation Of Therapy: 12 weeks Continuation Therapy: 24 to 48 weeks
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
34 of 99
High Risk in the Elderly Medications:
Tricyclic Antidepressants: Amitriptyline, Clomipramine, Doxepin, Imipramine,
Trimipramine
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions Authorization is required for formulary high risk medications for members 65 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria High Risk Tricyclic Antidepressants are approved if patient has a history of use. For patients initiating therapy, the high risk tricyclic antidepressant is approved if at least one of the suggested alternatives (nortriptyline, desipramine, citalopram, escitalopram, mirtazapine, sertraline, venlafaxine) with less sedation and fewer anticholinergic effects have been tried and failed or is not appropriate or contraindicated for the intended use.
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
35 of 99
High Risk in the Elderly Medications:
Zaleplon
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions Authorization is required for formulary high risk medications for members 65 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Lunesta (Zaleplon) is approved if at least one of the suggested alternatives, (low dose Trazodone (25-50mg) or Rozerem), has been tried and failed or is not appropriate or contraindicated for the intended use.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
36 of 99
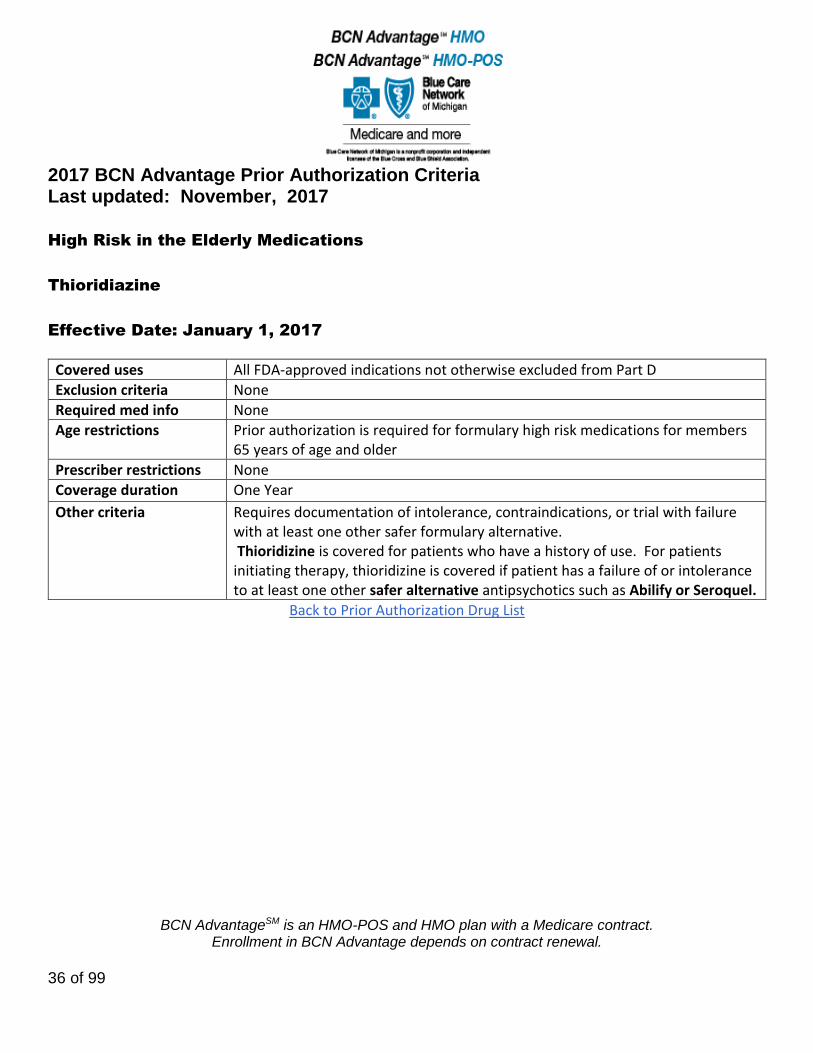
High Risk in the Elderly Medications
Thioridiazine
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions Prior authorization is required for formulary high risk medications for members 65 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Requires documentation of intolerance, contraindications, or trial with failure with at least one other safer formulary alternative. Thioridizine is covered for patients who have a history of use. For patients initiating therapy, thioridizine is covered if patient has a failure of or intolerance to at least one other safer alternative antipsychotics such as Abilify or Seroquel.
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
37 of 99
Ibrance
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Iclusig
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
38 of 99
Idhifa
Effective Date: November 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Ilaris
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Requires documentation of diagnosis.
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
39 of 99
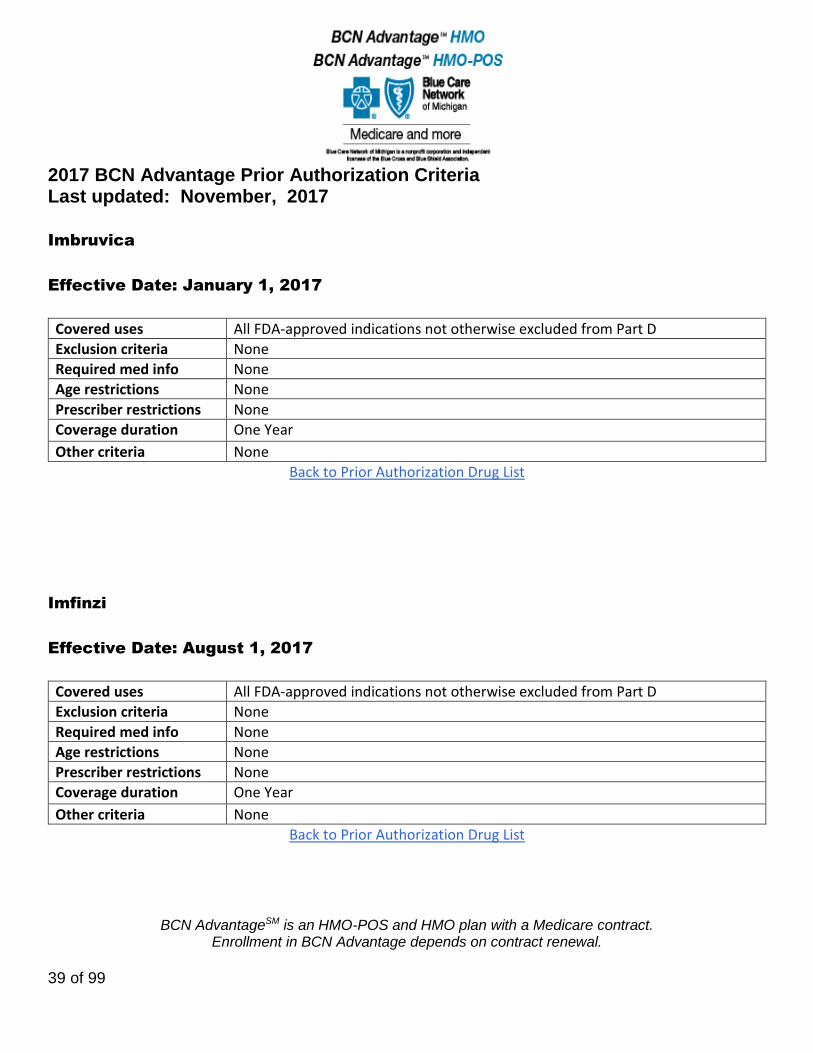
Imbruvica
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Imfinzi
Effective Date: August 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
40 of 99
Inflectra
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
41 of 99
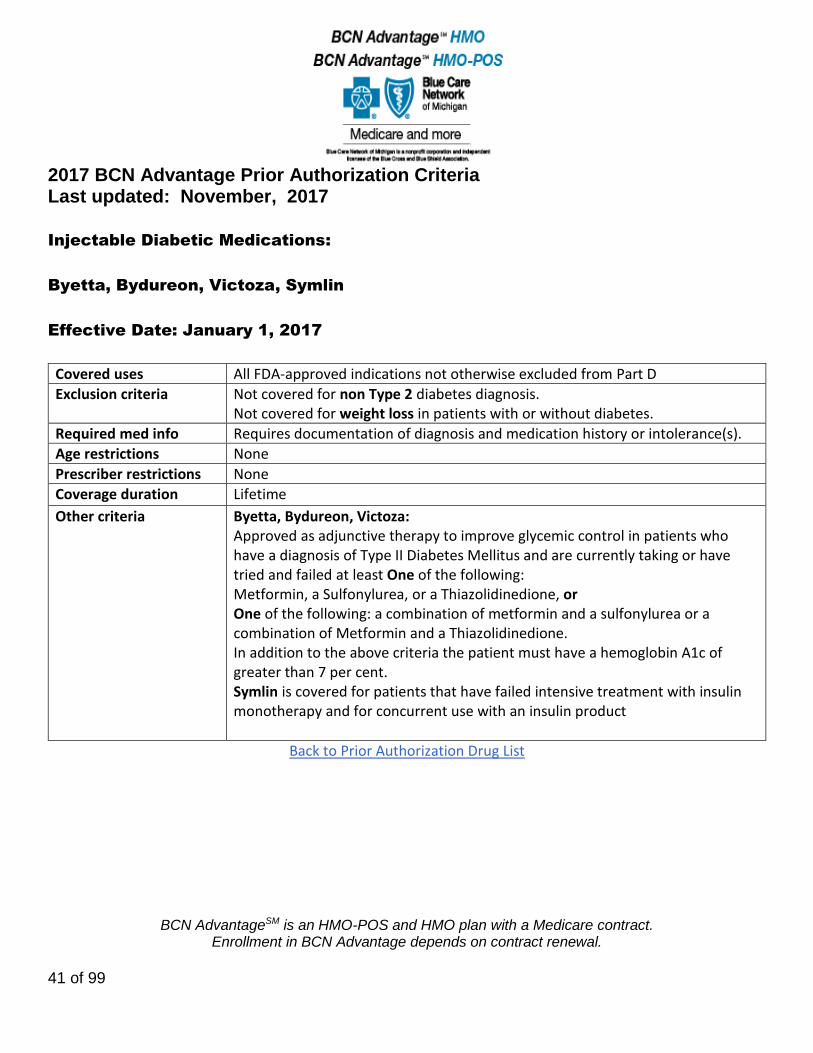
Injectable Diabetic Medications:
Byetta, Bydureon, Victoza, Symlin
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Not covered for non Type 2 diabetes diagnosis. Not covered for weight loss in patients with or without diabetes.
Required med info Requires documentation of diagnosis and medication history or intolerance(s).
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria Byetta, Bydureon, Victoza: Approved as adjunctive therapy to improve glycemic control in patients who have a diagnosis of Type II Diabetes Mellitus and are currently taking or have tried and failed at least One of the following: Metformin, a Sulfonylurea, or a Thiazolidinedione, or One of the following: a combination of metformin and a sulfonylurea or a combination of Metformin and a Thiazolidinedione. In addition to the above criteria the patient must have a hemoglobin A1c of greater than 7 per cent. Symlin is covered for patients that have failed intensive treatment with insulin monotherapy and for concurrent use with an insulin product
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
42 of 99
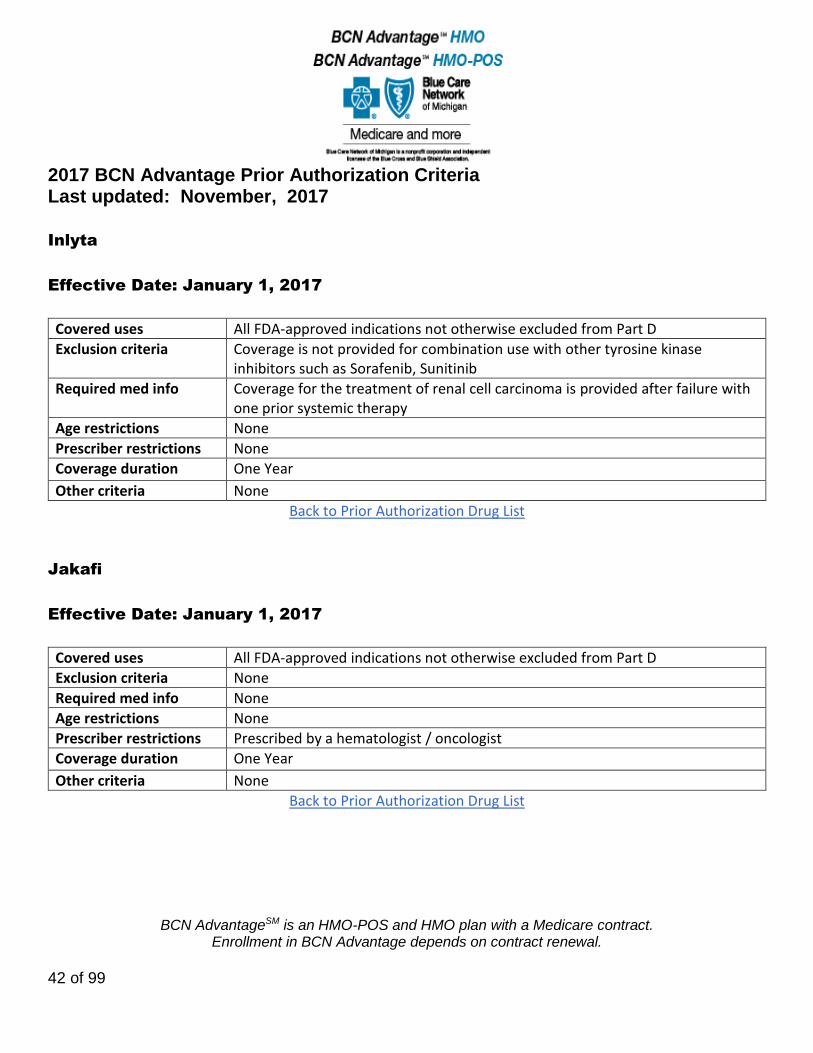
Inlyta
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Coverage is not provided for combination use with other tyrosine kinase inhibitors such as Sorafenib, Sunitinib
Required med info Coverage for the treatment of renal cell carcinoma is provided after failure with one prior systemic therapy
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Jakafi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by a hematologist / oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
43 of 99
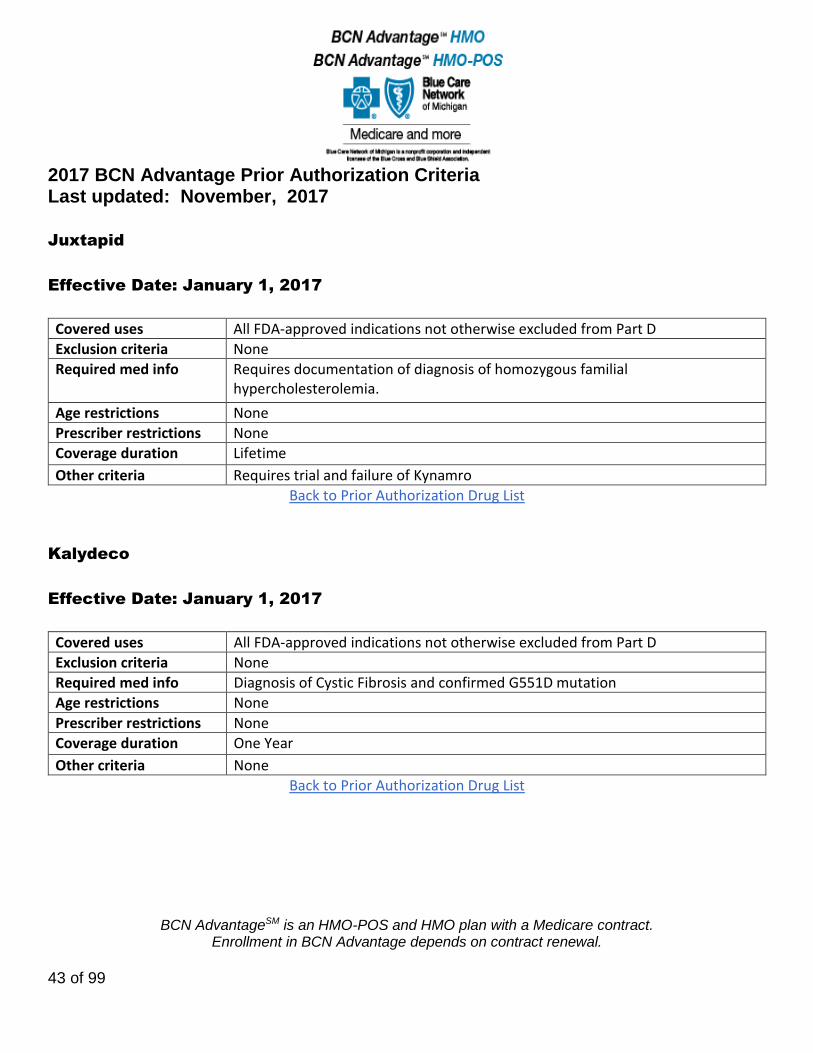
Juxtapid
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Requires documentation of diagnosis of homozygous familial hypercholesterolemia.
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria Requires trial and failure of Kynamro
Back to Prior Authorization Drug List
Kalydeco
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis of Cystic Fibrosis and confirmed G551D mutation
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
44 of 99
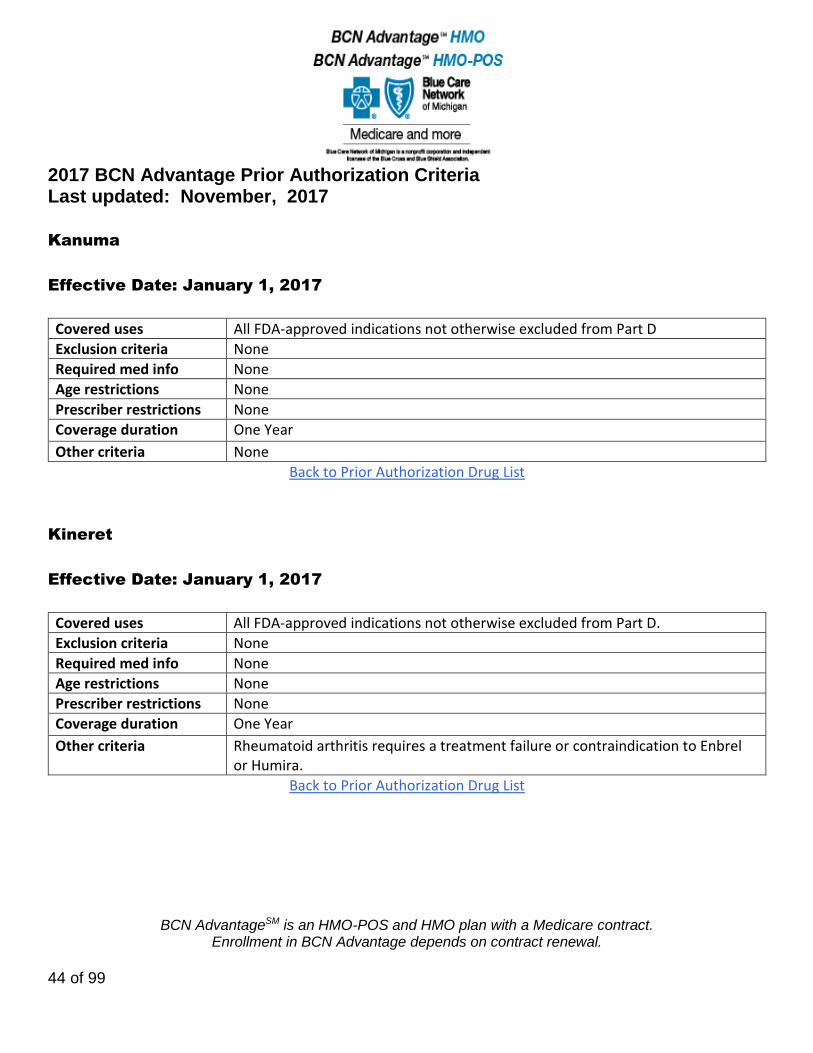
Kanuma
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Kineret
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Rheumatoid arthritis requires a treatment failure or contraindication to Enbrel or Humira.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
45 of 99
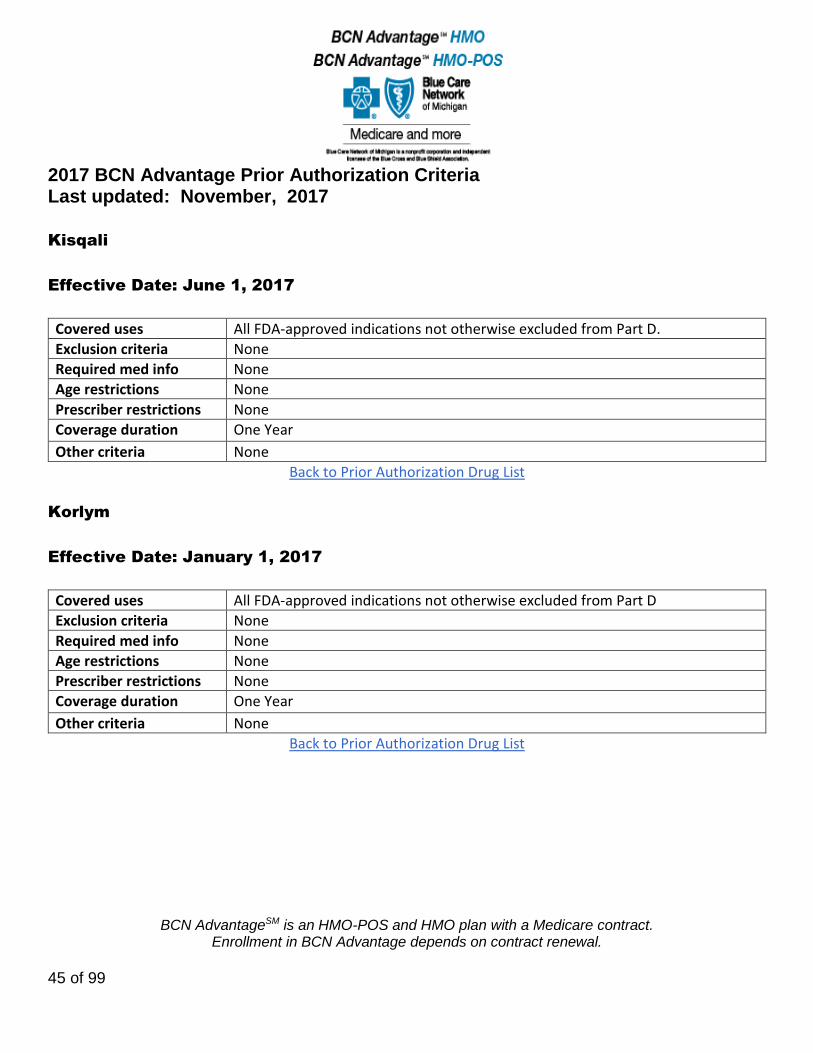
Kisqali
Effective Date: June 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Korlym
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
46 of 99
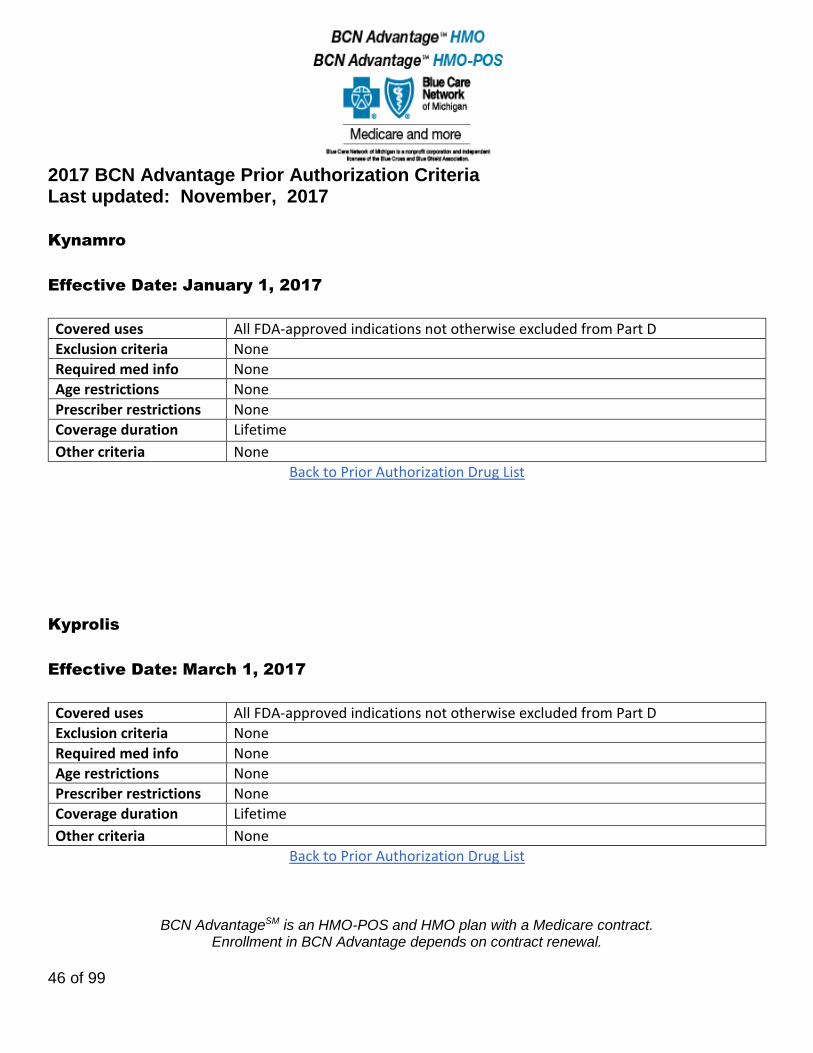
Kynamro
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Kyprolis
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
47 of 99
Lartruvo
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
48 of 99
Lenvima
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Lidocaine Transdermal Patch
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
49 of 99
Linzess
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions 18 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Chronic idiopathic constipation (CIC) requires documentation of failure within the last 12 months of use of a fiber laxative and one of the following: a stimulant laxative or an osmotic laxative. Drug-induced constipation must be ruled out.
Back to Prior Authorization Drug List
Lonsurf
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
50 of 99
Lynparza
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Mavyret
Effective Date: November 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
51 of 99
Mekinist
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Confirmation of the presence of BRAF V600E or V600K mutation in tumor specimen
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Methamphetamine HCL
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
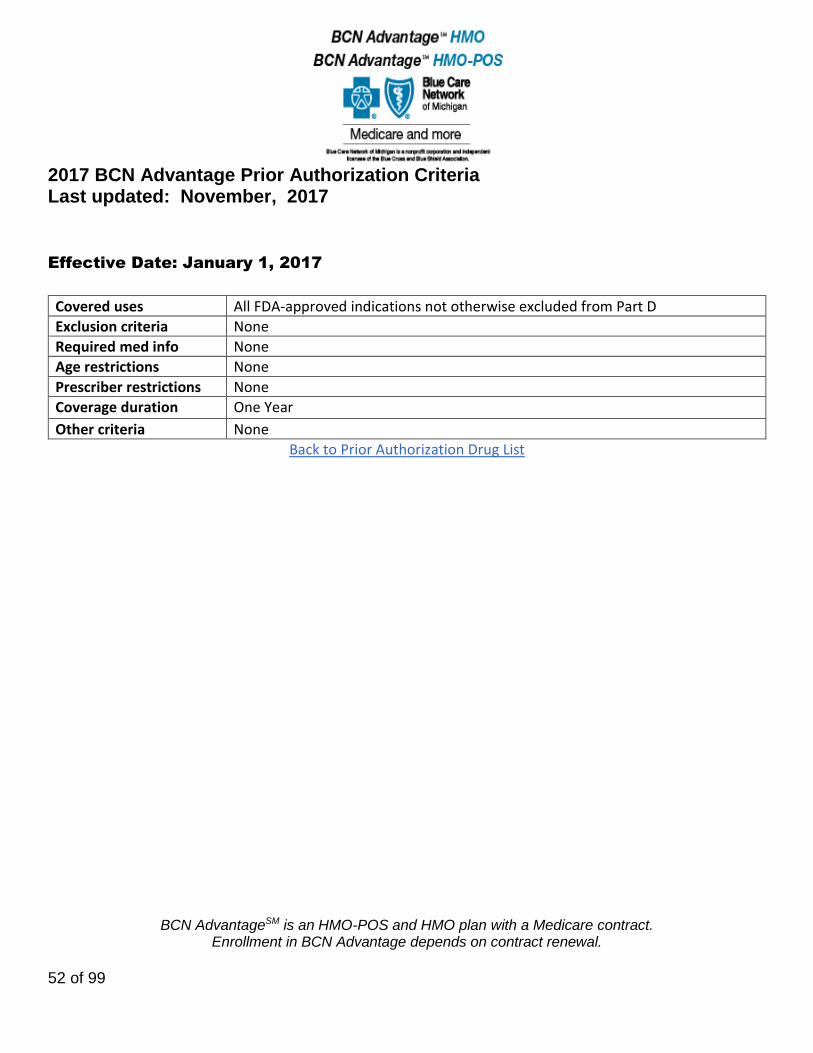
Modafinil, Armodafinil
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
52 of 99
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
53 of 99
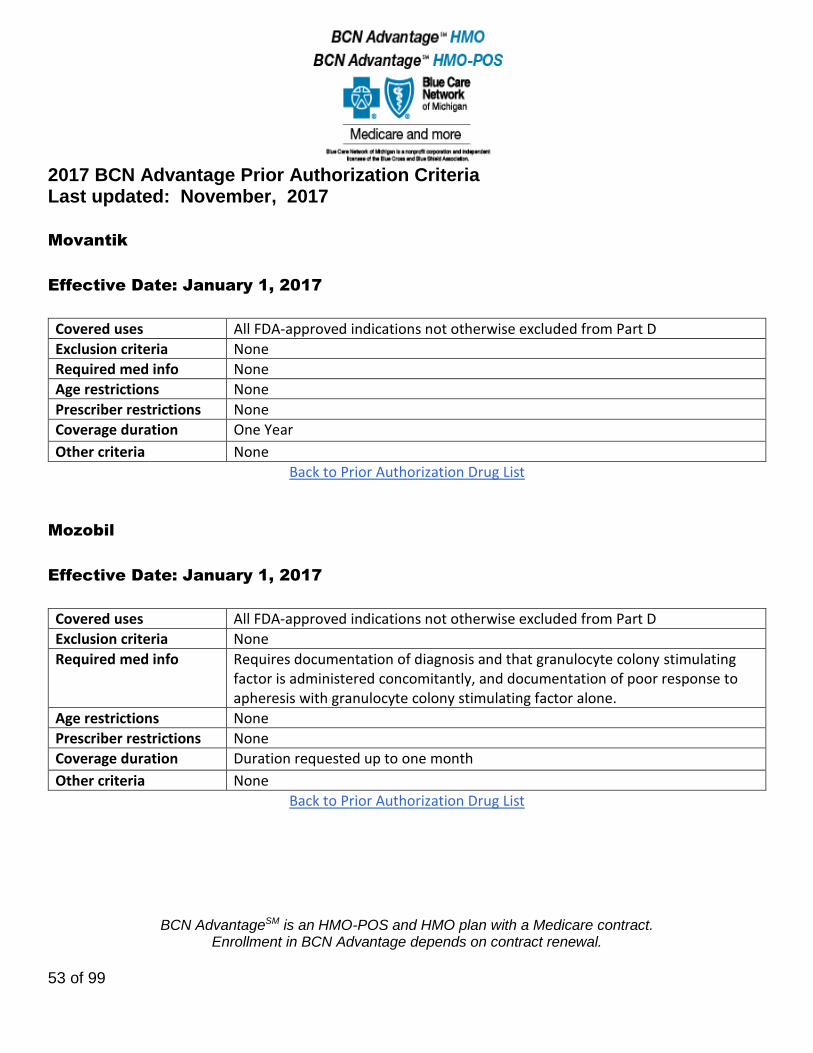
Movantik
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Mozobil
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Requires documentation of diagnosis and that granulocyte colony stimulating factor is administered concomitantly, and documentation of poor response to apheresis with granulocyte colony stimulating factor alone.
Age restrictions None
Prescriber restrictions None
Coverage duration Duration requested up to one month
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
54 of 99
Myalept
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Coverage is not provided for the following: general obesity, HIV-related lipodystrophy, partial lipodystrophy, metabolic disease (without concurrent generalized lipodystrophy) or liver disease.
Required med info Diagnosis of congenital or acquired generalized lipodystrophy
Age restrictions None
Prescriber restrictions Prescribing physician is an endocrinologist
Coverage duration Initial = 3 months Renewal = 1 year
Other criteria Renewal requires adherence to therapy and no signs or symptoms of pancreatic disease, lymphoma or events suggesting neutralizing antibody formation.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
55 of 99
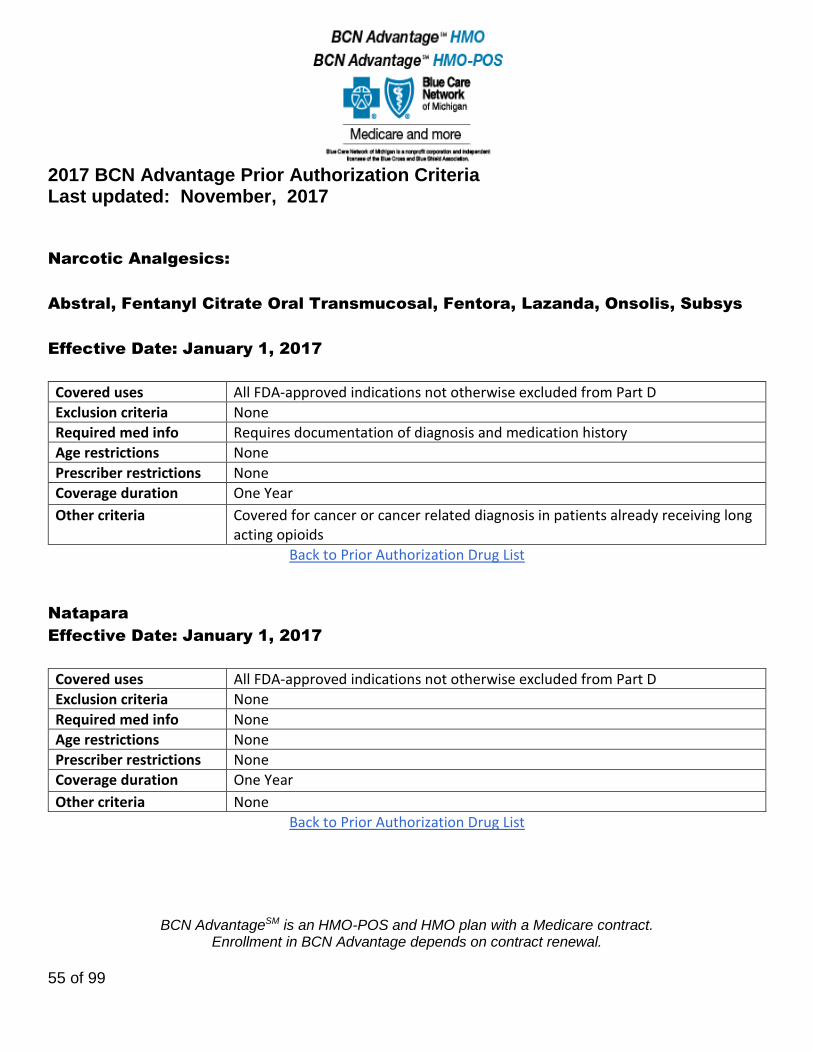
Narcotic Analgesics:
Abstral, Fentanyl Citrate Oral Transmucosal, Fentora, Lazanda, Onsolis, Subsys
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Requires documentation of diagnosis and medication history
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Covered for cancer or cancer related diagnosis in patients already receiving long acting opioids
Back to Prior Authorization Drug List
Natapara
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
56 of 99
Nerlynx
Effective Date: November 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Nexavar
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Hepato-cellular carcinoma: Prescribed by an oncologist, hepatologist, or gastroenterologist All other indications: Prescribed by an oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
57 of 99
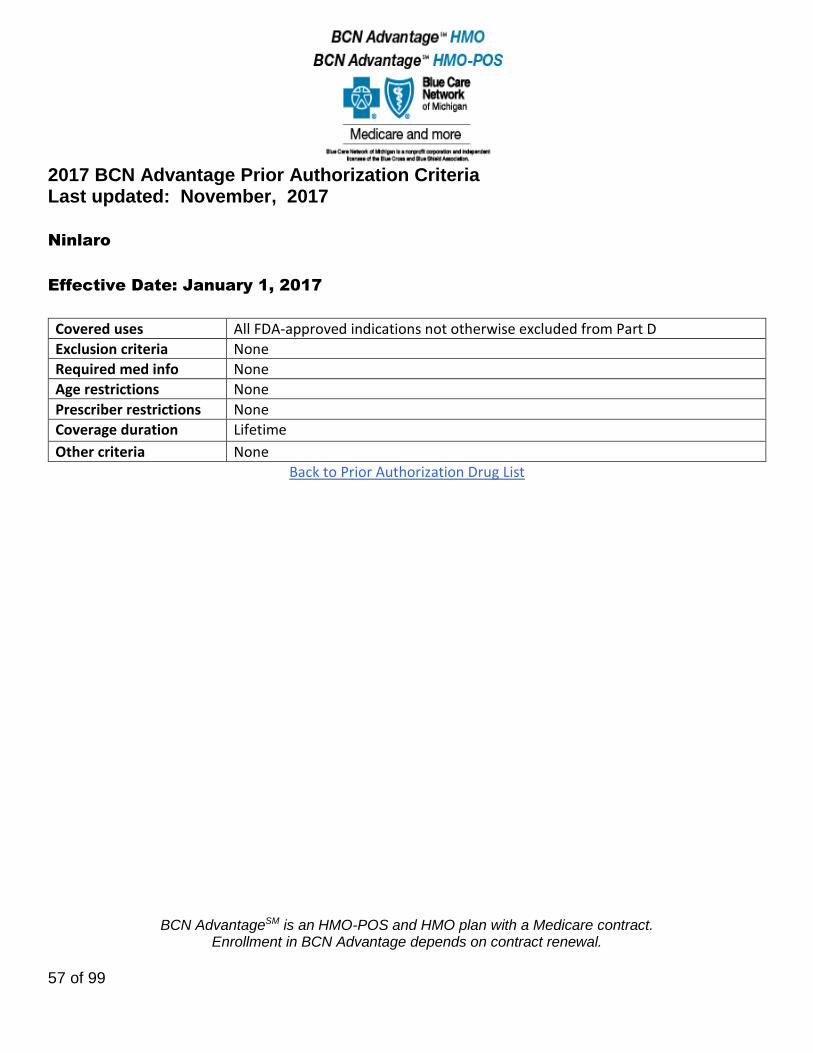
Ninlaro
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
58 of 99
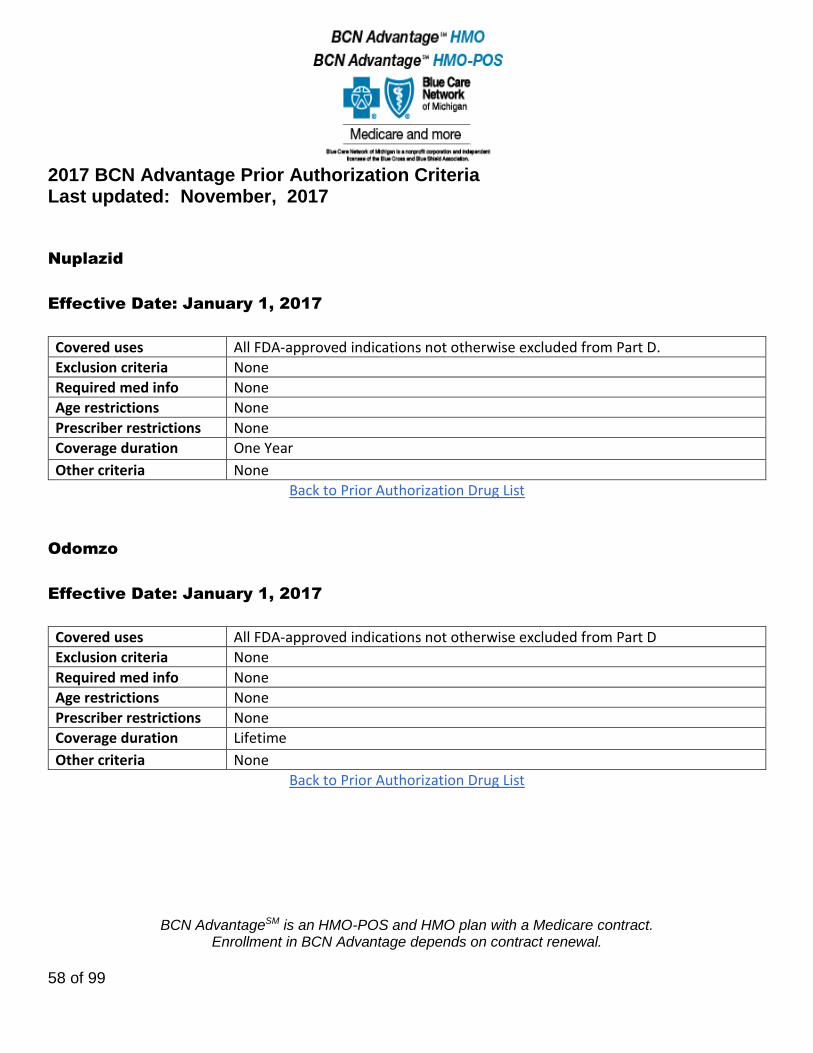
Nuplazid
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Odomzo
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
59 of 99
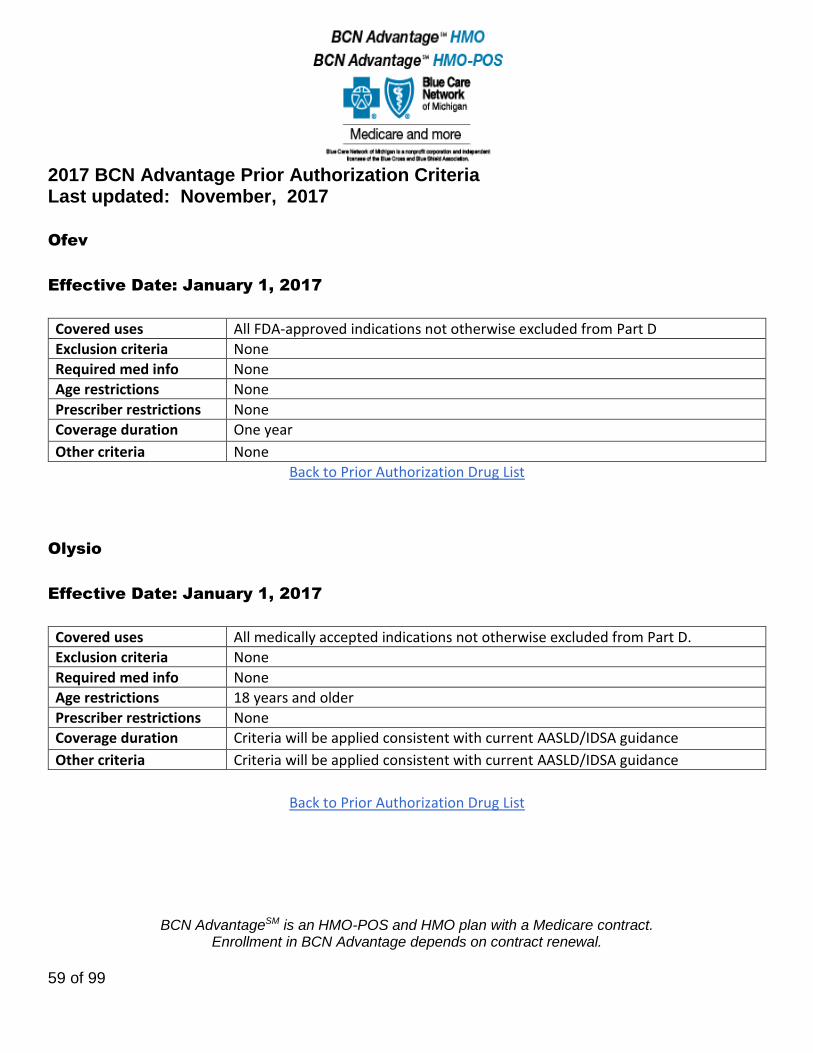
Ofev
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One year
Other criteria None
Back to Prior Authorization Drug List
Olysio
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions 18 years and older
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
60 of 99
Orencia, Orencia Clickject
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Verification that the patient has been evaluated for TB and treated accordingly
Age restrictions Rheumatoid Arthritis: 18 years and older.
Prescriber restrictions Prescribed by a rheumatologist
Coverage duration One Year
Other criteria Coverage is provided if: 1) Failed methotrexate or one DMARD and 2) Failure to at least one preferred biologic (Enbrel or Humira)
Back to Prior Authorization Drug List
Orenitram
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
61 of 99
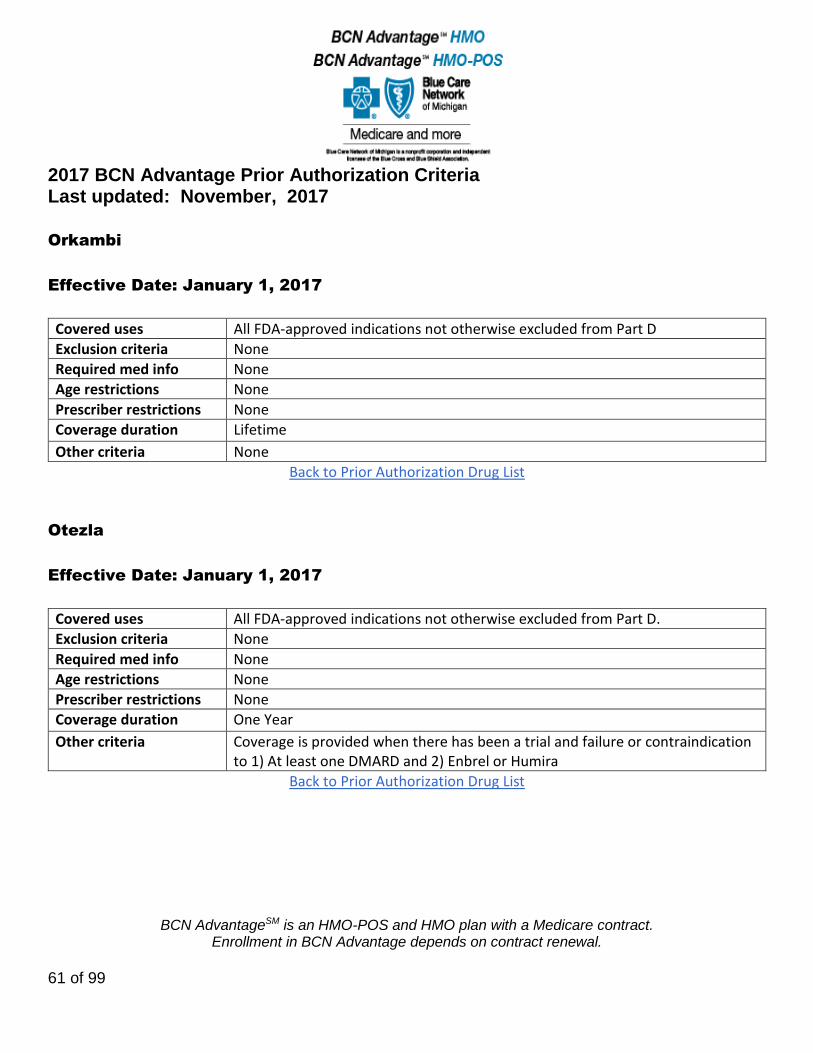
Orkambi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Otezla
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Coverage is provided when there has been a trial and failure or contraindication to 1) At least one DMARD and 2) Enbrel or Humira
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
62 of 99
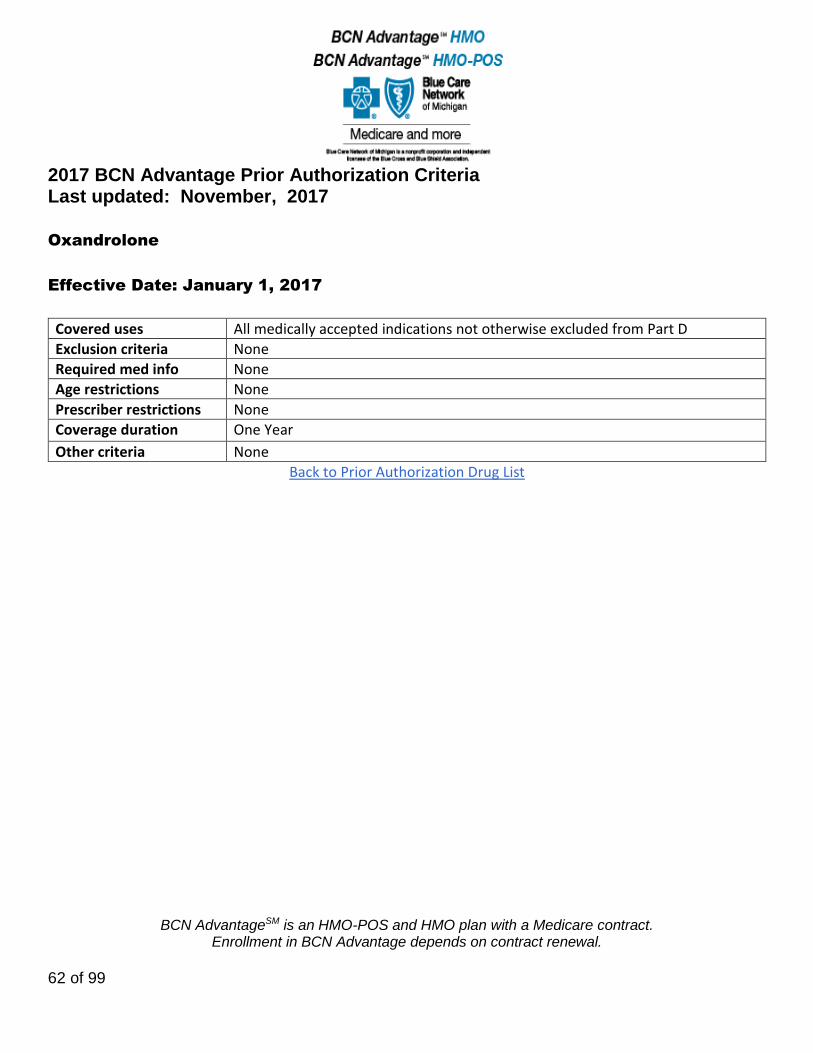
Oxandrolone
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
63 of 99
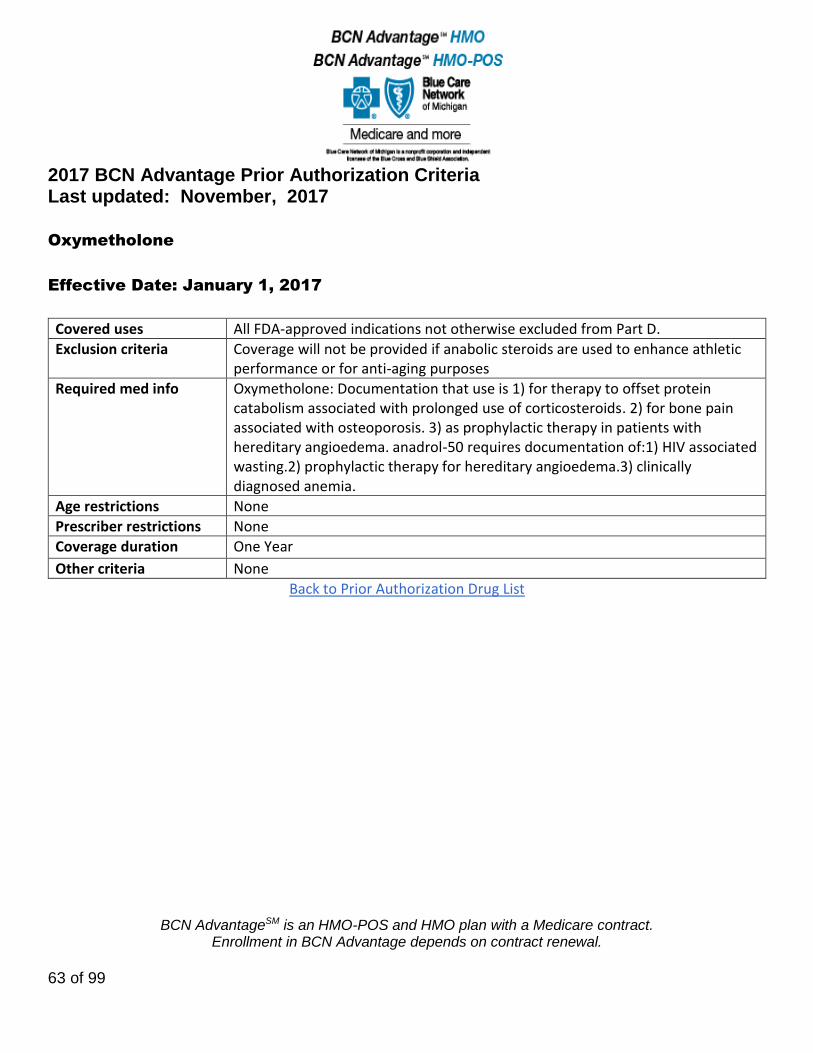
Oxymetholone
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria Coverage will not be provided if anabolic steroids are used to enhance athletic performance or for anti-aging purposes
Required med info Oxymetholone: Documentation that use is 1) for therapy to offset protein catabolism associated with prolonged use of corticosteroids. 2) for bone pain associated with osteoporosis. 3) as prophylactic therapy in patients with hereditary angioedema. anadrol-50 requires documentation of:1) HIV associated wasting.2) prophylactic therapy for hereditary angioedema.3) clinically diagnosed anemia.
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
64 of 99
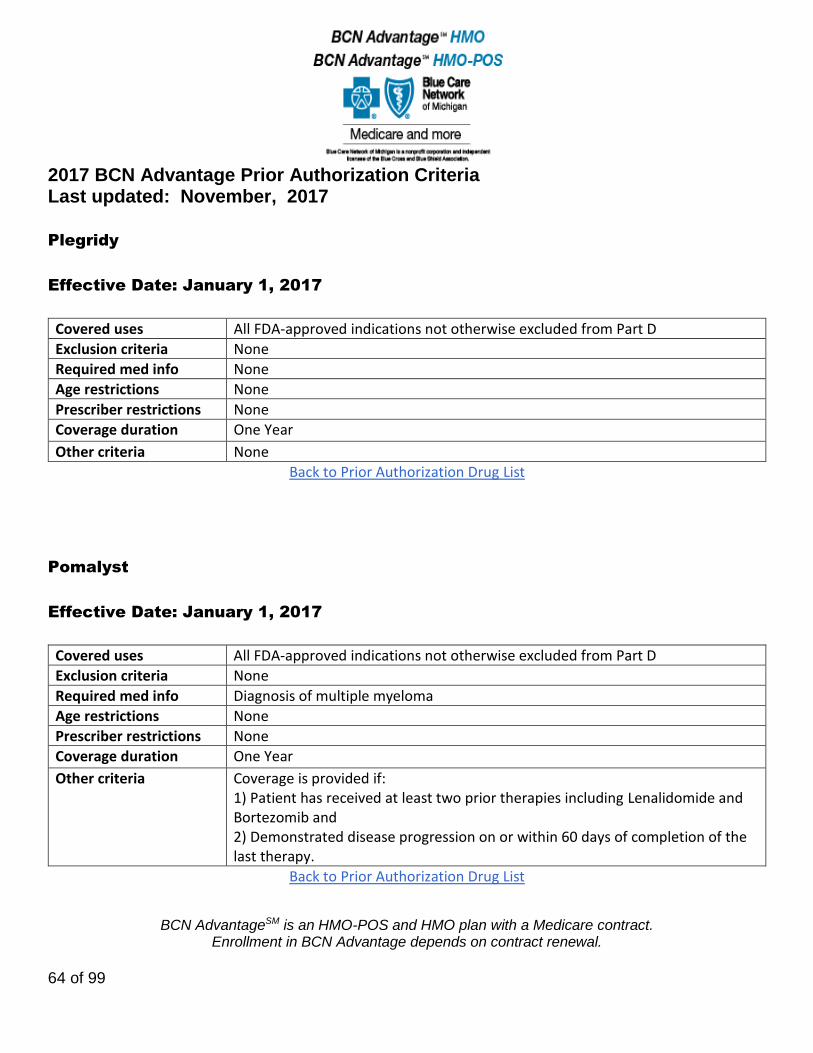
Plegridy
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Pomalyst
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis of multiple myeloma
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Coverage is provided if: 1) Patient has received at least two prior therapies including Lenalidomide and Bortezomib and 2) Demonstrated disease progression on or within 60 days of completion of the last therapy.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
65 of 99
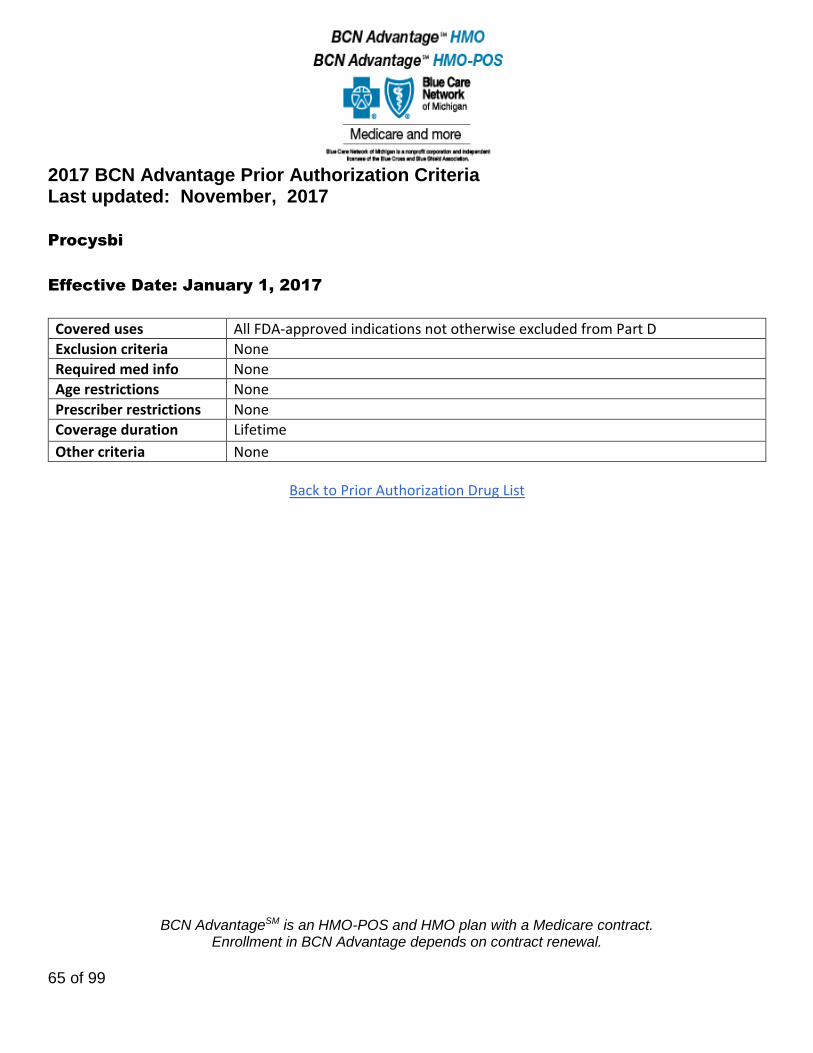
Procysbi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
66 of 99
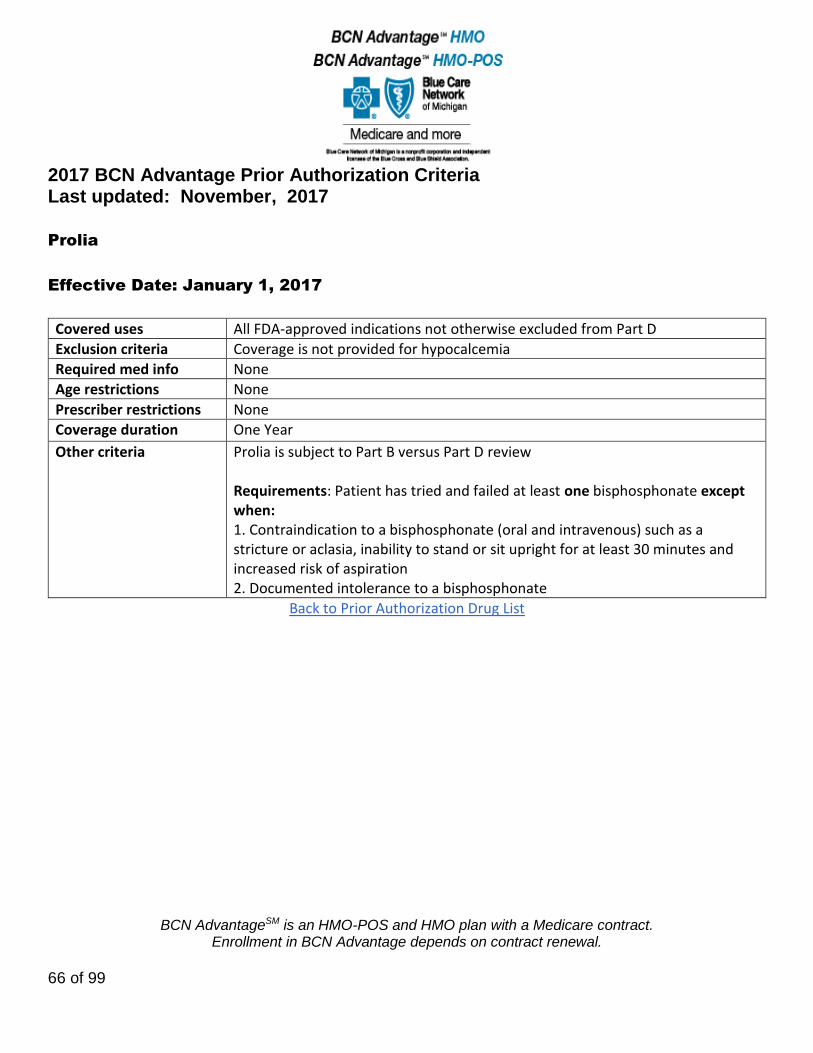
Prolia
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Coverage is not provided for hypocalcemia
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Prolia is subject to Part B versus Part D review Requirements: Patient has tried and failed at least one bisphosphonate except when: 1. Contraindication to a bisphosphonate (oral and intravenous) such as a stricture or aclasia, inability to stand or sit upright for at least 30 minutes and increased risk of aspiration 2. Documented intolerance to a bisphosphonate
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
67 of 99
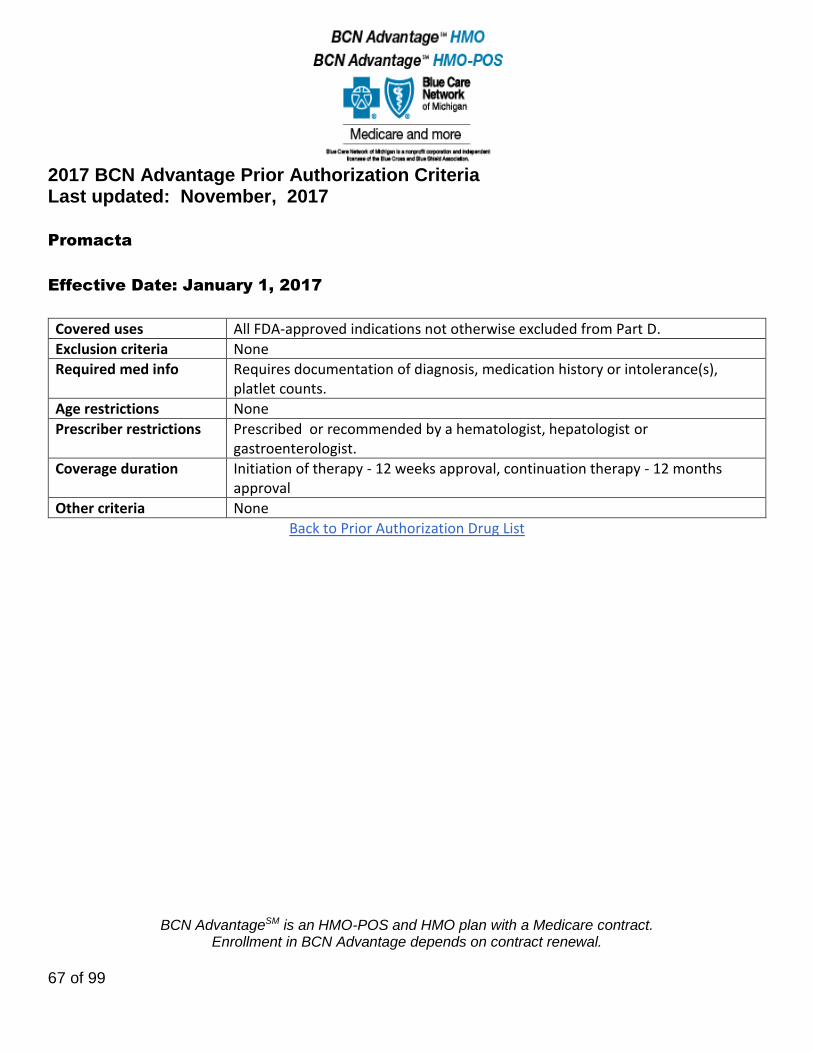
Promacta
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Requires documentation of diagnosis, medication history or intolerance(s), platlet counts.
Age restrictions None
Prescriber restrictions Prescribed or recommended by a hematologist, hepatologist or gastroenterologist.
Coverage duration Initiation of therapy - 12 weeks approval, continuation therapy - 12 months approval
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
68 of 99
Promethazine/Promethegan/Phenergan/Phenadoz
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions Authorization is required for members 65 years of age and older
Prescriber restrictions None
Coverage duration One Year
Other criteria Promethazine will be approved when used as part of an analgesia regimen. Promethazine is approved for other uses if at least one safer alternative has been tried and failed unless the alternative is not appropriate or contraindicated. Alternatives for allergic conditions: second generation antihistamine (e.g., cetirizine, desloratadine, loratadine, fexofenadine). Alternatives for sleep include low dose trazodone (25-50mg) , rozerem or melatonin. For nausea or vomiting or motion sickness, alternatives include prochlorperazine, ondansetron, granisetron and meclizine.
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
69 of 99
Pulmonary Agents:
Adcirca, Letairis, Opsumit, Revatio oral suspension, Sildenafil Citrate 20mg,
Remodulin, Tracleer
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Coverage for Revatio and Adcirca is not provided in situations where patients are receiving nitrate therapy.
Back to Prior Authorization Drug List
Radicava
Effective Date: November 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
70 of 99
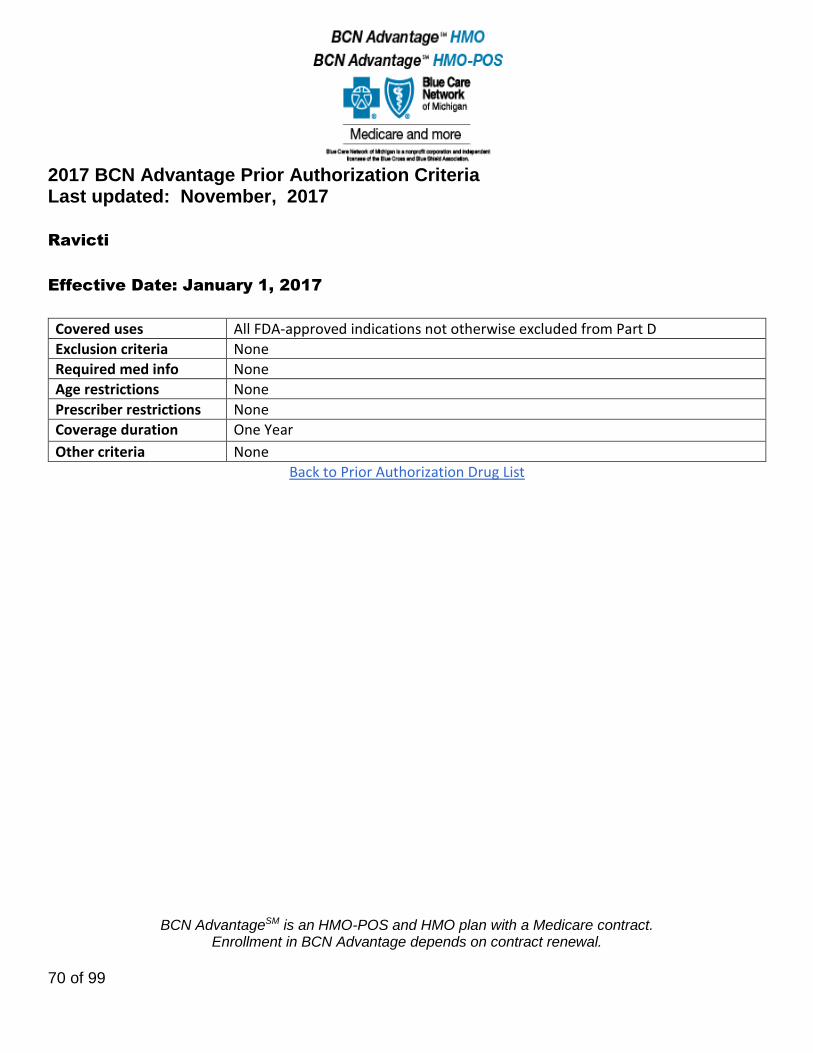
Ravicti
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
71 of 99
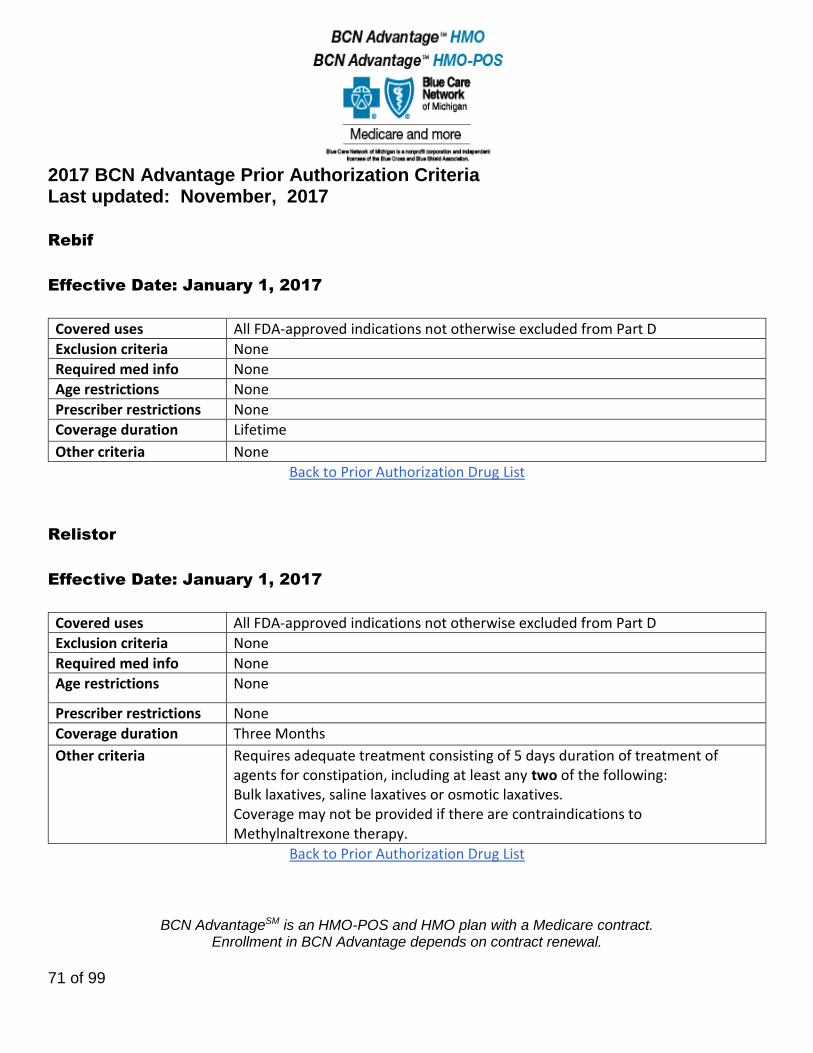
Rebif
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
Relistor
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Three Months
Other criteria Requires adequate treatment consisting of 5 days duration of treatment of agents for constipation, including at least any two of the following: Bulk laxatives, saline laxatives or osmotic laxatives. Coverage may not be provided if there are contraindications to Methylnaltrexone therapy.
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
72 of 99
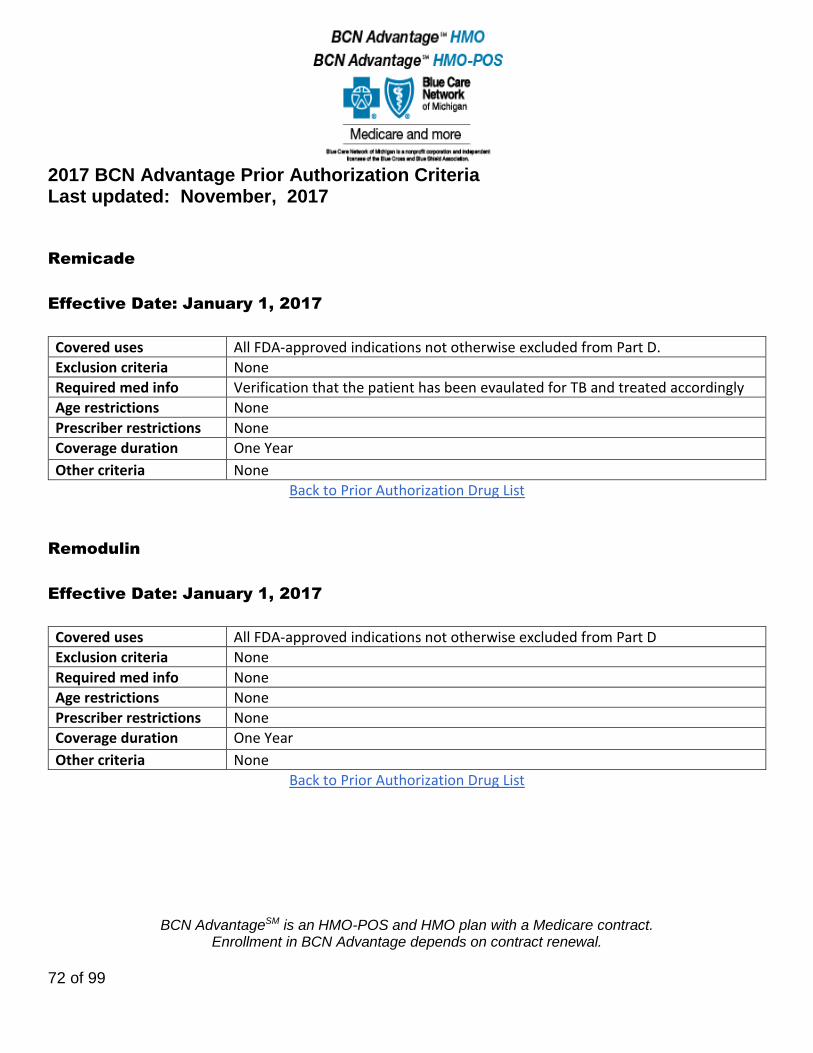
Remicade
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Verification that the patient has been evaulated for TB and treated accordingly
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Remodulin
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
73 of 99
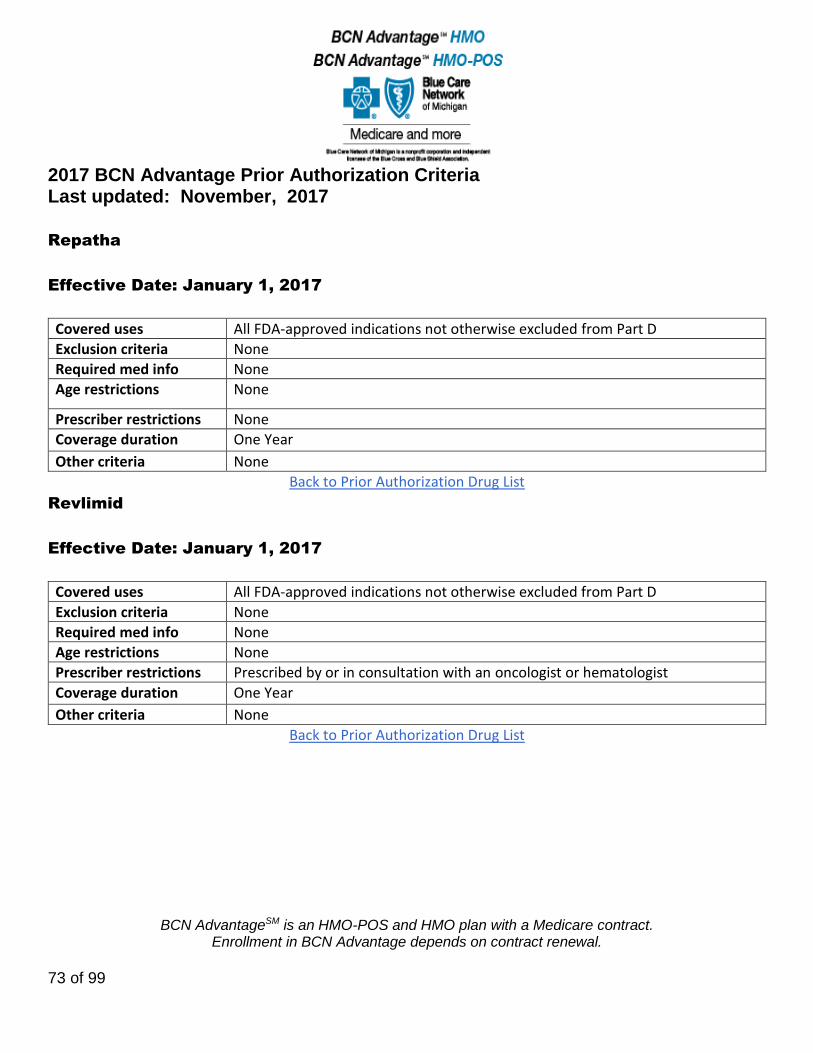
Repatha
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Revlimid
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by or in consultation with an oncologist or hematologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
74 of 99
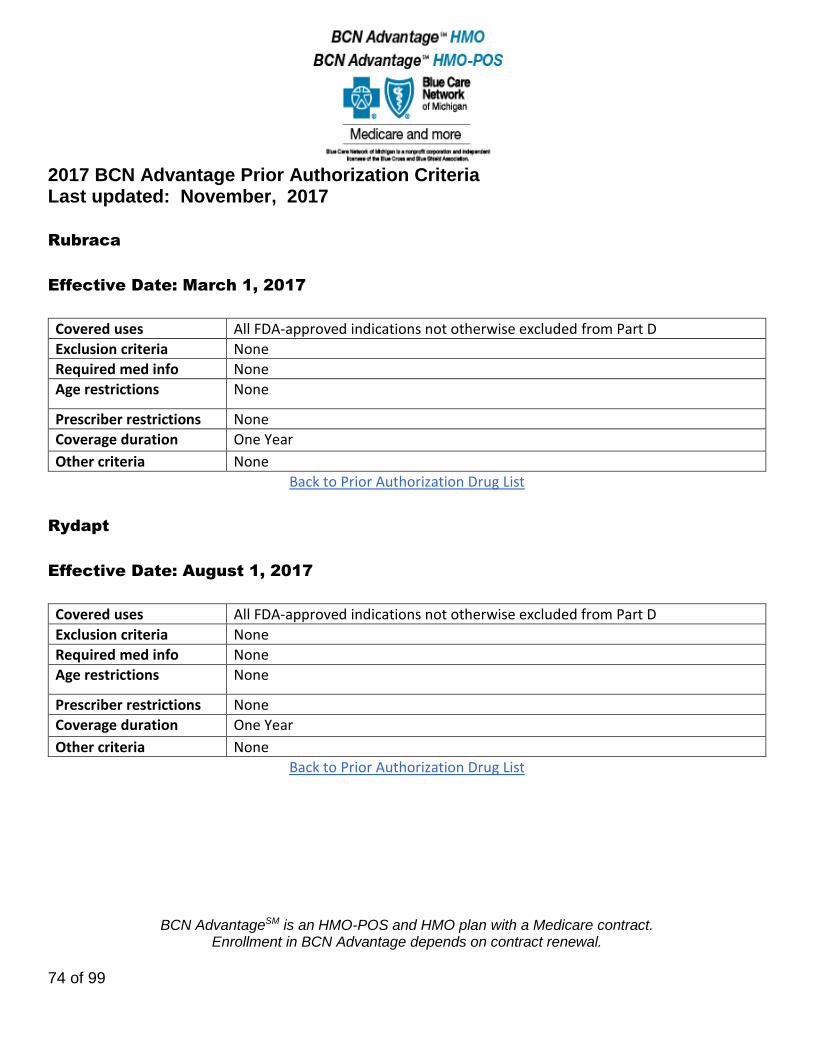
Rubraca
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Rydapt
Effective Date: August 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
75 of 99
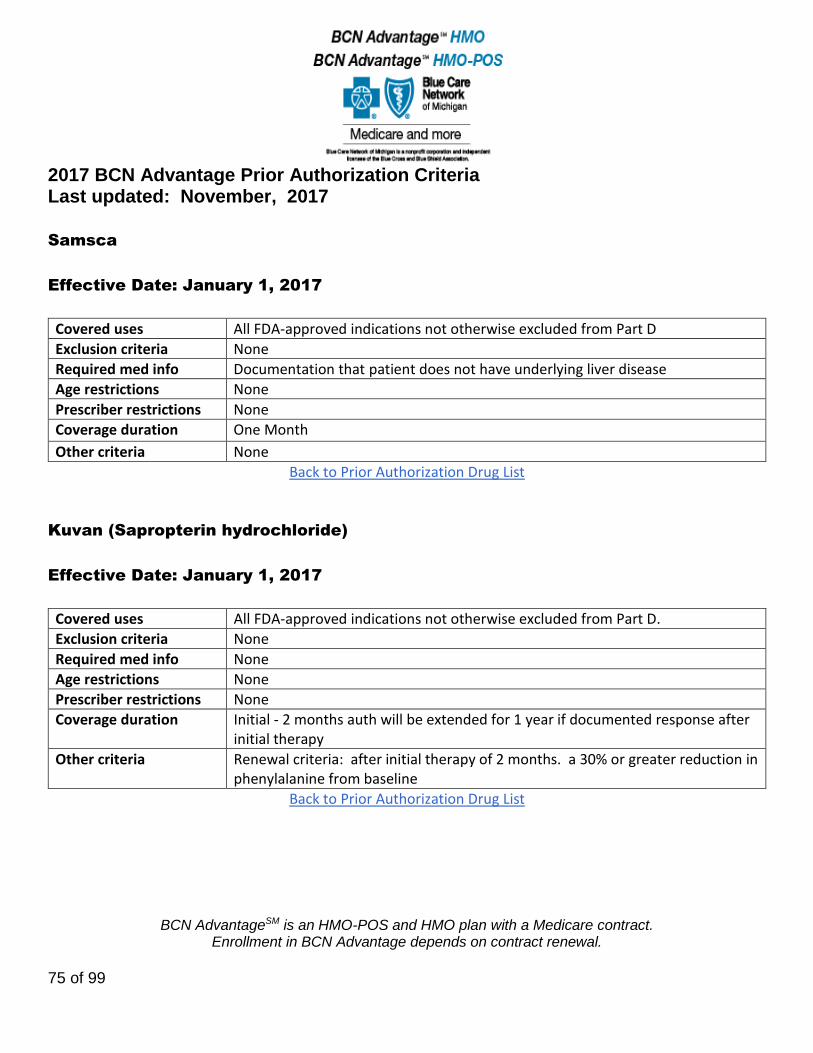
Samsca
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Documentation that patient does not have underlying liver disease
Age restrictions None
Prescriber restrictions None
Coverage duration One Month
Other criteria None
Back to Prior Authorization Drug List
Kuvan (Sapropterin hydrochloride)
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Initial - 2 months auth will be extended for 1 year if documented response after initial therapy
Other criteria Renewal criteria: after initial therapy of 2 months. a 30% or greater reduction in phenylalanine from baseline
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
76 of 99
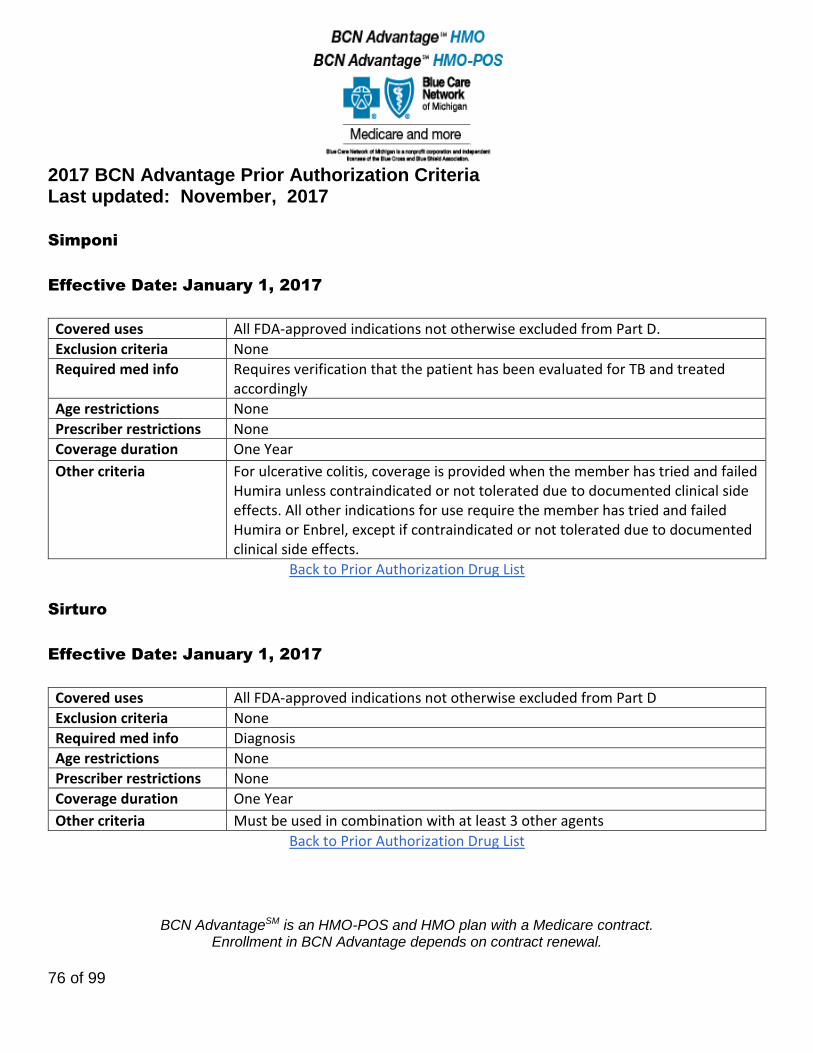
Simponi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Requires verification that the patient has been evaluated for TB and treated accordingly
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria For ulcerative colitis, coverage is provided when the member has tried and failed Humira unless contraindicated or not tolerated due to documented clinical side effects. All other indications for use require the member has tried and failed Humira or Enbrel, except if contraindicated or not tolerated due to documented clinical side effects.
Back to Prior Authorization Drug List
Sirturo
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Must be used in combination with at least 3 other agents
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
77 of 99
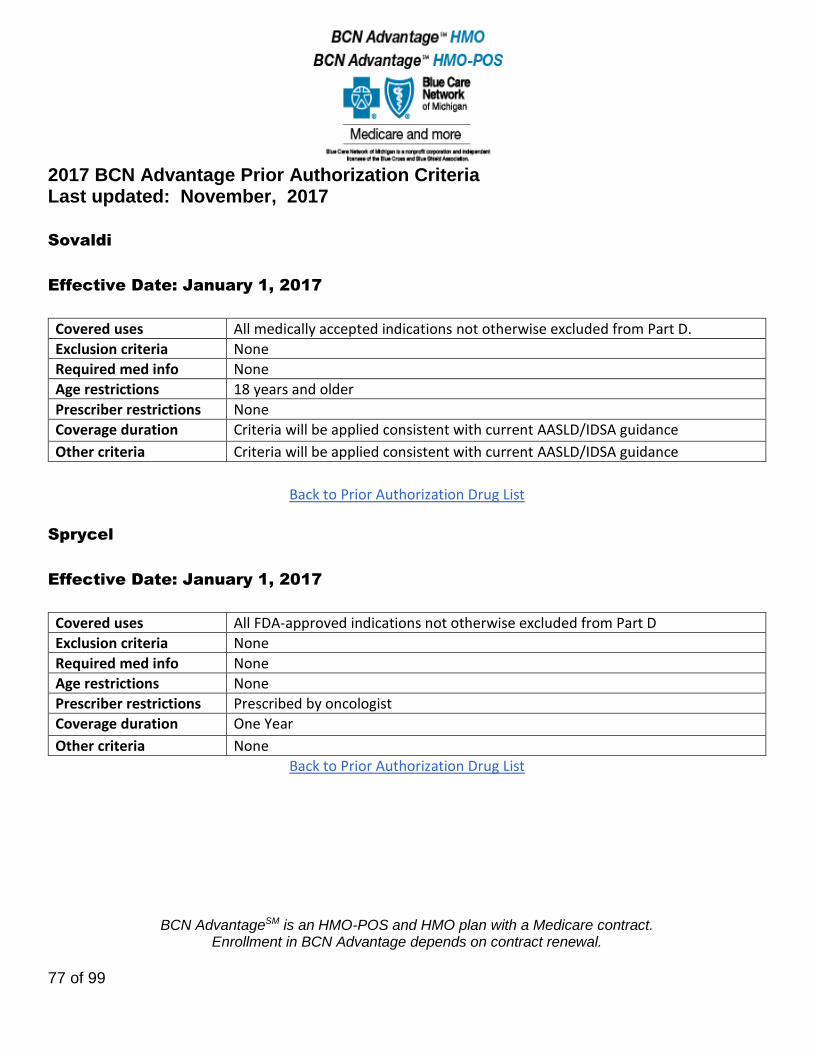
Sovaldi
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions 18 years and older
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
Sprycel
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
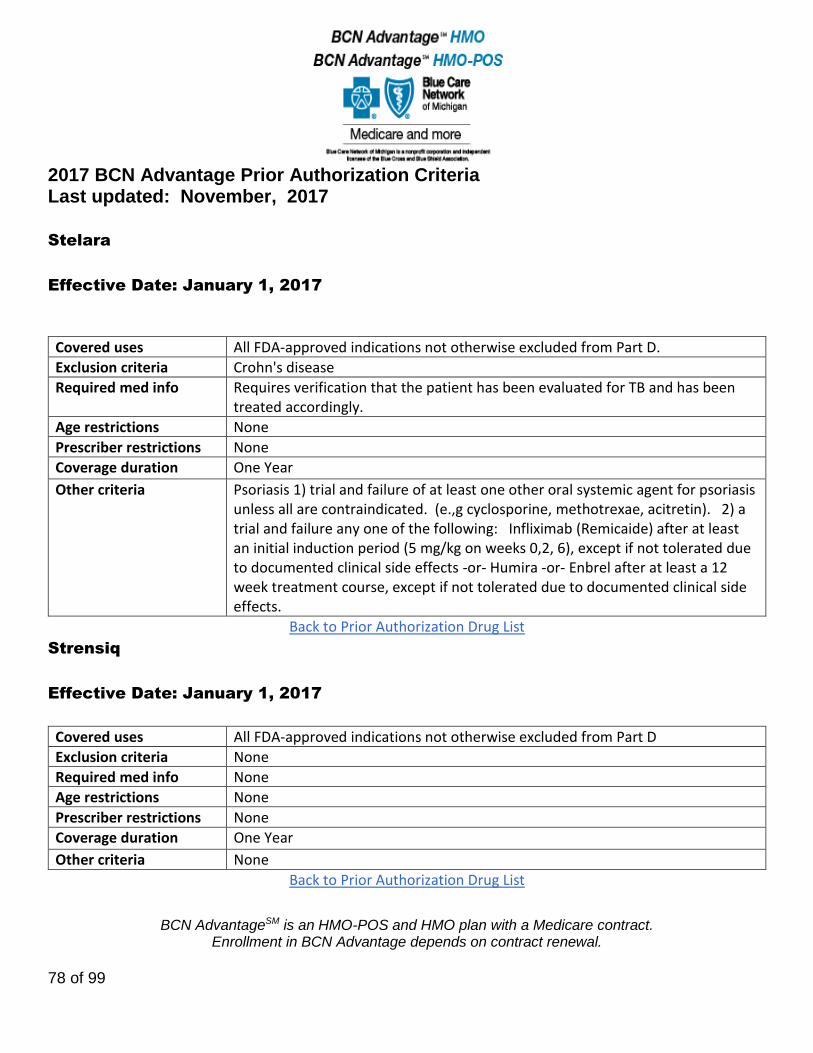
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
78 of 99
Stelara
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria Crohn's disease
Required med info Requires verification that the patient has been evaluated for TB and has been treated accordingly.
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria Psoriasis 1) trial and failure of at least one other oral systemic agent for psoriasis unless all are contraindicated. (e.,g cyclosporine, methotrexae, acitretin). 2) a trial and failure any one of the following: Infliximab (Remicaide) after at least an initial induction period (5 mg/kg on weeks 0,2, 6), except if not tolerated due to documented clinical side effects -or- Humira -or- Enbrel after at least a 12 week treatment course, except if not tolerated due to documented clinical side effects.
Back to Prior Authorization Drug List
Strensiq
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
79 of 99

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
80 of 99
Sutent
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Sylatron
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
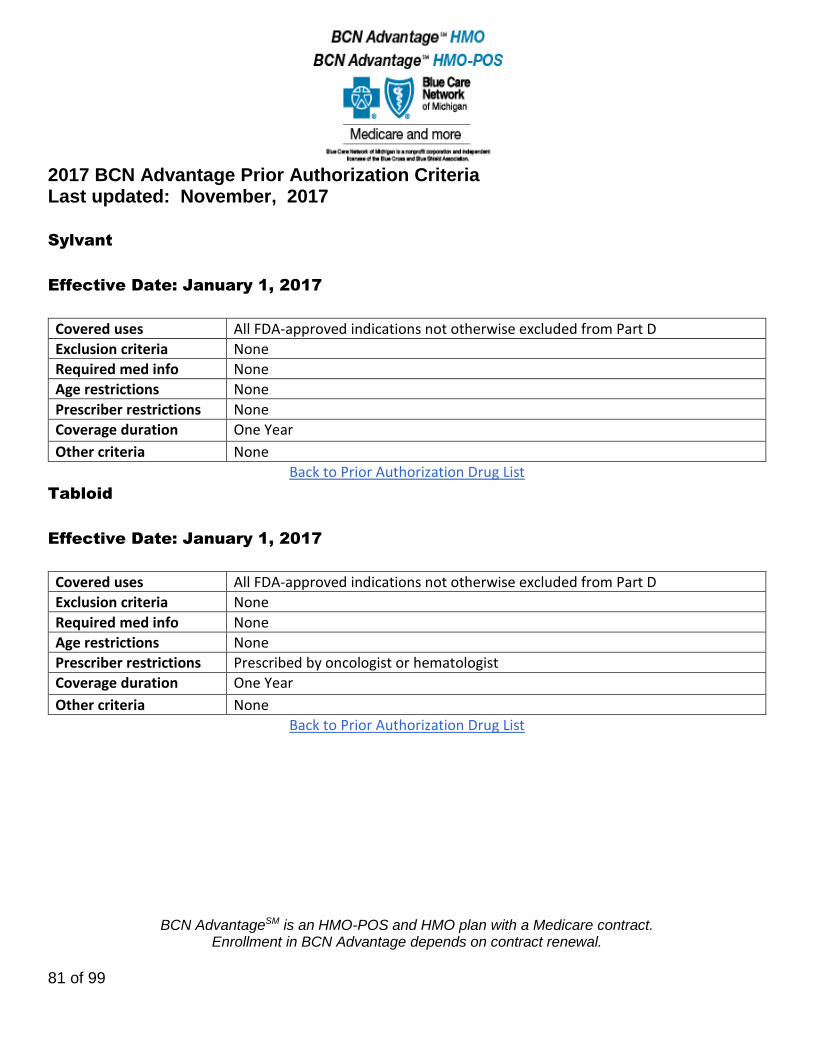
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
81 of 99
Sylvant
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Tabloid
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist or hematologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
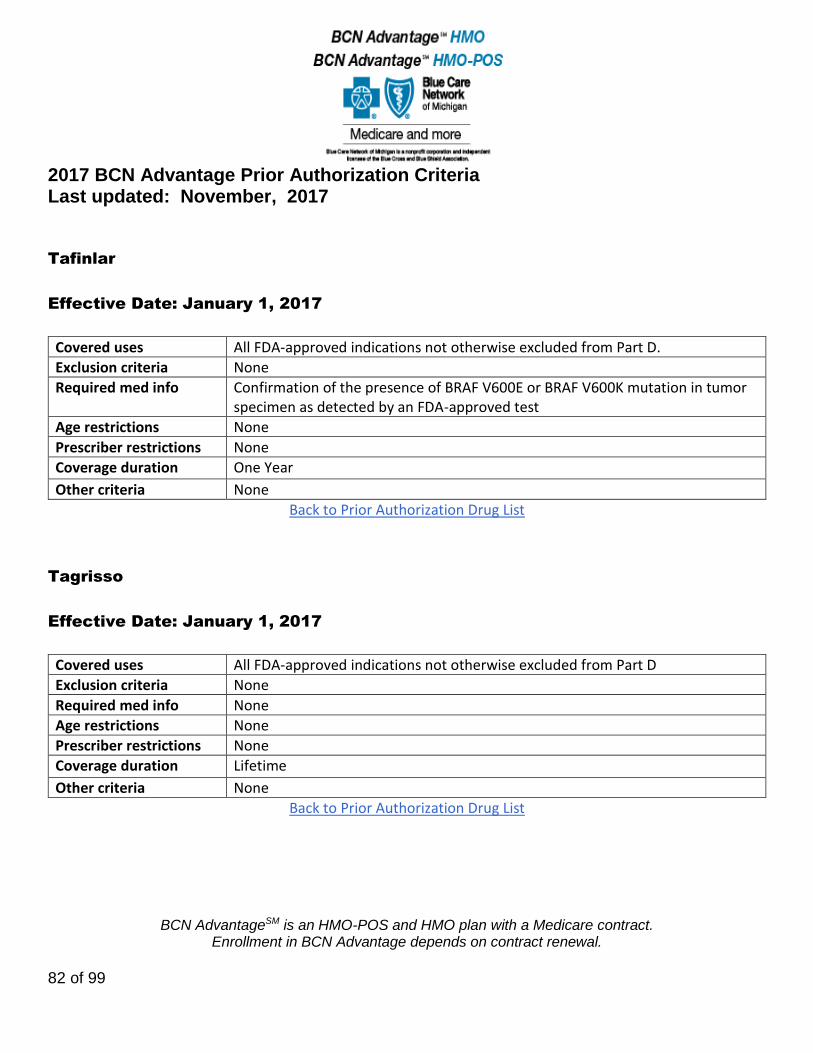
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
82 of 99
Tafinlar
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info Confirmation of the presence of BRAF V600E or BRAF V600K mutation in tumor specimen as detected by an FDA-approved test
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Tagrisso
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
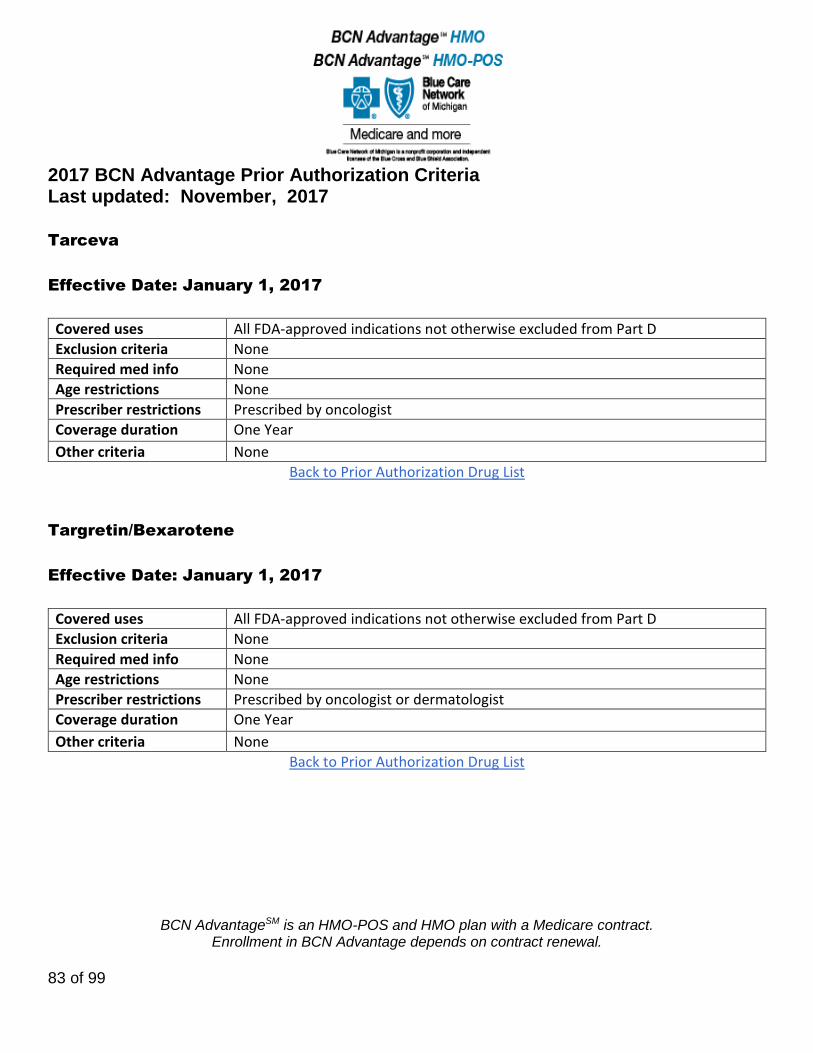
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
83 of 99
Tarceva
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Targretin/Bexarotene
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by oncologist or dermatologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
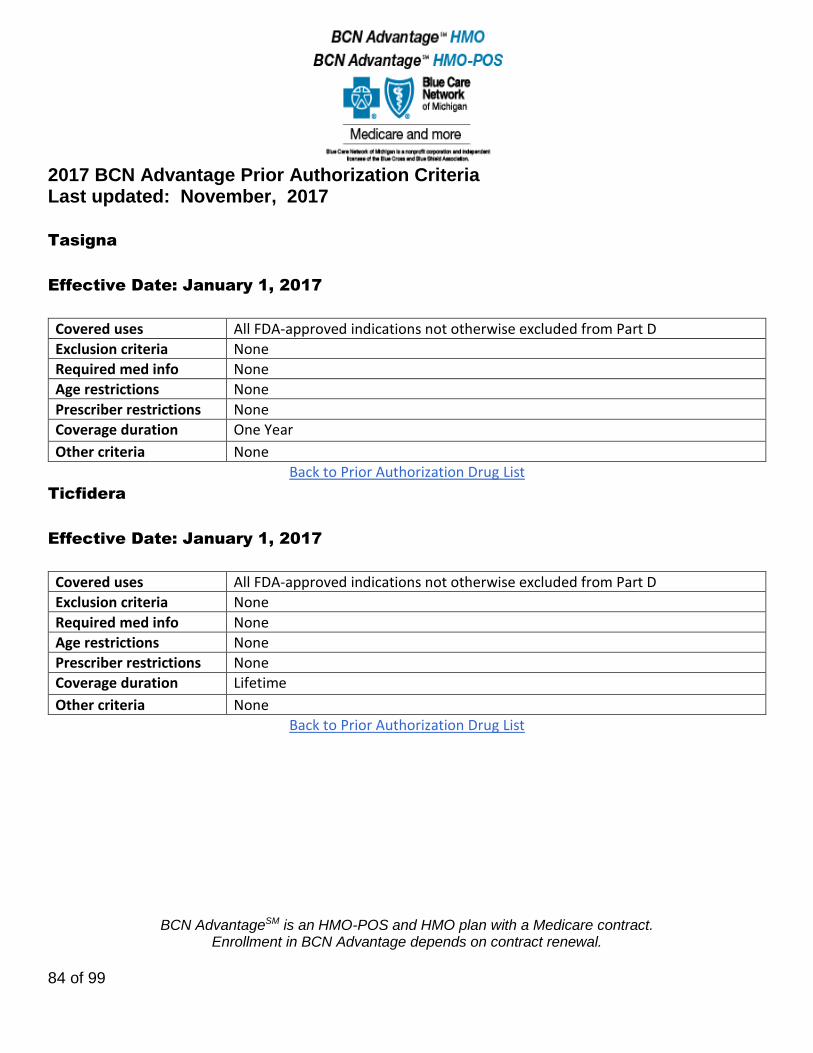
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
84 of 99
Tasigna
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Ticfidera
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
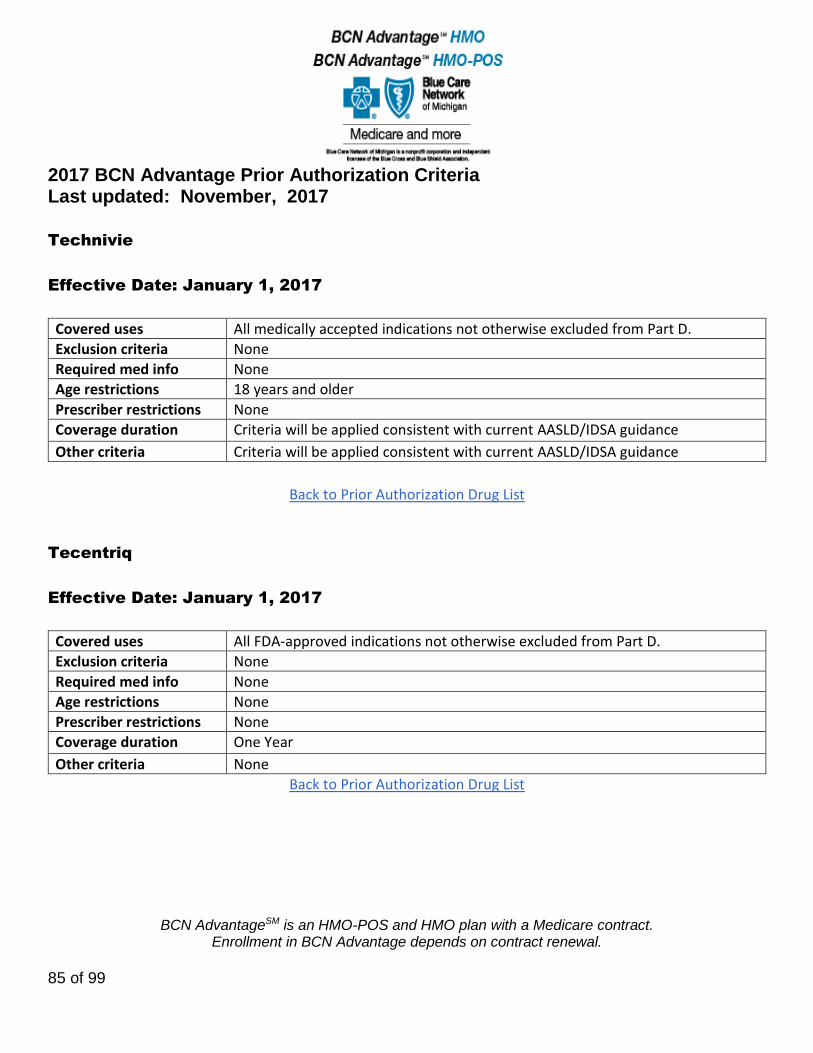
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
85 of 99
Technivie
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions 18 years and older
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
Tecentriq
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
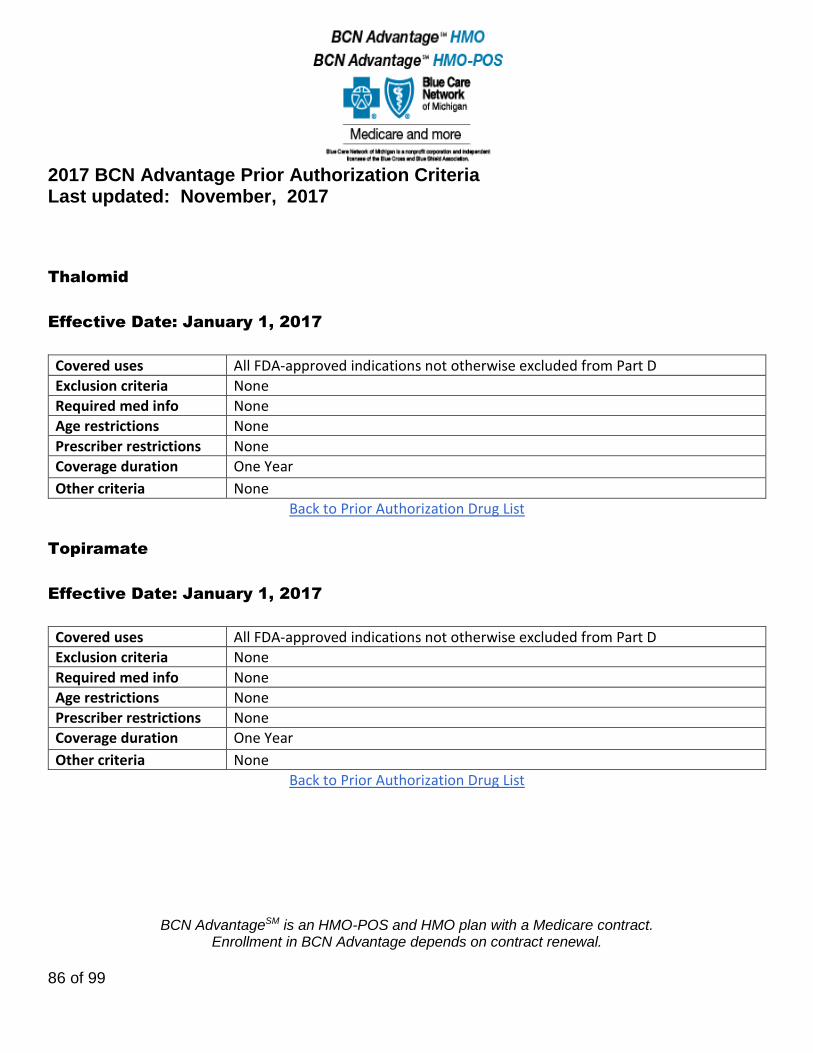
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
86 of 99
Thalomid
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Topiramate
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
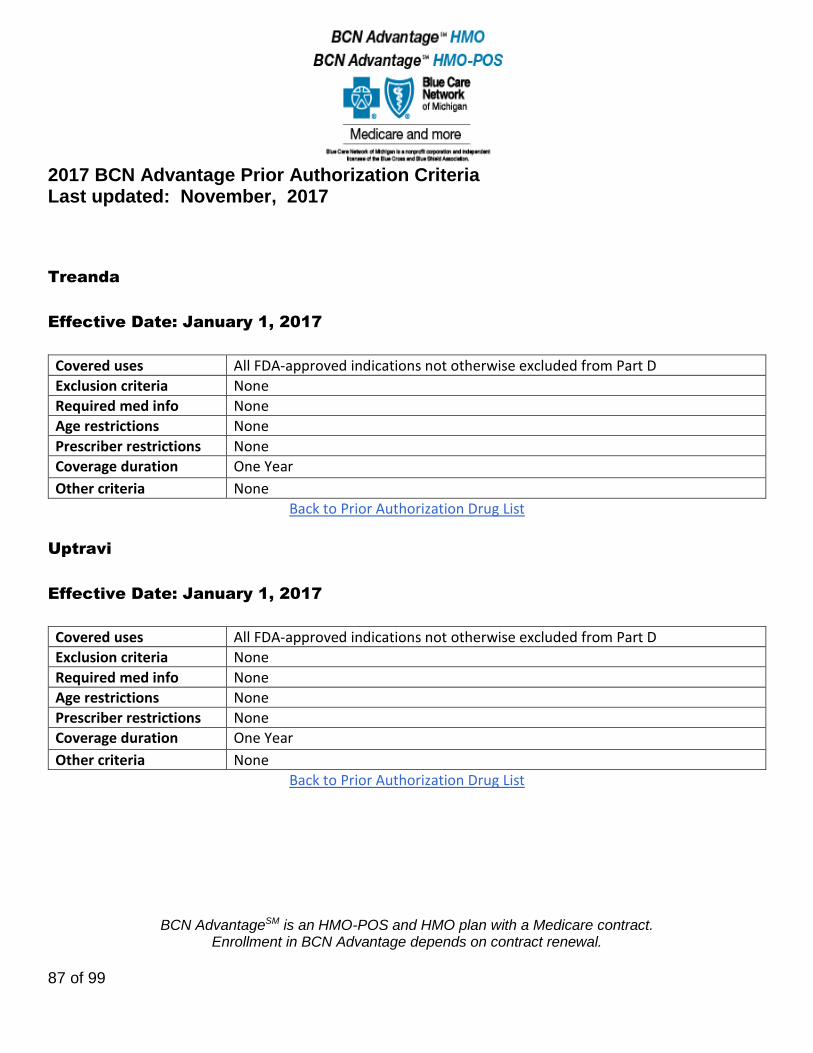
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
87 of 99
Treanda
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Uptravi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
88 of 99
Vecamyl
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Vectibex
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by an oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
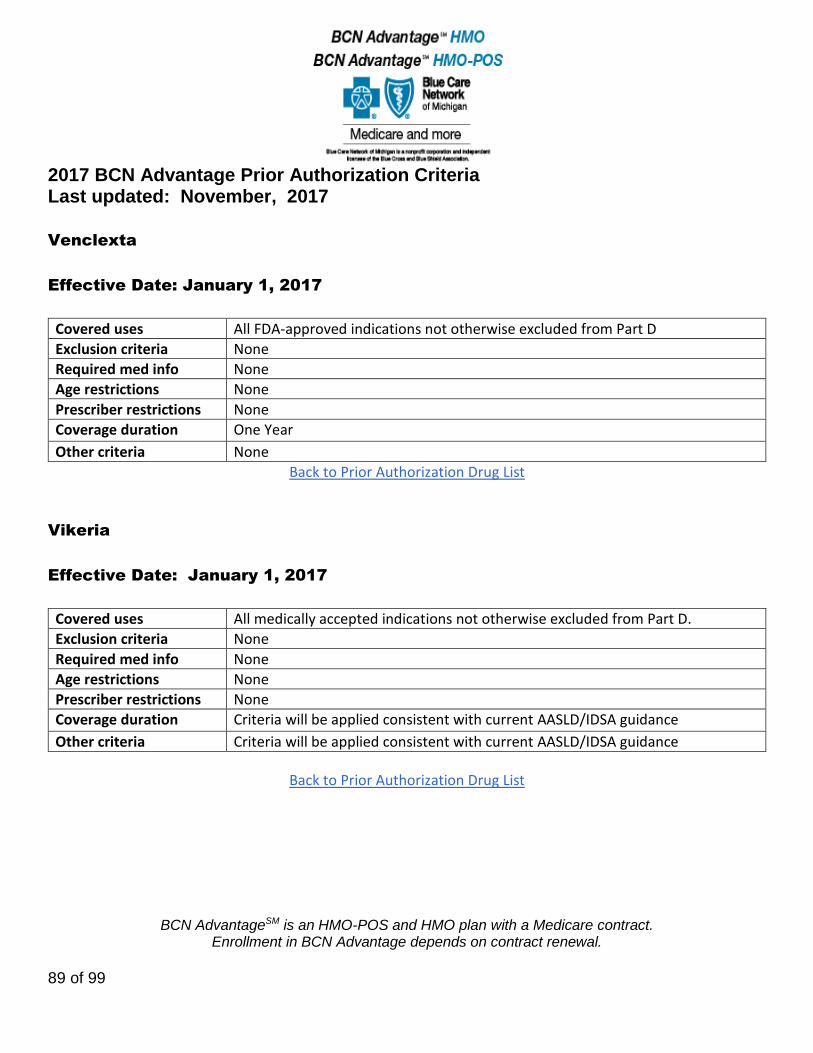
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
89 of 99
Venclexta
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Vikeria
Effective Date: January 1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List

2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
90 of 99
Votrient
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Documentation of advanced renal cell carcinoma
Age restrictions None
Prescriber restrictions Prescribed by an oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Xalkori
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Diagnosis of locally advanced or metastatic non-small cell lung cancer (NSCLC) that is anaplastic lymphoma kinase (alk)-positive as detected by a FDA-approved test.
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
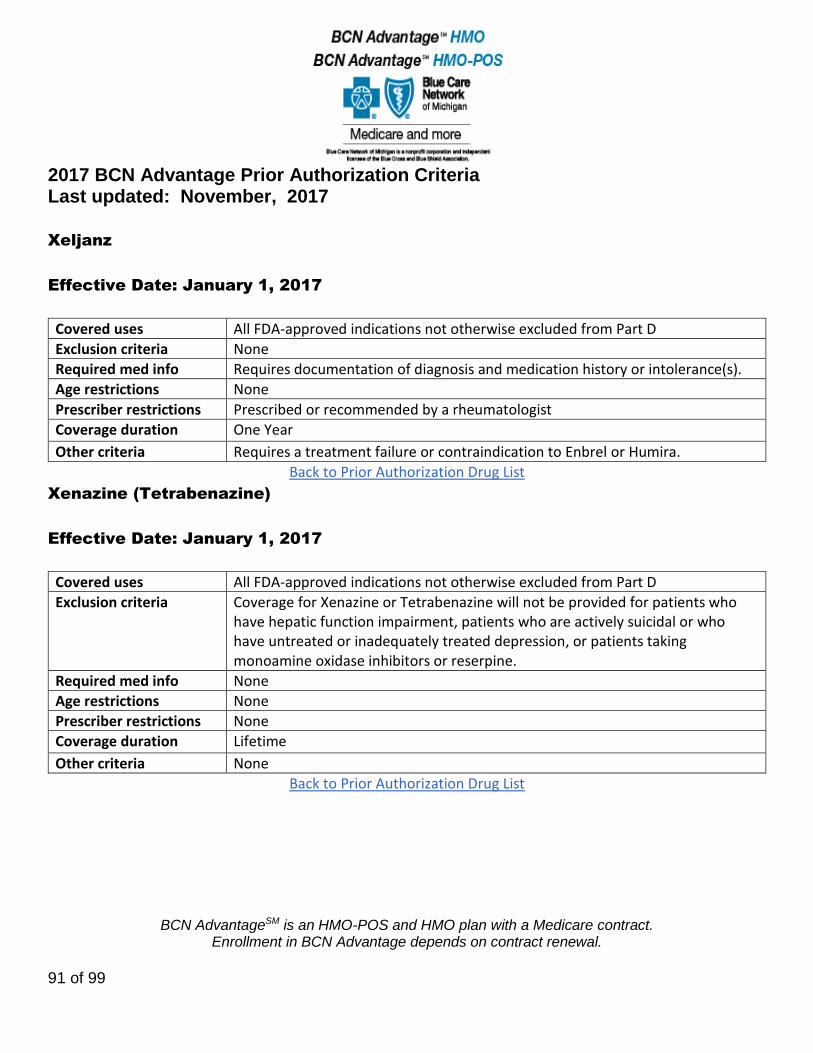
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
91 of 99
Xeljanz
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Requires documentation of diagnosis and medication history or intolerance(s).
Age restrictions None
Prescriber restrictions Prescribed or recommended by a rheumatologist
Coverage duration One Year
Other criteria Requires a treatment failure or contraindication to Enbrel or Humira.
Back to Prior Authorization Drug List
Xenazine (Tetrabenazine)
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Coverage for Xenazine or Tetrabenazine will not be provided for patients who have hepatic function impairment, patients who are actively suicidal or who have untreated or inadequately treated depression, or patients taking monoamine oxidase inhibitors or reserpine.
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration Lifetime
Other criteria None
Back to Prior Authorization Drug List
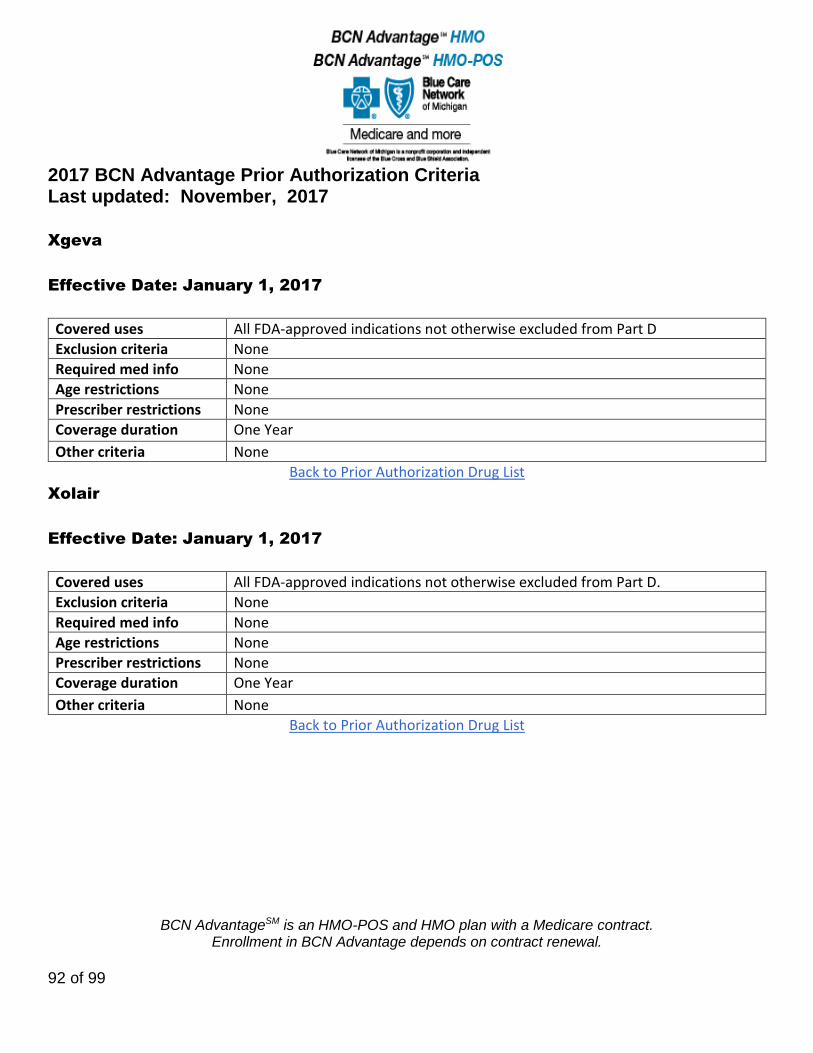
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
92 of 99
Xgeva
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Xolair
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
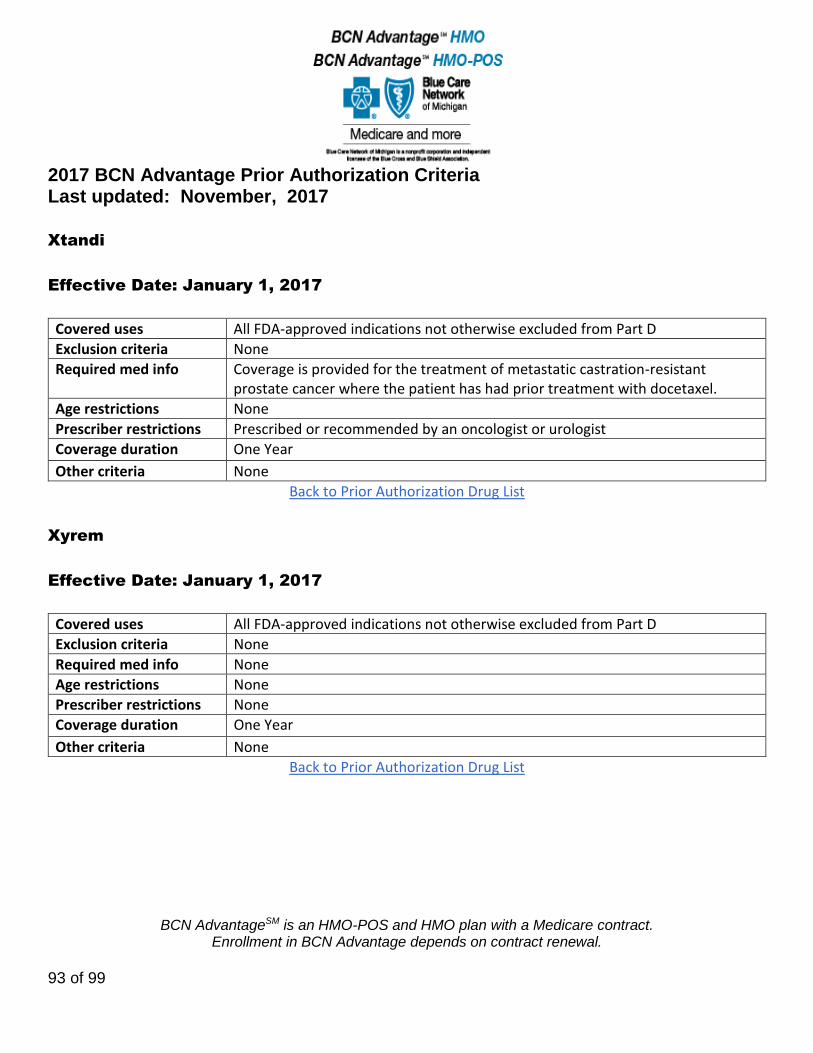
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
93 of 99
Xtandi
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info Coverage is provided for the treatment of metastatic castration-resistant prostate cancer where the patient has had prior treatment with docetaxel.
Age restrictions None
Prescriber restrictions Prescribed or recommended by an oncologist or urologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Xyrem
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
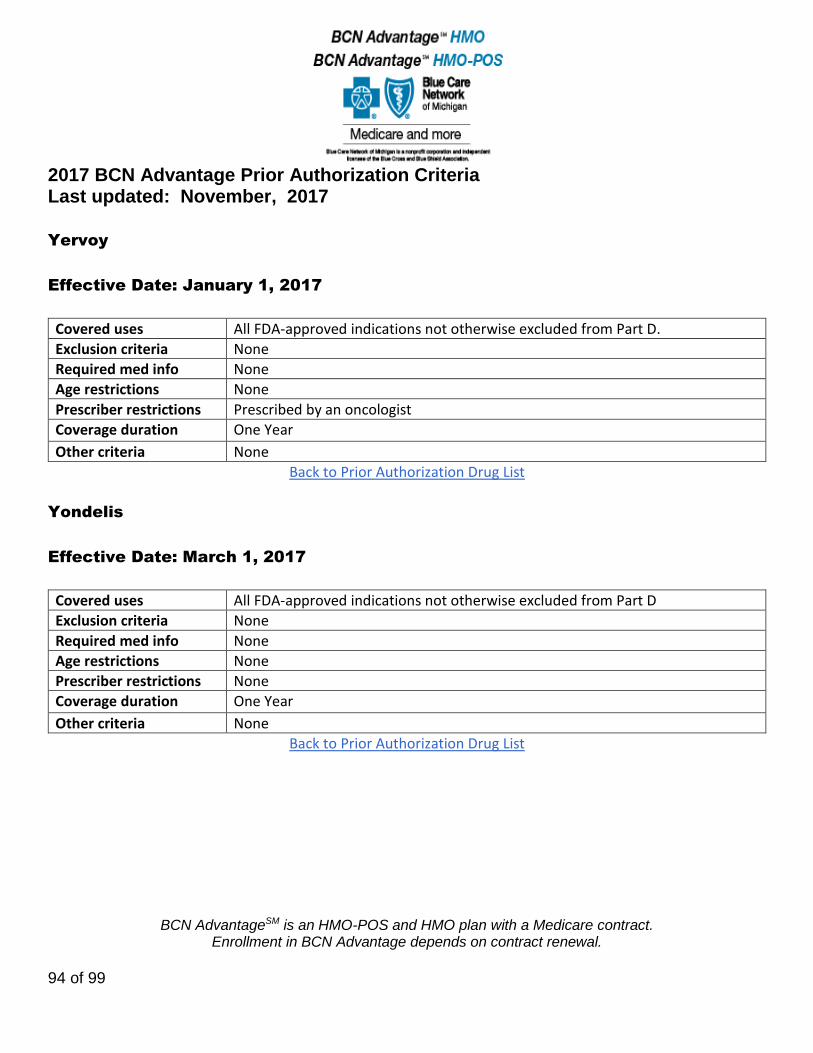
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
94 of 99
Yervoy
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions Prescribed by an oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Yondelis
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
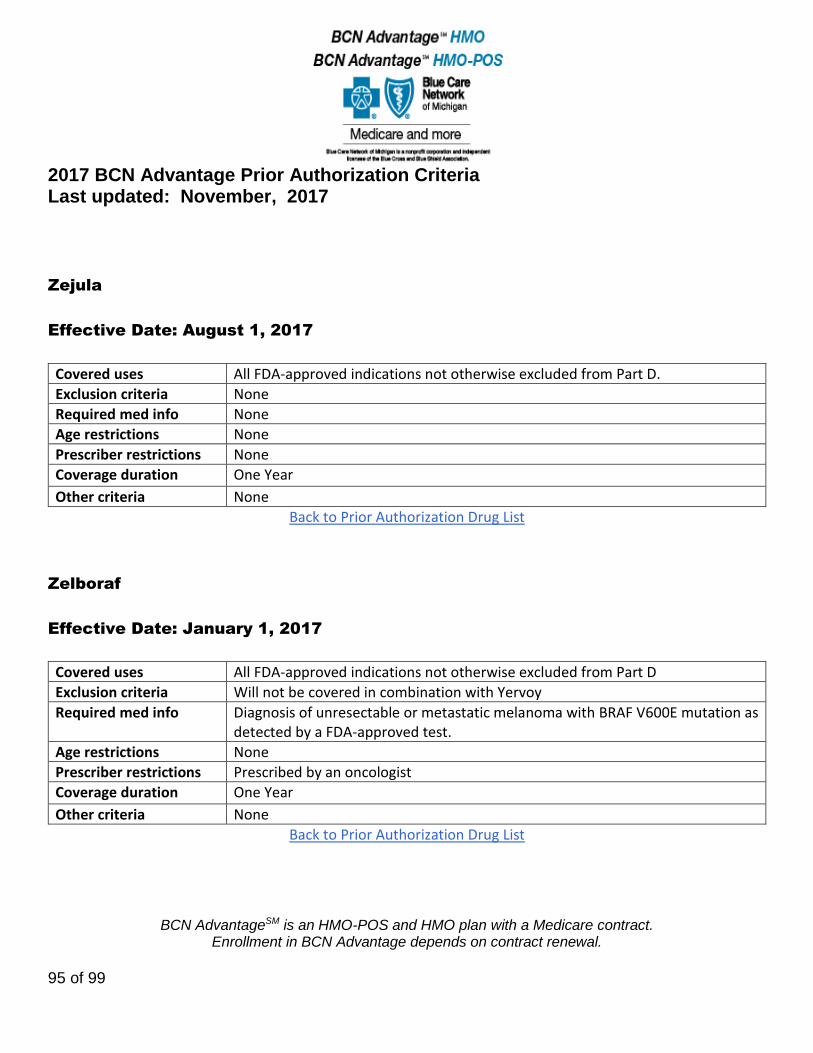
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
95 of 99
Zejula
Effective Date: August 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Zelboraf
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria Will not be covered in combination with Yervoy
Required med info Diagnosis of unresectable or metastatic melanoma with BRAF V600E mutation as detected by a FDA-approved test.
Age restrictions None
Prescriber restrictions Prescribed by an oncologist
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
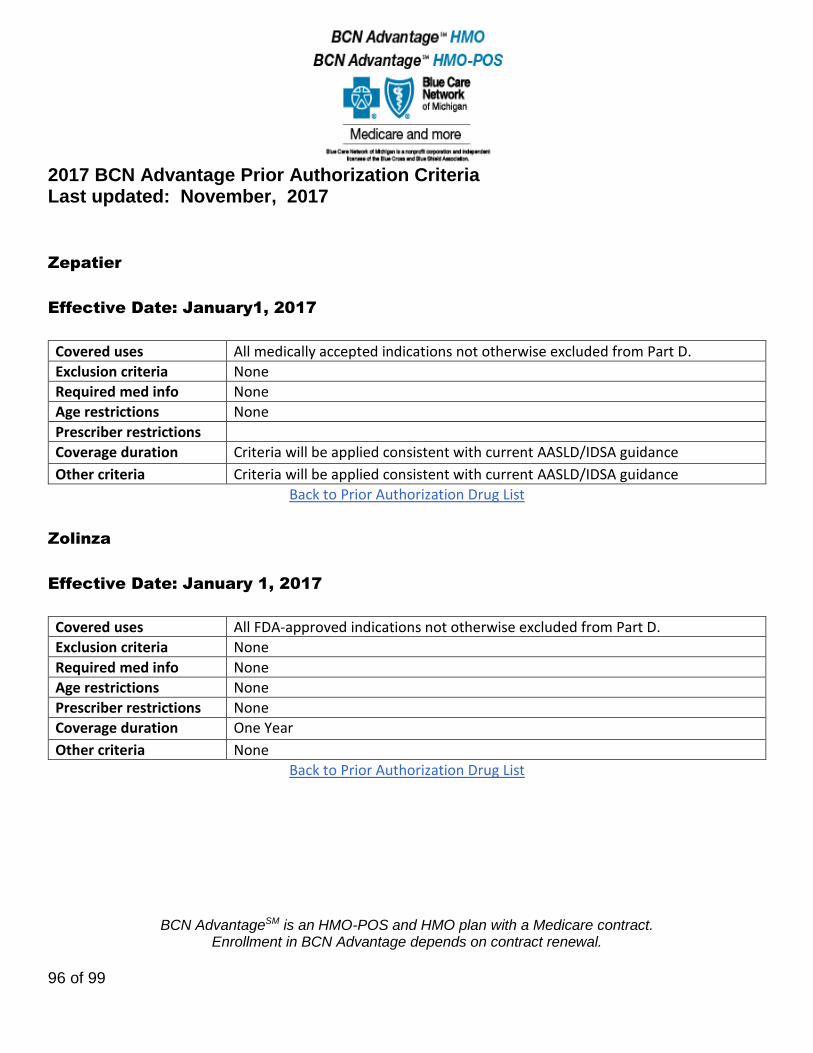
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
96 of 99
Zepatier
Effective Date: January1, 2017
Covered uses All medically accepted indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions
Coverage duration Criteria will be applied consistent with current AASLD/IDSA guidance
Other criteria Criteria will be applied consistent with current AASLD/IDSA guidance
Back to Prior Authorization Drug List
Zolinza
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
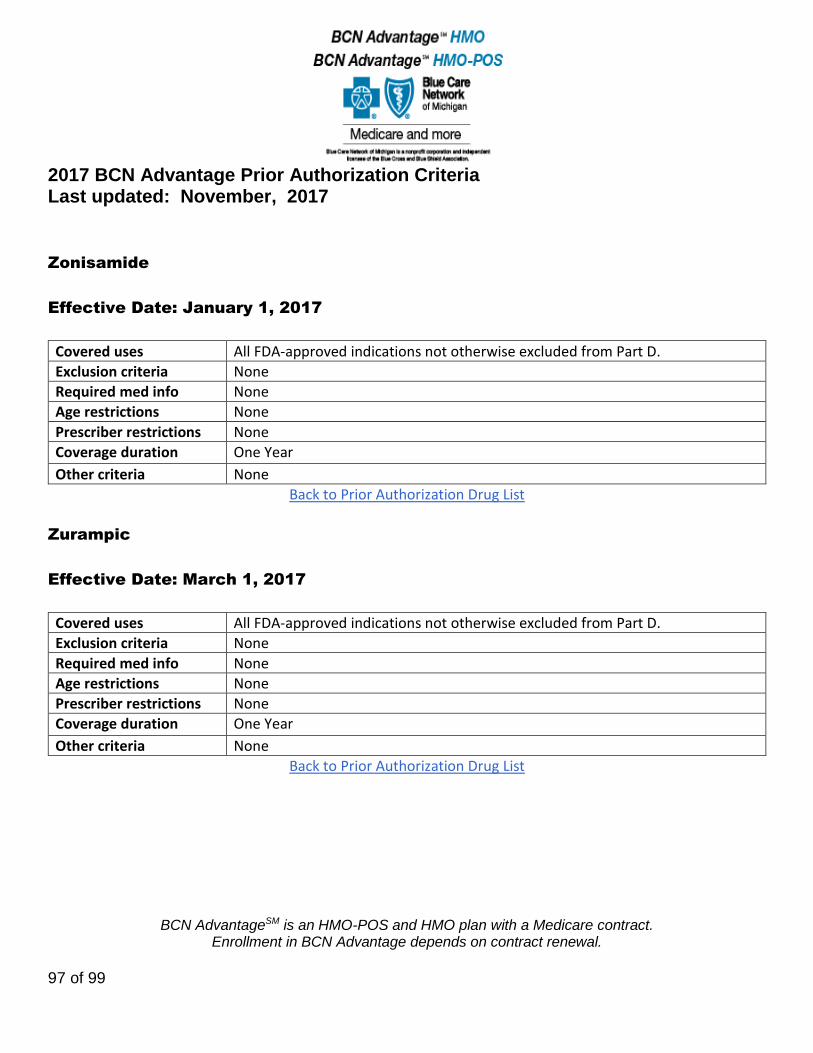
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
97 of 99
Zonisamide
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Zurampic
Effective Date: March 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
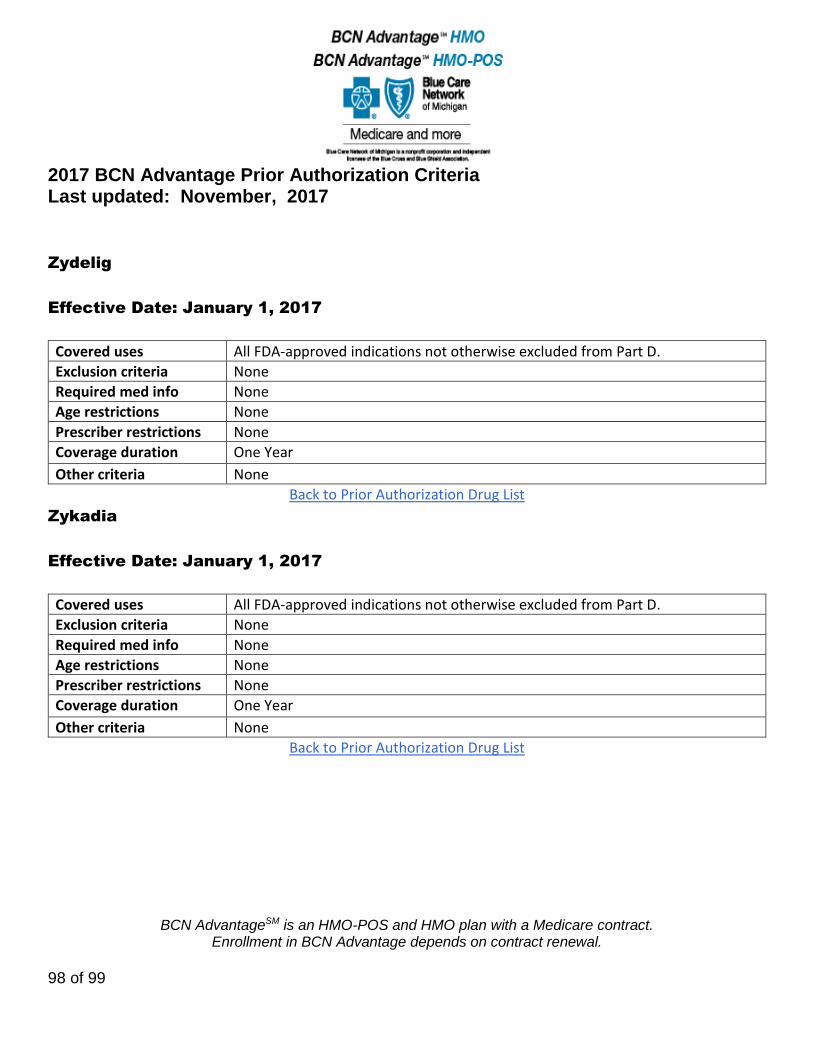
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
98 of 99
Zydelig
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
Zykadia
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D.
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
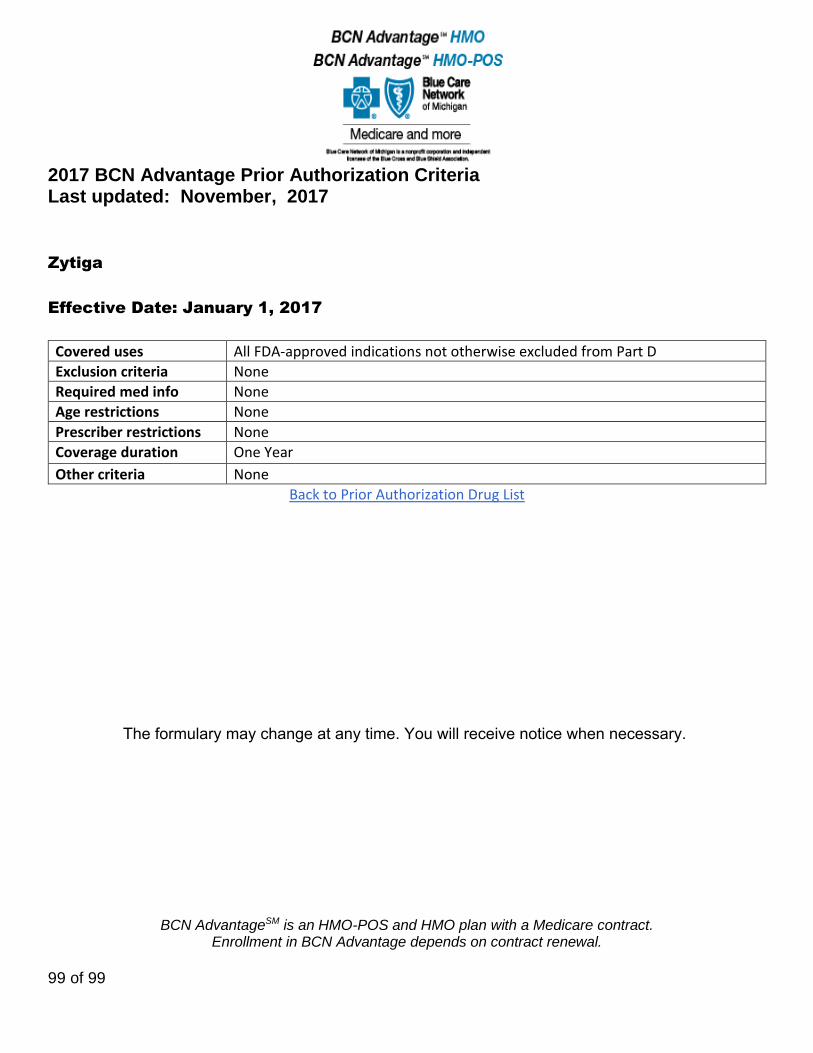
2017 BCN Advantage Prior Authorization Criteria Last updated: November, 2017
BCN AdvantageSM is an HMO-POS and HMO plan with a Medicare contract. Enrollment in BCN Advantage depends on contract renewal.
99 of 99
Zytiga
Effective Date: January 1, 2017
Covered uses All FDA-approved indications not otherwise excluded from Part D
Exclusion criteria None
Required med info None
Age restrictions None
Prescriber restrictions None
Coverage duration One Year
Other criteria None
Back to Prior Authorization Drug List
The formulary may change at any time. You will receive notice when necessary.





























