Embed Size (px)
Citation preview

2008© COPYRIGHT
Rare Coagulation Disorders: The Way Forward ATHN Data Summit 2008July 31, 2008Presenters: Donna DiMichele, M.D. and
Amy Shapiro, M.D.

2008© COPYRIGHT
2
The Need
• Patients with rare coagulation disorders (RCDs) need safe and effective therapies and deserve excellent long term health outcomes
– Many RCD patients still have no treatment options other than non-virally attenuated plasma products or non-specific PCC’s
– RCD patients may not have access to new product trials
• Industry sponsors and investigators need special incentives to develop products for and conduct trials on rare disease populations
2008© COPYRIGHT
3
Objectives
• Prioritize rare coagulation disorder-related initiatives for ATHN
• Explore the clinical need and current evidence base of support for RCD product development
• Begin to formulate a work plan for RCD data collection that ensures coordination among national and international efforts with the 3 primary goals of:
– Developing an evidence base for the clinical care of RCD patients
– Promoting and supporting RCD product development
– Stimulate clinical and basic research in this filed

2008© COPYRIGHT
4
ATHN’s Strategic Direction
Network Network InfrastructureInfrastructure
Data Data ManagementManagement
Public Health Public Health and Safetyand Safety
Outcomes Outcomes ImprovementImprovement
Data Analysis Data Analysis and Researchand Research
Data safety, back-up, and portability
Support surveillance and patient safety
Use data to drive quality, service, and patient centered care
Facilitate knowledge creation and advocacy
Develop electronic database capacity

2008© COPYRIGHT
5
ATHN’s Strategic Opportunities
Network Infrastructure
Develop electronic database capacity
• Gain and engage ATHN Affiliates re: database
• Build community trust
• Expand local capacity by funding and training data managers
• Establish regional data management structure
• Define and establish the core dataset: rare coagulation disorders

2008© COPYRIGHT
The Current State of Understanding :
RCD Epidemiology, Pathophysiology and Treatment Options

2008© COPYRIGHT
7
Rare Bleeding Disorders
Clotting Protein Disorders Platelet Defects
Fibrinogen
Prothrombin
Glanzmann Thrombasthenia
Factor V
Factor VII
Bernard Soulier Syndrome
Factor X Storage Pool Disease
Factor XI
Factor XIII
Combined Factors V & VIII
Combined Factors II, VII, IX, X
Connective Tissue Diseases
PAI – 1 Deficiency Collagen Defects

2008© COPYRIGHT
8
Rare Clotting Protein Disorders Prevalence
Rare Bleeding Disorders (Deficiencies of Factors II, VII, X, V, XIII, Fibrinogen & Dysfibrinogenemia)
Prevalence – 1 in 500,000 to 1 in 1,000,000 ( 0.0002%)
Iranian Registry
(RIBD)
UK Registry (HCDO)
Italian Registry
(AICE)
0.3 – 6.6% 0.02 – 3.3% 0.2 – 1.3%
Source: D DiMichele
2008© COPYRIGHT
9
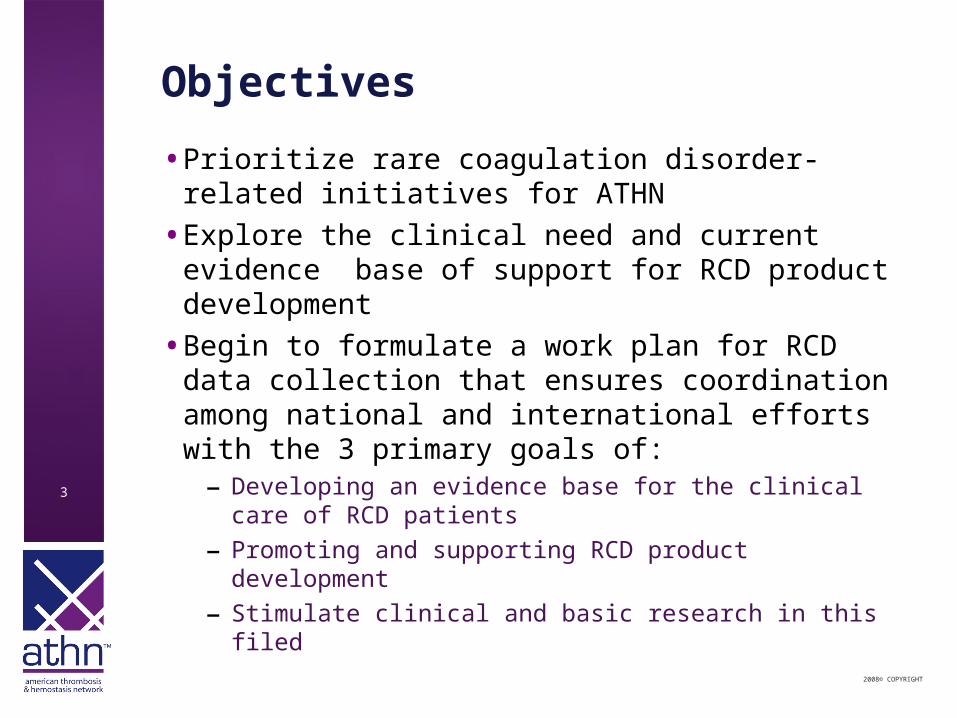
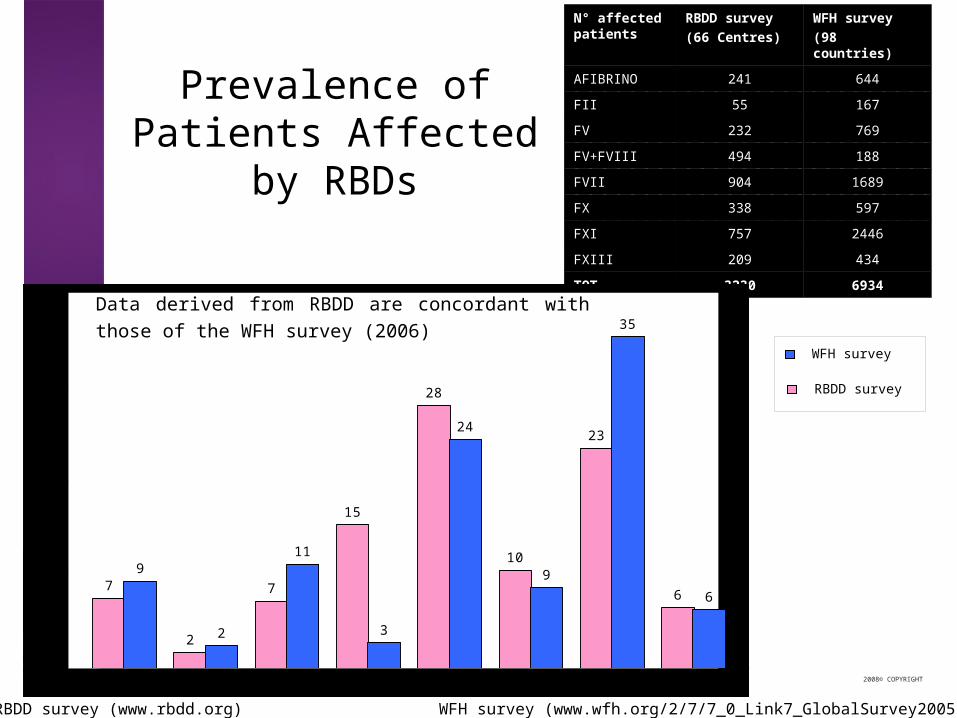
N° affected patients
RBDD survey(66 Centres)
WFH survey (98 countries)
AFIBRINO 241 644
FII 55 167
FV 232 769
FV+FVIII 494 188
FVII 904 1689
FX 338 597
FXI 757 2446
FXIII 209 434
TOT 3230 6934
Prevalence of Patients Affected by RBDs
WFH survey
RBDD survey
WFH survey (www.wfh.org/2/7/7_0_Link7_GlobalSurvey2005.htm)
7
2
7
15
28
10
23
6
0
10
20
30
40
FIBRINOGEN FI I FV FV+FVI I I FVI I FX FXI FXI I I
9
2
11
3
24
9
35
6
0
10
20
30
40
FIBRINOGEN FI I FV FV+FVI I I FVI I FX FXI FXI I I
Data derived from RBDD are concordant with those of the WFH survey (2006)
RBDD survey (www.rbdd.org)
2008© COPYRIGHT
10
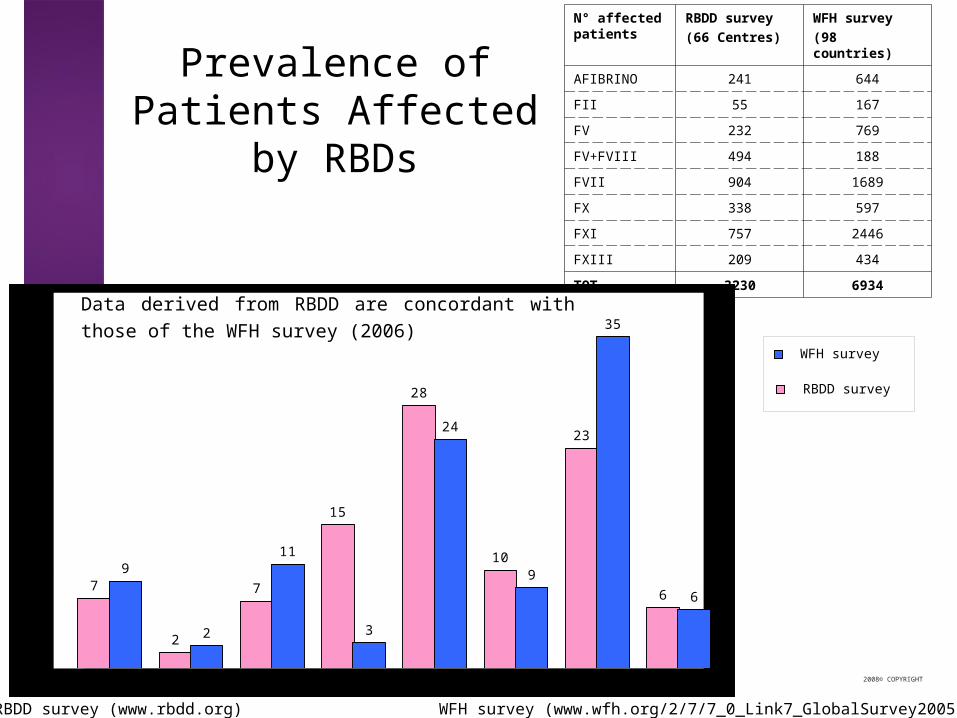
RBD distribution from National Registry data
reported during the SSC 2006-2007
F. Peyvandi
I ran
FII2% FV
10%
FV+FVIII15%
FVII31%
FX10%
FXI9%
FXIII13%
Fibrinogen10%
EMRO e Africa
FII1%
FV30%
FV+FVIII2%
FVII18%
FX13%
FXI19%
FXIII9%
Fibrinogen8%
Central and South America
FV7%
FV+FVIII4%
FVII23%
FX13%
FXI29%
FXIII3% FII
11%
Fibrinogen10%
France
FII0%
FV14%
FV+FVIII0%
FVII29%
FX5%
FXI25%
FXIII12%
Fibrinogen15%
UK
FVII19%
FX7%
FXI61%
FV4%
FII0%
Fibrinogen7%
FXIII2%
FV+FVIII0%
India
FV11%
FV+FVIII12%
FVII13%
FX10%
FXI2%
FXIII31%
FII4%
Fibrinogen37%Egypt
Fibrinogen23%
FII0%
FV29%
FVII12%
FX14%
FXI19%
FXIII2%
FV+FVIII1%
2008© COPYRIGHT
11
N° affected patients
RBDD survey(66 Centres)
WFH survey (98 countries)
AFIBRINO 241 644
FII 55 167
FV 232 769
FV+FVIII 494 188
FVII 904 1689
FX 338 597
FXI 757 2446
FXIII 209 434
TOT 3230 6934
Prevalence of Patients Affected by RBDs
WFH survey
RBDD survey
WFH survey (www.wfh.org/2/7/7_0_Link7_GlobalSurvey2005.htm)
7
2
7
15
28
10
23
6
0
10
20
30
40
FIBRINOGEN FI I FV FV+FVI I I FVI I FX FXI FXI I I
9
2
11
3
24
9
35
6
0
10
20
30
40
FIBRINOGEN FI I FV FV+FVI I I FVI I FX FXI FXI I I
Data derived from RBDD are concordant with those of the WFH survey (2006)
RBDD survey (www.rbdd.org)

2008© COPYRIGHT
12
Distribution Results (Families)
Fibrinogen17%
FI I5%
FV12%
FV+FVI I I13%
FVI I25%
FX16%
FXI11%
FXI I I1%
82%77%
55%
75%
7%
82%
73%
14%
3%
16%
5%
22%
6%
13%
5%
20%
29%
20%
71%
12% 13%
0
10
20
30
40
50
60
70
80
90
FII FV FV+FVIII FVII FX FXI FXIII
severe
moderate
mild
DEFICIENCYN° OF
PROBANDSN° OF
FAMILIES
FIBRINOGEN 55 50
FII 16 15
FV 39 36
FV+FVIII 42 34
FVII 81 69
FX 52 43
FXI 35 32
FXII 2 1
FXIII 35 34
TOTAL 357 314

2008© COPYRIGHT
13
Clinical Manifestations
FVIII Fibrinogen FII FV FVII FV+FVIII FX FXIIIFXI
Nose bleeding
Uterine bleeding
Haematuria
GI bleeding
Joint bleeding
Muscle bleeding
CNS bleeding
Cord bleeding
Post-partum, -operation bleeding
Oral cavity bleeding
15%
25%
13%
75%
81%
16%
75%
90%
0%
0%
60%70% 64% 72%57% 77%
75% 50%
60% 50% 35% 50% 58%
7% 10% 25% 6%
15% 14% 38% 10% 6% 7%
38% 50%
21% 69% 55%26% 25%
38% 12% 66% 58%29%
7%5% 17% 9% 25% 6%
15%75% 28% 73% 3% 22%
23% 40% 55% 84%43%
46%70% 66%57% 51%
48%
32%
10%
7%
4%
0%
0%
0%
0%
0%
20%
8%
0%
29%
32%
0%
63%
55%
34%
3%

2008© COPYRIGHT
14
North American Rare Bleeding Disorder Registry ( NARBDR)
• HTC’s U.S. and Canada (26% RR)
• 94 / 3809 – (2.4%) adults
• 200 / 4583 - (4.4%) children
• Age: 0-73 yrs (median – 7 yrs)
• Family history - 50%
• Gene studies - 5.4%
0
20
40
60
80
100
120
II
VII X V
XII
I
FB
N
Dys
FB
N
To
tal
Pe
rce
nta
ge
of
Pa
tie
nts
Hetero
Homo
(135)
(4
II(16)
XIII(32)
FBN(16)
DysF(13)
VII
X (37)
V(35)
Source: Acharya et al. J. Thromb Haemost 2000;2:248

2008© COPYRIGHT
15
N.A. Rare Bleeding Disorders Registry Ethnicity and Rare Factor Deficiencies
Caucasian
(%)
AA
(%)
Latino
(%)
Asian
(%)
Others
(%)
% US Dem 76 12 8.2* 3 0.8
% RBD 61 13 19* 2 5
*p < 0.00001
Source: D DiMichele

2008© COPYRIGHT
16
N.A. Rare Bleeding Disorders RegistryDisease Related Complications*
Anemia MS CNS Other None
Factor II (Homo)
49 17 11 0 23
Factor VII (Homo)
19 18 2 0 61
Factor X(Homo)
34 7 22 0 37
Factor V(Homo)
36 23 9 0 32
Factor XIII 24 15 15 2 44
Afibrin 0 23 22 0 56
DysFBN 0 10 0 0 60
Source: D DiMichele *Numbers refer to % of each group with the symptoms

2008© COPYRIGHT
17
• For the rare factor deficiencies fresh frozen plasma and cryoprecipitate infusions have been the primary therapeutic strategy for the treatment or prevention of bleeding episodes.
• This treatment modality has disadvantages– potential viral contamination – volume overload – allergic reactions
Rare Bleeding Disorders: General Treatment Principles
(Source: D DiMichele)
2008© COPYRIGHT
18
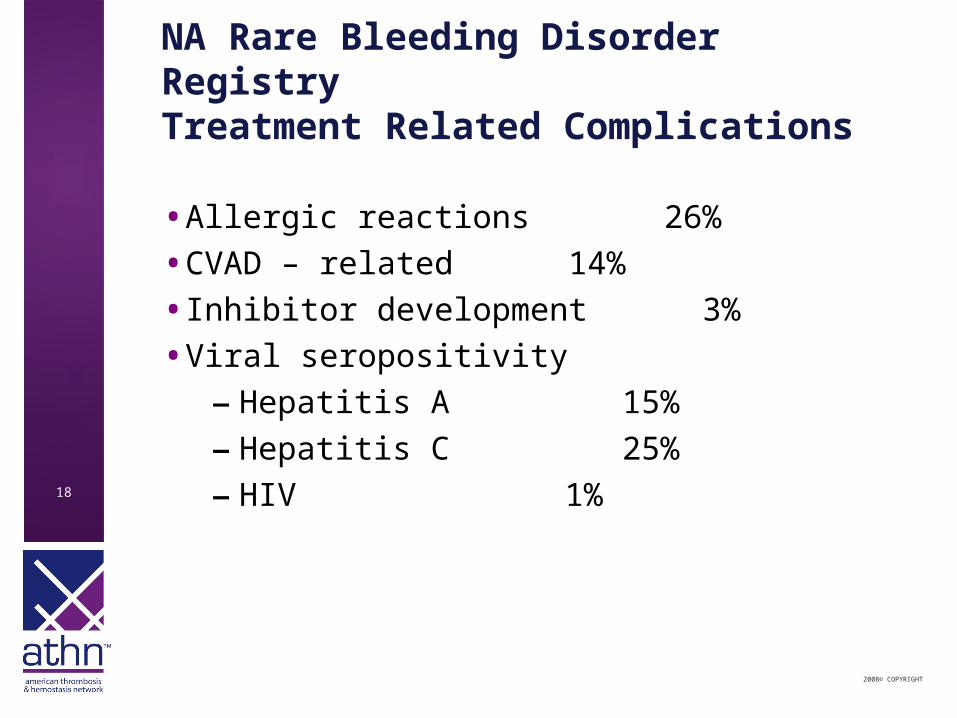
NA Rare Bleeding Disorder RegistryTreatment Related Complications
• Allergic reactions 26%
• CVAD – related 14%
• Inhibitor development 3%
• Viral seropositivity
– Hepatitis A 15%
– Hepatitis C 25%
– HIV 1%

2008© COPYRIGHT
19
Summary of Factor Replacement
Factor
Deficiency
FFP Platelets Cryo Plasma Concen-
trate
Prothrom-bin
Complex
Recom-binant Factor
Fibrinogen X X X X (study only)
Prothrombin X X
Factor V X X
Factor VII X X (not US) X
Factor X X X
Factor XI X X (not US)
Factor XIII X X X (study only)
X (study only)
Source: D DiMichele

2008© COPYRIGHT
20
New Product Development: Underway but Challenging
• Fibrinogen concentrate (Haemocomplettan; CSL- Behring)
• FXIII concentrate (Fibrogammin ( CSL- B); rFXIII (NovoNordisk)
• FXI concentrate (HemEleven; LFB)
• FX concentrate (BPL)
• FV concentrate (Kedrion)
• Possibly, plasminogen
Source: D. DiMichele

2008© COPYRIGHT
21
Rare Platelet Disorders

2008© COPYRIGHT
22
Collagen Defects

2008© COPYRIGHT
23
Need for Standardized Data
• Demonstrate service delivery.
• Better understand the epidemiology, clinical presentation, genetics and natural history of the disorders;
• Facilitate the development of standards of care;
• Support advocacy for drug development;
• Identify population subsets for special study;
• Identify subjects eligible for clinical trials of new products;
• Aid in post-marketing surveillance;
• Analyze clinical outcomes;
• Identify care providers with patients to facilitate communication & networking;

2008© COPYRIGHT
24
Proportion of Patients in UDC
Factor Deficiency
In HTCs In UDC Percent
Factor I 89 29 33%
Factor II 49 16 33%
Factor V 148 62 42%
Factor VII 615 218 35%
Factor X 94 39 41%
Factor XI 520 144 28%
Factor XIII 97 64 66%
Source: CDC Division of Blood Disorders, Updated July, 2008

2008© COPYRIGHT
25
RBD UDC Working Group
• Collaboration of the Lab Tracker (web) development to ultimately capture and report data to RDB UDC working group
– Formed July 2007; Multi-disciplinary
– Work on data collection forms started in August 2007 (demographics; diagnosis; bleeding manifestations; treatment; complications)
– Coordination with the CC and CDC grant research priorities (Diane Nugent, Chair)

2008© COPYRIGHT
ATHN Initiatives :
Present and Future

2008© COPYRIGHT
27
ATHN Roles and Activities:Stewardship of A Secure National Database
• Present platform: Lab Tracker
• Conversion to web based system
• Server housed at CDC
02040
6080
100
Hemophili
aVW
D
Other
Ble
edin
g
Throm
botic
Plate
let D
isord
ers
Carrie
rs
Other
% of HTC Lab Tracker Users
(Based on 61 users of the 78 responding HTCs)
85% 64%
Patient Types Entered into Lab Tracker
2008© COPYRIGHT
28
ATHN Roles and Activities:Coagulation Disorder Resource Room
• Planned link from ATHN to NHF, WFH and NATT web sites to help disseminate peer-reviewed information to providers, researchers and patients
– Spearheaded by Amy Shapiro MD
– 17 manuscripts (e.g., clinical manifestations, treatments, diagnostic testing, etc.)
– Publication date Sept. – Nov. 2008
– All manuscripts in final stages of review & revisions

2008© COPYRIGHT
29
ATHN Role and Activities:Rare Disorders Projects
• Plasminogen registry– In process
• International harmonization– Exploring data sharing/interface with EN-RBD
• Development of a data collection module & training more specific to rare disorders for national database
– Just starting

2008© COPYRIGHT
30
U.S. Rare Bleeding and Clotting Disorder Database Pilot Project
• ATHN funded by Baxter for next 2 years
• Uses the infrastructure funded by Novo Nordisk
• The purpose is to support the development and testing of standardized data collection and supporting components for rare coagulation factor deficiencies that is compatible with the ATHN infrastructure.
• Conference call held May 08 to discuss plans
• Members of MASAC RDB subcommittee included

2008© COPYRIGHT
31
Three Components to the Grant
• Rare coagulation deficiency standardized data collection
– Review existing data collection efforts;
– Identify data elements for rare disorders;
– Validate applicability of existing data fields in Lab Tracker (web)
– Integrate changes to Lab Tracker (web) data dictionary and data collection templates
• National system for patient identifier
• Portal for development of data collection forms
2008© COPYRIGHT
32
Desire to Collaborate and Harmonize
• HDS Reporting
• UDC Women Study, Rare Bleeding Disorder Group
• Rare Bleeding Disorder Resource Room
• EN-RBD approach
• ISTH RBD Working Group
• World Federation of Hemophilia efforts
• Others

2008© COPYRIGHT
33
Example Disease Specific TemplatePlasminogen Activator Inhibitor 1 (PAI-1) DeficiencyRegistration Form - Draft
• Demographics• Diagnosis (phenotypic and genotypic)
• Birth history (gestation, method of delivery, therapy, complications)
• Bleeding history (symptoms, provider intervention)
• Reproductive/gynecologic history (gynecologic abnormalities, menses, pregnancy)
• Other health impairments• Treatment history (product, dose, frequency, regimen, first
exposure, home infusion)
• Complications (anemia, infection, musculoskeletal, allergies, death)
Source: A. Shapiro

2008© COPYRIGHT
34
European Network on Rare Bleeding Disorders (EN-RBD)
• Type and severity of deficiency• Demographics• Family• Bleeding manifestation and treatment (frequency,
localization, duration, trigger, treatment, outcome, prophylaxis, complications)
• Surgery management (major/minor/delivery type, age, bleeding type, duration, treatment, outcome, prophylaxis, complications)
• Other associated diseases• Phenotype studies• Molecular defect / Polymorphisms
Source: F. Peyvandi

2008© COPYRIGHT
Beginnings of a Work Plan:
Journey Initiated

2008© COPYRIGHT
36
Advance The Web-Based Infrastructure
• ATHN should enable centers to collect the full spectrum of historical and cross sectional data needed to:
– Care for patients and anticipate their issues– Design studies– Enroll patients in studies– Complete study requirements– Track impact of interventions on care
• To get started, ATHN can provide guidance to centers to maximize the benefit

2008© COPYRIGHT
37
Staging Rare Disorder Data Collection
Stage Goal
1. How many patients?
Identify patients with rare disorders
2. Who’s served?
Gather what’s needed for HDS report
3. What if disaster strikes?
Other info for the emergency preparedness flash drive
4. Where is public health at risk?
(UDC specific measures in development)
5. What outcomes?
Specific disease management templates and research

2008© COPYRIGHT
38
Staging Rare Disorder Data Collection
Stage Data Types
1. How many patients?
Demographics; diagnosis; deaths
2. Who’s served?
Clinical presentation; factor level; visit date, type and disposition; co-morbidities; presence of inhibitor; genetic or acquired
3. What if disaster strikes?
Contacts, treatment type, dose and instructions; allergies; warnings; insurance
4. Where is public health at risk?
(UDC specific measures in development)
5. What outcomes?
Cause of death; lab tests; outcome measures; pregnancies/fertility; genetic mutations; risk factors; adverse events; surgeries, infusions, new product trials and long term surveillance, etc.

2008© COPYRIGHT
39
Synchronize with CDC
• Enter data into Lab Tracker today
• Encourage sites to start enrolling rare coagulation disorder patients in UDC
• Encourage CDC Coordinating Committee to include in the Data Sharing Agreement under development, the ability to share data with ATHN to facilitate study coordination and site recruitment through ATHN

2008© COPYRIGHT
40
Aid Implementation by Study Sites
• ATHN should aid HTCs and other potential study sites with implementation of studies
– Communications network to share knowledge of studies
– Database to identify subjects for study– Access to central IRB– Standardized templates for consent/data capture– Patients flags in Lab Tracker for easy reference – Ability to re-use data once captured– Funding to help cover costs

2008© COPYRIGHT
41
Help Companies Coordinate Studies
• ATHN should begin to build capacity to help companies coordinate studies in the U.S.
– Refer to experts to frame studies
– Identification of study sites
– Active tracking of site interest
– Data to help define data points
– Outcomes data to determine that the product is working
– Aid in post-marketing surveillance