Embed Size (px)
Citation preview

2012 Updates: SCPC Troponin
Turn-Around-Time Documentation Requirements
and CMS OP-16
1

Speaker Overview
Ruth Cantu, BSN, RN Accreditation Review Specialist
There are no disclosures
2

Objectives
3
Discuss turn-around-time (TAT) implications in healthcare studies, research and guidelines
Discuss the Society of Chest Pain Centers (SCPC) Troponin Turn-around-Time (TTAT) documentation
requirements for accreditation
Provide an update of the Centers for Medicare and Medicaid Services (CMS) Hospital Outpatient Quality Data
Reporting Program: OP-16
Discuss best demonstrated practices for improvement in process outcomes
Society of Chest Pain Centers
Patient-centric
Founded in science
Validated by accreditation and certification
The leader in establishing criteria helping hospitals develop superior processes that embrace
the full spectrum of cardiac care by providing tools, education and support to drive process improvement in
healthcare facilities worldwide.
We create communities of excellence that share understanding on quality, cost and patient satisfaction.
4

Benefits of SCPC Accreditation
Streamlines and standardizes intra/inter-facility processes from identification of symptoms to definitive care
Requires defined pathways to reduce missed MIs through a consistent approach to risk stratification of the ACS patient
Promotes evidence-based processes that result in improved quality outcomes and improves performance on quality indicators
Requires everyone who touches the cardiac patient to come together; breaking down silos that exist between disciplines and departments
5

Society of Chest Pain Centers
Cardiac Biomarkers &
Troponin Turn-Around-Time
6

Changing Perspectives of Turn-Around-Time Tracking and Healthcare Implications
Recent studies and research support the movement towards the following:
Assessing the “whole process” (ie: arrival)
Standardizing definitions of TAT
Assessing TAT with patient outcomes and length of stay
7

Changing Perspectives of Turn-Around-Time Tracking and Healthcare Implications
Study by Ervasti et al, Clin Chem Lab Med 2008
Proposed new concepts for TAT in the diagnostic process: As a “Patient-oriented” view or the “whole process”
Diagnostic TAT – arrival to reporting of results (outcomes median 122 min)
Clinical TAT – arrival to order Laboratory TAT – order to report/resulted
In Academic Emergency Medicine, 2010:17, Hwang et al noted: “Guidelines do not exist delineating times frames for when a troponin test should
optimally be resulted in association with improved patient outcomes.”
“ Prolonged laboratory TAT may delay recognition of conditions in the acutely ill , potentially affecting clinician decision-making and the initiation of timely treatment.” Outcomes median 107 minutes; “ordered to resulted”
8

SCPC Cardiac Biomarker Requirements
Measuring TAT is a guideline driven recommendation
No previous TAT requirement SCPC requirement starting in 2012
Track and demonstrate improvements
9

Troponin Measurement
10
0.8% Tn / MYO
39.3% Tn / CKMB
23.0% Tn/ CKMB / MYO
14.5% Diff combo
22.2% Tn only
Which do you measure in your lab/hospital today?
Troponin (Tn) and MyoglobinTroponin and CK-MBTroponin, CK-MB and MyoglobinA different combination of markersTroponin only
CLN – April 2009, vol 35, no 4
Troponin TAT only
Gold standard
Standardization

11
The facility has a process for reviewing and assessing baseline troponin quality metrics for ED patients. These metrics are tracked and shared between the ED and laboratory at appropriate committee meetings at least quarterly. At least six months of metrics are required AND at least two of the following green Tier III and/or pink Tier IV Items:
4.4.0.0
Yes No Item Baseline troponin “turnaround time" (TAT) is broken down into the
time segment of ORDER to COLLECT. 4.4.1.0
Baseline troponin TAT is broken down into the time segment of COLLECT to RECEIVE IN LAB.
4.4.2.0
Baseline troponin TAT is broken down into the time segment of RECEIVE IN LAB to RESULT.
4.4.3.0
Baseline troponin TAT is broken down into the time segment of DOOR to RESULT.
4.4.4.0
Baseline troponin TAT is broken down into the time segment of DOOR to ORDER.
4.4.5.0
Baseline troponin TAT is broken down into the time segment of ORDER to RESULT.
4.4.6.0
Baseline troponin TAT is broken down into the time segment of COLLECT to RESULT.
4.4.7.0
90% of baseline troponin TAT of ORDER TO RESULT or COLLECT to RESULT is within 60 minutes.
4.4.8.0
Yes No Item 90% of baseline troponin TAT of ORDER to
RESULTS or COLLECT to RESULT is within 30 minutes.
4.4.9.1
Item The facility's cardiac biomarker approach includes documentation of an evidenced-based serial troponin strategy that is consistent with the assay used AND at least one of the following green Tier III Items:
4.5.0.0
Yes No Item The facility has a process in place to monitor the TAT of serial
draws for troponin. 4.5.1.0
The cardiac biomarker protocol includes a serial troponin from ED arrival up to 6 hours. The protocol may last less than 6 hours if provocative cardiac testing or imaging takes place.
4.5.2.0
SCPC Tool Example

SCPC ACCREDITATION & BIOMARKER TESTING: Key Element 4 – 4.4.0.0 overview
Demonstrating a process for reviewing and assessing Troponin TAT for Emergency Department (ED) patients
Documentation requirements: Monthly or quarterly meeting notes Lab participates as an agenda item Metrics, process and action plans discussed
Minimum 6 months of data Goal times Required to provide TAT metrics: cumulative & secondary Point-of-Care Testing (POCT) Central Laboratory Analyzers
12

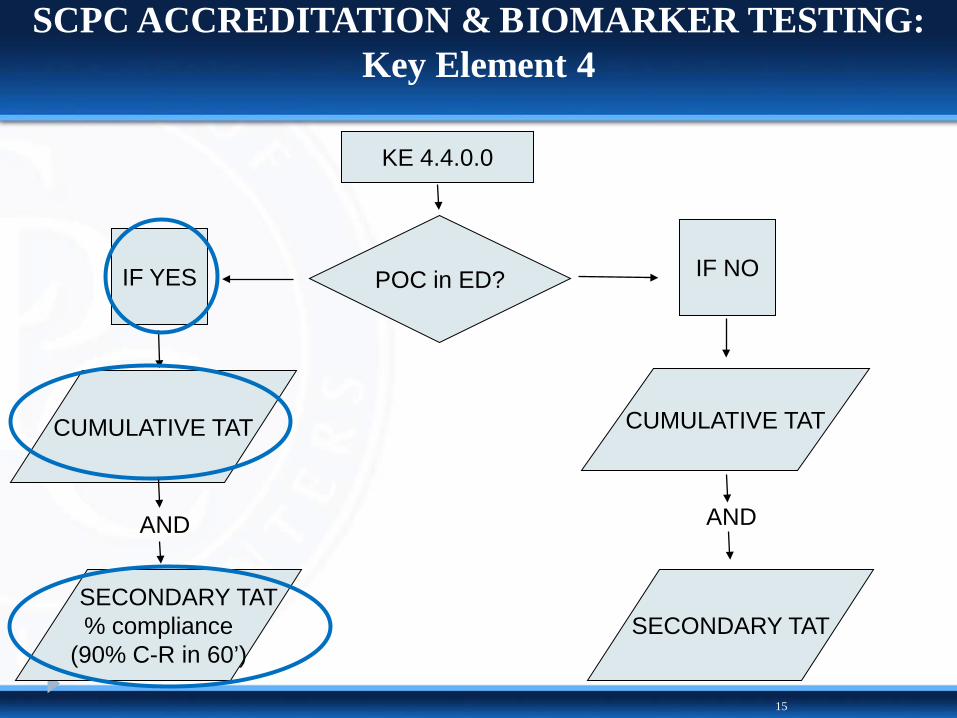
SCPC ACCREDITATION & BIOMARKER TESTING: Key Element 4
13
KE 4.4.0.0
POC in ED? IF NO IF YES
CUMULATIVE TAT CUMULATIVE TAT
AND AND
SECONDARY TAT % compliance
(90% C-R in 60’) SECONDARY TAT
Where does Point-of-Care Testing (POCT) fit in with CP Accreditation?
“To the extent that laboratory test TAT is only one factor impacting
ED length of stay and patient outcomes,
it is unlikely that POCT alone, in the absence of an interdepartmental approach to ED operations,
will produce measurable improvements in outcomes.”
Lewandrowski, E. et al. Cardiac Marker Testing As Part Of An
Emergency Department Point-of-Care Satellite Laboratory In A Large Academic Medical Center. Practical Issues Concerning Implementation. Point of Care. The Journal of Near Patient testing & Technology. Vol. 1,
No.3, pp. 145-154.
SCPC ACCREDITATION & BIOMARKER TESTING: Key Element 4
15
KE 4.4.0.0
POC in ED? IF NO IF YES
CUMULATIVE TAT CUMULATIVE TAT
AND AND
SECONDARY TAT % compliance
(90% C-R in 60’) SECONDARY TAT

CBM TAT EXAMPLE COLLECTION TOOL: 90% Goal w/in 60 minutes
Total (n=ED TnI)
# Collect to Result w/in
60 min
Collect-Result
<=60 min (=C/B) Goal
January 522 479 92% 90%February 554 453 82% 90%March 590 522 88% 90%April 520 477 92% 90%May 517 468 91% 90%June 507 471 93% 90%July 544 514 94% 90%August 473 440 93% 90%September 491 452 92% 90%October 534 484 91% 90%November 494 435 88% 90%December 490 463 94% 90%Totals: 6236 5658 91% 90%
Example: Troponin TAT
16
4.4.7.0
4.4.8.0
Year:____
DATA SUBMISSION OPTIONS
College of American Pathologist (CAP) QM1 monitor
The Society has partnered with the College of American Pathologist who have created a validation tool which collects data to meet the Society requirements for TAT tracking.
Additional benefits are having one source collecting data for research to track the “diagnostic TAT” or “door to result’ data through sampling.
17

SCPC ACCREDITATION & BIOMARKER TESTING: Key Element 4
18
4.5.1.0 – The facility has a process in place to monitor the TAT of serial draws for Troponin
Key concept: “Windows of Scheduled Time”
•Assessment and documentation of serial draw time points

SCPC Summary
19
Information is current as of 7/1/2012: SCPC KE 4.4.0.0
Troponin TAT tracking requirement? YES
Accreditation for PCI/Non-PCI
Admission/Disposition status dependant? NO
All ED baseline Troponin
Can use validation tools? YES
CAP QM1 monitor
Requires “door to result in 60 minutes”? NO
One cumulative (door/order/collect) and one secondary time-point; TAT goals must
be set by facility

SCPC Summary
20
Information is current as of 7/1/2012: SCPC KE 4.4.0.0
Requires % compliance? YES For POC, 90% collect-to-result in 60 min;
can also apply for main lab.
Includes PCI Hospitals? YES All facilities applying for
Chest Pain Accreditation
Includes Non-PCI Hospitals? YES
All facilities applying for Chest Pain Accreditation
Includes Critical Access Hospitals? YES
All facilities applying for Chest Pain Accreditation

Summary
Expectations and documentation requirements include:
TAT tracking for POC or central lab analyzers
Laboratory participation in meetings, at least quarterly
Metrics broken down into different time points with clear definitions of starting and end point goals and include: The number (n) of cases by month Data minimum: six months Policies for tracking of serial time-points
21

DISCLAIMER
CMS and OP-16 : Information and opinions included in this presentation
are based on interpretation of currently available regulatory resources.
No representation is made as to the completeness of the information.
Please refer to specific regulatory guidelines, hospital coding/billing or quality department as necessary for the latest updates.
The following information is derived from research of various sources, to include but not limited to the following:
CMS, Qualitynet.org, the Federal Register, QIO, industry guidance documents and industry representatives
22

Hospital Inpatient Quality Data Reporting Program Summary from Inpatient Prospective Payment System- Final Rule
23
INPATIENT Current and Proposed Measures Collected and Submitted by Hospital
HIQRP* VBP**
MEASURE Reporting effective
date Affects
APU
Reporting effective
date
Affects Reimburse
ment Acute Myocardial Infarction (AMI)
AMI-1 Aspirin at arrival *Ended
2011 *Retire FY 2014
AMI-2 Aspirin prescribed at discharge Ongoing Ongoing
AMI-3 Angiotensin Converting Enzyme Inhibitor (ACE-I) or Angiotensin II Receptor Blocker (ARB) for left ventricular systolic dysfunction
*Ended 2011
*Retire FY 2014
AMI-4 Adult smoking cessation advice/counseling *Ended
2011 *Retire FY 2014
AMI-5 Beta blocker prescribed at discharge *Ended
2011 *Retire FY 2014
AMI-7a Fibrinolytic (thrombolytic) agent received within 30 minutes of arrival Ongoing Ongoing July 2011 FY 2013
AMI-8a Timing of Receipt of Primary Percutaneous Coronary Intervention (PCI) Ongoing Ongoing July 2011 FY 2013 AMI-10 Statin prescribed at discharge Jan 2011 FY 2013 Emergency Department (ED)
Heart Failure (HF)
Pneumonia (PN)
Stroke
Surgical Care Improvement Project (SCIP)
Venous Thromboembolism (VTE)
Global Immunizations
*HIQRP - Hospital In-patient Quality Reporting Program
**VBP - Value Based Purchasing Program

Hospital Outpatient Quality Data Reporting Program Summary from Outpatient Prospective Payment System (OPPS) - Final Rule
24
Measure # Measure Short Name: CY2012, CY2013, CY2014 Payment Determination HOSPITAL COMPARE TJC ORYX Effective Collection MEASURE SET:
OP-1 Median Time to Fibrinolysis NO YES Ongoing Abstract AMI / SCPC OP-2 Fibrinolytic Therapy Received Within 30 Minutes YES YES Ongoing Abstract AMI / SCPC OP-3 Median Time to Transfer to Another Facility for Acute Coronary Intervention YES YES Ongoing Abstract AMI / SCPC OP-4 Aspirin at Arrival YES YES Ongoing Abstract
OP-5 Median Time to ECG YES YES Ongoing Abstract AMI / CP/ SCPC OP-6 Timing of Antibiotic Prophylaxis NO YES Ongoing Abstract
OP-7 Prophylactic Antibiotic Selection for Surgical Patients NO YES Ongoing Abstract
OP-8 MRI Lumbar Spine for Low Back Pain YES NA Ongoing Medicare Claims
OP-9 Mammography Follow-up Rates YES NA Ongoing Medicare Claims
OP-10 Abdomen CT - Use of Contrast Material YES NA Ongoing Medicare Claims
OP-11 Thorax CT - Use of Contrast Material YES NA Ongoing Medicare Claims
OP-12 The Ability for Providers with HIT to Receive Laboratory Data Electronically Directly into their Qualified/Certified EHR System as Discrete Searchable Data NO NA 1/1/2011 Structural (YES/NO) LAB
OP-13 Cardiac Imaging for Preoperative Risk Assessment for Non Cardiac Low-Risk Surgery YES NA 1/1/2011 Medicare Claims
OP-14 Simultaneous Use of Brain Computed Tomography (CT) and Sinus CT YES NA 1/1/2011 Medicare Claims
OP-15 Use of Brain Computed Tomography (CT) in the ED for Atraumatic Headache NA 1/1/2011 Medicare Claims Postponed 07/12
OP-16 Troponin Results for ED AMI or chest pain patients (with Probable Cardiac Chest Pain) Received Within 60 minutes of Arrival NA 1/1/2012 Abstract AMI / CP/ SCPC
& LAB OP-17 Tracking Clinical Results between Visits NA 1/1/2012 Structural (YES/NO) LAB OP-18 Median Time from ED Arrival to ED Departure for Discharged ED Patients 2013 NA 1/1/2012 Abstract
OP-19 Transition Record with Specified Elements Received by Discharged Patients
NA
1/1/2012
Abstract -YES or NO
SUSPENDED FROM VALIDATION / APU
04/12 OP-20 Door to Diagnostic Evaluation by a Qualified Medical Professional NA 1/1/2012 Abstract
OP-21 ED- Median Time to Pain Management for Long Bone Fracture NA 1/1/2012 Abstract
OP-22 ED- Patient Left Before Being Seen NA 1/1/2012 Abstract
OP-23 ED- Head CT Scan Results for Acute Ischemic Stroke or Hemorrhagic Stroke who Received Head CT Scan Interpretation Within 45 minutes of Arrival NA 1/1/2012 Abstract

Hospital Outpatient Quality Data Reporting Program Summary from Outpatient Prospective Payment System (OPPS)
25
Measure # CY2012, CY2013, CY2014 Payment Determination Effective Collection MEASURE SET
OP-1 Median Time to Fibrinolysis Ongoing Abstract AMI / SCPC
OP-2 Fibrinolytic Therapy Received Within 30 Minutes Ongoing Abstract AMI / SCPC
OP-3 Median Time to Transfer for Acute Coronary Intervention Ongoing Abstract AMI / SCPC
OP-5 Median Time to ECG Ongoing Abstract AMI/ CP/ SCPC
OP-12 The Ability for Providers with HIT to Receive Laboratory Data Electronically Directly into their Qualified/Certified
EHR System as Discrete Searchable Data 1/1/2011 Structural
(YES/NO) LAB
OP-16 Troponin Results for ED AMI or chest pain patients Received within 60 minutes of Arrival (aka: Door to Result)
1/1/2012 Abstract AMI/ CP/ SCPC & LAB
OP-17 Tracking Clinical Results between Visits 1/1/2012 Structural (YES/NO) LAB

UPDATE: CMS OP-16 MEASURE CHANGE
On August 13, 2012, CMS issued an SDPS Memorandum #12-257-OD for the removal of Hospital Outpatient Quality Reporting (HOQR) measure OP-16.
“The Centers for Medicare & Medicaid Services (CMS) announces the immediate removal of the following measure from the HOQR measure set: OP-16…
We are removing OP-16 from the HOQR measure set based on patient safety concerns. On July11, 2012 the Food and Drug Administration (FDA) issued a Class I recall on several point of care (POC) testing kits, including those that provide Troponin results. The Class I recall was due to false results… (see FDA website – ucm311405)
While OP-16 does not specify which type of laboratory equipment should be used to obtain Troponin results, hospitals may be using these POC tests in order to expedite results. In view of the recent Class I recall, CMS is concerned that continued collection of the measure may potentially impact patient safety because of the high probability of false results associated with such equipment.”
26

UPDATE: CMS OP-16 MEASURE CHANGE
“ CMS WILL NOT publically report, validate or use in CY 2013 payment determination any data collected on this measure…
…CMS is unable to immediately cease data collection in the system. In order to overcome CMS’s system limitation, hospitals can choose to submit a value that is not meaningful for this measure.
Please do not submit a blank value for OP-16, as a lack of a populated value for OP-16 will cause a case to be rejected. If a case is rejected due to lack of data, this could impact a hospital’s ability to meet Hospital OQR requirements for receiving a full outpatient hospital annual payment update…Hospitals are encouraged to work with their vendors to determine options to populate the OP-16 data field at submission.” CMS SDPD MEMORANDUM #12-257-OD
27

Hospital Outpatient Quality Data Reporting Program Summary from Outpatient Prospective Payment System (OPPS) –
Updates
28
Measure # Measure Short Name: MEASURE SET:
OP-15 Use of Brain Computed Tomography (CT) in the ED for Atraumatic Headache
Public Reporting Postponed until
2013 (07/12)
OP-16 Troponin Results for ED AMI or chest pain patients (with Probable Cardiac Chest Pain) Received Within 60 minutes of Arrival
SUSPENDED FROM VALIDATION / APU
08/12
OP-19 Transition Record with Specified Elements Received by Discharged Patients
SUSPENDED FROM VALIDATION / APU
04/12

29
Measure # Measure Short Name: CY2012, CY2013, CY2014 Payment Determination
OP-12 The Ability for Providers with HIT to Receive Laboratory Data Electronically Directly into their Qualified/Certified EHR System as Discrete Searchable Data
OP-17 Tracking Clinical Results between Visits
OP 12 and OP 17
= YES or NO answer only
Departments Included: ED, outpatient imaging, outpatient surgery, clinics
The "Yes" or "No" is not linked to APU, just whether it was answered
*EHR must be Office of the National Coordinator for Health Information Technology (ONC) certified

OPPS SUMMARY
Validation and Payment Requirements
All hospitals submit data to CMS; all measures must be addressed
Payment: ~2% percent 4 measures (OP 12, 16, 17 and 19) are currently not included in the determination for the APU
75% compliance requirement for reimbursement Failure to meet 75% = to failing to report = ~ 2% reduction in
annual payment update (APU)
30

Why OP-16 was implemented originally?
CMS statement of Troponin TAT as a measure of “quality”
“…The focus of this measure is on the timeliness of the receipt of the Troponin results…For this reason, we believe timeliness of the availability of the test results is a marker of quality because it results in more timely treatment decisions and treatment delivery, which in turn results in better outcomes for patients.” CMS-1525-FC
Suspension of this measure does not negate the real impact of why it was originally implemented. Facilities should continue to strive towards assessment and reductions in the diagnostic TAT (door –to-result).
Any progress and momentum in goal setting, improved communications and reductions of time will continue to impact patient care and quality outcomes.
31

Process Improvement Methods
Nurse driven or pre-approved standing order protocols
Validation tools CAP QM1 Monitor – meets SCPC requirements Goals need to be established from the various phases “door-to-result”
Lab workflow assessments and optimization: Door to Result Pre-analytical and analytical Lab and hospital information systems Connectivity Education for both the ED and Lab on detailed time-tracking processes
Key Players: Lab / ED / Cardiology ED Director / ED Medical Director / CPC Medical Director CPC Coordinator / Quality Department
32

Summary
Best demonstrated practices have requirements for defining and tracking cumulative turn-around-
time metrics of the whole-process or the patient-centric view.
As such, timeliness of the reporting of Troponin
equals timeliness of the diagnosis for the appropriate delivery of care in the Acute Coronary Syndrome patient population.
33

Links and Resources
Society of Chest Pain Centers www.scpcp.org or [email protected]
College of American Pathologists www.cap.org
34

Links and Resources
CMS and OPPS http://www.cms.gov/HospitalOutpatientPPS/
www.qualitynet.org http://www.hospitaloqr.com
http://www.hospitalcompare.hhs.gov
CMS is accepting public comments through September 4, 2012 for the proposed rules for 2013-2015 payment determinations. These can be found on the CMS website under “ CMS-1589-P” to download instructions of the Federal Register/ Vol. 77, No. 146/ Monday, July 30, 2012/ Proposed Rules/ PDF page 7 & 116-128, Hospital OQR Program.
35



![SATELLITE MODEM SCPC - Global Telesat · 2019-08-19 · satellite modem scpc user manual software release 3.2 [uhp.sc32.en] january 2015](https://img.dokumen.tips/doc/110x75/5e993c307d433045ed247eef/satellite-modem-scpc-global-telesat-2019-08-19-satellite-modem-scpc-user-manual.jpg)















![[17.07.18] SCPC 1회 본선 - 트리](https://img.dokumen.tips/doc/110x75/5a6635a57f8b9ac10a8b45d1/170718-scpc-1-.jpg)










