Embed Size (px)
Citation preview

Antihypertensive Drugs
PHR 242: Pharmacy Pharmacology
William B. Jeffries, Ph.D
Room 570A Criss III
280-4092
Email: [email protected]
flap.creighton.edu

Definition
Elevation of arterial blood pressure above 140/90 mm Hg. Can be caused by:
• an underlying disease process (secondary hypertension)
• Renal artery stenosis• Hyperaldosteronism• pheochromocytoma
• idiopathic process (primary or essential hypertension)

Mortality Is Related to Blood Pressure

JNC VI Stages of Hypertension
Stage Diastolic Range (mm Hg)
Systolic Range (mm Hg)
High Normal
85-89 130-139
Stage 1 90-99 140-159
Stage 2 100-109 160-179
Stage 3 > 109 >179

Treatment Rationale
Short-term goal of antihypertensive therapy:
Reduce blood pressure
• Primary (essential) hypertension• Secondary hypertension

Treatment Rationale
Long-term goal of antihypertensive therapy:Reduce mortality due to hypertension-induced disease
Stroke Congestive heart failure Coronary artery disease Nephropathy Peripheral artery disease Retinopathy

Ways of Lowering Blood Pressure
Reduce cardiac output (ß-blockers, Ca2+ channel blockers)
Reduce plasma volume (diuretics)
Reduce peripheral vascular resistance (vasodilators)
MAP = CO X TPR

Major Risk Factors That Increase Mortality in Hypertension
Smoking Dyslipidemias Diabetes Mellitus Age >60 Gender: men, postmenopausal women Family history

"Individualized Care"
Risk factors consideredMonotherapy is institutedNon pharmacological therapy tried firstConsiderations for choice of initial
monotherapy: Renin status Coexisting cardiovascular conditions Other conditions

Treatment Thresholds for Essential Hypertension
Stages Risk group A(no major risk factors, no target organ damage)
Risk Group BOne or more major risk factors (except diabetes), no organ damage
Risk Group CTarget organ damage and/or diabetes
High Normal
Lifestyle Modification
Lifestyle Modification
Lifestyle Modification and Drug Therapy
Stage 1 Lifestyle Modification (up to 12 months)
Lifestyle Modification and Drug Therapy
Lifestyle Modification and Drug Therapy
Stages 2 and 3
Lifestyle Modification and Drug Therapy
Lifestyle Modification and Drug Therapy
Lifestyle Modification and Drug Therapy

Monotherapy for Hypertension
• ACE inhibitors and ATII antagonists• Diuretics• ß-adrenoceptor blockers• α1-adrenoceptor blockers
• Ca2+ channel blockers

Benzothiazide Diuretics
Mechanism of action Indications
– Monotherapy for mild-moderate HTN– Adjunct agent– Usually necessary in severe HTN

Thiazide diuretics: considerations
Long-term hypokalemia appears to increase mortality.
K-sparing diuretics are superior to K supplementation when diuretics used.
Most efficacious in “low renin” or volume-expanded forms of hypertension

ß-Adrenoceptor blockers
Mechanism of Action:ß-adrenoceptor antagonism
Why blood pressure reduction?– Reduction of Cardiac output– Reduction of renin release– Central nervous system - reduction of sympathetic
outflow

Types of ß-blockers:
Non selectivePrototype: Propranolol (others: nadolol, timolol, pindolol,
labetolol)
CardioselectivePrototype: Metoprolol (others: atenolol, esmolol, betaxolol)
Non selective and cardioselective ß-blockers are EQUALLYEQUALLY effective in reducing blood pressure

Other Properties Relevant to Antihypertensive Effect:
Intrinsic sympathomimetic activity. Mixed antagonism.

Therapeutic Use in Hypertension
Monotherapy most effective in high renin
hypertension hypertension with coronary
insufficiency low cost to patient

Administration
Blah Blah Blah

Adverse Effects
Bradycardia Heart failure Bronchospasm Coldness of extremities Withdrawal effects Glucose metabolism

5. Adverse Effects (Cont)
CNS effects Pregnancy Rise in plasma triglyceride concentration;
decrease in HDL cholesterol Drug interactions:
– NSAID'S - can blunt effect of ß-blockers – Epinephrine - causes severe hypertension in
presence of ß-blockade – Ca2+channel blockers Conduction effects on heart
are additive w/ ß blockers.

α-Adrenoceptor Blockers
Mechanism of action: blockade of vascular α−adrenoceptors
Non selective (α1 and α2) blockers: Phentolamine, phenoxybenzamine and dibenamine
Selective (α1) prototype: prazosin (others: terazosin, doxazosin, trimazosin)

Therapeutic Use in Hypertension
Non selective (α1 and α2) blockers: used for treatment of hypertensive crises in pheochromocytoma
Selective (α1) blockers Monotherapy Adjunctive therapy

Administration of α1-Adrenoceptor Blockers
Read The Book

Side effects of α1-adrenoceptor blockers
First dose phenomenon Tachycardia GI effects (rare)

Adverse Effects of Non Specific α-Adrenoceptor Blockers
Postural hypotension Reflex tachycardia Fluid retention

Other Sympatholytics
Guanethidine Ganglionic blockers

Guanethidine
Mechanism of action Therapeutic use

Ganglionic Blockers (Trimethaphan)
Mechanism of action Therapeutic use

Drugs Interacting With the Renin-angiotensin System
ACE inhibitors ATII antagonists
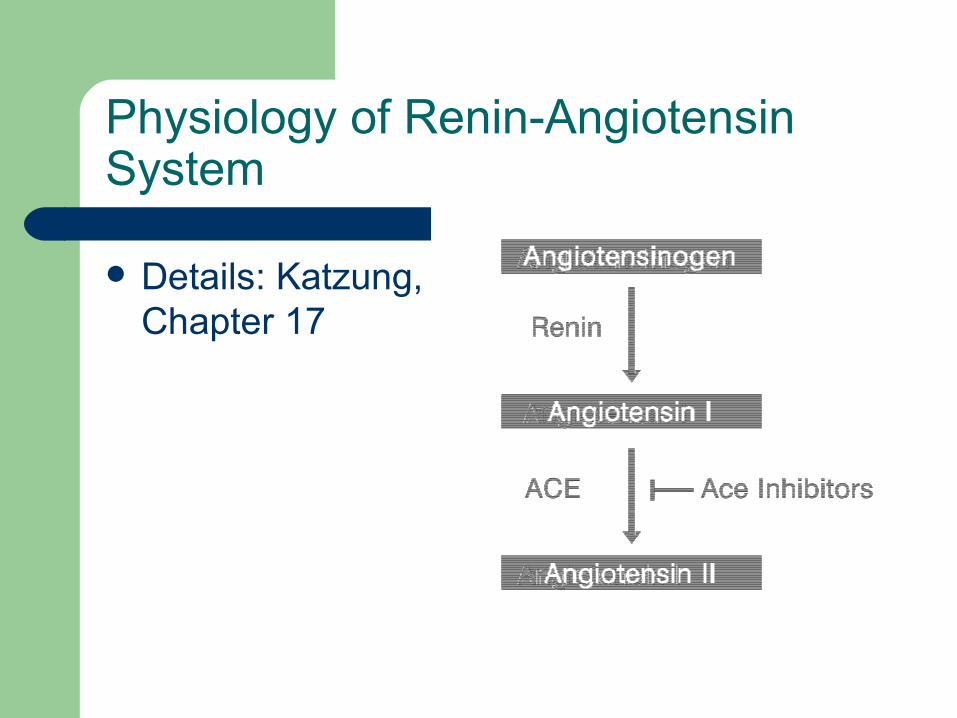
Physiology of Renin-Angiotensin System
Details: Katzung, Chapter 17

Receptor Subtypes for Angiotensin
AT1
– AT1A
– AT1B
– Prototype antagonist: Losartan
AT2 Primary antagonist available is PD123177
AT3?AT4
Angiotensin Converting Enzyme (ACE) Inhibitors
Mechanism of Action: Inhibition of angiotensin II formation
Competitive inhibition of angiotensin converting enzyme reduces circulating ang II, reducing vascular tone.

Systemic Effects of ACE Inhibitors
Reduction in systemic arteriolar resistance, systolic, diastolic and mean arterial pressure.
Regional hemodynamic effects: – Increased regional blood flow in proportion to
ang II sensitivity of the vascular bed – Increased large artery compliance– Cardiac output and heart rate unchanged
Aldosterone secretion reduced

Types of ACE Inhibitors
Active molecules: Captopril, Lisinopril, Enalaprilat
Prodrugs: Enalapril, Benazepril, Fosinopril, Quinapril, Ramipril, Moexipril, Spirapril

Therapeutic Uses in Hypertension
One of the initial choices for monotherapy of mild to moderate hypertension
Well tolerated as monotherapy. Drugs of choice in diabetes mellitus with hypertension
Most effective in high renin hypertension More effective in white vs. Black patients Excellent for patients with concomitant congestive
heart failure, LVH, cardiac arrhythmias or diabetes mellitus, consider in asthma instead of ß-blockers
Efficacy enhanced by diuretics
Administration
Captopril Prodrugs: inactive prodrug is hydrolyzed
in vivo to active compound, e.g., enalapril to enalaprilat
Lisinopril

ACE Inhibitor Adverse Reactions
Hypotension Renal insufficiency Cough Hyperkalemia Hyperreninemia

Minor Adverse Effects of ACE Inhibitors
Ageusia Skin rash Proteinuria Neutropenia

Pharmacology of AT-Receptor Antagonists
Losartan Valsartan Candesartan *sartan

Mechanism of Action of ATII Antagonists
Molecular: Competitive inhibitor of AT1 receptors. Blocks ability of angiotensins II and III to stimulate pressor and cell proliferative effects
Antihypertensive effects
Cell growth effects
Lack of “bradykinin” effects

Clinical Indications for ATII Antagonists
Hypertension Heart failure Prevention of restenosis following angioplasty

Ca2+ Channel Blockers
One of the initial choices for monotherapy of mild to moderate hypertension
all CEB's are equally effective when used as monotherapy for Stage 1 hypertension
Verapamil and diltiazem are vasodilators that do not cause reflex tachycardia due to direct inhibition of cardiac automaticity
Best in low renin hypertension: Blacks and elderly do not cause fluid retention

Hydralazine
Direct acting vasodilator: liberates NO from vascular endothelium which stimulates the production of cGMP in vascular smooth muscle, resulting in relaxation (arterioles > veins)
Can NOT be used for monotherapy Bioavailability dependent on genetic factors (fast or slow
acetylators) Tachycardia with palpitations, hypotension OFTEN Lupus-like syndrome may occur with chronic use that is reversible
upon continuation Never use as first choice; Try in refractory hypertension as part of
a multidrug regimen

Minoxidil
Prodrug of minoxidil N-O sulfate, which is a direct acting vasodilator
Mechanism: K+ channel opener, causes membrane hyperpolarization, reducing ability of smooth muscle to contract.
Other K channel openers: pinacidil, diazoxide
refractory hypertension Long duration of action (>24 hours)

Minoxidil Adverse Effects
Fluid and water retention: can lead to pulmonary hypertension
Tachycardia and increased cardiac output: can progress to congestive heart failure
Hypertrichosis: Occurs in all patients who take therapeutic doses of minoxidil for a prolonged time

Centrally Acting Sympatholytics: α2-Adrenoceptor Agonists
α−Methyldopa Clonidine Guanabenz Guanfacine

α2-Adrenoceptor Agonists Mechanisms of Action
Central Action: Stimulation of α2 adrenoceptors in the brainstem reduces sympathetic tone, causing a centrally mediated vasodilatation and reduction in heart rate
Prejunctional action: Stimulation of α2 adrenoceptors located prejunctionally on peripheral neurons reduces norepinephrine release
Vascular smooth muscle: α2 adrenoceptors located on vascular smooth muscle open Ca2+ channels and cause vasoconstriction. Not evident clinically unless given intravenously

Mechanisms of Action (cont.)
Clonidine, guanabenz and guanfacine: Direct acting α2 adrenoceptor agonists.
α-methyldopa: Prodrug taken up by central adrenergic neurons and converted to the α2 adrenoceptor agonist α-methylnorepinephrine.

Therapeutic Uses in Hypertension
Not generally used for monotherapy of mild to moderate hypertension
Considerations– fluid retention: must use diuretic
– Direct acting α2 adrenoceptor agonists: effective in lowering blood pressure in ALL patients.
– Direct acting α2 adrenoceptor agonists are equally efficacious but more efficacious than α-methyldopa

Other Use
Clonidine is useful in diagnosis of pheochromocytoma. Clonidine (single 0.3 mg dose) will reduce plasma norepinephrine concentration to below 500 pg/ml in tumor-free patients.

Administration: α−Methyldopa
Short plasma half life (2 hours) but longer action (peak at 6-8 hours, duration 24 hours
• Once or twice daily dosing due to long action
• Action prolonged in patients with renal insufficiency

Administration: Clonidine, Guanabenz and Guanfacine
• Orally active, good absorption, usually given twice daily
• Clonidine: available as a sustained release transdermal patch (avoids withdrawal syndrome)

Adverse Effects of α 2-Adrenoceptor Agonists
Hypotension especially in volume depleted patients
Sedation: more prominent for direct acting α2 adrenoceptor agonists - 50% of patients
Withdrawal syndrome: hypertension, tachycardia, nervousness and excitement.

Adverse Effects Unique to Methyldopa:
Heart block (methyldopa) Immunological changes: positive Coombs test
(20% after 1 year), lupus like syndrome, leukopenia, red-cell aplasia
Altered liver function 5% Hyperthermia Reduced mental acuity

Adverse Effects of Clonidine, et al:
Dry mouth, nasal stuffiness Contact dermatitis with clonidine patch: 20% Vivid dreams Restlessness Depression (infrequent)

α 2-Adrenoceptor Agonist Drug Interactions
Diuretics enhance hypotensive action Tricyclic antidepressants inhibit clonidine's
action

Reserpine
Molecular mechanism of action: Inhibition of noradrenergic function.
Reserpine binds to storage vesicles and releases norepinephrine and serotonin.
Storage vesicles are destroyed and nerve ending loses capacity to store and release norepinephrine and serotonin
Pharmacological consequences: reduction of cardiac output and TPR

Reserpine
Extremely long acting Tolerated well (as well as diuretic plus
propranolol in Veteran's cooperative study) CNS effects:
– Sedation, loss of concentration – psychotic depression. Depression: insidious
progression that can lead to suicide





























