Embed Size (px)
Citation preview
Howard B. Burchell, MD, was born in Athens, Ontario, Canada. He received his medical degree from the University of Toronto in 1932. He continued his training at Toronto General Hospital, the University of Pittsburgh, the Mayo Graduate School, and the London Hospital Medical School and Heart Hospital
in England. After World War II, during which Dr. Burchell served in the U.S. Army Medical Corps, he returned to the Mayo Clinic as a consultant, ultimately becoming Professor of Medicine. In 1968, Dr. Burchell was appointed Chief in Cardiology at the University of Minnesota Medical School, a position he held until his official retirement in 1975.
After retirement, Dr. Burchell was Professor Emeritus of Medicine and an active participant in the medical academic life of the Minneapolis/St. Paul community. He received several professional honors both during his career and after retirement. Today he is widely recognized as one of the foremost authorities in cardiology during the 1950s and 1960s. He is considered to have set the stage, with his colleagues, for the ablation of accessory AV connections, which ultimately led to the current era of interventional cardiac electrophysiology. The annual Burchell lecture is a tradition that was created over twelve years ago as a way to honor Dr. Burchell and his contributions to the world of medicine.
} CARDIOVASCULAR GRAND ROUNDSThursday, April 28, 2016
6:00 – 7:00 PM - Lecture ANW Education Building, Watson Room
7:00 – 8:00 PM – Reception MHI Foundation Building | Lower Level Foyer 920 East 28th Street | Minneapolis, MN 55407
2016 Howard B. Burchell Memorial LectureEmergence of Nonobstructive Coronary Artery Disease in Women
CARL J. PEPINE, MD, MACCProfessor of MedicineUniversity of Florida
LEARNING OBJECTIVES:At the completion of this activity, the participants should be able to:
} Review the problem of nonobstructive CAD in patients with symptoms/signs of ischemia.
} Discuss mechanisms of ischemia in these patients. } Discuss management strategies in these patients.
Pre-registration is required due to limited seating. Visit online at mplsheart.org/burchell to register.
For cancellation or changes, kindly provide a 48-hour notice by e-mail to [email protected].
See reverse side for Information about parking, accreditation statement, disclosure statements.
Next Day Community Event on April 29, 2016 | 9:00 AM | American Swedish Institute: Mars vs. Venus: True for your heart too? To attend, please register at www.mplsheart.org/venusmars
} ABOUT DR. HOWARD B. BURCHELL
ACKNOWLEDGMENT OF SUPPORT This presentation is partially funded by an educational grant from Abbott Vascular, a division of Abbott Laboratories.

PARKINGAttendance includes free parking in the Abbott Northwestern Hospital Visitor ramp off East 28th Street. Vouchers will be provided upon arrival.
ACCREDITATION STATEMENTPhysician: This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Allina Health and Minneapolis Heart Institute Foundation. Allina Health is accredited by the ACCME to provide continuing medical education for physicians.
Allina Health designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nurse: This activity has been designed to meet the Minnesota Board of Nursing continuing education requirements for 1.2 hours of credit. The nurse is responsible for determining whether this activity meets the requirements for acceptable continuing education.
DISCLOSURE STATEMENTSSpeaker: Dr. Pepine has declared that he does not have any conflicts of interest to disclose.
Planning Committee: Dr. Michael Miedema, Dr. Scott Sharkey and Jolene Bell Makowesky have declared that they do not have any conflicts of interest associated with the planning of this activity. Dr. Robert Schwartz declared the following relationship - consultant: Boston Scientific.
PLEASE SAVE A COPY OF THIS FLIER AS YOUR CERTIFICATE OF ATTENDANCE:
Signature:
My signature verifies that I have attended the above stated number of hours of the CME activity.
Allina Health - Learning & Development2925 Chicago Ave - MR 10701 - Minneapolis MN 55407
Facebook.com/MinneapolisHeart
Twitter.com/MHIF_Heart
Together, we can create a world without heart and vascular disease.

1
Carl J Pepine, MD, MACCUniversity of FloridaGainesville, Florida
Minneapolis Heart Institute Grand Rounds
Burchell Memorial Lecture April 28, 2016: 6:00‐7:00 PM
Emergence of Nonobstructive Coronary Artery Disease in Women
Carl J Pepine, MD
Grants/Research Support: Aastrom, Abbott/AbbVie, Amarin Pharma, Amorycyte, Angioblast/Mesoblast, Baxter Healthcare, Bayer HealthCare, Capricor, Cytori, Daiichi-Sankyo, Gilead, GlaxoSmithKline, Ikaria/Bellerophon, Juventas, Lilly, Merck, NeoStem, NIH/NHLBI/NIA, Pfizer, sanofi-aventis, TEVA, Viron.
Consultant: Aastrom, Abbott/AbbVie-DSMB, Amarin Pharma, Angioblast Systems-DSMB, Bayer HealthCare, BioCardia, Cytori, Gilead, Janssen, Juventas, Lilly/CCF-DSMB, Merck, Mesoblast-DSMB, Sanofi, Servier, Slack Inc.
Speakers Bureau: None
Stock Shareholder: None
Other Financial or Material Support:
Holds two patents with the University of Florida
Disclosures

2
Talking Points
1. Background for nonobstructive atherosclerotic CAD in stable CAD (prevalence, prognosis, predictors).
2. Role of coronary microvascular dysfunction (CMD).
3. Review major CMD mechanisms, emphasize multiplicity.
4. Illustrate complexities of chronic CMD phenotype and links with HFpEF.
5. Provide framework for novel approaches to address mechanisms useful for designing trials aimed at reducing
residual risk.
Emergence of Nonobstructive Coronary Artery Disease in Women
3
• Compared with men, more women have symptoms/signs of stable IHD and more die of IHD, yet most of these women have “normal coronary arteries” at angiography.
• Concerns led to the NHLBI‐WISE Project1 in 1996:
‐ Consecutive case cohort of women (n=936) with findings (stable angina/signs) suggesting IHD but ~65% had no obstructive CAD (e.g. ≥50%, Core Lab QCA).
‐ Clearly, not a benign syndrome!
‐ At 5‐yrs 13.1% death/MI (or 2.6%/yr).2
‐ At 10‐yrs 20% had died, of these, 115 (62%) were CV deaths.‐ 25% of all deaths and CV deaths occurred without obstructive CAD;
‐ 3/4 of these angios were read on‐site as “Normal Coronary Arteries”).2,3
1JACC 1999;33:1453-61. 2Arch Intern Med 2009;169:843-50. 3Am Heart J 2013;166:134-41..
What Causes SIHD? WISE Original Cohort‐

3
5
5- and 10-Yr CV Event Rates in Women With Symptomatic Ischemia and No Obstructive CAD vs Reference WomenWISE-WTH Collaboration
0
10
20
30
Eve
nt
Rat
e (%
)
Asymptomatic(n=1000)
2.4%
7.9%*
16.0%*
NormalCoronaryArteries(n=318)
NonobstructiveCAD
(n=222)
*Driven mostly by hospitalization for HF Gulati M, et al. Arch Intern Med. 2009;169:843-850. Sharaf, B et al. Am Heart J 2013;166:134-41.
5-Year Event Rates Vs Asymptomatic(MI, Hospitalization for HF,
Stroke, or CV death)Asymptomatic comparators
age- and race-matched participants in Women Take Heart Project
P=0.002 vs asymptomatic
P=0.001 vs normal coronary arteries
Symptomatic
6.7%
12.8%*
25.9%*
0
10
20
30
40
Normal CoronaryArteries
Non-obstructiveCAD
Obstructive CAD(Event Rate (%)
10-Year Event Rates(MI or CV death)
(n=339) (n=228)(n=350)
P=0.01 vs “normal coronary arteries”
P=0.001 vs normal coronary arteries
6
In IHD With Nonobstructive CAD, Symptoms and Disability Status Rival Obstructive CADWISE
0
20
40
60
80
100
5-Year Rates of Typical Angina and Functional DisabilityWomen with Myocardial Ischemia on Non-invasive Testing (n=883)
5-Y
ear
Rat
es o
f Ty
pic
al A
ng
ina
and
Fu
nct
ion
al D
isab
ilit
y(%
of
pat
ien
ts)
NonobstructiveCAD
1-VesselCAD
2-VesselCAD
3-VesselCAD
Shaw LJ, et al. Circulation. 2006;114:894-904.
Functional disability: Duke Activity Status Index score in metabolic equivalents <4.74.n=883 women presenting for evaluation of chest pain or other equivalent symptoms.
45%50%
39%
70%
39%
70%
35%
55%
Typical angina (P=0.68)
Functional disability (P=0.037)
Extent of CAD by Coronary Angiography

4
7
Cardiovascular Costs of Non-obstructive CAD in Women with Myocardial IschemiaWISE
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000Direct Costs
(2003 US Dollars )
5-Year Direct Cardiovascular Costs(Drug treatment, Office visits, Outpatient procedures, Hospitalization)
Cost componentsNon-obstructive
CAD1-Vessel CAD 2-Vessel CAD 3-Vessel CAD
Outpatient 6.7% 5.8% 14.3% 14.8%
Drug 32.6% 29.5% 27.0% 25.5%
Hospitalization 60.7% 64.7% 58.7% 59.7%
Shaw LJ, et al. Circulation. 2006;114:894-904.
*Women (n=883) who had clinically ordered coronary angiography after exhibiting myocardial ischemia on non‐invasive testing
P<0.0001(Nonobstructive CAD
vs 3-Vessel CAD
8
48%
17%
35%
19%14%
68%
010203040506070
Normal coronaryarteries
Diffuse non‐obstructive CAD
Obstructive CAD
(% of Patients )
• Retrospective cohort study (1998-2009)– Eastern Denmark
Stable Angina Without Obstructive CAD: Prevalence and Outcomes
Patients referred for coronary angiography for stable angina
(No history of CV disease)
Men(n=6512)
Women(n=4711)
Jespersen, L et al. Eur Heart J 2012;33:734‐44.
Findings on coronary angiography

5
9
Nonobstructive CAD and Risk of MI or Death in a Mostly Male Population
Death or MI at 1 Year
Obstructive CAD
3-Vessel or left main
2-Vessel
1-Vessel
Nonobstructive CAD
3-Vessel
2-Vessel
1-Vessel
No apparent CAD (ref)
HR (95% CI)
1.0 2.0 6.00.5
37,674 U.S. Veterans (96% Male) who had elective coronary
angiography(2007‐2012)
22%
22%55%
Obstructive CAD
Nonobstructive CAD
No apparent CAD
• Obstructive CAD on angiography more common than in studies of mostly women
• Nonobstructive CAD associated with increased risk of MI or death
Maddox, TM et al. JAMA 2014;312:1754‐63.
10Jespersen L, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risk of major adverse CV events. Eur Heart J 2012;33:734‐44.
Obstructive coronary artery disease by examination year among stable angina patients referred for angiography
Men Women

6
11
• Followed 11,223 pts with SAP and no prior CVD having a first angiogram (CAG) 1998‐2009 for SAP plus 5,695 asymptomatic reference individuals for 7.8 yrs (median).
• Pts with SAP had 3‐4X higher risk of CVD hospitalization irrespective of CAG findings and CV comorbidity. Multivariable adj HRs (95%CI) for pts with angiographically “normal coronary arteries” was 3.0(2.5‐3.5), for “diffuse nonobst CAD” 3.9(3.3‐4.6) and for “1‐3‐ves obst CAD” 3.6‐4.1(range)(all <P 0.001). Mean accumulated hospital time was 3.5(3.0‐4.0)(ds/10 yrs F/U) in reference individuals and 4.5(3.8‐5.2)/7.0(5.4‐8.6)/6.7(5.2‐8.1)/6.1(5.2‐7.4)/8.6(6.6‐10.7) in pts with “normal coronary arteries”, ”diffuse nonobstCAD”, and 1‐,2‐,3‐ves dis, respectively (all P< 0.05, age‐adjusted).
• SAP symptoms predicted repeat CAG with multivariable adj HRs for pts with “normal coronary arteries” being 2.3(1.9‐2.9), for “diffuse nonobst CAD” 5.5(4.4‐6.8) and for “obst CAD” 6.6‐9.4(range)(all P<0.001).
• SAP patients with “normal coronary arteries” or “diffuse nonobst CAD” have considerably greater CVD burdens in terms of CVD hospitalization and repeat CAG vs asymptomatic reference individuals even after adjustment for CV risk factors and exclusion of CV comorbidities.
• Contrary to common perception, excluding obst CAD by CAG in such patients does not ensure a benign CV prognosis.
Prognosis for Nonobstructive CAD with Stable Angina:
Risks for CVD hospitalization and repeat coronary angiography
Jespersen, et al. Burden of Hospital Admission and Repeat Angiography in Angina Pectoris Patients with and without Coronary Artery Disease: A Registry‐Based Cohort Study. Plos one. 2014;9:4(1 April) e93170
WISE: Continued:• Limitations: small sample, selection bias, no reference group, etc.
• WISE‐WTH collaboration1 provided a large case‐match reference group of asymptomatic women with normal exercise stress tests.
• Multiple larger registry studies2, free of selection bias replicated the high prevalence of nonobstructive CAD among stable angina pts, adverse prognosis in women, and also extended findings to men.
• WISE‐CVD in 2009 (n=375) consecutive case cohort of women with stable angina/IHD findings with no obstructive CAD.
• New model to study CMD (no collateral flow, PCI, etc.) and HFpEF in patients with IHD.
1Arch Intern Med 2009;169:843‐50 2Denmark, Canada, NCDR, VA‐Cart.
What Causes SIHD: Role of Nonobstructive CAD

7
Five‐year Rates of CV Outcomes in Asymptomatic Women (WTH) vs. Symptomatic Women With Nonobstructive CAD (WISE)
Arch Intern Med 2009; 169(9): 843‐50
Outcomes, %Reference WISE
AdjustedP Valuec
AdjustedP Valuec,dAsymptomatic
Women (WTH)(n=1000)
“Normal Coronary Arteries”(n=318)
Nonobstructive CAD
(n=222)
MI 0.7 0.9 3.9 07 31
HF Hospitalization 0.3 3.3 5.6 <0.001 0.002
Stroke 1.0 2.4 5.2 0.002 0.004
CV Death 0.6 1.5 4.4 0.11 0.82
All‐cause Death 2.1 3.0 8.2 0.04 0.74
“Primary” (CV Death, MI, Stroke, HF Hosp)
2.4 7.9 16.0 <0.001 0.002
“Secondary” (All‐cause Death, MI, Stroke, HF Hosp)
3.9 9.1 19.1 <0.001 0.008
cAdjusted for age, race, BMI, SBP, diabetes, education, employment, family CAD history, smoking, and metabolic syndrome
dCompares WTH cohort with WISE cohort who had “normal coronary arteries”(<20% diameter stenosis)
• All stable angina patients with “first” coronary angiography 1998 to 2009 (11,223 pts and 5,705 case‐matched subjects), Eastern Denmark Registry1, assessed outcomes at 7yrs. 65% of women (4,711) vs 32% of men (6,512) had non‐ obstructive CAD (<50% stenosis). Although event rates were higher among women, when adjusted (age, BMI, BM, smoking, and lipid/BP lowering), risks were similar for women vs men. Analyzing women + men, risks for MACE increased with increasing degrees of nonobstructive CAD: adj HRs were 1.52 for “normal coronary arteries” and 1.85 for “diffuse non obstructive CAD” vs reference. For all‐cause mortality, HRs were 1.29 and 1.52, respectively, also had higher CV‐hosp. rates
• All stable angina patients with coronary angiography (N= 13,695) 9/99 to 12/02 in British Columbia, Canada assessed outcomes at 3 yrs F/U Using WISE angiographic definitions, nonobstructive CAD occurred in 42% of women vs 14% of men: such women were ~3X more likely vs men to have MACE at 1‐yr.
MACE= CV death, MI, stroke, or HF hospitalization. 1Eur Heart J 2012;33:734‐44. 2Am Heart J 2013;166:38‐44.
What Causes SIHD: Role of Nonobstructive CAD

8
Prognosis: Non obstructive CAD and Stable Ischemic Syndromes
(CV death or hospitalization for MI, HF, or stroke)
N= 11,223 SAP patients and 5,705 reference subjects
Jespersen L, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risk of major adverse CV events. Eur Heart J. 2012;33:734‐44.
NHLBI‐WISE, continued:
‐ HF hospitalization most prevalent outcome.1,2,3
‐ Different from reference group women.2
‐ Median baseline LVEDP 16mmHg, normal EF.
‐ LVEF >60% in sample hospitalized for HF.
‐ >95% had multiple CAD risk factors, most had endothelial dysfunction.4,5
‐ ~50% of those tested (Ado) had CFR <2.5.6
‐ >80% with “NCA” had athero/plaque by IVUS.7
1Circulation 2004;109:726‐732, 2Arch Intern Med 2009;169:843‐50. 3Am Heart J 2013;166:134‐41..4Circulation 2004;109:722‐5. 5Clin. Cardiol. 2007;30:69‐74. 6JACC
2010;55:2825‐32. 7J Inter Cardiol. 2010; 23:511‐19.
What Causes SIHD: Role of Nonobstructive CAD

9
• An alternative explanation for relative lack of obstructive CAD among women vs men with SIHD, could be that women with obstructive CAD are more likely to die before reaching hospital vs women with nonobstructive CAD.
• Overall, women have a lower incidence of cardiac sudden death (CSD) vs men (adj for CAD severity, MI, and HF) and obstructive CAD found in only ~half of women vs ~90% of men1.
• Pathological findings in CSD cases with nonobstructive CAD2‐4 found sex differences in extent/severity of coronary and myocardial findings in people 21‐54 yo3,4. Obstructive CAD was less likely in women (~60 vs ~80% of men)4. Yet, scar was present in ~half with obst CAD vs 17% with nonobstructive CAD and did not vary by sex.
• Among younger adults dying of IHD, fewer women have obstructive CAD,consistent with angio data in other IHD syndromes and MI exists in many without obstructive CAD. Findings do not support the notion that relative lack of obstructive CAD among women vs men with SIHD is related to more prehospital deaths among women with obstructive CAD.
Non Obstructive CAD and Cardiac Sudden Death
1Hayashi et al Circ Res 2015;116:1887‐906. 2Burke et al. Circulation 2002;105:297‐303.3Johnson et al Circulation 2009;120: S394. 4Smilowitz et al. Am Heart J 2011;161: 681‐8.
• HTN, diabetes, metabolic syndrome and smoking1 important due to high and increasing prevalence among women and known associations with microvascular disease.
• In the large, prospective CONFIRM registry2, HTN was present in majority with nonobstructive. HTN (adjHR: 1.93), diabetes (HR: 2.13) and smoking (HR: 1.47) were all associated with increased adverse outcome risk. Among women, nonobstructive CAD was associated with 67% excess all‐cause mortality risk.
• Findings consistent with HTN being major risk factor for atherosclerosis that underlies most nonobstructive and obstructive CAD. Postmenopausal women with HTN have endothelial dysfunction and microvascular dsieasein heart, brain, eye, and kidney.
• The strong association with LV systolic function seen in obstructive CAD is absent: LVEF is usually preserved with nonobstructive CAD. Measures of CAD extent/severity also appear important in the nonobstructive cohort but are not well developed.
PREDICTORS OF ADVERSE OUTCOMES WITH NONOBSTRUCTIVE CAD
1WISE Am Heart J 2013; 166:134‐41. 2CONFIRM Investigators. J Am Coll Cardiol 2011;58:849‐60.

10
WISE: Persistent Chest Pain in Women with Nonobstructive CAD Predicts Future CV Events
0.5
0.6
0.7
0.8
0.9
1
Prognosis of women (n=673) with and without persistent chest pain at 1-yr visit (without CV death, MI, stroke, of HF hospitalization).
Eve
nt-
Fre
e S
urv
ival
(%
)
0 1 2 3 4 5 6
Time Since Persistent Chest Pain Diagnosis (yrs)
Nonobst CADHazard Ratio
1.89 (1.06-3.39)P=0.03
Johnson B, Shaw L, Pepine C, et al. Eur Heart J. 2006;27:1408-15.
Nonobst CAD- No persistent chest pain (10.1%)Nonobst CAD- Persistent chest pain (20.5%)CAD- No persistent chest pain (38.2%)CAD- Persistent chest pain (36.8%)
Obst CADHazard Ratio
1.17 (0.76-1.80)P=0.49
• Cohort of 11,462 patients with CTA
• Men and women propensity matched for:
– Age
– CAD risk factors
– Angina typicality
– CAD extent and distribution
• Major adverse cardiac events (MACE) =Death or MI.
0.95
0.96
0.97
0.98
0.99
1
0 1 2 3
MACE‐Free Survival In Propensity‐Matched Cohort According to Presence of Nonobstructive CAD: CONFIRM
Normal
Nonobstructive CAD
MA
CE
-Fre
e S
urv
ival
P<0.0001
Follow-up Duration (yrs)
Patients with non-obstructive CAD had significantly higher event rates than patients without CAD by CTA
Leipsic J, et al. Radiology 2014;273:393-400

11
21
Coronary macro and microvascular systems
Coronary arteriolar endothelium: healthy vs. diseased heart (“quiescent” nonproliferative state vs. “activated” proinflammatory state)
Adapted from Gutterman et al. Circulation Research. 2016;118:157-172

12
Variable combinations of impaired dilation (endothelium‐dependent and endothelium‐independent mechanisms) and increased constriction caused by various stimuli. (adapted from Crea, F. et al. Coronary Microvascular Dysfunction)
Increased constriction
23
Alteration Cause
“Functional”
Endothelial cell dysfunction Athero RFs (HTN, smoking, hyperlipidemia, diabetes, etc.)
Smooth muscle cell dysfunction Spasm, hypertrophic cardiomyopathy, HTN, SNS, etc.
Autonomic NS dysfunction Exercise, coronary recanalization, HTN, others
Combinations of above
Mechanisms of Coronary Microvascular DysfunctionPepine et al J Am Coll Cardiol. 2015;66(17):1918‐33
24

13
Mechanisms of Coronary Microvascular Dysfunction Pepine et al J Am Coll Cardiol. 2015;66(17):1918‐33
Alteration Cause
Structural
Atherosclerotic plaque Atheroembolization‐ ACS, after PCI/stenting, etc.
Embolic Microembolization in ACS or after PCI/stenting, plat micro aggcalcium, tumor, vegetation (infective/noninfective), etc.
Vascular wall infiltration Infiltrative heart disease (amyloid, Fabry, Hurler, Hunter, homocystinuria, etc.
Inflammation SLE, PAN, RA, Rheum Fever, Takayasu, Kawasaki, giant cell arteritis, syphilis, salmonella ‐other infections, allergic vasculitis, serum sickness, cryoglobulinemia, Henoch‐Schönlein purpura, inflammatory bowel dis, primary biliary cirrhosis, Goodpasture, etc.
Intimal proliferation Radiation therapy, cardiac transplantation
Thrombosis without underlying atherosclerotic plaque
Polycythemia, thrombocytosis, hypercoagulability
Substance abuse Cocaine, amphetamines, others
25
Alteration Cause
Structural‐ Continued
Perivascular fibrosis Aortic stenosis, HTN, etc.
Vascular rarefaction Aortic stenosis, HTN, etc.
Vascular remodeling Hypertrophic CM, HTN, DM, etc.
Non‐coronary
Extramural compression Aortic stenosis, hypertrophic CM, HTN
Increased conduit vessel (Ao) stiffness Increased pulse wave velocity (aPWV) and SBP
Reduced diastolic perfusion time Aortic stenosis, increased HR
Mechanisms of Coronary Microvascular DysfunctionPepine et al J Am Coll Cardiol. 2015;66(17):1918‐33
26

14
27
Alone or in combination:
• Epicardial and/or microvascular coronary dysfunction (endothelial and/or vascular smooth muscle cell),
• Macro‐ and/or microvascular coronary spasm,
• Plaque fissuring with microparticle emboli,
• Heightened thrombosis with lysis,
• Inflammation/immune activation,
• Myocardial bridging
• etc.
Likely mechanism(s) for ischemia in the absence of a flow‐limiting stenosis
CMD in Women with Angina and Nonobstructive CAD: (WISE)Clin. Cardiol. 2007;30:69‐74
.
Athero RF conditions including age, SBP, and inflammatory markers explained only ~20% of the variability in CFR
28

15
Risk Factors and CMD(PET)Graf, et al. J Nucl Med 2007; 48:175‐81
• 85% of pts with ≥5 RFs had CMD and 100% of those with <2 RFs had normal CFR. • In ~2/3 of pts, angina explained by CMD: RFs had cumulative negative effect on CFR. • RF analysis enables estimation of individual probability of CMD.• CFR measurements recommended for pts with intermediate number of RFs.
• Age ≥60 y*• Menopause• T‐C ≥200 mg/dL• Trig ≥170 mg/dL• BP >140* />90 mmHg• IVS ≥12 mm*• Smoking• BMI ≥25• Family Hx of CAD
Multivariable model*
• Age ≥60 y*• Menopause• T‐C ≥200 mg/dL• Trig ≥170 mg/dL• BP >140* />90 mmHg• IVS ≥12 mm*• Smoking• BMI ≥25• Family Hx of CAD
Multivariable model*
Angina pts with nonobst CAD and controls: CFR vs. number CV risk factors (NRF)
29
Inflammation and CFRPET in Asymptomatic Male TwinsVaccarino JACC. 2011;57:1271-79
30

16
Correlations between CFR and pertinent study variables Variable Coefficient
r valueP value
Age (yrs) −0.29 0.04
Aortic systolic pressure (mmHg) −0.49 0.001
Aortic pulse pressure (mmHg) −0.35 0.01
Reflected pressure wave amplitude (AP) (mmHg) −0.48 0.001
Aortic augmentation index (%) −0.44 0.001
Round trip travel time of wave to and from periphery (Tr)(msec) 0.29 0.04
Diastolic pressure time index (DPTI)(mmHg ∙ sec) x 102 −0.38 0.006
Systolic pressure time index (SPTI) (mmHg ∙ sec) x 102 −0.37 0.008
Pulse pressure amplification (dimensionless) 0.45 0.001
Wasted LV energy (dyne‐sec/cm2) x 102 −0.47 0.001
Aortic pulse wave velocity (aPWV) (cm/sec) −0.51 0.001
Heart rate × aortic systolic pressure (mmHg x beats/min) x 102 −0.29 0.04
Association of aortic stiffness and wave reflections with CFR in women without obstructive CAD: WISE
Am Heart J. 2015 Dec;170(6):1243‐54
31
Association of aortic stiffness and wave reflections with CFR in women without obstructive CAD: WISE
Am Heart J. 2015 Dec;170(6):1243‐54
Multivariable Predictors of CFR
Variable Coefficient Standardized Coefficient
Model R2
(add in order)∆R2
(add in order)P value
Age (×10) -0.04 (0.07) -0.10 0.13 0.13 0.008
HTN History -0.01 (0.13) -0.01 0.13 0.0003 0.90
Diabetes History -0.07 (0.17) -0.07 0.13 0.004 0.62
BMI (×10) -0.10 (0.10) -0.15 0.13 <0.0001 0.98
Aortic SP (×10) -0.01 (0.06) -0.02 0.24 0.11 0.01
aPWV -0.002(0.0005) -0.50 0.42 0.18 0.002
Time Travel of Wave 0.01(0.01) 0.15 0.46 0.04 0.14
Amplification 1.23(0.81) 0.27 0.50 0.04 0.14
BMI= body mass index, aPWV= aortic pulse wave velocity measured by catheter pull‐back, Standardized coefficients are standardized so that their means =0 and SDs =1 to allow comparison of relative effect size between predictors independent of original units, Model R2 are the R2 of multivariable regression model, and ΔR2 of a predictor is the change of model R2 when the predictor is added to the model. The P tests whether the ΔR2 is significantly different from zero.
32

17
33
Proposed progression and relationship between vessel stiffness and other factors (endothelial and/or vascular smooth muscle [VSM] cell dysfunction) and reduced CFR
Mechanistic role for CMD in IHD
[Na+]i Ca++ Overload
CMDlimits O2
supply/distribution
late INa
Microvascular compression
further limits O2supply/distribution
Impaired LV relaxation
(LVEDP)
Cardiomyocyte hypoxia, ischemia metabolites,
acidosis, ROS, etc
Oxygen supply-demand mismatch
Aortic Stiffness
(aPWV)
Aging
Inflammation
AoSP
Endothelial Cells-Stained/epifluorescent
AJP Jan 98;43:H1803rd Order A
rterio
le
GeneticATP2B1
(rs12817819) RNF39 (rs2301753)
34

18
• Investigated relationships between major adverse outcomes and baseline CFR after IC adenosine in women referred to evaluate suspected ischemia.
• Using ROC analysis CFR<2.32 provided best prediction of adverse outcomes with sensitivity of 62 and specificity of 65.
– Women with CFR <2.32: major CV event rate 27%,
– Those with CFR ≥2.32: major CV event rate 12% (p=0.01) at 5.4 years.
• Overall, CFR is continuous predictor of major CV events, rather than there being a threshold for normal/abnormal.
Is there a CFRAdo threshold for adverse outcomes?Pepine, et al J Am Coll Cardiol 2010;55:2825‐32
CFR and Event Free Survival in WISEPepine CJ, et al. J Am Coll Cardiol 2010;55: 2825‐32
CFR and Event Free Survival in WISEPepine CJ, et al. J Am Coll Cardiol 2010;55: 2825‐32
Event‐Free Survival : Freedom from death, nonfatal MI, HF hospitalization, or stroke 5.4 yrs follow up
CFR ≥2.32
CRF <2.32
CFR ≥2.32
CRF <2.32
19
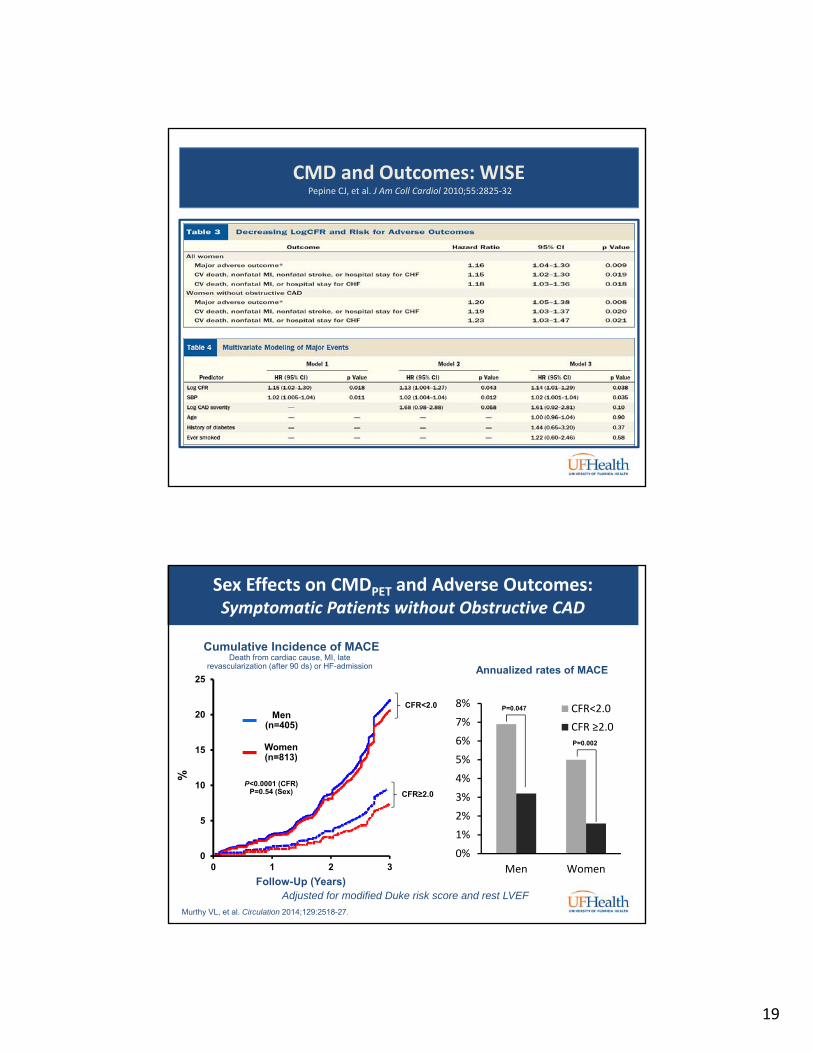
CMD and Outcomes: WISE Pepine CJ, et al. J Am Coll Cardiol 2010;55:2825‐32
Sex Effects on CMDPET and Adverse Outcomes:Symptomatic Patients without Obstructive CAD
0
5
10
15
20
25
0 1 2 3
Follow-Up (Years)
Men(n=405)
P<0.0001 (CFR)P=0.54 (Sex)
Cumulative Incidence of MACE Death from cardiac cause, MI, late
revascularization (after 90 ds) or HF-admission
Murthy VL, et al. Circulation 2014;129:2518-27.
Women(n=813)
%
CFR<2.0
CFR≥2.0
Adjusted for modified Duke risk score and rest LVEF
0%
1%
2%
3%
4%
5%
6%
7%
8%
Men Women
CFR<2.0
CFR ≥2.0
Annualized rates of MACE
P=0.047
P=0.002

20
Potential Therapies for CMD
• Nitrates
• Statins
• ACE inhibition
• ACE‐I + Aldosterone Blockade
• Calcium Antagonists
• Tricyclic antidepressants
• Estrogens
• PDE‐5 Inhibitions
• Exercise
• L‐arginine
• Ranolazine
• Ivabradine
• Ranolazine + Ivabradine
• Metformin
• Rho Kinase inhibitors
• Endothelin Receptor Blockers
Pharmacologic Non-Pharmacologic
• Exercise
• Cognitive behavioral therapy
• Transcendental meditation
• Transcutaneous electrical nerve stimulation
• Etc.
40
• Patients (N=45)– Typical angina at rest and/or effort– “Normal coronary angiograms”– Ischemia during exercise stress testing:
ECG plus reversible perfusion abnormalities
– Normal 12-lead ECG at rest– Normal left and right ventricular function
and absence of valvular disease– Total cholesterol <220 mg/dL – Not using statins or ACE inhibitors
Statin + ACE Inhibitor in Patients With Angina and Nonobstructive CAD
Results
• Ramipril + atorvastatin:
– Improved SAQ scores (P<0.001 vs placebo
– Improved mean exercise duration by 23.5% (vs no change with placebo)
– Greater increases in brachial flow-mediated dilation (P<0.001)
– Prevention of angina and ST depression during exercise stress test in 9 of 22 patients (vs none with placebo)
– Reductions in extracellular superoxide dismutase
Ramipril (10 mg/d) + Atorvastatin 40 mg/d)
Placebo
Randomized
6 months
Pizzi, C et al. Circulation 2004;109:53-8.

21
WISE Substudy: Effect of ACE Inhibition on CFR and Angina
• At 16 weeks, CFR significantly improved with ACE inhibition (quinapril 80 mg/d) vs placebo; adjusted for baseline CFR, diabetes history, and clinical site)
– Improvement concentrated among women with lower baseline CFR
• Improvement in CFR associated with reduction in angina
– ACE inhibition arm had higher (indicating improvement) SAQ scores at week 4 (P=0.0003) and 16 (P=0.02) versus placebo
– CFR improvement was independent predictor of SAQ improvement.
0
10
20
30
40
50
60
70CFR Improvement of >0.4
Pat
ien
ts (
%)
<2.5 >2.5
Baseline CFR
ACE inhibitor Placebo
CFR: coronary flow reserve.
Pauly DF, et al. Am Heart J. 2011;162:678-684.
P=0.03
62%
32%
12%15%
42
• Chronic stable angina, even in pts with “completely normal‐appearing” angiograms, carries a significant morbidity/overall adverse outcomes burden.
• Most have “nonobstructive CAD” and ~ half have coronary microvascular dysfunction (CMD):‐important prognostic factor,‐CMD linked with:
presence of multiple CVD risk factors, myocardial ischemia, as in pts with microvascular angina..
• Available invasive/noninvasive methods do not assess microvascular function in isolation‐total impact of both epicardial and microvascular disease on perfusion.
• Without epicardial obstruction, CFR <2.5‐generally considered abnormal (CMD).
• Management includes traditional life‐stlye modification and antianginals with novel therapies (e.g. metabolic agents, rho‐kinase inhibitors, ACE‐Is, late Na+
channel modifiers, statins, etc.).
Nonobstructive CAD in Women Summary
22
• Symptoms and signs of ischemia without obstructive CAD are highly prevalent (mostly women), have substantial morbidity, and contribute to significant health care costs.
• Optimal management strategy remains undefined, largely because the mechanism(s) are unclear. Coronary microvascular dysfunction is one prevalent mechanism.
• Clarifying mechanisms responsible for this syndrome would yield important clues to improve management.
43
44

























![PRESSURE VESSEL [Proses Pembuatan Pressure Vessel]](https://img.dokumen.tips/doc/110x75/546b26fab4af9fc2128b4e24/pressure-vessel-proses-pembuatan-pressure-vessel.jpg)

