Embed Size (px)
Citation preview

1
2016 Employee Benefits Guide
January 1, 2016 - December 31, 2016

2
This document is an outline of the coverage proposed by the carrier(s). It does not include all of the terms, coverage, exclusions, limitations, and conditions of the actual contract language. The policies and contracts themselves must be read for those details. Your full Summary Plan Document (SPD) is made available through your Benefits Department. The intent of this document is to provide you with general information regarding the status of, and/or potential concerns related to your current employee benefits environment. It does not necessarily fully address all of your specific issues. It should not be construed as, nor is it intended to provide, legal advice. Questions regarding specific coverage issues can be directed to the Benefit Advocates at Arthur J. Gallagher & Co., [email protected].

1
Customer Service and Contact Information 1
Eligibility, Enrollment and Useful Benefit Terms 2
Medical Plan Comparison Chart 3
Wellness Incentives 4
Dental Plan Summary 5
Vision Plan Summary 6
Group Life and AD&D 7
Voluntary Life Insurance Benefits & Rates 8
Short-Term and Long-Term Disability Benefits & Rates 9
Gap Plan 10
Long Term Care 11
Aflac - Worksite Products 12 - 13
Employee Assistance Program 14
Flexible Spending Account 15
Payroll Deductions 16
Important Information 17
CHIPRA Notice 18
Medicare D Notice 19 - 20
**If you (and/or your dependents) have Medicare or will become eligible for Medicare in the next 12 months, a Federal law gives you more choices about your prescription drug coverage. Please see pages 19 - 20 for more details.
Table of Contents

1
Arthur J. Gallagher & Co. is here to act as a liaison in your dealings with insurance carriers. If you have questions regarding your coverage or need assistance with claims, let us deal with the insurance company for you. Please contact anyone at Arthur J. Gallagher & Co. with questions regarding your employee benefits package.
For information on how to enroll in benefits, please contact
Rebekah Fontenot in the Benefits Department.
Customer Service and Contact Information
Phone: (844) 845-5125
Email: [email protected]
Hours of Operation: Monday - Friday
7:30 a.m. - 5:30 p.m. CST
Benefit Carrier Group Number/Network Customer Service Website
Medical United Healthcare Group # 903441 Network: ChoicePlus
866-633-2446 www.myuhc.com
Dental Assurant Group # 5469012 Network: Assurant Dental
800-442-7742 www.assurantemployee benefits.com
Vision Davis Vision Group # 503949 800-999-5431 www.davisvision.com
Group Life and AD&D
Reliance Standard Group # 153132 800-351-7500 www.reliancestandard.com
Voluntary Life Reliance Standard Group # 153132 800-351-7500 www.reliancestandard.com
Short-Term Disability Reliance Standard Group # 326577 800-351-7500 www.reliancestandard.com
Long-Term Disability Reliance Standard Group # 301619 800-351-7500 www.reliancestandard.com
GAP Plan American Fidelity N/A 888-485-1347 www.afadvantage.com
Employee Assistance Program (EAP)
HMSA N/A 800-847-7240 www.my-life-resource.com
Flexible Spending Account (FSA)
TASC N/A 800-422-4661 www.tasconline.com
Long Term Care Unum N/A 800-227-4165 N/A
Accident and Critical Illness/Cancer
Aflac N/A 800-433-3036 www.aflac.com
COBRA Administration
ADP N/A 800-526-2720 www.benedirect.adp.com

2
Eligibility, Enrollment and Useful Benefit Terms
Eligibility: New employees are effective the first of the month
following 59 days of full time employment. The first 59 days of employment are considered the employee’s initial eligibility period.
You are eligible if you are a full-time employee regularly scheduled to work at least an average of 30 hours a week.
Open enrollment applies to all lines of coverage and is subject to plan limitations.
The open enrollment period is the only time employees may enroll in the above listed coverage without the occurrence of a qualifying event (see definition below).
Certain benefits are offered during an employee’s initial eligibility period on a guaranteed-issue basis. Enrollments/changes requested in certain benefit plans when an employee is no longer within their initial eligibility period require evidence of insurability and enrollment is not guaranteed. Examples of such plans include: Voluntary Life, STD, LTD, Critical Illness/Cancer, and Long Term Care.
Making Enrollment Changes During the Year: In most cases, your benefit elections will remain in effect for the entire plan year (January 1st - December 31st). During the annual enrollment period, you have the opportunity to review your benefit elections and make changes for the coming year. You may only make changes to your elections during the year if you have one of the following status changes:
Marriage, divorce or legal separation (if your state recognizes legal separation);
Gain or loss of an eligible dependent for reasons such as birth, adoption, court order, disability, death; reaching the dependent child age limit; or
Significant changes in employment or employer-sponsored benefit coverage that affect you or your spouse’s benefit eligibility.
Your benefit change must be consistent with your change in family status.
Co-payment: Co-payments for office visits and prescription drugs do not apply toward the deductible but DO apply to the out-of-pocket payment limit.
Calendar Year Deductible and Out-of-Pocket Maximum: Expenses incurred toward your annual deductible and your out-of-pocket maximum are credited on a calendar year basis. A calendar year is January 1st - December 31st. Your deductible and out-of-pocket maximum will restart January 1st each year, regardless of the expenses you incurred in the prior calendar year or when your annual open enrollment period occurs.
Primary Care Physicians/Specialty Physician Referrals: You are NOT required to select a primary care physician (PCP) or obtain referrals for specialty physicians. For the best coverage be sure that all providers (doctors, labs, x-rays, etc.) participate in-network for the best coverage.
Dependent Age Limitation: Your dependent children are eligible for coverage on your Medical, Dental, Vision, Voluntary Life and Flexible Spending Account plans until the age of 26 regardless of their marital, student, or financial dependency status.
In-Network vs. Out-of-Network Benefits: AMERISAFE, Inc.’s medical plans offer in-network and out-of-network benefit levels. When a doctor or hospital agrees to be in the plan’s network, they are contractually bound not to charge over a specific amount for services covered by the plan. When you choose an in-network provider, they will file a claim on your behalf and you are not held responsible for amounts that the provider may charge in excess of their contracted rates. Out-of-network expenses are paid according to ‘Usual and Customary’ charges, which may leave you with significant out-of-pocket expenses. For the best benefit available under the plan, you should utilize in-network providers when possible. Out-of-network benefit levels can be found on the Summary of Benefits and Coverage.
IRS regulations require that for enrollment due to the qualifying events above, change forms must be submitted within 30 days of that qualifying event. Contact your Benefits Department for information on completing these forms.

3
Medical Plan Comparison Chart
Benefit PPO Plan
In-Network Benefits PPO Plan
Out-Of-Network Benefits
Annual Deductible Co-pays do not accumulate
$1,500 Individual $3,000 Family
$3,000 Individual $6,000 Family
Annual Out-of-pocket Maximum Includes deductible, co-insurance and co-pays
$3,500 Individual $7,000 Family
$7,000 Individual $14,000 Family
Co-insurance (amount you pay after deductible)
10% 30%
Hospital Services - Inpatient 10% after deductible 30% after deductible
Emergency Room Treatment (Emergency Situation)
$350 co-pay $350 co-pay
Urgent Care Center Services Additional services/supplies may incur additional fees
$75 co-pay 30% after deductible
Physician Visits Primary Care Physician Specialist
$20 co-pay $20 co-pay
30% after deductible 30% after deductible
Preventive Care (Office Visit) Physician’s Services Preventive Testing
Paid at 100% Not Covered
Outpatient Surgery 10% after deductible 30% after deductible
Diagnostic Lab and X-Ray - Outpatient Paid at 100% 30% after deductible
Major Diagnostic (CT, PET, MRI, MRA and Nuclear Medicine)
10% after deductible 30% after deductible
Prescription Drug Program1
(30 day supply) Tier 1 Tier 2 Tier 3
$10 co-pay $25 co-pay $50 co-pay
The applicable co-pay below plus the difference
in cost. $10 co-pay $25 co-pay $50 co-pay
1 Prescription Drug Program - Continued Mandatory Mail Order is required for Specialty Medications Mandatory Mail Order for Certain Maintenance Medications - Unless Opt Out is Selected Step Therapy and/or Prior Authorization May Be Required - More information on the Benefits Intranet
Please review your plan document for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.

4
Wellness Incentives
Wellness Incentives
One of the main goals of the AMERISAFE benefits program is to keep employees and their families healthy. To show our dedication to your health, AMERISAFE offers the following wellness incentives:
Gym Membership Reimbursement - All Eligible Employees
A reimbursement of up to $25.00 per month will be provided to employees actively enrolled in a gym membership. To qualify for this reimbursement you must provide documentation showing your monthly cost as well as the name of the gym you are attending to the Benefits Department. This reimbursement will be reflected on the final paycheck of each month. Recertification of membership status is required every July and January. Simply provide proof of your July and January payments to the Benefits Department to continue receiving the incentive. Employees who cancel their membership between recertification periods are required to notify Rebekah Fontenot in the Benefits Department immediately.
Time Off For Wellness Exam - All Eligible Employees
Even if you are not enrolled in the AMERISAFE Medical plan, you are eligible for up to four hours of paid time off once annually to obtain a Routine Wellness examination. To obtain this benefit, your health care provider must complete the Wellness Exam Certification Form, which is located on the Benefits intranet. Your form must be returned to Rebekah Fontenot in the Benefits Department.
Employees Enrolled in the AMERISAFE Medical Plan
A reimbursement of $115.00 will be provided to employees enrolled in the AMERISAFE Medical Plan who have a Routine Wellness examination between November 1, 2015 and November 1, 2016. The $115 reimbursement will be reflected on eligible employees’ mid-December paychecks and is subject to all applicable taxes. To obtain this benefit, your health care provider must complete the Wellness Exam Certification Form, which is located on the Benefits intranet. Your form must be returned to Rebekah Fontenot in the Benefits Department by November 10, 2016 in order to receive this incentive.

5
Dental Plan Summary
While there is a network of providers you can utilize, benefit percentages are the same regardless of whether you visit an in-network or out-of-network provider. Utilizing an in-network provider will result in a lower patient responsibility overall. Please review your plan document for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage. Out-of-Network benefits are subject to Reasonable and Customary charges and you may be balance billed if your dentist charges above this amount.
Benefit Basic Plan Enhanced Plan
Type I - Preventive Services Cleanings, exams, x-rays (Note: Preventive services do not apply towards your annual benefit maximum.)
20% - no deductible 20% - no deductible
Type II - Basic Services Fillings, root canals, non-surgical periodontal, oral surgery
20% after deductible 20% after deductible
Type III - Major Services Extractions, crowns (5-year replacement), inlays/onlays, bridges, dentures, repairs, surgical peri-odontal care
50% after deductible 50% after deductible
Annual Deductible $75 Individual $225 Family
$75 Individual $225 Family
Annual Maximum $1,000 $2,000
Orthodontia
50% to $1,000 lifetime maximum per person.
50% to $1,000 lifetime maximum per person.

6
Vision Plan Summary
Please review your plan document for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
Benefit In-Network
Eye Exam $10 co-pay
Contact Lens Evaluation & Fitting
$10 co-pay (in addition to Exam co-pay)
Frames/Lenses
Single Vision $10 co-pay
Bifocal Lenses $10 co-pay
Trifocal Lenses $10 co-pay
Frames Covered in full frames Frame Allowance
Any Fashion or Designer level frame from Davis Vision’s Collection
$130 allowance toward any frame plus 20% off balance
Contacts - in lieu of glasses Davis Vision Collection Standard, Soft Contacts
No charge for one year’s supply
No co-pay, $130 allowance
Exam Frequency Every calendar year
Lens Frequency Every calendar year
Frames Frequency Every other calendar year

7
Basic Term Life Insurance and AD&D
Group Life and AD&D Benefits
Benefit $50,000
Guarantee Issue Amount $50,000
Accidental Death & Dismemberment $50,000
Age Reduction Schedule 50% at age 70
Benefits end at retirement

8
Voluntary Life Insurance Benefits & Rates
Voluntary Life Benefits
Employee Life Amount $500,000 ($10,000 increments)
Employee Guarantee Issue Amount $200,000 (under age 70)
Spouse Life Amount $250,000 ($5,000 increments)
Spouse Guarantee Issue Amount $50,000 if under age 70
Child Life Amount 14 days to 6 months - $500
6 months to age 26 - $10,000
Age Reduction Schedule 50% at age 70
Portability Included
Newly-eligible: Employees and dependents may elect coverage up to the Guaranteed Issue amount without answering any medical questions. During annual open enrollment: Employees currently enrolled in the Voluntary Life Plan may request up to $40,000 in additional coverage for themselves, in $10,000 increments, without providing Evidence of Insurability (EOI). Employees who currently have their spouse enrolled in this plan may request up to $20,000 in additional coverage, in $5,000 increments, without providing EOI for their spouse. Please note that dependents in a state of limited ability are not eligible for increases without completion of an Evidence of Insurability form and approval by RSL.
Age Rated Premiums Employee and Spouse
(rate per $1,000)
Life Rate: Up to 30 $0.07
30 - 34 $0.08
35 - 39 $0.11
40 - 44 $0.16
45 - 49 $0.27
50 - 54 $0.47
55 - 59 $0.73
60 - 64 $0.95
65 - 69 $1.65
70 - 74 $2.65
75 - 79 $4.24
Child Life Rate (per $1,000) $0.20
$100,000 ÷ $1,000 = 100 x $0.11 = $11.00
Elected Benefit
Amount
Rate
Above
Your Monthly
Cost
**For example: A 36-year-old employee wants $100,000 of coverage**
To qualify for the Guarantee Issue Benefits of the plan as outlined above, employees and spouses must be under age 70. Employees must be actively at work and dependents may not be in a period of limited activity.

9
Short and Long-Term Disability
Short-Term Disability Benefits1
Weekly Benefit 60% of weekly income
Maximum Weekly Benefit $1,250
Elimination Period Accident Benefit Begins Illness Benefit Begins
15th day 15th day
Benefit Duration Up to 11 weeks
Long-Term Disability Benefits1
Monthly Benefit 60% of income
Maximum Monthly Benefit $5,000
Elimination Period 90 days
Maximum Benefit Duration Social Security Normal Retirement Age
Own Occupation Limitation 24 months
Mental/Nervous Limitation 24 months
Substance Abuse Limitation 24 months
Benefits Integration Full Family Direct
Pre-existing Limitation 3 / 12
Survivor Benefit 3 months
RATE PER $10 OF BENEFIT=$.30 **Example below is for an employee who earns $40,000 per year.**
To calculate your weekly salary
$40,000 ÷ 52 = $769.23
Annual Salary
Multiply your weekly salary by the 60% benefit, divide by the $10 benefit rate, then multiply by $.31. This is your monthly rate.
$769.23 x 60% ÷ $10 x $0.31 = $14.31
Weekly Salary
Rate
Above
Your Monthly Rate
RATE PER $100 OF COVERED PAYROLL = $.49 **Example below is for a 36 year-old employee who earns $30,000 per year**
Step 1: Divide annual salary by 12 (to get your monthly salary) $30,000 / 12 = $2,500.00
Step 2: Divide your monthly salary by 100 $2,500 / 100 = $25
Step 3: Multiply step 2 by $.49 to determine monthly premium 25 X .49 = $12.25
1Employees that have previously declined enrollment in the Short Term Disability Plan must submit
Evidence of Insurability and Enrollment is not guaranteed.
1Employees that have previously declined enrollment in the Long Term Disability Plan must submit
Evidence of Insurability and enrollment is not guaranteed.

10
GAP Plan - American Fidelity
Please see the Important Policy Provisions in the GAP Brochure located on the Intranet, under the Benefits Department tab.

11
Long Term Care
UNUM Long Term Care Benefit and Premium Information can be located on the Intranet, under the Benefits Department tab.

12
Aflac Information

13
Aflac Information
For more information on Aflac products, please refer to the plan documents located on the
AMERISAFE intranet.

14
Employee Assistance Program (EAP)
Confidential!
Free to all household members!
Not just for “counseling”!

15
Flexible Spending Account (FSA)
FSA annual election not to exceed $2,500 Dependent Care annual election not to exceed $5,000
16
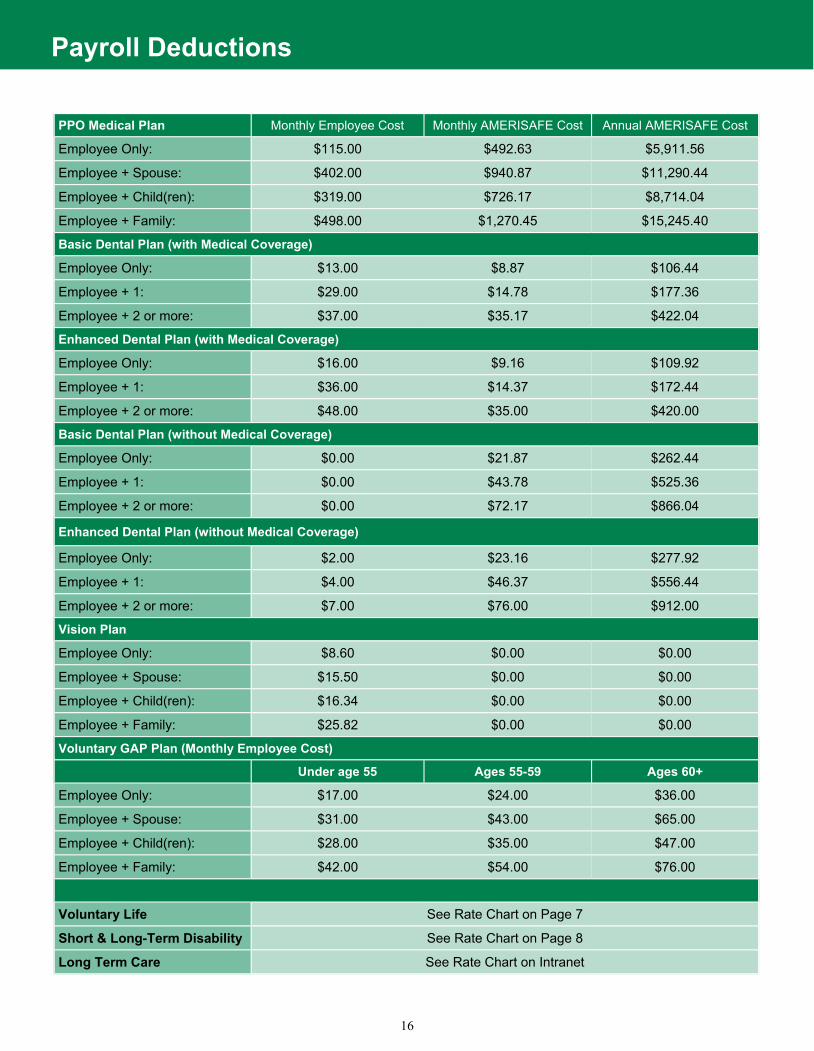
Payroll Deductions
PPO Medical Plan Monthly Employee Cost Monthly AMERISAFE Cost Annual AMERISAFE Cost
Employee Only: $115.00 $492.63 $5,911.56
Employee + Spouse: $402.00 $940.87 $11,290.44
Employee + Child(ren): $319.00 $726.17 $8,714.04
Employee + Family: $498.00 $1,270.45 $15,245.40
Basic Dental Plan (with Medical Coverage)
Employee Only: $13.00 $8.87 $106.44
Employee + 1: $29.00 $14.78 $177.36
Employee + 2 or more: $37.00 $35.17 $422.04
Enhanced Dental Plan (with Medical Coverage)
Employee Only: $16.00 $9.16 $109.92
Employee + 1: $36.00 $14.37 $172.44
Employee + 2 or more: $48.00 $35.00 $420.00
Basic Dental Plan (without Medical Coverage)
Employee Only: $0.00 $21.87 $262.44
Employee + 1: $0.00 $43.78 $525.36
Employee + 2 or more: $0.00 $72.17 $866.04
Enhanced Dental Plan (without Medical Coverage)
Employee Only: $2.00 $23.16 $277.92
Employee + 1: $4.00 $46.37 $556.44
Employee + 2 or more: $7.00 $76.00 $912.00
Vision Plan
Employee Only: $8.60 $0.00 $0.00
Employee + Spouse: $15.50 $0.00 $0.00
Employee + Child(ren): $16.34 $0.00 $0.00
Employee + Family: $25.82 $0.00 $0.00
Voluntary GAP Plan (Monthly Employee Cost)
Under age 55 Ages 55-59 Ages 60+
Employee Only: $17.00 $24.00 $36.00
Employee + Spouse: $31.00 $43.00 $65.00
Employee + Child(ren): $28.00 $35.00 $47.00
Employee + Family: $42.00 $54.00 $76.00
Voluntary Life See Rate Chart on Page 7
Short & Long-Term Disability See Rate Chart on Page 8
Long Term Care See Rate Chart on Intranet

17
Important Information
This book highlights some of the main features of your benefit programs, but does not include all plan rules, features, limitations or exclusions. The terms of your benefit plans are governed by legal documents, including insurance contracts. Should there be any inconsistencies between this book and the legal plan documents, the plan documents are the final authority. AMERISAFE, Inc. reserves the right to change or discontinue its benefit plans at any time.
HIPAA Privacy Notice HIPAA requires AMERISAFE, Inc. to notify you that a privacy notice is available upon request. Please contact Human Resources if you have any questions.
Summary of Material Modification/Reduction This summary of material modification (SMM) describes changes to the AMERISAFE, Inc. plans and supplements the Summary Plan Description (SPD) for the plan. The effective date of each of these changes is January 1st, 2015. You should read this SMM very carefully and retain this document with your copy of the SPD for future reference.
The Women’s Health and Cancer Rights Act Do you know that your plan, as required by the Women’s Health and Cancer Rights Act of 1998, provides benefits for mastectomy-related services including all stages of reconstruction and surgery to achieve symmetry between the breasts, prostheses, and complications resulting froma mastectomy, including lymphedema? Contact the Human Resources Department for more information. If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending physician and the patient, for:
All stages of reconstruction of the breast on which the mastectomy was performed;
Surgery and reconstruction of the other breast to produce a symmetrical appearance;
Prostheses; and
Treatment of physical complications of the mastectomy, including lymphedema.
These benefits will be provided subject to the same deductibles and co-insurance applicable to other medical and surgical benefits provided under the AMERISAFE, Inc. Health Plan. Please see the Medical Benefit Plan for specific details.

18

19
Medicare D Notice
Important Notice from AMERISAFE, Inc. About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with AMERISAFE, Inc. and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage: 1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get
this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium.
2. AMERISAFE, Inc. has determined that the prescription drug coverage offered by the AMERISAFE, Inc.
Medical Plan is, on average for all plan participants, expected to pay out as much as standard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to December 7th. However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan. What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current AMERISAFE, Inc. coverage will not be affected. Your current coverage pays for other health expenses in addition to prescription drug. Please see the Medical Benefit Plan in this book for specific details about the prescription drug coverage. If you enroll in a Medicare prescription drug plan, you and your eligible dependents will be eligible to receive all of your current health and prescription drug benefits and your coverage will coordinate with Medicare. If you do decide to join a Medicare drug plan and drop your current AMERISAFE, Inc. coverage, be aware that you and your dependents may not be able to get this coverage back.
CMS Form 10182-CC Updated April 1, 2011
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid
OMB control number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this infor-
mation collection is estimated to average 8 hours per response initially, including the time to review instructions, search existing data re-
sources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the
time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer,
Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.

20
Medicare D Notice
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current coverage with AMERISAFE, Inc. and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join. For More Information About This Notice Or Your Current Prescription Drug Coverage… Contact the person listed below for further information. NOTE: You will get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through AMERISAFE, Inc. changes. You also may request a copy of this notice at any time. More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
• Visit www.medicare.gov • Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook for their telephone number) for personalized help
• Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048. If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Date: January 2016 Name of Entity/Sender: AMERISAFE, Inc. Contact--Position/Office: Benefits Department Address: 2301 Highway 190 West DeRidder, LA 70634 Phone Number: (337) 460-3675
CMS Form 10182-CC Updated April 1, 2011
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid
OMB control number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this infor-
mation collection is estimated to average 8 hours per response initially, including the time to review instructions, search existing data re-
sources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the
time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer,
Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you are required to pay a higher premium (a penalty).

21











![[XLS] · Web view11/1/2016 1/25/2016 1/22/2016 1/22/2016 1/21/2016 1/21/2016 1/21/2016 1/21/2016 1/21/2016 1/21/2016 1/21/2016 1/21/2016 1/20/2016 1/20/2016 1/19/2016 1/18/2016 1/18/2016](https://img.dokumen.tips/doc/110x75/5c8e2bb809d3f216698ba81b/xls-web-view1112016-1252016-1222016-1222016-1212016-1212016-1212016.jpg)


![[XLS]engineeringstudentsdata.comengineeringstudentsdata.com/downloads/2016/Telangana... · Web view2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016 2016](https://img.dokumen.tips/doc/110x75/5b19478b7f8b9a23258c8745/xlseng-web-view2016-2016-2016-2016-2016-2016-2016-2016-2016-2016-2016-2016.jpg)














![[XLS]bapasi.combapasi.com/wp-content/uploads/2018/01/Kalachuvadu.xlsx · Web view100 2016 425 2016 175 2016 350 2016 675 2016 450 2016 200 2016 90 2016 75 2016 375 2016 350 2016 750](https://img.dokumen.tips/doc/110x75/5b5391a37f8b9add3a8bf721/xls-web-view100-2016-425-2016-175-2016-350-2016-675-2016-450-2016-200-2016.jpg)