Embed Size (px)
Citation preview

REPO
RT
SPECIAL REPORT FROM THE SOCIETY OF THORACIC SURGEONS
2012 ACCF/AATS/SCAI/STS Expert ConsensusDocument on Transcatheter Aortic ValveReplacementDeveloped in collaboration with the American Heart Association, American Society ofEchocardiography, European Association for Cardio-Thoracic Surgery, Heart Failure Society ofAmerica, Mended Hearts, Society of Cardiovascular Anesthesiologists, Society ofCardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance
Writing Committee Members:David R. Holmes, Jr., MD, Chair*, Michael J. Mack, MD, Vice Chair†,Sanjay Kaul, MBBS, Vice Chair*, Arvind Agnihotri, MD‡, Karen P. Alexander, MD*,Steven R. Bailey, MD§, John H. Calhoon, MD‡, Blase A. Carabello, MD*,Milind Y. Desai, MBBS�¶, Fred H. Edwards, MD†, Gary S. Francis, MD#,Timothy J. Gardner, MD†, A. Pieter Kappetein, MD, PhD**,Jane A. Linderbaum, MS, CNP*, Chirojit Mukherjee, MD††, Debabrata Mukherjee, MD*,Catherine M. Otto, MD*, Carlos E. Ruiz, MD, PhD§, Ralph L. Sacco, MD‡‡,
Donnette Smith§§, James D. Thomas, MD� �Author Recusals: Writing committee members are required to recusethemselves from voting on sections to which their specific relationshipwith industry and other entities may apply; see Appendix 1 for recusalinformation.
This document was approved by the American College of CardiologyFoundation (ACCF) Board of Trustees, American Association for ThoracicSurgery (AATS) Council, Society for Cardiovascular Angiography andInterventions (SCAI) Board of Directors, Society of Thoracic Surgeons(STS) Board of Directors in January 2012 and endorsed by the governingbodies of the American Heart Association (AHA) Science Advisory andCoordinating Committee, American Society of Echocardiography (ASE),European Association for Cardio-Thoracic Surgery (EACTS), Heart Fail-ure Society of America (HFSA), Mended Hearts, Society of Cardiovascu-lar Anesthesiologists (SCA), Society of Cardiac Computed Tomography(SCCT), and the Society for Cardiovascular Magnetic Resonance (SCMR)in January 2012. For the purpose of complete transparency, disclosureinformation for the ACCF Board of Trustees, the board of the conveningorganization of this document, is available at: http://www.cardiosource.org/ACC/About-ACC/Leadership/Officers-and-Trustees.aspx. ACCF board members with relevant relationships withindustry to the document may review and comment on the document butmay not vote on approval.
The Society of Thoracic Surgeons requests that this document be cited asfollows: Holmes DR Jr., Mack MJ, Kaul S, Agnihotri A, Alexander KP,Bailey SR, Calhoon JH, Carabello BA, Desai MY, Edwards FH, Francis GS,Gardner TJ, Kappetein AP, Linderbaum JA, Mukherjee C, Mukherjee D,Otto CM, Ruiz CE, Sacco RL, Smith D, Thomas JD. 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valvereplacement. Ann Thorac Surg 2012;93:1340–95.
This article has been copublished in Anesthesia and Analgesia, The Annalsof Thoracic Surgery, Catheterization and Cardiovascular Interventions, Journalof the American College of Cardiology, and the Journal of Thoracic andCardiovascular Surgery.
Copies: This document is available on the World Wide Web sites ofthe American College of Cardiology (http://www.cardiosource.org), the
American Association for Thoracic Surgery (http://www.aats.org), theSociety for Cardiovascular Angiography and Interventions (http://© 2012 by The Society of Thoracic Surgeons, the American College ofSurgery, and the Society for Cardiovascular Angiography and IntervenPublished by Elsevier Inc
Preamble
This document has been developed as an Expert Con-sensus Document (ECD) by the American College ofCardiology Foundation (ACCF), American Associationfor Thoracic Surgery (AATS), Society for CardiovascularAngiography and Interventions, and The Society of Tho-racic Surgeons (STS) in collaboration with the AmericanHeart Association (AHA), American Society of Echocar-diography, European Association for Cardio-Thoracic
www.scai.org), The Society of Thoracic Surgeons (http://sts.org), theAmerican Society of Echocardiography (http://www.asecho.org), theHeart Failure Society of America (http://www.hfsa.org), and MendedHearts (http://mendedhearts.org). For copies of this document, pleasecontact Elsevier Inc. Reprint Department, fax 212-633-3820, [email protected].
Permissions: Multiple copies, modification, alteration, enhancement,and/or distribution of this document are not permitted without theexpress permission of The Society of Thoracic Surgeons. Please contactElsevier’s permission department at [email protected].
*American College of Cardiology Foundation Representative;†Society of Thoracic Surgeons Representative;‡American Association for Thoracic Surgery Representative;§The Society for Cardiovascular Angiography and Interventions Repre-sentative;�Society of Cardiovascular Computed Tomography Representative;¶Society for Cardiovascular Magnetic Resonance Representative;#Heart Failure Society of America Representative;
**European Association for Cardio-Thoracic Surgery Representative;††Society of Cardiovascular Anesthesiologists Representative;‡‡American Heart Association Representative;§§Mended Hearts Consumer Advocate, Patient Representative;
� �American Society of Echocardiography Representative.Cardiology Foundation, the American Association for Thoracictions Ann Thorac Surg 2012;93:1340–95 • 0003-4975/$36.00
doi:10.1016/j.athoracsur.2012.01.084

1341Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
Surgery, Heart Failure Society of America, Society ofCardiovascular Computed Tomography, Society of Car-diac Magnetic Resonance, Society of Cardiovascular An-esthesiologists, and Mended Hearts. ECDs are intendedto inform practitioners, payers, and other interestedparties of the opinion of ACCF and document cosponsorsconcerning evolving areas of clinical practice and/ortechnologies that may be widely available or may be newto the practice community. Topics chosen for coverage byECDs are so designed because the evidence base, theexperience with technology, and/or clinical practice arenot considered sufficiently well developed to be evalu-ated by the formal ACCF/AHA Practice Guidelines pro-cess. Often the topic is the subject of considerable ongo-ing investigation. Thus, the reader should view the ECDas the best attempt of the ACCF and document cospon-sors to inform and guide clinical practice in areas whererigorous evidence may not yet be available or evidence todate is not widely applied to clinical practice. Whenfeasible, ECDs include indications or contraindications.Some topics covered by ECDs will be addressed subse-quently by the ACCF/AHA Practice Guidelines Committee.
To avoid actual, potential, or perceived conflicts ofinterest that may arise as a result of industry relation-
Abbreviation and Acronyms
AR � aortic regurgitationAS � aortic stenosisAVA � aortic valve areaAVR � aortic valve replacementCAD � coronary artery diseaseCMR � cardiac magnetic resonanceCOPD � chronic obstructive pulmonary
diseaseCT � computed tomographyEF � ejection fractionEOA � effective orifice areaEuroSCORE � European system for cardiac
operative risk evaluationLV � left ventricularLVOT � left ventricular outflow pactMDCT � multidetector computed
tomographyNCDR � National Cardiovascular Data
RegistryPARTNER � Placement of Aortic Transcatheter
Valve trialPH � pulmonary hypertensionRV � right ventricularSOURCE � SAPIEN Aortic Biosprosthesis
European Outcome registrySTS � Society of Thoracic SurgeonsTAVR � transcatheter aortic valve
replacementTEE � transesophageal echocardiogramTTE � transthoracic echocardiographyVARC � Valve Academic Research
Consortium
ships or personal interests among the writing committee,
all members of the writing committee, as well as peerreviewers of the document, are asked to disclose allcurrent healthcare-related relationships, including thoseexisting 12 months before initiation of the writing effort.The ACCF Task Force on Clinical Expert ConsensusDocuments (TF CECD) reviews these disclosures to de-termine what companies make products (on market or indevelopment) that pertain to the document under devel-opment. Based on this information, a writing committeeis formed to include a majority of members with norelevant relationships with industry or other entity (RWI),led by a chair with no relevant RWI. Authors with relevantRWI are not permitted to draft or vote on text or recom-mendations pertaining to their RWI. RWI is reviewed onall conference calls and updated as changes occur. Au-thor and peer reviewer RWI pertinent to this documentare disclosed in Appendices 1 and 2, respectively. Addi-tionally, to ensure complete transparency, authors’ com-prehensive healthcare-related disclosure information—including RWI not pertinent to this document—isavailable online (see Online Appendix). Disclosure infor-mation for the ACCF TF CECD is also available online atwww.cardiosource.org/ACC/About-ACC/Leadership/Guidel ines-and-Documents-Task-Forces .aspx ,as well as the ACCF disclosure policy for documentdevelopment at www.cardiosource.org/Science-And-Quality/Practice-Guidelines-and-Quality-Standards/Relationships-With-Industry-Policy.aspx.
The work of the writing committee was supported exclu-sively by the ACCF without commercial support. Writingcommittee members volunteered their time to this effort.Conference calls of the writing committee were confidentialand attended only by committee members.
Robert A. Harrington, MD, FACCChair, ACCF Task Force on Clinical Expert Consensus Documents
1. Introduction
1.1. Document Development Process1.1.1. WRITING COMMITTEE ORGANIZATION. The Writing Com-mittee consisted of a broad range of members repre-senting 12 societies and the following areas of exper-tise: cardiothoracic surgery, interventional cardiology,general cardiology, geriatric cardiology, echocardiog-raphy, cardiac anesthesiology, cardiac computed to-mography (CT), cardiac magnetic resonance (CMR),cardiac nursing, heart failure, neurology, valvularheart disease, structural heart disease, and the con-sumer perspective. Geographic distribution of mem-bers crossed most U.S. time zones and included inter-national representation. Members with expertise usingthis new and emerging technology and those withexpertise in their content area, but not in the procedure
ACCF Task Force Members: Robert A. Harrington, MD, Chair; Deepak L.Bhatt, MD, MPH, Vice Chair; Victor A. Ferrari, MD; John D. Fisher, MD;Mario J. Garcia, MD; Timothy J. Gardner, MD; Federico Gentile, MD;Michael F. Gilson, MD; Adrian F. Hernandez, MD; Alice K. Jacobs, MD;
Sanjay Kaul, MBBS; Jane A. Linderbaum, MS, CNP; David J. Moliterno,MD; Howard H. Weitz, MD
1342 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
discussed herein, served on the committee to provideappropriate balance of perspectives.
This writing committee met the College’s disclosurerequirements for relationships with industry as de-scribed in the Preamble. Important to note, if an authorworks in an institution that serves as a TAVR trial site buthas no direct relationship with the trial sponsor or otherrelevant company (that produces [competing] productsor services discussed in this document) or institutionalrelationship as defined by the ACCF Disclosure Policy forDocument Development, the trial site information wasnot deemed relevant to this writing effort and is notincluded in the table of relevant author disclosures (Ap-pendix 1). For example, if an author works in an institu-tion where TAVR is performed, but he/she: 1) does notpersonally perform the procedure; or 2) performs theprocedure but has no direct relationship to the trial (e.g.,principal investigator, investigator, steering committeemember, consultant) and does not oversee funds relatedto the trial, then the relationship is not included in thetable of relevant disclosures. In these situations, theserelationships do not even need to be disclosed. However,in the spirit of full disclosure, this information is recordedin the online disclosure table containing all authorhealthcare relationships.1.1.2. DOCUMENT DEVELOPMENT AND APPROVAL. The WritingCommittee convened by conference call and e-mail tofinalize the document outline, develop the initial draft,revise the draft per committee feedback, and ultimatelysign off on the document for external peer review. Allparticipating organizations participated in peer review,resulting in 48 reviewers representing 1,087 comments.Comments were reviewed and addressed by the writingcommittee. A member of the ACCF TF CECD served aslead reviewer to ensure that all comments were ad-dressed adequately. Both the Writing Committee and TFCECD approved the final document to be sent for boardreview. The ACCF Board of Trustees, AATS Council,SCAI Board of Directors, and STS Board of Directorsreviewed the document, including all peer review com-ments and Writing Committee responses, and approvedthe document in January 2012. The AHA, ASE, EACTS,HFSA, Mended Hearts, SCA, SCCT, and SCMR endorsedthe document in January 2012. This document is consid-ered current until the TF CECD revises or withdraws itfrom publication.
1.2. Purpose of This DocumentTranscatheter aortic valve replacement (TAVR) offersnew and potentially transformational technology for pa-tients with severe aortic valvular stenosis who are eitherextremely high-risk candidates or inoperable for surgicalaortic valve replacement (AVR) or who are inoperable byvirtue of associated comorbidities. In the future, thistechnology may be utilized in lower risk surgical candi-dates. An estimated 40,000 patients have received TAVRworldwide. Multiple single and multicenter registries,and a single randomized trial, have documented favor-able outcomes using a wide spectrum of endpoints,
including survival, symptom status, quality of life, andneed for repeat hospitalization. The implementation ofTAVR into the flow of patient care is complex, involvingconsideration of several key factors such as clinical siteselection, operator and team training and experience,patient selection and evaluation, procedural performanceand complication management, and postprocedural care.Collaborative stakeholder involvement is required in themanagement of this high-risk patient population withextensive coexistent medical conditions. A previouslypublished document by ACCF and STS identified ahigh-level series of issues to be addressed regarding thistechnology [1]. This current collaborative expert consen-sus document, which involves 12 professional societies,addresses these issues in greater detail with the intent toexamine the current state of the evidence, facilitate theintegration of this technology into the armamentarium oftherapeutic options for patients with aortic valvular ste-nosis, and to enable responsible adoption and diffusionof this promising technology. This document has focusedon published data; it must be remembered that there isonly 1 single completed randomized trial, although oth-ers are in progress or planned; much of the data in thisexpert consensus document is based upon informationfrom studies and registries, both surgical and TAVR,which are frequently retrospective and include self-reported clinical events rather than adjudicated events.
2. Background and Historical Aspects
The most common cause of valvular aortic stenosis (AS)in adults is calcification of a normal trileaflet or congen-ital bicuspid valve [2–4]. Calcific AS is characterized bylipid accumulation, inflammation, fibrosis, and calcifica-tion [5, 6] and is common in the United States. It typicallypresents in older individuals (i.e., �75 years) in contrastto bicuspid AS, which presents a decade or moreearlier. Rheumatic AS, uncommon in the Westernworld, occurs due to fusion of the commissures withscarring and calcification of the cusps, and retraction ofthe leaflets resulting in the valve being both regurgi-tant and stenotic.
2.1. Pathophysiology and Clinical CourseIn adults with valvular AS, the obstruction developsgradually, typically over many years during which theleft ventricle (LV) adapts to the systolic pressure overloadwith progressive concentric hypertrophy that results indiastolic dysfunction [4, 7, 8], reduced coronary reserve[9, 10], myocardial ischemia [11], and eventually, de-pressed contractility resulting in LV systolic dysfunction[12–14]. Ultimately, in some patients, heart failure orsudden death occurs. Typically, patients with AS are freefrom cardiovascular symptoms (i.e., angina, syncope, andheart failure) until late in the course of the disease.However, once symptoms manifest, the prognosis ispoor, with the interval from the onset of symptoms to thetime of death being approximately 2 years in patientswith heart failure, 3 years in those with syncope, and 5years in those with angina [15]. Gardin et al. reported that
among symptomatic patients with moderate-to-severe
1343Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
AS treated medically, mortality rates after the onset ofsymptoms were approximately 25% at 1 year and 50% at2 years [16], with approximately 50% of deaths beingsudden. In the elderly high-risk patients in the PART-NER (Placement of Aortic Transcatheter Valve) trial whowere treated medically (Cohort B), the survival at 1 yearwas only 50% [15].
The natural history of AS has changed since thepublication of the seminal paper by Morrow and col-leagues in 1968 [17]. The original data were derivedlargely from patients with rheumatic AS or AS due to abicuspid aortic valve, with an average age of death of63 years. On the contrary, patients being consideredfor TAVR on a trileaflet valve present much later in life,typically in their late 70s or older, and have dominantlyfibrocalcific AS. Although now occurring later in life,the onset of symptoms still heralds a rapid decline withmedical therapy alone [15].
2.2. Diagnosis2.2.1. ECHOCARDIOGRAPHY VERSUS CATHETERIZATION. Assess-ment of the severity of stenosis does not differ in TAVRpatients compared with the general AS population, anddecisions should therefore be based upon establishedguidelines [18]. Although invasive cardiac catheteriza-tion has historically been the standard for quantifica-tion of AS, this function has been largely replaced byechocardiography [19].
Echocardiographic diagnosis is made by the observa-tion of a calcified valve with restricted leaflet opening bytwo-dimensional (2D) echocardiography with quantifica-tion of the peak and mean AV gradient made by applyingthe simplified Bernoulli equation (�p � 4v2) to themaximal velocity recorded through the aortic valve bycontinuous-wave Doppler. Multiple imaging windows(apical 4-chamber and long-axis, right parasternal, su-prasternal notch, and subcostal views) should be ob-tained to assure acquisition of the maximal velocity andto avoid angle-related errors. Although aortic valve area(AVA) can be measured by planimetry, it is more accu-rately assessed by application of the continuity equation,using pulsed-wave Doppler in the left ventricular outflowtract (LVOT) and continuous-wave Doppler across thevalve. Severe stenosis is defined in the guidelines as apeak velocity �4.0 m/s (corresponding to a peak gradientof 64 mm Hg), a mean gradient �40 mm Hg, OR valvearea �1.0 cm2 when LV systolic function is normal. Toaccount for patient size, the valve area is often indexed tobody surface area, with 0.6 cm2/m2 considered to be thethreshold for severe AS. An important exception is whenthe gradient suggests less severe stenosis than the valvearea, most commonly due to low stroke volume, either indilated ventricles with low ejection fraction (EF) or smallventricles with normal EF. In this setting, a dobutaminestress study (maximum stress dose 20 mcg/kg/min), maybe helpful. If the maximum jet velocity rises over 4 m/swith the dobutamine-induced increase in stroke volumewhereas the AVA remains less than 1.0 cm2, then thevalve is truly severely stenotic. On the other hand, if
stroke volume increases with little rise in gradient (caus-ing valve area to increase substantially), then the AS isonly mild to moderate in severity, and the LV dysfunc-tion is due to causes other than AS [20–22].
Occasionally, the AVA appears larger than the ele-vated gradient would suggest, usually due to elevatedstroke volume from aortic regurgitation (AR), anemia,fever, or hyperthyroidism. Sometimes, though, it reflectsa technical error in applying the continuity equation,when the blood accelerates within the LVOT due to anupper septal bulge, which may result in an overestima-tion of valve area. To avoid this, one can try to measurethe LVOT area at the point of maximal velocity, thoughthe geometry is often quite distorted in this region,making estimation of the LVOT area difficult. Alterna-tively, one can use the LV stroke volume (from 2D orthree-dimensional [3D] measurements of the LV, ideallywith contrast infusion) or right ventricular (RV) strokevolume (from RV outflow tract) as the input into thecontinuity equation. Dividing this stroke volume by thetime velocity integral of the AV continuous-wave Dopp-ler will also yield the AVA, independent of any distortionin the LVOT.
Despite the convenience and wide-spread applicabilityof transthoracic echocardiography (TTE), there are occa-sions when invasive measurements are needed, such asin patients with a discrepancy between clinical andechocardiographic assessments. In such cases, catheter-ization should generally be performed with dual cathe-ters, 1 placed in the LV, the other in the proximal aorta toobtain simultaneous pressure measurements and obtainthe most accurate assessment of the gradient. Infusion ofdobutamine may allow assessment of low-output, low-gradient AS in the catheterization laboratory [23]. Otheradjunctive testing used in quantifying AS includes trans-esophageal echocardiography (TEE) [24], CT scanning(dynamic or gated during systole) [25], and CMR [26].2.2.2. STRESS TESTING. The presence or absence of symptomsshould guide the management of AS patients, yet inmany cases, this important clinical benchmark is difficultto establish, owing to the subjective nature of the symp-toms and comorbid conditions such as chronic lungdisease in this patient population. In general, stresstesting is contraindicated when symptoms are presentbecause of the potential for complications in these pa-tients. However, in patients with equivocal symptoms,stress testing, and in particular stress echocardiography,can be very helpful [27]. Simple determination of func-tional capacity may help show limitations of which apatient may be unaware. Isolated echocardiographic(ECG) changes during the stress test without symptomsor change in blood pressure should not be interpreted asa positive indicator of severe AS. Other potential markersfor AS severity include signs of LV dysfunction onexercise echo or a rise in left atrial or right ventricularpressure [28, 29].
2.3. Special Considerations2.3.1. SYMPTOM STATUS. With severe, symptomatic, calcificAS, AVR is the only effective treatment that improves
symptoms and prolongs survival [30, 31]. These results
1344 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
are partly dependent on LV function. In the setting ofLV dysfunction caused by afterload mismatch, survivalis still improved, although improvement in LV functionand resolution of symptoms might be incomplete afterAVR. Age itself is a risk factor for adverse outcome, butit is not a contraindication to AVR even in the veryelderly [32, 33].2.3.2. ASSOCIATED CORONARY ARTERY DISEASE. In patients withmoderate AS, who are undergoing coronary arterybypass graft surgery (CABG), AVR should be per-formed at the time of revascularization irrespective ofsymptoms related to moderate AS [34, 35]. There are nodata to support performing AVR for mild AS at thetime of CABG. Patients undergoing surgical AVR withsignificant stenoses (�50% to 70% stenosis) in majorcoronary arteries should be treated with concomitantCABG. Options in patients with combined AS andCAD continue to grow with the use of hybrid proce-dures where PCI is followed by valve surgery. It ispossible that such a strategy could be performed in thesetting of TAVR [36, 37].2.3.3. ASSOCIATED LESIONS—AR, MR, PULMONARY HYPERTENSION, TR.
Patients with severe AS often have additional associatedsignificant valvular heart disease. Treatment of theselesions in patients undergoing AVR should be under-taken using standard criteria. However, treatment ofassociated valvular lesions may increase the risk of AVR[38]. A special circumstance is that of pulmonary hyper-tension (PH) either primary or secondary (reactive orrelated to increased LV end-diastolic pressure). Bothconditions may increase the risk of AVR and must betaken into consideration in the risk/benefit ratio.
PH can be present in patients with severe AS, eitherfrom the transmission of increased LV diastolic and/orleft atrial pressures, associated mitral regurgitation(MR), or from a secondary increase in pulmonaryvascular tone. The prevalence of PH in patients withAS is undefined, varying widely on the definition usedand the population studied [39, 40]. Clinically, PHassociated with critical AS portends a poor prognosisand is associated with an increased risk of suddencardiac death [41]. Consistent with the surgical valveimplant experience, PH after TAVR is a predictivefactor for both early (30-day) and late (1-year) mortal-ity, similar in risk to major access site complicationsand renal insufficiency [39,42– 46]. The presence of PHmakes patients more susceptible to any hemodynamicand electrical instability related to the procedure andmay increase the risk of postprocedural complications.In addition, PH may result in right heart failure andsevere tricuspid regurgitation (TR), both of whichcomplicate management and increase risks.
In the setting of severe AS and PH several treatmentstrategies have been used [47]. Persistently elevatedleft-sided cardiac filling pressures increase the risk ofpulmonary edema when challenged with a pulmonaryvasodilator. Pulmonary vasodilators, such as nitric oxide,prostacylin, and sildenafil, have been administered dur-
ing and following cardiac surgery with improved hemo-dynamic effects [48–50]. However, their overall clinicalutility in improving late survival in the surgical popula-tion and their role in TAVR remains unclear. Furtherinvestigation is needed to determine the optimal proce-dural and periprocedural management of patients withAS and PH undergoing TAVR.2.3.4. LOW GRADIENT–LOW EF. As mentioned, the combinationof overt congestive heart failure and low aortic valvegradient is relatively common. This may be a conse-quence of excessive afterload (despite left ventricularhypertrophy [LVH]) or reduced contractile function [51]likely due to increased myocardial fibrosis [52]. When there isovert heart failure due to low forward flow and a lowtransvalvular gradient (mean gradient �30 mm Hg), bothmechanisms may be present. Because of reduced con-tractility in the low-flow/low-gradient AS patient, prog-nosis with surgical AVR is adversely affected with oper-ative mortality as high as 20%. However the 5-yearsurvival is still reported to be better in patients treatedsurgically [53, 54]. When the primary reason for poor LVperformance is excessive afterload, the prognosis follow-ing surgical AVR is usually good [14]. In general, patientswith low gradient, low EF who have the best prognosisare those with inotropic reserve (shown by an increase instroke volume with dobutamine infusion), who havelimited coronary disease and a mean gradient that al-though low, still exceeds 20 mm Hg [53].2.3.5. BASAL SEPTAL HYPERTROPHY—OUTFLOW TRACT GRADIENTS.
Although infrequent, proximal septal bulging with LVOTobstruction may present unique issues in the presence ofAS. While this can be readily addressed during AVR viamyomectomy, such an approach would not be possiblewith TAVR. Thus, careful preprocedural echocardio-graphic screening is recommended to specifically avoidthis scenario in patients being considered for TAVR.
3. Current Treatment Options
3.1. Surgical AVRAVR is the only effective treatment considered a Class Irecommendation by ACCF/AHA and ESC guidelines inadults with severe symptomatic AS [28, 29]. Not onlydoes it offer symptomatic relief, the operation improveslong-term survival. Since 1960, when AVR was firstintroduced, advancement in prosthetic technology in-cluding improved hemodynamics, durability and throm-boresistance, and techniques in cardiac surgery such ascardioplegia, management of the small aortic root, resec-tion of associated subvalvular disease, and replacementof associated aortic aneurysm have resulted in improve-ments in both operative and long-term results.
3.1.1. VALVE TYPE. Current AVR options include mechanical,bioprosthetic, and in specific situations homograft andautograft techniques. Each has their advantages anddrawbacks, but the trend in some centers in the recentera has been toward tissue valve replacement in a ma-jority of patients because of improved durability and the
lack of requirement for anticoagulation therapy.
1345Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
3.1.1.1. Mechanical Valves. Mechanical valves are nowextremely durable, have excellent hemodynamics, and areminimally thrombogenic with adequate anticoagulation.Current anticoagulation is mostly based on Vitamin Kantagonists. Newer agents such as oral direct thrombininhibitors and factor Xa inhibitors have been studied inother patient populations, mainly atrial fibrillation, andhave been found to be associated with decreased bleedingrisk and minimum drug or food interaction [55]. They havenot been well studied in patients with AVR. With warfarinthere is a risk of serious thromboembolism of approxi-mately 0.5% a year and a similar risk of major hemorrhageannually [56]. Mechanical valves are typically preferred inyounger patients given their reliable long-term durability.
3.1.1.2. Bioprosthetic Valves. Compared with mechanicalvalves, bioprosthetic valves do not require anticoagula-tion with warfarin, and thus have a lower risk of bleed-ing. However, long-term durability varies substantiallywith age for these valves. Structural valve degenerationleading to symptoms or reoperation, commonly associ-ated with calcification of the biologic leaflets, occurs at anaverage of 10 to 12 years in younger patients and 15 to 18years in older patients. Actuarial freedom from reopera-tion following implant of a modern bioprosthetic valvesis approximately 95% at 5 years, 90% at 10 years, butdrops to 70% at 15 years [57]. Thus, bioprosthetic valvesare generally preferred in older patients who are unlikelyto tolerate bleeding risk associated with anticoagulationtreatment and in whom a 15-year durability is reason-able. In patients with bioprosthetic valves, if prostheticdysfunction occurs, TAVR may play an important role insolving the clinical issues in the future.
3.1.2. PROCEDURAL HAZARDS. Current data from The Societyof Thoracic Surgeons (STS) registry documents a mortal-ity that is under 3% for all patients undergoing AVR. Aswith any procedure, operative mortality is strongly cor-related with the severity of the disease and comorbidityof patients. The operative risks can be estimated withonline risk calculators from the STS (http://209.220.160.181/STSWebRiskCalc261/) and the European Systemfor Cardiac Operative Risk Evaluation (www.euroscore.org) [58, 59]. In selected patients with minimal comorbidity,mortality and major morbidity are under 1% each in manycenters. In general, perioperative stroke rates are 1.5% (withmajor life-debilitating stroke being somewhat less) andother major complications are relatively rare. Renal failure,pulmonary failure, and gastrointestinal complications arenot common. As older, more frail patients with extensivecomorbidities undergo AVR, the risk of death and morbid-ity as well as length of hospitalization increases significantly[60, 61]. In addition to comorbidity, preoperative functionalperformance is also a maker of postoperativemorbidity/mortality.
A recent study reviewed the results of high-risk surgi-cal AVR in 4 centers with significant experience. Thepatients were a mean age of 76 and the mean STSpredicted risk of mortality was 16.3%. Complications
included stroke in 4.4%, new permanent pacemaker in5%, multisystem organ failure in 6.9%, pneumonia in7.5%, and dialysis in 8.2%. Postoperative length of staywas 12.6 days and in-hospital mortality was 16.4%. One-,3- and 5-year survival was 70.9%, 56.8%, and 47.4%. Thisstudy was performed between 2002 and 2007 in 4 centersbefore participation in the PARTNER Trial commencedand therefore serves as a reasonable baseline for com-paring the results of TAVR [62].
3.1.3. PATIENT SELECTION. Patient selection for AVR for AS iswell outlined by ACCF/AHA and ESC guidelines [29, 63].Problems arise when the clinicians and patients note sig-nificant symptoms and significant structural disease thatare complicated by the presence of significant comorbidity.Although current STS risk score and EuroSCORE giveinformation concerning short-term operative risks and ben-efits, they are not able to predict symptom resolution,quality-of-life improvement, or return to independentliving.
3.1.3.1. Use of STS and euroscore Models in Patient Selectionfor Conventional AVR. Although a number of risk algo-rithms for cardiac surgery have been developed, the STSand logistic EuroSCORE are the most commonly used.Although both are accurate in low-risk patients, accuracyis less in higher-risk subsets. These 2 scores includedifferent covariates. The logistic EuroSCORE is based on12 covariates derived from 14,799 patients undergoing alltypes of cardiac operations (mostly coronary bypass) in 8European countries in 1995. On the other hand, the STSrisk predictor is based on 24 covariates derived from67,292 patients undergoing isolated AVR only in theUnited States over a relatively more contemporary pe-riod between 2002 and 2006. The STS model is thestandard most commonly used in the United States.
3.1.3.2. Patient Risk of AVR. Information from the STSNational Database shows that the operative mortality forisolated AVR has declined from 3.4% in 2002 to 2.6%today (http://www.sts.org/sites/default/files/documents/20112ndHarvestExecutiveSummary.pdf). The most im-portant preoperative patient risk factors are the need foremergency surgery, the presence of endocarditis, and ahistory of previous cardiac surgery. The present modelsdo not include some risk factors that may be particularlyimportant in the prediction of outcomes for very high-risk populations including frailty, PH, porcelain aorta,and the presence of hepatic dysfunction, although allhave been added to a recent upgraded version [64, 65].
It should be emphasized that risk models serve as 1aspect of patient selection, but need to be considered inconcert with clinical judgment and the other methods ofrisk assessment. In the final analysis, patient risk andbenefit is determined, not by statistical models, but bythe experience, knowledge, and expertise of the physi-cians charged with rendering care.
3.1.3.2.1. Specific Surgical Risks3.1.3.2.1.1. Stroke. Although ischemic stroke can result
from many causes after AVR, a major concern is the role
1346 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
of thromboembolism. The risks of thromboembolism areusually greater in the first few days and months afterbioprosthetic AVR implantation before the sewing ring ofthe prosthesis is endothelialized [66]; risks after mechan-ical AVR continue. The risk of stroke within 30 daysamong 67,292 cases of AVR in the STS Registry was 1.5%;this data set was used to develop a model for predicting30-day stroke risk [61]. Within the STS database among108,687 AVR operations between 1996 through 2006, therisk of in-hospital permanent stroke decreased 21% from1.7% to 1.3% [67]. It is important to note, however, thatindependent neurological assessment was not done inthese patients, so the actual stroke incidence in thesepatients may be underestimated. Overall, embolicstroke risks are greater with mechanical valves, whichrequire long-term oral anticoagulation, than with bio-prosthetic valves, which have a 0.7% per year risk ofthromboembolism in patients with normal sinusrhythm without warfarin anticoagulation [68].
Of note, many AVR patients are older, with othercomorbid cardiac conditions that increase stroke risk,including atrial fibrillation, cardiomyopathy, and carotidstenosis or aortic arch atheroma [69]. However, evencarefully selected octogenarians can safely undergo AVRwith a 2% incidence of stroke [32, 70].
Because of the risk of stroke, the 2006 ACC/AHAguidelines for the management of patients with valvularheart disease include a variety of recommendations re-garding the use of antithrombotic therapy to reduce throm-boembolism risk after AVR [63]. The choice of antithrom-botic agents include warfarin with target internationalnormalized ratios (INRs) typically in the range from 2.0 to4.0 depending on the specific prosthesis, aspirin 75 mg to325 mg per day, and clopidogrel 75 mg per day, as well ascombinations. Recommendations depend upon the type ofvalve, timing after surgery, presence or absence of riskfactors such as atrial fibrillation, and ability of the patient totake warfarin or aspirin [63].
Given the greater risk of thromboembolism, particu-larly stroke, which usually occurs within the first 72 hourspost-procedure, many centers start heparin (target aPTT55 s to 70 s) as soon as the risk of surgical postoperativebleeding is acceptable, which is usually within 48 hoursof surgery. Heparin can be discontinued when warfarintherapy reaches a therapeutic INR usually above 2.0 [63].
3.1.3.2.1.2. Other Complications. Aside from other surgi-cal complications of renal, hepatic, neurological, andpulmonary disease compromise, a major risk of conven-tional AVR is sternal wound infection. In most centers,this risk is under 1% for deep infection, but the risk of anytype of infection is still present and particularly increasedin patients with diabetes, obesity, smoking, immunosup-pressive therapy, and prior radiation therapy. With theadvent of negative pressure wound therapy and contin-ued advances in surgical technique, these risks are nowrarely fatal, but remain morbid. Blood requirement aftervalve replacement can lead to hepatitis C, human immu-
nodeficiency virus, or other viral infection. These trans-fusion-acquired infections are now extremely rare due totransfusion guidelines and systems precautions.
3.1.3.3. Prohibitive Risk, Extreme Risk, Inoperability. De-spite substantial contemporary experience with success-ful AVR in elderly patients, multiple series have docu-mented that 30% to 40% of patients with severe AS do notundergo surgery owing to advanced age, LV dysfunction,multiple coexisting conditions, and patient preference orphysician recommendation [71–76].
The definitions used to describe patient populationsconsidered for TAVR vary; for example, prohibitive riskwould describe a patient in whom the procedure couldbe performed from a technical standpoint but would beassociated with prohibitively high morbidity and mortal-ity [77]. Inoperability might identify a patient group inwhom technical success would not be possible; for exam-ple, no vascular access. Different trials have used theseterms for patient enrollment; for example, the CoreValveTrial identifies extreme risk, whereas the PARTNER(Placement of AoRtic TraNscathetER Valve) Trial usedthe term inoperable. For this document, we prefer theterm prohibitive risk. This includes some patients in whomsurgery might be deemed unsuitable based on the phy-sician’s assessment of the patient’s risk for surgery;whereas in others, the surgeon may decide that theoperation cannot be performed successfully because oftechnical considerations. Assessment of inoperability isalso driven by surgeon and institutional experience andthus varies. The incidence of patients undergoing AVRwith an STS predicted risk of mortality �5% is low butvary significantly amongst institutions and may be re-lated to volume and referral patterns. Experience withsuch patients is pivotal for TAVR teams. Referral to suchteam and another opinion/consultation is crucial beforedeeming a patient inoperable. Whereas practice guide-lines have been developed to assist physicians and sur-geons in determining appropriate use of treatmentoptions [29, 63], there are, however, no specific recom-mendations for defining inoperability. Current ACCF/AHA guidelines acknowledge that special consider-ations are required for the management of advancedelderly patients with AS, since age-related and comor-bid conditions commonly exist in patients in their 80sand 90s even though AVR is technically feasible evenin this group [67, 78].
In the absence of literature evidence and guidelinesrecommendations, the determination of inoperability inany given patient depends on the judgment of the med-ical team. It is generally agreed that patients with limitedlife expectancy due to concurrent conditions such asmalignancy, dementia, primary liver disease, chronicobstructive pulmonary disease (COPD), among others,are not appropriate for AVR. Frailty and related con-ditions of debility and deconditioning are known toresult in inability to recover from major heart surgerysuch as AVR, despite operative survival and hospitaldischarge [65]. These conditions can potentially con-tribute to increased surgical mortality and morbidity in
the elderly [79].
1347Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
Inoperability from the surgeon’s judgment may resultfrom technical considerations that preclude safe perfor-mance of AVR, such as prior mediastinal irradiation,porcelain aorta or severe periannular calcification, severeaortic atheromatous disease, prior cardiac operations,among others including the internal mammary arterycrossing the midline. Although infrequent, aortic valvebypass with a LV apex-to-descending aortic conduit hasbeen used in some patients with severe AS judged to beinoperable via a mediastinal approach and cardiopulmo-nary bypass [80].
In summary, a substantial percentage of patients withAS are judged to be inoperable for surgery based primar-ily on the physician’s or surgeon’s determination ofoperative risk and survivability. Although some patientsmay be found to be inoperable for technical and surgicalreasons, most inoperable patients are felt to be too illfrom associated comorbid conditions.
3.2. Alternatives to AVR3.2.1. MEDICAL THERAPY. There are no proven medical treat-ments to prevent or delay the disease process in theaortic valve leaflets. However, evaluation and modifica-tion of cardiac risk factors is important in patients withaortic valve disease to prevent concurrent coronary ar-tery disease (CAD). The association of AS with riskfactors similar to those associated with atherosclerosis [5,6] had suggested that intervention may be possible toslow or prevent disease progression in the valve leaflet[81, 82], but prospective, randomized, placebo-controlledtrials failed to demonstrate a benefit of statins in reduc-ing the progression of aortic valve stenosis.
Longer-term palliative medical management of symp-tomatic AS may be appropriate for patients who areeither not candidates for aortic valve surgery due tocomorbidities or in patients who refuse AVR. The overallgoal of medical therapy is to treat coexisting cardiovas-cular conditions, and treat superimposed diseases thatoften exacerbate the disease process. Patients should beeducated about the effects of sodium intake, change inweight, and other factors that may lead to clinical decom-pensation. Medical therapy should be judicious andinclude treating concurrent cardiovascular conditionssuch as correction of anemia and fever, and preventativemeasures such as pneumococcal or influenza vaccina-tion. Given the severe hypertrophy, optimizing hemody-namics by maintaining sinus rhythm may help withsymptom stabilization.
Even with optimal care, adults with severe symptom-atic inoperable AS will have exacerbations of symptomsand frequent hospitalizations. Palliative care should in-clude end-of-life discussions and counseling as appropri-ate. Counseling is also indicated regarding true risk ofAVR, and the importance of accurate risk predictioncannot be overemphasized. Many patients may refusesurgery based on misunderstood operative risk.3.2.2. BALLOON AORTIC VALVULOPLASTY. First reported in 1986[83], balloon aortic valvuloplasty was considered to be a
less invasive and safe alternative to AVR, particularly inhigh surgical risk patients with multiple medical comor-bidities. Although balloon aortic valvuloplasty results inimmediate hemodynamic improvement with a signifi-cant decrease in transvalvular gradients resulting inlarger valve area, it does not result in sustained clinicalimprovement because of high recurrence rates; resteno-sis or recoil of the aortic valve usually occurs within 6months. Patients treated with balloon aortic valvulo-plasty alone have shown poor prognosis, with survivalrates of 50% at 1 year, 35% at 2 years, and 20% at 3 years[15,84–86]. In addition, serious complications due toballoon aortic valvuloplasty occur in 15% to 25% ofpatients [84, 87, 88]. Balloon aortic valvuloplasty, there-fore, should not be used as a substitute for AVR inpatients who are candidates for surgical AVR. Even as apalliative treatment, balloon aortic valvuloplasty datasuggest that there is much uncertainty regarding im-proved longevity or quality of life after the procedurewith a mean duration of symptom improvement of only 1year [63, 89]. There has been no significant difference inlong-term survival demonstrated between patients un-dergoing balloon aortic valvuloplasty and those under-going medical therapy alone [86]. Although balloon aorticvalvuloplasty as a stand-alone treatment is not recom-mended [63, 87, 88], it may still be used in contemporarypractice as a bridge to subsequent AVR (both Class IIb,Level of Evidence C recommendation) [28, 84, 90]. In thecurrent era of TAVR, there has been increased interest inballoon aortic valvuloplasty. In this setting, balloon aorticvalvuloplasty may be used to assess whether there is initialclinical improvement, in which case, then the patient maybe a candidate for TAVR.
4. Transcatheter Aortic Valve Replacement
4.1. Background and HistoryGiven the increased mortality and morbidity of AVRsurgery for high-risk patients and the poor long-termresults of balloon aortic valvuloplasty, there has beeninterest in the development of a percutaneously deliv-ered aortic heart valve [91]. As early as 1992, investigatorsevaluated stent-based porcine bioprostheses delivered tovarious aortic sites in animal models [92]. This early workculminated in 2000 with implantation of a percutaneousheart valve in a 12-year-old patient with a failing rightventricular to pulmonary arterial conduit that had beenplaced 8 years previously for the treatment of pulmonaryatresia and ventricular septal defect. This initial seminalexperience was followed in 2002 by the first human TAVRusing the antegrade approach to implant a balloon ex-pandable equine pericardial leaflet stent valve [93]. Sincethat early experience, there have been multiple iterationsand a number of new designs.
4.2. Device DescriptionAt the present time, the most data available for TAVRare based upon 2 specific devices—the Sapien valve(Figure 1) Edwards Life Sciences, Inc., Irvine, CA) and the
CoreValve (Figure 2) (Medtronic, Inc., Minneapolis, MN).
1348 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
The most recent iteration of the former is a trileafletbovine pericardial valve mounted with a tubular slottedballoon-expandable stent composed of a cobalt chromiumalloy. The Sapien valve is available in 23-mm and 26-mmsizes in the United States and 23-mm, 26-mm, and 29-mmsizes in Europe. The initial devices required a 22- or24-French sheath for delivery of the prosthesis. Recentiterations (NovaFlex) have decreased this to 18-French. Thefirst and second generations of this device have been testedin randomized controlled trials for both transfemoral andtransapical implantation.
The second device (CoreValve) is comprised of 3 por-cine pericardial tissue leaflets mounted in a self-expanding nitinol frame. It is available in 3 sizes—26 mm,29 mm, and 31 mm. This valve has also continued toiterate, with the initial devices being 25-French, but now18-French delivery sheaths are used. This valve has onlybeen used by a retrograde approach—either via trans-femoral, subclavian, or direct aortic access.
A wide range of new devices has been tested withsome first-in-man experiences. These devices have beencharacterized by smaller size, the ability to reposition oreven recapture the device after deployment if an opti-mized device position is not obtained initially, and,modular prosthetic elements to design in situ moreoptimal conformance to the natural valve and aorticannulus among others.
Specific anatomic issues must be considered in devicedesign. These include the rigid structure of the pattern ofvalvular calcification and aortic annulus, and the need foras full apposition as possible to the annulus in an attemptto minimize periprosthetic leak which, given sometimeseccentric, bulky calcification, may be difficult. The closeproximity to the coronary ostia, the width and height ofthe sinuses, the membranous ventricular septum withthe His bundle and the anterior leaflet of the mitral valve
Fig 1. Sapien Valve.Source: Edwards Lifesciences.
are also important anatomical considerations. In addi-
tion, the size and degree of severity of peripheral arterialdisease are all factors that could limit catheter size. Otherissues include avoidance of central prosthetic leak, leafletdurability, hemodynamic performance, ability to treatboth tricuspid and bicuspid valve anatomy, surfacesdesigned to minimize thrombogenicity, and the need tooptimally position the devices and retrieve and reposi-tion when necessary [94].
Fundamental issues for all current and future devicesare hemodynamic results, valve durability, and residualor new aortic regurgitation (AR). The initial hemody-namic performance of TAVR valves must be similar orsuperior to that obtained with surgical AVR. This iscrucial because high residual transprosthetic gradientsresult in less symptomatic improvement and poorerregression of left ventricular mass [95]. These transpros-thetic gradients are a function of prosthetic size as well asthe specific type of prosthesis and can result in patient–prosthesis mismatch. Typical immediate postproceduralgradients after surgical AVR range from 8 mm Hg to 12mm Hg, whereas the AV area or effective orifice area(EOA) ranges from 1.4 to 1.9 cm2. As documented belowin the PARTNER trial, the valve hemodynamics of theTAVR early on are approximately 10% better than thespecific surgical aortic prostheses used in that trial.
There are only limited clinical data on the durability ofTAVR valves—up to 2 years—in the PARTNER trial andup to 5 years in other registry experiences. Although theabsolute number of patients is small, there have been noreports of structural valve deterioration. The fundamen-tal clinical need for durability may depend in part on thespecific patient population. In the PARTNER trial, themean age at implant was 83 years, and serious comor-bidities were frequent. In this setting, the need for dura-bility of 20 years is less important than if the patientselection criteria are broadened to include patients in theirearly to mid 60s who have isolated AS without comorbidconditions. In this latter group, the TAVR valve must have
Fig 2. CoreValve.The Medtronic CoreValve System is currently limited to investiga-
tional use in the United States. Source: Medtronic, Inc.
ittees
1349Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
at least equivalent clinical durability to currently availablesurgically implanted valves.
4.3. Current State of the Evidence4.3.1. REGISTRY EXPERIENCE. Registry data provide importantinformation for assessing the role of TAVR in a large numberof patients who are not eligible for randomized controlledtrials because of strict selection criteria. Several multicenterregistries, including Edwards Lifesciences and Medtronic Cor-eValve (Tables 1 and 2), have reported early and late outcomeswith TAVR. However, patient selection criteria varied
Table 1. Edwards Sapien Transcatheter Heart Valve Registrie
Characteristic
REVIVE, REVIVAL,PARTNER EU
(N�222)
SOURegist
(N�
DemAge (y) 83 82Female (%) 55 56EuroSCORE (mean, %) 26 24NYHA functional class III/IV (%) 89 76Aortic valve area (cm2) 0.59 0Mean gradient (mm Hg) 45 49Prior CABG (%) 26 15Ejection fraction (%) 51 52
Ou30-day mortality (%) 10.4 71-y mortality (%) 24 18Stroke (%) 3.3 3Major vascular complications (%) 27.9 11Permanent pacemaker (%) 1.8 6
CABG � coronary artery bypass graft; NR � not reported; NYHA
Data are derived from the Edwards Lifesciences briefing document for themeeting on TAVR on July 21, 2011 (http://www.fda.gov/AdvisoryCommCommittee/CirculatorySystemDevicesPanel/ucm240575.htm).
Table 2. Medtronic CoreValve Transcatheter Heart Valve Reg
Characteristic
Tamburinoet al. [109](N�663)
Milan[107]
(N�61)
Fr[
(N
DemAge (y) 82 79Female (%) 56 47EuroSCORE (mean, %) 23 26.6NYHA functional class III/IV (%) 71.5 69Mean gradient (mm Hg) 52 54
OuProcedural success (%) 98 98.430-day mortality (%) 5.9 2.21-y mortality (%) 15 18.4*Stroke (%) 2.5 2.2Major vascular complications (%) 2.0 21.3Permanent pacemaker (%) 19.1 26.1
* 6-month survival. ** 2-year survival.
N � number; NR � not reported; NYHA � New York Heart Associati
amongst the different registries; standardized definitions forclinical events such as those described by the Valve AcademicResearch Consortium (VARC) [96] were not used; and end-points were not prospectively adjudicated using a blindedclinical event committee.
CoreValve system real-world clinical experience to dateis comprised of multiple registries from several participat-ing national sites [97, 105–110, 115]. These study sizes rangefrom 61 to 663 patients, with a combined clinical patientexperience of nearly 2,350 patients that includes follow-upof up to 2 years. (See Table 2 for details.)
F) France Registry(N�1,137)
Belgium Registry(N�303)
Canada Registry (TF)(N�162)
hics83 83 8349 46 4423 29 2675 80 93
0.67 0.60 0.6348 47 4819 20 3053 50 55
es7.8 8 9.5NR NR NR3.5 5.0 3.0
11.3 NR 13.18.5 4.0 3.6
ew York Heart Association; TF � transfemoral.
Food and Drug Administration (FDA) Circulatory Devices Advisory Panel/CommitteesMeetingMaterials/MedicalDevices/MedicalDevicesAdvisory
s
Spanish[97]
(N�108)
UK/Ireland[108]
(N�288)UK [115](N�452)
German[110]
(N�588)
Buellesfeldet al. [105](N�126)
hics78.6 81 81.3 81.4 81.954.6 NR 48 55.8 57.116 22 18.1 20.8 23.458.4 74 73.9 88.2 74.655 NR NR 48.7 46.8
es98.1 97.5 98.2 NR 72.67.4 4.7 5.8 12.4 15.2
17.7 NR 21.7 NR 38.1**0.0 4.2 4.0 2.8 NR5.6 9.0 6.2 4.0 NR
35.2 26 24.4 42.5 26.2
s
RCEry (T920)
ograp
.70
tcom.5.9.5.3.7
� N
U.S.
istrie
ench106]�66)
ograp82.551.524.774.646tcom
92.615.1NR4.57.5
25.7
on.

1350 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
4.3.1.1. Demographics. Tables 1 and 2 summarize themajor patient characteristics for the Sapien and Cor-eValve family of registries, respectively. The patientsselected for entry are elderly (average age typically over80 years), with symptomatic severe AS (mean gradient�45 mm Hg), significant comorbidities, and an averageEuroSCORE of �23 (Sapien) and �16 (CoreValve)[97,105–110], indicating a significant risk with conven-tional AVR. However, unlike the PARTNER trial, all ofthese registries used the EuroSCORE risk predictionsystem for defining high risk and inoperability. Euro-SCORE is generally not regarded as valid in high-riskpatients for surgical AVR, and surgeon input as to oper-ability was not required in these registries. As a result,the registry results are difficult to interpret because it isunclear whether the patients who were enrolled in theseregistries were truly “inoperable” versus “high-risk”[110, 111].4.3.1.2. Outcomes.4.3.1.2.1. Procedural Success and Hazards. In theSOURCE (SAPIEN Aortic Biosprosthesis European Out-come) registry, procedural success rate (defined as 1valve implanted, AR �2�, and patient left procedureroom alive) was 93% for transfemoral TAVR and 92% fortransapical TAVR. The procedural success rate reportedfor CoreValve is �92% except for 1 study that enrolledvery high-risk patients [105]. Significant variations be-tween registries were not observed in terms of deploy-ment, relief of obstruction and avoidance of significantAR [110, 111].4.3.1.2.2. Early and Late Morbidity and Mortality. Theearly and late major outcomes with Sapien and Cor-eValve registries are summarized in Tables 1 and 2. Theearly morbidity of TAVR includes strokes, coronary oc-clusion, pacemaker implantation, vascular complica-tions, renal failure, cardiac rupture and tamponade,bleeding, aortic dissection, and death. The overall riskof any 30-day major complication ranges from 20% toover 40%. Early mortality ranges from an in-hospitalrate of 5% to 8% and a 30-day mortality rate from 8% to10%. In the SOURCE registry, the incidence of a majorbleeding event was significantly greater among patientsundergoing transapical versus transfemoral TAVR (3.9% vs.2.3%), whereas the incidence of vascular access-relatedcomplications was significantly higher among patients hav-ing transfemoral TAVR (major—11.3% vs. 2.0%; minor—10.4% vs. 1.0%) [110–114].
Permanent pacemaker placement is reported in be-tween 1.8% up to 8.5% of patients with Sapien and 19.1%to 42.5% with the CoreValve; renal failure in under 3%;and stroke in 1% to 5%. Registry data reflect an overallmortality rate at 1 year of 19% to 24%. In the SOURCEregistry, more than half (51.6%) of deaths up to 1 year hada noncardiac etiology and were related to baseline comor-bidities [110, 111].
The recent UK TAVR Registry included 452 MedtronicCoreValve implantations [115]. In this group, standard-ized data forms were used and audited. Procedural
success was achieved in 98.2% in this high-risk group ofpatients who had a baseline logistic EuroSCORE of18.1%. Thirty-day mortality was 5.8%, and 1- and 2-yearmortality was 21.7% and 23.9%, respectively. In-hospitalstroke occurred in 4% of patients and myocardial infarc-tion in 1.1%. A permanent pacemaker was required in24.4% (compared with 7.4% with Sapien). Rates of mod-erate to severe postimplant AR were 17.3% (comparedwith 9.6% with Sapien). Mortality rates at all time pointswere significantly lower among patients treated via atransfemoral route as compared with nontransfemoralroutes (�85% transapical). In this study, LV function, thepresence of moderate/severe AR, and COPD, but notvascular access site, were independent predictors ofmortality.4.3.1.2.3. Quality of Life in Registries. Quality of life is akey patient-centered outcome. Although death is the lowestpossible functional status, for many, survival marked byreduced physical function or independence may be worsethan death. The PARTNER EU Registry is a multicenterstudy of the early European experience in TAVR. Patientsundergoing TAVR by transapical or transfemoral approachwere followed to 12 months for symptoms by New YorkHeart Association (NYHA) functional class, and heart fail-ure–related quality of life as assessed by the Kansas CityCardiomyopathy Questionnaire [116]. All patients im-proved, with no significant differences in NYHA functionalclass improvement noted between transapical or trans-femoral approaches.
Several single-center registries have added additionalinformation on quality of life using disease-specific orgeneral surveys (Short Form-36 Health Questionnaire,Short Form-12 Health Questionnaire, Kansas City Car-diomyopathy Questionnaire, Minnesota Living withHeart Failure Questionnaire) and on symptoms (NYHAfunctional class, and 6-minute walk). Improvements fol-lowing TAVR in vitality, physical functioning, and generaland mental health scores have been identified with physicalfunction demonstrating the greatest improvement. Patientswho do not experience improvement are more likely tohave comorbidities that contribute to continued symptomsand impair quality of life, such as COPD and reduced EF(Table 3).4.3.1.2.4. Learning Curve. Each registry has identified aprocedural learning curve, but the exact definition of thiscurve and a clear method to decrease it are not yet clearlyreported. This curve has important components such aspatient selection, anesthesia, improvement in the equip-ment over time, and technical decision making regardingvalve deployment. The SOURCE registry enrolled 1,038(Cohort 1) and 1,306 patients (Cohort 2) undergoingTAVR procedures over 2 sequential years. Age andEuroSCORE were not significantly different between the2 cohorts. Compared with the first year of experience,valve malposition (1.6% vs. 1.2%), and vascular accesscomplications (2.1% vs. 1.8%) were not significantly lowerin the second year. However, reductions in the rates ofpostprocedure AR �2� (4.5% vs. 2.1%, p�0.011) andconversion to open surgery (3.7% vs. 1.5%, p�0.0315)
were improved [110, 111, 121]. Overall 30-day and 1-year
life;T
1351Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
survival was similar in both cohorts despite higher num-ber of patients with heart failure and mitral regurgitationenrolled in Cohort 2.
In summary, the registries demonstrate in high-riskpatients that TAVR may be deployed with a high degreeof procedural success, predictable risk of stroke, device-dependent high risk of pacemaker implantation (partic-ularly with CoreValve), and a 30-day mortality rate thatseems potentially acceptable in a debilitated and illpatient population. Importantly, TAVR seems to alleviateAS to a similar degree as surgical AVR and patients tendto return to Class I or II symptoms with substantialimprovements in quality of life.
Future registries should be designed to include con-temporary (i.e., VARC) definitions of procedural andquality-of-life outcomes and utilize an independent clin-ical events committee when possible to standardize eventreporting. Longer-term follow-up studies are needed todemonstrate the continued durability of TAVR in thehigh-risk and inoperable patients.4.3.2. RANDOMIZED CONTROLLED TRIAL.
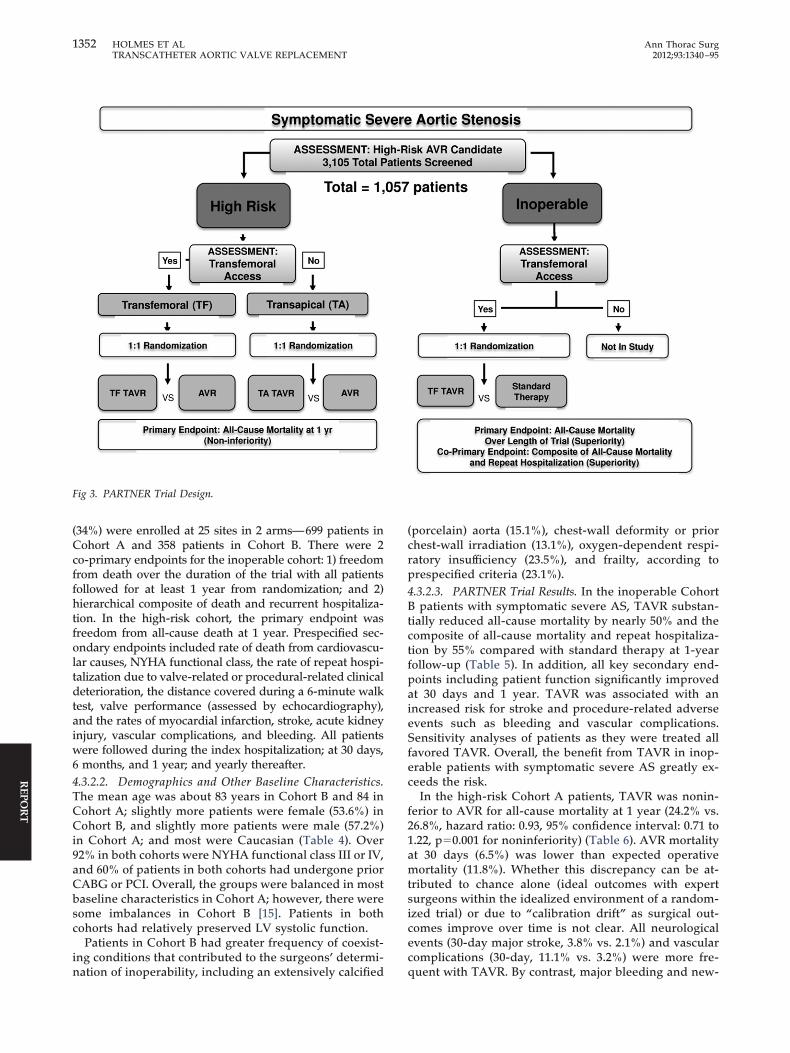
4.3.2.1. PARTNER Trial Design. The PARTNER trial (Fig-ure 3) was a prospective, unblinded, randomized, con-
Table 3. Quality of Life and Symptom Assessment in TAVR R
Study Population NYHA Functional Class 6-Mi
PARTNER EU Registry;Lefevre et al.(Multicenter; N�130Sapien) [116]
Improved class at 1 year in84.5% of patients (85%NYHA functional classIII/IV at baseline, 15%NYHA functional classat 1 year); changes notedat 30 days weresustained
Buellesfeld et al.(Multicenter; N�126CoreValve) [105]
Improved in 80% at 30days; 74% at 2 years (in50% by 1 level, in 20%by 2 or more levels)
Krane et al. (Single-centerregistry; N�99 TAVR)[117]
More class I/II at 3 months(NYHA functional classIII/IV from 98% to 2% at3 months)
Ussia et al. (Single-centerregistry; N�57 TAVR)[118]
More class I/II (average 1.8NYHA functional classimprovement) at 5months (p�0.001)
Bekeredjian et al. (Single-center registry; N�87TAVR) [119]
Improved class (average of1.7 NYHA functionalclass improvement) at6 months (p�0.001)
Gotzmann et al. (Single-center registry; N�44TAVR) [120]
Decrease of percentage ofNYHA functional classIII/IV from 90% to 16%at 30 days
Imprtimday
BNP � brain natriuretic peptide; EQ-5D � EuroQol Five DimenQuestionnaire; LOS � length of stay; MLHFQ � Minnesota LivinYork Heart Association; PF � physical function; QOL � quality ofHealth Questionnaire; SF-36 � Short Form 36 Health Questionnaire;
trolled, multicenter pivotal trial evaluating the safety and
effectiveness of the Edwards Sapien THV transcatheteraortic valve; 2 distinct populations were enrolled—inoperable, or Cohort B, and high-risk operable, or Co-hort A. Potential candidates were presented on a nationalconference call for approval for treatment. Randomiza-tion was stratified based on operability for AVR surgeryand within cohorts by vascular access for transfemoraldelivery. Patients who were considered high surgical riskand eligible for transfemoral access were stratified intoCohort A and randomized to treatment (transfemoralAVR) or control (surgical AVR). Cohort A patients whowere not eligible for transfemoral access were evaluatedas candidates for transapical delivery and, if appropriate,randomized to treatment (transapical AVR) or control(surgical AVR). Nonsurgical candidates were stratifiedinto Cohort B and randomized to treatment (transfemoralAVR) or control (“standard” therapy). Inoperability wasformally defined as “�50% predicted probability of mor-tality or serious irreversible complication by 30 days by 1cardiologist and 2 cardiothoracic surgeons” [15]. Cohort Bpatients who did not meet the criteria for transfemoraldelivery were not enrolled in the study because transapi-cal delivery was deemed too risky in Cohort B (Figure 3).
tries
Walk Questionnaire Other
KCCQ improvement at 1 yearin 72.7% (p�0.0002)
Small improvement inEQ-5D was notsignificant
NR NR
Improved SF-36 PF generalhealth and vitality pre/postat 3 months (all p�0.01).No change mental health.
85% would do TAVRagain
SF-12; Improved (p�0.001)physical and mentalcomponent scores, return topopulation norms, greatestchange in PF
NR
SF-36 Improved physical andmental component scores,greatest change in PF
70% average decreasein NT-proBNPlevels of 4,000 ng/L(p�0.0001)
walk30
MLHFQ; Improved HF-related QOL
Lower averagedecrease in BNPlevels of 400 pg/mL(p�0.005) and 25%increase in 6-minutewalk time (p�0.005)
; HF � heart failure; KCCQ � Kansas City CardiomyopathyHeart Failure Questionnaire; NR � not reported; NYHA � New
SAVR � surgical aortic valve replacement; SF-12 � Short Form 12AVR � transcatheter aortic valve replacement.
egis
nute
NR
NR
NR
NR
NR
ovede ats
sionsg with
Of the 3,105 patients screened, a total of 1,057 subjects
1352 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
(34%) were enrolled at 25 sites in 2 arms—699 patients inCohort A and 358 patients in Cohort B. There were 2co-primary endpoints for the inoperable cohort: 1) freedomfrom death over the duration of the trial with all patientsfollowed for at least 1 year from randomization; and 2)hierarchical composite of death and recurrent hospitaliza-tion. In the high-risk cohort, the primary endpoint wasfreedom from all-cause death at 1 year. Prespecified sec-ondary endpoints included rate of death from cardiovascu-lar causes, NYHA functional class, the rate of repeat hospi-talization due to valve-related or procedural-related clinicaldeterioration, the distance covered during a 6-minute walktest, valve performance (assessed by echocardiography),and the rates of myocardial infarction, stroke, acute kidneyinjury, vascular complications, and bleeding. All patientswere followed during the index hospitalization; at 30 days,6 months, and 1 year; and yearly thereafter.4.3.2.2. Demographics and Other Baseline Characteristics.The mean age was about 83 years in Cohort B and 84 inCohort A; slightly more patients were female (53.6%) inCohort B, and slightly more patients were male (57.2%)in Cohort A; and most were Caucasian (Table 4). Over92% in both cohorts were NYHA functional class III or IV,and 60% of patients in both cohorts had undergone priorCABG or PCI. Overall, the groups were balanced in mostbaseline characteristics in Cohort A; however, there weresome imbalances in Cohort B [15]. Patients in bothcohorts had relatively preserved LV systolic function.
Patients in Cohort B had greater frequency of coexist-ing conditions that contributed to the surgeons’ determi-
Fig 3. PARTNER Trial Design.
nation of inoperability, including an extensively calcified
(porcelain) aorta (15.1%), chest-wall deformity or priorchest-wall irradiation (13.1%), oxygen-dependent respi-ratory insufficiency (23.5%), and frailty, according toprespecified criteria (23.1%).4.3.2.3. PARTNER Trial Results. In the inoperable CohortB patients with symptomatic severe AS, TAVR substan-tially reduced all-cause mortality by nearly 50% and thecomposite of all-cause mortality and repeat hospitaliza-tion by 55% compared with standard therapy at 1-yearfollow-up (Table 5). In addition, all key secondary end-points including patient function significantly improvedat 30 days and 1 year. TAVR was associated with anincreased risk for stroke and procedure-related adverseevents such as bleeding and vascular complications.Sensitivity analyses of patients as they were treated allfavored TAVR. Overall, the benefit from TAVR in inop-erable patients with symptomatic severe AS greatly ex-ceeds the risk.
In the high-risk Cohort A patients, TAVR was nonin-ferior to AVR for all-cause mortality at 1 year (24.2% vs.26.8%, hazard ratio: 0.93, 95% confidence interval: 0.71 to1.22, p�0.001 for noninferiority) (Table 6). AVR mortalityat 30 days (6.5%) was lower than expected operativemortality (11.8%). Whether this discrepancy can be at-tributed to chance alone (ideal outcomes with expertsurgeons within the idealized environment of a random-ized trial) or due to “calibration drift” as surgical out-comes improve over time is not clear. All neurologicalevents (30-day major stroke, 3.8% vs. 2.1%) and vascularcomplications (30-day, 11.1% vs. 3.2%) were more fre-
quent with TAVR. By contrast, major bleeding and new-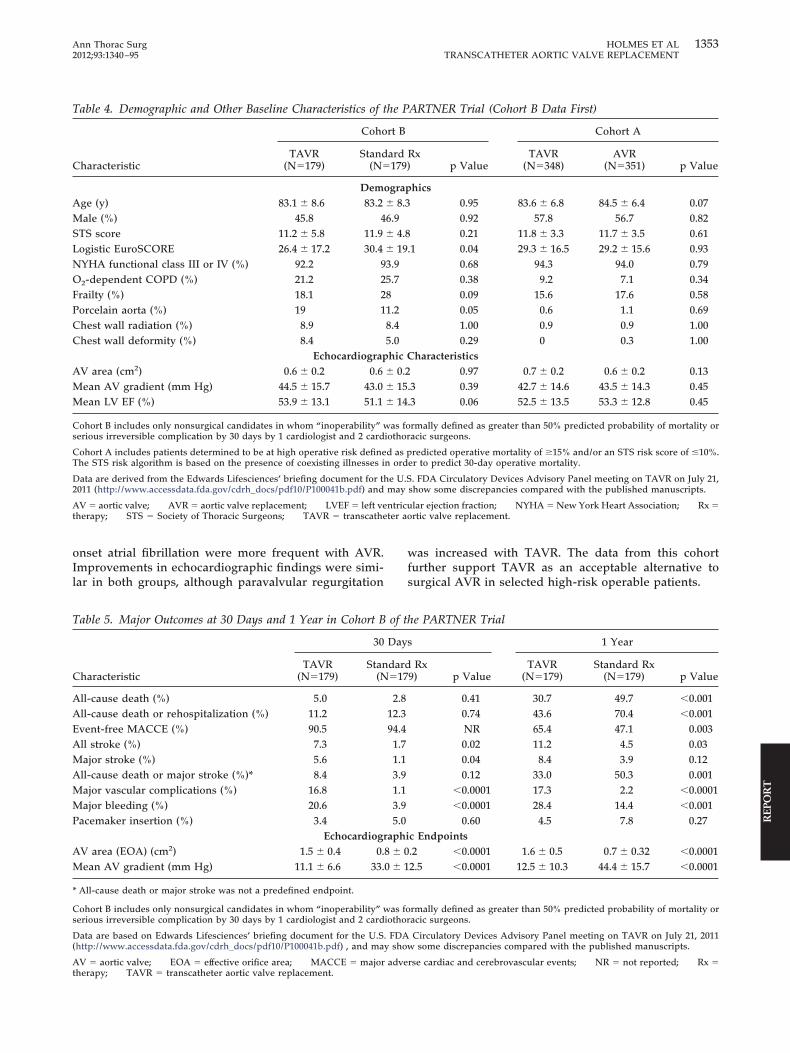
ntricuter a
1353Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
onset atrial fibrillation were more frequent with AVR.Improvements in echocardiographic findings were simi-lar in both groups, although paravalvular regurgitation
Table 4. Demographic and Other Baseline Characteristics of
Characteristic
Coho
TAVR(N�179)
Stand(N�
DemAge (y) 83.1 � 8.6 83.2Male (%) 45.8 4STS score 11.2 � 5.8 11.9Logistic EuroSCORE 26.4 � 17.2 30.4NYHA functional class III or IV (%) 92.2 9O2-dependent COPD (%) 21.2 2Frailty (%) 18.1 2Porcelain aorta (%) 19 1Chest wall radiation (%) 8.9Chest wall deformity (%) 8.4
EchocardiograpAV area (cm2) 0.6 � 0.2 0.6Mean AV gradient (mm Hg) 44.5 � 15.7 43.0Mean LV EF (%) 53.9 � 13.1 51.1
Cohort B includes only nonsurgical candidates in whom “inoperability”serious irreversible complication by 30 days by 1 cardiologist and 2 card
Cohort A includes patients determined to be at high operative risk defineThe STS risk algorithm is based on the presence of coexisting illnesses i
Data are derived from the Edwards Lifesciences’ briefing document for t2011 (http://www.accessdata.fda.gov/cdrh_docs/pdf10/P100041b.pdf) and
AV � aortic valve; AVR � aortic valve replacement; LVEF � left vetherapy; STS � Society of Thoracic Surgeons; TAVR � transcathe
Table 5. Major Outcomes at 30 Days and 1 Year in Cohort B
Characteristic
30
TAVR(N�179)
Stan(N
All-cause death (%) 5.0All-cause death or rehospitalization (%) 11.2Event-free MACCE (%) 90.5All stroke (%) 7.3Major stroke (%) 5.6All-cause death or major stroke (%)* 8.4Major vascular complications (%) 16.8Major bleeding (%) 20.6Pacemaker insertion (%) 3.4
EchocardiogAV area (EOA) (cm2) 1.5 � 0.4 0.Mean AV gradient (mm Hg) 11.1 � 6.6 33.
* All-cause death or major stroke was not a predefined endpoint.
Cohort B includes only nonsurgical candidates in whom “inoperability”serious irreversible complication by 30 days by 1 cardiologist and 2 card
Data are based on Edwards Lifesciences’ briefing document for the U.S(http://www.accessdata.fda.gov/cdrh_docs/pdf10/P100041b.pdf) , and ma
AV � aortic valve; EOA � effective orifice area; MACCE � major advetherapy; TAVR � transcatheter aortic valve replacement.
was increased with TAVR. The data from this cohortfurther support TAVR as an acceptable alternative tosurgical AVR in selected high-risk operable patients.
ARTNER Trial (Cohort B Data First)
Cohort A
Rxp Value
TAVR(N�348)
AVR(N�351) p Value
hics0.95 83.6 � 6.8 84.5 � 6.4 0.070.92 57.8 56.7 0.820.21 11.8 � 3.3 11.7 � 3.5 0.61
.1 0.04 29.3 � 16.5 29.2 � 15.6 0.930.68 94.3 94.0 0.790.38 9.2 7.1 0.340.09 15.6 17.6 0.580.05 0.6 1.1 0.691.00 0.9 0.9 1.000.29 0 0.3 1.00
haracteristics0.97 0.7 � 0.2 0.6 � 0.2 0.13
.3 0.39 42.7 � 14.6 43.5 � 14.3 0.45
.3 0.06 52.5 � 13.5 53.3 � 12.8 0.45
rmally defined as greater than 50% predicted probability of mortality oracic surgeons.
redicted operative mortality of �15% and/or an STS risk score of �10%.er to predict 30-day operative mortality.
. FDA Circulatory Devices Advisory Panel meeting on TAVR on July 21,show some discrepancies compared with the published manuscripts.
lar ejection fraction; NYHA � New York Heart Association; Rx �ortic valve replacement.
he PARTNER Trial
s 1 Year
Rx9) p Value
TAVR(N�179)
Standard Rx(N�179) p Value
0.41 30.7 49.7 �0.0010.74 43.6 70.4 �0.001NR 65.4 47.1 0.0030.02 11.2 4.5 0.030.04 8.4 3.9 0.120.12 33.0 50.3 0.001
�0.0001 17.3 2.2 �0.0001�0.0001 28.4 14.4 �0.001
0.60 4.5 7.8 0.27c Endpoints.2 �0.0001 1.6 � 0.5 0.7 � 0.32 �0.00012.5 �0.0001 12.5 � 10.3 44.4 � 15.7 �0.0001
rmally defined as greater than 50% predicted probability of mortality oracic surgeons.
Circulatory Devices Advisory Panel meeting on TAVR on July 21, 2011w some discrepancies compared with the published manuscripts.
the P
rt B
ard179)
ograp� 8.36.9� 4.8� 193.95.781.28.45.0hic C
� 0.2� 15� 14
was foiothor
d as pn ord
he U.Smay
of t
Day
dard�17
2.812.394.41.71.13.91.13.95.0
raphi8 � 00 � 1
was foiothor
. FDAy sho
rse cardiac and cerebrovascular events; NR � not reported; Rx �

tive o
1354 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
Of note, the 30-day mortality (generally thought to beprocedure-related) in Cohort A (3.4%) and Cohort B (5.0%)was lower than the published SOURCE registry mortality(8.5%), despite a relatively lower-risk patient populationenrolled in the latter (1-year mortality of 30.7% in Cohort B,22.2% in Cohort A, and 18.9% in SOURCE). This arguablyraises questions about the generalizability of the random-ized trial data to clinical practice.4.3.2.3.1. Quality of Life. The quality-of-life results fromCohort B arm, the inoperable cohort, TAVR patients hadimprovement in the 6-minute walk performance com-pared with baseline (p�0.002), whereas standard therapypatients did not (p�0.67) [15]. In addition, TAVR patientswere less symptomatic (New York Heart Associationclass), had reduced hospitalization stay, and improvedphysical functioning compared with standard therapy. Inthe high-risk cohort, both New York Heart Association
Table 6. Major Outcomes at 30 Days and 1 Year in Cohort A
Characteristic
30 Day
TAVR(N�348)
Surgical A(N�35
ClinicaAll-cause death (%) 3.4 6.5All-cause death or rehospitalization (%) 7.2 9.7All stroke (%) 5.5 2.4Major stroke (%) 3.8 2.1All-cause death or major stroke (%)* 6.9 8.2Major vascular complications (%) 17.0 3.8Major bleeding (%) 9.3 19.5Atrial fibrillation (%) 8.6 16.0Pacemaker insertion (%) 3.8 3.6
EchocardiogAV area (EOA) (cm2) 1.7 � 0.5 1.5 � 0Mean AV gradient (mm Hg) 9.9 � 4.8 10.8 � 5
* All-cause death or major stroke was not a predefined endpoint.
Cohort A includes patients determined to be at high operative risk defineThe STS risk algorithm is based on the presence of coexisting illnesses i
AV � aortic valve; AVR � aortic valve replacement; EOA � effec
Table 7. Quality of Life and Symptom Assessment in TAVR T
Study Population NYHA Functional Class 6-Minu
PARTNER B (Trial)TAVR vs.placebo(multicenter;N�358) [15, 122]
More class I, II with TAVRat 1 year (74.8% vs.42.0%)
TAVR imptime preyear; nono-TAV
PARTNER A (Trial)TAVR vs. SAVR(multicenter;N�699) (124)
More class I, II with TAVRat 30 days; No differencebetween TAVR andSAVR at 1 year
TAVR imptime at 3compareSAVR; NdifferencTAVR a1 year
HRQOL � health-related quality of life; KCCQ � Kansas City Cardreported; QOL � quality of life; SAVR � surgical aortic valve replacem
class and 6-minute walk test favored TAVR at 30 days,but the differences were not significant at 1 year. TAVRpatients had shorter index hospitalization length of stay(8 vs. 12 days, p�0.001). Quality of life as assessed bydisease-specific measures (Kansas City CardiomyopathyQuestionnaire [KCCQ]) and by general health-relatedquality of life (Short Form-12 Health Questionnaire)improved at 1, 6, and 12 months in the TAVR group andwere significantly higher than in the control arm(p�0.001). This supports that general and disease-specific quality of life are improved with TAVR to 1 yearover standard care among inoperable patients [122] (Ta-ble 7). The quality of life results from the Cohort A arm ofthe PARTNER trial were presented in November 2011.The preliminary conclusions were that among patientswith severe AS who were at high risk for standard valvereplacement, both surgical and transcatheter AVR re-
he PARTNER Trial
1 Year
p ValueTAVR
(N�348)Surgical AVR
(N�351) p Value
tcomes0.07 24.2 26.8 0.440.24 34.6 35.9 0.730.04 8.3 4.3 0.040.20 5.1 2.4 0.070.52 26.5 28.0 0.68
�0.01 18.0 4.8 �0.01�0.01 14.7 25.7 �0.01�0.01 12.1 17.1 0.07
0.89 5.7 5.0 0.68c Endpoints
0.001 1.6 � 0.5 1.4 � 0.5 0.0020.16 10.2 � 4.3 11.5 � 5.4 0.008
redicted operative mortality of �15% and/or an STS risk score of �10%.er to predict 30-day operative mortality.
rifice area; TAVR � transcatheter aortic valve replacement.
alk Questionnaire Other
d walkt at 1ge inup
KCCQ; Marked improvementwith TAVR at 1 year; SF12;improvement in physicaland mental HRQOL withTAVR
TAVR had fewerrehospitalizationsat 1 year
d walkysth
tweenVR at
NR Shorter LOS withTAVR
of t
s
VR1)
l Ou
raphi.4.0
d as pn ord
rials
te W
rove/poschan
R gro
rove0 dad wioe be
nd SA
iomyopathy Questionnaire; LOS � length of stay; NR � notent; TAVR � transcatheter aortic valve replacement.

1355Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
sulted in substantial improvement in disease-specificand generic health-related quality-of-life assessmentover 1-year follow-up, including KCCQ Summary Scale,SF-12 Physical, and SF-12 Mental tests. The benefits weregreater at earlier time points in the transfemoral TAVRgroup and were equivalent at 1 year [123].4.3.2.3.2. Continued-Access Protocol. Upon completion ofthe randomized PARTNER trial, patients have been al-lowed to have access to TAVR under a continued-accessprotocol. Enrollment in the randomized continued-access cohort was initiated following completion of theenrollment for PARTNER cohort B trial. From March toSeptember 2009, 91 inoperable patients were en-rolled—41 were randomized to TAVR and 50 to standardcare. Both short-term (30 days) and long-term (6 monthsto 1 year) results have been reported (http://www.fda.gov/downloads/AdvisoryCommittees/Committees-MeetingMaterials/MedicalDevices/MedicalDevicesAdvisoryCommittee/CirculatorySystemDevicesPanel/UCM262935.pdf). However, between-group analyseswere not conducted due to the small sample size. Enroll-ment in nonrandomized continued-access cohort wasinitiated in September 2009 after both cohorts of PART-NER had completed randomized enrollment. Over 600patients with transfemoral TAVR are being followedcurrently in this cohort.4.3.2.4. TAVR-Specific Clinical Issues.4.3.2.4.1. Stroke. Stroke is one of the major adverseevents associated with TAVR. Standardized criteria for
Table 8. Stroke
Stroke Diagnostic CriteriaRapid onset of a focal or global neurological deficit with at leas
hemiparesis, numbness or sensory loss affecting 1 side of tother neurological signs or symptoms consistent with strok
Duration of a focal or global neurological deficit �24 h; OR �2thrombolytic therapy or intracranial angioplasty); OR availthe neurological deficit results in death
No other readily identifiable nonstroke cause for the clinical prperipheral lesion, pharmacological influences)*
Confirmation of the diagnosis by at least 1 of the following:Neurology or neurosurgical specialistNeuroimaging procedure (MR or CT scan or cerebral angiogLumbar puncture (i.e., spinal fluid analysis diagnostic or intr
Stroke DefinitionsTransient ischemic attack:
New focal neurological deficit with rapid symptom resolutionNeuroimaging without tissue injury
Stroke: (diagnosis as above, preferably with positive neuroimagMinor—Modified Rankin score �2 at 30 and 90 days†Major—Modified Rankin score �2 at 30 and 90 days
* Patients with nonfocal global encephalopathy will not be reportedies. † Modified Rankin score assessments should be made by qualifiedthe 30- and 90-day Modified Rankin scores, a final determination of maclinical events committee.
CT � computed tomography; MR � magnetic resonance.
Reprinted with permission from Leon et al. [96].
the definition of stroke endpoints for TAVR clinical trials
have been published by the VARC (Table 8). The inci-dence of stroke depends on the assessment techniqueused for ascertainment. In the PARTNER Cohort A, therisk of clinically apparent “major” stroke defined asmodified Rankin score �2 was 3.8% at 30 days and 5.1%at 1 year among the TAVR group compared with 2.1%and 2.4%, respectively, in the surgical group [124]. In thePARTNER Cohort B, the stroke risk was 5% with TAVRcompared with 1.1% with standard therapy at 30 daysand 8.4% versus 3.9% at 1 year [15]. Using magneticresonance imaging-diffusion weighted imaging (MRI-DWI) studies, the incidence of cerebral ischemic lesionspost-TAVR has been reported to be as high as 68% to 84%in some studies, although clinically apparent stroke wasreported in �4% of cases [125–128]. Thus, the clinicalsignificance of these new CMR-defined lesions post-TAVR is not clear.
Most stroke cases are due to thromboembolism fromthe valve site or due to atherothrombotic emboli origi-nating from ulcerative plaque in the great vessels such asthe aortic arch. Such particles can be dislodged duringcatheter manipulation and embolize to the carotids orvertebrals to cause occlusions of distal intracerebral brancharteries. Other potential causes include hypotension asso-ciated with rapid ventricular pacing or hemodynamicinstability during the procedure, and rarely due to aorticdissection complicating TAVR. It is important to recog-nize that many patients who have AS may also haveother causes for an ischemic stroke such as age, hyper-
f the following: change in level of consciousness, hemiplegia,dy, dysphasia or aphasia, hemianopia, amaurosis fugax, or
f therapeutic intervention(s) were performed (e.g.,neuroimaging documents a new hemorrhage or infarct; OR
tation (e.g., brain tumor, trauma, infection, hypoglycemia,
)ial hemorrhage)
ally 1 to 2 h), always within 24 h
tudy)
troke without unequivocal evidence based upon neuroimaging stud-iduals according to a certification process. If there is discordance betweenrsus minor stroke will be adjudicated by the neurology members of the
t 1 ohe boe4 h, iable
esen
raphyacran
(usu
ing s
as a sindiv
jor ve
tension, diabetes, or other cardiac conditions, including

1356 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
atrial fibrillation, which is a potent risk factor for cardio-embolic stroke [69]. Differentiating the cause of the strokeis not always easy, but most trials and registries definestrokes within 30 days of an interventional procedure asattributable to the procedure. After 30 days, other comor-bid risk factors may account for stroke, which might,therefore, not be attributable to the prosthetic valve.Diagnostic evaluations are needed to assess the neck andcerebral vessels, cardiac function, and other potentialcauses of stroke in order to differentiate the strokesubtype and embark on the best treatment to prevent arecurrent stroke [129, 130]. Nearly two thirds of thestrokes related to TAVR at 1 year occurred within the first30 days in PARTNER Cohort B (13/20), suggesting thatmost events were likely procedure-related [15]. The inci-dence of stroke may lessen as patient selection becomesmore refined, delivery systems improve in their profile,and embolic protection devices and protocol-driven an-tithrombotic regimens are routinely used during TAVR.4.3.2.4.2. Conduction Defects. Atrioventricular conduc-tion disturbances after TAVR are associated with manypatient-related and procedural-related factors, includingpreoperative comorbid status, the degree and bulkinessof aortic valve and annular calcification, interventricularseptal thickness, pre-existing electrocardiogram abnor-malities, the depth of prosthesis implantation, and theprofile of the implanted prosthesis [131, 132]. Unlikeconventional AVR, where there may be localized traumadue to decalcification of the annulus and/or suture place-ment in the proximity of the AV node or the bundles,TAVR may cause conduction abnormalities through me-chanical impingement of the conduction system by theprosthesis.
The incidence of new left bundle-branch block andcomplete heart block after TAVR ranges from 14% to 83%and 19% to 22%, respectively. Patients with pre-existingright bundle-branch block may be at the highest risk forthe development of complete heart block and the needfor subsequent pacing [133]. The majority of conductionabnormalities occur prior to actual valve implantation,with 46% occurring during balloon aortic valvuloplasty,25% during balloon/prosthesis positioning and wire-crossing of the aortic valve, and the remaining 29%during prosthesis expansion [134]. The incidence of com-plete heart block requiring permanent pacemaker im-plantation has been higher with the CoreValve (19.2% to42.5%) than with the Sapien valve (1.8% to 8.5%), poten-tially due to its larger profile and extension low into theLV outflow tract. In the most recent UK Registry, pace-makers were implanted in 24.4% of patients receiving theCoreValve.
Overall, permanent pacemaker implantation rates withthe CoreValve, but not Sapien valve, are higher thanconventional surgical AVR rates of 1% to 10%. The needfor permanent pacemaker implantation occurs earlypostprocedure and rarely after hospital discharge. Theneed for permanent pacemaker implantation has noeffect on survival, both early at 30 days postprocedure
and late at 1 year [135]. Continuous postoperative elec-trocardiogram monitoring should be performed in allpatients early after TAVR procedures. Patients with pre-existing or new conduction abnormalities and those re-ceiving the CoreValve device may require longermonitoring.4.3.2.4.3. Vascular Complications. Vascular complicationsare the most frequent adverse outcome of TAVR and areespecially common with transfemoral approach [136].These complications relate to the large-caliber sheathsnecessary for device deployment, as well as severe ath-erosclerosis of the arteries, which is common [137]. Cen-ter/operator experience, the degree and location of vas-cular calcification, vascular tortuosity, and sheath-toartery ratio are predictors of major vascular complication[137, 138]. Major vascular complications are classified inaccordance with the definitions provided by the VARC andinclude aortic dissection, perforation, rupture, or bleedingrequiring significant blood transfusions, or additional per-cutaneous or surgical intervention [96]. Incidence of majorvascular complications ranges from 2% to 26% with trans-femoral access and is related to vessel size, tortuosity, anddegree of aortoiliac occlusive disease and from 5% to 7%with transapical access [107, 109, 111, 116, 139].
Subclavian access may represent an alternative ap-proach in some patients in whom transfemoral ortransapical direct aortic access cannot be utilized. Sub-clavian artery injury is rare with such access althoughtransient brachial plexus neuropathy has been reportedwith this approach [140]. As delivery systems improve intheir profile, the incidence of these complications willlessen [136, 141]. Of note, left subclavian arterial accessfor TAVR may not be appropriate in patients with priorCABG with left internal thoracic arterial graft becausetemporary interruption of blood flow in the left internalthoracic artery may cause coronary insufficiency.4.3.2.4.4. Patient Preferences. Informed consent requiresthe patient and/or support system be appropriately in-formed of the procedure benefits and risks, possesspersonal decision-making capacity, and ultimately beable to make a voluntary decision. Older adults often relyon trusted physicians, family, or friends to participateand guide medical decision making at the point ofmedical care. A central goal in this interaction is theexchange of relevant, detailed information about treat-ment strategies delivered in terminology that is under-stood by the patient and family. This patient-centriceducational effort is essential in providing the patient andfamily information to facilitate interaction with thehealthcare team, and promote personalized decisionmaking for each patient. It is important to remember thatrisk tolerance and patient expectations vary across manypatient populations. Thus, a thorough review of person-alized risk/benefit profile is essential for each patientundergoing an invasive procedure.4.3.2.4.5. Benefit/Risk Assessment. The complex task ofbalancing the benefit and risk of TAVR depends uponaccurate information regarding prognosis for survival,morbidity, and expected quality of life. Ideally, an accu-
rate validated model that predicts both in-hospital and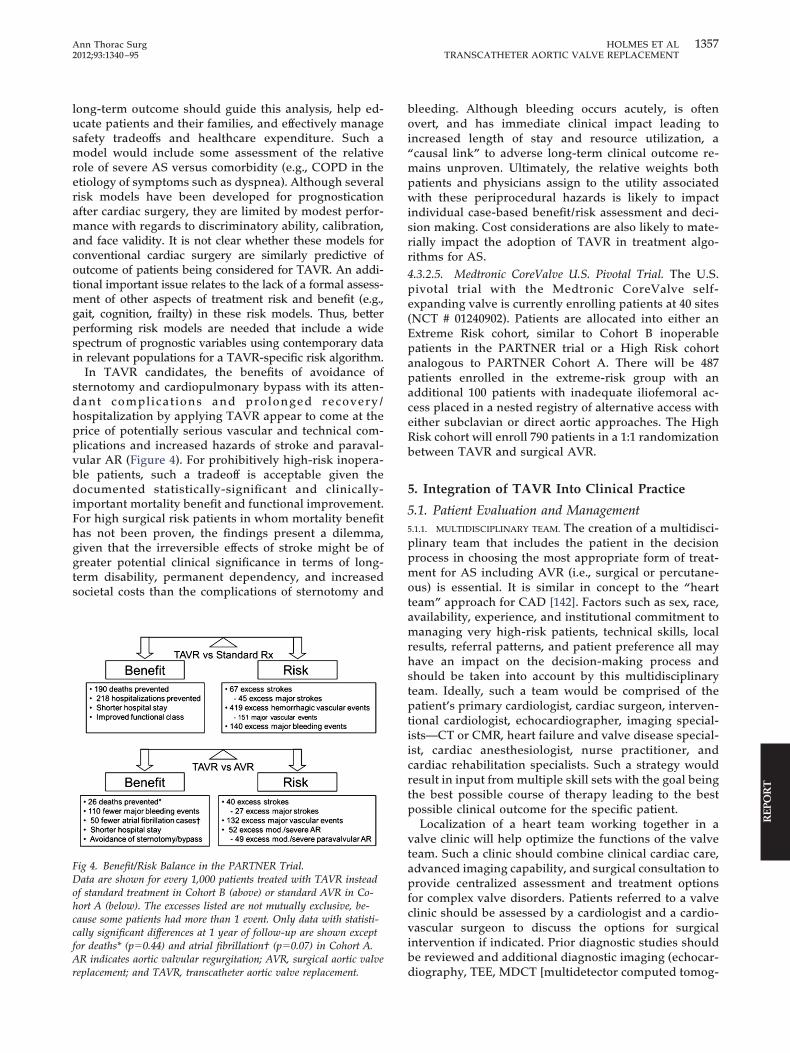
1357Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
long-term outcome should guide this analysis, help ed-ucate patients and their families, and effectively managesafety tradeoffs and healthcare expenditure. Such amodel would include some assessment of the relativerole of severe AS versus comorbidity (e.g., COPD in theetiology of symptoms such as dyspnea). Although severalrisk models have been developed for prognosticationafter cardiac surgery, they are limited by modest perfor-mance with regards to discriminatory ability, calibration,and face validity. It is not clear whether these models forconventional cardiac surgery are similarly predictive ofoutcome of patients being considered for TAVR. An addi-tional important issue relates to the lack of a formal assess-ment of other aspects of treatment risk and benefit (e.g.,gait, cognition, frailty) in these risk models. Thus, betterperforming risk models are needed that include a widespectrum of prognostic variables using contemporary datain relevant populations for a TAVR-specific risk algorithm.
In TAVR candidates, the benefits of avoidance ofsternotomy and cardiopulmonary bypass with its atten-dant complications and prolonged recovery/hospitalization by applying TAVR appear to come at theprice of potentially serious vascular and technical com-plications and increased hazards of stroke and paraval-vular AR (Figure 4). For prohibitively high-risk inopera-ble patients, such a tradeoff is acceptable given thedocumented statistically-significant and clinically-important mortality benefit and functional improvement.For high surgical risk patients in whom mortality benefithas not been proven, the findings present a dilemma,given that the irreversible effects of stroke might be ofgreater potential clinical significance in terms of long-term disability, permanent dependency, and increasedsocietal costs than the complications of sternotomy and
Fig 4. Benefit/Risk Balance in the PARTNER Trial.Data are shown for every 1,000 patients treated with TAVR insteadof standard treatment in Cohort B (above) or standard AVR in Co-hort A (below). The excesses listed are not mutually exclusive, be-cause some patients had more than 1 event. Only data with statisti-cally significant differences at 1 year of follow-up are shown exceptfor deaths* (p�0.44) and atrial fibrillation† (p�0.07) in Cohort A.AR indicates aortic valvular regurgitation; AVR, surgical aortic valve
replacement; and TAVR, transcatheter aortic valve replacement.bleeding. Although bleeding occurs acutely, is oftenovert, and has immediate clinical impact leading toincreased length of stay and resource utilization, a“causal link” to adverse long-term clinical outcome re-mains unproven. Ultimately, the relative weights bothpatients and physicians assign to the utility associatedwith these periprocedural hazards is likely to impactindividual case-based benefit/risk assessment and deci-sion making. Cost considerations are also likely to mate-rially impact the adoption of TAVR in treatment algo-rithms for AS.4.3.2.5. Medtronic CoreValve U.S. Pivotal Trial. The U.S.pivotal trial with the Medtronic CoreValve self-expanding valve is currently enrolling patients at 40 sites(NCT # 01240902). Patients are allocated into either anExtreme Risk cohort, similar to Cohort B inoperablepatients in the PARTNER trial or a High Risk cohortanalogous to PARTNER Cohort A. There will be 487patients enrolled in the extreme-risk group with anadditional 100 patients with inadequate iliofemoral ac-cess placed in a nested registry of alternative access witheither subclavian or direct aortic approaches. The HighRisk cohort will enroll 790 patients in a 1:1 randomizationbetween TAVR and surgical AVR.
5. Integration of TAVR Into Clinical Practice
5.1. Patient Evaluation and Management5.1.1. MULTIDISCIPLINARY TEAM. The creation of a multidisci-plinary team that includes the patient in the decisionprocess in choosing the most appropriate form of treat-ment for AS including AVR (i.e., surgical or percutane-ous) is essential. It is similar in concept to the “heartteam” approach for CAD [142]. Factors such as sex, race,availability, experience, and institutional commitment tomanaging very high-risk patients, technical skills, localresults, referral patterns, and patient preference all mayhave an impact on the decision-making process andshould be taken into account by this multidisciplinaryteam. Ideally, such a team would be comprised of thepatient’s primary cardiologist, cardiac surgeon, interven-tional cardiologist, echocardiographer, imaging special-ists—CT or CMR, heart failure and valve disease special-ist, cardiac anesthesiologist, nurse practitioner, andcardiac rehabilitation specialists. Such a strategy wouldresult in input from multiple skill sets with the goal beingthe best possible course of therapy leading to the bestpossible clinical outcome for the specific patient.
Localization of a heart team working together in avalve clinic will help optimize the functions of the valveteam. Such a clinic should combine clinical cardiac care,advanced imaging capability, and surgical consultation toprovide centralized assessment and treatment optionsfor complex valve disorders. Patients referred to a valveclinic should be assessed by a cardiologist and a cardio-vascular surgeon to discuss the options for surgicalintervention if indicated. Prior diagnostic studies shouldbe reviewed and additional diagnostic imaging (echocar-
diography, TEE, MDCT [multidetector computed tomog-
1358 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
raphy], CMR) performed as clinically indicated. Overall,a valve clinic should offer patients a personalized ap-proach for the evaluation and treatment of complex valvedisorders with the availability of a cardiologist and acardiac surgeon specializing in valve disorders.5.1.2. PATIENT SELECTION.
5.1.2.1. Inclusion/Exclusion Criteria. TAVR is appropriatecurrently only for a highly select population and thevalve team should systematically identify the charac-teristics that define that population with most benefitand acceptable risk. These identification criteriashould be operationalized into practice and may evolveover time with this new technology as new data be-come available.
The inclusion and exclusion criteria in extant random-ized studies are generally appropriate for use in clinicalpractice (Table 9). These vary somewhat, but there aresome criteria common to most studies. Some criteria canbe precisely identified with objective measurements, butmany require subjective estimates based on clinical judg-ment. These subjective assessments are at least as impor-
Table 9. Patient Selection: Inclusion and Exclusion Criteria in
Inclusion Criteria1. Patient has calcific aortic valve stenosis with echocardiogra
�4.0 m/s and an initial AVA of �0.8 cm2 or indexed EOAwithin 45 days of the date of the procedure.
2. A cardiac interventionalist and 2 experienced cardiothoracare high risk for surgical AVR, based on a conclusion thatthe probability of meaningful improvement. The surgeons’to that conclusion and include a printout of the calculationAt least 1 of the cardiac surgeon assessors must have phys
3. Patient is deemed to be symptomatic from his/her aortic vconditions, and as demonstrated by NYHA functional class
Exclusion Criteria (candidates will be excluded if any of the fo1. Evidence of an acute myocardial infarction �1 month (30 d
non–Q-wave MI with total CK elevation of CK-MB � twiceelevation [WHO definition])
2. Aortic valve is a congenital unicuspid or congenital bicusp3. Mixed aortic valve disease (aortic stenosis and aortic regur4. Hemodynamic or respiratory instability requiring inotropic
within 30 days of screening evaluation5. Need for emergency surgery for any reason6. Hypertrophic cardiomyopathy with or without obstruction7. Severe left ventricular dysfunction with LVEF �20%8. Severe pulmonary hypertension and RV dysfunction9. Echocardiographic evidence of intracardiac mass, thrombu
10. A known contraindication or hypersensitivity to all anticoaprocedure
11. Native aortic annulus size �18 mm or �25 mm as measur12. MRI confirmed CVA or TIA within 6 months (180 days) of13. Renal insufficiency (creatinine �3.0 mg/dL) and/or end-sta14. Estimated life expectancy �12 months (365 days) due to no15. Severe incapacitating dementia16. Significant aortic disease, including abdominal aortic or th
greater; marked tortuosity (hyperacute bend), aortic arch anarrowing (especially with calcification and surface irregultortuosity of the thoracic aorta
17. Severe mitral regurgitation
* The boundaries of annulus size will continue to change in concert with
AVA � aortic valve area; AVR � aortic valve replacement; CK � crarea; LVEF � left ventricular ejection fraction; MB � MB isoenzy
NYHA � New York Heart Association; RV � right ventricular; STSWHO � World Health Organization.tant as the objective determinations and necessarilycreate some variability in the process of patient selection.The criteria presented here are based on current technol-ogy and experience. As technology improves and expe-rience is gained, it is likely that many of these criteria willchange to expand TAVR to different populations that willbe optimally treated with the next generation of devices.In addition, the arbitrary criteria such as qualifying aorticAVA measurement within 45 days within the procedurewill be modified and made more flexible.5.1.2.2. Specific Patient Subsets.5.1.2.2.1. Porcelain Aorta, Friable Aortic Atheroma, Radi-ation Heart Disease. Occasionally, otherwise fairlyhealthy candidates for AVR will have local factors such asprior radiation therapy to their mediastinum and/orsevere calcific changes within their ascending aorta(“porcelain aorta”) that add significant risk to a tradi-tional open AVR. Rarely, transesophageal echocardiog-raphy will reveal advanced atherosclerosis with mobileand pedunculated atheromata that also increase risk forstroke or a major embolic event with traditional TAVR.
ical Trials
ally derived criteria: mean gradient �40 mm Hg or jet velocitycm2/m2. Qualifying AVA baseline measurement must be
geons agree that medical factors either preclude operation orrobability of death or serious, irreversible morbidity exceedsult notes shall specify the medical or anatomic factors leadinge STS score to additionally identify the risks in the patient.evaluated the patient.
stenosis, as differentiated from symptoms related to comorbidr greater.ng conditions are present)before the intended treatment (defined as: Q-wave MI, ormal in the presence of MB elevation and/or troponin level
lve, or is noncalcifiedion with predominant aortic regurgitation �3�)port, mechanical ventilation, or mechanical heart assistance
vegetationtion regimens, or inability to be anticoagulated for the study
echocardiogram*rocedurenal disease requiring chronic dialysis at the time of screeningdiac comorbid conditions
c aneurysm defined as maximal luminal diameter 5 cm orma [especially if thick (�5 mm), protruding or ulcerated] ors) of the abdominal or thoracic aorta, severe “unfolding” and
ging device size.
e kinase; CVA � cerebrovascular accident; EOA � effective orificeMI � myocardial infarction; MRI � magnetic resonance imaging;
Clin
phic�0.5
ic surthe pconsof th
icallyalve
II ollowiays)nor
id vagitatsup
s orgula
ed bythe pge rencar
oracitheroaritie
chan
eatinme;
� Society of Thoracic Surgeons; TIA � transient ischemic attack;

1359Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
Cases such as these are approached individually and thecorrect approach is at best an educated judgment on thepart of the surgical team. TAVR offers an alternative forthe treatment of AS when there is severe circumferentialcalcification (porcelain aorta) or heavy atherosclerotic dis-ease burden in the ascending aorta [143]. Patients withextensive atherothrombotic burden involving the ascend-ing aorta should be approached very carefully irrespectiveof whether either a transapical or transfemoral procedurebecause of the potential for embolization.5.1.2.2.2. Very Elderly. Advanced age has important im-plications, as typically these patients have several comor-bid conditions (in addition to advanced age) that increasethe risk of AVR or TAVR. Functional status and compre-hensive assessment of comorbidities including CAD,history of transient ischemic attack or stroke, chronickidney disease, and dementia should be performed.Finally, risk and benefit, including prognosis of existingconditions, should be thoroughly discussed with thepatient and family as part of the initial meeting with theTAVR team and should include a review of postproce-dural complications that may extend hospitalization. Onthe other hand, successful procedures result in improve-ment in dyspnea, a heightened energy level, and an overallimproved quality of life. Life expectancy can be prolonged,since the mortality of medically-treated symptomatic se-vere AS carries a high mortality.
As noted above, symptoms usually improve followingvalve replacement, but a caveat exists for elderly patientsregarding dyspnea and the presence of LVH. LVH is seenin 54% of men and 81% of women with severe AS[144–147] whereas men more often have less LVH, someLV chamber enlargement, and some reduction in EF.Occasionally women will have such severe diastolic dys-function that even when the afterload stress is relievedby TAVR, elevated LV filling pressures may result inpersistent symptoms of shortness of breath. Since LVHmay eventually regress following TAVR, shortness ofbreath may also eventually improve over several monthsfollowing valve replacement. Men, who tend to have agreater degree of LV myocardial fibrosis and abnormalLV collagen network patterns [148], may have moreinherent reduced contractility, so that relieving afterloadwith TAVR may also not result in early or markedsymptomatic improvement. When discussing TAVR withthe very elderly, they should be made aware that symp-tomatic improvement may be delayed or minimal insome cases.5.1.2.2.3. Frailty and Futility Versus Utility. As previouslydiscussed, the concepts of frailty and futility will assumecentral importance in patient selection for TAVR byvirtue of the extensive comorbidities present in thispopulation. Frailty is an important and frequent condi-tion in elderly patients and should be considered whendealing with invasive care in older adults [149]. Althoughit can have significant overlap with disability and comor-bidity, it is a distinct syndrome and is characterized by avicious cycle of decreasing muscle mass, energy expen-
diture, and malnutrition culminating in vulnerability toadverse events [150]. In the PARTNER trial, frailty waspresent in as many as 23% of patients in Cohort B and16% in Cohort A. Besides comorbidities, and frequentlyin combination with them, it is likely to play a role in theassessment of the individual’s candidacy for invasivecare and therefore in withholding any intervention innearly one half of high-risk patients with AS [151]. It isimportant to consider that frailty may be a reversiblephysiological phenotype in some cases, and therefore it ispremature to consider this a permanent characteristic ofthe individual patient. To the extent that AS may con-tribute to the declining health state, AVR or TAVR mayreverse frailty. In this case, frailty may be a marker fortreatment benefit. Conversely, if the individual is frailfrom multiple other organ system declines, frailty may bea marker of treatment risk.
The impact of frailty on the clinical course and out-come of patients presenting with severe AS is beginningto be investigated but is difficult to assess because of itsmultidimensional phenotype and the lack of a clear andagreed-upon assessment. The definition of frailty used inrecent studies ranges from the qualitative “eyeball test”to more quantitative scores such as the Fried FrailtyIndex [150]. A simple test for defining frailty is a timedgait speed over 5 m. In a recent Canadian study [152], atime of �6 seconds as a measure of frailty was found tobe an independent predictor of mortality compared withthe STS risk algorithm alone. As such, it has recentlybeen added to the STS database upgrade (Version 2.73,July 1, 2011) and will be uniformly collected in patientsundergoing cardiac surgery [152]. Future studies shouldaim at developing more reliable and reproducible waysof identifying frailty, as well as incorporating these as-sessments in development of risk and benefit prediction.
Futility is also an important consideration for TAVR.There may be some patients in whom this procedureshould not be performed because the clinical condition istoo far advanced; in these patients, even a successfultechnical procedure is futile and does not improve healthoutcomes.
Therapeutic futility may be determined based upon:1) lack of medical efficacy, as judged by the patient’sphysician; or 2) lack of a meaningful survival, as judgedby the personal values of the patient [153, 154]. Althoughtherapeutic futility may be invoked to justify denial,limitation, or withdrawal of care, the threshold for defin-ing it is unclear, controversial, and often viewed differ-ently by different stakeholders. In the PARTNER trial, thecriterion for inoperability—used as a surrogate for futil-ity with regards to surgical intervention—was an esti-mate of probability of death or serious, irreversiblemorbidity �50% by a cardiologist and 2 experiencedcardiothoracic surgeons [15]. Despite successful correc-tion of AS leading to an absolute 20% survival advantage,there was still 30% mortality in the TAVR treatment armat 1 year, mainly due to noncardiac causes. The key totreatment in this group of “inoperable” patients is todefine the “futility versus utility” treatment paradigm.Clearer definition of comorbid conditions that adversely
affect survival despite successful valve implementation
1360 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
as well as quality of life and health economic assessmentin those “inoperable” patients is crucial so that thistherapy is appropriately used in patients likely to benefit(utility) compared with those unlikely to benefit despitesuccessful therapy (futility). Although some might arguethat it is inappropriate and misleading to say that treat-ment is futile simply because the probability that it willsucceed is small, especially given the substantial uncer-tainty in our ability to prognosticate in individual pa-tients and lack of validated tools that universally discrim-inate survivors from nonsurvivors of critical illness, it isnonetheless important to define meaningful cutoff points.This is particularly true when, in the course of a progres-sive illness, continued use of resources other than mea-sures for comfort, is no longer reasonable, practical, orappropriate. Ultimately, these decisions must be guidedby what our society considers to be the inherent value ofhuman life and the resultant financial burden society iswilling to bear for the provision of modern public healthcare [155].5.1.3. CARE PLAN IN CANDIDATES FOR TAVR. The healthcareteam needs to be intimately involved in discussions onrisk/benefits including detailed information on individu-alized risks for each patient and alignment of quality-of-life expectations. Failure to understand and comply witha plan of care may account for dissatisfaction with pro-cedural outcomes and potential rehospitalizations [156,157]. One critical intervention to ensure effective carecoordination and transition is that of comprehensive planof care and educational material given to patient and/orcaregivers prior to the planned procedures, and againduring and after hospitalization. This process may en-courage full participation of the patient and family aboutadherence to medication therapy and activity recommen-dations. Transitions of care and follow-up will be im-proved by discussion and written instructions reviewedwith each patient including medications, timely fol-low-up with the various healthcare professionals in-volved with the patient’s ongoing care, and appropriatepostprocedural activities. The ongoing care and coordi-nation with the cardiovascular care team may decreaselikelihood of readmission and improve overall adher-ence. Healthcare providers should pay close attention topsychosocial and socioeconomic issues that the patientand family face, including access to care, risk of depres-sion, and healthcare disparities [158–160].5.1.4. IMAGING ASSESSMENT. Imaging plays an essential rolein patient selection and procedural planning, perfor-mance, and follow-up [161]. In each of these steps,optimal imaging can help to enhance successful outcome.There is variability in the specific imaging protocolspreferred in individual institutions. This variability is theresult of institutional and individual experience andequipment, as well as the specific patient characteristicsto be considered.5.1.4.1. Echocardiography. The following general recom-mendations can be made for echo assessment of patientsbeing considered for TAVR. More detailed instructions can
be found in a recent expert consensus statement from theAmerican Society of Echocardiography and the EuropeanSociety of Echocardiography [161].5.1.4.1.1. Annulus Size and Cusp and Root Anatomy.Accurate assessment of annular size is critical. Underes-timation of annular size could lead to selection anddeployment of a valve which is too small, with risks ofpoor hemodynamics, paravalvular regurgitation, andvalve migration and embolism. Overestimation of annu-lar size and placement of a valve that is too large can leadto other adverse outcomes, including incomplete deploy-ment (with both valvular and paravalvular regurgitation)or catastrophic annular rupture. In general, all TAVRsare designed to be deployed in annuli that are slightlysmaller than the prosthesis size. This oversizing is re-quired because the valves are sutureless and depend onradial force to prevent dislodgement. For the initialSapien valves, the 23-mm valve was designed for 18-mmto 22-mm annuli, whereas the 26-mm prosthesis wasdesigned for 21-mm to 25-mm annuli. The Sapien XTvalve, with 23-mm, 26-mm, and 29-mm sizes, is designedfor annuli from 18 mm to 27 mm. The CoreValve has26-mm, 29-mm, and 31-mm prosthesis sizes (using adifferent sizing convention from the Sapien valve) de-signed for annuli from 20 mm to 23 mm for the 26-mmprosthesis, 24 mm to 27 mm for the 29-mm prosthesis,and 26 mm to 29 mm for the 31-mm annuli. Annulardimensions can be measured with either TTE or TEE[162]. With either modality, the annular anteroposteriordiameter is measured from a long-axis view. Care mustbe taken to identify the true annulus, not overlyingcalcium. Measurements are made in systole at the hingepoint of the leaflets into the LVOT with a trailing edge toleading edge convention. Because the annulus is oftenelliptical, optimal assessment should include measure-ment of the transverse (coronal) diameter, using theshort-axis view, ideally with biplane TEE approach or CT,which allows simultaneous long- and short-axis interro-gation of the annular plane.5.1.4.1.2. Aortic Root Disease and Ascending AorticDimensions. Assessment of cusp and root anatomy isalso critical. The PARTNER trial excluded all patientswith bicuspid aortic valves for concern that such valvesmight distort the prosthesis, leading to paravalvularregurgitation. Thus, TAVR in any nontricuspid valvewould be considered an off-label use, though successfultreatment of bicuspid valves has been reported [163]. It isoften difficult to determine cusp anatomy in the denselycalcified valves commonly treated by TAVR. In thissetting, CT or review of old echocardiograms may allowbetter assessment of the underlying anatomy. Pathologyreviews have demonstrated progressive increase with agein the proportion of trileaflet valves in severe AS patients,from 15% in those under 60 years to 60% over 70 years (72%for those over 80 years) [2]. Of note, this study showed thateven pathological examination cannot determine cuspanatomy in some heavily distorted valves.
Several issues must be considered in assessing rootanatomy and pathology. Care must be taken to assure
that valve deployment will not compromise the coronary
ic res
1361Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
ostia, either from the device itself or from cusp calcifica-tion being shifted and displaced into the coronary. Ingeneral, CT scanning provides a more comprehensiveassessment of the relationship of the coronary arteries tothe annulus and valve leaflets, demonstrating an averageannular–left coronary artery distance of 13.4�3.2 mm andannular-right coronary artery distance of 13.6�2.8 mm[164]. Nevertheless, echo, particularly TEE, can measurethe distance from the aortic valve annulus to the rightcoronary ostium. Since the left coronary does not lie in astandard TEE or TTE imaging plane that intersects theannulus, measurement from 3D datasets may be a feasi-ble approach for this.
Accurate assessment of the aortic root and tubularportion is also important. The CoreValve Revalving Sys-tem is designed with a supra-annular location of theporcine pericardial valve, located in the sinus of Valsalva.As a result, the CoreValve nitinol frame has a longerlength than conventional surgical valves, ranging from 52mm ( for the 31-mm valve) to 55 mm (for the 26-mmvalve) including its deployment hooks. It is recom-mended that the upper dimensions of the tubular aortameasured at 45 mm above the annulus be 40 mm for the26-mm valve and 43 mm for the 29-mm and 31-mmCoreValve prostheses.
Preprocedural assessment of AR in TAVR candidatesshould be governed by guidelines from the AmericanSociety of Echocardiography [165]. This assessment isbased on multiple parameters, including LV size, AR jetsize and morphology, AR pressure half-time, and dia-stolic flow reversal in the aortic arch. Patients with �3�AR were excluded from the PARTNER trial and shouldbe considered relatively contraindicated for TAVR.5.1.4.1.3. Three-Dimensional Echocardiography. Real-time 3D TEE is an important modality for preproceduraland intraprocedural assessment of TAVR patients [166,167]. Similar to MDCT and CMR, it can help with preciseassessment of the aortic root and annulus, potentiallyhelping reduce the chance for prosthesis-sizing error inpatients. However, multiple studies have demonstratedsignificant differences in dimensions of the aortic rootand annulus measured by 2D TTE, 2D TEE, 3D TEE, and
Table 10. Potential Approaches for Imaging in TAVR
Preprocedural Assessment1. Assessment of aortic annular size and shape (CT, CMR, 22. Assessment of aortic valve for number of cusps, degree o
echocardiography)3. Measurement of the distance between annulus and coron4. Planning for precise coaxial alignment of the stent-valve a5. Assessment of aortic dimensions (2D and 3D echocardiog
CMR)6. Assessment of dimensions and atherosclerosis of iliofemo
Postprocedural Assessment1. Assessment of degree of aortic regurgitation (echocardiog2. Assessment of cerebral embolization (cerebral MRI)
2D � 2-dimensional; 3D � 3-dimensional; CMR � cardiac magnetimaging; TAVR � transcatheter aortic valve replacement.
MDCT [166, 167]. Hence, it is imperative to realize that
the imaging technique utilized might impact TAVR sizeselection and strategy. TEE, including real-time 3D TEEcan help evaluate the extent of and precisely locate the jetof AR following prosthesis implantation.5.1.4.2. Tomographic Imaging.5.1.4.2.1. Rationale for Tomographic Imaging. Optimiz-ing outcome relies heavily on image guidance for patientselection, preprocedural planning, and intraoperativedecision making [168]. Correct positioning of the pros-thesis relative to the annulus is critical. If valve deploy-ment is too high, increased risk of paravalvular regurgi-tation, aortic injury, coronary occlusion, or embolizationof the prosthesis can occur. If positioning is too low,mitral valve dysfunction, heart block, paravalvular regur-gitation, or embolization into the left ventricular cavitycan occur [169]. In addition, the relatively large deliverycatheters currently required for valve insertion are asso-ciated with the risk of vascular complications, necessitat-ing assessment of iliofemoral vasculature. This has led tothe application of 3D imaging approaches for TAVR, in-cluding CT, CMR, 3D echocardiography, and C-arm CT[162, 166, 170, 171] (Table 10).5.1.4.2.2. Multidetector Computed Tomography. MDCT pro-vides comprehensive assessment of the aortic root, ath-erosclerotic burden, and course of the thoracoabdominalaorta and its iliofemoral branches (Figure 5). MDCT inthe context of TAVR eligibility assessment has becomeroutine in many large-volume centers [172].
MDCT systems with at least 64 detectors and a spatialresolution of 0.5 mm to 0.6 mm are recommended. Thespecific scan protocols used for assessment vary butgenerally include imaging of the aortic root and thethoracoabdominal aorta and its iliofemoral branches.ECG-synchronized imaging of the aortic root is impor-tant to avoid image quality degradation due to motionartifacts, and image reconstruction is performed at thedesired phase of the cardiac cycle (e.g., a systolic 30% to40% phase for valve area and annular assessment). Usingthe retrospectively ECG-gated helical acquisition, CTdata can be acquired throughout the entire cardiac cycle,enabling 4D image reconstructions for evaluation of
d 3D echocardiography)ification and valve area by planimetry (CT, CMR, 2D and 3D
stia (CT, CMR, 2D and 3D echocardiography)the centerline of the aortic valve and aortic root (CT)
y, CT or CMR) and atherosclerosis (echocardiography, CT, or
essels (CT, MR, angiography)
y or CMR)
onance; CT � computed tomography; MRI � magnetic resonance
D anf calc
ary olong
raph
ral v
raph
valvular function, albeit at the expense of a higher

1362 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
radiation dose [173]. Alternatively, prospectively ECG-triggered axial CT data acquisition requires much lessradiation; however, images are acquired during a pre-specified phase of the cardiac cycle and reconstruction inother phases or 4D cine loops may not be reconstructible[174]. However, protocols with newer generation scan-ners allow prospective acquisition at a lower radiationdose with subsequent display of cine loops [175]. Al-though radiation exposure is important to consider withany CT acquisition, it is less a concern in the elderlypatients currently considered for TAVR.
Because a standard bolus of 80 mL to 120 mL oflow-osmolar iodinated contrast is necessary, the ben-efits versus risks of iodinated contrast need to becarefully weighed [176]. An alternative approach in-volves a pelvic scan after intra-arterial contrast injec-tion into the infrarenal abdominal aorta (catheter leftin place after cardiac catheterization) using a very lowdose (15 mL) of contrast [177]. If contrast administra-tion is not feasible, a noncontrast scan, although notoptimal, still allows the assessment of overall vesselsize, calcification, and tortuosity.
As previously mentioned, analysis and measurementof the annulus size and shape are crucial for proceduralsuccess. Typical annulus measurements, obtained using2D TTE or TEE provide a single diameter measurement,assuming a circular annular orifice [178]. In contrast, 3DCT systolic reconstruction of the annulus orthogonal tothe center-axis of the LVOT allows for the assessment ofminimal and maximal diameter, circumference, and areameasurements [162, 164, 166, 179–183]. Indeed, thesestudies have demonstrated that the LVOT is often oval,rather than circular. Hence, multimodality imagingmight improve the accuracy of AV measurements andreduce the chance for prosthesis-sizing errors in patients
Fig 5. Reconstructed Multidetector ComputedTomographic Images of the Abdominal Aortaand Its Pelvic Branches Demonstrating Tortu-osity and Extensive Calcific Atherosclerosis.The extent and degree of peripheral arterialdisease is essential in determining the feasibil-ity and safety of transfemoral approaches. Insome patients with extensive disease, alterna-tive approaches such as direct aortic, subcla-vian, or transapical procedures should beconsidered.
considered for TAVR.
Complete coronary assessment with MDCT is obvi-ously limited in the current population evaluated forTAVR because of the very high prevalence of advancedcalcified disease, precluding precise assessment of lumi-nal stenosis. However, MDCT allows measurement of thedistance between annulus and coronary ostia, whichidentifies patients at risk for coronary occlusion duringTAVR. Although no definite criteria exist to excludepatients, a �10 mm distance might identify increased riskof coronary ostial occlusion [184]. In this setting, place-ment of a guidewire or balloon catheter in the left mainartery could be considered to ensure access in case ofcomplications.
Although echocardiography is used extensively to as-sess the aortic valve, cine MDCT can provide incrementalvalue in its assessment, including number of cusps,especially in cases of heavy calcification, where echocar-diography can be difficult. Also, cine MDCT can be usedto perform planimetry of the aortic valve [180, 185].
Optimal coaxial alignment of the stent valve alongthe centerline of the aortic valve and aortic root isimportant during positioning. Ascertainment of theright height to avoid too high or too low placement isimportant to avoid AR and optimize valve function[169]. Although traditional assessment of root orienta-tion is performed using multiple invasive aortogramsin 1 or 2 orthogonal planes, double-oblique multipla-nar MDCT reconstruction allows preprocedural pre-diction of the aortic root angle [186, 187]. This poten-tially decreases the number of aortograms requiredduring the procedure, therefore shortening both pro-cedure time and contrast usage, and improves preci-sion of deployment. The emergence of C-arm CTwould further allow the incorporation of fusion imag-
ing in the catheterization laboratory [170].
1363Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
5.1.4.2.3. Cardiac Magnetic Resonance. Similar to MDCT,CMR can also potentially provide comprehensive assess-ment of the aortic valve, annulus, aortic root, course ofthe thoracoabdominal aorta and luminal caliber of theiliofemoral branches, without the ionizing radiation. 2DECG-gated noncontrast cine CMR sequences across theaortic valve (even avoiding the calcium blooming com-monly seen on CT) and aortic root can provide a detailedassessment of LV function, aortic annulus, valve, root,and coronary ostia, similar to that obtained on MDCT[188]. In addition, free-breathing noncontrast navigator-gated 3D whole-heart acquisition can also be obtained tomimic the volumetric acquisition of a CT image [171]. Italso enables assessment of the aortic root in addition toassessing the LVOT–aortic root angulation and predict-ing imaging planes. The use of 3D gadolinium-enhancedmagnetic resonance imaging can provide precise luminaldimensions of the thoracoabdominal aorta and its iliopel-vic branches [189]. In cases with renal insufficiency, anavigator-gated, free-breathing, 3D noncontrast steady-state free precession sequence can be used to assessluminal dimensions. However, CMR is not optimal forassessment of aortic wall changes, especially dense aorticcalcifications, because it would lead to signal voids andhence, appear dark. Postprocedural assessment of resid-ual aortic insufficiency by quantitative CMR might have apotential role in TAVR patients [190]. However, CMR is atime-intensive technique, which could be a limiting fac-tor, particularly in older patients. In patients with tenu-ous renal function, the benefits of gadolinium adminis-tration have to be balanced against the risks ofnephrogenic systemic fibrosis [191]. In addition to theabove-mentioned constraints, CMR is not recommendedin patients with pacemakers, defibrillators, or intracra-nial aneurysm clips, although the currently used valvesare CMR compatible.
5.2. Procedural Performance5.2.1. ROLE OF SURGEON AND/OR CARDIOLOGIST. The centralposition of the heart team in optimizing TAVR patientevaluation, procedure performance, and outcomes hasbeen emphasized. Candidacy for TAVR should be deter-mined together by both the surgeon and cardiologist,ideally in an established valve or structural heart diseaseclinic. During procedural performance, both cardiologistand surgeon should be active participants. There areseveral specific tasks to be considered among others: 1)gaining access to the vascular tree by either varioustransarterial sites or by the transapical route; 2) crossingthe stenotic aortic valve; 3) balloon aortic valvuloplasty;4) optimal positioning and deployment of the aorticprosthesis; 5) achieving secure vascular closure; 6) as-sessment and treatment of procedural-related complica-tions, which encompasses vascular access, cardiac struc-ture, coronary artery anatomy, and electrophysiologyissues; and 7) considerations for access for hemodynamicsupport and the need for cardiopulmonary bypass needto be determined by the cardiovascular (CV) surgeon andteam. Each of these tasks contains within it multiple
component parts, e.g., the need for rapid ventricularpacing during either balloon aortic valvuloplasty or pros-thetic deployment, and identifying the optimal fluoro-scopic position to be used.
The above-mentioned tasks often require different skillsets. In the future, as training programs evolve withintegration of cardiovascular surgery and interventionalcardiology, the roles of either or both specialties maychange. However, at the present time and for the fore-seeable future, both a surgeon and an interventionalcardiologist should be integrally involved with each pro-cedure. Prior to the start of each procedure, a specificteam leader should be identified, either the surgeon orthe interventional cardiologist. That individual shouldhave overall supervision for the specific case to optimizethe procedure. The specific person identified will dependon the operator experience as well as the unique charac-teristics and challenges of each individual case; for ex-ample, the cardiovascular surgeon should be the primaryteam member responsible for the surgical aspects oftransapical and transaortic procedures or if a subclaviancutdown is to be required. Interventional cardiologistsusually assume the lead operator position in transfemo-ral procedures, whereas cardiothoracic surgeons usuallylead transapical procedures. The specific roles of theother individuals involved should be identified. Somewill be shared, e.g., deciding what specific angle identi-fies the optimal fluoroscopic view for visualizing theplane of the aortic valve for deployment. Other roles willinvolve just 1 individual, e.g., taking the team through thepre-and postprocedure checklists and selection of thespecific pacing algorithm for deployment. It is importantfor all members of the team to be present for all stages ofthe procedure.
The most important considerations are team-based care,identification of a specific team leader, close communica-tion, and preplanning for outlining management of poten-tial complications. Likewise postprocedure care is optimallydelivered on a multispecialty team care service similar to atransplant service where all specialties are participatory toachieve optimal patient outcomes.5.2.2. PROCEDURAL LOCATION. Procedural location will varyfrom institution to institution related to several factorsincluding resources currently available in the facility. Thespecific location has important physical implications, aswell as personnel and equipment implications. Optimalequipment requirements include a state-of-the-art,large-field-of-view fluoroscopic imaging system—preferably a fixed overhead or floor-mounted system thathas positioning capability rather than a portable C-armsystem. This system needs to have the ability to store andreview images and accommodate varying patient sizes. Apotentially important adjunct for this is the availability ofeither biplane imaging or imaging programs that canautomatically help aid in the selection of orthogonalviews for imaging during positioning of the valve. Inte-gration of TEE echocardiographic images, particularly 3Dcapabilities, is helpful; the availability of CT or CMR is asignificant advantage, particularly if image overlay is
possible, which will become more widely used in the
1364 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
future. Full catheterization laboratory hemodynamic ca-pability is also required for hybrid rooms. Other re-sources required include present cardiopulmonary by-pass machines, perfusionists, and related ancillarysupplies with an inventory of interventional cardiologyequipment for balloon aortic valvuloplasty, coronary bal-loons, stents, and 0.014-inch wires if coronary occlusionoccurs as a complication of device deployment. As vas-cular access is critical, a variety of peripheral arterialballoons and covered stents for treatment of peripheralvascular complications such as iliac rupture, and a vari-ety of vascular closure devices are also important forcompletion of the procedure. The procedure locationshould also be fully capable of providing anesthesiaservices including advanced airway management, gen-eral anesthesia, full hemodynamic monitoring, and ad-ministration of vasoactive agents into the centralcirculation.
As can be seen, these requirements mandate specificroom sizes and configurations. Such a hybrid room maybe situated in a surgical suite or may be in a largemodified catheterization laboratory (approximately �800square feet) with appropriate air handling and air ex-change modifications. In the future, as procedures for thetreatment of a variety of structural heart and endovasculardisease procedures increase, it is anticipated that hybridrooms will become more standard of care for these team-based therapies.
Personnel requirements are also of great importance.Personnel who are trained to deal with complicatedhemodynamics, the specific equipment to be used, andcomplication management are critical. This has signif-icant implications. For example, if the procedures arecarried out in a modified cardiac catheterization labo-ratory staffed by cardiac laboratory personnel, al-though there would be expert experience with percu-taneous procedures and vascular complications, ifurgent cardiopulmonary bypass was required, theremay be undue treatment delays related to inexperiencewith that specific procedure. On the other hand, if theprocedures are carried out in an operating room withlimited catheterization laboratory capabilities and per-sonnel, the ability to promptly address and treat acoronary or a vascular complication requiring imme-diate attention may be compromised. Team-basedtraining and care that includes complication manage-ment remain a cornerstone.5.2.3. ANESTHETIC CONSIDERATIONS FOR TAVR. Patients under-going TAVR are at a high risk for procedural complica-tions, including hemodynamic collapse. Careful planningand intraoperative anesthetic management can mitigaterisk [67, 192, 193]. During the preoperative evaluation,special attention is paid to factors that may predict higherrisk of intraprocedural instability, in particular: de-pressed EF, elevated pulmonary pressures, significantMR, incomplete revascularization, collateral dependentcoronary circulation, COPD, HF, and acute/chronic kid-ney disease. In patients least likely to tolerate rapid
ventricular pacing and hypotension, preventive mea-sures may be instituted [194] and steps taken to allow forrapid institution of cardiopulmonary bypass. Rarely,elective bypass may be utilized. Routine surgical antibi-otic prophylaxis administered prior to surgical incision orvascular access is warranted to decrease the risk ofwound infection and endocarditis.
TAVR is typically performed under general anesthesiawith central monitoring, using a pulmonary artery cath-eter and transesophageal echocardiography. Single-lungventilation is not necessary for TA procedures. Althougha temporary ventricular pacing wire can be placedthrough a hemodynamic catheter, more commonly, atemporary transvenous lead is passed through the fem-oral or subclavian vein or, in the case of transapicalprocedures, sewn directly on the epicardial surface. Aftera ventricular wire is passed, thresholds are checked at apacing of rate 10 to 20 beats/min higher than the patientsintrinsic rates. For placement of the CoreValve, rapidpacing for device placement is not required. Arterialpressure monitoring may be done via the radial artery,but in the case of ipsilateral axillary bypass, a plan mustbe made for additional monitoring either from the con-tralateral radial or femoral artery. At least 1 large-volumeline is obtained peripherally or centrally. Immediateaccess to a defibrillator device is necessary becauseventricular fibrillation can occur with manipulation ofcatheters within the heart or with rapid ventricular pac-ing. This may be best accomplished with preapplieddefibrillator pads connected to the defibrillator beforestarting the procedure.
Steps are required to prevent significant hypothermia,and these are often similar to those used in off-pumpCABG. The room is heated, fluid warmers are used, andsome type of underbody heating system (either forced airor fluid) is generally used. This is important because alimiting step in early extubation of these patients is oftenthe time needed to warm them following the procedure.
Communication in this multidisciplinary approach isthe key word for intraoperative success. The importanceof training a dedicated team cannot be overemphasized.Frequent changes of personnel will dilute the learningcurve. Standard doses of anesthetic, sedative, and nar-cotic analgesic agents may need to be reduced on thebasis of the age and frailty of the patient [195]. Intraop-erative challenges may be encountered even before in-duction. Use of ultrasound for venous access is beneficialto prevent hemorrhage and complications associatedwith placement of central line.
Unless otherwise indicated, volume status needs to besupplemented as the patients in this age group areusually volume depleted. Generally, 1.0 L to 1.5 L of fluidare required, but a combination of pulmonary arterypressures, central venous pressure, and echocardio-graphic evaluation can guide tailored therapy. Severelyunderfilled ventricles may pose an additional problem toguidewire/applicator device insertion in these hypertro-phied ventricles. Patients with severe concentric LV hy-pertrophy and intravascular volume depletion may ex-hibit a rapid and sustained deterioration of
hemodynamic status in response to ventricular pacing,
1365Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
rapid ventricular pacing, intracardiac guidewire or cath-eter manipulations, or balloon aortic valvuloplasty. Inpatients with low cardiac output and those with morethan moderate PH, inotropes such as milrinone or dobut-amine may be considered prior to the procedure, withthe goal of obtaining a cardiac index of at least 1.8L/min/m2. Inhaled nitric oxide or inhaled epoprostenolshould be available for the treatment of severe PH andright ventricular failure.
Avoidance of prolonged hypotension is perhaps themost important step in preventing hemodynamic col-lapse. The cycle of hypotension, subendocardial isch-emia, low output and further hypotension with ultimateventricular fibrillation is best avoided as treatment isdifficult once these events occur. Maintenance of a meanpressure of �75 mm Hg (or systolic of at least 120 mmHg) is advisable before initiation of rapid ventricularpacing. The frequency and duration of rapid ventricularpacing episodes may need to be limited to allow enoughtime between episodes to permit recovery of circulatoryfunction in patients with limited hemodynamic reserve.In patients with a slow recovery of spontaneous circula-tion after ventricular pacing, pre-emptive therapy withvasopressor therapy such as norepinephrine, epineph-rine, or phenylephrine as an intravenous infusion or asincremental intravenous boluses may be important totreat hypotension and facilitate recovery after rapid ven-tricular pacing. Hypertension may be dangerous andincrease the risk of bleeding and ventricular rupture,especially during transapical TAVR.
Anticoagulation therapy is usually initiated after inser-tion of the regular sheaths and prior to placement of thelarge sheath into the vasculature, and repeated to main-tain an activated clotting time (ACT) of �300 seconds.Heparin anticoagulation can be reversed by the admin-istration of protamine sulfate on a milligram to milligramneutralization dose, although it may not be necessary toreverse heparin anticoagulation for transfemoral TAVR ifthere is a minimal risk of surgical bleeding. A trans-venous pacing wire should be secured in position inpatients with postprocedural interventricular conductionabnormalities, at high risk for heart block, or with heartblock until it is determined whether a permanent pace-maker is necessary [196].
Although general anesthesia is generally used fortransapical procedures, some experienced institutionsare performing transfemoral implantation with conscioussedation [197]. With this approach, with conscious seda-tion, the patient is awake and spontaneously breathingwithout an artificial airway. Intraoperative TEE for pro-cedural guidance may be difficult or impossible if TAVRis performed under conscious sedation. Adequacy ofventilation and oxygenation should be continuously as-sessed during conscious sedation and qualified person-nel and equipment to perform intubation of the trachea,provide airway protection, and administer mechanicalventilatory support should be immediately available todetect and treat acute respiratory failure in patients
managed during TAVR with conscious sedation.5.2.4. VASCULAR ACCESS. Placement of TAVR is accom-plished via femoral artery, subclavian artery, or the aorta.The Sapien valve may be deployed by major transvascu-lar access as well as transapically, whereas the CoreValveuses only major transvascular access [110]. Careful eval-uation of the patient’s atherosclerotic load and location,arterial size and tortuosity, and presence of mural throm-bus are required for the best possible delivery site. Thereare specific advantages and disadvantages to each vas-cular access approach. Selection of the optimal routerequires consideration of specific patient anatomy andthe specific device to be used.5.2.4.1. Cardiopulmonary Bypass Requirement. Cardiopul-monary bypass is infrequently (�5%) required for sup-port during the valve implantation due to cardiac decom-pensation as a consequence of cardiac tamponade,coronary occlusion, severe acute AR, aortic rupture, oracute aortic dissection. With experience, and excellenthemodynamic and anesthetic management, this require-ment is rarely necessary. Accessory cannulation sites inthe femoral vessels or with an adjunctive axillary graft andvenous cannula should be considered if femoral access sitesare not suitable. Risk of vascular compromise, injury, orparticulate embolism should be weighed with the risk ofcardiac support needs.5.2.4.2. Percutaneous or Cutdown Access. Both percutane-ous and cutdown access approaches are used; there areadvantages and disadvantages to each. Complicationswith access in this high-risk and generally older popula-tion are frequent. Decisions about access technique andsite depend on the degree and severity of atherosclerosis,vessel size, specific prosthetic device to be used, and theheart team’s experience [136–138, 198]. Use of percuta-neous approaches preferentially occurs when access sitesare relatively large and free of significant atheroscleroticdisease. Less favorable vessels may require cutdown,often with placement of axillary, iliac, or aortic insertiongrafts or conduits to provide access sites. Percutaneousinsertions are occasionally converted to open repair orhybrid repairs, utilizing percutaneous closure devicesand surgical techniques as needed [199].5.2.4.3. Deployment Technique. The goals of deploymentare to avoid hemodynamic compromise while obtaining astable valve, positioned without coronary obstruction, in-terference of mitral valve function, conduction system im-pingement, or overhanging native aortic leaflets, and avoid-ance of aortic root complications (rupture and dissection).There are several approaches to the aortic valve, which canbe broadly categorized as retrograde or antegrade.
Retrograde passage is generally performed via thefemoral artery. There are obvious limitations in patientswith peripheral arterial disease or small vessels. Addi-tional, reported retrograde options include the axillaryapproach and direct ascending aortic puncture. A femo-ral approach is used in the vast majority of retrogradedeployments, starting with either a standard percutane-ous femoral arterial access or a surgical exposure of theartery. A series of dilators is employed, under fluoro-
scopic vision, to reach the size of the deployment sheath.
1366 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
The sheath is passed into the body of the thoracoabdomi-nal aorta. Crossing the aortic valve is accomplished usingstandard interventional techniques, and a stiff wire ex-change is performed, with redundancy in the LV cavity toprevent loss of position. Care must be taken to avoiddamage to the LV, resulting in perforation.
The transapical approach is the only currently avail-able antegrade approach, and equipment is only avail-able for this approach for the Sapien valve. Access isobtained via a left anterior thoracotomy, which is madeafter localization of the apex by fluoroscopy or TTE. Afterentering the pleural space, digital inspection can furtherlocalize the position of the apex and a 2-inch to 3-inchsegment of rib may be resected to facilitate exposure. Toreduce postoperative pain, soft tissue retractors are pre-ferred to heavy metal retraction. The proper site ofpuncture is on the left ventricular apex, which is moreanterior and proximal than the anatomic cardiac apex.TEE is of great value in helping to localize the apex of theLV. Either 2 concentric purse-string sutures or 2 mattresssutures are placed with felt buttress. Puncture is madeand a 0.035-inch guidewire is passed through the nativevalve. A balloon catheter may help facilitate wire place-ment by avoiding the mitral subvalvular apparatus. Afterthe guide wire is placed in the ascending aorta, a coro-nary catheter such as a JR-4 can be used to guide the wireinto the descending aorta, and the wire is exchanged fora stiffer wire (super or extra stiff). The deployment sheathis then passed to a depth of 3 cm to 4 cm, following which,balloon aortic valvuloplasty of the native valve is per-formed prior to valve implantation.
A more recent approach that has gained interest andacceptance is the direct aortic or transaortic approach. Thisapproach is being employed with both the balloon expand-able and self-expanding techniques. The access is througheither an upper partial sternotomy or a second or third rightintercostal space minithoracotomy. Concentric feltpledgeted reinforced purse-string sutures are placed inthe ascending aorta at least 5 cm above the valve. Aguidewire is then placed retrograde across the valve, andballoon aortic valvuloplasty and valve deployment per-formed similar to the other access techniques. The ad-vantages of this approach include the short distance fromthe aortic valve, allowing optimal control and enhancedsurgeon comfort level with a technique they are alreadyusing routinely for cardiopulmonary bypass cannulationas compared with the left ventricular apex approach.Another possible advantage is a less painful incision thanwith a left anterior thoracotomy at a lower interspace.Disadvantages include manipulation of the ascendingaorta with possible embolization of atherosclerotic debriswhen disease is present. Current-generation deliverysystems are being modified for this approach [200].5.2.4.4. Balloon Expandable Versus Self-ExpandingProstheses. There are significant differences between theballoon-expandable and self-expanding valves. Balloon-expandable valves, such as the Sapien, cannot be col-lapsed once expanded. Self-expanding, nitinol-based
valves such as the CoreValve can be partially deployedand repositioned to some extent. The promise of recap-ture and repositioning newer nitinol-based valves offersignificant potential advantages in reducing complica-tions from malpositioning. Both valves must be “over-sized,” but the CoreValve in particular seems to workbest when the valve is somewhat underexpanded. Risksof overaggressive sizing include leaflet dysfunction andannular or aortic rupture [110].5.2.5. IMAGING DURING TAVR. The mainstay of intraproce-dural imaging is fluoroscopy and angiography for deviceplacement. TEE is an important adjunct to this and isused at the operator’s discretion. The role of intraopera-tive rotational CT scan is currently in evolution. TEE isused for both transfemoral and transapical deployment,but with transfemoral procedures increasingly being per-formed under local anesthesia combined with conscioussedation [197], the role of TEE in this setting may de-crease, though imaging around the time of valve deploy-ment in this setting is possible [201] and transnasal TEEwith smaller probes may allow prolonged monitoringwithout general anesthesia, though clearly with signifi-cant compromise in comparison to standard TEE. TTEmay also be used for guidance, though image quality islimited. Similarly, intracardiac echocardiography hasbeen reported for TAVR guidance, though imaging ca-pabilities are much less than TEE [202]. Personnel per-forming TEE guidance of TAVR, whether cardiologists oranesthesiologists, must be fully trained in the full spec-trum of transesophageal and intraoperative echo withspecial emphasis on the aortic valve and associatedstructures [203]. Training guidelines indicate the need forinvolvement in 300 intraoperative studies, 150 as anoperator [203]. Additional training is necessary to be-come familiar with the specifics of TAVR. Frequentchanges of the personnel performing TEE guidance dilutesthe learning curve and is not recommended. Patients un-dergoing TAVR tend to be elderly, unstable, and havemultiple comorbidities, and thus attention must not bediverted from critical anesthesia management. It is possiblefor the attending anesthesiologist to provide echocardio-graphic procedural guidance, but in many situations, suchguidance will need to be provided by a dedicated cardiol-ogist or anesthesiologist not distracted by clinical anesthe-sia needs.5.2.5.1. Recommendations for TEE Guidance for PatientsUndergoing TAVR. The following brief recommendationscan be made for TEE guidance of patients undergoingTAVR. More detailed instructions of procedural echocar-diography can be found in a recent expert consensusstatement from the American Society of Echocardiogra-phy and the European Society of Echocardiography [161].
1. Guidewire placement: After confirming annular sizefor proper device selection, TEE can help withguidewire placement. This is particularly importantin transapical TAVR, where manual dimpling of theapex can be visualized and guidewire passagethrough the AV can be confirmed, avoiding the
submitral apparatus or the hypertrophied septum.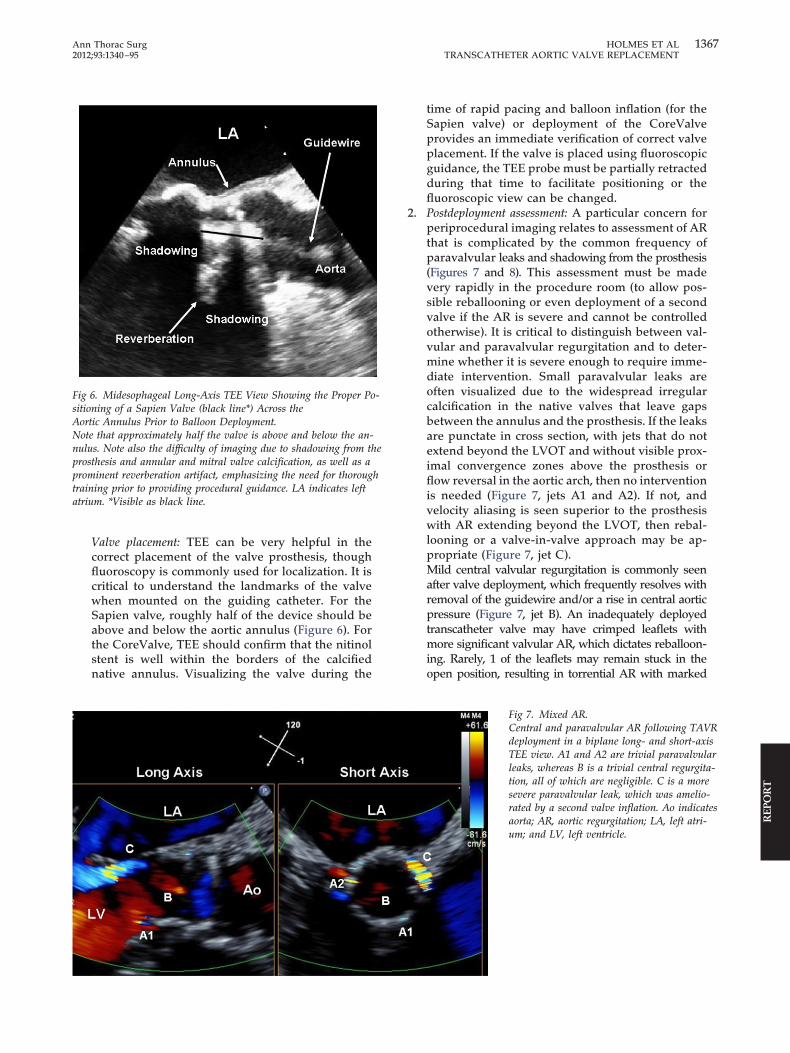
1367Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
Valve placement: TEE can be very helpful in thecorrect placement of the valve prosthesis, thoughfluoroscopy is commonly used for localization. It iscritical to understand the landmarks of the valvewhen mounted on the guiding catheter. For theSapien valve, roughly half of the device should beabove and below the aortic annulus (Figure 6). Forthe CoreValve, TEE should confirm that the nitinolstent is well within the borders of the calcifiednative annulus. Visualizing the valve during the
Fig 6. Midesophageal Long-Axis TEE View Showing the Proper Po-sitioning of a Sapien Valve (black line*) Across theAortic Annulus Prior to Balloon Deployment.Note that approximately half the valve is above and below the an-nulus. Note also the difficulty of imaging due to shadowing from theprosthesis and annular and mitral valve calcification, as well as aprominent reverberation artifact, emphasizing the need for thoroughtraining prior to providing procedural guidance. LA indicates leftatrium. *Visible as black line.
time of rapid pacing and balloon inflation (for theSapien valve) or deployment of the CoreValveprovides an immediate verification of correct valveplacement. If the valve is placed using fluoroscopicguidance, the TEE probe must be partially retractedduring that time to facilitate positioning or thefluoroscopic view can be changed.
2. Postdeployment assessment: A particular concern forperiprocedural imaging relates to assessment of ARthat is complicated by the common frequency ofparavalvular leaks and shadowing from the prosthesis(Figures 7 and 8). This assessment must be madevery rapidly in the procedure room (to allow pos-sible reballooning or even deployment of a secondvalve if the AR is severe and cannot be controlledotherwise). It is critical to distinguish between val-vular and paravalvular regurgitation and to deter-mine whether it is severe enough to require imme-diate intervention. Small paravalvular leaks areoften visualized due to the widespread irregularcalcification in the native valves that leave gapsbetween the annulus and the prosthesis. If the leaksare punctate in cross section, with jets that do notextend beyond the LVOT and without visible prox-imal convergence zones above the prosthesis orflow reversal in the aortic arch, then no interventionis needed (Figure 7, jets A1 and A2). If not, andvelocity aliasing is seen superior to the prosthesiswith AR extending beyond the LVOT, then rebal-looning or a valve-in-valve approach may be ap-propriate (Figure 7, jet C).Mild central valvular regurgitation is commonly seenafter valve deployment, which frequently resolves withremoval of the guidewire and/or a rise in central aorticpressure (Figure 7, jet B). An inadequately deployedtranscatheter valve may have crimped leaflets withmore significant valvular AR, which dictates reballoon-ing. Rarely, 1 of the leaflets may remain stuck in theopen position, resulting in torrential AR with marked
Fig 7. Mixed AR.Central and paravalvular AR following TAVRdeployment in a biplane long- and short-axisTEE view. A1 and A2 are trivial paravalvularleaks, whereas B is a trivial central regurgita-tion, all of which are negligible. C is a moresevere paravalvular leak, which was amelio-rated by a second valve inflation. Ao indicatesaorta; AR, aortic regurgitation; LA, left atri-um; and LV, left ventricle.

1368 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
aortic flow reversal and a short pressure half-time (Fig-ure 8) [204]. In such a case, gentle probing with a softguidewire or catheter may free up the stuck leaflet; ifnot, immediate placement of a second transcathetervalve should be considered. This will be less of an issuewith newer generation valve designs.Postdeployment echocardiography commonly disclosessmall areas of paravalvular or central valvular leak. Mostcommonly, these originate around areas of extremeleaflet calcification, particularly at the commissural ar-eas. If significant, these may be treated with repeatballooning of the prosthesis to further expand it to closeparavalvular leaks or inadequate noncircular deploy-ment. A small additional amount of fluid (1 mL) may beadded to the system prior to reballooning to insurecomplete inflation [110, 205–210]. For CoreValve, indica-tions are similar—significant paravalvular leak with ARand underexpanded prosthesis (assessed by TEE and/orfluoroscopy).There are a number of other complications that mustbe recognized immediately after TAVR if poor clinicaloutcome is to be averted. Persistent hypotension mayresult from occlusion of a coronary artery by thedevice or displaced calcium. This can be recognizedby characteristic regional hypokinesis, best appreci-ated from the transgastric view and possibly by eval-uating flow in the coronary arteries themselves.Global dysfunction with preserved coronary flowmay reflect persistent depression from rapid pacingand balloon inflation, requiring inotropes and possi-bly intra-aortic counterpulsation or full bypass. Fi-
Fig 8. Severe AR.Long-axis TEE view showing severe AR fol-lowing TAVR deployment (Panel A), con-firmed by flow reversal in the descendingaorta (Panel B). Short axis imaging (Panels Cand D) demonstrates that this is due to failureof the leaflet in the left coronary position (ar-row) to close in diastole, ultimately treated bydeploying a second valve inside this one. Aoindicates aorta; AR, aortic regurgitation; LA,left atrium; and LV, left ventricle.
nally, hypotension may result from LVOT obstruction
following the abrupt fall in afterload, requiring vol-ume, negative inotropes, and vasopressors. Otheretiologies such as severe MR, dislodgement of the AVprosthesis, pericardial tamponade, RV perforationfrom the pacemaker lead, air embolism, vascularaccess bleeding, and aortic dissection must be consid-ered. Although TEE is very helpful for initial deviceplacement and deployment, it is in the setting ofhemodynamic instability that TEE is essential to rap-idly diagnose these complications.
5.2.5.2. Balloon Dilation and Size. Prior to passage of thevalve, predilation of the annulus is performed. Standardtechniques of percutaneous balloon aortic valvuloplastyare employed, with rapid pacing during inflation. Radio-graphic contrast opacification of the root during maximalinflation may provide useful information when the loca-tion of the coronary ostia in relation to the annulus andthe leaflet calcification or any other aortic root pathologyrequires further delineation. The valvuloplasty balloon sizeused is generally 20 mm to 23 mm, depending on the size ofthe annulus [110, 211, 212].
5.2.5.3. Rapid Pacing. Rapid ventricular pacing is gener-ally required for deployments with balloon-expandingdevices. The goal is to create a transient reversibledecrease in ventricular ejection, thereby reducing forcesleading to valve migration during deployment. Typically,this requires pacing at a rate of 160 to 220 beats/min.Ideally, there should be a decrease in systolic pressure to�70 mm Hg, with a pulse pressure �20 mm Hg. Pacing is
accomplished by either transvenous or, less frequently,
1369Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
epicardial electrodes. Reducing the number and durationof pacing runs is important in this tenuous patientpopulation to prevent instability [110, 213].
5.2.5.4. Experience With TAVR. An important issue inevaluating the results of TAVR is standardization ofdefinitions for success, as well as efficacy. The VARCConsortium has proposed the definitions for device suc-cess, combined safety endpoint at 30 days, and thecombined efficacy endpoint at 1 year or longer (Table 11)[96]. Application of these standard definitions will facili-tate comparability and analysis of outcome betweendifferent registries and studies. Another important issueon outcomes as well as learning curves relates to theexperience of the center, patient selection criteria, andthe expert onsite technical support provided by thecompanies in each case. For example, the UK TAVRexperience documented similar results with proctoredand nonproctored cases, as well as the first 20 casesversus continued cases in each center. This finding mustbe considered in light of the fact that the review ofpotential cases is influenced by the experience that otheroperators and centers have gained. The presence of theindustry representatives in the procedures is also aninvaluable asset in recognizing the potential for compli-cations and treatment of same. These 2 backgroundissues enhance the chance of success and may havecontributed to the accelerated learning curve [115].
Compared with patients who underwent TAVR earlyafter its introduction, patients treated more recently havebenefited from shared experiences, more careful patientselection, advances in equipment and technique, andexpanded operator experience. Prior reports have dem-onstrated a steep learning curve with TAVR using theCoreValve and Sapien valves [214–217]. Whether im-
Table 11. Composite Endpoints
Device Success● Successful vascular access, delivery and deployment of th● Correct position of the device in the proper anatomical lo● Intended performance of the prosthetic heart valve (aortic
peak velocity, 3 m/s, without moderate or severe prosthet● Only 1 valve implanted in the proper anatomical location
Combined Safety Endpoint (at 30 Days)● All-cause mortality● Major stroke● Life-threatening (or disabling) bleeding● Acute kidney injury—Stage 3 (including renal replacemen● Periprocedural MI● Major vascular complication● Repeat procedure for valve-related dysfunction (surgical o
Combined Efficacy Endpoint (at 1 Year or Longer)● All-cause mortality (after 30 days)● Failure of current therapy for AS, requiring hospitalization● Prosthetic heart valve dysfunction (aortic valve area 1.2 cm
m/s, OR moderate or severe prosthetic valve AR)
AR � aortic regurgitation; AS � aortic stenosis.
Reprinted with permission from Leon et al [96].
proved operator experience alone can improve certainoutcomes more than others remains unclear.
Since its introduction, increasing experience with the Cor-eValve TAVR revealed a trend of improved combined safetyendpoint at 30 days from 30% to 17%, predominately drivenby a reduction in life-threatening periprocedural bleedingcomplications occurring from TAVR [215]. The most recentUK experience [115] identified a 30-day mortality of 5.8%.Furthermore, there was a significant reduction in cerebrovas-cular complications. Despite these trends, all-cause and CVmortality at 1 and 2 years remain high. Experience using theEdwards Sapien valve, on the other hand, revealed that, in 1analysis, procedural experience was an independent predictorof 30-day mortality [214]. The overall combined 30-day mor-tality decreased with increased experience, 10.5% to 8.5%.Procedural success rates also improved from 92.6% to 97.8%with time, predominately in the transfemoral approach, 89.3%to 98.8%.
Overall, consistent with other percutaneous thera-pies, the evidence demonstrates that procedural suc-cess and mortality rates improve with experience,whereas periprocedural complications are reduced.The introduction of smaller valve platforms introducessome uncertainty in defining whether the improvedoutcomes are solely related to the operator’s experi-ence. Nonetheless operational volumes of given indi-viduals and centers are critical to consider. Currenttraining protocols attempt to accelerate the learningcurve by utilizing experienced proctors and didacticteaching, represented in both the PARTNER and Cor-eValve trials. If the learning curve can be truncated,procedural outcomes may continue to improve even asmore operators enter this clinical arena. Specific crite-ria regarding operator and center training and experi-
ice and successful retrieval of the delivery system
e area 1.2 cm2 and mean aortic valve gradient, 20 mm Hg orve AR)
rapy)
erventional therapy)
symptoms of valve-related or cardiac decompensationd mean aortic valve gradient �20 mm Hg or peak velocity �3
e devcation
valvic val
t the
r int
for2 an

1370 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
ence are the focus of a multisocietal credentialingdocument [218].
5.3. Complication ManagementComplications with TAVR are fairly common due to boththe complexity of the procedure, as well as the morbidityof the patients being treated (Table 12). This has led todevelopment of new tools and techniques to manage
Table 12. TAVR Complications and Management
Complication
Management Options Dependingon the Clinical Condition,
Hemodynamic Status, and Numberof Options Available
Shock, low cardiacoutput
● Careful systemic pressuremanagement, inotropic support,IABP, or CPB
Occlusion of coronaryostia
● PCI or CABG
Significant annularrupture
● Pericardial drainage,autotransfusion, conversion toopen surgical closure.
● If no other options, care andsedation
Ventricular perforation ● Pericardial drainage,autotransfusion, conversion toopen surgical closure.
Paravalvular aorticregurgitation
● Postdeployment balloon dilation
Central valvular aorticregurgitation
● Usually self-limited, but mayrequire gentle probing of leafletswith a soft wire or catheter
● Delivery of a second TAVR device
Heart block ● Pacemaker implantation
Device malpositionDevice embolization
● Deployment of overlapping 2ndvalve
● Urgent endovascular or surgicalmanagement
Atrial fibrillation ● Rate control, rhythm control viapharmacological or electricalcardioversion
Major ischemic strokeMinor ischemic strokeHemorrhagic stroke
● Catheter-based, mechanicalembolic retrieval
● Aspirin, anticoagulants● Reversal of anticoagulation,
correction of coagulopathy
Major bleeding ● Hemodynamic support, bloodtransfusion
Vascular complications ● Urgent endovascularrepair/surgery
Acute kidney injury ● Supportive care● Maintain optimal fluid status
Each of the management options mentioned should be at least consideredin the treatment of these complications.
CABG � coronary artery bypass graft; CPB � cardiopulmonary by-pass; IABP � intra-aortic balloon pump; PCI � percutaneouscoronary intervention.
these complications [219].
5.3.1. SHOCK, LOW CARDIAC OUTPUT POST-TAVR. The noncompli-ant hypertrophied ventricles in these patients are verysusceptible to myocardial ischemia. The combination ofanesthesia, rapid pacing, volume shifts, and brief periodsof no cardiac output have made hemodynamic shock andlow cardiac output a not infrequent occurrence duringand immediately after deployment.
The need for careful management of systemic pressure,inotropic support, and optimal ventilation to avoid and miti-gate PH is clear. In patients at extreme risk for hemodynamicinstability (i.e., those with low EF, collateral dependent coro-nary circulation, or PH), elective cardiopulmonary bypass(CPB) has been used to facilitate the procedure. Not infre-quently, IABP support may be required to bridge these pa-tients to adequate cardiac output. Also rare, but reported, isocclusion of coronary ostia by deployment (approximately 1%of cases). These may be addressed at times percutaneously,but may require CPB support for brief periods to allowrecovery. Using a combination of these techniques, cardiacfailure as a cause of death in TAVR has been rare [109,220–224]. Rarely, “suicide” LV can occur and must be lookedfor. This occurs in patients with combined AS and subaorticstenosis or severe LV hypertrophy and cavity obliteration [109,224, 225]. The situation is exacerbated by diuresis and ino-tropes and is instead managed with volume expansion andbeta blockade.
5.3.2. ANNULAR RUPTURE. Annular rupture is a rare but dev-astating complication of TAVR. Predisposing factors in-clude bulky and dense calcification, small sinotubular junc-tion, smaller annular size, aggressive balloon predilation,and possibly porcelain aorta. Once seen, mortality is high.Management can include decisions for comfort care andsedation, attempts at medical management with pericardialdrainage and autotransfusion of smaller leaks, and emer-gent conversion to open operation, which makes it evenmore important to define and plan for or against thispossibility in patients in a “high-risk” substrate [226].
5.3.3. POST-TAVR AORTIC REGURGITATION. Post-TAVR AR mustbe characterized as to its location, severity, and cause andshould integrate both central and paravalvular origins toestimate overall volumetric impact. Central regurgitationis generally a result of improper valve deployment orsizing. Heavy guidewires through the valve can cause asubstantial leak by holding a leaflet open, and full eval-uation of central leak can only be undertaken once thesewires are removed. Overhanging leaflet material canchange the diastolic flow pattern and lead to improperleaflet closure. Damage to the leaflets can occur duringcrimping; significant central AR requires rapid consider-ation of a valve-in-valve deployment.
Paravalvular leaks of varying degrees are common. Theseare generally caused by inadequate inflation of the prosthesisor by calcific deposits that prevent the valve unit to properlyseat and seal within the annulus. Acute leaks may respond torepeat ballooning the valve to obtain a better seal and moreexpansion. Predisposing factors include eccentric calcificationand heavy irregular calcific deposits within the annular area,
and incorrectly sized prostheses. In addition, an increased
1371Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
LVOT angulation in relation to the aorta, and a valve seatedless deeply in the annulus predispose to paravalvular leak.Paravalvular regurgitation is quite common immediately post-TAVR, occurring at an incidence of 85%. At 1 year, up to 75%still have mild or more paravalvular regurgitation, and onethird have more than mild regurgitation.
The incidence of residual mild or moderate AR (�1 and�2) is significantly higher in TAVR patients compared withsurgical procedures, whereas hemodynamically severepostprocedural AR (�3 and �4) is rare. Experience hasdemonstrated that aortic paravalvular regurgitation afterself-expanding TAVR devices can be reduced by sufficientballoon aortic valvuloplasty prior to deployment of a per-cutaneous prosthesis for self-expanding valves. Occasion-ally in heavily calcified valves, repeat balloon dilation aftervalve deployment is needed to fully expand the prosthesis.Post-valve dilation can be performed safely with a slightlyoversized balloon, without causing significant structuraldamage to the prosthesis. Appropriate preprocedural plan-ning utilizing both echocardiography and CT for annularanalysis is important in order to avoid undersizing of thevalve compared with the annulus because this can alsocause significant paravalvular regurgitation.
Acute postprocedural regurgitation requires continuedsurveillance because regurgitation may change in the sub-sequent days post-TAVR. The self-expanding properties ofthe stent in the CoreValve prosthesis may reduce the gradeof paravalvular AR or recoil from the compressive forces ofthe heavy calcification on either prosthesis may worsen thedegree [227, 228]. Clinical concern about the impact ofparavalvular regurgitation after TAVR is prudent, given thefindings that after surgical AVR, patients with moderate-severe or severe AR develop chronic volume overload thatcan lead to left ventricular remodeling/dysfunction andincrease the risk for hemolysis. At the present time, there isnot sufficient long-term follow-up after TAVR to under-stand the clinical significance of paravalvular regurgitationand whether the severity of paravalvular regurgitationprogresses with time. However, it is clear that postproce-dural regurgitation is associated with adverse outcomes[109, 225]. There are no reported cases of hemolysis withTAVR despite paravalvular AR.
5.3.4. POST-TAVR HEART BLOCK. TAVR is associated with avariable incidence of complete heart block and/or needfor pacemaker implantation [132, 227–231]. This is muchmore common in CoreValve recipients [227–231]. Preop-erative conduction delay is associated with an increasedincidence of permanent pacemaker implantation as well.Although heart block occurs usually early after TAVR, itmay be delayed up to 30 days. Enhanced surveillance forthis complication is important, particularly if the patientsare dismissed early following the procedure.
5.3.5. POST-TAVR DEVICE MIGRATION/MALPOSITION. Rarely,TAVR devices will become malpositioned or migrate. Inthe self-expanding models, they can be moved to somedegree until fully deployed. The balloon-expandablemodels do not enjoy this degree of flexibility with posi-
tioning. A malpositioned valve may be “unstable” or mayembolize. If the valve is unstable, rapid placement of asecond overlapping valve may salvage the procedure.Valves embolizing distally may occasionally be extractedin the aorta and a second device implanted. Ventricularembolization requires urgent surgery [185, 232, 233].
5.3.6. VENTRICULAR AND VASCULAR PERFORATION. Ventricularperforation is a rare complication of transfemoral TAVR.Its management is similar to that for this complicationduring percutaneous balloon aortic valvuloplasty, withpericardial drainage and autotransfusion or conversionto open closure. Large-vessel aortoiliac injury similarly isuncommon, but if present, can be managed in most casesby introduction of a covered stent. Some operators place aguidewire down the leg from the contralateral femoralartery for rapid access and control. Readiness for vesselrupture with occlusion balloon cannot be overemphasized.Preparation for this complication is critical with preplan-ning. It is best managed by avoiding it. Careful mainte-nance of a good wire position and use of a stiff wire with asoft tip are helpful in prevention of perforation duringTAVR [234].
5.4. Postprocedural Care5.4.1. POSTPROCEDURAL RECOVERY. Designated units for post-procedural recovery are imperative for optimal care andbetter outcome of this group of high-risk patients under-going TAVR [221]. Although the particulars of postpro-cedural care will vary from institution to institution andcountry to country, as well as with the maturity of theTAVR program, the principles of care remain the samethat these complex patients should be treated in postpro-cedural units experienced with both cardiac surgical andinterventional cardiology procedures.5.4.1.1. Recommendations for Procedural Care After TAVR.
1. Immediate or early extubation, early mobilization, andmeticulous attention to the many potential complica-tions in this elderly, frail group of patients.
2. Post-anesthetic care unit (PACU) or intensive care unit(ICU). There should be a common care pathway with allpatients cared for in the same setting so that the careteam is conversant with the care pathway. The criteriafor weaning in a fast-track concept are as follows:a. Adequate core temperature of �36°Cb. Hemodynamically stablec. No active bleeding from drainage site
3. The care is somewhat different for transapical andtransfemoral patients. Prevention of postoperative hy-pertension and hypertension upon tracheal extuba-tion is crucial in patients undergoing transapicalTAVR to decrease the risk of bleeding or ventricularrupture. Patients undergoing transapical TAVR alsorequire postoperative analgesia for thoracotomy inci-sional pain and management of thoracostomy tubedrainage and subsequent thoracostomy tube removal.Transfemoral TAVR patients require supine position-ing until femoral vascular access sheaths are removed
and hemostasis has been achieved. Patients undergo-
1372 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
ing direct aortic and subclavian approaches also needto be carefully monitored for any mediastinal/thoracicbleeding with particular attention paid to avoidingpostoperative hypertension.
4. The monitoring includes vital parameters includingfluid balance therapy, renal status, and atrioventricu-lar conduction system. Adequate hydration and avoid-ance of early diuretic administration is important tominimize renal failure. Completion of perioperativesurgical antibiotic prophylaxis, resuming preoperativemedications such as beta blockers, and initiation ofprophylaxis for venous thromboembolism should beaddressed within the first 24 hours after operation. Apain management regimen should be initiated imme-diately if necessary after operation in the postproce-dural unit and may consist of intercostal nerve block,infiltration of the wound with local anesthetics, nar-cotics, or non-narcotic analgesics. Epidural analgesiais not normally required for transapical TAVR becausethe thoracotomy incision is limited and satisfactorypostoperative pain control can be achieved with par-enteral or patient-controlled analgesics. Patients un-dergoing transfemoral TAVR should be evaluated forlower extremity vascular insufficiency, groin hema-toma, retroperitoneal bleeding, and femoral arterypseudoaneurysm formation in the instrumented limb.
5. When stable, patients should be transferred to atelemetry unit with hemodynamic and electrocardio-graphic monitoring capability. The duration of moni-toring will depend on the patients response to TAVRand the specific prosthesis used. There are differencesin the need for permanent pacemaker implantationbetween the Edwards Sapien and Medtronic Cor-eValve device with rates being lower with the former;accordingly, longer electrocardiographic monitoringmay be required after implantation of the latter [132].Depending on institutional protocols, patients shouldbe discharged from the hospital after a final examina-tion with TTE. Antiplatelet therapy with aspirin andclopidogrel is recommended to decrease the risk ofthrombotic or thromboembolic complications if thereare no contraindications to these medications [235].
5.4.2. HEMODYNAMIC ASSESSMENT. Echocardiographic assess-ment early after TAVR generally reveals a favorablehemodynamic response, with the presence of a signifi-cantly lower mean transvalvular gradient and a largereffective orifice area (EOA), usually �10 mm Hg and �1.5cm2, respectively. Techniques used for assessment of aorticvalve performance vary. The use of measurements of theleft of the LVOT diameter and velocity immediately proxi-mal to the stent has been emphasized [236]. At short- andlong-term follow-up, percutaneously implanted valves pro-vide sustained improvements in hemodynamic perfor-mance with slightly lower mean transvalvular gradientsand larger EOAs than surgically implanted valves, eitherstented or stentless [237].
Postprocedure hemodynamic assessment is particularlyimportant to exclude potential prosthesis complications.
Transcatheter aortic valves differ, not only in design, butalso in implantation technique from surgical AVR. TAVRpreserves the native calcified aortic valve compared withsurgical AVR, which requires that the native valve beremoved prior to prosthesis implantation. The native valveand annular calcification may potentially prevent the ad-herence of the prosthesis to the aortic wall, whereas lowprosthesis deployment into the LV outflow tract may lead toincomplete and/or irregular expansion of the prosthesis, aswell as paravalvular prosthetic leak.
An additional concern is severe patient–prosthesis mis-match, which is defined as an effective orifice area index�0.65cm2/m2 [238]. Patient–prosthesis mismatch in surgicalAVR is associated with a reduction in functional status andincreased morbidity and mortality at short-term and long-term follow-up [239, 240]. The stent in TAVR prosthesis isthinner than that of the stented valves employed for surgi-cal AVR, minimizing the obstruction to blood flow andreducing the incidence of patient–prosthesis mismatch.Whether reduced rates of patient–prosthesis mismatch willtranslate to improved functional status and improved sur-vival remains to be defined.
5.4.3. ATRIAL FIBRILLATION. The incidence of new-onset atrialfibrillation (AF) after successful TAVR ranges from 0.6% to8.6% [15, 124, 132, 241]. However, over 25% of patientsundergoing TAVR have pre-existing AF. Continuouspostprocedural electrocardiogram monitoring should beperformed for at least 3 days in all patients after trans-catheter therapy. Management of atrial fibrillation post-TAVR is based on the ACC/AHA/ESC guidelines formanagement of atrial fibrillation [242].
5.4.4. TREATMENT OF STROKE. The treatment of a stroke willdepend on the subtype of stroke diagnosed by brainimaging, timing of the event after any procedure, and theseverity of the neurological deficit. A large intracerebralhemorrhage could call for reversal of any anticoagulantsand correction of any coagulopathy with fresh-frozenplasma or other transfusions [243]. The diagnosis of anacute ischemic stroke with moderate to severe neurolog-ical deficits may require thrombolysis or mechanical clotretrieval depending on the size, location, and whetherany major intracerebral artery is occluded. An in-hospitalstroke within 8 hours of the onset of neurological symp-toms usually requires urgent consultation by a strokeneurologist or neurosurgeon. Angiography and strokeintervention may be recommended for large and/or dis-abling strokes. These treatments are generally availableat comprehensive stroke centers. Typical embolic strokesin this setting are the result of calcific emboli. If the strokeis the result of thromboembolism, local rt-PA may beconsidered although bleeding risk in this elderly popu-lation is very high.
Minor strokes, small infarcts on brain imaging, or theabsence of any evidence of any major cerebral vesselocclusions can usually be treated with aspirin [244]. Ifatrial fibrillation is present, then institution of an oralanticoagulant program is warranted [129]. If any intra-cardiac thrombus is detected, then early institution of
heparin followed by oral anticoagulants is suggested
1373Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
[63]. When the patient is stable, other diagnostic eval-uations should be done to evaluate for other potentialcauses of stroke, including vascular imaging to detectany extracranial carotid or vertebral stenosis or intra-cranial occlusive disease, echocardiography, andHolter monitoring. If no definite source of cardiacembolism is detected, then long-term treatment withantiplatelet options to prevent recurrent stroke may beinstituted, which include aspirin, extended-release di-pyridamole, and clopidogrel [129].
5.5. Long-Term Care5.5.1. ROLE OF PRIMARY CARDIOLOGIST. The long-term care ofthe patient after TAVR will be mainly guided by theprimary referring cardiologist. In contrast to patientsundergoing surgical AVR, patients undergoing TAVRtend to be older, with more severe comorbidities andlower functional status, mandating more frequent cardi-ology follow-up.
The role of the primary cardiologist is to:
1. Prescribe and monitor medical therapy for concur-rent cardiovascular disease, including hyperten-sion, atrial fibrillation, heart failure, CAD, andperipheral and cerebrovascular disease, as well asdiabetes and dyslipidemia.
2. Prescribe and monitor antithrombotic and/or anti-platelet therapy as recommended for the prostheticaortic valve and concurrent conditions such ascoronary stents or atrial fibrillation.
3. Monitor cardiac and TAVR function with periodicclinical evaluation and echocardiography.
4. Surveillance for and treatment of early and lateprocedural-related complications
5. Maintain close communication with the implantingphysicians if complications occur that may be re-lated to the procedure.
5.5.2. FOLLOW-UP VISITS. The patient should be followedclosely by the implanting physician team for the first 30days after TAVR to diagnose and follow any proceduralcomplications. Evaluations should include a post-TAVRbaseline echocardiogram and ECG (to document anyconduction abnormalities) occurring during that timeperiod. After 30 days, a suggested schedule for follow-upby the primary cardiologist is noted in Table 13.
Follow-up is then continued at the first 6 months, at1 year, and annually thereafter. The frequency offollow-up evaluations should be increased if there issignificant post-TAVR paravalvular leak or any change
Table 13. Recommended Patient Follow-Up Post-TAVR
Timing Post-TAVR Clinical Evaluation Echocardiography
30 days X X6 months X1 year X XAnnually thereafter X X
TAVR � transcatheter aortic valve replacement.
in clinical status or echocardiographic findings. Asexperience grows with TAVR, the frequency of echo-cardiography assessment will likely decrease towardsthat of surgical AVR, deemed appropriate every 3 years[245]. Additional diagnostic studies may be consideredas clinically warranted, including evaluation for coro-nary disease if symptoms are present.
5.5.3. HEMODYNAMIC EVALUATION. Hemodynamic evaluationshould be performed by echocardiography as indicatedin Section 5.5.2 above. Invasive measurement of LV andaortic pressure is not routinely needed unless there areunresolved questions, discrepancies between echocar-diographic and physical examination findings, or otherunresolved clinical issues.
5.5.4. INTERACTION OF CO-TREATMENTS. Given the frequencyof coexisting conditions, multiple antiplatelet or antico-agulant strategies may be required. For example, somepatients may be receiving antiplatelet therapy for acoronary stent or antithrombotic therapy for atrial fibril-lation. This is complicated by the fact that most patientsundergoing TAVR are elderly and often have comorbidi-ties that increase bleeding risk. It is prudent to avoid, ifpossible, the use of multiple anticoagulant therapies. Inpatients treated with warfarin, a direct thrombin inhibi-tor, or Factor Xa inhibitor, it is reasonable to continuelow-dose aspirin, but other antiplatelet therapy shouldbe avoided, if possible.
5.5.5. MANAGEMENT OF AR. AR after TAVR typically is para-valvular and most often only mild or mild to moderate inseverity. At 1-year follow-up, 13% of patients have no AR,with only trace or mild regurgitation in 80% of patients[15, 124]. These patients do not require any specifictherapy for AR other than medical therapy for concurrenthypertension and periodic echocardiography monitoringas described above.
Moderate or severe AR is present after TAVR (evenafter interventions during the procedure to reduce ARseverity) in about 12% of patients at 30 days and 7% at1-year follow-up [15, 124].
5.5.5.1. Recommendations for Managing Severe AR AfterTAVR.
1. When severe AR is present after TAVR, treatmentis similar to native valve AR as detailed in theACCF/AHA valvular heart disease guidelines [63].
2. With acute severe AR or chronic severe AR withsymptoms of heart failure, surgical AVR may beconsidered if the patient is a surgical candidate andsurgical risk is acceptable. Other options includeplacement of a second TAVR within the leakingprosthesis (“valve-in-valve”).
6. Technology Evolution
Next-generation devices promise the potential for im-provements, offering expanded clinical utility with ad-
vances that include: lower profile delivery catheters,
ble
14.
TAV
RV
alve
Type
san
dQ
ualit
ies
vice
Com
pan
yE
xpan
sion
Mec
han
ism
Val
veM
ater
ial
Sten
tM
ater
ial
Rep
osit
ion
able
Ret
riev
able
Clin
ical
Tri
als
FIM
CE
Mar
kFr
ench
Size
libri
Hea
rtV
alve
En
dol
um
inal
Tec
hn
olog
yR
esea
rch
Bal
loon
-an
dse
lf-
exp
and
able
Per
icar
diu
mSt
ain
less
stee
l/N
itin
olN
oN
oN
o20
03N
oB
allo
on:1
6Se
lf:1
2ec
tFl
owD
irec
tFl
owM
edic
alP
olym
er-i
nje
cted
Per
icar
diu
mP
olym
erY
esN
oN
o20
06N
o22
tus
Sad
raM
edic
alSe
lf-e
xpan
dab
leP
eric
ard
ium
Nit
inol
Yes
No
No
2007
No
21aV
alve
Jen
aVal
veT
ech
nol
ogy
Self
-exp
and
able
Per
icar
diu
mN
itin
olY
esN
oN
o20
07Y
es28
art
Lea
flet
Hea
rtL
eafl
etT
ech
nol
ogie
sSe
lf-e
xpan
dab
leP
eric
ard
ium
Nit
inol
Yes
Yes
No
N/A
No
16
tter
N/A
Self
-exp
and
able
Tis
sue
engi
nee
red
Nit
inol
No
No
No
N/A
No
N/A
rcV
alve
Ad
van
ced
Bio
pro
sth
etic
Surf
aces
Self
-exp
and
able
e-N
itin
ole-
Nit
inol
No
No
No
N/A
No
10
rtic
oSt
.Ju
de
Self
-ex
pan
dab
leP
eric
ard
ium
Nit
inol
Yes
Yes
Yes
2011
No
22u
rate
Sym
etis
Self
-exp
and
able
Per
icar
diu
mN
itin
olY
esY
esY
es20
09Y
es28
�C
onfo
rmit
éE
uro
pée
nn
e,a
man
dat
ory
con
form
ity
for
pro
du
cts
pla
ced
onth
em
arke
tin
the
Eu
rop
ean
Eco
nom
icA
rea;
FIM
�fi
rsti
nm
an;
N/A
�n
otap
plic
able
;T
AV
R�
tran
scat
het
erao
rtic
vere
pla
cem
ent.
difi
edfr
omC
hia
man
dR
uiz
[94]
.
1374 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
more accurate positioning, reduced paravalvular leak,and ability to either reposition or even retrieve (Table 14)[246]. Many of the new device technologies utilize aself-expandable, high radial strength repositionableprosthesis consisting of pericardial tissue on a nitinolframe. Two additional valves have recently receivedapproval for commercial sale in Europe. The JenaValve(JenaValve Technology, Munich, Germany) and AcurateValve (Symetis, Inc., Lausanne, Switzerland) are bothdelivered currently via a transapical approach.
Other valve designs currently in early clinical stud-ies include Portico Valve (St. Jude Medical, St. Paul,MN), Direct Flow Medical (Direct Flow Medical, SantaRosa, CA), and Sadra Lotus Valve (Sadra Medical, LosGatos, CA). Other new designs include flexible sealingmembranes aimed at more optimal conformation tothe calcified native annulus to reduce paravalvularleaks. New valve designs and materials can also pro-vide the possibility of new prosthesis technology. TheLutter valve was created in an effort to create a morephysiological heart valve by utilizing tissue engineer-ing [247]. The PercValve (Advanced Bioprosthetic Sur-faces, San Antonio, TX) uses nanotechnology in itselastic nitinol frame and leaflets. These leaflets aredesigned to allow for the growth of endothelial cells,essentially converting it to a tissue valve. Initial animalstudies have shown complete endothelialization of thee-nitinol leaflets within 10 days and may eliminate theneed for anticoagulation [248]. A final novel approachinvolves anchoring the prosthesis by using an inject-able polymer that cures in position to maintain theimplant permanently in place. The outcome with thesenew technologies will be the focus of multiple regis-tries and then randomized trials.
7. Applications in New Patient Populations andNew Study Designs
As experience is gained and technology evolves, thepatient population best served with TAVR is likely tochange, and 3 areas that merit specific consideration arethe “valve-in valve” technique for patients with dysfunc-tional aortic bioprostheses, the use of TAVR in patientswith stenotic bicuspid aortic valves, and application tolower-risk surgical patients. Other patient populations,such as those with chronic or end-stage renal disease,may also be candidates for this technology and will bethe subject of future investigations.
7.1. Valve-in-ValvePatients with dysfunction of a conventional aortic pros-thesis present therapeutic challenges. Although repeatoperation can be considered, an attractive option is to usea TAVR procedure in which the device is deployedwithin the previously placed bioprosthesis [209, 249–254].In multiple small series, transcatheter aortic valve-in-valve implantation appears to be a safe option for themanagement of bioprosthetic valve failure in patients athigh risk for reoperative conventional AVR. In this set-
ting, coronary anatomy should be carefully defined in Ta De
Co
Dir
Lo
Jen
He
Lu
Pe
Po
Ac
CE
val
Mo

1375Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
order to minimize the possibility of coronary obstructionby the transcatheter prosthesis [209, 220, 250, 255]. Inaddition, valve-in-valve procedures require a largeenough bioprosthetic valve inserted at the index opera-tion to prevent patient prosthetic mismatch with theTAVR valve.
7.2. Bicuspid Aortic ValveThe asymmetric valvular anatomy often seen with abicuspid aortic valve theoretically predisposes to anoncircular expansion of the TAVR device, therebycreating an increased risk of paravalvular regurgitation[256].
Because of this concern, the presence of a bicuspidaortic valve is considered a relative contraindication toTAVR. Since bicuspid aortic valve patients have gener-ally been excluded from major TAVR trials, there is littleclinical experience in this area. Several centers, however,have achieved reasonable success in selected bicuspidaortic valve patients with AS [163, 256, 257]. It should benoted that in the Canadian bicuspid aortic valve experi-ence, moderate paravalvular leaks occurred in 2 of 11patients, and another patient experienced late devicemigration [256]. Bicuspid aortic valve patients with bulkyleaflets, markedly asymmetric valvular anatomy, andsignificant aortic incompetence appear to have a higherrisk of suboptimal device seating. Whether new valvedesigns, perhaps those with self-sealing membranes, willimprove device performance in this group remains to bedetermined.
7.3. Lower-Risk PopulationsData from the STS Registry indicate that approxi-mately 10% of patients undergoing AVR have an STSscore �8 and therefore would be potential candidatesfor TAVR using current selection criteria. There hasbeen interest in expanding the potential group ofcandidates for TAVR to include patients with an STSscore �4. This would broaden to 25% the number ofpatients who might be treated with TAVR rather thanAVR. There has been concern about the potential for“selection creep,” with more lower-risk patientstreated with TAVR. This should be avoided until moreevidence-based data become available on the outcomeof TAVR versus AVR in these patients. The plannedand ongoing trials evaluating both the Sapien and theCoreValve in lower-risk populations will be of centralimportance in identifying subsequent utilization of thistechnology in expanded patient groups.
8. Introduction of TAVR Into Practice:U.S. Versus European Perspective
8.1. U.S. PerspectiveThe U.S. perspective reflects the fact that TAVR approvalrequired a randomized controlled trial, the full extent ofwhich has just now been published [124]. This contrastswith Europe where 5 new valves or iterations of current
valves are already in relatively widespread clinical use.Accordingly, from the U.S. perspective, the rollout of thistechnology is a key issue. This rollout is influenced by thesocietal beliefs in a free market; convenient and timelyaccess to medical care; patient and physician expecta-tions; as well as return on investment by companies andinstitutions alike. These latter issues have led to theproliferation of advanced cardiovascular facilities, whichcould complicate the rollout of new-device strategiessuch as TAVR. For example, the state of California alonehas 125 facilities that perform percutaneous coronaryintervention, the county/city of Los Angeles has 33 car-diovascular surgical and primary ST-elevation myocar-dial infarction centers. The Dallas–Fort Worth Metropol-itan region also has 33 full-service cardiovascular surgicalcenters. To plan for each of these centers in either LosAngeles or the Dallas–Fort Worth region to offer TAVRwould result in the dilution of concentrated experience.Thus, for a complicated procedure such as TAVR, whichis applied in some of the highest-risk patients treated forcardiovascular disease, such as those enrolled in thePARTNER and CoreValve trials, setting up specializedcenters of excellence should be a top consideration foroptimizing patient care and outcomes.
The concept of development of these specialized heartcenters is likely to be somewhat controversial, given theexpectation in the United States that each hospital withexperienced personnel should be able to perform anyand all indicated procedures. However, results of TAVRare likely to be optimal when performed by a heart teamof experienced surgeons, structural interventional cardi-ologists, and CV imaging specialists working together inhigh-volume tertiary care centers with ancillary supportservices capable of dealing with very complex patientswith advanced comorbid conditions. For detailed recom-mendations, please refer to the Multisocietal PositionStatement on Operator and Institutional Requirementsfor TVRR [218]. The specific details of the U.S. rollout andreimbursement for this procedure are as yet to be fullydetermined. The criteria for regulatory approval andreimbursement by appropriate federal agencies shouldbe based upon expertise; high, adjudicated procedurevolumes; and documentation of a healthcare team ap-proach. In addition, mandatory enrollment in structuralheart disease registries should be required so that short-and longer-term outcomes can be assessed and updatedwith new evolving data.
8.2. European PerspectiveAdoption of TAVR has been rapid, and the changingtrends in Europe have escalated; in selected centers inGermany, TAVR accounts for over 30% of all AVRs. Forexample, 1 single center has an experience of more than1,300 TAVRs and has trained more than 360 doctors inover 32 centers from more than 30 countries. Germanyitself has approximately 87 centers performing TAVR.The miniaturization of the applicator device, the optionto implant newer valves from different manufacturers,and the need for high-quality intraoperative imaging arechallenges consistent with the high costs involved with
these procedures. Reimbursement varies in different
1376 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
countries. In general, at present, the insurance providersin Europe are bearing the high costs involved in theseoperative procedures which may be questioned in thefuture, unless outcomes of improved long-term survivalare available. The United Kingdom approach to thedevelopment of active TAVR centers has recently beendescribed and can serve as a model for other countries.This rollout included 2 specific technologies (i.e.,Medtronic CoreValve and Edwards Sapien). The devel-opment of this program consisted of didactic session,simulator training, observation of cases at experiencedcenters, and proctoring at new centers. Core essentials ofthe program included a multidisciplinary team processfor patient selection and for procedural performance. Allpatients undergoing TAVR were entered into a CentralCardiac Audit Database, which included clinical as wellas administrative data using standardized data elementsand definitions. This approach has the advantage ofincluding all patients with either of the 2 devices, moni-toring the potential of changing patient selection criteria,the ability to document learning curve and the opportu-nity to evaluate the outcome of patients treated with eachof the devices. Particularly relevant findings include theobservation that: 1) 30-day and mid-term mortality wasequivalent in proctored and nonproctored cases; and 2)the fact that outcomes in the first 20 cases were similar tosubsequent cases in each of the 25 centers involved.
9. Role of Registries
Post-marketing data collection for medical device evalu-ation is an essential component in the assessment ofdevice performance and its benefit/risk balance through-out the product life cycle. In addition to confirmation ofdata observed in pre-approval studies, post-marketingstudies provide information regarding ‘real world’ use inpatient subsets not fully tested in pre-market clinicaltrials. Registries offer an important platform for post-marketing device evaluation. For example, the STS Na-tional Database and ACC’s National Cardiovascular DataRegistry (NCDR®) that have traditionally focused onnational benchmarking, quality improvement, and re-search, are rapidly emerging to fulfill this important role.The ability to link clinical registry data with administra-tive data opens an untapped resource for monitoring andpredicting both short- and potentially long-term out-comes. In general, the short-term clinical information canbe used for risk stratification and identification of impor-tant clinical subgroups, whereas the administrative datacan be used to track patterns of use and ultimatelylong-term events.
In the past, device monitoring has typically been car-ried out through industry-supported trials and post-approval studies. It has been necessary for industry toundertake the very expensive and time-consuming taskof developing data registries. In the development of theseregistries, there has been little coordination with existingsocietal registries to harmonize definitions or data spec-ifications. An unfortunate byproduct of this approach has
led to the well-recognized inconsistencies seen in cardio-vascular data reporting. In addition, there is the unavoid-able potential for a conflict of interest that might arisefrom a manufacturer conducting studies of its owndevice.
The use of clinical registries can address many of theseconcerns. Registries such as the STS Database and ACC’sNCDR® have a high degree of national participation, sothe data represents a true national experience. Theseregistries have a well-established protocol for data col-lection, with trained abstractors and onsite rigorous au-dits to ensure high data quality and completeness ofentry. Database definitions are generally regarded asnational standards, and there is a high degree of harmo-nization between terms common to these registries.These definitions should be based upon consensus doc-uments; for example, VARC definitions of stroke [96].Furthermore, each registry can be linked to administra-tive databases in order to obtain long-term outcomeinformation. These facts demonstrate the ability of thenational cardiovascular registries to serve as the founda-tion for comprehensive device registries. In the last fewyears, the FDA has collaborated with various organiza-tions to use registry data to investigate several importantdevice-related studies. Although there is no specific legis-lative mandate to use clinical registries, FDA leadershipdoes actively encourage the use of registries for devicesurveillance.
Registries offer distinct theoretical advantages in thisfield, but it should be remembered that practical appli-cation presents unchartered waters. Perhaps 1 majorchallenge lies in the fact that a successful program willrequire close cooperation between multiple organiza-tions. For example, the STS and ACCF have a longhistory of cooperation and collaboration on registry-related projects, holding monthly conference calls de-voted to registry coordination, thus laying the foundationfor collaborative projects such as device surveillance.Similar collaborations will require the need for contrac-tual agreements to address issues such as data owner-ship, data access, and governance of linked registries.Sophisticated statistical analysis will be a central featureof surveillance projects, so coordination with an analyticcenter will also be necessary. Certainly, FDA input willbe central to any device-related project, and coordinationwith the Centers for Medicare and Medicaid Services(CMS) may be necessary as well. The device manufac-turer will have an essential role, especially in post-approval studies, so coordination with industry will be akey element of any project.
Device surveillance will require fundamentalchanges in the clinical database operations. Presently,there is no provision for timely data entry, but post-approval studies will require exactly that in order tocapture adverse events as they occur. Likewise, post-approval studies require long-term follow-up of infor-mation that cannot be obtained from administrativedatabases. Provision must be made to capture infor-mation such as echocardiographic findings and quali-ty-of-life data months to years after device insertion. It
should also be noted that the use of CMS MedPAR data
1377Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
may have limited usefulness in this context because ofthe inability to acquire contemporary data limited toonly those patients �65 years. (In general, the mostcurrent available MedPAR data are 2 years old.) Addi-tional challenges include standardized rigorous meth-odology adapted for sparse data and standardizedreporting formats modeled after the CONSORT (Con-solidated Standards of Reporting Trials) guidelines forrandomized trials, PRISMA (Preferred Reporting Itemsfor Systematic reviews and Meta-Analyses) guidelinesfor meta-analyses, or STROBE (STrengthening theReporting of Observational studies in Epidemiology)guidelines for observational studies [182, 258 –260]. Itshould be emphasized that the registry should capturedata on all devices that are placed. Specific post-approval studies may focus on a smaller, more selectpopulation, but a comprehensive registry should col-lect information on all devices for complete analysesindependent of industry-sponsored studies. A poten-tial incentive for participation in the device registrymight be linking it to CMS coverage criteria or otherform of federal legislation.
Funding the device registries requires innovative consid-eration. Despite the fact that federal agencies encourage theuse of clinical registries, funding for such projects is notavailable for device-related projects. Although industryfunding for studies related to their specific product offersthe most straightforward approach other models rely uponcenters to pay a fee in return for registry participation.
As registries are developed, a “silo” constructionmust be avoided. It is critically important to keep aneye on the future so that present plans fit seamlesslywith the vision for future initiatives. This means that adevice-specific registry should be designed to serve asa building block for the next generation of registries.Planning for interoperability, resource sharing, andavoidance of duplication will be necessary to create thesystem of integrated, coordinated registries that will bethe hallmark of registries for the next decade.
10. Summary and Recommendations
There are a number of potential treatment recommen-dations for patients with AS (Table 15). Considerationof the risk/benefit of each option needs to be carefullyevaluated and discussed with the patient and family.The involvement of the heart team in decision makingis also essential.
The approval of TAVR represents a fundamental changein the management of aortic valvular heart disease byoffering an alternative to traditional surgical aortic valvereplacement in carefully selected patients. The penetrationof this technology in the broad group of patients with ASremains to be determined and will depend on the contin-ued evolution of the technology and the results of clinicaltrials conducted in these patients. At the present time,several observations and recommendations can be made.
1. Complex Technology: Although the technique and
equipment continue to evolve, TAVR is a complexprocedure with many interlocking steps that requiremeticulous attention to achieve optimal results andminimize complications.
2. Team-Based Approach: A foundational requirementof TAVR is a team-based approach to patientcare. Given the high-risk profile of patients, whooften have multiple comorbidities, as well as thetechnical complexity of the procedure involved,this team-based care will need to include multi-ple contributors at different stages in the processbut will be mainly centered around the primarycardiologist, the cardiovascular surgeon, and theinterventional cardiologist. Patients and familiesmust be included in the care team. Other teammembers will include cardiac anesthesiologists,heart failure specialists, structural heart diseasephysicians, imaging specialists and the nursingcare team, among others.
3. Patient Selection: In adults with severe, symptomatic,calcific stenosis of a trileaflet aortic valve who haveaortic and vascular anatomy suitable for TAVR anda predicted survival �12 months:
● TAVR is recommended in patients with prohibi-tive surgical risk.
● TAVR is a reasonable alternative to surgical AVRin patients at high surgical risk.
Definitions of severe AS have varied between regis-tries, trials, and guidelines. In general, all require se-verely reduced, calcified leaflet motion, and aortic jetvelocity �4.0 m/s OR an AVA �1.0 cm2 OR AV index�0.6 cm2/m2 OR a mean gradient �40 mm Hg. In thesetting of LV systolic dysfunction, severe AS is presentwhen the leaflets are calcified, with reduced systolicmotion, and dobutamine stress echocardiography showsan aortic velocity of �4.0 m/s OR mean gradient �40 mmHg with a valve area �1.0 cm2 OR AV index �0.6 cm2/m2
at any flow rate.Prohibitive surgical risk is defined as:
● An estimated 50% or greater risk of mortality orirreversible morbidity at 30 days (as assessed byone cardiologist and 2 cardiothoracic surgeons),or other factors such as frailty, prior radiationtherapy, porcelain aorta, and severe hepatic orpulmonary disease.
● Suitable aortic and vascular anatomy is defined as:● Both aortic annulus size and valve plane to coro-
nary ostium height suitable for placement of anavailable TAVR.
● Adequate vascular access for passage of the TAVRsystem (femoral iliac, subclavian, axillary) or suit-ability for an apical implantation approach.TAVR is not currently recommended because oflimited available information in adults who have:
● An acceptable surgical risk for conventional sur-gical AVR
● Known bicuspid aortic valve● Failing bioprosthetic aortic valve
● Severe mitral annular calcification or severe MR
1378 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
● Moderate AS● Other (e.g., severe AR and subaortic stenosis)
In these groups, additional scientific data will need tobe collected to ascertain risk/benefit ratio prior to inte-gration into routine clinical care.
4. TAVR Screening: Screening protocols should be partof every TAVR evaluation. These may vary from insti-tution to institution. Some information may be obtainedfrom referring institutions, whereas some will be ob-tained within the institution performing the TAVR. Inthe former case, the information obtained must be ofhigh quality so that optimal recommendations can be
Table 15. Current Treatment Recommendations for Patients W
Treatment Indication
Surgical Aortic ValveReplacement
● Symptomatic severe AS (Class I, LO● Severe AS undergoing CABG, aortic
surgery (Class I, LOE: C)● Symptomatic moderate AS undergo
surgery or other valve surgery (Clas● Asymptomatic severe AS with hypo
exercise (Class IIb; LOE: C)● Asymptomatic extremely severe AS
gradient �50 mm Hg, or jet velocityLOE: C)
Transcatheter AorticValve Replacement
● TAVR is recommended in patients wsymptomatic, calcific stenosis of a trwho have aortic and vascular anatomand a predicted survival�12 months, and who have a prohibdefined by an estimated 50% or greairreversible morbidity at 30 days orfrailty, prior radiation therapy, porcehepatic or pulmonary disease.
● TAVR is a reasonable alternative topatients at high surgical risk (PARTNSTS�8%*)
Balloon AorticValvuloplasty
● Reasonable for palliation in adult pawhom surgical AVR cannot be perfoserious comorbid conditions (Class I
● Bridge to surgical AVR (Class IIb, LOMedical Therapy ● No specific therapy for asymptomati
● Medical therapy not indicated for sy● Appropriate control of blood pressu
factors as indicated● Statins not indicated for preventing● Diuretics, vasodilators and positive i
avoided in patients awaiting surgerydestabilization
* The original PARTNER protocol specified inclusion criteria as a minimthe minimum STS-predicted risk of mortality was changed to �8. In bothwas �15.
Class I: Conditions for which there is evidence for and/or general agreeII: Conditions for which there is conflicting evidence and/or a divergenceWeight of evidence/opinion is in favor of usefulness/efficacy; Class IIb:derived from a single randomized trial or nonrandomized studies; LO
AR � aortic regurgitation; AS � aortic stenosis; AVR � aortic valevidence; STS � Society of Thoracic Surgeons; TAVR � transcath
Source of Class/LOE recommendations: Bonow et al. [28].
formulated. Requisite pieces of information include:
● Data sufficient to calculate STS score● Measurement of clinical parameters related to the
presence of comorbid conditions such as pulmo-nary function tests in patients with COPD or extentand severity of malignancy if present
● Assessment for the degree of cognitive impairment asappropriate
● Imaging data to confirmX Presence and severity o f aortic stenosisX Presence and severity of associated CADX Left ventricular functionX Presence and severity of associated valvular
heart disease lesions
Aortic Stenosis
Major Complications
ery or other valve
ABG, aorticLOE: C)e response to
�0.6 cm2, mean/s) (Class IIb,
● Mortality (3%)● Stroke (2%)● Prolonged ventilation (11%)● Thromboembolism and bleeding● Prosthetic dysfunction● Perioperative complications are higher
when surgical AVR is combined withCABG
evere,et aortic valveitable for TAVR
surgical risk asisk of mortality orfactors such as
aorta, and severe
cal AVR inTrial Criteria:
● Mortality (3% to 5%)● Stroke (6% to 7%)● Access complications (17%)● Pacemaker insertion
Π2% to 9% (Sapien)Π19% to 43% (CoreValve)
● Bleeding● Prosthetic dysfunction● Paravalvular AR● Acute kidney injury● Other
ΠCoronary occlusionΠValve embolizationΠAortic rupture
s with AS inbecause of
OE: C))
● Mortality● Stroke● Access complications● Restenosis
matic severe ASd other risk
ression of ASpes should beuse of risk of
● Hemodynamic instability
S-predicted risk of mortality of �10. During the trial enrollment phase,ces, 2 surgeons had to document that the true predicted risk of mortality
that the procedure or treatment is beneficial, useful, and effective; Classinion about the usefulness/efficacy of a procedure or treatment; Class IIa:lness/efficacy is less well established by evidence/opinion; LOE B: DataOnly consensus opinion of experts, case studies, or standard-of-care.
lacement; CABG � coronary artery bypass graft; LOE � level ofaortic valve replacement.
ith
E: B)surg
ing Cs IIa,tensiv
(AVA�5 m
ith sileafl
y su
itiveter r
otherlain
surgiER
tientrmedIb, L
E: Cc ASmptore an
prognotrobeca
um STinstan
mentof opUsefu
E C:
ve repeter
X Presence and extent of cerebral vascular disease

1379Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
● Preprocedural imaging for planning should bedone by the institution performing TAVRX Assessment of annular size for device selectionX Assessment of details of arterial anatomy includ-
ing the peripheral aortoiliac vessels as well as theaortic arch and ascending aorta which may im-pact on access selection
5. Site Selection: Centers should have experience withstructural heart disease. All members of the heartteam should be available onsite. In addition, astructural heart disease center or clinic, a proce-dural performance area (either a hybrid surgicalroom or a specially modified cardiac catheterizationlaboratory room), a postprocedure care team, andexpert imaging using echocardiography and CTshould be available. Setting up specialized centersof excellence with convenient access to patientsshould be a top priority for responsible dissemina-tion of this technology. For more details, please seefacility requirements in the “SCAI/AATS/ACCF/STS Multisociety Expert Consensus Statement: Op-erator & Institutional Requirements for Transcath-eter Valve Repair and Replacement; Part 1 TAVR”[218].
6. Center and Physician Experience: Expertise with sur-gical AVR is essential—the number of surgicalprocedures has been recommended to be 50 withinthe past 12 months. For the interventional cardiol-ogist, experience with balloon aortic valvuloplastyas well as experience in a team-based care ap-proach is recommended. During the rollout of theprocedure, experienced proctors will form part ofthe heart care team. These physicians will be onsitefor the first several cases after a site has beeninitiated. After the performance of these initialprocedures, centers will be eligible to qualify forindependent TAVR. Physician teams need to beexperienced with transapical, transarterial, and al-ternative arterial approaches for TAVR. For de-tailed information on requirements for interven-tional cardiologists and surgeons to perform TAVR,please refer to the “SCAI/AATS/ACCF/STS Multi-society Expert Consensus Statement: Operator &Institutional Requirements for Transcatheter ValveRepair and Replacement; Part 1 TAVR.” [218].
7. Procedural Performance: TAVR should be performedin either specially modified, large cardiac catheter-ization laboratories or hybrid rooms. Fixed imagingand intraprocedural echocardiography are requiredas are capabilities for cardiopulmonary bypass formanagement of procedural complications. In addi-tion to the valve implantation equipment, peripheraland coronary interventions equipment must beavailable for urgent treatment of complications.The ability to provide general anesthesia should beavailable.
8. Postprocedural Care: The intensity of postproceduralcare depends on the presence of comorbidities, as
well as the results of the TAVR itself. Protocolsshould be defined for routine care, as well asmanagement of specific problems and complica-tions. Ideally, a dedicated recovery area should beestablished at each site to which all patients shouldbe transferred for optimal postprocedural care.Postdischarge care plans should include consider-ation of rehabilitation, and home health or othersupport needed during recovery. In addition, fol-low-up with the primary care team can ensuresuccessful transitions of care.
9. Registries: Participation is recommended in nationalTAVR registries that include clinical and administra-tive claims data that will allow careful evaluation ofboth short-term and long-term risks and benefits andtrack changes in patient selection criteria, proceduralperformance, and device iteration. Preferably, regis-tries should also capture demographics and mortalityoutcome data of surgically and medically treatedpatients in order to facilitate comparison of differenttherapeutic strategies to improve identification andselection of optimal therapeutic options.
References
1. Holmes DR Jr., Mack MJ. Transcatheter valve therapy aprofessional society overview from the American College ofCardiology Foundation and the Society of Thoracic Sur-geons. J Am Coll Cardiol. 2011;58:445–55.
2. Roberts WC, Ko JM. Frequency by decades of unicuspid,bicuspid, and tricuspid aortic valves in adults having iso-lated aortic valve replacement for aortic stenosis, with orwithout associated aortic regurgitation. Circulation. 2005;111:920–5.
3. Selzer A. Changing aspects of the natural history of valvu-lar aortic stenosis. N Engl J Med. 1987;317:91–8.
4. Stephan PJ, Henry AC III, Hebeler RF Jr., et al. Comparisonof age, gender, number of aortic valve cusps, concomitantcoronary artery bypass grafting, and magnitude of leftventricular-systemic arterial peak systolic gradient inadults having aortic valve replacement for isolated aorticvalve stenosis. Am J Cardiol. 1997;79:166–72.
5. Ghaisas NK, Foley JB, O’Briain DS, et al. Adhesion mole-cules in nonrheumatic aortic valve disease: endothelialexpression, serum levels and effects of valve replacement.J Am Coll Cardiol. 2000;36:2257–62.
6. Otto CM, Kuusisto J, Reichenbach DD, et al. Characteriza-tion of the early lesion of ’degenerative’ valvular aorticstenosis. Histological and immunohistochemical studies.Circulation. 1994;90:844–53.
7. Peterson KL, Tsuji J, Johnson A, et al. Diastolic left ventric-ular pressure-volume and stress-strain relations in patientswith valvular aortic stenosis and left ventricular hypertro-phy. Circulation. 1978;58:77–89.
8. Spann JF, Bove AA, Natarajan G, et al. Ventricular perfor-mance, pump function and compensatory mechanisms inpatients with aortic stenosis. Circulation. 1980;62:576–82.
9. Carabello BA, Paulus WJ. Aortic stenosis. Lancet. 2009;373:956–66.
10. Marcus ML, Doty DB, Hiratzka LF, et al. Decreased coro-nary reserve: a mechanism for angina pectoris in patientswith aortic stenosis and normal coronary arteries. N EnglJ Med. 1982;307:1362–6.
11. Koyanagi S, Eastham CL, Harrison DG, et al. Increased sizeof myocardial infarction in dogs with chronic hypertension
and left ventricular hypertrophy. Circ Res. 1982;50:55–62.
1380 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
12. Gunther S, Grossman W. Determinants of ventricular func-tion in pressure-overload hypertrophy in man. Circulation.1979;59:679–88.
13. Krayenbuehl HP, Hess OM, Ritter M, et al. Left ventricularsystolic function in aortic stenosis. Eur Heart J. 1988;9 SupplE:19–23.
14. Carabello BA, Green LH, Grossman W, et al. Hemody-namic determinants of prognosis of aortic valve replace-ment in critical aortic stenosis and advanced congestiveheart failure. Circulation. 1980;62:42–8.
15. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who can-not undergo surgery. N Engl J Med. 2010;363:1597–607.
16. Gardin JM, Kaplan KJ, Meyers SN, et al. Aortic stenosis: canseverity be reliably estimated noninvasively? Chest. 1980;77:130–1.
17. Morrow AG, Roberts WC, Ross J Jr., et al. Obstruction toleft ventricular outflow. Current concepts of managementand operative treatment. Ann Intern Med. 1968;69:1255–86.
18. Baumgartner H, Hung J, Bermejo J, et al. Echocardiographicassessment of valve stenosis: EAE/ASE recommendationsfor clinical practice. J Am Soc Echocardiogr. 2009;22:1–23.
19. Popovic AD, Thomas JD, Neskovic AN, et al. Time-relatedtrends in the preoperative evaluation of patients withvalvular stenosis. Am J Cardiol. 1997;80:1464–8.
20. Blais C, Burwash IG, Mundigler G, et al. Projected valvearea at normal flow rate improves the assessment of steno-sis severity in patients with low-flow, low-gradient aorticstenosis: the multicenter TOPAS (Truly or Pseudo-SevereAortic Stenosis) study. Circulation. 2006;113:711–21.
21. Grayburn PA. Assessment of low-gradient aortic stenosiswith dobutamine. Circulation. 2006;113:604–6.
22. Monin JL, Monchi M, Gest V, et al. Aortic stenosis withsevere left ventricular dysfunction and low transvalvularpressure gradients: risk stratification by low-dose dobut-amine echocardiography. J Am Coll Cardiol. 2001;37:2101–7.
23. Nishimura RA, Grantham JA, Connolly HM, et al. Low-output, low-gradient aortic stenosis in patients with de-pressed left ventricular systolic function: the clinical utilityof the dobutamine challenge in the catheterization labora-tory. Circulation. 2002;106:809–13.
24. Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCAguidelines for performing a comprehensive intraoperativemultiplane transesophageal echocardiography examina-tion: recommendations of the American Society of Echocar-diography Council for Intraoperative Echocardiographyand the Society of Cardiovascular Anesthesiologists TaskForce for Certification in Perioperative TransesophagealEchocardiography. Anesth Analg. 1999;89:870–84.
25. Greenland P, Bonow RO, Brundage BH, et al. ACCF/AHA2007 clinical expert consensus document on coronary arterycalcium scoring by computed tomography in global cardio-vascular risk assessment and in evaluation of patients withchest pain: a report of the American College of CardiologyFoundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Con-sensus Document on Electron Beam Computed Tomogra-phy). J Am Coll Cardiol. 2007;49:378–402.
26. Hundley WG, Bluemke DA, Finn JP, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document oncardiovascular magnetic resonance: a report of the Ameri-can College of Cardiology Foundation Task Force on ExpertConsensus Documents. J Am Coll Cardiol. 2010;55:2614–62.
27. Lancellotti P, Lebois F, Simon M, et al. Prognostic impor-tance of quantitative exercise Doppler echocardiography inasymptomatic valvular aortic stenosis. Circulation. 2005;112:I377–82.
28. Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focusedupdate incorporated into the ACC/AHA 2006 guidelines forthe management of patients with valvular heart disease: a
report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Writ-ing Committee to Revise the 1998 Guidelines for theManagement of Patients With Valvular Heart Disease).J Am Coll Cardiol. 2008;52:e1–142.
29. Vahanian A, Baumgartner H, Bax J, et al. Guidelines on themanagement of valvular heart disease: the Task Force onthe Management of Valvular Heart Disease of the Euro-pean Society of Cardiology. Eur Heart J. 2007;28:230–68.
30. Connolly HM, Oh JK, Orszulak TA, et al. Aortic valvereplacement for aortic stenosis with severe left ventriculardysfunction. Prognostic indicators. Circulation. 1997;95:2395–400.
31. Kvidal P, Bergstrom R, Horte LG, et al. Observed andrelative survival after aortic valve replacement. J Am CollCardiol. 2000;35:747–56.
32. Kolh P, Kerzmann A, Honore C, et al. Aortic valve surgeryin octogenarians: predictive factors for operative and long-term results. Eur J Cardiothorac Surg. 2007;31:600–6.
33. Litmathe J, Feindt P, Kurt M, et al. Aortic valve replacementin octogenarians: outcome and predictors of complications.Hellenic J Cardiol. 2011;52:211–5.
34. Pereira JJ, Balaban K, Lauer MS, et al. Aortic valve replace-ment in patients with mild or moderate aortic stenosis andcoronary bypass surgery. Am J Med. 2005;118:735–42.
35. Smith WT, Ferguson TB Jr., Ryan T, et al. Should coronaryartery bypass graft surgery patients with mild or moderateaortic stenosis undergo concomitant aortic valve replace-ment? A decision analysis approach to the surgical di-lemma. J Am Coll Cardiol. 2004;44:1241–7.
36. Adams DH, Chikwe J, Filsoufi F, et al. The year in cardio-vascular surgery. J Am Coll Cardiol. 2011;57:1425–44.
37. Byrne JG, Leacche M, Unic D, et al. Staged initial percuta-neous coronary intervention followed by valve surgery(“hybrid approach”) for patients with complex coronaryand valve disease. J Am Coll Cardiol. 2005;45:14–8.
38. He GW, Acuff TE, Ryan WH, et al. Aortic valve replace-ment: determinants of operative mortality. Ann ThoracSurg. 1994;57:1140–6.
39. Pai RG, Varadarajan P, Kapoor N, et al. Aortic valvereplacement improves survival in severe aortic stenosisassociated with severe pulmonary hypertension. Ann Tho-rac Surg. 2007;84:80–5.
40. Kapoor N, Varadarajan P, Pai RG. Echocardiographic pre-dictors of pulmonary hypertension in patients with severeaortic stenosis. Eur J Echocardiogr. 2008;9:31–3.
41. McHenry MM, Rice J, Matlof HJ, et al. Pulmonary hyper-tension and sudden death in aortic stenosis. Br Heart J.1979;41:463–7.
42. Rodes-Cabau J, Webb JG, Cheung A, et al. Transcatheteraortic valve implantation for the treatment of severe symp-tomatic aortic stenosis in patients at very high or prohibi-tive surgical risk: acute and late outcomes of the multi-center Canadian experience. J Am Coll Cardiol. 2010;55:1080–90.
43. Ben-Dor I, Goldstein SA, Pichard AD, et al. Clinical profile,prognostic implication, and response to treatment of pul-monary hypertension in patients with severe aortic steno-sis. Am J Cardiol. 2011;107:1046–51.
44. Cam A, Goel SS, Agarwal S, et al. Prognostic implications ofpulmonary hypertension in patients with severe aorticstenosis. J Thorac Cardiovasc Surg. 2011;142:800–8.
45. Khandhar S, Varadarajan P, Turk R, et al. Survival benefitof aortic valve replacement in patients with severe aorticregurgitation and pulmonary hypertension. Ann ThoracSurg. 2009;88:752–6.
46. Zuern CS, Eick C, Rizas K, et al. Prognostic value ofmild-to-moderate pulmonary hypertension in patients withsevere aortic valve stenosis undergoing aortic valve re-placement. Clin Res Cardiol. 2012;101:81–8.
47. McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA2009 expert consensus document on pulmonary hyperten-sion: a report of the American College of Cardiology
Foundation Task Force on Expert Consensus Documents
1381Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
and the American Heart Association. J Am Coll Cardiol.2009;53:1573–619.
48. Santini F, Casali G, Franchi G, et al. Hemodynamic effectsof inhaled nitric oxide and phosphodiesterase inhibitor(dipyridamole) on secondary pulmonary hypertension fol-lowing heart valve surgery in adults. Int J Cardiol. 2005;103:156–63.
49. Fattouch K, Sbraga F, Bianco G, et al. Inhaled prostacy-clin, nitric oxide, and nitroprusside in pulmonary hyper-tension after mitral valve replacement. J Card Surg.2005;20:171– 6.
50. Trachte AL, Lobato EB, Urdaneta F, et al. Oral sildenafilreduces pulmonary hypertension after cardiac surgery.Ann Thorac Surg. 2005;79:194–7.
51. Huber D, Grimm J, Koch R, et al. Determinants of ejectionperformance in aortic stenosis. Circulation. 1981;64:126–34.
52. Herrmann S, Stork S, Niemann M, et al. Low-gradientaortic valve stenosis myocardial fibrosis and its influenceon function and outcome. J Am Coll Cardiol. 2011;58:402–12.
53. Tribouilloy C, Levy F, Rusinaru D, et al. Outcome afteraortic valve replacement for low-flow/low-gradient aorticstenosis without contractile reserve on dobutamine stressechocardiography. J Am Coll Cardiol. 2009;53:1865–73.
54. Quere JP, Monin JL, Levy F, et al. Influence of preoperativeleft ventricular contractile reserve on postoperative ejectionfraction in low-gradient aortic stenosis. Circulation. 2006;113:1738–44.
55. Kolh P, Wijns W, Danchin N, et al. Guidelines on myocar-dial revascularization. Eur J Cardiothorac Surg. 2010;38Suppl:S1–52.
56. Toole JM, Stroud MR, Kratz JM, et al. Twenty-five yearexperience with the St. Jude medical mechanical valveprosthesis. Ann Thorac Surg. 2010;89:1402–9.
57. Braunwald E. Aortic valve replacement: an update at theturn of the millennium. Eur Heart J. 2000;21:1032–3.
58. Nashef SA, Roques F, Hammill BG, et al. Validation ofEuropean System for Cardiac Operative Risk Evaluation(EuroSCORE) in North American cardiac surgery. EurJ Cardiothorac Surg. 2002;22:101–5.
59. Shroyer AL, Coombs LP, Peterson ED, et al. The Society ofThoracic Surgeons: 30-day operative mortality and morbid-ity risk models. Ann Thorac Surg. 2003;75:1856–64.
60. Society of Thoracic Surgeons national cardiac surgery da-tabase. Available at: http://www.sts.org/national-database.Accessed January 13, 2012.
61. O’Brien SM, Shahian DM, Filardo G, et al. The Society ofThoracic Surgeons 2008 cardiac surgery risk models: part2—isolated valve surgery. Ann Thorac Surg. 2009;88:S23–42.
62. Thourani VH, Ailawadi G, Szeto WY, et al. Outcomes ofsurgical aortic valve replacement in high-risk patients: amultiinstitutional study. Ann Thorac Surg. 2011;91:49–55.
63. Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA2006 guidelines for the management of patients with val-vular heart disease: a report of the American College ofCardiology/American Heart Association Task Force onPractice Guidelines (Writing Committee to Revise the 1998Guidelines for the Management of Patients With ValvularHeart Disease). J Am Coll Cardiol. 2006;48:e1–148.
64. Melby SJ, Moon MR, Lindman BR, et al. Impact of pulmo-nary hypertension on outcomes after aortic valve replace-ment for aortic valve stenosis. J Thorac Cardiovasc Surg.2011;141:1424–30.
65. Sundermann S, Dademasch A, Praetorius J, et al. Compre-hensive assessment of frailty for elderly high-risk patientsundergoing cardiac surgery. Eur J Cardiothorac Surg. 2011;39:33–7.
66. Heras M, Chesebro JH, Fuster V, et al. High risk of throm-boemboli early after bioprosthetic cardiac valve replacement.J Am Coll Cardiol. 1995;25:1111–9.
67. Brown JM, O’Brien SM, Wu C, et al. Isolated aortic valve
replacement in North America comprising 108,687 patientsin 10 years: changes in risks, valve types, and outcomes inthe Society of Thoracic Surgeons National Database.J Thorac Cardiovasc Surg. 2009;137:82–90.
68. Bloomfield P, Wheatley DJ, Prescott RJ, et al. Twelve-yearcomparison of a Bjork-Shiley mechanical heart valve withporcine bioprostheses. N Engl J Med. 1991;324:573–9.
69. Goldstein LB, Bushnell CD, Adams RJ, et al. Guidelines forthe primary prevention of stroke: a guideline for healthcareprofessionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:517–84.
70. Ferrari E, Tozzi P, Hurni M, et al. Primary isolated aorticvalve surgery in octogenarians. Eur J Cardiothorac Surg.2010;38:128–33.
71. Bach DS, Cimino N, Deeb GM. Unoperated patients withsevere aortic stenosis. J Am Coll Cardiol. 2007;50:2018–9.
72. Bach DS, Siao D, Girard SE, et al. Evaluation of patientswith severe symptomatic aortic stenosis who do not un-dergo aortic valve replacement: the potential role of sub-jectively overestimated operative risk. Circ CardiovascQual Outcomes. 2009;2:533–9.
73. Dua A, Dang P, Shaker R, et al. Barriers to surgery in severeaortic stenosis patients with Class I indications for aorticvalve replacement. J Heart Valve Dis. 2011;20:396–400.
74. Iung B, Baron G, Butchart EG, et al. A prospective survey ofpatients with valvular heart disease in Europe: the EuroHeart Survey on Valvular Heart Disease. Eur Heart J.2003;24:1231–43.
75. Iung B, Cachier A, Baron G, et al. Decision-making inelderly patients with severe aortic stenosis: why are somany denied surgery? Eur Heart J. 2005;26:2714–20.
76. Varadarajan P, Kapoor N, Bansal RC, et al. Clinical profileand natural history of 453 nonsurgically managed patientswith severe aortic stenosis. Ann Thorac Surg. 2006;82:2111–5.
77. Bouma BJ, van Der Meulen JH, van Den Brink RB, et al.Variability in treatment advice for elderly patients withaortic stenosis: a nationwide survey in the Netherlands.Heart. 2001;85:196–201.
78. Varadarajan P, Kapoor N, Bansal RC, et al. Survival inelderly patients with severe aortic stenosis is dramaticallyimproved by aortic valve replacement: results from a cohortof 277 patients aged � or �80 years. Eur J CardiothoracSurg. 2006;30:722–7.
79. Mihaljevic T, Nowicki ER, Rajeswaran J, et al. Survival aftervalve replacement for aortic stenosis: implications for de-cision making. J Thorac Cardiovasc Surg. 2008;135:1270–8.
80. Gammie JS, Brown JW, Brown JM, et al. Aortic valve bypassfor the high-risk patient with aortic stenosis. Ann ThoracSurg. 2006;81:1605–10.
81. Palta S, Pai AM, Gill KS, et al. New insights into theprogression of aortic stenosis: implications for secondaryprevention. Circulation. 2000;101:2497–502.
82. Rajamannan NM, Otto CM. Targeted therapy to preventprogression of calcific aortic stenosis. Circulation. 2004;110:1180–2.
83. Cribier A, Savin T, Saoudi N, et al. Percutaneous translu-minal valvuloplasty of acquired aortic stenosis in elderlypatients: an alternative to valve replacement? Lancet. 1986;1:63–7.
84. Ben-Dor I, Pichard AD, Satler LF, et al. Complications andoutcome of balloon aortic valvuloplasty in high-risk orinoperable patients. J Am Coll Cardiol Intv. 2010;3:1150–6.
85. Lieberman EB, Bashore TM, Hermiller JB, et al. Balloonaortic valvuloplasty in adults: failure of procedure to im-prove long-term survival. J Am Coll Cardiol. 1995;26:1522–8.
86. Otto CM, Mickel MC, Kennedy JW, et al. Three-yearoutcome after balloon aortic valvuloplasty. Insights intoprognosis of valvular aortic stenosis. Circulation. 1994;89:642–50.
87. Percutaneous balloon aortic valvuloplasty. Acute and30-day follow-up results in 674 patients from the NHLBI
Balloon Valvuloplasty Registry. Circulation. 1991;84:2383–97.
1382 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
88. Ben-Dor I, Maluenda G, Looser PM, et al. Outcomes ofconcomitant percutaneous coronary intervention and balloonaortic valvuloplasty. Catheter Cardiovasc Interv. 2011: pub-lished online before print July 6, 2011, doi:10.1002/ccd.23193.Accessed January 13, 2012.
89. Hara H, Pedersen WR, Ladich E, et al. Percutaneous bal-loon aortic valvuloplasty revisited: time for a renaissance?Circulation. 2007;115:e334–8.
90. Ussia GP, Capodanno D, Barbanti M, et al. Balloon aorticvalvuloplasty for severe aortic stenosis as a bridge tohigh-risk transcatheter aortic valve implantation. J InvasiveCardiol. 2010;22:161–6.
91. Chiam PT, Ruiz CE. Percutaneous transcatheter aortic valveimplantation: assessing results, judging outcomes, andplanning trials: the interventionalist perspective. J Am CollCardiol Intv. 2008;1:341–50.
92. Andersen HR, Knudsen LL, Hasenkam JM. Transluminalimplantation of artificial heart valves: description of a newexpandable aortic valve and initial results with implanta-tion by catheter technique in closed chest pigs. Eur Heart J.1992;13:704–8.
93. Cribier A, Eltchaninoff H, Bash A, et al. Percutaneoustranscatheter implantation of an aortic valve prosthesis forcalcific aortic stenosis: first human case description. Circu-lation. 2002;106:3006–8.
94. Chiam PT, Ruiz CE. Percutaneous transcatheter aortic valveimplantation: evolution of the technology. Am Heart J.2009;157:229–42.
95. Dalmau MJ, Gonzalez-Santos JM, Blazquez JA, et al. He-modynamic performance of the Medtronic Mosaic andPerimount Magna aortic bioprostheses: five-year results ofa prospectively randomized study. Eur J Cardiothorac Surg.2011;39:844–52.
96. Leon MB, Piazza N, Nikolsky E, et al. Standardized end-point definitions for Transcatheter Aortic Valve Implanta-tion clinical trials: a consensus report from the ValveAcademic Research Consortium. J Am Coll Cardiol. 2011;57:253–69.
97. Avanzas P, Munoz-Garcia AJ, Segura J, et al. Percutaneousimplantation of the CoreValve self-expanding aortic valveprosthesis in patients with severe aortic stenosis: earlyexperience in Spain. Rev Esp Cardiol. 2010;63:141–8.
98. Deleted in proof.99. Deleted in proof.
100. Deleted in proof.101. Deleted in proof.102. Deleted in proof.103. Deleted in proof.104. Deleted in proof.105. Buellesfeld L, Gerckens U, Schuler G, et al. 2-year fol-
low-up of patients undergoing transcatheter aortic valveimplantation using a self-expanding valve prosthesis. J AmColl Cardiol. 2011;57:1650–7.
106. Eltchaninoff H, Prat A, Gilard M, et al. Transcatheter aorticvalve implantation: early results of the FRANCE (FRenchAortic National CoreValve and Edwards) registry. EurHeart J. 2011;32:191–7.
107. Godino C, Maisano F, Montorfano M, et al. Outcomes aftertranscatheter aortic valve implantation with both Edwards-SAPIEN and CoreValve devices in a single center: theMilan experience. J Am Coll Cardiol Intv. 2010;3:1110–21.
108. Moynagh AM, Scott DJ, Baumbach A, et al. CoreValvetranscatheter aortic valve implantation via the subclavianartery: comparison with the transfemoral approach. J AmColl Cardiol. 2011;57:634–5.
109. Tamburino C, Capodanno D, Ramondo A, et al. Incidenceand predictors of early and late mortality after transcathe-ter aortic valve implantation in 663 patients with severeaortic stenosis. Circulation. 2011;123:299–308.
110. Zahn R, Gerckens U, Grube E, et al. Transcatheter aorticvalve implantation: first results from a multi-centre real-
world registry. Eur Heart J. 2011;32:198–204.111. Thomas M, Schymik G, Walther T, et al. Thirty-day resultsof the SAPIEN aortic Bioprosthesis European Outcome(SOURCE) Registry: a European registry of transcatheteraortic valve implantation using the Edwards SAPIEN valve.Circulation. 2010;122:62–9.
112. di Marco F, Gerosa G. Percutaneous aortic valve replace-ment: which patients are suitable for it? A quest for acontrolled use. J Thorac Cardiovasc Surg. 2007;133:294–8.
113. ElBardissi AW, Shekar P, Couper GS, et al. Minimallyinvasive aortic valve replacement in octogenarian, high-risk, transcatheter aortic valve implantation candidates.J Thorac Cardiovasc Surg. 2011;141:328–35.
114. Higgins J, Ye J, Humphries KH, et al. Early clinical out-comes after transapical aortic valve implantation: a propen-sity-matched comparison with conventional aortic valvereplacement. J Thorac Cardiovasc Surg. 2011;142:e47–52.
115. Moat NE, Ludman P, de Belder MA, et al. Long-termoutcomes after transcatheter aortic valve implantation inhigh-risk patients with severe aortic stenosis: the U.K. TAVI(United Kingdom Transcatheter Aortic Valve Implantation)registry. J Am Coll Cardiol. 2011;58:2130–8.
116. Lefevre T, Kappetein AP, Wolner E, et al. One year fol-low-up of the multi-centre European PARTNER transcath-eter heart valve study. Eur Heart J. 2011;32:148–57.
117. Krane M, Deutsch MA, Bleiziffer S, et al. Quality of lifeamong patients undergoing transcatheter aortic valve im-plantation. Am Heart J. 2010;160:451–7.
118. Ussia GP, Mule M, Barbanti M, et al. Quality of lifeassessment after percutaneous aortic valve implantation.Eur Heart J. 2009;30:1790–6.
119. Bekeredjian R, Krumsdorf U, Chorianopoulos E, et al.Usefulness of percutaneous aortic valve implantation toimprove quality of life in patients �80 years of age. Am JCardiol. 2010;106:1777–81.
120. Gotzmann M, Hehen T, Germing A, et al. Short-term effectsof transcatheter aortic valve implantation on neurohor-monal activation, quality of life and 6-minute walk test insevere and symptomatic aortic stenosis. Heart. 2010;96:1102–6.
121. Wendler O, Walther T, Schroefel H, et al. The SOURCEregistry: what is the learning curve in trans-apical aorticvalve implantation? Eur J Cardiothorac Surg. 2011;39:853–9.
122. Reynolds MR, Magnuson EA, Lei Y, et al. Health-relatedquality of life after transcatheter aortic valve replacement ininoperable patients with severe aortic stenosis. Circulation.2011;124:1964–72.
123. Cohen DJ. Health-related quality of life after transcathetervs. surgical aortic valve replacement in high-risk patientswith severe aortic stenosis. Results from the PARTNER trial(Cohort A). Presented at: TCT 2011; November 10, 2011; SanFrancisco, CA.
124. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versussurgical aortic-valve replacement in high-risk patients.N Engl J Med. 2011;364:2187–98.
125. Rodes-Cabau J, Dumont E, Boone RH, et al. Cerebralembolism following transcatheter aortic valve implanta-tion: comparison of transfemoral and transapical ap-proaches. J Am Coll Cardiol. 2011;57:18–28.
126. Kahlert P, Knipp SC, Schlamann M, et al. Silent andapparent cerebral ischemia after percutaneous transfemo-ral aortic valve implantation: a diffusion-weighted magneticresonance imaging study. Circulation. 2010;121:870–8.
127. Arnold M, Schulz-Heise S, Achenbach S, et al. Emboliccerebral insults after transapical aortic valve implantationdetected by magnetic resonance imaging. J Am Coll CardiolIntv. 2010;3:1126–32.
128. Ghanem A, Muller A, Nahle CP, et al. Risk and fate ofcerebral embolism after transfemoral aortic valve implan-tation: a prospective pilot study with diffusion-weightedmagnetic resonance imaging. J Am Coll Cardiol. 2010;55:1427–32.
129. Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the
prevention of stroke in patients with stroke or transient
1383Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
ischemic attack: a guideline for healthcare professionalsfrom the American Heart Association/American StrokeAssociation. Stroke. 2011;42:227–76.
130. Gutsche JT, Cheung AT, McGarvey ML, et al. Risk factorsfor perioperative stroke after thoracic endovascular aorticrepair. Ann Thorac Surg. 2007;84:1195–200.
131. Bleiziffer S, Ruge H, Horer J, et al. Predictors for new-onsetcomplete heart block after transcatheter aortic valve im-plantation. J Am Coll Cardiol Intv. 2010;3:524–30.
132. Piazza N, Onuma Y, Jesserun E, et al. Early and persistentintraventricular conduction abnormalities and require-ments for pacemaking after percutaneous replacement ofthe aortic valve. J Am Coll Cardiol Intv. 2008;1:310–6.
133. Koos R, Mahnken AH, Aktug O, et al. Electrocardiographicand imaging predictors for permanent pacemaker require-ment after transcatheter aortic valve implantation. J HeartValve Dis. 2011;20:83–90.
134. Nuis RJ, Van Mieghem NM, Schultz CJ, et al. Timing andpotential mechanisms of new conduction abnormalitiesduring the implantation of the Medtronic CoreValve Sys-tem in patients with aortic stenosis. Eur Heart J. 2011;32:2067–74.
135. D’Ancona G, Pasic M, Unbehaun A, et al. Permanentpacemaker implantation after transapical transcatheteraortic valve implantation. Interact Cardiovasc Thorac Surg.2011;13:373–6.
136. Wenaweser P, Pilgrim T, Roth N, et al. Clinical outcomeand predictors for adverse events after transcatheter aorticvalve implantation with the use of different devices andaccess routes. Am Heart J. 2011;161:1114–24.
137. Kahlert P, Al-Rashid F, Weber M, et al. Vascular access sitecomplications after percutaneous transfemoral aortic valveimplantation. Herz. 2009;34:398–408.
138. Hayashida K, Lefevre T, Chevalier B, et al. Transfemoralaortic valve implantation new criteria to predict vascularcomplications. J Am Coll Cardiol Intv. 2011;4:851–8.
139. Kodali SK, O’Neill WW, Moses JW, et al. Early and late(one year) outcomes following transcatheter aortic valveimplantation in patients with severe aortic stenosis (fromthe United States REVIVAL trial). Am J Cardiol. 2011;107:1058 – 64.
140. Modine T, Obadia JF, Choukroun E, et al. Transcutaneousaortic valve implantation using the axillary/subclavian access:feasibility and early clinical outcomes. J Thorac CardiovascSurg. 2011;141:487–91, 491.
141. Nuis RJ, Piazza N, Van Mieghem NM, et al. In-hospitalcomplications after transcatheter aortic valve implanta-tion revisited according to the valve academic researchconsortium definitions. Catheter Cardiovasc Interv. 2011;78:457– 67.
142. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneouscoronary intervention versus coronary-artery bypass graft-ing for severe coronary artery disease. N Engl J Med.2009;360:961–72.
143. Kempfert J, Van Linden A, Linke A, et al. Transapical aorticvalve implantation: therapy of choice for patients withaortic stenosis and porcelain aorta? Ann Thorac Surg.2010;90:1457–61.
144. Douglas PS, Otto CM, Mickel MC, et al. Gender differencesin left ventricle geometry and function in patients under-going balloon dilatation of the aortic valve for isolatedaortic stenosis. NHLBI Balloon Valvuloplasty Registry. BrHeart J. 1995;73:548–54.
145. Carroll JD, Carroll EP, Feldman T, et al. Sex-associateddifferences in left ventricular function in aortic stenosis ofthe elderly. Circulation. 1992;86:1099–107.
146. Aurigemma GP, Silver KH, McLaughlin M, et al. Impact ofchamber geometry and gender on left ventricular systolicfunction in patients � 60 years of age with aortic stenosis.Am J Cardiol. 1994;74:794–8.
147. Legget ME, Kuusisto J, Healy NL, et al. Gender differences
in left ventricular function at rest and with exercise inasymptomatic aortic stenosis. Am Heart J. 1996;131:94–100.148. Villari B, Campbell SE, Schneider J, et al. Sex-dependentdifferences in left ventricular function and structure inchronic pressure overload. Eur Heart J. 1995;16:1410–9.
149. Lunney JR, Lynn J, Foley DJ, et al. Patterns of functionaldecline at the end of life. JAMA. 2003;289:2387–92.
150. Fried LP, Tangen CM, Walston J, et al., CardiovascularHealth Study Collaborative Research Group. Frailty inolder adults: evidence for a phenotype. J Gerontol A BiolSci Med Sci. 2001;56:M146–56.
151. Himbert D, Descoutures F, Al-Attar N, et al. Results oftransfemoral or transapical aortic valve implantation fol-lowing a uniform assessment in high-risk patients withaortic stenosis. J Am Coll Cardiol. 2009;54:303–11.
152. Afilalo J, Eisenberg MJ, Morin JF, et al. Gait speed as anincremental predictor of mortality and major morbidity inelderly patients undergoing cardiac surgery. J Am CollCardiol. 2010;56:1668–76.
153. Consensus statement of the Society of Critical Care Medi-cine’s Ethics Committee regarding futile and other possiblyinadvisable treatments. Crit Care Med. 1997;25:887–91.
154. American Thoracic Society. Withholding and withdraw-ing life-sustaining therapy. This Official Statement of theAmerican Thoracic Society was adopted by the ATSBoard of Directors, March 1991. Am Rev Respir Dis.1991;144:726 –31.
155. McDermid RC, Bagshaw SM. Prolonging life and delay-ing death: the role of physicians in the context of limitedintensive care resources. Philos Ethics Humanit Med.2009;4:3.
156. Krumholz HM, Merrill AR, Schone EM, et al. Patterns ofhospital performance in acute myocardial infarction andheart failure 30-day mortality and readmission. Circ Car-diovasc Qual Outcomes. 2009;2:407–13.
157. Bernheim SM, Grady JN, Lin Z, et al. National patterns ofrisk-standardized mortality and readmission for acutemyocardial infarction and heart failure: update on publiclyreported outcomes measures based on the 2010 release.Circ Cardiovasc Qual Outcomes. 2010;3:459–67.
158. Bernheim SM, Spertus JA, Reid KJ, et al. Socioeconomicdisparities in outcomes after acute myocardial infarction.Am Heart J. 2007;153:313–9.
159. Rahimi AR, Spertus JA, Reid KJ, et al. Financial barriers tohealth care and outcomes after acute myocardial infarction.JAMA. 2007;297:1063–72.
160. Smolderen KG, Spertus JA, Reid KJ, et al. The association ofcognitive and somatic depressive symptoms with depres-sion recognition and outcomes after myocardial infarction.Circ Cardiovasc Qual Outcomes. 2009;2:328–37.
161. Zamorano JL, Badano LP, Bruce C, et al. EAE/ASE recom-mendations for the use of echocardiography in new trans-catheter interventions for valvular heart disease. J Am SocEchocardiogr. 2011;24:937–65.
162. Messika-Zeitoun D, Serfaty JM, Brochet E, et al. Multi-modal assessment of the aortic annulus diameter: implica-tions for transcatheter aortic valve implantation. J Am CollCardiol. 2010;55:186–94.
163. Delgado V, Tops LF, Schuijf JD, et al. Successful deploymentof a transcatheter aortic valve in bicuspid aortic stenosis: roleof imaging with multislice computed tomography. Circ Car-diovasc Imaging. 2009;2:e12–3.
164. Akhtar M, Tuzcu EM, Kapadia SR, et al. Aortic root mor-phology in patients undergoing percutaneous aortic valvereplacement: evidence of aortic root remodeling. J ThoracCardiovasc Surg. 2009;137:950–6.
165. Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recom-mendations for evaluation of the severity of native valvularregurgitation with two-dimensional and Doppler echocar-diography. J Am Soc Echocardiogr. 2003;16:777–802.
166. Ng AC, Delgado V, van der Kley F, et al. Comparison ofaortic root dimensions and geometries before and aftertranscatheter aortic valve implantation by 2- and 3-dimen-
sional transesophageal echocardiography and multislice
1384 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
computed tomography. Circ Cardiovasc Imaging.2010;3:94–102.
167. Janosi RA, Kahlert P, Plicht B, et al. Measurement of theaortic annulus size by real-time three-dimensional trans-esophageal echocardiography. Minim Invasive Ther AlliedTechnol. 2011;20:85–94.
168. Schoenhagen P, Tuzcu EM, Kapadia SR, et al. Three-dimensional imaging of the aortic valve and aortic root withcomputed tomography: new standards in an era of trans-catheter valve repair/implantation. Eur Heart J. 2009;30:2079–86.
169. Al Ali AM, Altwegg L, Horlick EM, et al. Prevention andmanagement of transcatheter balloon-expandable aorticvalve malposition. Catheter Cardiovasc Interv. 2008;72:573–8.
170. Schwartz JG, Neubauer AM, Fagan TE, et al. Potential roleof three-dimensional rotational angiography and C-arm CTfor valvular repair and implantation. Int J Cardiovasc Im-aging. 2011;27:1205–22.
171. Koos R, Altiok E, Mahnken AH, et al. Evaluation of aorticroot for definition of prosthesis size by magnetic resonanceimaging and cardiac computed tomography: implicationsfor transcatheter aortic valve implantation. Int J Cardiol.2011: published online before print February 9, 2011, doi:10.1016/j.ijcard.2011.01.044. Accessed January 13, 2012.
172. Schoenhagen P, Numburi U, Halliburton SS, et al. Three-dimensional imaging in the context of minimally invasiveand transcatheter cardiovascular interventions usingmulti-detector computed tomography: from pre-operative planning to intra-operative guidance. EurHeart J. 2010;31:2727– 40.
173. Chenot F, Montant P, Goffinet C, et al. Evaluation ofanatomic valve opening and leaflet morphology in aorticvalve bioprosthesis by using multidetector CT: comparisonwith transthoracic echocardiography. Radiology. 2010;255:377–85.
174. Earls JP, Berman EL, Urban BA, et al. Prospectively gatedtransverse coronary CT angiography versus retrospectivelygated helical technique: improved image quality and re-duced radiation dose. Radiology. 2008;246:742–53.
175. Feuchtner G, Goetti R, Plass A, et al. Dual-step prospectiveECG-triggered 128-slice dual-source CT for evaluation ofcoronary arteries and cardiac function without heart ratecontrol: a technical note. Eur Radiol. 2010;20:2092–9.
176. Bagur R, Webb JG, Nietlispach F, et al. Acute kidney injuryfollowing transcatheter aortic valve implantation: predic-tive factors, prognostic value, and comparison with surgicalaortic valve replacement. Eur Heart J. 2010;31:865–74.
177. Joshi SB, Mendoza DD, Steinberg DH, et al. Ultra-low-doseintra-arterial contrast injection for iliofemoral computedtomographic angiography. J Am Coll Cardiol Img. 2009;2:1404–11.
178. Moss RR, Ivens E, Pasupati S, et al. Role of echocardiogra-phy in percutaneous aortic valve implantation. J Am CollCardiol Img. 2008;1:15–24.
179. Leipsic J, Gurvitch R, Labounty TM, et al. Multidetectorcomputed tomography in transcatheter aortic valve im-plantation. J Am Coll Cardiol Img. 2011;4:416–29.
180. O’Brien B, Schoenhagen P, Kapadia SR, et al. Integration of3D imaging data in the assessment of aortic stenosis:impact on classification of disease severity. Circ CardiovascImaging. 2011;4:566–73.
181. Pontone G, Andreini D, Bartorelli AL, et al. Feasibility andaccuracy of a comprehensive multidetector computed to-mography acquisition for patients referred for balloon-expandable transcatheter aortic valve implantation. AmHeart J. 2011;161:1106–13.
182. Schulz KF, Altman DG, Moher D. CONSORT 2010 state-ment: updated guidelines for reporting parallel group ran-domized trials. Ann Intern Med. 2010;152:726–32.
183. Tops LF, Wood DA, Delgado V, et al. Noninvasive evalua-
tion of the aortic root with multislice computed tomogra-phy implications for transcatheter aortic valve replacement.J Am Coll Cardiol Img. 2008;1:321–30.
184. Masson JB, Kovac J, Schuler G, et al. Transcatheter aorticvalve implantation: review of the nature, management, andavoidance of procedural complications. J Am Coll CardiolIntv. 2009;2:811–20.
185. Delgado V, Ng AC, van de Veire NR, et al. Transcatheteraortic valve implantation: role of multi-detector row com-puted tomography to evaluate prosthesis positioning anddeployment in relation to valve function. Eur Heart J.2010;31:1114–23.
186. Gurvitch R, Wood DA, Leipsic J, et al. Multislice computedtomography for prediction of optimal angiographic deploy-ment projections during transcatheter aortic valve implan-tation. J Am Coll Cardiol Intv. 2010;3:1157–65.
187. Kurra V, Kapadia SR, Tuzcu EM, et al. Pre-proceduralimaging of aortic root orientation and dimensions: compar-ison between x-ray angiographic planar imaging and 3-di-mensional multidetector row computed tomography. J AmColl Cardiol Intv. 2010;3:105–13.
188. Jabbour A, Ismail TF, Moat N, et al. Multimodality imagingin transcatheter aortic valve implantation and post-procedural aortic regurgitation: comparison among cardio-vascular magnetic resonance, cardiac computed tomogra-phy, and echocardiography. J Am Coll Cardiol. 2011;58:2165–73.
189. Yucel EK, Anderson CM, Edelman RR, et al. AHA scientificstatement. Magnetic resonance angiography: update onapplications for extracranial arteries. Circulation. 1999;100:2284–301.
190. Sherif MA, Abdel-Wahab M, Beurich HW, et al. Haemody-namic evaluation of aortic regurgitation after transcatheteraortic valve implantation using cardiovascular magnetic res-onance. EuroIntervention. 2011;7:57–63.
191. Juluru K, Vogel-Claussen J, Macura KJ, et al. MR imaging inpatients at risk for developing nephrogenic systemic fibro-sis: protocols, practices, and imaging techniques to maxi-mize patient safety. Radiographics. 2009;29:9–22.
192. Billings FT, Kodali SK, Shanewise JS. Transcatheter aorticvalve implantation: anesthetic considerations. AnesthAnalg. 2009;108:1453–62.
193. Klein AA, Webb ST, Tsui S, et al. Transcatheter aortic valveinsertion: anaesthetic implications of emerging new tech-nology. Br J Anaesth. 2009;103:792–9.
194. Guinot PG, Depoix JP, Etchegoyen L, et al. Anesthesia andperioperative management of patients undergoing trans-catheter aortic valve implantation: analysis of 90 consecu-tive patients with focus on perioperative complications.J Cardiothorac Vasc Anesth. 2010;24:752–61.
195. Burnakis TG, Berman DE. Hostility and hallucinations as aconsequence of midazolam administration. DICP. 1989;23:671–2.
196. Latsios G, Gerckens U, Buellesfeld L, et al. “Device landingzone” calcification, assessed by MSCT, as a predictivefactor for pacemaker implantation after TAVI. CatheterCardiovasc Interv. 2010;76:431–9.
197. Fassl J, Seeberger MD, Augoustides JG. Transcatheter aor-tic valve implantation: is general anesthesia superior toconscious sedation? J Cardiothorac Vasc Anesth. 2011;25:576–7.
198. Kurra V, Schoenhagen P, Roselli EE, et al. Prevalence ofsignificant peripheral artery disease in patients evaluatedfor percutaneous aortic valve insertion: preprocedural as-sessment with multidetector computed tomography. J Tho-rac Cardiovasc Surg. 2009;137:1258–64.
199. Sharp AS, Michev I, Maisano F, et al. A new technique forvascular access management in transcatheter aortic valveimplantation. Catheter Cardiovasc Interv. 2010;75:784–93.
200. Etienne PY, Papadatos S, El Khoury E, et al. Transaortictranscatheter aortic valve implantation with the EdwardsSAPIEN valve: feasibility, technical considerations, and
clinical advantages. Ann Thorac Surg. 2011;92:746–8.
1385Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
201. Guarracino F, Cabrini L, Baldassarri R, et al. Non-invasiveventilation-aided transoesophageal echocardiography inhigh-risk patients: a pilot study. Eur J Echocardiogr. 2010;11:554–6.
202. Bartel T, Bonaros N, Muller L, et al. Intracardiac echocar-diography: a new guiding tool for transcatheter aortic valvereplacement. J Am Soc Echocardiogr. 2011;24:966–75.
203. Cahalan MK, Stewart W, Pearlman A, et al. AmericanSociety of Echocardiography and Society of CardiovascularAnesthesiologists task force guidelines for training in peri-operative echocardiography. J Am Soc Echocardiogr. 2002;15:647–52.
204. Al-Attar N, Himbert D, Vahanian A, et al. Severe intrapros-thetic regurgitation by immobile leaflet after trans-catheteraortic valve implantation. Eur J Cardiothorac Surg. 2011;39:591–2.
205. Ussia GP, Sarkar K, Tamburino C. Aortic valve perforationduring aortic valvuloplasty: identification and strategies forprevention. Catheter Cardiovasc Interv. 2011;77:876–80.
206. Ussia GP, Barbanti M, Ramondo A, et al. The valve-in-valvetechnique for treatment of aortic bioprosthesis malpositionan analysis of incidence and 1-year clinical outcomes fromthe Italian CoreValve registry. J Am Coll Cardiol. 2011;57:1062–8.
207. Sherif MA, Abdel-Wahab M, Stocker B, et al. Anatomic andprocedural predictors of paravalvular aortic regurgitationafter implantation of the Medtronic CoreValve bioprosthe-sis. J Am Coll Cardiol. 2010;56:1623–9.
208. Latib A, Michev I, Laborde JC, et al. Post-implantationrepositioning of the CoreValve percutaneous aortic valve.J Am Coll Cardiol Intv. 2010;3:119–21.
209. Webb JG, Wood DA, Ye J, et al. Transcatheter valve-in-valve implantation for failed bioprosthetic heart valves.Circulation. 2010;121:1848–57.
210. Ruiz CE, Cohen H, Del Valle-Fernandez R, et al. Closure ofprosthetic paravalvular leaks: a long way to go. Eur Heart JSuppl. 2010;12 Suppl E:E52–62.
211. Schultz CJ, Moelker A, Piazza N, et al. Three dimensionalevaluation of the aortic annulus using multislice computertomography: are manufacturer’s guidelines for sizing forpercutaneous aortic valve replacement helpful? Eur Heart J.2010;31:849–56.
212. Babaliaros VC, Liff D, Chen EP, et al. Can balloon aorticvalvuloplasty help determine appropriate transcatheteraortic valve size? J Am Coll Cardiol Intv. 2008;1:580–6.
213. Witzke C, Don CW, Cubeddu RJ, et al. Impact of rapidventricular pacing during percutaneous balloon aortic val-vuloplasty in patients with critical aortic stenosis: shouldwe be using it? Catheter Cardiovasc Interv. 2010;75:444–52.
214. Gurvitch R, Tay EL, Wijesinghe N, et al. Transcatheteraortic valve implantation: lessons from the learning curveof the first 270 high-risk patients. Catheter CardiovascInterv. 2011;78:977–84.
215. Nuis RJ, Van Mieghem NM, Van der Boon RM, et al. Effectof experience on results of transcatheter aortic valve im-plantation using a Medtronic CoreValve System. Am JCardiol. 2011;107:1824–9.
216. Webb JG, Pasupati S, Humphries K, et al. Percutaneoustransarterial aortic valve replacement in selected high-riskpatients with aortic stenosis. Circulation. 2007;116:755–63.
217. Webb JG, Altwegg L, Boone RH, et al. Transcatheter aorticvalve implantation: impact on clinical and valve-relatedoutcomes. Circulation. 2009;119:3009–16.
218. Tommaso C, Bolman RM, Feldman T, et al. Multisocietyexpert consensus statement: operator & institutional require-ments for transcatheter valve repair and replacement; part 1TAVR. J Am Coll Cardiol. 2012. March 1 [E-pub ahead ofprint], doi: 10.1016/j.jacc.2012.02.016.
219. Himbert D, Roy D, Brecker S, et al. Tools & techniques:transcatheter aortic valve implantation: transfemoral ap-proach. EuroIntervention. 2011;6:784–5.
220. Gurvitch R, Cheung A, Bedogni F, et al. Coronary obstruc-tion following transcatheter aortic valve-in-valve implanta-
tion for failed surgical bioprostheses. Catheter CardiovascInterv. 2011;77:439–44.
221. Ussia GP, Scarabelli M, Mule M, et al. Postproceduralmanagement of patients after transcatheter aortic valveimplantation procedure with self-expanding bioprosthesis.Catheter Cardiovasc Interv. 2010;76:757–66.
222. Burkhoff D, O’Neill W, Brunckhorst C, et al. Feasibilitystudy of the use of the TandemHeart percutaneous ventric-ular assist device for treatment of cardiogenic shock. Cath-eter Cardiovasc Interv. 2006;68:211–7.
223. Maganti MD, Rao V, Borger MA, et al. Predictors of lowcardiac output syndrome after isolated aortic valve surgery.Circulation. 2005;112:I448–52.
224. Suh WM, Witzke CF, Palacios IF. Suicide left ventriclefollowing transcatheter aortic valve implantation. CatheterCardiovasc Interv. 2010;76:616–20.
225. Abdel-Wahab M, Zahn R, Horack M, et al. Aortic regurgita-tion after transcatheter aortic valve implantation: incidenceand early outcome. Results from the German transcatheteraortic valve interventions registry. Heart. 2011;97:899–906.
226. Himbert D, Brochet E, Serfaty JM, et al. Contained aorticroot rupture after transcatheter aortic valve implantation.Eur Heart J. 2010;31:2995.
227. Grube E, Laborde JC, Gerckens U, et al. Percutaneousimplantation of the CoreValve self-expanding valve pros-thesis in high-risk patients with aortic valve disease: theSiegburg first-in-man study. Circulation. 2006;114:1616–24.
228. Grube E, Schuler G, Buellesfeld L, et al. Percutaneous aorticvalve replacement for severe aortic stenosis in high-riskpatients using the second- and current third-generationself-expanding CoreValve prosthesis: device success and30-day clinical outcome. J Am Coll Cardiol. 2007;50:69–76.
229. Khawaja MZ, Rajani R, Cook A, et al. Permanent pace-maker insertion after CoreValve transcatheter aortic valveimplantation: incidence and contributing factors (the UKCoreValve Collaborative). Circulation. 2011;123:951–60.
230. Haworth P, Behan M, Khawaja M, et al. Predictors forpermanent pacing after transcatheter aortic valve implan-tation. Catheter Cardiovasc Interv. 2010;76:751–6.
231. Sinhal A, Altwegg L, Pasupati S, et al. Atrioventricularblock after transcatheter balloon expandable aortic valveimplantation. J Am Coll Cardiol Intv. 2008;1:305–9.
232. Tuzcu EM. Transcatheter aortic valve replacement mal-position and embolization: innovation brings solutionsalso new challenges. Catheter Cardiovasc Interv. 2008;72:579 – 80.
233. Tay EL, Gurvitch R, Wijeysinghe N, et al. Outcome ofpatients after transcatheter aortic valve embolization. J AmColl Cardiol Intv. 2011;4:228–34.
234. Aminian A, Lalmand J, El Nakadi B. Perforation of thedescending thoracic aorta during transcatheter aortic valveimplantation (TAVI): an unexpected and dramatic proce-dural complication. Catheter Cardiovasc Interv. 2011;77:1076–8.
235. Sun JC, Davidson MJ, Lamy A, et al. Antithrombotic man-agement of patients with prosthetic heart valves: currentevidence and future trends. Lancet. 2009;374:565–76.
236. Clavel MA, Rodes-Cabau J, Dumont E, et al. Validation andcharacterization of transcatheter aortic valve effective ori-fice area measured by Doppler echocardiography. J AmColl Cardiol Img. 2011;4:1053–62.
237. Clavel MA, Webb JG, Pibarot P, et al. Comparison of thehemodynamic performance of percutaneous and surgicalbioprostheses for the treatment of severe aortic stenosis.J Am Coll Cardiol. 2009;53:1883–91.
238. Pibarot P, Dumesnil JG. Hemodynamic and clinical impactof prosthesis-patient mismatch in the aortic valve positionand its prevention. J Am Coll Cardiol. 2000;36:1131–41.
239. Mohty D, Malouf JF, Girard SE, et al. Impact of prosthesis-patient mismatch on long-term survival in patients withsmall St Jude Medical mechanical prostheses in the aortic
position. Circulation. 2006;113:420–6.
1386 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
240. Blais C, Dumesnil JG, Baillot R, et al. Impact of valveprosthesis-patient mismatch on short-term mortality afteraortic valve replacement. Circulation. 2003;108:983–8.
241. Gutierrez M, Rodes-Cabau J, Bagur R, et al. Electrocardio-graphic changes and clinical outcomes after transapicalaortic valve implantation. Am Heart J. 2009;158:302–8.
242. Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients withatrial fibrillation: a report of the American College ofCardiology Foundation/American Heart Association TaskForce on Practice Guidelines. J Am Coll Cardiol. 2011;57:e101–98.
243. Morgenstern LB, Hemphill JC III, Anderson C, et al. Guide-lines for the management of spontaneous intracerebralhemorrhage: a guideline for healthcare professionals fromthe American Heart Association/American Stroke Associa-tion. Stroke. 2010;41:2108–29.
244. Adams HP Jr., del Zoppo G, Alberts MJ, et al. Guidelines forthe early management of adults with ischemic stroke: aguideline from the American Heart Association/AmericanStroke Association Stroke Council, Clinical CardiologyCouncil, Cardiovascular Radiology and Intervention Coun-cil, and the Atherosclerotic Peripheral Vascular Diseaseand Quality of Care Outcomes in Research Interdisciplin-ary Working Groups: the American Academy of Neurologyaffirms the value of this guideline as an educational tool forneurologists. Stroke. 2007;38:1655–711.
245. Douglas PS, Garcia MJ, Haines DE, et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 appro-priate use criteria for echocardiography. A report of theAmerican College of Cardiology Foundation AppropriateUse Criteria Task Force, American Society of Echocardiog-raphy, American Heart Association, American Society ofNuclear Cardiology, Heart Failure Society of America,Heart Rhythm Society, Society for Cardiovascular Angiog-raphy and Interventions, Society of Critical Care Medicine,Society of Cardiovascular Computed Tomography, andSociety for Cardiovascular Magnetic Resonance. J Am CollCardiol. 2011;57:1126–66.
246. Webb J, Cribier A. Percutaneous transarterial aortic valveimplantation: what do we know? Eur Heart J. 2011;32:140–7.
247. Lutter G, Kuklinski D, Berg G, et al. Percutaneous aorticvalve replacement: an experimental study. I. Studies onimplantation. J Thorac Cardiovasc Surg. 2002;123:768–76.
248. Levi DS, Kusnezov N, Carman GP. Smart materials appli-
cations for pediatric cardiovascular devices. Pediatr Res.2008;63:552–8.249. Dainese L, Fusari M, Trabattoni P, et al. Redo in aortichomograft replacement: transcatheter aortic valve as a validalternative to surgical replacement. J Thorac CardiovascSurg. 2010;139:1656–7.
250. de Weger A, Ewe SH, Delgado V, et al. First-in-manimplantation of a trans-catheter aortic valve in a mitralannuloplasty ring: novel treatment modality for failedmitral valve repair. Eur J Cardiothorac Surg. 2011;39:1054 – 6.
251. Kelpis TG, Mezilis NE, Ninios VN, et al. Minimally invasivetransapical aortic valve-in-a-valve implantation for severeaortic regurgitation in a degenerated stentless bioprosthe-sis. J Thorac Cardiovasc Surg. 2009;138:1018–20.
252. Maroto LC, Rodriguez JE, Cobiella J, et al. Transapical off-pump aortic valve-in-a-valve implantation in two elderlypatients with a degenerated porcine bioprosthesis. Eur J Car-diothorac Surg. 2010;37:738–40.
253. Rodes-Cabau J, Dumont E, Doyle D, et al. Transcathetervalve-in-valve implantation for the treatment of stentlessaortic valve dysfunction. J Thorac Cardiovasc Surg. 2010;140:246–8.
254. Walther T, Kempfert J, Borger MA, et al. Human minimallyinvasive off-pump valve-in-a-valve implantation. Ann Tho-rac Surg. 2008;85:1072–3.
255. Mack MJ. Coronary obstruction following transcatheteraortic valve-in-valve implantation for failed surgical bio-prostheses. Catheter Cardiovasc Interv. 2011;77:445–6.
256. Wijesinghe N, Ye J, Rodes-Cabau J, et al. Transcatheteraortic valve implantation in patients with bicuspid aorticvalve stenosis. J Am Coll Cardiol Intv. 2010;3:1122–5.
257. Chiam PT, Chao VT, Tan SY, et al. Percutaneous transcath-eter heart valve implantation in a bicuspid aortic valve.J Am Coll Cardiol Intv. 2010;3:559–61.
258. Ivers NM, Taljaard M, Dixon S, et al. Impact of CONSORTextension for cluster randomised trials on quality of report-ing and study methodology: review of random sample of300 trials, 2000-8. BMJ. 2011;343:d5886.
259. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMAstatement for reporting systematic reviews and meta-analyses of studies that evaluate health care interven-tions: explanation and elaboration. J Clin Epidemiol.2009;62:e1–34.
260. Rios LP, Ye C, Thabane L. Association between framing ofthe research question using the PICOT format and report-
ing quality of randomized controlled trials. BMC Med ResMethodol. 2010;10:11.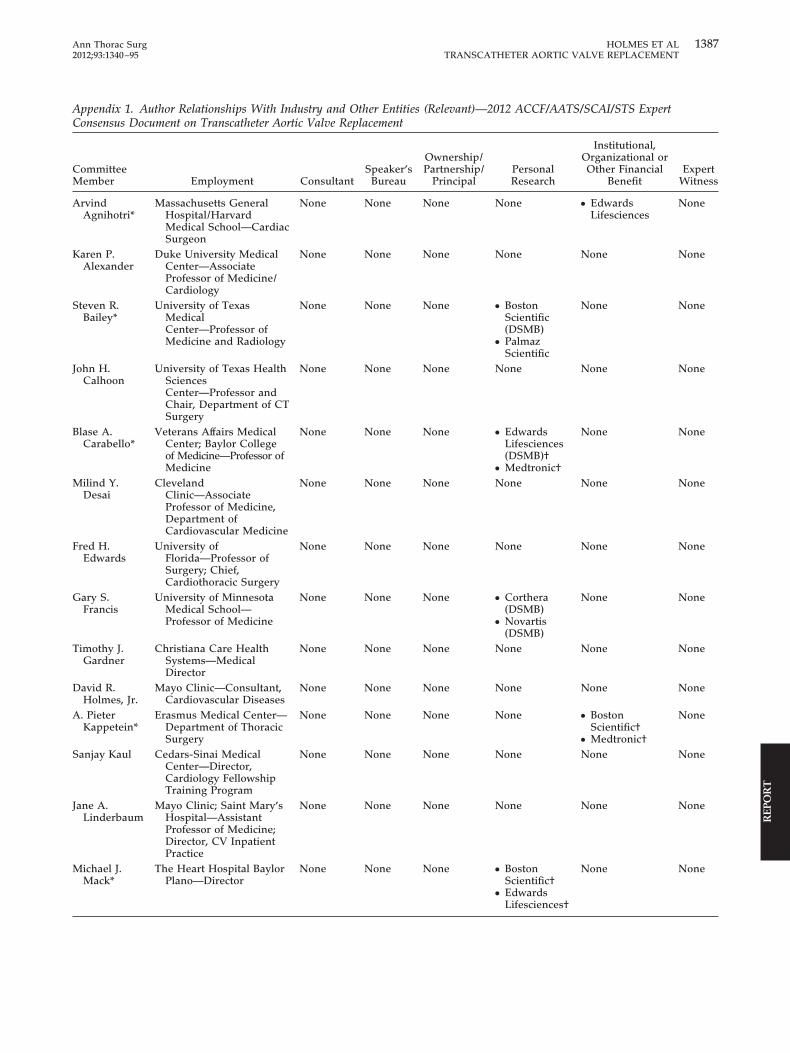
1387Ann Thorac Surg HOLMES ET AL2012;93:1340–95 TRANSCATHETER AORTIC VALVE REPLACEMENT
REP
OR
T
Appendix 1. Author Relationships With Industry and Other Entities (Relevant)—2012 ACCF/AATS/SCAI/STS ExpertConsensus Document on Transcatheter Aortic Valve Replacement
CommitteeMember Employment Consultant
Speaker’sBureau
Ownership/Partnership/
PrincipalPersonalResearch
Institutional,Organizational orOther Financial
BenefitExpert
Witness
ArvindAgnihotri*
Massachusetts GeneralHospital/HarvardMedical School—CardiacSurgeon
None None None None ● EdwardsLifesciences
None
Karen P.Alexander
Duke University MedicalCenter—AssociateProfessor of Medicine/Cardiology
None None None None None None
Steven R.Bailey*
University of TexasMedicalCenter—Professor ofMedicine and Radiology
None None None ● BostonScientific(DSMB)
● PalmazScientific
None None
John H.Calhoon
University of Texas HealthSciencesCenter—Professor andChair, Department of CTSurgery
None None None None None None
Blase A.Carabello*
Veterans Affairs MedicalCenter; Baylor Collegeof Medicine—Professor ofMedicine
None None None ● EdwardsLifesciences(DSMB)†
● Medtronic†
None None
Milind Y.Desai
ClevelandClinic—AssociateProfessor of Medicine,Department ofCardiovascular Medicine
None None None None None None
Fred H.Edwards
University ofFlorida—Professor ofSurgery; Chief,Cardiothoracic Surgery
None None None None None None
Gary S.Francis
University of MinnesotaMedical School—Professor of Medicine
None None None ● Corthera(DSMB)
● Novartis(DSMB)
None None
Timothy J.Gardner
Christiana Care HealthSystems—MedicalDirector
None None None None None None
David R.Holmes, Jr.
Mayo Clinic—Consultant,Cardiovascular Diseases
None None None None None None
A. PieterKappetein*
Erasmus Medical Center—Department of ThoracicSurgery
None None None None ● BostonScientific†
● Medtronic†
None
Sanjay Kaul Cedars-Sinai MedicalCenter—Director,Cardiology FellowshipTraining Program
None None None None None None
Jane A.Linderbaum
Mayo Clinic; Saint Mary’sHospital—AssistantProfessor of Medicine;Director, CV InpatientPractice
None None None None None None
Michael J.Mack*
The Heart Hospital BaylorPlano—Director
None None None ● BostonScientific†
● EdwardsLifesciences†
None None

1388 HOLMES ET AL Ann Thorac SurgTRANSCATHETER AORTIC VALVE REPLACEMENT 2012;93:1340–95
REPO
RT
CommitteeMember Employment Consultant
Speaker’sBureau
Ownership/Partnership/
PrincipalPersonalResearch
Institutional,Organizational orOther Financial
BenefitExpert
Witness
ChirojitMukherjee
Heart Center LeipzigUniversity of Leipzig,Germany—SeniorConsultant & DirectorFellowship ProgramAnesthesia and IntensiveMedicine II
None None None None None None
DebabrataMukherjee
Texas Tech UniversityHealth SciencesCenter—Chief,Cardiovascular Medicine
None None None None None None
Catherine M.Otto
University of Washington,Divisionof Cardiology—Professorof Medicine
None None None None None None
Carlos E. Ruiz Lenox Hill Heart andVascular Institute ofNew York—Professorand Chief, Division ofPediatric Cardiology
None None None None None None
Ralph L.Sacco
Miller School of Medicine,Jackson MemorialHospital, University ofMiami—Chairman ofNeurology, Professor ofNeurology, PublicHealth & Epidemiology,Human Genetics, andNeurosurgery; ExecutiveDirector, McKnightBrain Institute
None None None None None None
DonnetteSmith
MendedHearts—ConsumerAdvocate
None None None None None None
James D.Thomas
Cleveland ClinicFoundation—MooreChair of CardiovascularImaging
None None None None None None
* Recused from writing initial text and voting on document recommendations due to relevant relationships with industry to this document.
† No financial benefit.
This table represents the relationships of committee members with industry and other entities that were determined to be relevant to this document.These relationships were reviewed and updated in conjunction with all meetings and/or conference calls of the writing committee during the documentdevelopment process. The table does not necessarily reflect relationships with industry at the time of publication. A person is deemed to have asignificant interest in a business if the interest represents ownership of 5% or more of the voting stock or share of the business entity, or ownership of�$10,000 of the fair market value of the business entity; or if funds received by the person from the business entity exceed 5% of the person’s gross incomefor the previous year. Relationships that exist with no financial benefit are also included for the purpose of transparency. Relationships in this table aremodest unless otherwise noted. Please refer to http://www.cardiosource.org/Science-And-Quality/Practice-Guidelines-and-Quality-Standards/Rela-tionships-With-Industry-Policy.aspx for definitions of disclosure categories or additional information about the ACCF Disclosure Policy for WritingCommittees.
According to the ACCF, a person has a relevant relationship IF: a) the relationship or interest relates to the same or similar subject matter, intellectualproperty or asset, topic, or issue addressed in the document; or b) the company/entity (with whom the relationship exists) makes a drug, drug class, ordevice addressed in the document, or makes a competing drug or device addressed in the document; or c) the person or a member of the person’shousehold, has a reasonable potential for financial, professional or other personal gain or loss as a result of the issues/content addressed in the document.
DSMB � Data Safety Monitoring Board.
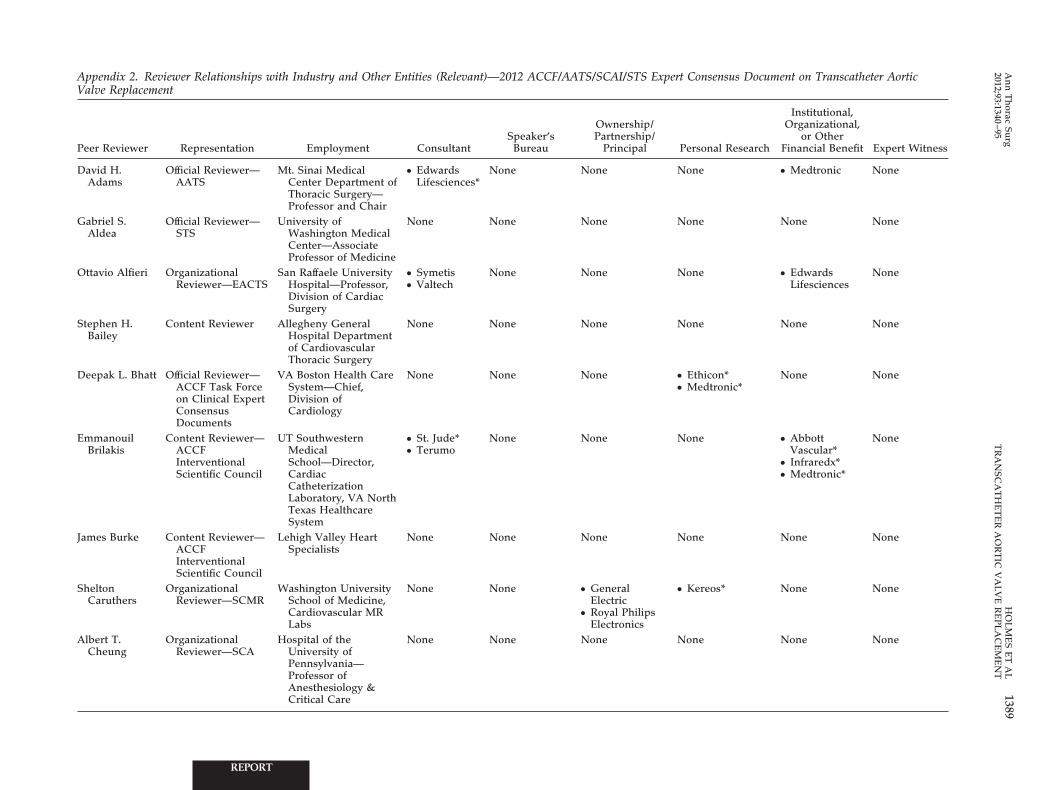
Appendix 2. Reviewer Relationships with Industry and Other Entities (Relevant)—2012 ACCF/AATS/SCAI/STS Expert Consensus Document on Transcatheter AorticValve Replacement
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
David H.Adams
Official Reviewer—AATS
Mt. Sinai MedicalCenter Department ofThoracic Surgery—Professor and Chair
● EdwardsLifesciences*
None None None ● Medtronic None
Gabriel S.Aldea
Official Reviewer—STS
University ofWashington MedicalCenter—AssociateProfessor of Medicine
None None None None None None
Ottavio Alfieri OrganizationalReviewer—EACTS
San Raffaele UniversityHospital—Professor,Division of CardiacSurgery
● Symetis● Valtech
None None None ● EdwardsLifesciences
None
Stephen H.Bailey
Content Reviewer Allegheny GeneralHospital Departmentof CardiovascularThoracic Surgery
None None None None None None
Deepak L. Bhatt Official Reviewer—ACCF Task Forceon Clinical ExpertConsensusDocuments
VA Boston Health CareSystem—Chief,Division ofCardiology
None None None ● Ethicon*● Medtronic*
None None
EmmanouilBrilakis
Content Reviewer—ACCFInterventionalScientific Council
UT SouthwesternMedicalSchool—Director,CardiacCatheterizationLaboratory, VA NorthTexas HealthcareSystem
● St. Jude*● Terumo
None None None ● AbbottVascular*
● Infraredx*● Medtronic*
None
James Burke Content Reviewer—ACCFInterventionalScientific Council
Lehigh Valley HeartSpecialists
None None None None None None
SheltonCaruthers
OrganizationalReviewer—SCMR
Washington UniversitySchool of Medicine,Cardiovascular MRLabs
None None ● GeneralElectric
● Royal PhilipsElectronics
● Kereos* None None
Albert T.Cheung
OrganizationalReviewer—SCA
Hospital of theUniversity ofPennsylvania—Professor ofAnesthesiology &Critical Care
None None None None None None
1389A
nn
Th
oracSu
rgH
OL
ME
SE
TA
L2012;93:1340
–95T
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
REPORT
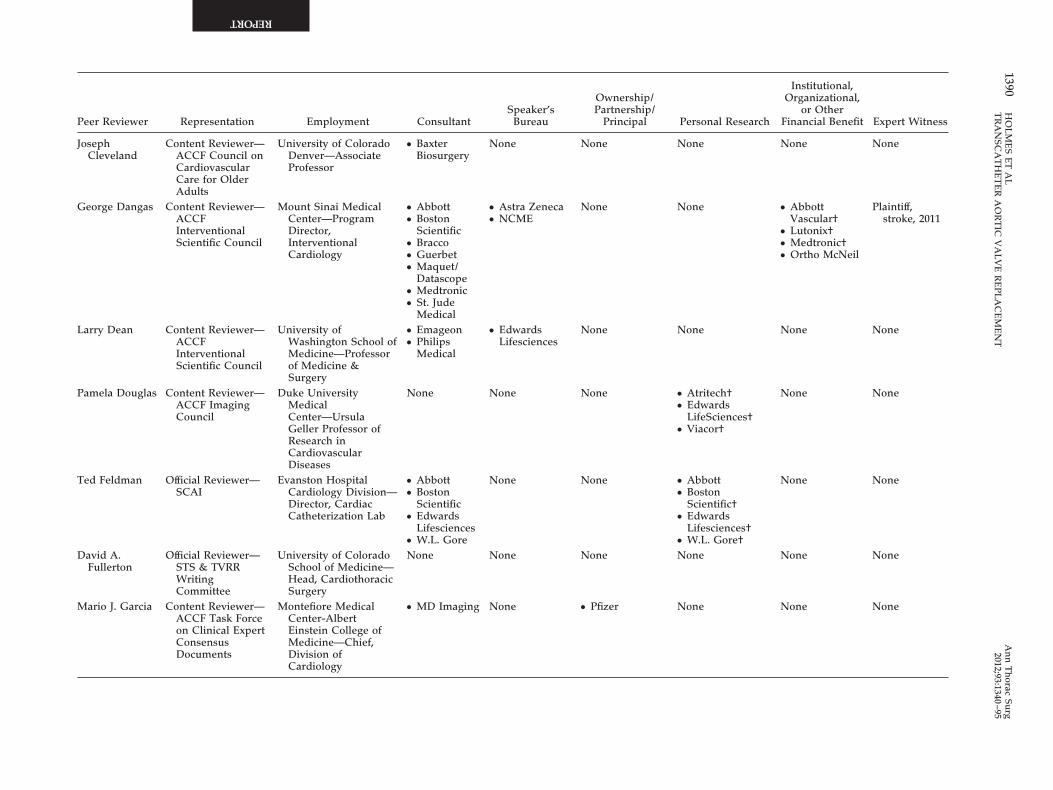
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
JosephCleveland
Content Reviewer—ACCF Council onCardiovascularCare for OlderAdults
University of ColoradoDenver—AssociateProfessor
● BaxterBiosurgery
None None None None None
George Dangas Content Reviewer—ACCFInterventionalScientific Council
Mount Sinai MedicalCenter—ProgramDirector,InterventionalCardiology
● Abbott● Boston
Scientific● Bracco● Guerbet● Maquet/
Datascope● Medtronic● St. Jude
Medical
● Astra Zeneca● NCME
None None ● AbbottVascular†
● Lutonix†● Medtronic†● Ortho McNeil
Plaintiff,stroke, 2011
Larry Dean Content Reviewer—ACCFInterventionalScientific Council
University ofWashington School ofMedicine—Professorof Medicine &Surgery
● Emageon● Philips
Medical
● EdwardsLifesciences
None None None None
Pamela Douglas Content Reviewer—ACCF ImagingCouncil
Duke UniversityMedicalCenter—UrsulaGeller Professor ofResearch inCardiovascularDiseases
None None None ● Atritech†● Edwards
LifeSciences†● Viacor†
None None
Ted Feldman Official Reviewer—SCAI
Evanston HospitalCardiology Division—Director, CardiacCatheterization Lab
● Abbott● Boston
Scientific● Edwards
Lifesciences● W.L. Gore
None None ● Abbott● Boston
Scientific†● Edwards
Lifesciences†● W.L. Gore†
None None
David A.Fullerton
Official Reviewer—STS & TVRRWritingCommittee
University of ColoradoSchool of Medicine—Head, CardiothoracicSurgery
None None None None None None
Mario J. Garcia Content Reviewer—ACCF Task Forceon Clinical ExpertConsensusDocuments
Montefiore MedicalCenter-AlbertEinstein College ofMedicine—Chief,Division ofCardiology
● MD Imaging None ● Pfizer None None None
1390H
OL
ME
SE
TA
LA
nn
Th
oracSu
rgT
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
2012;93:1340–95
REPORT
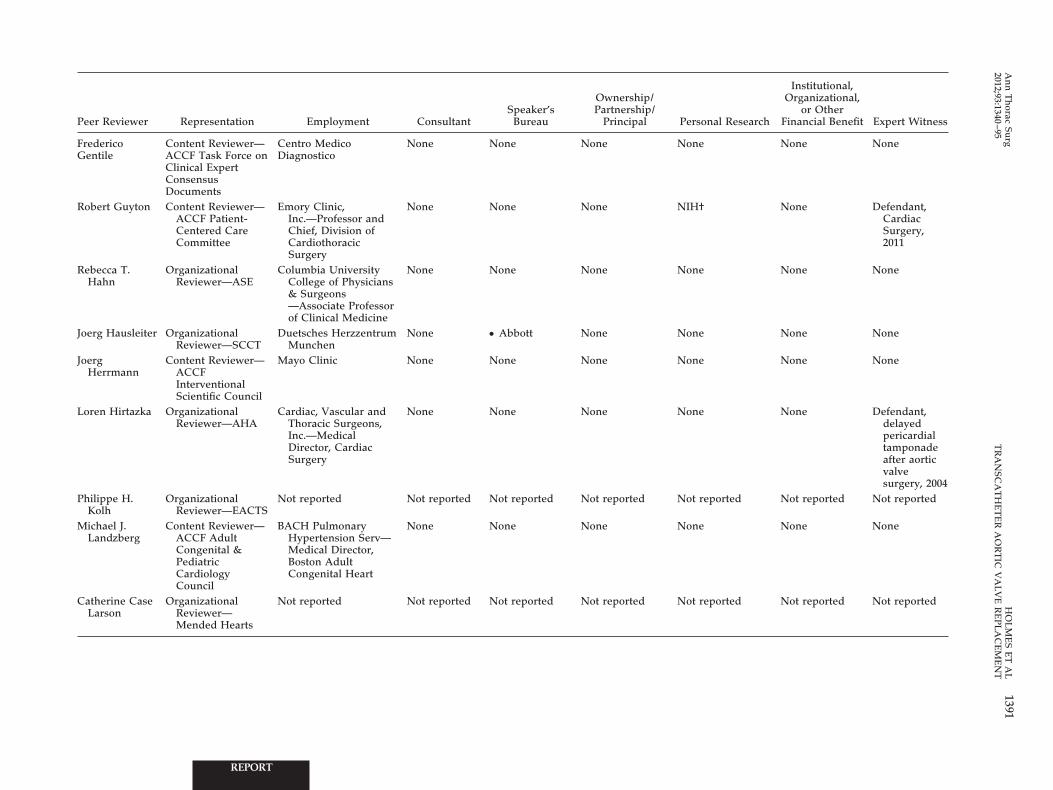
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
FredericoGentile
Content Reviewer—ACCF Task Force onClinical ExpertConsensusDocuments
Centro MedicoDiagnostico
None None None None None None
Robert Guyton Content Reviewer—ACCF Patient-Centered CareCommittee
Emory Clinic,Inc.—Professor andChief, Division ofCardiothoracicSurgery
None None None NIH† None Defendant,CardiacSurgery,2011
Rebecca T.Hahn
OrganizationalReviewer—ASE
Columbia UniversityCollege of Physicians& Surgeons—Associate Professorof Clinical Medicine
None None None None None None
Joerg Hausleiter OrganizationalReviewer—SCCT
Duetsches HerzzentrumMunchen
None ● Abbott None None None None
JoergHerrmann
Content Reviewer—ACCFInterventionalScientific Council
Mayo Clinic None None None None None None
Loren Hirtazka OrganizationalReviewer—AHA
Cardiac, Vascular andThoracic Surgeons,Inc.—MedicalDirector, CardiacSurgery
None None None None None Defendant,delayedpericardialtamponadeafter aorticvalvesurgery, 2004
Philippe H.Kolh
OrganizationalReviewer—EACTS
Not reported Not reported Not reported Not reported Not reported Not reported Not reported
Michael J.Landzberg
Content Reviewer—ACCF AdultCongenital &PediatricCardiologyCouncil
BACH PulmonaryHypertension Serv—Medical Director,Boston AdultCongenital Heart
None None None None None None
Catherine CaseLarson
OrganizationalReviewer—Mended Hearts
Not reported Not reported Not reported Not reported Not reported Not reported Not reported
1391A
nn
Th
oracSu
rgH
OL
ME
SE
TA
L2012;93:1340
–95T
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
REPORT
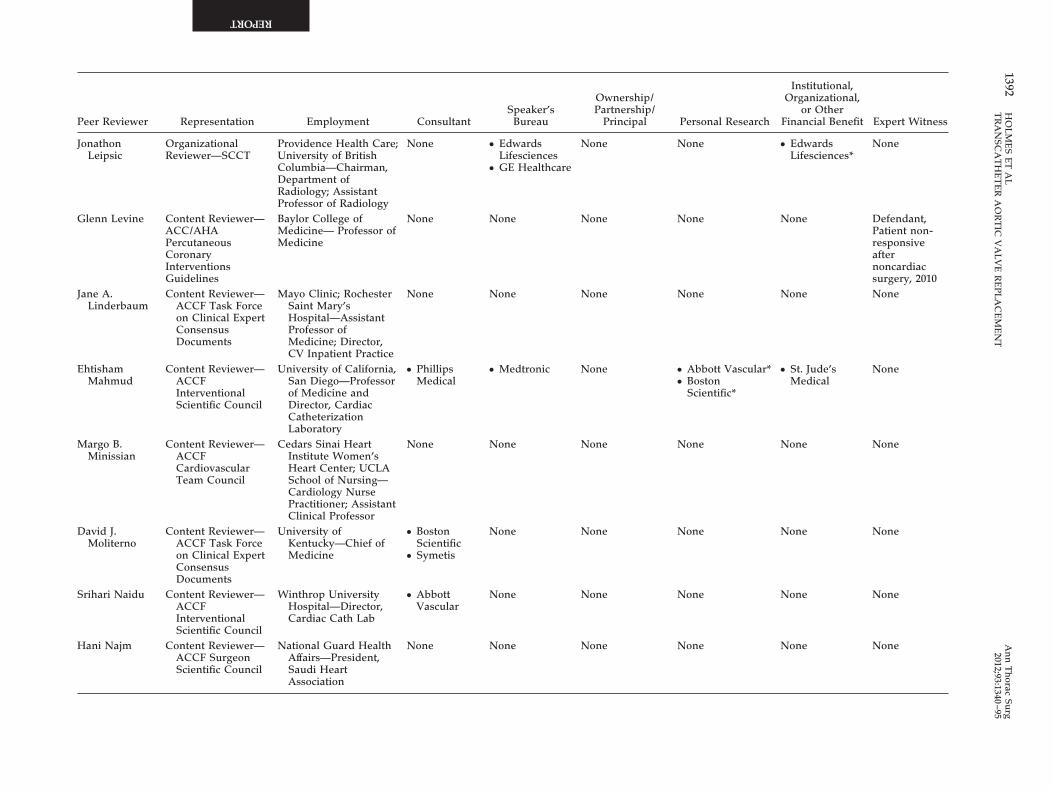
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
JonathonLeipsic
OrganizationalReviewer—SCCT
Providence Health Care;University of BritishColumbia—Chairman,Department ofRadiology; AssistantProfessor of Radiology
None ● EdwardsLifesciences
● GE Healthcare
None None ● EdwardsLifesciences*
None
Glenn Levine Content Reviewer—ACC/AHAPercutaneousCoronaryInterventionsGuidelines
Baylor College ofMedicine— Professor ofMedicine
None None None None None Defendant,Patient non-responsiveafternoncardiacsurgery, 2010
Jane A.Linderbaum
Content Reviewer—ACCF Task Forceon Clinical ExpertConsensusDocuments
Mayo Clinic; RochesterSaint Mary’sHospital—AssistantProfessor ofMedicine; Director,CV Inpatient Practice
None None None None None None
EhtishamMahmud
Content Reviewer—ACCFInterventionalScientific Council
University of California,San Diego—Professorof Medicine andDirector, CardiacCatheterizationLaboratory
● PhillipsMedical
● Medtronic None ● Abbott Vascular*● Boston
Scientific*
● St. Jude’sMedical
None
Margo B.Minissian
Content Reviewer—ACCFCardiovascularTeam Council
Cedars Sinai HeartInstitute Women’sHeart Center; UCLASchool of Nursing—Cardiology NursePractitioner; AssistantClinical Professor
None None None None None None
David J.Moliterno
Content Reviewer—ACCF Task Forceon Clinical ExpertConsensusDocuments
University ofKentucky—Chief ofMedicine
● BostonScientific
● Symetis
None None None None None
Srihari Naidu Content Reviewer—ACCFInterventionalScientific Council
Winthrop UniversityHospital—Director,Cardiac Cath Lab
● AbbottVascular
None None None None None
Hani Najm Content Reviewer—ACCF SurgeonScientific Council
National Guard HealthAffairs—President,Saudi HeartAssociation
None None None None None None
1392H
OL
ME
SE
TA
LA
nn
Th
oracSu
rgT
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
2012;93:1340–95
REPORT

Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
Rick Nishimura Content Reviewer—ACC/AHAValvular HeartDiseaseGuidelines
Mayo Clinic, Division ofCardiovascularDisease—Judd andMary Morris LeightonProfessor of Medicine
None None None None None None
Amit R. Patel OrganizationalReviewer—SCMR
Chicago Department ofMedicine—Assistant Professor ofMedicine
None None None None None None
Stephen Ramee Official Reviewer—ACC Board ofGovernors
Ochsner ClinicFoundation—Director, CardiacCatheterization
None None ● AccessClosure*
● BostonScientific*
● Hot Spur*
● Abbott†● Boston
Scientific†● Edwards
Lifesciences†● Medtronic†
None None
PasalaRavichandran
Content Reviewer—ACCF SurgeonScientific Council& ACCF HeartFailure &TransplantCommittee
Oregon Health &Science University—Associate Professor
None None None None None None
Jack Shanewise OrganizationalReviewer—SCA
Columbia UniversityCollege of Physicians& Surgeons—Professor of ClinicalAnesthesiology
None None None None None Defendant,rupturedpulmonaryartery by PAcath, 2011
Defendant, airembolismduring heartsurgery, 2010
Plaintiff, failedendotrachealtube ex-change, 2011
William J.Stewart
OrganizationalReviewer—ASE
Cleveland ClinicFoundation—Professor of Medicine
None None None None ● EdwardsLifesciences†
None
1393A
nn
Th
oracSu
rgH
OL
ME
SE
TA
L2012;93:1340
–95T
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
REPORT
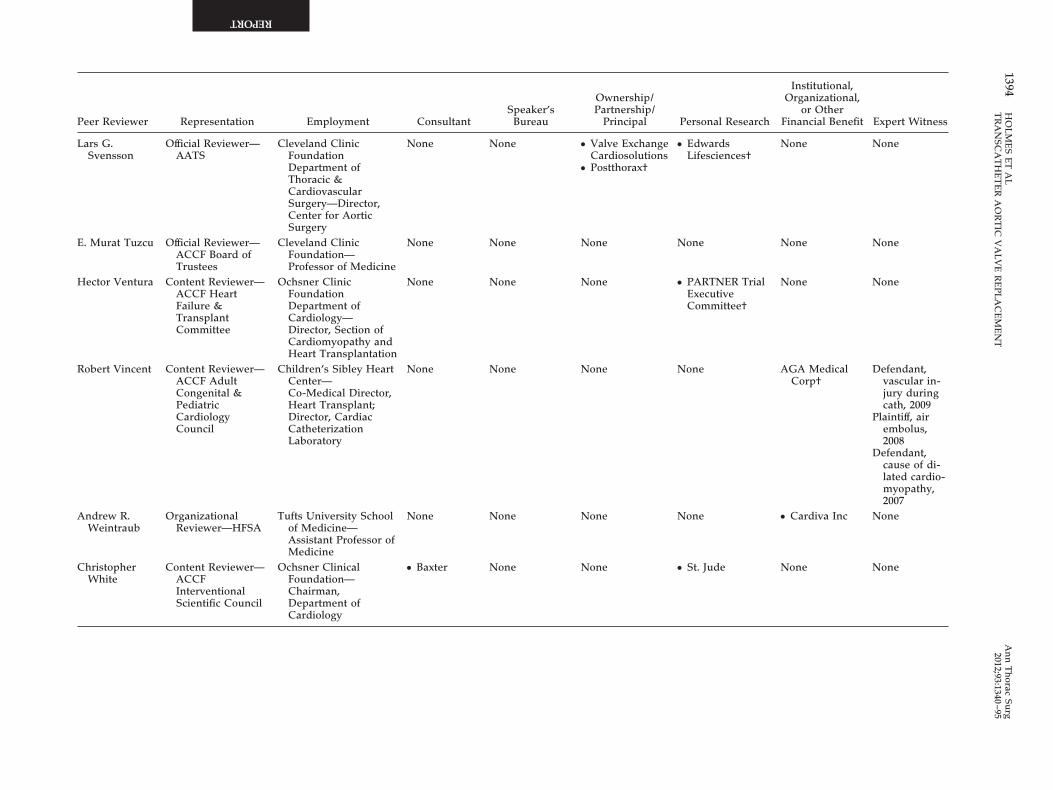
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
Lars G.Svensson
Official Reviewer—AATS
Cleveland ClinicFoundationDepartment ofThoracic &CardiovascularSurgery—Director,Center for AorticSurgery
None None ● Valve ExchangeCardiosolutions
● Postthorax†
● EdwardsLifesciences†
None None
E. Murat Tuzcu Official Reviewer—ACCF Board ofTrustees
Cleveland ClinicFoundation—Professor of Medicine
None None None None None None
Hector Ventura Content Reviewer—ACCF HeartFailure &TransplantCommittee
Ochsner ClinicFoundationDepartment ofCardiology—Director, Section ofCardiomyopathy andHeart Transplantation
None None None ● PARTNER TrialExecutiveCommittee†
None None
Robert Vincent Content Reviewer—ACCF AdultCongenital &PediatricCardiologyCouncil
Children’s Sibley HeartCenter—Co-Medical Director,Heart Transplant;Director, CardiacCatheterizationLaboratory
None None None None AGA MedicalCorp†
Defendant,vascular in-jury duringcath, 2009
Plaintiff, airembolus,2008
Defendant,cause of di-lated cardio-myopathy,2007
Andrew R.Weintraub
OrganizationalReviewer—HFSA
Tufts University Schoolof Medicine—Assistant Professor ofMedicine
None None None None ● Cardiva Inc None
ChristopherWhite
Content Reviewer—ACCFInterventionalScientific Council
Ochsner ClinicalFoundation—Chairman,Department ofCardiology
● Baxter None None ● St. Jude None None
1394H
OL
ME
SE
TA
LA
nn
Th
oracSu
rgT
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
2012;93:1340–95
REPORT
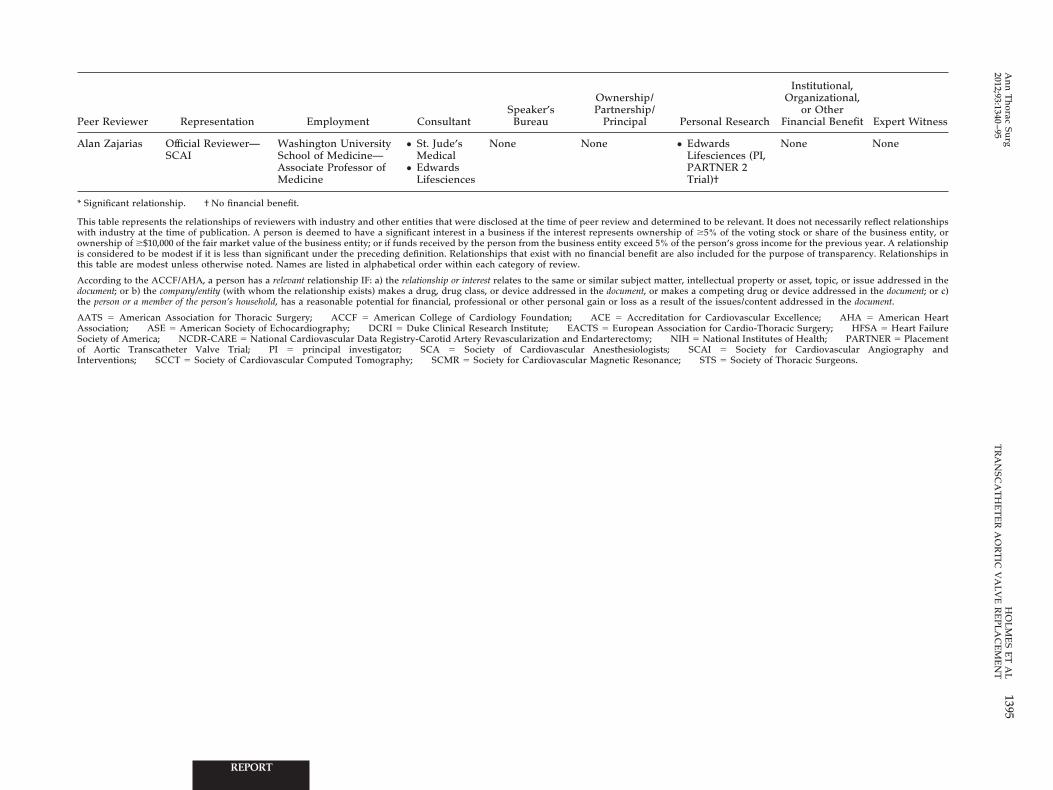
Research
Institutional,Organizational,
or OtherFinancial Benefit Expert Witness
snces (PI,ER 2
None None
e relevant. It does not necessarily reflect relationshipsof the voting stock or share of the business entity, orn’s gross income for the previous year. A relationshiped for the purpose of transparency. Relationships in
ual property or asset, topic, or issue addressed in theeting drug or device addressed in the document; or c)sues/content addressed in the document.
diovascular Excellence; AHA � American HeartCardio-Thoracic Surgery; HFSA � Heart Failure
onal Institutes of Health; PARTNER � PlacementSociety for Cardiovascular Angiography and
Society of Thoracic Surgeons.
1395A
nn
Th
oracSu
rgH
OL
ME
SE
TA
L2012;93:1340
–95T
RA
NSC
AT
HE
TE
RA
OR
TIC
VA
LV
ER
EP
LA
CE
ME
NT
Peer Reviewer Representation Employment ConsultantSpeaker’s
Bureau
Ownership/Partnership/
Principal Personal
Alan Zajarias Official Reviewer—SCAI
Washington UniversitySchool of Medicine—Associate Professor ofMedicine
● St. Jude’sMedical
● EdwardsLifesciences
None None ● EdwardLifesciePARTNTrial)†
* Significant relationship. † No financial benefit.
This table represents the relationships of reviewers with industry and other entities that were disclosed at the time of peer review and determined to bwith industry at the time of publication. A person is deemed to have a significant interest in a business if the interest represents ownership of �5%ownership of �$10,000 of the fair market value of the business entity; or if funds received by the person from the business entity exceed 5% of the persois considered to be modest if it is less than significant under the preceding definition. Relationships that exist with no financial benefit are also includthis table are modest unless otherwise noted. Names are listed in alphabetical order within each category of review.
According to the ACCF/AHA, a person has a relevant relationship IF: a) the relationship or interest relates to the same or similar subject matter, intellectdocument; or b) the company/entity (with whom the relationship exists) makes a drug, drug class, or device addressed in the document, or makes a compthe person or a member of the person’s household, has a reasonable potential for financial, professional or other personal gain or loss as a result of the is
AATS � American Association for Thoracic Surgery; ACCF � American College of Cardiology Foundation; ACE � Accreditation for CarAssociation; ASE � American Society of Echocardiography; DCRI � Duke Clinical Research Institute; EACTS � European Association forSociety of America; NCDR-CARE � National Cardiovascular Data Registry-Carotid Artery Revascularization and Endarterectomy; NIH � Natiof Aortic Transcatheter Valve Trial; PI � principal investigator; SCA � Society of Cardiovascular Anesthesiologists; SCAI �Interventions; SCCT � Society of Cardiovascular Computed Tomography; SCMR � Society for Cardiovascular Magnetic Resonance; STS �
REPORT




























