Embed Size (px)
Citation preview

2013 Lumbar Spine: Fusion Guidelines Effective 07-01-2013
MedSolutions, Inc. Clinical Decision Support Tool for Spinal Fusion
Common symptoms and symptom complexes are addressed by this tool. Requests for patients with atypical symptoms
or clinical presentations that are not specifically addressed will require physician review.
Consultation with the referring physician may provide additional insight.
MedSolutions, Inc. This tool addresses common symptoms and symptom complexes. Requests for patients with atypical Clinical Decision Support Tool symptoms or clinical presentations that are not specifically addressed will require physician review.
For Spinal Fusion Consultation with the referring physician, specialist and/or patient’s Primary Care Physician (PCP) may
provide additional insight.

2 RETURN
Lumbar Spine: Fusion Guidelines
2013 MedSolutions
2013 LUMBAR SPINE: FUSION GUIDELINES
LUMBAR SPINE: FUSION GUIDELINES PAGE
LSF-1 INTRODUCTION & GENERAL GUIDELINES 3
LSF-2 INSTABILITY 6
LSF-3 DEGENERATIVE DISORDERS 8
LSF-4 SPONDYLOLYSIS & SPONDYLOLISTHESIS 10
LSF-5 STENOSIS 12
LSF-6 PRIOR LUMBAR SPINE SURGERY 14
LSF-7 DEFORMITY 18
LSF-8 TRAUMA 20
LSF-9 NEOPLASTIC DISORDERS 22
LSF-10 INFECTION 23
LSF-11 APPENDIX - DEVICES 25
LSF-12 APPENDIX – ABBREVIATIONS 26
LSF-13 APPENDIX – GLOSSARY 27
LSF-14 APPENDIX – CPT® CODES 28
LSF-15 APPENDIX – SUPPORTING LITERATURE 29
LSF-16 APPENDIX – PROCEDURE DEFINTIONS 34

3 RETURN
LUMBAR SPINE: FUSION GUIDELINES
LSF-1: INTRODUCTION AND GENERAL GUIDELINES
LSF-1.1: Introduction
These guidelines address lumbar spine fusion (LSF) procedures and/or devices for
the adult patient population 18 years of age and older. Both spinal conditions and
procedural approaches and devices are described for their appropriateness and
coverage.
Accepted indications for lumbar spinal fusion procedures and/or devices based
primarily on appropriate supportive medical evidence will be addressed in
condition specific sections outlined below. Those procedures and/or devices
described as “not indicated” are based on a lack of a significant body of medical
evidence supporting their efficacy.
The indications for lumbar spinal fusion will be further examined in the following
condition-specific sections, which include:
Degenerative Disorders
Spondylolysis & Spondylolisthesis
Stenosis
Prior Lumbar Spine Surgery
Deformity
Trauma
Neoplastic Disease
Infection

4 RETURN
LSF-1.2: Tenets of Lumbar Spine Fusion Surgery: General Requirements
The table below represents the essential documentation of conditions and
evaluations that should be received prior to any considerations for all lumbar spine
fusion procedures (exceptions as noted). All subsequent guidelines and
indications in this document will reference these general requirements.
Continued next page . . .
Requirement Details
Diagnosis and rational for fusion NA
Non-operative care
Lifestyle modifications, weight loss, nicotine cessation,
medications, nonsteroidal anti-inflammatory medications,
physical therapy, medical exercise, bracing, spinal
manipulation, epidural steroid injections (when indicated),
behavioral therapy, etc.
Relative contraindications to
spine fusion, to be weighed
against the risks of not
performing surgery
Relative contraindications to spinal fusion include the
following:
Osteoporosis
Smoking
Malnutrition
Systemic infection
Anemia
Chronic hypoxemia
Severe cardiopulmonary disease
Severe depression, psychosocial issues, and secondary
gain issues
Recent history & examination in
the preceding 6 weeks
Detailed neurological exam relevant to fusion request
Bowel/bladder abnormalities
Motor deficits defined by location
Grading of manual muscle
testing in the preceding 6 weeks
0= No evidence of muscle function
1= Muscle contraction but no or very limited joint
motion (“trace”)
2=Complete range of motion with gravity eliminated
(“poor”)
3=Complete range of motion against gravity (“fair”)
4=Complete range of motion against gravity with some
resistance (“good”)
5=Complete range of motion against gravity with full or
normal resistance (“normal”)
5 RETURN
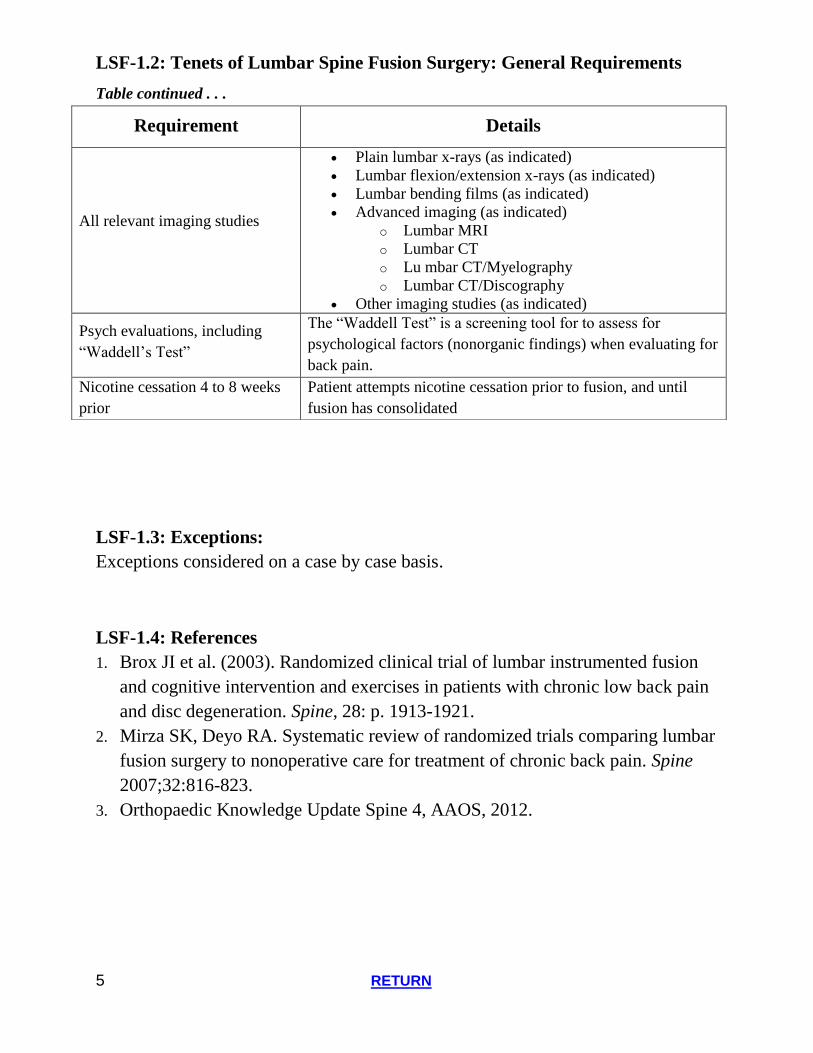
LSF-1.2: Tenets of Lumbar Spine Fusion Surgery: General Requirements
Table continued . . .
LSF-1.3: Exceptions:
Exceptions considered on a case by case basis.
LSF-1.4: References
1. Brox JI et al. (2003). Randomized clinical trial of lumbar instrumented fusion
and cognitive intervention and exercises in patients with chronic low back pain
and disc degeneration. Spine, 28: p. 1913-1921.
2. Mirza SK, Deyo RA. Systematic review of randomized trials comparing lumbar
fusion surgery to nonoperative care for treatment of chronic back pain. Spine
2007;32:816-823.
3. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Requirement Details
All relevant imaging studies
Plain lumbar x-rays (as indicated)
Lumbar flexion/extension x-rays (as indicated)
Lumbar bending films (as indicated)
Advanced imaging (as indicated)
o Lumbar MRI
o Lumbar CT
o Lu mbar CT/Myelography
o Lumbar CT/Discography
Other imaging studies (as indicated)
Psych evaluations, including
“Waddell’s Test”
The “Waddell Test” is a screening tool for to assess for
psychological factors (nonorganic findings) when evaluating for
back pain.
Nicotine cessation 4 to 8 weeks
prior
Patient attempts nicotine cessation prior to fusion, and until
fusion has consolidated

6 RETURN
LUMBAR SPINE: FUSION GUIDELINES
LSF-2: INSTABILITY
LSF-2.1: Background
The stable spine is recognized as having normal sagittal and coronal plane alignment without evidence of imbalance. For the stable spine, there is no evidence on imaging of abnormal segmental alignment such as intersegmental translation, angulation, or subluxation, either at rest or with motion. By contrast, there is no agreed upon definition for spine instability. Generally, instability refers to a loss of spinal integrity to withstand physiologic loads or stresses resulting in increased or abnormal motion between vertebral motion segments that result in pain, deformity and/or neurologic compromise, and/or significant angular and/or rotational and/or translational changes in the spine. Diagnostic checklists are often used to diagnose spinal instability including, White and Panjabi's classification, Holdsworth's two-column theory, and Denis’ three-column theory; however, documentation of these checklists is not required for consideration of fusion surgery.
Ultimately, instability may be the result of a variety of spine conditions and can result in pain, deformity and/or neurologic compromise. Despite lack of an agreed upon clinical definition, instability is generally accepted as the underlying primary indication for a lumbar spinal fusion procedure.
LSF-2.2: Indicated
Instability from angular and translational changes in the spine
Instability from spondylolisthesis as defined below under LSF-4
Instability from deformity as defined below under LSF-7
Instability from trauma as defined below under LSF-8
Instability from neoplastic disorders as defined below under LSF-9
Instability from infection as defined below under LSF-10
Instability resulting in neuroforaminal stenosis with neurologic compression
Instability created surgically:
o Unilateral facetectomy

7 RETURN
o Bilateral partial facetectomy of 50% or greater
o Pars resection or fracture
o Corpectomy and vertebrectomy
o Any other decompressive procedures known to cause instability
o Adjacent Segment Disease (ASD) associated with clinically symptomatic
spinal stenosis
LSF-2.3: Not Indicated
Initial routine laminectomy without instability
Initial routine hemilaminectomy, partial laminectomy, laminotomy or
foraminotomy without instability
Initial routine discectomy without instability, single or multiple levels
LSF-2.4: References
1. Posner I, White AA 3rd, Edwards WT, Hayes WC. A biomechanical analysis of
the clinical stability of the lumbar and lumbosacral spine. Spine 1982; 7:374–
389.
2. Leone A, Guglielmi G, et al. (2007). Lumbar Intervertebral Instability: A
Review. Radiology, 245:62-77.
3. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
4. Hu SS, Tribus CB, Tay BK, Bhatia NN. Chapter 5. Disorders, Diseases, &
Injuries of the Spine. In: Skinner HB, ed. CURRENT Diagnosis & Treatment in
Orthopedics. 4th Ed. New York: McGraw-Hill; 2006.
http://www.accessmedicine.com/content.aspx?aID=2319334. Accessed June
14, 2013.
5. Dixit RK. Chapter 10. Approach to the Patient with Low Back Pain. In:
Imboden JB, Hellmann DB, Stone JH, eds. CURRENT Rheumatology
Diagnosis & Treatment. 2nd Ed. New York: McGraw-Hill; 2007.
http://www.accessmedicine.com/content.aspx?aID=2724130. Accessed June
14, 2013.

8 RETURN
LUMBAR SPINE: FUSION GUIDELINES
LSF-3: DEGENERATIVE DISORDERS OF THE SPINE
LSF-3.1: Background
Disc degeneration is a term used to describe the natural changes that occur in the
spinal discs as a result of the aging process. These changes involve
disc desiccation as well as loss of disc height among other changes. Disc
degeneration is most commonly asymptomatic. In some cases degeneration of the
spinal elements can cause pain and be clinically relevant. These changes can cause
disorders of the disc and facet joints, as well as the spinal motion segments. Painful
degenerative clinical syndromes include lumbar spondylosis, facet syndrome and
Degenerative disc disease (also called internal disc derangement in discographic
positive patients). Degenerative disc disease is believed to occur in patients who
have variable degrees of degeneration of the disc in association with intervertebral
disc mediated pain. A concordantly painful discogram is believed by some
surgeons and clinicians to be the gold standard method of diagnosis.
LSF-3.2: Indicated
Lumbar spinal fusion surgery is indicated in the setting of Degenerative Disc
Disease (DDD) at a maximum of two identifiable motion segments or facet
syndrome joints levels, when all of the following conditions are met:
o LSF-1.2: General Requirements
o Significant degeneration is confined to two or less identifiable levels and is
reasonably expected to be the source of pain based on clinical evaluation and
advanced imaging (MRI or CT or discography)
o Has failed six consecutive months of physician guided non-operative care,
including exercise based/spine stabilization physical therapy and cognitive
behavioral therapy (if available in the community)
LSF-3.3: Not Indicated
3 or greater levels of spinal degeneration with diffuse, non-radicular pain
Chronic low back pain without a clear cause demonstrated by imaging or other
studies

9 RETURN
LSF-3.4: References
1. Fairbank J, Frost H (2005). Randomised controlled trial to compare surgical
stabilisation of the lumbar spine with an intensive rehabilitation programme for
patients with chronic low back pain: the MRC spine stabilisation trial. BMJ.
2005;330:1233.
2. Brox JI et al. (2003). Randomized clinical trial of lumbar instrumented fusion
and cognitive intervention and exercises in patients with chronic low back pain
and disc degeneration, Spine, 28: p. 1913-1921.
3. Nguyen TH, Randolph DC, Talmage J, Succop P, Travis R (2011). Long-term
Outcomes of Lumbar Fusion Among Workers’ Compensation Subjects: A
Historical Cohort Study. Spine, 36(4) 320-31.
4. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
5. Whang W, Erens G, Jarrett CD, Hoffler CE. Chapter 65. Common Orthopedic
Surgical Procedures. In: Lawry GV, McKean SC, Matloff J, Ross JJ, Dressler
DD, Brotman DJ, Ginsberg JS, eds. Principles and Practice of Hospital
Medicine. New York: McGraw-Hill; 2012.
http://www.accessmedicine.com/content.aspx?aID=56195770. Accessed June
14, 2013.

10 RETURN
LUMBAR SPINE: FUSION GUIDELINES
LSF-4: SPONDYLOLYSIS & SPONDYLOLISTHESIS
LSF-4.1: Background
Spondylolysis is a defect or fracture of part of the vertebral bones called the pars interarticularis. It usually occurs in the fifth and, less often, in the fourth lumbar vertebra. It is the most common cause of spondylisthesis in which one vertebral body is slipped forward over another.
There are also several subtypes of spondylolisthesis (isthmic, dysplastic, degenerative, traumatic, pathologic and iatrogenic) but in general the most common subtypes for which lumbar fusion is performed in adults are isthmic and degenerative.
LSF-4.2: Indicated
Single-level or multi-level spondylolysis and spondylolisthesis may be eligible for lumbar fusion when all of the following are met:
o LSF-1.2: General Requirements
o For adult patients, 6 months of non-operative care without improvement
Two level fusions may be covered, following the above criteria, for certain cases of high grade slips and/or sacral inclination where a one level fusion would not reasonably be expected to achieve a successful outcome
Degenerative spondylolisthesis with significant stenosis requiring a laminectomy is covered for lumbar fusion if all of the following criteria are met:
o LSF-1.2: General Requirements
o 3 months of non-operative care without improvement
LSF-4.3: References
1. Weinstein JN et al., (2007). Surgical versus Nonsurgical Treatment for Lumbar Degenerative Spondylolisthesis. New England Journal of Medicine, 356:2257–70.
2. Weinstein JN, Lurie JD, Tosteson TD, et al (2009). Surgical versus non-operative treatment for lumbar degenerative spondylolisthesis: four-year results

11 RETURN
of the Spine Patient Outcomes Research Trial (SPORT) randomized and
observational cohorts. J Bone Joint Surg Am, 91:1295–304.
3. NASS Clinical Practice Guidelines, Diagnosis and Treatment of Degenerative
Lumbar Spondylolisthesis
http://www.spine.org/Documents/Spondylolisthesis_Clinical_Guideline.pdf.
Accessed June 2011
4. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
5. Herman MJ, Pizzutillo PD, Cavalier R. Spondylolysis and spondylolisthesis in
the child and adolescent athlete. Orthop Clin North Am 2003, 34, 461-467.

12 RETURN
LUMBAR SPINE: FUSION GUIDELINES
LSF-5: STENOSIS LSF-5.1: Background
Spinal stenosis refers to the narrowing of the spinal canal and/or the neuroforamina. It can be asymptomatic or can impair nerve function resulting in radicular pain, neurogenic claudication, loss of sensation, altered reflexes, loss of motor control and rarely cauda equine syndrome.
Lumbar fusion is not generally necessary as an adjunct to decompressive procedures carried out for most cases of routine spinal stenosis with exceptions as outlined below.
LSF-5.2: Indicated
Established instability: see required criteria under LSF-2.2
Spondylolisthesis: see required criteria under LSF-4.2
Surgically created instability:
o Unilateral facetectomy
o Bilateral partial facetectomy of 50% or greater
o Pars resection or fracture
o Corpectomy and vertebrectomy
o Any other decompressive procedures known to cause instability
LSF-5.3: Not Indicated
Routine lumbar decompressive procedures that do not have pre-existing instability or do not cause expectation of iatrogenic instability as a result of the procedure itself.

13 RETURN
LSF-5.4: References
1. Amundsen T, et al. (2000). Lumbar spinal stenosis: conservative or surgical
management? A prospective 10-year study. Spine; 25(11):1424-1435.
2. Radcliff K, et al. (2011). Does the duration of symptoms in patients with spinal
stenosis and degenerative spondylolisthesis affect outcomes? Analysis of the
Spine Outcomes Research Trial. Spine, 36(25), 2197–2210.
3. Hurri H et al., (1998). Lumbar Spinal Stenosis: Assessment of Long-Term
Outcome 12 Years After Operative and Conservative Treatment. Journal of
Spinal Disorders, 11(2):110-115.
4. Chou et al., (2007). Diagnosis and treatment of low back pain: a joint clinical
practice guideline from the American College of Physicians and the American
Pain Society. Annals of Internal Medicine, 147 (7), 478-491.
5. NASS guidelines, 2011,
http://www.spine.org/Documents/NASSCG_Stenosis.pdf.
6. Resnick DK, et al., (2005). Guidelines for the performance of fusion procedures
for degenerative disease of the lumbar spine. Part 10: fusion following
decompression in patients with stenosis without spondylolisthesis J Neurosurg
Spine, 2(6):686-91.
7. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
8. Weinstein JN, Tosteson TD, Lurie JD, Tosteson A, Blood E, Herkowitz H,
Cammisa F, Albert T, Boden SD, Hilibrand A, Goldberg H, Berven S, An H
(2010). Surgical Versus Nonoperative Treatment for Lumbar Spinal Stenosis
Four-Year Results of the Spine Patient Outcomes Research Trial. Spine,
35(14)1329–1338.
9. Yone K, Sakou T (1999). Usefulness of Posner's definition of spinal instability
for selection of surgical treatment for lumbar spinal stenosis. J Spinal Disord,
12:40–44.

14 RETURN
LSF-6: PRIOR LUMBAR SPINE SURGERY
LSF-6.1: Background
Prior lumbar spine surgery includes such procedures as discectomy, laminectomy, partial laminectomy, laminotomy, foraminotomy, percutaneous or minimally invasive procedures and various types of spinal fusion procedures (anterior, posterior, lateral combined 360 degree fusions, etc.) with or without internal fixation and/or interbody devices. Under certain circumstances, revision or additional surgery may be indicated and a lumbar spinal fusion procedure may be considered as outlined below.
LSF-6.2: Indicated
LSF-6.21: Instrumentation Removal
Instrumentation (internal fixation device) removal may be considered for the following indications:
o Painful instrumentation e.g. insufficient soft tissue coverage
o This does not occur often. Diagnostic intervention should be used to determine if instrumentation is the cause of pain.
o Instrumentation that poses a risk to a patient, e.g. loose or malpositioned devices that pose a threat to the anterior great vessels or neurological structures
o Instrumentation removal or reimplantation as part of a subsequent surgery
LSF-6.22: Pseudarthrosis
Pseudarthrosis is the failure of bone graft to consolidate or fuse solidly to the spine, i.e. non-union. Revision fusion of the same level may be considered if all of the following criteria are met:
o LSF-1.2: General Requirements
o It has been at least 12 months from the prior fusion procedure OR identified failure of implant instrumentation has occurred at any time (e.g. broken rod )
o 3 months of non-operative care without improvement
o If 3 months of non-operative care occur less than 12 months after the first procedure, the patient must still wait the full 12

15 RETURN
months before being considered for follow-up surgery
o Except when failure of identified implant instrumentation
o Low back pain improvement for at least 3 months following the prior surgery
o Imaging studies confirm a pseudarthrosis (x-rays and/or CT) or presence of failed instrumentation demonstrated on plain x-ray and/or CT
LSF-6.23: Adjacent Segment Disease
Other terms for Adjacent Segment Disease (ASD) include Adjacent Level Disease and Transitional Syndrome. Adjacent Segment Disease is defined as the degenerative changes that take place over time above and/or below a spinal fusion as a result of transferred stress. An additional fusion procedure directed at the involved single level may be considered if all of the following criteria are met:
o LSF-1.2: General Requirements
o It has been greater than 12 months from the prior fusion procedure and the prior fusion procedure was successful (solid fusion with significantly decreased pain and increased function)
o 6 months of ongoing non-operative care without improvement
o If 6 months of ongoing non-operative care occur less than 12 months after the first procedure, the patient must still wait the full 12 months before being considered for follow-up surgery
o Significant degeneration is confined to one identifiable level and is reasonably expected to be the source of pain based on clinical evaluation and advanced imaging (MRI or CT or discography)
LSF-6.24: Recurrent Herniated Disc
The surgical treatment for most cases of recurrent herniated discs (involving neurological compression) does not require adjunctive spinal fusion. However, an adjunctive fusion procedure directed at the involved single level may be considered if all of the following criteria are met:
o LSF-1.2: General Requirements
o The patient has had prior discectomy at the same level

16 RETURN
o It has been greater than 3 months from the prior procedure and the
prior procedure was initially successful for radicular pain relief
o Recurrent symptoms and pathology with neurological compression
confined to one identifiable level which is reasonably expected to be
the source of pain based on clinical evaluation and advanced imaging
(MRI or CT or myelography)
o The patient has new pain or neurological symptoms consistent with
the level of recurrence.
o There is associated foraminal stenosis, concomitant segmental
instability, or spondylolisthesis or resultant instability from the
procedure itself
o 3 months of non-operative care without improvement
LSF-6.3: Not Indicated
Prior lumbar laminectomy without instability, or where the currently proposed
surgery would not be expected to result in instability
Prior hemilaminectomy, partial laminectomy, laminotomy or foramintomy
without instability, or where the currently proposed surgery would not be
expected to result in instability
Prior routine discectomy without instability or where the currently proposed
surgery would not be expected to result in instability, single or multiple levels
Routine instrumentation removal without cause
LSF-6.4: References
1. Lee C, Dorcil J, Radomisli TE (2004). Nonunion of the Spine: A Review. Clin
Orthop, 419: 71-75.Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
2. Hu SS, Tribus CB, Tay BK, Bhatia NN. Chapter 5. Disorders, Diseases, &
Injuries of the Spine. In: Skinner HB, ed. CURRENT Diagnosis & Treatment in
Orthopedics. 4th ed. New York: McGraw-Hill; 2006.
3. http://www.accessmedicine.com/content.aspx?aID=2319334. Accessed May 9,
2013.
4. Resnick DK, Choudri TF, Dailey AT, Groff MW, et al. Guidelines for the
performance of fusion procedures for degenerative disease of the lumbar spine.
Part 8: lumbar fusion for disc herniation and radiculopathy. J Neursurg: Spine

17 RETURN
2, 2005, 673-678.
5. Lee JK, Amorosa L, Cho SK, Weidenbaum M, Kim Y. Recurrent lumbar disk
herniation. J Am Acad Orthop Surg 2010, 18(6), 327-337
6. International Society for the Advancement of Spine Surgery (ISASS). Policy
Statement on Lumbar Spinal Fusion Surgery.
http://www.isass.org/public_policy/2011-07-
15_policy_statement_lumbar_surgery.pdf, accessed June 18, 2013.

18 RETURN
LSF-7: DEFORMITY
LSF-7.1: Background
This particular section refers to spinal deformities that result from scoliosis and kyphosis, not deformities that are caused by one or two motion segments that have become unstable.
Scoliosis is a lateral (sideways) spinal curvature in the frontal plane. Kyphosis is a forward curvature (rounding or ‘humpback’) of the spine in the sagittal plane. Progressive deformities are documented with sequential radiographs.
Pain associated with scoliosis will be due to facet/ disc degenerative changes from asymmetric forces on the deformed segment of the spine or from compression or stretching of neural elements and/or other soft tissue structures.
The goal and primary indication of arthrodesis in these types of spinal deformities is to stop progression of the deformity. Conditions in which deformity progression may occur include the following:
Progression of idiopathic scoliosis
Degenerative scoliosis in association with neurological compromise (spinal stenosis-central, lateral recess, or foraminal in association with scoliosis)
Acquired progressive spinal deformity in the face of a neurologic deficit or disease (e.g. traumatic neurological deficit, neuromuscular scoliosis) with or without progression of neurological or functional deficit:
Iatrogenic flat back syndrome, acquired loss of lumbar lordosis, and loss of sagittal plane balance secondary to a pre-existing spinal fusion where initial balance was not achieved or maintained over time.
LSF-7.2: Indicated
Instrumented arthrodesis: anterior, posterior or combined
LSF-7.3: Not Indicated
As indicated under LSF-11 and LSF-12 below

19 RETURN
LSF-7.4: References
1. Oskouia RJ, Shaffrey CI (2006). Degenerative Lumbar Scoliosis. Neurosurg
Clin North America 2006;17(3):299-315.
2. Ploumis A, Transfledt, Denis F (2007). Degenerative lumbar scoliosis
associated with spinal stenosis. Spine, 7(4):428-36.
3. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
4. Bridwell K P (2012). What's New in Spine Surgery. Journal of Bone and Joint
Surgery , 1140-1148.
5. Kalantar SB, Laurman WC (2012). Adult Scoliosis: Etiology and Management.
Orthopaedic Knowledge Online Journal .
6. Deviren V, Metz LN. Anterior instrumented arthrodesis for adult idiopathic
scoliosis (2007). Neurosurg Clin N Am, 18(2):273-80.
7. Gelalis ID, Kang JD (1998). Thoracic and lumbar fusions for degenerative
disorders: rationale for selecting the appropriate fusion techniques. Orthop Clin
North Am, 29(4):829-42.
8. Gupta M (2003). Degenerative scoliosis: options for surgical management.
Orthop Clin North Am, 34(2):269-79.
9. Kim et al. Scoliosis Imaging: What Radiologists Should Know.
RadioGraphics, 2010, 30, 1823-1842.

20 RETURN
LSF-8: TRAUMA
LSF-8.1: Background
Disruption of the bony and/or ligamentous structures of the spine may lead to
instability, either acute or chronic. Neurological compromise may necessitate
decompression of neural elements which may cause additional potential for
instability. This often requires reduction and arthrodesis to restore stability and
spinal balance. The most common fracture patterns are at the level of the
thoracolumbar junction: acute compression fractures, burst fractures, fractures of
the posterior elements, and Chance fractures. These fractures also occur below L2.
LSF-8.2: Indicated
Three spinal column injuries Burst fractures (burst fractures by definition
involve two of the three spinal columns)
Compression fractures with severe posterior ligamentous disruption and/or
kyphotic deformity with likelihood of chronic instability with further
segmental angulation
Chance fractures with primarily soft tissue disruption and/or significant
angular deformity with potential for further chronic progression of deformity
In conjunction with neurologic decompression when iatrogenic instability is
necessary
Techniques include:
Fracture reduction and/or instrumented arthrodesis: posterior, anterior or
combined
Decompression (as indicated) combined with arthrodesis but not as an
isolated procedure
PMMA (polymethylmethacrylate)supplementation for pedicle screws in
osteopenic bone
LSF-8.3: Not Indicated
Dynamic Spine Stabilization Devices (e.g., Dynesys® , Stabilimax NZ®)
Interlaminar/ Interspinous Internal Fixation Devices (e.g., ILIF™)
Axial Lumbar Interbody Fusion (AxiaLIF)

21 RETURN
Dynamic Spine Stabilization Device Systems (e.g., Dynesys®, Stabilimax
NZ®)
LSF-8.4: References
1. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
2. Bridwell K P (2012). What's New in Spine Surgery. Journal of Bone and Joint
Surgery , 1140-1148.
3. Kalantar SB, Laurman WC (2012). Adult Scoliosis: Etiology and Management.
Orthopaedic Knowledge Online Journal .
4. Bambakidis NC, Feiz-Erfan I, Klopfenstein JD, Sonntag VK. Indications for
surgical fusion of the cervical and lumbar motion segment. Spine 2005, 30(16
suppl), S2-6.
5. Sasagawa T, Kawahara N, Murakami H, Demura S, Tomita K. Decompression,
correction, and interbody fusion for lumbar burst fractures using a single
posterior approach. Orthopedics 2009, 32(10).

22 RETURN
LSF-9: NEOPLASTIC DISORDERS
LSF-9.1: Background
Neoplastic disorders frequently involve the spine and usually are metastatic, although primary bone tumors can also affect the spine.
Tumors of the spinal column may destroy vertebrae and associated bony structures or result in epidural compression and/or spinal instability. When surgery is indicated, the procedure may result in instability requiring stabilization and fusion. This may be known prior to surgical intervention (based on structures destroyed by the tumor) or determined intraoperatively.
LSF-9.2: Indicated
Established instability
o See LSF-2 above
o Spondylolisthesis
o Certain cases with associated spinal deformity: see LSF-7 above
o Certain cases with associated fracture: see LSF-8
Surgically created instability:
o Unilateral facetectomy
o Bilateral partial facetectomy of 50% or greater
o Pars resection or fracture
o Corpectomy and vertebrectomy
o Any other decompression procedures known to cause instability
LSF-9.3: Not Indicated
See LSF 2.3 above
LSF-9.4: References
1. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.

23 RETURN
LSF-10: INFECTION
LSF-10.1: Background
Infections involving the spine such as discitis and/or osteomyelitis may be bacterial or fungal in origin and primary or secondary. They may be a result of invasive procedures (e.g. epidural steroid injections) or prior surgery. Surgery is considered when medical management dictates tissue culture for diagnosis and/or drainage of associated abscess loss of structural integrity of the spine, progressive deformity, and/or neurologic compression.
LSF-10.2: Indicated
Established instability
o See LSF-2 above
o Spondylolisthesis
o Certain cases with associated spinal deformity: see LSF-7 above
o Certain cases with associated fracture: see LSF-8
Surgically created instability:
o Unilateral facetectomy
o Bilateral partial facetectomy of 50% or greater
o Pars resection or fracture
o Corpectomy and vertebrectomy
o Any other decompressive procedures known to cause instability
LSF-10.3: Not Indicated
Initial routine laminectomy without instability
Initial routine hemilaminectomy, partial laminectomy, laminotomy or foraminotomy without instability
Initial routine discectomy without instability, single or multiple levels

24 RETURN
LSF-10.4: References
1. Dietz DD, Fessler RG, Jacob PR (1997). Primary reconstruction for spinal
infections. J Neurosurg, 86:981-989.
2. Arnold PM, Baek PN, Bernardi RJ, et al (1997). Surgical management of
nontuberculous thoracic and lumbar vertebral osteomyelitis: report of 33 cases.
Surg Neurol , 47:551-561.
3. Kim CW, Perry A, Currier B, Yaszemski M, Garfin SR (2006). Fungal
Infections of the Spine. Clinical Orthopaedics & Related Research, 444:92-99.
4. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.

25 RETURN
LSF-11: APPENDIX - DEVICES
LSF-11.1: Background
A broad variety of internal fixation devices and interbody devices exists that is
beyond the scope of these guidelines. However, some of the general and specific
fusion devices that are covered and non-covered are mentioned below.
LSF-11.2: Indicated
LSF-11.21: Standard Pedicle Screw Rod/Plate Internal Fixation Devices
LSF-11.22: Standard Interbody Fusion Devices
LSF-11.3: Not Indicated
LSF-11.31: Dynamic Spine Stabilization Devices
(e.g., Dynesys® , Stabilimax NZ®)
LSF-11.32: Interlaminar/ Interspinous Internal Fixation Devices
(e.g., ILIF™)
LSF-11.33: Axial Lumbar Interbody Fusion (AxiaLIF)
LSF-11.34: Dynamic Spine Stabilization Device Systems (e.g., Dynesys®,
Stabilimax NZ®)
LSF-11.4: References
1. Orthopaedic Knowledge Update Spine 4, AAOS, 2012.

26 RETURN
LSF-12: APPENDIX - ABBREVIATIONS
AAOS American Academy of Orthopaedic Surgeons
ACP American College of Physicians
ALIF Anterior lumbar interbody fusion
ASF Anterior spinal fusion
APS American Pain Society
AANS American Association of Neurological Surgeons
CNS Congress of Neurological Surgeons
DDD Degenerative disc disease
HWR Instrumentation removal
IF Internal fixation
LADR Lumbar Artificial Disc Replacement
NASS North American Spine Society
PLIF Posterior lumbar interbody fusion
PSF Posterior or posterolateral fusion
TLIF Transforaminal lumbar interbody fusion

27 RETURN
LSF-13: APPENDIX - GLOSSARY
Adjacent Segment
Disease Degenerative changes that take place over time above and/or below a spinal
fusion as a result of transferred stress and/or natural progression of spinal
degeneration, also called “Transition Syndrome” or “Adjacent Level Disease.”
Advance Imaging MRI, CT, CT/myelography, CT/discography, PET scans, etc.
Arthrodesis Bony fusion of a motion segment. In the spine, this means fusion of a vertebral
motion segment which is two adjacent vertebrae and the associated
intervertebral disc and facet joints. This may be accomplished by fusing one
vertebral body to another and/or fusion of the facet joints and/or fusion of one
transverse processes to another, as in a posterolateral fusion.
Arthroplasty Joint repair or replacement
Non-Operative Care Non-surgical treatment that may include activity modifications, weight loss,
nicotine cessation, medications, physical therapy, medical exercise, bracing,
spinal manipulation, injections, behavioral therapy, etc.
Degenerative Disc
Disease (DDD) Degenerative disc disease refers to the degenerative changes that take place in a
disc over time or as a result of trauma or altered stresses on the spine such as a
transition syndrome.
Instability Instability refers to a loss of spinal integrity to withstand physiologic loads or
stresses resulting in increased or abnormal motion between vertebral motion
segments that result in pain, deformity and/or neurologic compromise, and/or
significant angular and/or rotational and/or translational changes in the spine.
Kyphosis Convex posterior curvature in the sagittal plane
Pseudarthrosis Failure of bone graft to consolidate or fuse solidly between two vertebrae in the
spine (non-union)
Spinal Stenosis Narrowing of the spinal canal and/or neuroforamina
Spondylolysis A defect of the pars intraarticularis
Spondylolisthesis Translation of one vertebral body relative to the vertebral body below
(anterolisthesis=anterior translation; retrolisthesis=posterior translation)
Scoliosis Lateral curvature in the coronal plain greater than 10 degrees
Transition
Syndrome
Degenerative changes that take place over time above and/or below a spinal
fusion as a result of transferred stress and/or natural progression of spinal
degeneration, also called “Adjacent Level Disease” or “Adjacent Segment
Disease.”

28 RETURN
LSF-14: APPENDIX – CPT® CODES
CPT® (Current Procedural Terminology) is a registered trademark of the American Medical Association (AMA). CPT® five digit codes, nomenclature and other data are copyright 2013 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values or related listings are included in the CPT® book. AMA does not directly or indirectly practice medicine or dispense medical services. AMA assumes no liability for the data contained herein or not contained herein.
Code Procedure22533 Arthrodesis, lateral extracavitary technique, including minimal discectomy to
prepare interspace (other than for decompression); thoracic.
22534 Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic or lumbar, each additional vertebral segment.
22558 Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar.
22585 Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); each additional interspace.
22612 Arthrodesis, posterior or posterolateral technique, single level; lumbar (with or without lateral transverse technique).
22614 Arthrodesis, posterior or posterolateral technique, single level; each additional vertebral segment.
22630 Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar.
22632 Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; each additional interspace.
0195T Arthrodesis, pre-sacral interbody technique, including instrumentation, imaging (when performed), and discectomy to prepare interspace, lumbar; single interspace
0196T Arthrodesis, each additional interspace (List separately in addition to code for primary procedure)
22633 Arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than decompression), single interspace and segment; lumbar.
22634 Each additional interspace and segment (List separately in addition to code for primary procedure)

29 RETURN
LSF-15: APPENDIX – SUPPORTING LITERATURE
LSF-1: INTRODUCTION & GENERAL GUIDELINES
Mirza SK, Deyo RA (2007). Systematic review of randomized trials comparing lumbar fusion surgery to nonoperative care for treatment of chronic back pain. Spine, 32:816-823.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
LSF-2: INSTABILITY
Hu SS, Tribus CB, Tay BK, Bhatia NN. Chapter 5. Disorders, Diseases, & Injuries of the Spine. In: Skinner HB, ed. CURRENT Diagnosis & Treatment in Orthopedics. 4th ed. New York: McGraw-Hill; 2006. http://www.accessmedicine.com/content.aspx?aID=2319334. Accessed June 14, 2013.
Dixit RK. Chapter 10. Approach to the Patient with Low Back Pain. In: Imboden JB, Hellmann DB, Stone JH, eds. CURRENT Rheumatology Diagnosis & Treatment. 2nd ed. New York: McGraw-Hill; 2007. http://www.accessmedicine.com/content.aspx?aID=2724130. Accessed June 14, 2013.
Leone A, Guglielmi G, Victor N, Cassar-Pullicino VN, and Bonomo L (2007). Lumbar Intervertebral Instability: A Review. Radiology, 245:62-77.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Posner I, White AA 3rd, Edwards WT, Hayes WC (1982). A biomechanical analysis of the clinical stability of the lumbar and lumbosacral spine. Spine,7:374–389.
LSF-3: DEGENERATIVE DISC DISEASE
Brox, J, et al. (2003). Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine, 28: p. 1913-1921.
Fairbank J et al. (2005). Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: the MRC spine stabilisation trial. BMJ, 330:1233.

30 RETURN
Nguyen TH, Randolph DC, Talmage J, Succop P, Travis R. (2011). Long-term Outcomes of Lumbar Fusion Among Workers’ Compensation Subjects: A Historical Cohort Study. Spine, 36(4) 320-31.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Whang W, Erens G, Jarrett CD, Hoffler CE. Chapter 65. Common Orthopedic Surgical Procedures. In: Lawry GV, McKean SC, Matloff J, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS, eds. Principles and Practice of Hospital Medicine. New York: McGraw-Hill; 2012. http://www.accessmedicine.com/content.aspx?aID=56195770. Accessed June 14, 2013.
LSF-4: SPONDYLOLYSIS & SPONDYLOLISTHESIS
NASS Clinical Practice Guidelines, Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis http://www.spine.org/Documents/Spondylolisthesis_Clinical_Guideline.pdf.Accessed June 2011
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Weinstein JN, Lurie JD, Tosteson TD, et al. (2007). Surgical versus nonsurgical treatment for lumbar degenerative spondylolisthesis. N Engl J Med, 356:2257-70.
Weinstein JN, Lurie JD, Tosteson TD, et al. (2009). Surgical versus non-operative treatment for lumbar degenerative spondylolisthesis: four-year results of the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am, 91:1295–304.
Herman MJ, Pizzutillo PD, Cavalier R. Spondylolysis and spondylolisthesis in the child and adolescent athlete. Orthop Clin North Am 2003, 34, 461-467.
LSF-5: STENOSIS
Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleas F (2000).Lumbar spinal stenosis: conservative or surgical management: a prospective 10-year study. Spine, 25(11):1424-1435.
Chou et al (2007). Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the

31 RETURN
American Pain Society. Annals of Internal Medicine , 147(7): 478-491.
Hurri H, Slatis P, Soini J, et al. (1998). Lumbar spinal stenosis: assessment of long-term outcome 12 years after operative and conservative treatment. JSpinal Disord, 11(2):110-115.
NASS Clinical Practice Guidelines .Diagnosis and treatment of degenerative lumbar spinal stenosis. 2007 Jun http://www.spine.org/Documents/NASSCG_Stenosis.pdf. Accessed June 2011
Resnick DK et al. (2005). American Association of Neurological Surgeons/Congress of Neurological Surgeons. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: fusion following decompression in patients with stenosis without spondylolisthesis. J Neurosurg Spine, 2(6):686-91.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Weinstein JN et al. (2010). Surgical Versus Nonoperative Treatment for Lumbar Spinal Stenosis Four-Year Results of the Spine Patient Outcomes Research Trial. Spine, 35(14)1329–1338.
Yone K, Sakou T. (1999). Usefulness of Posner's definition of spinal instability for selection of surgical treatment for lumbar spinal stenosis. J Spinal Disord, 12:40–44.
LSF-6: PRIOR LUMBAR SPINE SURGERY
Hu SS, Tribus CB, Tay BK, Bhatia NN. Chapter 5. Disorders, Diseases, & Injuries of the Spine. In: Skinner HB, ed. CURRENT Diagnosis & Treatment in Orthopedics. 4th ed. New York: McGraw-Hill; 2006. http://www.accessmedicine.com/content.aspx?aID=2319334. Accessed May 9, 2013.
Lee C, Dorcil J, Radomisli TE (2004). Nonunion of the Spine: A Review. Clin Orthop, 419: 71-75.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Resnick DK, Choudri TF, Dailey AT, Groff MW, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar
32 RETURN
spine. Part 8: lumbar fusion for disc herniation and radiculopathy. JNeursurg: Spine 2, 2005, 673-678.
Lee JK, Amorosa L, Cho SK, Weidenbaum M, Kim Y. Recurrent lumbar disk herniation. J Am Acad Orthop Surg 2010, 18(6), 327-337
International Society for the Advancement of Spine Surgery (ISASS). PolicyStatement on Lumbar Spinal Fusion Surgery.http://www.isass.org/public_policy/2011-07-15_policy_statement_lumbar_surgery.pdf, accessed June 18, 2013.
LSF-7: DEFORMITY
Bridwell K P (2012). What's New in Spine Surgery. Journal of Bone and Joint Surgery , 1140-1148.
Deviren V, Metz LN (2007). Anterior instrumented arthrodesis for adult idiopathic scoliosis. Neurosurg Clin N Am ,18(2):273-80.
Gelalis ID, Kang JD (1998). Thoracic and lumbar fusions for degenerative disorders: rationale for selecting the appropriate fusion techniques. OrthopClin North Am, 29(4):829-42.
Gupta M (2003). Degenerative scoliosis: options for surgical management. OrthopClin North Am, 34(2):269-79.
Kalantar SB, Laurman WC (2012). Adult Scoliosis: Etiology and Management. Orthopaedic Knowledge Online Journal .
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Oskouian RJ, Shaffrey CI (2006). Degenerative lumbar scoliosis. NeurosurgeryClinics of North America,17(3):299-315, vii.
Ploumis A, Transfledt EE, Denis F (2007). Degenerative lumbar scoliosis associated with spinal stenosis. Spine Journal, 2007;7(4):428-36.
Kim et al. Scoliosis Imaging: What Radiologists Should Know. RadioGraphics,2010, 30, 1823-1842.
LSF-8: TRAUMA
Bridwell K P (2012). What's New in Spine Surgery. Journal of Bone and Joint Surgery, 1140-1148.

33 RETURN
Kalantar SB, Laurman WC (2012). Adult Scoliosis: Etiology and Management. Orthopaedic Knowledge Online Journal .
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
Bambakidis NC, Feiz-Erfan I, Klopfenstein JD, Sonntag VK. Indications for surgical fusion of the cervical and lumbar motion segment. Spine 2005, 30(16 suppl), S2-6.
Sasagawa T, Kawahara N, Murakami H, Demura S, Tomita K. Decompression, correction, and interbody fusion for lumbar burst fractures using a single posterior approach. Orthopedics 2009, 32(10).
LSF-9: NEOPLASTIC DISEASE
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
LSF-10: INFECTION
Arnold PM, Baek PN, Bernardi RJ, et al. (1997). Surgical management of nontuberculous thoracic and lumbar vertebral osteomyelitis: report of 33 cases. Surg Neurol, 47:551-561.
Dietze DD Jr, Fessler RG, Jacob RP (1997). Primary reconstruction for spinal infections. J Neurosurg, 86:981-989.
Kim CW, Perry A, Currier B, Yaszemski M, Garfin SR (2006). Fungal Infections of the Spine. Clinical Orthopaedics & Related Research , 444:92-99.
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.
LSF-11: DEVICES
Orthopaedic Knowledge Update Spine 4, AAOS, 2012.

34 RETURN
LSF-16: APPENDIX – PROCEDURE DEFINTIONS
LSF 12.5: Appendix - Procedure Definitions
This section provides terminology and context for procedures that are often used in lumbar spinal fusion surgery. This is intended for informational purposes only, and should not be used when adjudicating spine fusion surgery requests.
A number of procedures have been devised, with and without internal fixation devices and/or interbody devices, to accomplish the goal of a solid arthrodesis.
A bone graft and/or bone graft substitute is the material that forms a bridge between vertebral segments, which facilitates the fusion of spinal segments. Bone graft types are generally categorized as autograft (harvested from the patient), allograft (harvested from a human cadaver) or synthetic (artificial, manufactured). They are further subcategorized as structural and non-structural. Autograft is generally recognized as the gold standard for spinal fusions because it possesses the key elements of fusion biology, including osteoconductivity, osteoinductivity and osteogenicity. Some of the shortcomings of autograft (such as availability and donor site morbidity) are addressed by the use of allografts and synthetic grafts.
Biological bone graft adjuvants such as rhBMP (e.g. INFUSE ® Bone Graft) can also serve as fusion adjuncts. However, recent data analysis has revealed that rhBMP-2 provides little benefit to patients compared to other graft procedures, and that there was in increased risk of at 24 months post procedure (although the overall cancer risk was low).
Basic Lumbar Procedures Anterior Spinal Fusion (ASF) Anterior Lumbar Interbody Fusion (ALIF) Posterior or Posterolateral Spine Fusion (PSF) Transforaminal Lumbar Interbody Fusion (TLIF) Lateral Interbody Fusion Direct Lateral Interbody Fusion (DLIF) Extreme Lateral Interbody Fusion (XLIF) Combined, Anterior/Posterior Fusion (also called a 360oFusion)Interlaminar/ Interspinous Lumbar Instrumented Fusion (e.g., ILIF™) Isolated Facet Fusions: Includes allograft bone graft substitutes used exclusively as stand-alone stabilization devices (e.g., TruFuse®, NuFix™)

35 RETURN
Additional Bone Graft Terms Cell-based substitutes (e.g., mesenchymal stem cell therapy) Human growth factors (e.g., fibroblast growth factor, insulin-like growth factor) Platelet rich plasma (e.g., autologous platelet derived growth factor)Allograft bone graft substitutes (e.g., TruFuse® for isolated facet fusion, NuFix™ for isolated facet fusion, BacFast® HD for isolated facet fusion) Bone graft substitutes used to reduce donor site morbidity (e.g., iliac crest donor site reconstruction)





























